Back to Journals » Clinical Ophthalmology » Volume 19
Translation and Preliminary Validation of the Computer Vision Syndrome Scale-17 (CVSS-17) into Arabic: A Pilot Study
Authors Alfarhan H
Received 4 September 2025
Accepted for publication 27 November 2025
Published 13 December 2025 Volume 2025:19 Pages 4613—4621
DOI https://doi.org/10.2147/OPTH.S561486
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Haya Alfarhan
College of Applied Medical Sciences, Optometry Department, King Saud University, Riyadh, Saudi Arabia
Correspondence: Haya Alfarhan, King Saud University, College of Applied Medicine Science, Optometry Department, PO Box 145111, Riyadh, 4545, Kingdom of Saudi Arabia, Tel +966508381107, Email [email protected]
Purpose: To create and validate a culturally appropriate Arabic translation of the Computer Vision Syndrome Scale-17 (CVSS-17) for assessing computer vision syndrome (CVS) symptoms among Arabic-speaking populations.
Patients and Methods: Following established cross-cultural adaptation guidelines, the CVSS-17 was translated into Arabic by two independent translators, then reviewed by an interdisciplinary committee and back-translated. The questionnaire was administered to 60 healthy Arabic-speaking participants (aged 18– 40 years) across 2 sessions conducted 2– 5 days apart. The psychometric evaluation included internal consistency and test–retest reliability.
Results: The participants had an average age of 20.7 ± 1.3 years (45% male, 55% female), with mean CVSS-17 scores of 34.4 ± 11.0 (range: 20– 60). The Arabic CVSS-17 demonstrated excellent internal consistency (Cronbach’s α = 0.904, range: 0.890– 0.905) and test–retest reliability ranging from 0.50– 0.93, and item–retest correlations ranging from 0.57– 0.91 (p < 0.001). The floor and ceiling effects were minimal (1.7% each), indicating good discriminative ability.
Conclusion: The Arabic CVSS-17 demonstrated excellent reliability and internal consistency, highlighting its utility as a culturally appropriate screening tool for CVS symptoms in Arabic-speaking populations. The cultural adaptation of this questionnaire successfully maintains psychometric integrity and establishes a solid foundation for standardized CVS assessment research in Arabic-speaking regions.
Keywords: computer vision syndrome, CVSS-17, Arabic translation, validation, psychometric properties, digital eye strain
Introduction
The widespread use of digital technology has fundamentally transformed individuals’ daily visual habits, especially due to the increased screen time.1,2 This has contributed to the development of computer vision syndrome (CVS), wherein individuals experience ocular and visual symptoms both during and after prolonged use of digital devices. CVS presents with various symptoms, including eyestrain, headaches, dry eye sensation, blurred vision, diplopia, burning, itching, photophobia, and musculoskeletal discomfort.3
Its pathophysiology involves two mechanisms: accommodative and binocular vision stress result in internal symptoms, whereas ocular surface dysfunction secondary to altered blink dynamics and environmental factors cause external symptoms.4–6 There is substantial variation in the prevalence of CVS worldwide, ranging from 12% (95% confidence interval [CI]: 9–15%) in Japan7 to 99% (95% CI: 97–100%) in Pakistan,8 which could be attributed to differences in usage patterns, occupational requirements, and digital devices. Within Saudi Arabia, CVS has a reported prevalence of 43.5% to 95.1%,9,10 highlighting the significant burden in the region and the critical need for standardized assessment tools.
The Computer Vision Syndrome Scale-17 (CVSS-17) is a subjective tool that consists of 17 items divided into 2 factors: 1) external symptom factor (ESF, 11 items), which assesses ocular surface-related symptoms, and 2) internal symptom factor (ISF, 6 items), which evaluates accommodative and binocular vision-related manifestations.11,12 Each item is given a corresponding score (with a maximum score of either 4, 6, or 7), which is then totaled to calculate the final score. Psychometric validation of the original Spanish version has confirmed its excellent reliability and validity,11 with successful cross-cultural adaptations for English,13 Malaysian,14 and Italian15 populations. However, its cross-cultural validations have shown some factor structure variations. For example, the Malaysian version included 13 ESF items and 4 ISF items due to cultural and linguistic factors affecting symptom perception,14 whereas the Italian version maintained the original structure.
At present, there is no validated Arabic translation for the CVSS-17, thus hindering the use of this tool in 400 million Arabic speakers across 26 countries.16 This limits research capabilities, evidence-based screening programs, and even standardized CVS care provision. Clinicians in Arabic-speaking populations typically depend on objective examinations or unvalidated translations of questionnaires that can potentially compromise diagnostic accuracy and treatment monitoring. The Tear Film and Ocular Surface Society has emphasized the importance of standardized symptom questionnaires,17 highlighting the vital need for validated tools in various languages.
The increasing prevalence of digital device use in Arabic-speaking regions, alongside the absence of validated CVS assessment instruments in Arabic, represents urgent need both clinically and from a research standpoint. A culturally adapted, psychometrically validated CVSS-17 in Arabic can facilitate comprehensive prevalence studies, aid in systematic detection protocols, support multinational research initiatives, and provide clinicians with a standardized instrument for evaluating CVS. Accordingly, this study aimed to translate the CVSS17 into Arabic and assess its psychometric properties such as reliability, internal consistency, and test–retest stability. Ultimately, a successful translation can serve as an effective screening tool for dry eye symptoms in both clinical and research environments among Arabic speakers.
Methods
This observational, cross-sectional pilot study followed established guidelines for cross-cultural adaptation.18–20 Transaltion adhered to established guidelines18 (Figure 1). Two native Arabic-speaking professional translators independently translated the English CVSS-17 (Supplementary File 1) into Arabic. An interdisciplinary committee was formed, comprised of eight native Arabic-speaking cornea and ocular surface specialists that were professionally proficient in English. They reviewed both versions, compared them with the original, and established a consensus version through discussion. Backward translation was performed by a qualified native English speaker without knowledge of the original text. After two rounds of proofreading by the committee and an additional native Arabic-speaking translator proficient in English, the committee confirmed that the back-translated English version maintained conceptual equivalence with the original English CVSS-17, with no fundamental differences identified.
 |
Figure 1 Flowchart illustrating cross-cultural adaptation process for the Arabic translation of the Computer Vision Syndrome Scale-17 (CVSS-17). |
Tsang et al (2017) recommended 30–50 measurements for the initial assessment of new translations. Accordingly, 60 study participants were recruited; these were healthy, native Arabic speakers aged 18–40 years, representing a homogeneous population consistent with standard validation practices for pilot studies.20 This was done based on recommendations of Beaton et al (2000) and Sousa & Rojjanasrirat (2011) to reduce confounding variables and improve internal validity by ensuring that the observed differences were attributable to the instrument itself rather than confounding factors related to age.18,21 The exclusion criteria included contact lens use, history of systemic or ocular diseases, refractive surgery, and eyelid conditions affecting the ocular surface. An objective refraction was performed using a Topcon KR-800 autorefractor to determine the spherical equivalent refractive error for each participant prior to questionnaire administration.
The Arabic CVSS-17 was administered across 2 sessions conducted 2–5 days apart. Participants completed questionnaires independently without assistance. Disease severity was determined based on the total score, with higher levels indicating greater severity: Level 1 (17–22), Level 2 (23–28), Level 3 (29–35), Level 4 (36–42), and Level 5 (43–53).13 Participants provided written informed consent, with the right to withdraw maintained throughout. The study was conducted in accordance with the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board, King Saud University (approval number: E-23-7931).
Statistical Analysis
Descriptive statistics included means, standard deviations, medians, interquartile ranges, and skewness. Floor and ceiling effects >15% were considered problematic in terms of discriminative ability.22 Internal consistency was evaluated using Cronbach’s alpha and 95% CIs, with ≥0.7 considered adequate.23 Item–total correlations were calculated to assess the individual contributions of each item to scale reliability. Test–retest reliability was assessed using intraclass correlation coefficients (ICC) and Spearman correlations with the corresponding interpretations: very low, ≤0.2; low, 0.2–0.4; moderate, 0.4–0.6; good, 0.6–0.8; and excellent, ≥0.8.24 Agreement between test sessions was evaluated via Bland–Altman analysis with a calculation of the mean difference and limits of agreement. Statistical significance was set at p < 0.05, with analyses performed using SPSS version 29.0.
Results
The questionnaire was completed by 60 participants (27 men [45%] and 33 women [55%]) with a mean age of 20.7 ± 1.3 years. The mean spherical equivalent for the right eye was −0.92 ± 1.90 diopters, indicating mild myopia. The average daily digital device usage was 5.5 ± 2.9 hours, with a cumulative experience of 9.7 ± 4.5 years and a short average rest time of 1.3 ± 2.2 hours.
The mean total CVSS-17 score was 34.0 ± 11.0 (range: 20–63). The individual item scores ranged from 1.13 ± 0.39 to 2.78 ± 1.68, with skewness values from −0.20 to 3.21. Floor and ceiling effects (both 1.7%) were minimal and well within acceptable limits (<15%), indicating excellent discriminative ability. Notably, 96.6% of participants scored within the functional range. The distribution of clinical severity revealed strong discriminative ability across all five levels, with observed patterns confirming the ability of the tool to stratify CVS severity levels for clinical assessment and intervention (Figure 2).
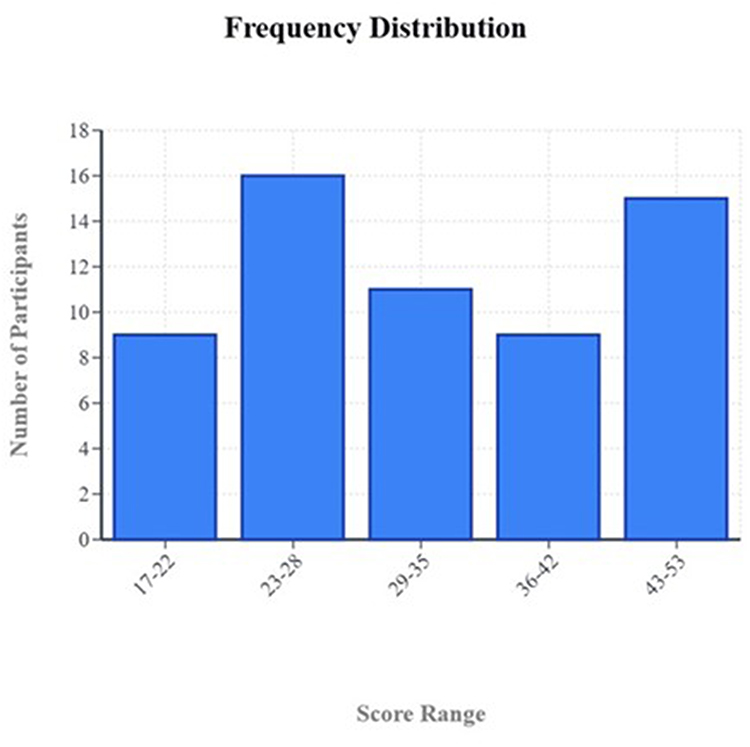 |
Figure 2 Distribution of Computer Vision Syndrome Scale-17 (CVSS-17) severity levels among study participants, demonstrating discriminative ability across five clinical severity categories. |
Spearman correlation coefficients were calculated to evaluate the strength of the relationship between repeated questionnaire measurements. Strong positive correlations were seen across all items, with an average of 0.77 (range: 0.57–0.91, p < 0.001). All correlations were statistically significant (p < 0.001), indicating substantial consistency in the participants’ responses over time (Table 1). Most items (82.4%) demonstrated correlations above 0.70, suggesting acceptable to excellent reliability for repeated measurement applications. Bland–Altman analysis also confirmed acceptable agreement between test sessions, with a mean difference of 0.40 in the total score which fell within the limits of agreement (−6.40 to 7.20) (Figure 3), indicating good agreement between observations.
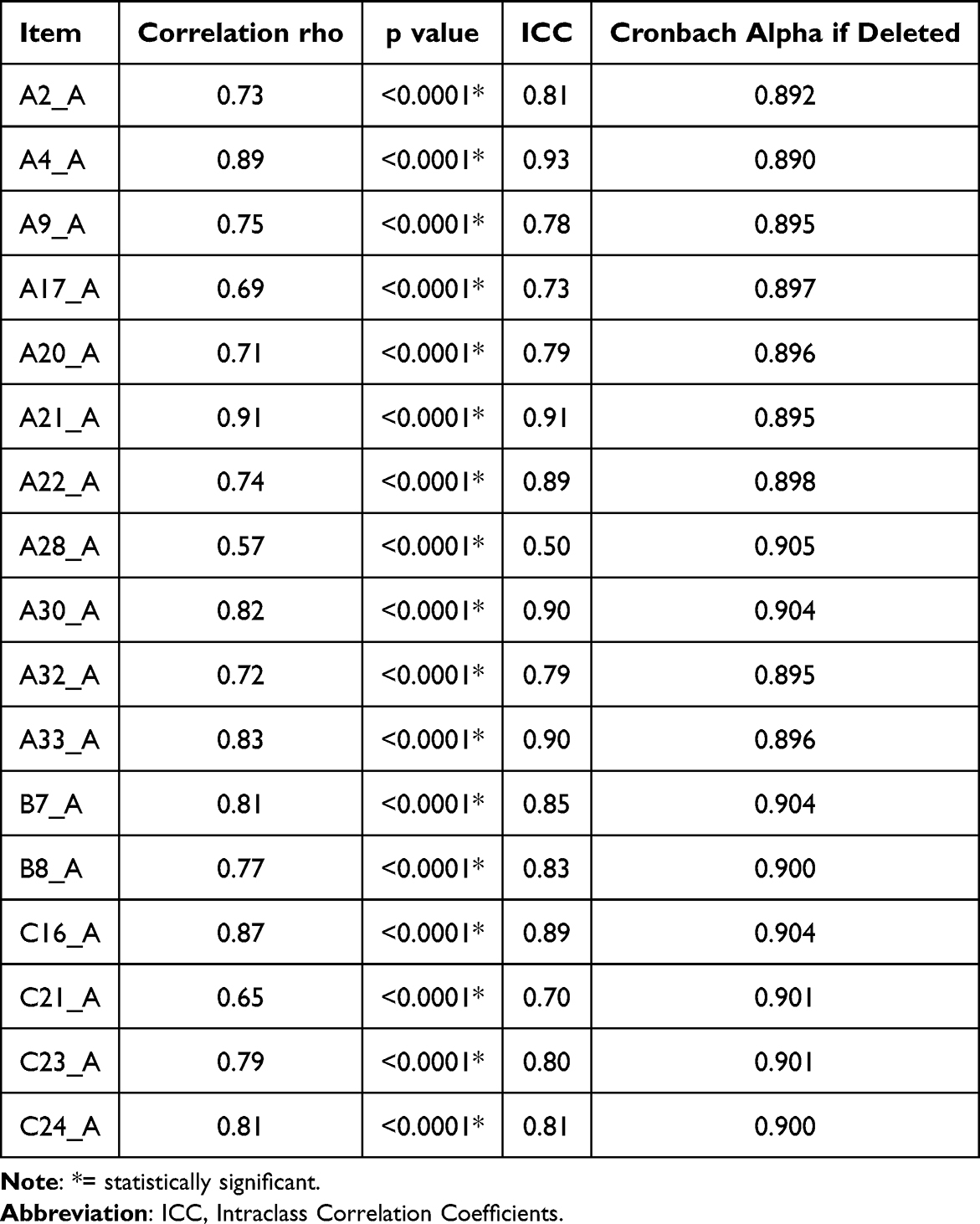 |
Table 1 Psychometric properties of the Arabic Computer Virsion Syndrome Sacle-17: Internal consistency, test-retest reliability, and item- total corrlations (n= 60) |
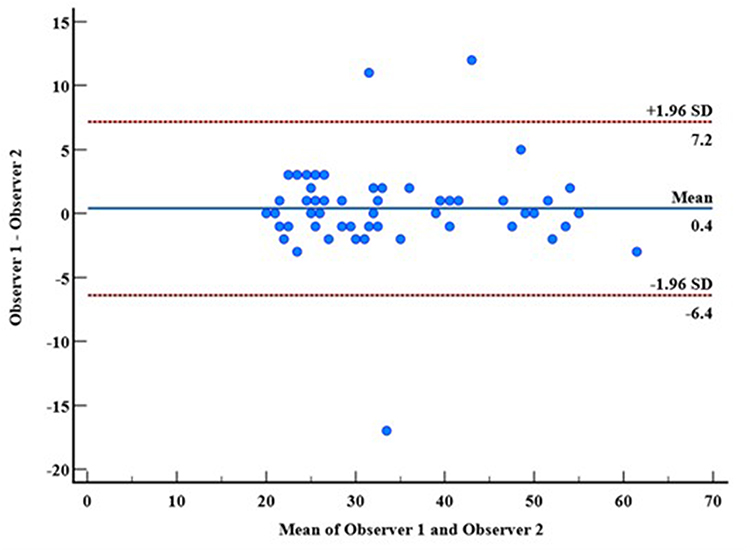 |
Figure 3 Bland–Altman plot showing agreement between test and retest measurements of the Arabic Computer Vision Syndrome Scale-17 (CVSS-17) total scores, with mean difference and limits of agreement. |
The overall ICC was 0.81 (range: 0.50–0.93), indicating variable levels of inter-rater reliability across items. Excellent reliability was demonstrated by 4 variables: A4A (ICC = 0.93), A21A (ICC = 0.91), A30A (ICC = 0.90), and A33A (ICC = 0.90). Meanwhile, good reliability was seen in 10 variables (ICC = 0.75–0.89), while moderate reliability was seen in 3 variables (ICC = 0.50–0.74). Overall, 82.4% of the variables achieved good-to-excellent inter-rater reliability (ICC ≥ 0.75), indicating acceptable agreement between observers for the majority of questionnaire items (Table 1).
The Arabic CVSS-17 demonstrated excellent internal consistency (Cronbach’s α = 0.904, range: 0.890–0.905). The removal of any individual item resulted in only a minimal change in Cronbach’s alpha (range: 0.890–0.905), indicating that all items meaningfully contributed to the reliability of the scale (Table 1).
Discussion
This validation study demonstrated the robust psychometric properties of the Arabic translation of the CVSS-17. This aligns well with previous international validations, while revealing some characteristics unique to the studied Arabic-speaking population.
The study population (20.7 ± 1.3 years, 55% female) represents a younger demographic compared to other validation studies. The Italian CVSS-17 validation study included participants with a mean age of 42.7 ± 15.3 years,1 while the English validation included participants with a mean age of 38.57 years (range: 18–65 years).2 The predominantly young adult sample in the present study reflects contemporary digital device usage patterns among university-age Arabic populations.
In this study, the average daily digital device use was 5.5 ± 2.9 hours, similar to the Mexican study reporting a mean exposure of 5.96 ± 2.5 hours per day.25 This consistency across different populations suggests universal patterns of computer usage in academic and professional settings. Notably, the Mexican study found significant correlations between computer exposure time and dry eye disease tests, revealing a negative correlation between exposure and tear break-up time (rho −0.463, p < 0.001).25 This highlights the clinical relevance of measuring computer usage duration.
The translation process proceeded smoothly, likely due to the semantic precision of Arabic vocabulary in conveying the meaning of the original CVSS-17. By contrast, the Malaysian validation study documented significant linguistic challenges that necessitated substantial structural modifications, including reallocation of items between domains.14 These cross-cultural variations exemplify how linguistic characteristics influence questionnaire adaptation. The straightforward Arabic translation enabled preservation of the original factorial structure without requiring item modifications, whereas languages with different lexical characteristics may require more extensive adaptations to maintain conceptual equivalence and psychometric validity.
The Arabic CVSS-17 demonstrated excellent psychometric properties across all reliability measures. Internal consistency was excellent (α = 0.904, range: 0.890–0.905) and comparable to that of other validated translations: Spanish11 (α = 0.902), Malaysian14 (α = 0.867), and Italian15 (α = 0.925). The preservation of the original factorial structure without requiring item reallocation between domains may have contributed to maintaining psychometric integrity. The minimal impact of removing individual items on Cronbach’s alpha confirms that all items contributed meaningfully to scale reliability.
The Arabic version demonstrated good temporal stability, with comprehensive reliability analysis revealing item–total correlations of 0.77 and test–retest ICC of 0.81, which is comparable to that of the Spanish version11 (ICC = 0.85) and Malaysian version14 (ICC = 0.87). The differences observed across studies may reflect variations in sample size and study methodology.26,27 Bland–Altman analysis confirmed acceptable measurement agreement (mean difference = 0.40), similar to the English version13 (mean difference = 0.42), indicating consistent measurement precision.
The Arabic CVSS-17 demonstrates promising psychometric properties for Arabic-speaking populations. Its excellent reliability in this pilot study supports its potential utility for standardized screening and symptom monitoring in research contexts. As the first validated CVS assessment tool for over 400 million Arabic speakers, it provides a foundation for inclusion in international research initiatives and standardized symptom evaluation across Arabic-speaking regions, pending further validation in larger and more diverse samples.
Limitations
This study only included healthy participants aged 18–40 years, thus limiting its generalizability to older adults and clinical populations with CVS. The pilot sample size (n = 60) had an insufficient number of participants for demographic comparisons, precluding a stratified subgroup analysis. The homogeneous participant demographics also restrict its external validity across diverse Arabic-speaking populations. Lastly, validation was conducted without clinically diagnosed CVS patients or objective accommodative measures, thus limiting the criterion validity assessment.
Future Research
Before clinical implementation can be recommended, future studies are needed to complete the validation process. A confirmatory factor analysis with a larger sample size (n ≥ 150–200) and diverse age groups is essential to verify that the factorial structure of the Arabic CVSS-17 matches the original instrument, confirming its cross-cultural validity. Demonstrating structural equivalence across languages is a fundamental requirement for international comparability, and it ensures that the Arabic version measures the same underlying constructs as the validated versions in other languages. Additionally, validation in patients clinically diagnosed with CVS with objective accommodative testing is needed to establish criterion validity. Once structural and criterion validity are confirmed, the tool can then be used to explore potential population-specific variations in CVS symptom patterns among Arabic-speaking populations.
Conclusion
This pilot study successfully established the first Arabic translation of the CVSS-17, which demonstrates excellent reliability and internal consistency, indicating its measurement stability and clinical potential. This culturally appropriate and psychometrically sound tool enables the standardized assessment of CVS among Arabic-speaking populations. This opens opportunities for research and establishes a solid foundation for comprehensive validation studies. Future validation in larger, more diverse samples can further enhance its clinical applicability and diagnostic precision. This represents a significant advancement in regional ophthalmology capabilities and contributes to global CVS research standardization, ultimately advancing evidence-based eye care for a major global population.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request, subject to appropriate ethical approval and data protection regulations. The study was approved by the Institutional Review Board Sub-Committee, Health Sciences Colleges Research on Human Subjects, King Saud University (approval number: E-23-7931).
Acknowledgments
The author would like to express sincere gratitude to the eight cornea and ocular surface specialists who served on the interdisciplinary committee for their valuable expertise in reviewing the Arabic translation. Special thanks to the professional translators who conducted the forward and back-translation processes with meticulous attention to cultural and linguistic nuances. The author acknowledges the 60 study participants for their time and cooperation in completing the validation testing.
Author Contributions
Haya Al Farhan, the author, made a significant contribution to the work reported in the conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting, revising and critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agrees to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The author declares no conflicts of interest in relation to this study. No financial or personal relationships exist that could inappropriately influence the work presented in this paper.
References
1. Kaewpradit K, Ngamchaliew P, Buathong N. Digital screen time usage, prevalence of excessive digital screen time, and its association with mental health, sleep quality, and academic performance among Southern University students. Front Psychiatry. 2025;16:1535631. PMID: 40195967; PMCID: PMC11973388. doi:10.3389/fpsyt.2025.1535631
2. Devi KA, Singh SK. The hazards of excessive screen time: impacts on physical health, mental health, and overall well-being. J Educ Health Promot. 2023;12:413. PMID: 38333167; PMCID: PMC10852174. doi:10.4103/jehp.jehp_447_23
3. Parihar JK, Jain VK, Chaturvedi P, Kaushik J, Jain G, Parihar AK. Computer and visual display terminals (VDT) vision syndrome (CVDTS). Med J Armed Forces India. 2016;72(3):270–276. doi:10.1016/j.mjafi.2016.03.016
4. Alemayehu AM, Alemayehu MM. Pathophysiologic mechanisms of computer vision syndrome and its prevention: review. W J Opthalmol Vision Res. 2019;2(5). doi:10.33552/WJOVR.2019.02.000547
5. Kahal F, Al Darra A, Torbey A. Computer vision syndrome: a comprehensive literature review. Future Sci OA. 2025;11(1):2476923. PMID: 40055942; PMCID: PMC11901492. doi:10.1080/20565623.2025.2476923
6. Lema AK, Anbesu EW. Computer vision syndrome and its determinants: a systematic review and meta-analysis. SAGE Open Med. 2022;10:20503121221142402. PMID: 36518554; PMCID: PMC9743027. doi:10.1177/20503121221142402
7. Uchino M, Yokoi N, Uchino Y, et al. Prevalence of dry eye disease and its risk factors in visual display terminal users: the Osaka study. Am J Ophthalmol. 2013;156(4):759–766. doi:10.1016/j.ajo.2013.05.040
8. Noreen K, Ali K, Aftab K, Umar M. Computer vision syndrome (CVS) and its associated risk factors among undergraduate medical students in midst of COVID-19. Pakistan J Ophthalmol. 2021;37(1):102–108.
9. Al Subaie M, Al-Dossari S, Bougmiza MI. Computer vision syndrome among mobile phone users in Al-Ahsa, Kingdom of Saudi Arabia. Al-Basar Int J Ophthalmol. 2017;4(4):99–103. doi:10.4103/bijo.bijo_13_18
10. Abudawood GA, Ashi HM, Almarzouki NK. Computer vision syndrome among undergraduate medical students in King Abdulaziz University, Jeddah, Saudi Arabia. J Ophthalmol. 2020;2020:ArticleID2789376. doi:10.1155/2020/2789376
11. González-Pérez M, Susi R, Antona B, Barrio A, González E. The computer-vision symptom scale (CVSS17): development and initial validation. Invest Ophthalmol Visual Sci. 2014;55(7):4504–4511. doi:10.1167/iovs.13-13818
12. González-Pérez M, Susi R, Barrio A, Antona B. Five levels of performance and two subscales identified in the computer-vision symptom scale (CVSS17) by Rasch, factor, and discriminant analysis. PLoS One. 2018;13(8):e0202173. PMID: 30153272; PMCID: PMC6112632. doi:10.1371/journal.pone.0202173
13. González-Pérez M, Pérez-Garmendia C, Hoang K, et al. English version of the computer vision symptom scale (CVSS17): translation and Rasch analysis-based cultural adaptation. PLoS One. 2025;20(4):e0316936. PMID: 40238743; PMCID: PMC12002468. doi:10.1371/journal.pone.0316936
14. Md-Yasin M, Din NSS, Tharek Z, Abd Aziz NA, Mohamad M. Translation and validation of computer vision syndrome scale 17 (CVSS 17) -- The Malay version. IIUM Med J Malaysia. 2022;21(2). doi:10.31436/imjm.v21i2.1963
15. Rossi GCM, Bettio F, González-Pérez M, Briola A, Pasinetti GLM, Scudeller L. The 17-item computer vision symptom scale questionnaire (CVSS17): translation, validation and reliability of the Italian version. Int J Environ Res Public Health. 2022;19(5):2514. doi:10.3390/ijerph19052517
16. United Nations. Arabic Language Day. Available from: https://www.un.org/en/observances/arabiclanguageday#:~:text=2024%20Theme%20%E2%80%94%20Arabic%20Language%20and%20AI:,a%20global%20language%20with%20immense%20cultural%20significance.
17. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II diagnostic methodology report. Ocul Surf. 2017;15(3):539–574. PMID: 28736342. doi:10.1016/j.jtos.2017.05.001
18. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
19. Cruchinho P, López-Franco MD, Capelas ML, et al. Handovers4SafeCare. translation, cross-cultural adaptation, and validation of measurement instruments: a practical guideline for novice researchers. J Multidiscip Healthc. 2024;17:2701–2728. PMID: 38840704; PMCID: PMC11151507. doi:10.2147/JMDH.S419714
20. Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J Anaesthesia. 2017;11(5):80–89. doi:10.4103/sja.SJA_203_17
21. Sousa VD, Rojjanasrirat W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. J Eval Clin Pract. 2011;17(2):268–274. doi:10.1111/j.1365-2753.2010.01434.x
22. Terwee CB, Bot SD, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42. doi:10.1016/j.jclinepi.2006.03.012
23. Taber KS. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res Sci Educ. 2018;48:1273–1296. doi:10.1007/s11165-016-9602-2
24. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–63. Erratum in: J Chiropr Med. 2017 Dec;16(4):346. doi: 10.1016/j.jcm.2017.10.001. doi:10.1016/j.jcm.2017.01.0001
25. Sánchez-Valerio MDR, Mohamed-Noriega K, Zamora-Ginez I, Baez Duarte BG, Vallejo-Ruiz V. Dry eye disease association with computer exposure time among subjects with computer vision syndrome. Clin Ophthalmol. 2020;14:4311–4317. doi:10.2147/OPTH.S252889
26. Deo N, Nagrale P. Dry eye disease: an overview of its risk factors, diagnosis, and prevalence by age, sex, and race. Cureus. 2024;16(2):e54028. doi:10.7759/cureus.54028
27. Normie L. Older people, computers, and ethnicity – an academic research backwater? Gerontechnology. 2003;2(4):285–288. doi:10.4017/GT.2003.02.04.001.00
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Spotlight on Digital Eye Strain
Mylona I, Glynatsis MN, Floros GD, Kandarakis S
Clinical Optometry 2023, 15:29-36
Published Date: 27 February 2023
Prevalence of Digital Eye Strain Among University Students and Its Association with Virtual Learning During the COVID-19 Pandemic
AlQarni AM, AlAbdulKader AM, Alghamdi AN, Altayeb J, Jabaan R, Assaf L, Alanazi RA
Clinical Ophthalmology 2023, 17:1755-1768
Published Date: 20 June 2023
Digital Eye Strain: Updated Perspectives
Pucker AD, Kerr AM, Sanderson J, Lievens C
Clinical Optometry 2024, 16:233-246
Published Date: 18 September 2024
Validation of the Thai Version of the Chronic Pain Acceptance Questionnaire-8 (CPAQ-8T) in Chronic Pain Patients
Pasutharnchat K, Seangrung R, Lertmongkonaksorn P, Kamdeang S
Journal of Pain Research 2025, 18:947-957
Published Date: 26 February 2025
From the Ocular Surface to Neurophysiology: An Integrative Review of Digital Eye Strain

Manna P
Clinical Optometry 2026, 18:586750
Published Date: 3 March 2026