")
Back to Journals » Clinical Ophthalmology » Volume 17
Prevalence of Digital Eye Strain Among University Students and Its Association with Virtual Learning During the COVID-19 Pandemic
Authors AlQarni AM , AlAbdulKader AM , Alghamdi AN, Altayeb J , Jabaan R , Assaf L , Alanazi RA
Received 2 February 2023
Accepted for publication 12 June 2023
Published 20 June 2023 Volume 2023:17 Pages 1755—1768
DOI https://doi.org/10.2147/OPTH.S406032
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Amani M AlQarni,1 Assim M AlAbdulKader,1 Asma N Alghamdi,2 Jumana Altayeb,2 Raghad Jabaan,2 Lujain Assaf,3 Rawan A Alanazi1
1Family and Community Medicine Department, King Fahd Hospital of the University, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 2Medical Intern, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 3Epidemiology Senior Specialist, Clinical Leadership, Center for National Health Insurance, Riyadh, Saudi Arabia
Correspondence: Rawan A Alanazi, Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman bin Faisal University, P.O. Box 77134, Khobar, 31952, Saudi Arabia, Tel +966556999190, Email [email protected]
Introduction: The prolonged use of digital devices is a major risk factor for digital eye strain (DES) syndrome.
Aim: To estimate the prevalence of DES symptoms among students at Imam Abdulrahman University who use digital devices for virtual learning and leisure activities.
Methods: This was a retrospective cross-sectional study conducted by asking medical students of Imam Abdulrahman bin Faisal University to complete a self-administered online questionnaire. The questionnaire was used to determine the effect of the hours spent on digital devices and other factors, such as screen distance and not using artificial tears, on the development of DES. The severity (moderate or severe) and frequency (occasionally, always, or never) of 16 eye strain-related symptoms, including eye pain, headache, and itching, were evaluated by using the Computer Vision Syndrome Questionnaire.
Results: The overall prevalence of DES in the sample was found to be 68.53%. The largest proportion of students were found to have mild DES (43.20%), and only 11% had severe DES. The most common symptoms reported in our sample were headache, dryness, and burning. Female gender, using smartphones for online classes, and not using eye lubricants were significantly associated with increased severity of DES.
Conclusion: In the wake of the COVID-19 pandemic, virtual learning has become an integral part of education, leading to increased use of digital technology. The aim of this study was to investigate the impact of virtual learning on eye strain and to determine the prevalence and effects of DES. A questionnaire was administered to participants, and the findings revealed a DES prevalence of 68.53%. The use of eye drops for lubrication and smartphones for classes was significantly associated with DES. Furthermore, females were found to be more susceptible to severe DES symptoms than males. The development of a tool such as the Computer Vision Syndrome Questionnaire to predict DES prevalence could reduce clinic time and resources by minimizing unnecessary follow-up and ophthalmology referrals.
Keywords: digital eye strain, digital devices, computer vision syndrome, virtual learning
Introduction
The use of electronic devices has markedly increased in the last few years among all age groups. Prolonged screen time results in a noticeable impact on vision. During the COVID-19 pandemic period, the time spent on digital screens increased with the shift to virtual learning. Hence, students tend to suffer from a condition known as digital eye strain (DES). The American Optometric Association defines DES as “a complex of eye and vision problems related to activities, which stress the near vision and which are experienced in relation or during the use of computer.”1 The prevalence of DES has been estimated to be above 50% among prolonged screen users in most of the literature, with a high incidence of DES in the lockdown period accordingly.2–18
DES symptoms include blurred vision, eye dryness, burning eyes, lacrimation, eye redness, and headache1. The sustained state of focusing and refocusing creates ophthalmic muscle fatigue and causes accommodative symptoms related to DES. Reduced blink rate and horizontal gaze both increase the surface area of the cornea and result in evaporative dry eye.2 The extent of digital learning’s impact on vision depends on the screen time, the body posture adopted, the type of device, the brightness and distance of the screen, and the lighting conditions in the room.1 Having uncorrected refractive errors, wearing contact lenses (which are associated with an increased risk of dry eye and cause friction on the eye surface area), having a history of eye disease, being a female (due to the use of cosmetic products that cause eye irritation and, as mentioned in Bahkir et al study, the fact that females have a higher incidence of dry eye), and having diabetes or autoimmune diseases increase the risk of developing more severe symptoms of DES.2,12,19
The extensive use of digital devices in teaching and learning during the pandemic necessitated an evaluation of the disorder’s effect on the students. Although symptoms are usually transient, the condition can be severe and interferes with concentration and academic performance.3 Recent studies are reviewed in our research to present data and information on the use of digital devices, the prevalence of DES, risk factors, and protective measures.
Aim
The aim of this study was to estimate the prevalence of DES among medical field students at Imam Abdulrahman bin Faisal University who participated in virtual learning during the COVID-19 pandemic.
Method
Study Setting and Participants
Our inclusion criteria were medical students 18 years of age or older who were taking online classes. The exclusion criteria were a) students suffering from amblyopia, conjunctivitis, eye infection, strabismus, glaucoma, or cataract and b) students suffering from preexisting medical conditions, such as arthritis or hypertension.
Procedure and Ethical Considerations
Approval from the Imam Abdulrahman bin Faisal ethical committee was obtained. In addition, all participants chose to complete the survey of their own free will and were fully informed about the essential elements of the research project.
Prior to completing the survey, participants were given an informed consent form that included details about the research study, such as the research statement and purpose. Furthermore, the confidentiality of the subjects was protected.
The study was performed following the standards of the 1964 Helsinki Declaration and its later amendments.
Measures
The symptoms and severity of DES were measured by using the Computer Vision Syndrome Questionnaire (CVS-Q) developed by Segui et al.2 The severity (moderate or severe) and frequency (occasionally, always, or never) of 16 eye strain-related symptoms (eye pain, headache, itching, burning, foreign body sensation, watering, excessive blinking, double vision, vision worsening, eyelid heaviness, dryness, blurred vision, colored halos, near vision difficulty, light intolerance, and redness) were evaluated by using the CVS-Q.5,6
Statistical Analysis
The data were entered initially into Excel. After counterchecking and data cleaning, STATA software version 17 was used to analyze the data. Frequencies with proportions were used to describe the categorical variables, and the continuous variable was presented as standard deviation and mean. The chi-square test was used to investigate the association between participants with and without DES in relation to several risk factors. Moreover, to create a model of the relationship between the three DES groups and predictor variables, ordinal logistic regression was used. The strength of the association was displayed as the odds ratio. Furthermore, multivariate analysis was chosen as a method to adjust for suspected confounding factors. P-value < 0.05 was considered statistically significant.
Results
A total of 750 participants were included in the analysis. The study subjects were aged between 18 and 27, with a mean age of 21.6. Most students were females (60%) versus males (40%), and the majority of them were in their third academic year (27.6%), followed by fourth-year students (20%). Students in their second year were the least observed in the sample, constituting only 13.20%. With regard to preexisting eye conditions, nearly half of the participants reported having myopia at baseline (47.60%). In contrast, amblyopia and strabismus were the least detected among students, each recording below 3% (2.93% and 1.87%, respectively). The overall prevalence of DES in the sample was found to be 68.53%. The largest proportion of students were found to have mild DES (43.20%), and only 11% had severe DES (Table 1).
 |
Table 1 Participants’ Demographic Characteristics and Prevalence of DES |
With respect to eye risk factors and their relationship with DES, only the use of eye drops for lubrication was significantly associated with DES (P = 0.004; Table 2). Furthermore, using a smartphone for classes was found to be significantly associated with DES (P = 0.002; Table 3).
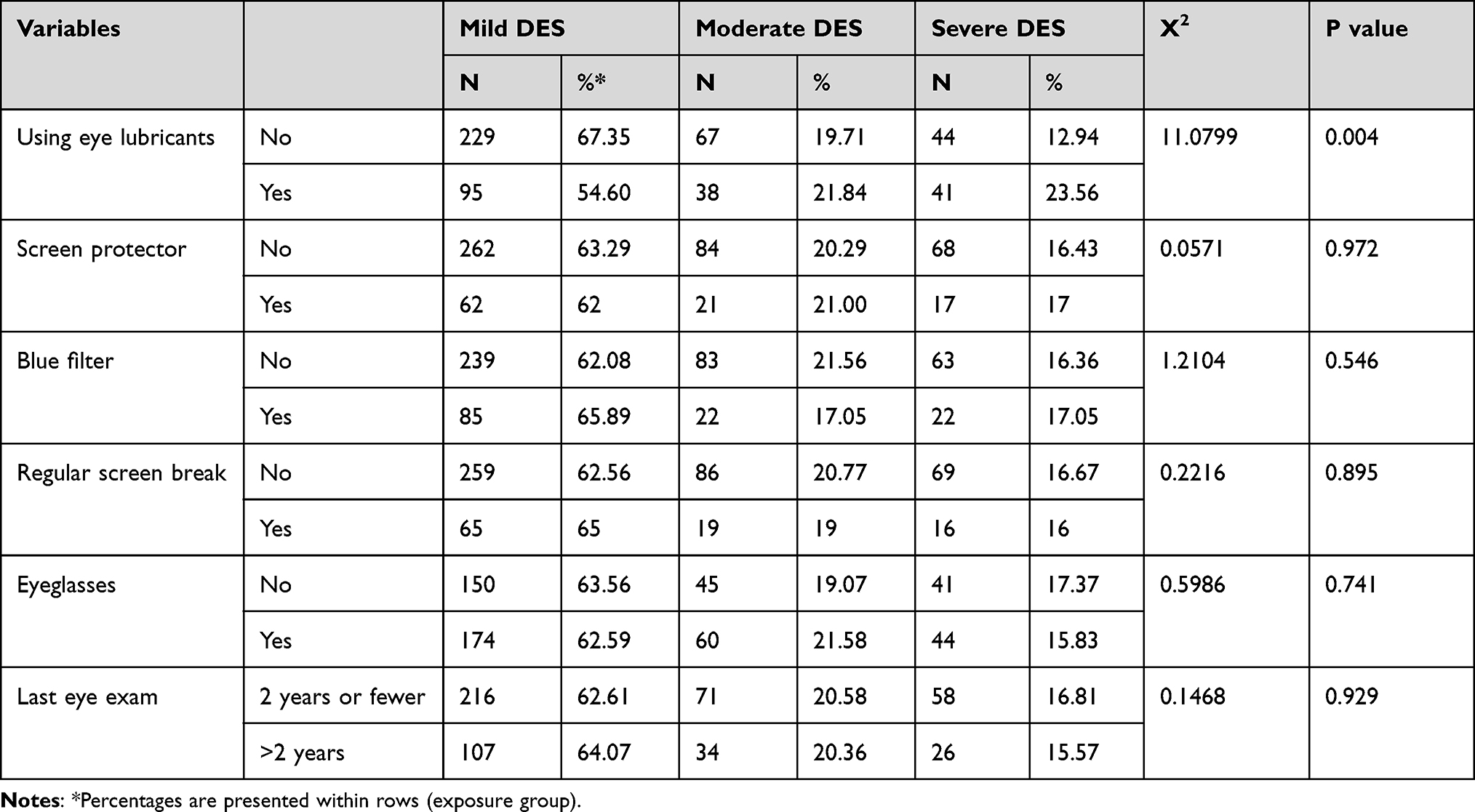 |
Table 2 Distributions of Eye Risk Factors in Relation to DES Symptom Severity |
 |
Table 3 The Distribution of Online Learning Risk Factors in Relation to Digital Eye Strain Symptom Severity |
The most common reported symptoms in the current study included headache (n = 423), dryness (n = 408), and burning (n = 405), whereas the least reported symptoms were having double vision (n = 89) and observing halos around objects (n = 149). Figures 1–17 shows the frequency of students reporting different CVS-Q symptoms in terms of their frequency and severity.
 |
Figure 1 Frequency of symptoms in relation to DES. |
 |
Figure 2 Frequency and intensity of burning as a symptom of DES. |
 |
Figure 3 Frequency and intensity of itching as a symptom of DES. |
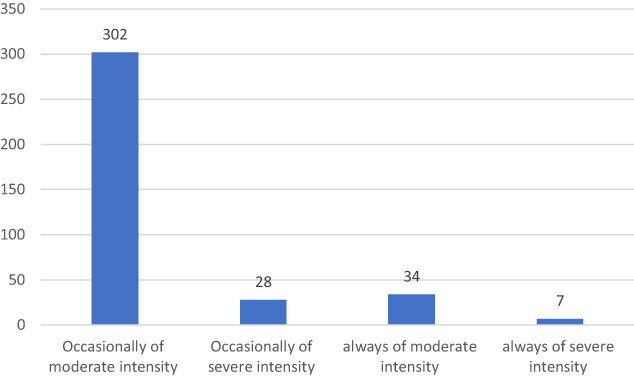 |
Figure 4 Frequency and intensity of redness as a symptom of DES. |
 |
Figure 5 Frequency and intensity of foreign body sensation as a symptom of DES. |
 |
Figure 6 Frequency and intensity of watering/tearing as a symptom of DES. |
 |
Figure 7 Frequency and intensity of excessive blinking as a symptom of DES. |
 |
Figure 8 Frequency and intensity of pain as a symptom of DES. |
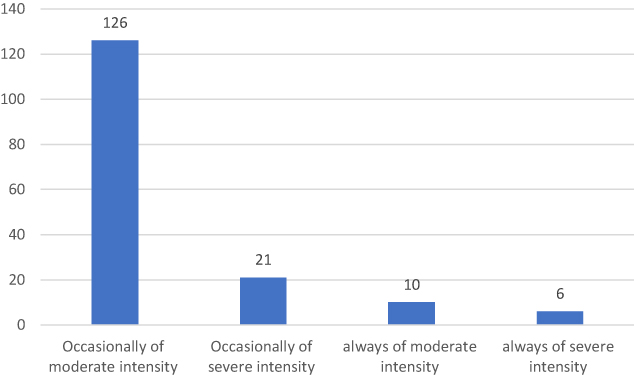 |
Figure 9 Frequency and intensity of heaviness in the eyelids as a symptom of DES. |
 |
Figure 10 Frequency and intensity of dryness as a symptom of DES. |
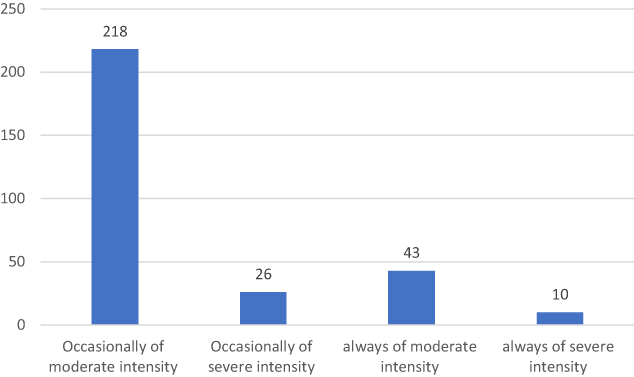 |
Figure 11 Frequency and intensity of blurred vision as a symptom of DES. |
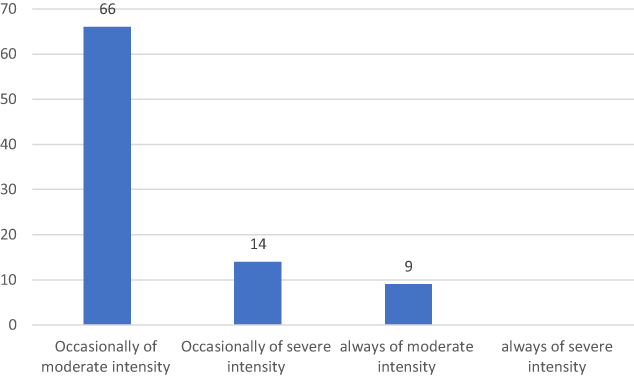 |
Figure 12 Frequency and intensity of double vision as a symptom of DES. |
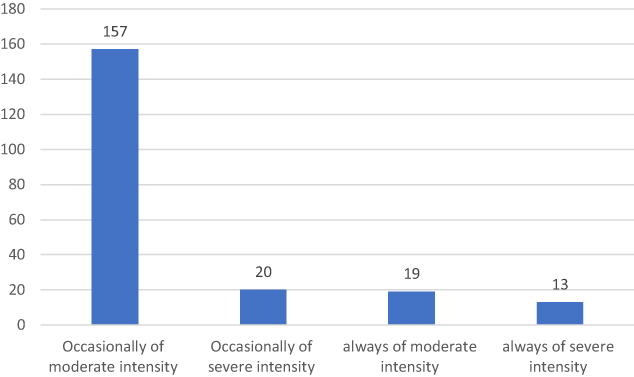 |
Figure 13 Frequency and intensity of difficulty in focusing near as a symptom of DES. |
 |
Figure 14 Frequency and intensity of halos around objects as a symptom of DES. |
 |
Figure 15 Frequency and intensity of increased sensitivity to light as a symptom of DES. |
 |
Figure 16 Frequency and intensity of headache as a symptom of DES. |
 |
Figure 17 Frequency and intensity of worsening of eyesight as a symptom of DES. |
The enter method was applied in ordinal logistic regression, and Table 4 shows the significant association of some covariates with the main outcome variable. In the univariate model, gender, using eye lubricants, and using a smartphone were significant predeterminants of DES. Females had a 1.5-times greater risk than males of scoring severe in DES versus mild and moderate (OR= 1.498; 95% CI 1.021–2.199, P = 0.001). Additionally, not using eye lubricants and using smartphones for classes were significantly associated with increased severity of DES (P < 0.05). When the significant covariates were adjusted in the multivariate model, gender was no longer significant (P = 0.181). After adjustment for potential confounders, students who reported not using eye lubricants had a 1.6-times increased risk of having severe DES compared with mild and moderate (OR = 1.623; 95% CI 1.1132–2.3675; P = 0.012). In addition, those who used their smartphone for online classes had a nearly twofold higher risk of experiencing severe versus mild or moderate DES (OR = 1.8; 95% CI 1.2235–2.5069; P = 0.002).
 |
Table 4 Ordinal Regression Model of Risk Factors Associated with DES |
Discussion
Since the revolution of digital devices in the 1980s, the use of these devices has been increasing and will continue to rise over time. The coronavirus pandemic further contributed to increased use of electronics through the shift toward online teaching and working. The increased use of electronics predisposes users to a syndrome known as digital eye strain. According to the American Optometric Association, DES involves an array of eye- and vision-related symptoms that result from prolonged usage of digital devices that increase stress in the near vision.6 Blehm defined computer vision syndrome, or DES, as a group of visual and nonvisual symptoms experience by digital device users. Among the two groups, visual symptoms are more common.13
The prevalence of DES in our sample was found to be 68.53%. This is a lower prevalence in comparison with the prevalence reported in other studies (90.42% and 78%).2,3 This could be explained by the timing of these studies, which correlated with the COVID-19 lockdown and increased use of digital devices during that period. The most common symptoms reported in our sample were headache (56%), dryness (54%), and burning (54%), whereas the least present symptoms were having double vision (11.8%) and observing halos around objects (19.8%). The most frequently reported symptoms in other studies were headache, dryness, and burning sensation.4,7 Other symptoms, such as difficulty focusing near and worsening of eyesight, were experienced more by students using digital devices for attending online classes for more than 2 hours. This could be attributed to the continuous and frequent accommodation changes that overwhelm the accommodative muscle capability.8
With respect to risk factors associated with the severity of DES symptoms, the univariate analysis of this study showed that only gender, using eye lubricants, and using a smartphone for classes were significantly associated with increased symptom severity. In the current study, not using eye lubricants was found to increase the risk of experiencing severe DES symptoms by 1.6 times. The American Optometric Association also reported that using lubricating eye drops was found to be significantly associated with DES, in addition to other factors including gender, age, and screen time.1 The association between not using lubricating eye drops and the severity of symptoms could be explained by the reduction in blinking rate when using digital devices for a long time, which would lead to eye dryness and exacerbation of symptoms.9–12 Moreover, several studies suggested that using lubricating eye drops can help alleviate the severity of dryness and DES symptoms.12–17 Regarding the gender risk factor, the results of the current study showed that females were at a 1.5-times greater risk than males of scoring severe in DES versus mild and moderate. This could be attributed to high somatic symptoms amplification in females compared with males, as was found in different studies.18,20,21
In the current study, the use of smartphones for online classes was found to be a statistically significant predeterminant of DES. In a similar cross-sectional study done by Mohan et al, a statistically significant association of DES with the use of smartphones was reported.4 Moreover, other similar studies reported that the use of smartphones over other devices was significantly associated with DES and considered an independent risk factor.4,22–25 This could be attributed to the fact that using smartphones requires viewing screens from a shorter distance compared with larger devices, thus leading to more stress on ocular muscles and development of DES.4,25 The total hours spent using digital devices per day was not found to be significantly associated with the severity of DES symptoms in the current study (P = 0.141). However, several studies showed that the duration of digital device use was considered a significant risk factor for DES.4,26,27 In a cross-sectional study involving secondary school students, Mohan et al reported that using devices for 5 hours or more was significantly associated with increasing the risk of DES (P = 0.0007).4 Several studies reported that DES prevalence was found to be higher in participants who use digital devices for 4 hours or more per day.27–30 In other studies, using digital devices for more than 2 hours daily was associated with a higher prevalence of DES among adolescents.4,30 A different study conducted on college students showed that there was a relationship between symptoms of DES and the duration of digital device use per day and reported that 93.9% of students who spent 6 hours or more using digital devices suffered from DES.31 Hence, the researchers suggested that using digital devices for more than 6 hours was one of the risk factors for developing DES.31–34 This difference in results could be attributed to the difficulty of determining the accuracy of self-reported answers to the exact number of hours spent using digital devices each day.31 Furthermore, the majority of the previous studies examined the prevalence of DES in relation to the duration spent using electronic devices in hours, but none mentioned the effect of total hours spent per day on the severity of symptoms.
The main purpose of the survey in the current study was to gather more data about DES and determine students’ habits in using digital devices in order to help them avoid DES. The symptoms of DES can be effectively managed and relieved by taking frequent breaks.12 Many experts recommend implementing the 20-20-20 rule during screen time. This rule consists of taking a break for 20 seconds every 20 minutes by gazing at a distance of 20 feet. Regular use of lubricating eye drops is another way to manage DES symptoms.35 Regarding vision screening, the American Optometric Association recommends vision screening at least every 2 years in asymptomatic low-risk adults from age 18 through 64.36
There are some limitations to our study. Data obtained from self-reported questionnaires are inherently biased. Subjects may overestimate or underestimate their symptoms. Additionally, the impact of refractive errors was not examined, despite the fact that DES symptoms may be impacted by the type of refractive errors and their correction. Another limitation is that our study did not include eye examinations.
Conclusion
In the wake of the COVID-19 pandemic, virtual learning has become an integral part of education, leading to increased use of digital technology. The aim of this study was to investigate the impact of virtual learning on eye strain and to determine the prevalence and effects of DES. A questionnaire was administered to participants, and the findings revealed a prevalence of 68.53%. The use of eye drops for lubrication and smartphones for classes was significantly associated with DES. Furthermore, females were found to be more susceptible to severe DES symptoms than males. The development of a tool such as the CVS-Q to predict DES prevalence could reduce clinic time and resources by minimizing unnecessary follow-up and ophthalmology referrals.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Optometric Association. Computer vision syndrome. Available from: https://www.aoa.org/healthy-eyes/eye-and-vision-conditions/computer-vision-syndrome?sso=y.
2. Bahkir F, Grandee S Impact of the COVID-19 lockdown on digital device-related ocular health; 2020. Available from: https://pubmed.ncbi.nlm.nih.gov/33120622/.
3. Alabdulkader B Effect of digital device use during COVID-19 on digital eye strain; 2021. Available from: https://pubmed.ncbi.nlm.nih.gov/33689614/.
4. Mohan A, Sen P, Shah C, Jain E, Jain S. Prevalence and risk factor assessment of digital eye strain among children using online e-learning during the COVID-19 pandemic: digital eye strain among kids (DESK study-1). Indian J Ophthalmol. 2021;69(1):140–144. doi:10.4103/ijo.IJO_2535_20
5. Seguí Mdel M, Cabrero-García J, Crespo A, Verdú J, Ronda E. A reliable and valid questionnaire was developed to measure computer vision syndrome at the workplace. J Clin Epidemiol. 2015;68:662–673. doi:10.1016/j.jclinepi.2015.01.015
6. Tripathy K Computer vision syndrome (digital eye strain); 2022 Available from: https://eyewiki.aao.org/Computer_Vision_Syndrome_(Digital_Eye_Strain).
7. Shantakumari N, Eldeeb R, Sreedharan J, Gopal K. Computer use and vision-related problems among university students in Ajman, United Arab Emirates. Ann Med Health Sci Res. 2014;4(2):258–263. doi:10.4103/2141-9248.129058
8. Verma SB Computers and vision. J. Postgrad. Med. U.S. National Library of Medicine; 2001. Available from: https://pubmed.ncbi.nlm.nih.gov/11832604/.
9. Patel S, Henderson R, Bradley L, et al. Effect of visual display unit use on blink rate and tear stability. Optom Vis Sci. 1991;68:888–892. doi:10.1097/00006324-199111000-00010
10. Schlote T, Kadner G, Freudenthaler N. Marked reduction and distinct patterns of eye blinking in patients with moderately dry eyes during video display terminal use. Graefes Arch Clin Exp Ophthalmol. 2004;242:306–312. doi:10.1007/s00417-003-0845-z
11. Tsubota K, Nakamori K. Dry eyes and video display terminals. N Engl J Med. 1993;328:584. doi:10.1056/NEJM199302253280817
12. Coles‐brennan C, Sulley A, Young G. Management of digital eye strain. Clin Exp Optometry. 2019;102(1):18–29. doi:10.1111/cxo.12798
13. Blehm C, Vishnu S, Khattak A, et al. Computer vision syndrome: a review. Surv Ophthalmol. 2005;50(3):253–262. doi:10.1016/j.survophthal.2005.02.008
14. Reddy SC, Low CK, Lim YP, et al. Computer vision syndrome: a study of knowledge and practices in university students. Nepal J Ophthalmol. 2013;5:161–168. doi:10.3126/nepjoph.v5i2.8707
15. Abelson MB, Ousler GW. How to fight computer vision syndrome. Rev Ophthalmol. 1999;4:114–116.
16. Tribley J, McClain S, Karbasi A, et al. Tips for computer vision syndrome relief and prevention. Work. 2011;39(1):85–87. doi:10.3233/WOR-2011-1183
17. Guillon M, Maissa C, Pouliquen P, et al. Effect of povidone 2 per cent preservative-free eyedrops on contact lens wearers with computer visual syndrome: pilot study. Eye Contact Lens. 2004;30(1):34–39. doi:10.1097/01.ICL.0000101489.13687.9A
18. Nakao M, Tamiya N, Yano E. Gender and somatosensory amplification in relation to perceived work stress and social support in Japanese workers. Women Health. 2005;42(1):41–54. doi:10.1300/J013v42n01_03
19. Wang MTM, Craig JP. Investigating the effect of eye cosmetics on the tear film: current insights. Clinical Optometry. 2018;10:33–40. doi:10.2147/opto.s150926
20. Kroenke K, Spitzer RL. Gender differences in the reporting of physical and somatoform symptoms. Psychosom Med. 1998;60(2):150–155. doi:10.1097/00006842-199803000-00006
21. Bingefors K, Isacson D. Epidemiology, co-morbidity, and impact on health-related quality of life of self-reported headache and musculoskeletal pain--a gender perspective. Eur J Pain. 2004;8(5):435–450. doi:10.1016/j.ejpain.2004.01.005
22. Kaur K, Gurnani B, Nayak S, et al. Digital eye strain- a comprehensive review. Ophthalmol Ther. 2022;11:1655–1680. doi:10.1007/s40123-022-00540-9
23. Al-Mohtaseb Z, Schachter S, Shen Lee B, Garlich J, Trattler W. The relationship between dry eye disease and digital screen use. Clin Ophthalmol. 2021;15:3811–3820. doi:10.2147/OPTH.S321591
24. Auffret E, Mielcarek M, Bourcier T, Delhommais A, Speeg-Schatz C, Sauer A. Digital eye strain. Functional symptoms and binocular balance analysis in intensive digital users. J Fr Ophtalmol. 2022;45(4):438–445. doi:10.1016/j.jfo.2020.10.026
25. Moon JH, Lee MY, Moon NJ. Association between video display terminal use and dry eye disease in school children. J Pediatr Ophthalmol Strabismus. 2014;51:87–92. doi:10.3928/01913913-20140128-01
26. Kanitkar K, Carlson AN, Richard Y. Ocular problems associated with computer use: the ever‐increasing hours spent in front of video display terminals have led to a corresponding increase in visual and physical ills. Rev Ophthalmol E-Newsletter. 2005;12:6453.
27. Ichhpujani P, Singh RB, Foulsham W, Thakur S, Lamba AS. Visual implications of digital device usage in school children: a cross‐sectional study. BMC Ophthalmol. 2019;19:76. doi:10.1186/s12886-019-1082-5
28. Cantó-Sancho N, Ronda E, Cabrero-García J, et al. Rasch-Validated Italian Scale for diagnosing digital eye strain: the computer vision syndrome questionnaire IT©. Int J Environ Res Public Health. 2022;19(8):4506. doi:10.3390/ijerph19084506
29. Owens DA. The resting state of the eyes. Am Sci. 1984;72(4):378–387.
30. Kim J, Hwang Y, Kang S, et al. Association between exposure to smartphones and ocular health in adolescents. Ophthal Epidemiol. 2016;23:269–276. doi:10.3109/09286586.2015.1136652
31. Gammoh Y. Digital eye strain and its risk factors among a university student population in Jordan: a cross-sectional study. Cureus. 2021. doi:10.7759/cureus.13575
32. Artime Ríos EM, Sánchez Lasheras F, Sánchez AS, Iglesias-Rodríguez FJ, Del Mar Seguí Crespo M. Prediction of computer vision syndrome in health personnel by means of genetic algorithms and binary regression trees. Sensors. 2019;19:2800. doi:10.3390/s19122800
33. Rahman Z, Sanip S. Computer user: demographic and computer related factors that predispose user to get computer vision syndrome. IJBHT. 2011;1:84–91.
34. Mutti DO, Zadnik K. Is computer use a risk factor for myopia? J Am Optom Assoc. 1996;67:521–530.
35. Sheppard AL, Wolffsohn JS. Digital eye strain: prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018;3:e000146. doi:10.1136/bmjophth-2018-000146
36. American Optometric Association. Comprehensive eye exam. Available from: https://www.aoa.org/healthy-eyes/caring-for-your-eyes/eye-exams?sso=y.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.