Back to Journals » Advances in Medical Education and Practice » Volume 17
Translating Social Accountability Values into Practice: Doctors’ Experiences from Problem-Based Learning Medical Curriculum in the United Arab Emirates
Authors Dash NR, Hasswan AA, Samaha MAAE, Samara KA, Taha MH
Received 21 October 2025
Accepted for publication 28 January 2026
Published 6 February 2026 Volume 2026:17 575836
DOI https://doi.org/10.2147/AMEP.S575836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sateesh Arja
Nihar Ranjan Dash,1 Ahmed Alrazzak Hasswan,1,2 Mayar Abbas Ahmed Essam Samaha,1,3 Kamel Aladdein Samara,1,4 Mohamed Hassan Taha5
1Clinical Sciences Department, College of Medicine, University of Sharjah, Sharjah, United Arab Emirates; 2TEWV NHS Foundation Trust, Cross Lane Hospital, Scarborough, UK; 3General Paediatrics, Al Jalila Children’s Hospital, Dubai, United Arab Emirates; 4Medicine, Jefferson Abington Hospital, Abington, Pennsylvania, USA; 5Medical Education Center, College of Medicine, University of Sharjah, Sharjah, United Arab Emirates
Correspondence: Nihar Ranjan Dash, Clinical Sciences Department, College of Medicine, University of Sharjah, Sharjah, P Box – 27272, United Arab Emirates, Tel +971 6 505 7217, Email [email protected]
Purpose: Medical schools play a crucial role in preparing future doctors to address the health needs of patients and their communities. Graduates are expected to provide socially accountable care by upholding values such as relevance, equity, quality, and cost-effectiveness. This study explores how these values are understood and applied by medical graduates trained in problem-based learning (PBL) curricula.
Methods: A cross-sectional online survey was conducted among University of Sharjah medical graduates to assess their exposure to and practice of social accountability values.
Results: Of the 689 graduates invited, 503 (73%) responded, including 329 (65%) women. Most respondents, 375 (75%), were practicing in the United Arab Emirates (UAE), with 310 (62%) working in secondary healthcare. During training, PBL was generally effective in covering local health issues (378, 75%), although areas such as multidisciplinary collaboration and cost-effectiveness showed lower integration (p < 0.0005). In clinical practice, 362 (72%) reported addressing major health issues and 332 (66%) considered the social determinants of health. Professionalism and quality were well embedded, but gaps persisted in patient-centered care, cost, and teamwork across disciplines (p < 0.0005).
Conclusion: These findings highlight the gap between undergraduate training and real-world application. Strengthening the medical curriculum to embed social accountability more explicitly is essential for meeting evolving community health needs.
Keywords: social accountability values, curriculum design, PBL, medical education, clinical education, patient-centered care
Introduction
Medical schools bear the responsibility for training competent doctors to meet society’s health needs and expectations. Consequently, medical schools all over the world must be socially accountable, which the World Health Organization defines as “the obligation of medical schools to direct their education, research, and/or service activities toward addressing the priority health concerns of the community, region, and/or nation they have the mandate to serve”.1 Collaboration between governments, healthcare entities, experts, and the public is essential for identifying priority health challenges. The WHO outlines four fundamental values that guide social responsibility in medical education: relevance, quality, cost-effectiveness, and equity.1 These core values manifest when a medical school’s curriculum integrates local community health concerns (relevance), fosters the development of graduates equipped to provide exceptional care within societal contexts (quality), emphasizes efficient utilization of available resources for individual and societal health (cost-effectiveness), and ensures that students are exposed to diverse societal issues (equity) across educational, research, and service domains.
Since the incorporation of social accountability requirements into accreditation standards for medical education programs by the World Federation for Medical Education (WFME) in 2015,2 there has been a growing inclination among medical schools worldwide to integrate social accountability values into their educational programs.2,3 Additionally, these schools have begun assessing the compliance of their educational programs with social accountability standards using validated tools, grids, and inventories at the institutional level.4–6 Through these assessments, medical schools have conducted effective situational analyses to identify challenges and obstacles to the implementation of social accountability values in their medical education programs.7,8 While there is a visible effort to instill the values of social accountability into the educational curriculum and training of future doctors, there remains a gap in the literature showing its translation from theory to practice.9–11
Medical schools’ social accountability responsibilities can differ widely depending on cultural and geographic contexts. For example, in resource-limited settings, medical schools may focus on training to address local health challenges such as endemic diseases, maternal and child health, and emergency care.12,13 In contrast, schools in more developed regions might concentrate on preparing graduates to manage issues related to an aging population, mental health, or non-communicable diseases.14 It is imperative that medical graduates uphold socially accountable care throughout their careers by remaining responsive to the health needs of their patients and communities. Some studies have been conducted to measure the integration of social accountability values into undergraduate medical curricula, such as those in the United Arab Emirates, Egypt, and Ireland.15,16 However, these studies have primarily focused on the implementation of these values during physician training, and to the best of our knowledge, no studies have examined the transfer of these values from educational settings to real-world clinical practice after graduation.
This study explored the translation of social accountability values from learning to practice among a cohort of medical graduates who underwent problem-based learning (PBL) in their undergraduate curriculum. As PBL promotes student-centered approach in which learning begins with a real-world problem that students collaboratively analyze, research, and solve. Grounded in the idea that knowledge is best constructed through active engagement, PBL promotes meaningful and relevant learning while developing critical thinking, problem-solving, collaboration, and self-directed learning skills.17 In medical education, PBL promotes social accountability by engaging students with problems reflecting the actual healthcare needs and societal challenges. PBL cases may be tailored to local disease patterns, social priorities, and health systems, reflecting national contexts. Through problem-solving, students develop the skills and values needed to contribute meaningfully to societal well-being, making education more responsive to public needs and priorities.16,18 PBL curricula show significant international variability due to differences in educational philosophies, cultural contexts, institutional resources, and healthcare or workforce needs.19 In UAE, we have adopted hybrid model that combine PBL with traditional lectures as it leverages the strengths of both approaches by ensuring comprehensive content coverage while fostering active learning, clinical reasoning, and learner engagement. The findings of this study will assist in calibrating the social accountability vision of medical schools by demonstrating the connection between physician training and practical application of social accountability values. This is vital to ensure that the medical education of the future physician workforce is sensitive to the requirements of the society they aim to serve.
Materials and Methods
Study Design
This cross-sectional study was carried out between January and April 2024, focusing on the alumni of the College of Medicine at the University of Sharjah in the United Arab Emirates who were actively practicing medical professionals. A cross-sectional study design was chosen because it allows data collection at a single point in time, making it ideal for assessing how graduates apply these values in their professional settings. This design enabled the comparison of multiple variables, such as various domains of social accountability (relevance, equity, quality, and cost-effectiveness), without requiring a longitudinal follow-up, making it a practical choice for the study.
Ethics Statement
Ethical approval for this study was granted by the Research Ethics Committee of the University of Sharjah (REC-23-04-05-01-F). All participants provided informed consent prior to participating in the study. The online questionnaire included an introductory section explaining the study’s objectives, the voluntary nature of participation, confidentiality assurances, and the right to withdraw at any time without any consequences.
Sample Selection
The study sample included alumni of the College of Medicine, University of Sharjah, who were practicing as medical professionals. The inclusion criteria were graduates from 2015 onward, to minimize recall bias and ensure recent exposure to problem-based learning (PBL). The college alumni database contained approximately 1250 entries dating from 2008 onward. Alumni who graduated between 2015 and 2023 were eligible for participation, and a total of 689 invitations were sent out. Participants needed to actively practice primary, secondary, or tertiary care, either locally or internationally. The exclusion criteria were graduates before 2015, non-practicing professionals, and those who were unwilling or unable to provide consent. Participants were recruited through alumni networks, professional and social media platforms, such as LinkedIn and WhatsApp, and personal contacts to maximize outreach and encourage broad participation. After the initial invitation, three follow-up reminders were sent at two-week intervals.
Study Settings
The University of Sharjah’s MBBS program spans six years, following an outcome-based student-centered approach with a problem-based learning curriculum. It consists of three phases: Phase I (foundation year), Phase II (pre-clerkship, years 1–3), and Phase III (clerkship, years 4–5). In Phase II, the students engaged in 70 PBL scenarios (Supplementary Table 1), reflecting real patient problems. In Phase III, they transitioned to hospital rotations and interacted with real patients. The curriculum emphasizes social accountability—relevance, equity, quality, and cost-effectiveness— and prepares graduates for diverse local and global healthcare roles. It trains doctors to address the UAE and Middle East and North Africa (MENA) regional health needs through patient-centered, multidisciplinary approaches.
Adaptation Process of the Questionnaire and Its Validity
This study used a questionnaire adapted from a validated social accountability inventory to assess the integration of social accountability values into medical education.6 While the original social accountability inventory comprised 17 items, the adapted version included 15 items. This reduction resulted from merging the ethnicity, age, and gender equity items into a single composite item rather than retaining them as three separate items. The adaptation process ensured relevance for graduates trained in the University of Sharjah’s problem-based learning (PBL) curriculum. The research team aligned statements with the local context and refined terminology to reflect the UAE and MENA health issues. An expert panel reviewed and refined the questionnaire to ensure its clarity and relevance. Pilot testing of 20 graduates led to minor revisions. Validation included face, content, and construct validity, aligned with WHO’s social accountability values, and achieved high reliability (Cronbach’s alpha > 0.8).
Questionnaire Administration
To evaluate the acquisition and application of social accountability values acquired during undergraduate medical education (learning) and patient care as practicing physicians (practice), we administered an online questionnaire through the Google Forms® platform. The questionnaire (Supplementary Figure 1) utilized a slightly modified and adapted version of a validated 15-statement social accountability inventory in English.6 This inventory covers four core social accountability values: relevance, equity, quality, and cost-effectiveness. The first ten statements focus on relevance, followed by two statements each for equity and quality, and the final statement addresses the concept of cost-effectiveness. Participants were asked to respond to the questions using four options: yes, no, maybe, or not sure.
Statistical Analysis
Data from Google Forms were exported as CSV files and analyzed using Python 3 with Matplotlib v3.3.4, pandas v1.2.4, and SciPy v1.10.0. Frequency distributions were generated, and responses to the social accountability inventory were categorized as “No,” “Maybe/Not sure,” and “Yes,” assigned values of 0, 1, and 2, respectively. The Wilcoxon Signed-Rank test, which is suitable for paired non-normally distributed data, assessed changes in reported coverage between undergraduate education and practice. Statistical significance was set at P < 0.05. Missing data were excluded from paired analyses, and the sensitivity analysis confirmed a minimal impact on the overall findings.
Results
Demographics
Of the 689 invitations sent, 503 responses were received, yielding a response rate of 73%. Among the respondents, 329 (65%) were female, and 174 (35%) were male. Among the respondents, 277 (55%) were resident doctors, 129 (26%) were interns, and the remaining 97 (19%) had various other roles, such as general practitioners, family physicians, emergency physicians, specialists, and consultants. Most study participants 377 (75%) were currently practicing in the United Arab Emirates (UAE), while the rest were in different countries. Regarding healthcare settings, 310 (62%) worked in secondary healthcare, 107 (21%) in tertiary healthcare, and the remaining 86 (17%) in primary healthcare (Table 1).
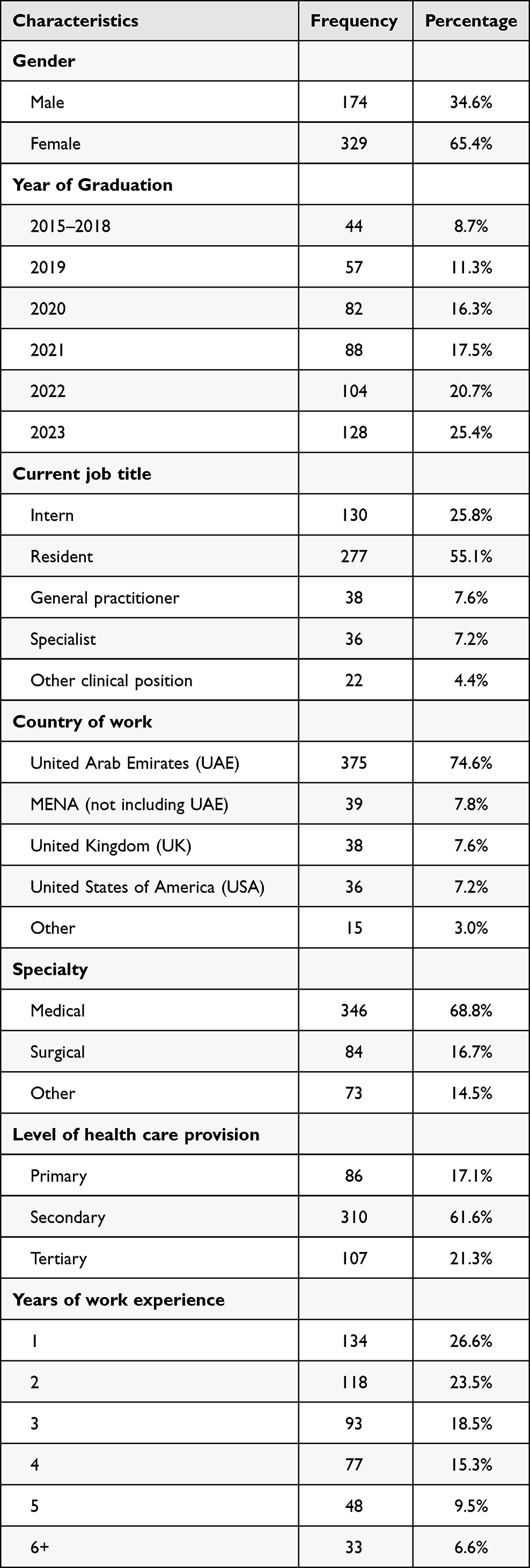 |
Table 1 Demographics and Baseline Characteristics of Participants |
Social Accountability Values Exposure During Undergraduate Education Through PBL Cases
Most respondents 378 (75%) agreed that problem-based learning (PBL) case scenarios effectively addressed major local health issues. Similarly, 311 (62%) fully agreed and 96 (20%) partially agreed that PBL cases incorporated social determinants of health such as income, education, and employment. Regarding health promotion and preventive measures, 277 (55%) participants agreed, 121 (24%) partially agreed, and 105 (21%) disagreed with them. When evaluating key healthcare concepts in PBL cases, including stakeholder engagement, professionalism, referral systems, evolving doctor roles, and multidisciplinary approaches, the agreement rates were lower at 213 (42%), 230 (46%), 214 (42.5%), and 174 (34.5%), respectively. The disagreement rates ranged from 19% to 29%, indicating varied perspectives on inclusion (Figure 1).
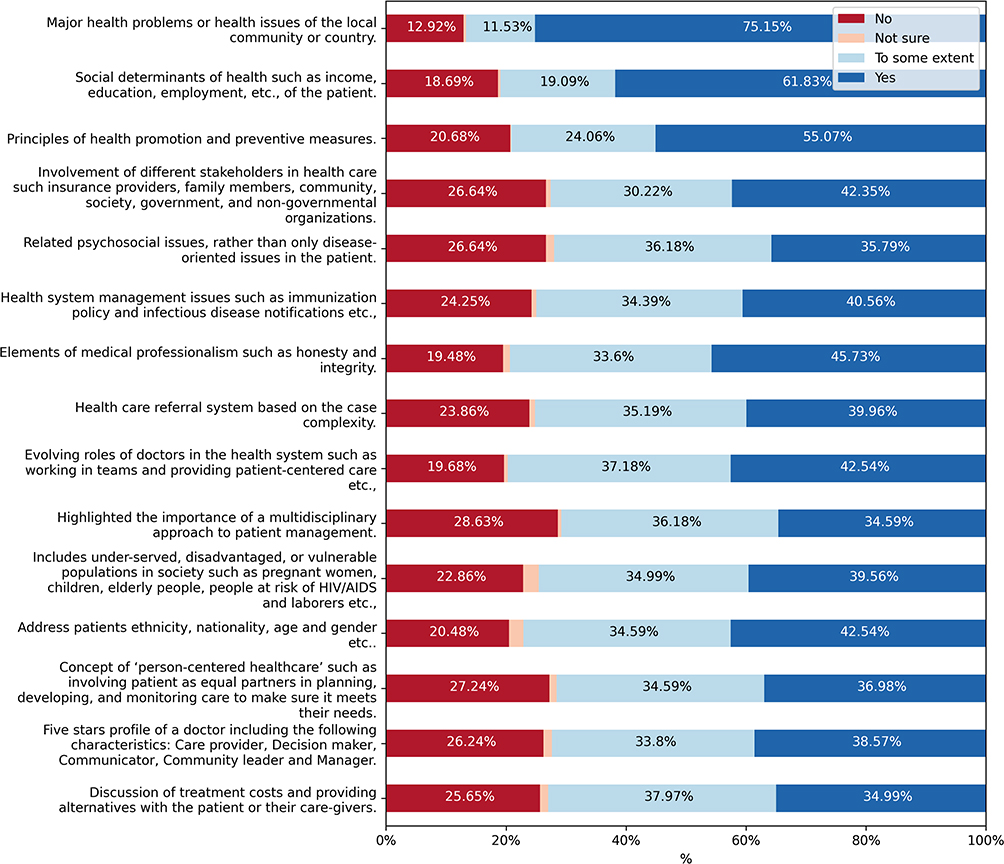 |
Figure 1 Exposure to social accountability values during undergraduate education. |
In the equity domain, 214 (42.5%) agreed and 174 (34.5%) partially agreed that PBL cases consider patient demographics. Similarly, 199 (40%) agreed and 176 (35%) partially agreed that vulnerable populations were present. Regarding quality, 186 (37%) agreed, 174 (34.5%) partially agreed, and 137 (27%) disagreed that PBL cases reflected person-centered healthcare. Similarly, 194 (38.5%) participants agreed, 170 (34%) partially agreed, and 132 (26%) disagreed with the five-star doctor’s profile. Regarding cost-effectiveness, 191 (38%) partially agreed and 129 (26%) disagreed that treatment costs and alternatives were sufficiently discussed.
Coverage of Social Accountability Values in Current Medical Practice
As medical professionals transitioned to practice, most respondents acknowledged the importance of social accountability. Among them, 362 (72%) fully agreed, and 97 (19%) partially agreed that addressing major local health issues was integrated into their daily practice.
Additionally, 332 (66%) fully agreed and 124 (25%) partially agreed that they considered the social determinants of health, such as income, education, and employment, in patient care. Similarly, 328 (65%) fully agreed and 124 (25%) partially agreed with applying health promotion and prevention in daily practice (Figure 2).
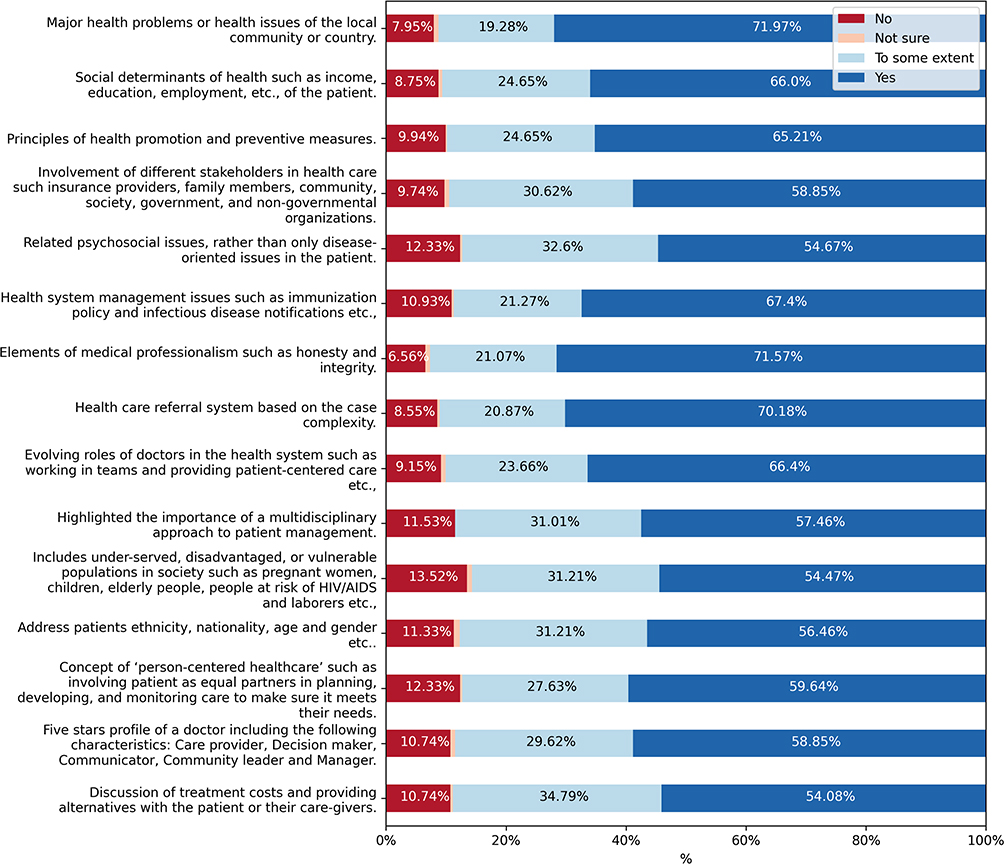 |
Figure 2 Coverage of social accountability values during medical practice. |
The medical professionalism components also showed strong agreement, with 362 (72%) endorsing honesty and integrity and 352 (70%) supporting the healthcare referral system based on case complexity. A multidisciplinary approach was used by 287 (57%) patients, with 156 (31%) partially agreeing to participate. The evolving roles of doctors in team-based, patient-centered care were acknowledged by 332 (66%), with 121 (24%) partial agreements. Regarding equity, 274 (54%) fully agreed, 157 (31%) partially agreed that they addressed underserved populations, and 284 (56%) fully agreed that they considered the patient demographics. Healthcare quality was affirmed by 302 (60%) participants through person-centered care and by 297 (59%) through the five-star doctor profile. Regarding cost-effectiveness, 272 (54%) participants discussed treatment expenses and 176 (35%) partially engaged in such discussions.
Comparison Between Learning and Practice
Apart from addressing “major health problems within the local community or country,” there was a notable disparity between undergraduate education and current practices concerning the coverage of social accountability values. (Table 2). Furthermore, to estimate the gap between learning and practice, the average scores for each item were compared (Figure 3). The greatest disparity (p < 0.0005) was observed in psychosocial issues and multidisciplinary care. These domains were frequently emphasized in practice (56%, 275/503 and 58%, 289/503, respectively) but were substantially less covered during education (36%, 180/503 and 35%, 174/503, respectively). Person-centered healthcare and the five-star doctor profile were underrepresented in the curriculum (p < 0.0005). Although clinical practitioners have addressed patient diversity and equity, these topics have not been thoroughly explored in the education field. Additionally, cost-effectiveness—encompassing treatment costs and alternative care options—was more frequently emphasized in clinical practice (55%, 272/503) than during education and training (35%, 176/503), with this difference reaching statistical significance (p < 0.0005).
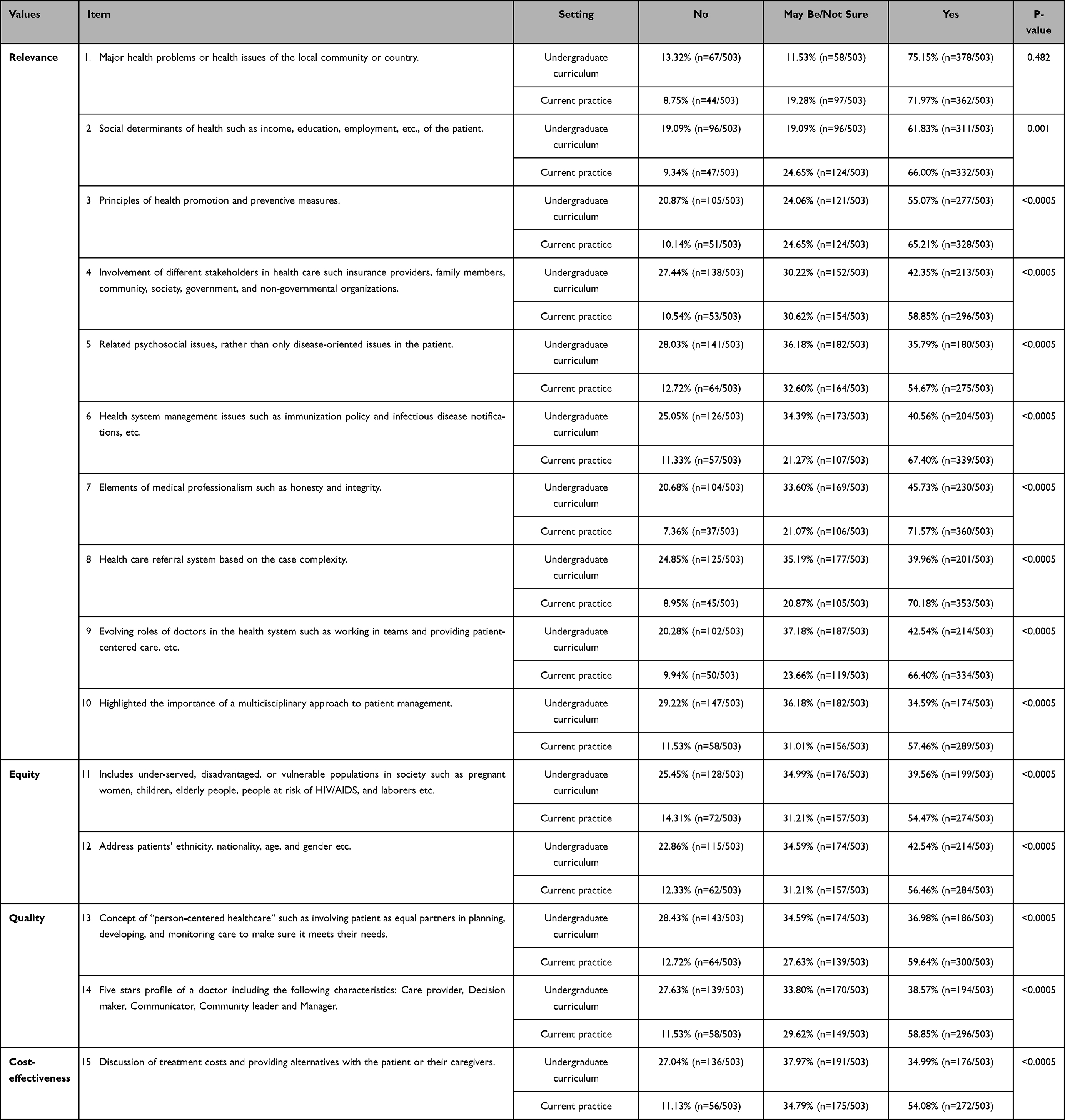 |
Table 2 Wilcoxon Signed-Rank Tests Comparing the Reported Coverage of the Social Accountability Values for Each Item During Undergraduate Education and Current Practice |
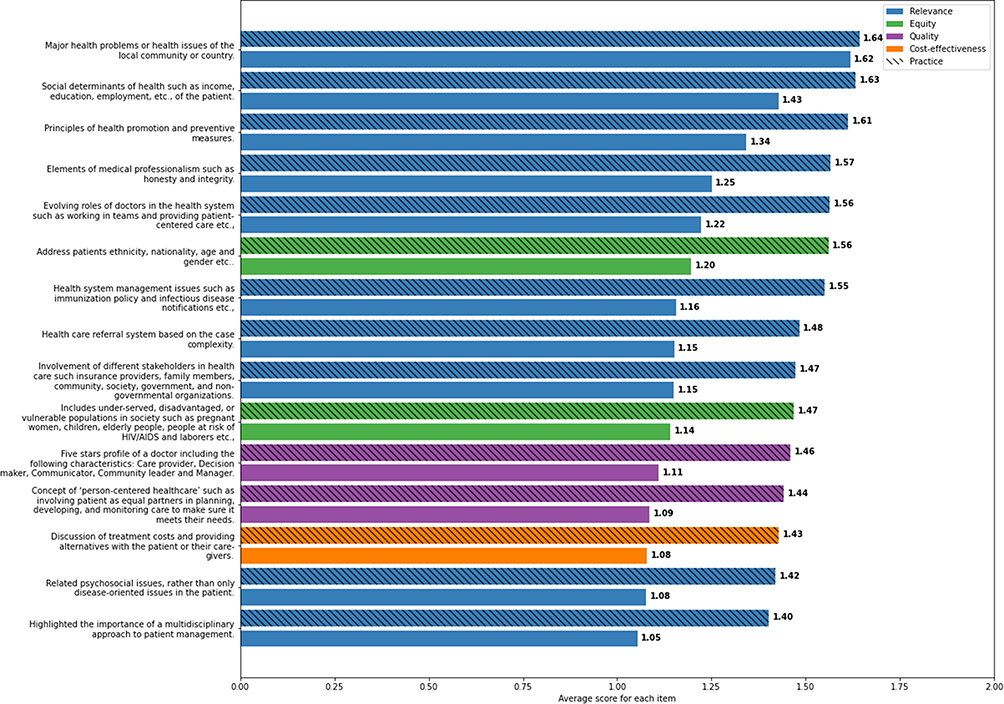 |
Figure 3 The comparison between the average scores of each social accountability value during education and practice. |
Discussion
Medical schools bear the responsibility of training future physicians to meet society’s health care needs. Social accountability is the foundation of both medical education and practice, ensuring that medical schools direct their efforts toward addressing pressing health concerns.20 This study examined the correlation between the social accountability values learned in a problem-based learning (PBL) curriculum and their application in graduates’ current practice. The findings reveal significant gaps in translating social accountability values into practice, particularly regarding relevance, equity, quality, and cost-effectiveness.
The only positive equilibrium between learning and practice is addressing major health issues within the local community or country, a key goal of social accountability.21 However, a substantial gap was noted in the emphasis on the social determinants of health and the inclusion of underserved, disadvantaged, and vulnerable populations. Medical schools that incorporate social accountability into their curricula often expose students to community-based learning experiences, which are essential for understanding and addressing healthcare disparities. This approach has been proven effective in meeting the diverse healthcare needs of the population.2
Several social accountability values, such as a multidisciplinary approach to patient management, medical professionalism, and a referral system based on case complexity, were more frequently applied in practice than emphasized during undergraduate education. Similarly, evolving roles of doctors, including teamwork and patient-centered care, were better addressed in professional settings than in PBL curricula. Integrating the Entrustable Professional Activities (EPAs) framework in undergraduate training could help bridge these gaps by enhancing assessment- and competency-based education.22 By embedding values such as equity, cost-effective care, multidisciplinary collaboration, and responsiveness to community needs within routine professional activities, EPAs align educational outcomes with societal healthcare priorities. This approach not only reinforces social accountability through authentic clinical practice but also provides measurable outcomes through assessments requiring demonstrated proficiency in these domains, thereby narrowing the gap between undergraduate education and real-world professional expectations.23
This study revealed that important gaps between learning and practice exist across the board, including the equity, quality, and cost-effectiveness values of social accountability. Bridging the learning-practice gap requires targeted strategies. One approach is to incorporate triggers into PBL case scenarios to encourage discussions on patient empowerment, financial considerations, and healthcare alternatives.24 Additionally, interprofessional educational activities can foster collaborative patient-centered care planning. Innovative educational strategies can play a critical role in strengthening the integration of social accountability within medical curricula. Approaches such as Team-Based Learning (TBL), which promote collaborative problem-solving and reflect real-world multidisciplinary care, can be redesigned to explicitly incorporate social accountability values. This may include predefined learning outcomes such as effective interprofessional communication and cost-effective clinical decision-making. Student performance can be assessed using standardized team readiness assurance tests and peer evaluation scores to ensure measurable and objective outcomes. Similarly, Case Method (CM) can encourage learners to engage with context-specific clinical scenarios that highlight ethical decision-making, equity, and cost-effectiveness. Additionally, scaffolding strategies may support the progressive development of competencies by building on prior knowledge and skills, enabling learners to apply social accountability values with increasing independence. Collectively, these learner-centered approaches can facilitate deeper engagement, practical application, measurable outcomes and sustained translation of social accountability values into clinical practice.25,26 Strengthening these aspects in medical curricula will help graduates to apply social accountability values more effectively.
This study builds on previous research examining the integration of social accountability values in PBL scenarios.9 That study found that critical aspects such as a multidisciplinary approach, health promotion, underserved population considerations, and cost-effectiveness were inadequately addressed. In contrast, issues such as major public health concerns, social determinants of health, and evolving roles of doctors were well integrated. However, the current study highlights the disconnect between learning experiences and real-world medical practices. Understanding the root cause of this disparity can help improve medical education. Curriculum design limitations, faculty training gaps, and institutional barriers may contribute to insufficient translation of social accountability values into practice. Addressing these challenges requires structured curriculum review, faculty development programs, and institutional support for social accountability initiatives. For example, faculty development programs are essential to equip educators with the skills to model, teach, and assess social accountability values such as social determinates of health, multidisciplinary collaboration, patient centered healthcare, equity, cost-effective care, and community responsiveness within clinical and classroom settings.27 Similarly, at the institutional level, aligning curriculum design, assessment frameworks, and promotion criteria with social accountability priorities reinforces their importance and sustainability. Supportive policies such as community-based teaching, incentives for interprofessional education, and partnerships with community and primary care facilities can further facilitate the integration of social accountability into routine training. Together, these system-level factors create an enabling environment that supports consistent reinforcement of social accountability values from undergraduate education through clinical practice.28
This study has some limitations. Recall bias may affect participants’ recollections of their education, although limiting the study to graduates from 2015 onwards helped reduce this issue. Selection bias is another concern, as only practicing alumni willing to participate were included. Efforts have been made to include diverse specialties and healthcare settings in order to mitigate this issue. Response bias is also a risk, although anonymity and confidentiality were assured to encourage honest feedback.
Conclusion
This study identifies notable gaps between social accountability values taught in PBL curricula and their application in clinical practice, particularly in equity, quality, cost-effectiveness, and care for underserved populations. While addressing major public health concerns aligns with practice, other critical areas such as social determinants of health, multidisciplinary collaboration, and patient-centered care remain underemphasized. Bridging these gaps requires targeted strategies, including Entrustable Professional Activities, Team-Based Learning, the Case Method, scaffolding competencies, and community-based experiences. Faculty development, curriculum alignment, and supportive institutional policies are essential to reinforce social accountability, ensuring graduates are equipped to meet society’s healthcare needs.
Data Sharing Statement
All relevant data are within the paper and its supporting information files. Data can also be share from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Ethical approval for this study was granted by the Research Ethics Committee of the University of Sharjah (REC-23-04-05-01-F). All participants provided informed consent prior to participating in the study. The online questionnaire included an introductory section explaining the study’s objectives, the voluntary nature of participation, confidentiality assurances, and the right to withdraw at any time without any consequences.
Funding
The authors report no funding was involved in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Boelen C, Heck JE, Organization WH. Defining and measuring the social accountability of medical schools; 1995.
2. Rourke J. Social accountability: a framework for medical schools to improve the health of the populations they serve. Acad Med. 2018;93(8):1120–13. doi:10.1097/ACM.0000000000002239
3. Boelen C. Why should social accountability be a benchmark for excellence in medical education? Educación Médica. 2016;17(3):101–105. doi:10.1016/j.edumed.2016.06.004
4. Reddy AT, Lazreg SA, Phillips RL Jr, Bazemore AW, Lucan SC. Toward defining and measuring social accountability in graduate medical education: a stakeholder study. J Graduate Med Educ. 2013;5(3):439–445. doi:10.4300/JGME-D-12-00274.1
5. Yazdani S, Akbarilakeh M, Abdalla ME, Charles B, Arbabisarjou A, Moonaghi HK. Measuring social accountability of medical universities’ education function-design, development, and validation of instrument. J Evol Med Dent Sci. 2019;8(26):2110–2114. doi:10.14260/jemds/2019/464
6. Abdalla ME, Dash NR, Shorbagi S, Taha MH. Development and validation of inventory tool to evaluate social accountability principles in case scenarios used in problem-based curriculum (Social accountability inventory for PBL). Med Educ Online. 2021;26(1):1847243. doi:10.1080/10872981.2020.1847243
7. Yamani N, Fakhari M. Social accountability of medical education curriculum: barriers and implications. Iran J Med Educ. 2014;13(12):1082–1098.
8. Dehghani M-R, Azizi F, Haghdoost A, Nakhaee N, Khazaeli P, Ravangard Z. Situation Analysis of Social Accountability Medical Education in University of Medical Sciences and Innovative Point of View of Clinical Faculty Members towards its Promotion Using Strengths Weaknesses Opportunities and Threats (SWOT) analysis model. Strides Develop Med Educ. 2014;10(4):403–412.
9. Dash NR, Taha MH, Shorbagi S, Abdalla ME. Evaluation of the integration of social accountability values into medical education using a problem-based learning curriculum. BMC Med Educ. 2022;22(1):1–7. doi:10.1186/s12909-022-03245-6
10. Boelen C. Social accountability: medical education’s boldest challenge. MEDICC Rev. 2008;10(4):52.
11. Ghaffari R, Taghizadieh A, Behshid M, et al. Accountability in medical education from theory to practice Tabriz 2018 statement: a step towards the implementation of this social necessity. Med J Islamic Republic Iran. 2020;34:93. doi:10.34171/mjiri.34.93
12. Laugen C, Siagian C, Bennouna C, Participation KSH. Healthy people: a review of social accountability initiatives in Indonesian policies and programs; 2018.
13. Elsanousi S, Elsanousi M, Khalafallah O, Habour A. Assessment of the social accountability of the faculty of medicine at University of Gezira, Sudan. EMHJ-East Mediterranean Health J. 2016;22(4):258–266. doi:10.26719/2016.22.4.258
14. Lambert T, Goldacre M. Trends in doctors’ early career choices for general practice in the UK: longitudinal questionnaire surveys. Br J Gen Pract. 2011;61(588):e397–e403. doi:10.3399/bjgp11X583173
15. Ghaly M, Taha MH, Abdalla ME, Hosny S. Assessment of the compliance of problem-based learning case scenarios with the social accountability values in undergraduate medical education curriculum. Health Professions Educ. 2023;9(3):4. doi:10.55890/2452-3011.1045
16. Kelly D, Hyde S, Abdalla ME. Mapping health, social and health system issues and applying a social accountability inventory to a problem based learning medical curriculum. Med Educ Online. 2022;27(1):2016243. doi:10.1080/10872981.2021.2016243
17. Neville AJ. Problem-based learning and medical education forty years on: a review of its effects on knowledge and clinical performance. Med Princ Pract. 2008;18(1):1–9. doi:10.1159/000163038
18. Kelly D, Neville S, Abdalla ME. Embedding social accountability into the medical curriculum: strategies, insights, and real-world applications. In: Social Accountability of Medical Schools: Empowering the Future of Medical Education and Healthcare Systems. Springer; 2025:179–202.
19. Kolmos A, De Graaff E, Du X. Diversity of PBL–PBL learning principles and models. In: Research on PBL Practice in Engineering education. Brill; 2009:9–21.
20. Rourke J. AM last page: social accountability of medical schools. Acad Med. 2013;88(3):430. doi:10.1097/ACM.0b013e3182864f8c
21. Organization WH. Towards unity for health: challenges and opportunities for partnership in health development; 2000.
22. Ten Cate O. Entrustability of professional activities and competency-based training. Med Educ. 2005;39(12):1176–1177. doi:10.1111/j.1365-2929.2005.02341.x
23. Gummesson C, Alm S, Cederborg A, et al. Entrustable professional activities (EPAs) for undergraduate medical education–development and exploration of social validity. BMC Med Educ. 2023;23(1):635. doi:10.1186/s12909-023-04621-6
24. Hardee JT, Platt FW, Kasper IK. Discussing health care costs with patients: an opportunity for empathic communication. J Gen Intern Med. 2005;20:666–669. doi:10.1111/j.1525-1497.2005.0125.x
25. Abubshait LS, Guirguis S, Pocquette S, Cofer T, Omodt‐Lopez A. Beyond the symptoms: team‐based learning for social determinants in emergency medicine training. AEM Educ Train. 2024;8(5):e11030. doi:10.1002/aet2.11030
26. Masava B, Nyoni CN, Botma Y. Scaffolding in health sciences education programmes: an integrative review. Med Sci Educator. 2023;33(1):255–273. doi:10.1007/s40670-022-01691-x
27. Fleet LJ, Kirby F, Cutler S, Dunikowski L, Nasmith L, Shaughnessy R. Continuing professional development and social accountability: a review of the literature. J Interprofessional Care. 2008;22(sup1):15–29. doi:10.1080/13561820802028360
28. Wood B, Fitzgerald M, Kendall C, Cameron E. Integrating socially accountable health professional education and learning health systems to transform community health and health systems. Learn Health Syst. 2021;5(3):e10277. doi:10.1002/lrh2.10277
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Understanding the Impact of Generation Gap on Teaching and Learning in Medical Education: A Phenomenological Study
Josephine J, Jones L
Advances in Medical Education and Practice 2022, 13:1071-1079
Published Date: 16 September 2022
Incorporation of Comprehensive Examinations for a Time-Efficient Remediation Method
Gonzalez P, Moreno M, Iida T, Sieck B, Bester J, Simanton E
Advances in Medical Education and Practice 2022, 13:1417-1422
Published Date: 17 November 2022
Emotional Intelligence and Resilience “PROGRAM” Improves Wellbeing and Stress Management Skills in Preclinical Medical Students
Versel JL, Plezia A, Jennings L, Sontag-Milobsky I, Adams W, Shahid R
Advances in Medical Education and Practice 2023, 14:1309-1316
Published Date: 20 November 2023
Educating Our Future Medical Leaders: An Innovative Longitudinal Course Across Surgical and Medical Specialties in Graduate Education
Jaramillo-Restrepo V, Losee JE, Bump GM, Bison-Huckaby M, Merriam S
Journal of Healthcare Leadership 2024, 16:255-262
Published Date: 1 July 2024