Back to Journals » Nature and Science of Sleep » Volume 18

Translating Evidence into Obstetric Care: Developing a Best Practice-Informed Stepped-Care Clinical Algorithm for the Management of Gestational Insomnia
Authors Zhao FY ![]() , Yue LP, Ho YS, Xu P, Broadbear JH, Zhang WJ, Wang YM, Fu QQ
, Yue LP, Ho YS, Xu P, Broadbear JH, Zhang WJ, Wang YM, Fu QQ ![]() , Conduit R
, Conduit R ![]()
Received 17 March 2026
Accepted for publication 4 June 2026
Published 19 June 2026 Volume 2026:18 607896
DOI https://doi.org/10.2147/NSS.S607896
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sarah L Appleton
Fei-Yi Zhao,1– 4,* Li-Ping Yue,1,* Yuen-Shan Ho,5,* Peijie Xu,6,* Jillian H Broadbear,7,8 Wen-Jing Zhang,4 Yan-Mei Wang,4 Qiang-Qiang Fu,9 Russell Conduit2
1Department of Nursing, School of International Medical Technology, Shanghai Sanda University, Shanghai, 201209, People’s Republic of China; 2School of Health and Biomedical Sciences, RMIT University, Bundoora, VIC, 3083, Australia; 3Sydney School of Health Sciences, Faculty of Medicine and Health, The University of Sydney, Camperdown, NSW, 2050, Australia; 4Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 200071, People’s Republic of China; 5School of Nursing, Faculty of Health and Social Sciences, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China; 6School of Computing Technologies, RMIT University, Melbourne, VIC, 3000, Australia; 7Spectrum Personality Disorder and Complex Trauma Service, Richmond, VIC, 3121, Australia; 8Eastern Health Clinical School, Monash University, Clayton, VIC, 3800, Australia; 9Yangpu Hospital, School of Medicine, Tongji University, Shanghai, 200090, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jillian H Broadbear, Spectrum Personality Disorder and Complex Trauma Service, Richmond, Victoria, 3121, Australia, Tel +61 3 8413 8750, Fax +61 3 9871 3911, Email [email protected] Qiang-Qiang Fu, Yangpu Hospital, School of Medicine, Tongji University, Shanghai, 200090, People’s Republic of China, Tel + 86 021-6569 0520, Fax +86 021-6569 6249, Email [email protected]
Background and Aims: Insomnia during pregnancy is potentially associated with adverse outcomes, including gestational diabetes mellitus, pre-eclampsia, cesarean delivery, preterm birth, and depression. This study aimed to synthesize available evidence on the management of gestational insomnia and develop a clinical algorithm to inform obstetric care practice.
Methods: Based on the best available evidence, a clinical algorithm was developed as follows. First, a systematic search was conducted following the 6S evidence pyramid, including clinical practice guidelines, expert consensus statements, evidence summaries, and algorithms or decision aids published from database inception to January 2026. Second, four reviewers independently screened and appraised the literature. Third, two sleep medicine physicians extracted and synthesized the evidence using the JBI Grading of Evidence and Recommendation System. Finally, the clinical algorithm was constructed based on the synthesized evidence.
Results: Nineteen publications were included, i.e., nine expert consensus statements, eight clinical guidelines, one clinical decision aid, and one evidence summary, from which 31 practice recommendations were derived. These recommendations fit within five key domains: (1) overarching principles emphasizing symptom control, stress management, and family support; (2) lifestyle-based interventions; (3) CBT-i and its digital delivery modalities; (4) pharmacotherapy; and (5) complementary and alternative medicine (CAM). Collectively, they create a stepped-care management pathway for gestational insomnia, beginning with lifestyle modifications, followed by CBT-i for patients with more severe symptoms (which can be supplemented by CBT-i Coach app to enhance self-management during treatment), and finally considers pharmacotherapy (at the lowest effective dose and shortest feasible duration) or CAM therapies (e.g. acupuncture) for women who respond poorly to psychotherapy or present with comorbid somatic/emotional disorders.
Conclusion: This study proposes a stepped-care algorithm for managing gestational insomnia. As it is based on evidence synthesis rather than prospective clinical validation, its real-world effectiveness remains to be established. Furthermore, its implementation should be tailored to patient preferences and local healthcare resources to ensure contextual relevance and clinical feasibility.
Keywords: sleep disturbance, sleep disorder, pregnancy, summary of evidence, best practice summary, restless legs syndrome/Willis-Ekbom disease, obstructive sleep apnea
Background
Insomnia, a common adult disorder, is defined by dissatisfaction with sleep quality or duration, including sleep initiation difficulty, nocturnal or early-morning awakenings, or non-restorative sleep, along with daytime impairments such as fatigue, cognitive dysfunction, and emotional distress.1 Its global prevalence is estimated at 16.2%,2 with markedly higher rates during pregnancy. Approximately 20% of Chinese pregnant women meet the clinical criteria for insomnia.3 In Lebanon, 40.4%, 25.5%, and 8.5% of pregnant women experienced subclinical, moderate, and severe insomnia, respectively.4 In Poland, among pregnant women, 20.2% reported difficulties initiating sleep and 52.8% reported frequent nocturnal awakenings.5 A meta-analysis encompassing 15,564 participants further indicated that insomnia prevalence varies by trimester, peaking in the third trimester (39.7%) compared to the first (25.3%) and second (27.2%) trimesters.6 Several factors contribute to insomnia in pregnancy, including hormonal fluctuations, physical discomforts (such as nausea, back pain, and frequent urination), inadequate respiration, and changes in body position due to abdominal enlargement.7 Addressing gestational insomnia is critical, as it not only impairs quality of life (QoL)7 and social functioning,8 but is also associated with adverse pregnancy outcomes such as gestational diabetes,9 hypertensive disorders of pregnancy including preeclampsia,8 and preterm birth.9 Furthermore, prenatal insomnia may elevate the risk of postpartum depression.10
Cognitive Behavioral Therapy for Insomnia (CBT-i) is recommended as the first-line strategy for insomnia11 and has demonstrated efficacy in managing gestational insomnia.12 CBT can be delivered through multiple modalities, including traditional in-person formats (individual or group-based), fully digital or multimedia-based approaches (eg., telephone support, email, computer- or mobile applications-based platforms, audio/video programs, and self-help books), and blended models that combine face-to-face (F2F) sessions with multimedia components.13 Hypnotic and sedative agents are also commonly prescribed for insomnia management.12 However, the use of benzodiazepines and Z-hypnotics to treat gestational insomnia presents considerable challenges due to potential risks to both maternal and fetal health.14 Beyond obstetricians and midwives, pregnant women may consult other healthcare providers—such as acupuncturists or naturopaths—who may recommend complementary and alternative medicine (CAM) therapies for insomnia.15 A systematic review suggests that exercise, acupuncture, and massage are commonly advised for gestational insomnia and may be associated with improved sleep quality; however, the supporting evidence is of low quality.15
In 2022, a joint position paper by the European Insomnia Network, the Italian Marcè Society, and the International Experts Task Force for Perinatal Mental Health provided guidance on assessing and managing peripartum insomnia.16 It endorsed CBT-i as the preferred treatment for gestational insomnia, noting that pharmacotherapy may be considered when nonpharmacological interventions are ineffective, in cases of severe insomnia linked to mood or anxiety disorders, or when no alternatives exist and the anticipated benefits outweigh potential risks.16 Professional organizations, including the BSA17 and the CSRS,18 have also periodically updated their clinical practice guidelines (CPGs) to incorporate recommendations for managing gestational insomnia. Nevertheless, due to variations in the objectives, focus areas, and target populations across these guidelines and expert consensus statements, the existing evidence remains fragmented and lacks an integrated framework. Notably, certain recommendations across guidelines/consensuses are not entirely consistent and occasionally contradictory. For instance, a 2019 consensus by the BAP suggests that mild-to-moderate exercise in the evening improves gestational insomnia,19 whereas the 2020 NICE guideline advises pregnant women with sleep disturbances to reduce activity before bedtime.20 Similarly, guidance on the use of Zopiclone and Eszopiclone during pregnancy differs between the BSA17 and the CSRS.21 Systematic integration of these recommendations, with clarification of areas of consensus and divergence, is a prerequisite for establishing a unified and actionable basis for clinical decision-making. Accordingly, this study conducted a systematic review of the available evidence to identify core intervention components for gestational insomnia, critically appraised the strength of the evidence, and formulated a clinical algorithm based on consolidated best-practice recommendations to inform the clinical management of insomnia during pregnancy.
Methods
This evidence summary was developed following the JBI Manual for Evidence Synthesis.22 Its methodological framework included problem formulation, systematic literature retrieval, study selection and quality appraisal, evidence synthesis and grading, as well as evidence translation and recommendation development.23
Problem Formulation
The PIPOST tool24 was applied to structure the clinical question— “How can gestational insomnia be managed effectively and safely?”—into an evidence-based format. The population (P) consisted of pregnant women diagnosed with insomnia. Interventions (I) included lifestyle modification, psychological and behavioral therapies, pharmacological options, and CAM. The intended professionals (P) were clinicians working in obstetrics, clinical psychology, and sleep medicine. Outcomes (O) comprised insomnia severity, pregnancy-related QoL, and childbirth outcomes. Settings (S) involved obstetric clinics or wards, sleep medicine units, psychological service centers, and community health facilities. Evidence Types (T) encompassed decision-support tools, consensus statements, CPGs, and evidence summaries.
Evidence Retrieval
Evidence retrieval was guided by the 6S evidence pyramid,25 with a hierarchical search strategy proceeding from higher- to lower-level evidence sources. Initial searches targeted databases of decision support systems and best-practice resources (eg., BMJ Best Practice, UpToDate, and the JBI EBP Database), as well as guideline repositories (eg., SIGN, GIN, NGC/AHRQ, NICE, and CPG Infobase). Additional searches were performed in comprehensive English and Chinese databases (eg., CNKI, SinoMed, Wanfang, CQVIP, MEDLINE, CENTRAL, and Embase) and websites of professional organizations in obstetrics and sleep medicine (eg., RACGP, RNAO, AASM, CSRS, ESRS, SOGC, CMDA, and ACOG). Reference lists of eligible studies were manually screened to ensure comprehensiveness. The search covered publications from the inception of each database through January 2026. Detailed search strategies are provided in Appendix 1.1 and Appendix 1.2. The search was executed on February 1, 2026, in compliance with the PRISMA-S Checklist (Appendix 1.3).
Literature Screening and Quality Appraisal
Inclusion and Exclusion Criteria
Literature was included if it met the following criteria: (1) the study population comprised pregnant women diagnosed with insomnia; (2) the content focused on strategies for managing gestational insomnia; (3) evidence types were limited to consensus statements, CPGs (including consensus-based guidelines), algorithms or clinical decision aids (including recommended practices), and evidence summaries, to ensure clinical applicability and comprehensiveness. Systematic reviews were excluded to avoid duplication, as guidelines and consensus statements are typically developed based on systematic review evidence. Primary studies, situated at the base of the 6S evidence pyramid,25 were also excluded, as their findings are susceptible to sample size, design bias, and confounding factors.26 The inherent instability and limited generalizability of results from individual primary studies render them lower in evidentiary priority than higher-level sources—such as recommendations from guidelines and consensus statements—which undergo systematic synthesis; (4) publications were written in English or Chinese. In cases where multiple versions of a guideline or consensus from the same organization existed, recommendations were primarily extracted from the most recent version, with supplementary content from earlier versions if omitted in the update, to ensure completeness of the extracted recommendations.
Literature was excluded if it met any of the following criteria: (1) research protocols, drafts, or abstracts without full text; (2) unavailability of full text despite reasonable efforts to obtain them; (3) significant methodological flaws (ie., extremely low quality); (4) translations or interpretations of original publications.
Literature Screening
All retrieved records were imported into Zotero (version 7.0) for management, and duplicates were removed. Two researchers (QQ-F and P-X), both trained in systematic literature retrieval and data entry, independently screened titles and abstracts against the inclusion and exclusion criteria. Disagreements were resolved through consultation with a third reviewer (FY-Z). Subsequently, the same reviewers independently extracted data using a standardized form, with blinding to each other’s results. Extracted information included study characteristics such as first author or organization, publication year, language, source, literature type, and thematic focus.
Literature Quality Assessment
Quality appraisal tools were selected based on literature type. CPGs were evaluated using the AGREE II instrument.27 Consensus statements were assessed with the JBI Critical Appraisal Checklist for Textual Evidence: Expert Opinion.28 For clinical algorithms or decision aids, quality was determined based on the methodological rigor of the source documents (eg., guidelines or consensus statements). Evidence summaries were appraised using the Revised CASE Worksheet.29
Four researchers (WJ-Z, LP-Y, FY-Z, and QQ-F), all trained in evidence-based methodology and with relevant practical experience, independently conducted the quality appraisal. Discrepancies were resolved through discussion until consensus was reached. Inter-rater reliability was quantified using the intraclass correlation coefficient (ICC).
Evidence Synthesis, Translation, and Development of Practical Recommendations
First, following an established framework for evidence synthesis,30 two researchers (FY-Z and WJ-Z), each with over a decade of clinical experience in sleep medicine, independently and concurrently extracted and summarized evidence from the included literature according to the following criteria: (1) for evidence with identical content, the version with the clearest, most specific, and most concise expression was retained; (2) for evidence with similar or complementary content, individual statements were merged into a unified recommendation; (3) for conflicting evidence, the original sources were traced, and priority was given to higher-quality and more recently published evidence from authoritative sources. All included evidence was graded according to the JBI Levels of Evidence System (Levels 1–5),31 based on study design.
Subsequently, the two researchers cross-verified the synthesized evidence and corresponding levels. Disagreements were resolved through discussion; if consensus could not be achieved, a third expert in sleep medicine (R-C) provided adjudication.
Finally, the strength of each synthesized recommendation was determined using the FAME (Feasibility, Appropriateness, Meaningfulness, and Effectiveness) Scale, in conjunction with the JBI Grades of Recommendation. Following panel discussions, each recommendation was classified as either a Strong Recommendation (Grade A) or a Weak Recommendation (Grade B).31 The FAME-based grading methodology is detailed in Appendix 2.
Results
Literature Search Results and Overview
The systematic search identified 178 records. After duplicate removal using Zotero, 81 records remained. Following full-text assessment, 19 documents were ultimately included: nine consensus statements, eight CPGs, one clinical decision aid, and one evidence summary. The detailed screening process is presented in Appendix 3, and the excluded literature with reasons for exclusion are provided in Appendix 4.
The basic characteristics of the included literature are summarized in Appendix 5. Among the eight CPGs, five involved version updates. Three were published by the Sleep Disorders Group of the CMA, with the initial version released in 2012,32 followed by updates in 201733 and 2023.34 The other two were published by the CSRS, with the first edition in 201721 and an updated version in 2025.18 As specified in the Methods section, during evidence extraction and synthesis, priority was given to the most recent versions, with earlier versions serving as supplementary sources. No updated versions were identified for the remaining included documents.
Literature Quality Appraisal Results
Among the eight included CPGs, two17,20 achieved standardized scores of 60% or higher across all six AGREE II domains, meeting the criteria for a Grade A recommendation. The remaining six guidelines were rated as Grade B (Appendix 6).
All expert consensus statements were included. One statement issued by the BAP19 demonstrated clarity and explicitness across all appraisal dimensions. Only one statement35 lost points on “Item 5 Is there reference to the extant literature?” due to the absence of clearly cited sources supporting the recommendations related to insomnia management during pregnancy (Appendix 7).
The single evidence summary36 was rated as moderate in quality. Downgrading was primarily attributable to “No” ratings for the items “Are the reviewer(s)/editor(s) of the summary transparent?” and “Are the recommendations current?”, as well as “Not Completely” ratings for “Are the search methods transparent and comprehensive?” and “Are the recommendations appropriately cited?” (Appendix 8).
The single clinical decision aid16 was based on a high-quality guideline concerning antenatal and postnatal mental health management and service provision issued by NICE.20 Accordingly, it was classified as a high-quality evidence source (Level A) (Appendix 9).
Inter-rater reliability during the quality appraisal process was high. ICC values ranged from 0.76 to 0.84 across all evaluated documents, exceeding the 0.75 threshold indicative of strong agreement.
Generation of Recommendations and Clinical Decision-Making Algorithm
Through iterative comparison, analysis, and discussion, the extracted evidence was organized into five overarching themes: (1) general principles for managing gestational insomnia; (2) behavioral interventions; (3) CBT-i-centered psychotherapy; (4) pharmacotherapy for primary insomnia and insomnia comorbid with other somatic/emotional disorders; and (5) complementary and integrative therapies. A total of 31 actionable recommendations were formulated, including 17 strong recommendations and 14 weak recommendations (see Table 1).
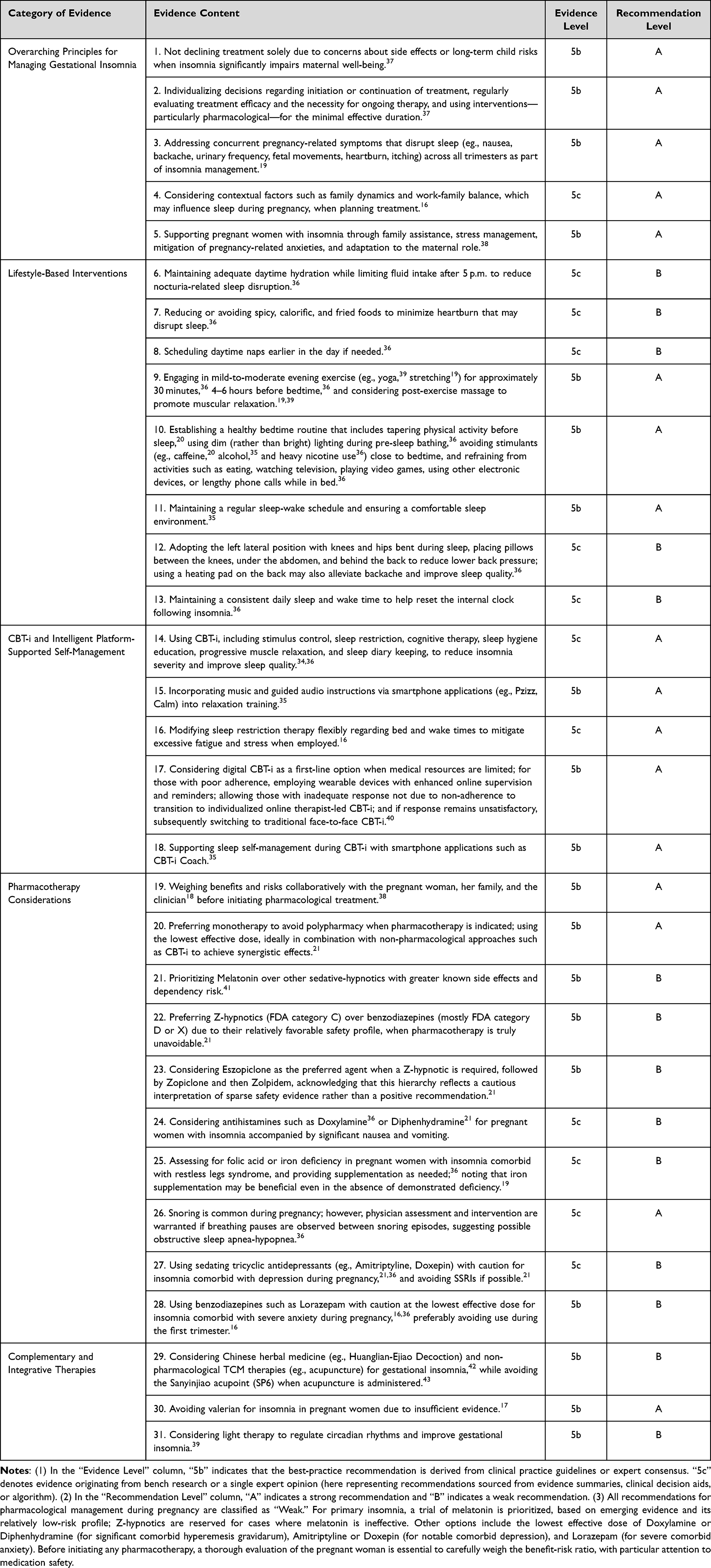 |
Table 1 Best-Practice Recommendations for the Multimodal Management of Gestational Insomnia |
These five themes can be conceptualized as a stepped-care model: within this comprehensive treatment framework, lifestyle modifications are prioritized as the first-line approach, followed by CBT-i. Pharmacological or CAM interventions are considered only when CBT-i yields insufficient clinical response. The corresponding implementation pathway has been operationalized as a clinical decision-making algorithm (see Figure 1).
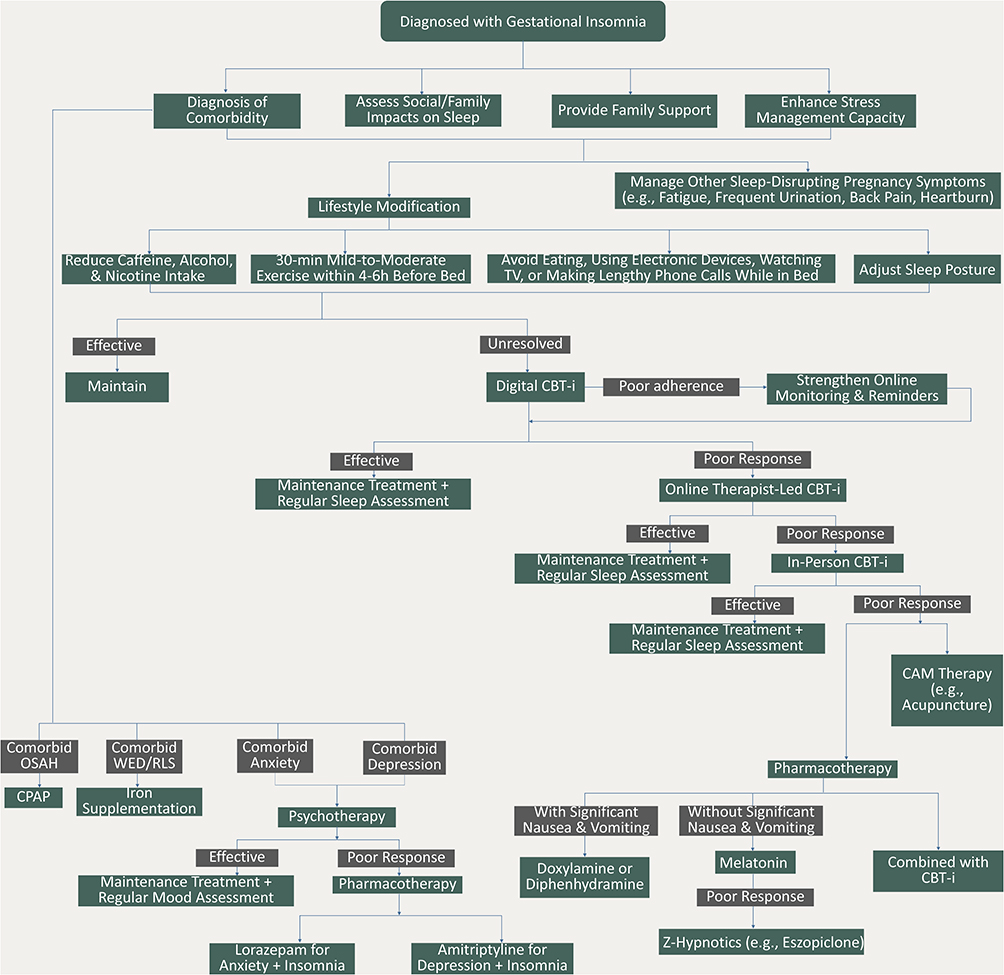 |
Figure 1 Evidence-Based Clinical Algorithm for the Management of Gestational Insomnia. Abbreviations: CBT-i, Cognitive Behavioral Therapy for Insomnia; CPAP, Continuous Positive Airway Pressure; OSAH, Obstructive Sleep Apnea-Hypopnea; WED/RLS, Willis-Ekbom Disease/Restless Legs Syndrome. |
Discussion
Overarching Principles: Symptom Control, Stress Management, and Family Support
Emerging evidence suggests that identifying and managing sleep disorders during pregnancy may help reduce adverse pregnancy outcomes and enhance maternal and fetal well-being.44 Pregnant women often express substantive concerns about their sleep. For instance, a cross-sectional study at the University of California found that among pregnant women with moderate-to-severe insomnia (ISI score > 14), 57% had discussed their sleep issues with a healthcare provider.45 Accordingly, our algorithm recommends that when insomnia adversely affects a pregnant woman’s well-being, a personalized treatment plan should be initiated, with ongoing monitoring and evaluation to guide dynamic clinical decision-making.37
Sleep quality is influenced by gestational stage and associated symptoms. In the first trimester, nausea, back pain, and frequent urination are the primary disruptors. During the second trimester, fetal movements and heartburn may disturb sleep. By the third trimester, in addition to the recurrence of back pain and urinary frequency, women may experience cramps, itching, and vivid or unpleasant dreams, resulting in more frequent nocturnal awakenings compared with earlier trimesters.19 Effective management of these pregnancy-specific symptoms is therefore likely to alleviate insomnia.
Beyond fostering a positive coping attitude toward insomnia and addressing pregnancy-related symptoms, clinical practitioners—particularly psychologists—are encouraged to strengthen pregnant individuals’ capacity for stress management.38 This may include guiding them to alleviate distressing thoughts related to pregnancy and childbirth and supporting adaptation to role transitions.38 Evidence indicates that perceived stress is strongly associated with poorer sleep quality in pregnant women, who are more sensitive to stress than non-pregnant women; higher stress levels correlate with shorter sleep duration and progressively worse sleep.46 Conversely, interventions that reduce prenatal stress may effectively ameliorate insomnia.46 Enhanced family support also moderates the impact of pregnancy-related stress on sleep,47 highlighting the importance of educating women about available support and encouraging families to provide increased care and attention, which can reduce the incidence or severity of pregnancy insomnia.16,38,47
Lifestyle Modifications: From Diet and Exercise to Environment and Body Positioning
Lifestyle modifications are strongly supported by the included evidence as a primary approach for preventing and alleviating gestational insomnia (Table 1). This aligns with prior research indicating that greater adherence to healthy lifestyle behaviors in pregnant women is associated with fewer sleep disturbances and improved sleep quality.48
Nocturnal eating is common due to increased physiological appetite,49 but prospective data indicate it correlates with sleep disturbances as evidenced by higher PSQI scores.50 Thus, minimizing nighttime eating—particularly in bed—is advised.36 Consumption of spicy, calorific, or fried foods should also be limited to reduce heartburn-related sleep disruption.36 Psychoactive substances such as caffeine,20 alcohol,35 and heavy nicotine use36 should be avoided before bedtime. Pregnant women are physiologically prone to nocturia due to elevated progesterone levels and increased glomerular filtration rate,51 a factor that contributes to sleep disruption during the first and third trimesters.19 Therefore, while adequate daytime hydration is encouraged, fluid intake after 5 p.m. should be restricted to minimize nocturia-related sleep interruptions.36
Exposure to artificial light at night has been identified as a general risk factor for poor sleep.50 Reducing nighttime light exposure is recommended, and dim nightlights can be used when necessary, such as during evening bathroom visits.36
Although early AASM guidance suggested in 2001 that exercise before sleep may impair sleep quality,50 subsequent research, including the 2013 Sleep in America Poll, found no adverse association with evening exercise.52 A 2019 meta-analysis further challenged the notion that evening exercise negatively affects sleep, though it cautioned that vigorous exercise performed within one hour of bedtime might impair sleep due to inadequate cardiovascular recovery, resulting in elevated heart rate and reduced parasympathetic activity at bedtime.53 Based on these findings, pregnant women are recommended to engage in approximately 30 minutes of mild-to-moderate evening exercise, ideally 4–6 hours before bedtime,36 such as prenatal yoga39 or stretching.19
Sleep discomfort due to body position is another common disturbance.54 Pregnant women should avoid supine sleep, particularly in late pregnancy, due to risks of maternal cardiovascular compromise and stillbirth.55 A left lateral tilt posture—lying on the left side with knees and hips flexed and pillows placed under the abdomen, between the knees, and behind the back—can reduce lower back pressure and improve sleep comfort.36
CBT-i: Digital Delivery and Platform-Supported Self-Management
Numerous systematic reviews have demonstrated that CBT-i effectively improves gestational insomnia12,56 and may concurrently alleviate depressive and anxiety symptoms in affected women.12 A Canadian cross-sectional survey indicated that, compared with other therapies, pregnant women preferred CBT-i for managing insomnia.57 Consistently, most clinical guidelines and expert consensus statements recommend that, when insomnia persists despite lifestyle modifications, psychological interventions—particularly CBT-i—should be prioritized.34,35,40
A major barrier to the widespread use of CBT-i is the insufficient availability of trained clinicians relative to clinical demand.58 Digital CBT-i programs help bridge this science-care gap and are particularly relevant for pregnant women, who favor flexible mental health care and benefit from timely interventions.58 Several randomized controlled trials (RCTs) have shown that digital CBT-i reduces insomnia symptoms, prolongs sleep duration,58,59 mitigates subclinical anxiety and depressive symptoms associated with insomnia,58 and may even prevent postpartum sleep loss.59
The 2024 Chinese Expert Consensus on Digital Therapeutics for Insomnia advises clinicians to enhance adherence among pregnant women receiving digital CBT-i by strengthening online supervision and reminders, or by requiring them to use wearable devices to collect objective sleep data.40 Only when insomnia persists due to “non-adherence reasons” should in-person CBT-i (i.e., F2F-CBT-i) be considered.40 Another Chinese expert consensus published in 2025 further recommends CBT-i Coach—featuring sleep diaries, prescription updates, alarms, and reminders—to support F2F-CBT-i in pregnant women.35 Developed by the U.S. Department of Veterans Affairs and Department of Defense, CBT-i Coach is a free mobile health application delivering core CBT-i components.60 Evidence from an RCT confirms that integrating CBT-i Coach with individual CBT-i is highly feasible and acceptable to patients, enhancing their access to therapy materials and yielding significant improvements in sleep quality.61
In resource-limited settings where digital or F2F-CBT-i is unavailable, brief behavioral treatment for insomnia (BBT-i) offers a feasible alternative. Compared with standard CBT-i, BBT-i requires fewer visits, a shorter treatment duration, and can be delivered by primary care nurses rather than specialized psychologists, lowering barriers to access.62 Although current CPGs, consensus statements and decision aids do not yet include BBT-i, a randomized controlled trial in Australia has shown its preliminary efficacy for alleviating sleep disturbances, including insomnia, in late-pregnancy women.63 We recommend that guideline developers continue to monitor emerging evidence on BBT-i’s safety and efficacy for gestational insomnia and consider its potential inclusion in future updates.
Pharmacological Management: Indications, Principles, and Considerations for Comorbid Conditions
Pharmacotherapy should be considered only for severe cases where symptoms persist despite CBT-i and other non-pharmacological interventions. Prior to initiating medication, the potential benefits and risks must be thoroughly weighed,38 and the treatment decision should be made collaboratively by the patient, her family members, and the clinicians.18 Key principles for medication use include prescribing the minimum effective dose, limiting treatment duration, and preferring monotherapy whenever feasible to avoid polypharmacy.21 The integration of pharmacological and non-pharmacological approaches (eg., CBT-i) is encouraged to augment sleep-promoting effects.21
Due to the lack of extensive clinical trials on pregnant women, the safety profiles of sedative-hypnotics remain unestablished. The U.S. FDA classifies most benzodiazepines as Category D and Z-hypnotics as Category C;64 while this suggests a relatively lower risk for the latter, the inference is drawn from limited data.21 Therefore, in clinical practice where pharmacotherapy is deemed unavoidable, Z-hypnotics like Eszopiclone38 and Zopiclone19,65 are considered acceptable under strict therapeutic supervision, though they should not be interpreted as first-line treatments. Additionally, a Singapore expert consensus, based on limited evidence, recommends melatonin over other sedative-hypnotics with greater side effects and dependence risks.41
Pharmacological management may also be indicated for insomnia comorbid with other conditions. In cases where gestational insomnia coexists with mood disorders and shows inadequate response to psychotherapy, tricyclic antidepressants (eg., Amitriptyline, Doxepin) may be cautiously prescribed for comorbid depression,21,36 or low-dose Lorazepam for comorbid anxiety.16,36 For pregnant women with insomnia accompanied by significant nausea and vomiting, antihistamines such as Doxylamine36 or Diphenhydramine21 may be appropriate. Comorbid conditions such as restless legs syndrome (RLS)66 and obstructive sleep apnea-hypopnea (OSAH)67 are also frequently observed in pregnant women with insomnia. Patients with concurrent RLS often experience prolonged sleep onset latency and more severe depressive symptoms, with iron and folate deficiencies playing a mediating role in this association.66 Accordingly, timely screening for and correction of these deficiencies is recommended.19,36 Data from a U.S. survey indicate that 15.7% of women in their third trimester report comorbid habitual snoring and insomnia, which is associated with increased risk of hypertension and other adverse pregnancy outcomes.67 Thus, screening for OSAH and prompt intervention are warranted in pregnant women with insomnia and suspected OSAH.36
CAM Strategies in Prenatal Insomnia Care: Focus on Acupuncture, Herbal Remedies, and Light Therapy
Limited access to CBT-i and concerns regarding the adverse effects of sedative-hypnotics are primary drivers for the adoption of CAM among individuals with insomnia.11 The popularity of CAM among pregnant women, specifically, is also partly motivated by a desire to maintain greater personal control over health and well-being.57 A national Australian survey reported that 48.1% of pregnant women consulted a CAM practitioner, and 52.0% used CAM products (excluding vitamins and minerals) during pregnancy.68
Two small controlled clinical trials have demonstrated that acupuncture can significantly improve sleep quality in pregnant women with insomnia.69,70 One of these studies further suggested that this effect may be mediated by increased melatonin secretion.69 Consequently, acupuncture has been incorporated into several Chinese guidelines and consensus statements for managing gestational insomnia.42,43 However, a specific precaution is noted: the Sanyinjiao acupoint (SP6) is generally considered contraindicated for needling43 due to concerns that its stimulation might provoke preterm uterine contractions.71
In addition to acupuncture, a Chinese guideline also recommends Huanglian-Ejiao Decoction for managing gestational insomnia.42 This aligns with China’s long tradition of using herbal medicine during pregnancy.72 A large cohort study of 199,710 pregnant individuals reported that 65.7% used Chinese herbal formulas.72 Similarly, a Swiss study found that 89.9% used herbal medicines during pregnancy.73 Among these, valerian and lavender are frequently employed to alleviate sleep disturbances and restlessness,73 though not currently recommended by guidelines for gestational insomnia.17 Given limited safety evidence, scholars advise obstetricians to routinely inquire about herbal or natural product use during prenatal checkups, and to educate pregnant women against assuming such medicines are inherently harmless.74
Evidence for other CAM modalities is more limited. Light therapy is recommended for pregnancy-related insomnia in only one consensus statement to date,39 although a previous meta-analysis supports its efficacy in improving both sleep disturbances and depressive symptoms in pregnant women.75
Implementation Considerations for the Algorithm: Multidisciplinary Collaboration and Role Delineation
Efficient implementation of the proposed stepped-care algorithm in real-world clinical settings requires overcoming traditional barriers among obstetrics, sleep medicine, clinical psychology, and community-based nursing. Obstetricians and midwives are responsible for delivering first-line, low-intensity interventions following a confirmed diagnosis of gestational insomnia (eg., sleep hygiene education, lifestyle modification guidance, etc.) while screening for comorbidities such as RLS or OSAH. Clinical psychotherapists oversee subsequent treatments, prioritizing digital CBT-i to reach a larger cohort of pregnant women with mild-to-moderate insomnia and reserving face-to-face therapy for severe cases or those with comorbidities. Community nurses should longitudinally monitor treatment adherence during lifestyle modification and CBT-i interventions, promptly identifying poor responders and alerting sleep medicine physicians and obstetricians to collaboratively evaluate and initiate pharmacological treatment when necessary.
Limitations
In an effort to enhance the clinical relevance and practical applicability of the existing recommendations, this study synthesized evidence exclusively from CPGs, consensus statements, and decision-support materials. Although this approach bolsters the authority of the recommendations, the exclusion of primary research studies precludes the incorporation of the most recent research advancements.30 Therefore, the future accumulation of primary study findings will necessitate periodic systematic reviews and updates of guidelines and consensus statements, enabling the ongoing integration of emerging high-quality, high-level evidence into this clinical algorithm, thereby preserving its currency and evidentiary rigor.
Although each individual component of our algorithm (eg., lifestyle modifications, CBT-i, pharmacotherapy) is supported by evidence from various moderate-to-high-quality authoritative guidance sources, the stepped-care algorithm as a whole—including decision thresholds (eg., escalation from CBT-i to pharmacotherapy) and the sequential logic linking intervention tiers—has not been prospectively validated. Consequently, whether adherence to this algorithm is more effective in improving clinical outcomes relative to existing obstetric care protocols warrants careful evaluation in future implementation science research.30
In addition, the literature search was confined to publications in Chinese and English, potentially omitting critical evidence from databases in other languages.
Finally, the synthesized evidence inherently reflects the contextual conditions, regional variations, and demographic characteristics of the settings in which the included sources were developed. Socioeconomic, cultural, and behavioral barriers that may differentially affect adherence to these interventions among pregnant women with insomnia in other regions or ethnic groups were not systematically evaluated. Consequently, cultural adaptation and local validation are necessary when applying these recommendations across diverse populations and healthcare settings worldwide.76
Conclusion
Through a systematic and comprehensive evidence synthesis, this study developed 31 recommendations and established an integrated clinical algorithm for the management of gestational insomnia. This algorithm operationalizes a patient-centered, stepped-care approach supported by the available evidence. Initially, pregnant women with insomnia are advised to implement multidimensional lifestyle modifications encompassing diet, exercise, and sleeping positions. For those with more severe insomnia, CBT-i is recommended, potentially augmented by smart platforms such as CBT-i Coach to facilitate daily self-management and enhance treatment adherence. Pharmacological interventions or CAM therapies are reserved for cases exhibiting inadequate response to psychological and behavioral interventions. Concurrently, the algorithm emphasizes stress management training for pregnant women and advocates for adequate family support from relatives. By translating existing evidence into a clear step-by-step decision pathway, this algorithm has the potential to narrow the gap between evidence and clinical practice and contribute to improved sleep health among pregnant women experiencing insomnia. Nevertheless, it should be emphasized that this algorithm should currently be interpreted as an evidence-informed structured framework rather than a definitive clinical protocol, as its feasibility and effectiveness require prospective validation in real-world obstetric settings.
Abbreviations
AASM, American Academy of Sleep Medicine; AGREE II, Appraisal of Guidelines for Research and Evaluation II; AHRQ, Agency for Healthcare Research and Quality; ACOG, American College of Obstetricians and Gynecologists; BAP, British Association for Psychopharmacology; BBT-i, Brief Behavioral Treatment for Insomnia; BMJ, British Medical Journal; BSA, Brazilian Sleep Association; CASE, Critical Appraisal for Summaries of Evidence; CAM, Complementary and Alternative Medicine; CBT, Cognitive Behavioral Therapy; CBT-i, Cognitive Behavioral Therapy for Insomnia; CMA, Chinese Medical Association; CMDA, Chinese Medical Doctor Association; CSRS, Chinese Sleep Research Society; CPG(s), Clinical Practice Guideline(s); CPG Infobase, Canadian Clinical Practice Guidelines Infobase; EBP, Evidence-based Practice; ESRS, European Sleep Research Society; F2F-CBT, Face-to-Face CBT; GIN, Guidelines International Network; ICC, Intraclass Correlation Coefficient; ISI, Insomnia Severity Index; JBI, Joanna Briggs Institute; NGC, National Guideline Clearinghouse; NICE, National Institute for Health and Care Excellence; OSAH, Obstructive Sleep Apnea-Hypopnea; PSQI, Pittsburgh Sleep Quality Index; QoL, Quality of Life; RACGP, Royal Australian College of General Practitioners; RCT(s), Randomized Controlled Trial(s); RLS, Restless Legs Syndrome; RNAO, Registered Nurses’ Association of Ontario; SIGN, Scottish Intercollegiate Guidelines Network; SOGC, Society of Obstetricians and Gynecologists of Canada.
Data Sharing Statement
The recommendations in this article are supported by data from the published literature identified through a systematic search. All referenced studies are listed in the reference section.
Author Contributions
Fei-Yi Zhao: Conceptualization, Formal analysis, Funding Acquisition, Investigation, Methodology, Writing - Original Draft Preparation. Li-Ping Yue: Formal analysis, Investigation, Writing - Review & Editing. Yuen-Shan Ho: Formal analysis, Investigation, Writing - review & editing. Peijie Xu: Data Curation, Writing - Review & Editing. Jillian H. Broadbear: Methodology, Supervision, Validation, Writing - Review & Editing. Wen-Jing Zhang: Investigation, Formal Analysis, Writing - Review & Editing. Yan-Mei Wang: Investigation, Formal Analysis, Writing - Review & Editing. Qiang-Qiang Fu: Visualization, Formal analysis, Investigation, Writing - Review & Editing. Russell Conduit: Conceptualization, Project administration, Supervision, Validation, Writing - review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Shanghai Key Laboratory for Pharmaceutical Metabolite Research Project [SHZYDX2023–01] and the Scientific Research Fund Project of Shanghai Sanda University [2024BSZX03] to FY-Z; and the Three-Year Action Plan for the Inheritance and Innovation of Traditional Chinese Medicine in Shanghai [ZY (2025-2027)-3-2-1] to YM-W.
Disclosure
The authors declare no competing interests in the reporting of this work.
References
1. Morin CM, Benca R. Chronic insomnia. Lancet. 2012;379(9821):1129–15. doi:10.1016/s0140-6736(11)60750-2
2. Benjafield AV, Sert Kuniyoshi FH, Malhotra A, et al. Estimation of the global prevalence and burden of insomnia: a systematic literature review-based analysis. Sleep Med Rev. 2025;82:102121. doi:10.1016/j.smrv.2025.102121
3. Wang WJ, Hou CL, Jiang YP, et al. Prevalence and associated risk factors of insomnia among pregnant women in China. Compr Psychiatry. 2020;98:152168. doi:10.1016/j.comppsych.2020.152168
4. Mourady D, Richa S, Karam R, et al. Associations between quality of life, physical activity, worry, depression and insomnia: a cross-sectional designed study in healthy pregnant women. PLoS One. 2017;12(5):e0178181. doi:10.1371/journal.pone.0178181
5. Smyka M, Kosińska-Kaczyńska K, Sochacki-Wójcicka N, et al. Sleep Problems in Pregnancy-A Cross-Sectional Study in over 7000 Pregnant Women in Poland. Int J Environ Res Public Health. 2020;17(15):5306. doi:10.3390/ijerph17155306
6. Sedov ID, Anderson NJ, Dhillon AK, et al. Insomnia symptoms during pregnancy: a meta-analysis. J Sleep Res. 2021;30(1):e13207. doi:10.1111/jsr.13207
7. Kızılırmak A, Timur S, Kartal B. Insomnia in pregnancy and factors related to insomnia. ScientificWorldJournal. 2012;2012:197093. doi:10.1100/2012/197093
8. Kember AJ, Elangainesan P, Ferraro ZM, et al. Common sleep disorders in pregnancy: a review. Front Med Lausanne. 2023;10:1235252. doi:10.3389/fmed.2023.1235252
9. Friedlander R, Huang X, Zee P, et al. Insomnia in pregnancy and obstetric outcomes. Sleep. 2025;48(2). doi:10.1093/sleep/zsae288
10. Chung TC, Chung CH, Peng HJ, et al. An analysis of whether sleep disorder will result in postpartum depression. Oncotarget. 2018;9(38):25304–25314. doi:10.18632/oncotarget.25219
11. Zhao FY, Spencer SJ, Kennedy GA, et al. Acupuncture for primary insomnia: effectiveness, safety, mechanisms and recommendations for clinical practice. Sleep Med Rev. 2024;74:101892. doi:10.1016/j.smrv.2023.101892
12. Zheng X, Zhu Z, Chen J, et al. Efficacy of cognitive behavioural therapy for insomnia or sleep disturbance in pregnant women: a systematic review ad meta-analysis. J Sleep Res. 2023;32(2):e13808. doi:10.1111/jsr.13808
13. Wu Q, Li J, Parrott S, et al. Cost-Effectiveness of Different Formats for Delivery of Cognitive Behavioral Therapy for Depression: a Systematic Review Based Economic Model. Value Health. 2020;23(12):1662–1670. doi:10.1016/j.jval.2020.07.008
14. Meng LC, Lin CW, Chuang HM, et al. Prescription Patterns and Predisposing Factors of Benzodiazepine and Z-Hypnotic Use During Pregnancy: a Nationwide Cohort Study. Pharmacoepidemiol Drug Saf. 2024;33(6):e5847. doi:10.1002/pds.5847
15. Hollenbach D, Broker R, Herlehy S, et al. Non-pharmacological interventions for sleep quality and insomnia during pregnancy: a systematic review. J Can Chiropr Assoc. 2013;57(3):260–270.
16. Palagini L, Bramante A, Baglioni C, et al. Insomnia evaluation and treatment during peripartum: a joint position paper from the European Insomnia Network task force “Sleep and Women,” the Italian Marcè Society and international experts task force for perinatal mental health. Arch Womens Ment Health. 2022;25(3):561–575. doi:10.1007/s00737-022-01226-8
17. Drager LF, Assis M, Bacelar AFR, et al. 2023 Guidelines on the Diagnosis and Treatment of Insomnia in Adults - Brazilian Sleep Association. Sleep Sci. 2023;16(Suppl 2):507–549. doi:10.1055/s-0043-1776281
18. Chinese Sleep Research Society. Guidelines for the Diagnosis and Treatment of Insomnia (2025 Edition). Nat Med J China. 2025;105(34):2960–2981. doi:10.3760/cma.j.cn112137-20250421-00981
19. Wilson S, Anderson K, Baldwin D, et al. British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders: an update. J Psychopharmacol. 2019;33(8):923–947. doi:10.1177/0269881119855343
20. National Institute for Health and Care Excellence NICE. Antenatal and postnatal mental health clinical management and service guidance updated edition. NICE Clinical Guidelines. 2020;192:1.
21. Chinese Sleep Research Society. Guidelines for the Diagnosis and Treatment of Insomnia in China. Nat Med J China. 2017;97(24):1844–1856.
22. Aromataris E, Lockwood C, Porritt K, et al. JBI Manual for Evidence Synthesis. JBI Collaboration; 2024. Available from: https://synthesismanual.jbi.global/.
23. Munn Z, Lockwood C, Moola S. The Development and Use of Evidence Summaries for Point of Care Information Systems: a Streamlined Rapid Review Approach. Worldviews Evid Based Nurs. 2015;12(3):131–138. doi:10.1111/wvn.12094
24. Tang J, Fan Y, Lu J, et al. Best Evidence for Preventing Urinary Tract Infections and Optimizing Care in Adults with Indwelling Urinary Catheters. Risk Manag Healthc Policy. 2025;18:3593–3608. doi:10.2147/rmhp.S557548
25. Krishnan V. From 4S to 6S: the growing evidence-based pyramid. J World Federat Orthodont. 2019;8(2):41–42. doi:10.1016/j.ejwf.2019.05.002
26. Khangura S, Konnyu K, Cushman R, et al. Evidence summaries: the evolution of a rapid review approach. Syst Rev. 2012;1:10. doi:10.1186/2046-4053-1-10
27. Dans AL, Dans LF. Appraising a tool for guideline appraisal (the AGREE II instrument). J Clin Epidemiol. 2010;63(12):1281–1282. doi:10.1016/j.jclinepi.2010.06.005
28. McArthur A, Cooper A, Edwards D, et al. Textual evidence systematic reviews series paper 3: critical appraisal of evidence from narrative, opinion, and policy. JBI Evid Synth. 2025;23(5):833–839. doi:10.11124/jbies-24-00293
29. Foster MJ, Shurtz S. Making the Critical Appraisal for Summaries of Evidence (CASE) for evidence-based medicine (EBM): critical appraisal of summaries of evidence. J Med Libr Assoc. 2013;101(3):192–198. doi:10.3163/1536-5050.101.3.008
30. Li J, Chen B, Liu N, et al. Best Evidence Summary of Folic Acid Supplementation for Prevention of Neural Tube Defects in Women of Childbearing Age. Nutrients. 2026;18(4):641. doi:10.3390/nu18040641
31. Liu R, Fan Z, Ma H, et al. Best evidence summary on sexual health management for patients undergoing intracavitary brachytherapy for gynecological neoplasms. Front Oncol. 2026;16:1770806. doi:10.3389/fonc.2026.1770806
32. Sleep Disorders Group Society of Neurology Chinese Medical Association. Guidelines for the Diagnosis and Treatment of Adult Insomnia in China. Chin J Neurol. 2012;45(7):534–540.
33. Sleep Disorders Group Society of Neurology Chinese Medical Association. Guidelines for the Diagnosis and Treatment of Adult Insomnia in China (2017 Edition). Chin J Neurol. 2018;51(5):324–335.
34. Sleep Disorders Group Society of Neurology Chinese Medical Association. Guidelines for the Diagnosis and Treatment of Adult Insomnia in China (2023 Edition). Chin J Neurol. 2024;57(6):560–584.
35. Sleep Group of Neurology Branch of Chinese Medical Doctor Association. Expert Consensus on Intelligent Hierarchical Diagnosis, Treatment and Prognostic Assessment of Insomnia Disorder. J Apoplexy Nervous Dis. 2025;42(10):867–877.
36. Hashmi AM, Bhatia SK, Bhatia SK, et al. Insomnia during pregnancy: diagnosis and Rational Interventions. Pak J Med Sci. 2016;32(4):1030–1037. doi:10.12669/pjms.324.10421
37. McAllister-Williams RH, Baldwin DS, Cantwell R, et al. British Association for Psychopharmacology consensus guidance on the use of psychotropic medication preconception, in pregnancy and postpartum 2017. J Psychopharmacol. 2017;31(5):519–552. doi:10.1177/0269881117699361
38. Chen GH, Deng LY, Du YJ, et al. Expert Consensus on Diagnosis and Treatment of Insomnia in Specific Populations. Chin J Clin Pharmacol Ther. 2024;29(8):841–852.
39. Collaborative Group on Perinatal Mental Disorders Psychosomatic Medicine Branch Chinese Medical Association. Expert Consensus on Screening, Diagnosis and Treatment of Perinatal Mental Disorders. Chin General Pract. 2023;26(28):3463–3470.
40. Chinese Sleep Research Society. Chinese Expert Consensus on Digital Therapeutics for Insomnia. Chin General Pract. 2024;27(4):381–390.
41. Ho R, Lim CS, Tor PC, et al. Pharmacological management of chronic insomnia disorder in Singapore: recommendations from an expert panel. Proc Singapore Healthcare. 2025;34:20101058251318763. doi:10.1177/20101058251318763
42. Li Y. Research on the Development of the “Guidelines for the Integrated Medicine Diagnosis and Treatment of Insomnia Disorder”. Henan University of Chinese Medicine; 2023.
43. Committee of Mental Diseases of Chinese Association of Integrative Medicine Committee of Psychosomatic Medicine of Chinese Association of Integrative Medicine. Expert Consensus on Integrative Medicine for the Diagnosis and Treatment of Insomnia Disorder. Chin J New Drugs. 35(6):597–608.
44. Nodine PM, Matthews EE. Common sleep disorders: management strategies and pregnancy outcomes. J Midwifery Womens Health. 2013;58(4):368–377. doi:10.1111/jmwh.12004
45. Felder JN, Hartman AR, Epel ES, et al. Pregnant Patient Perceptions of Provider Detection and Treatment of Insomnia. Behav Sleep Med. 2020;18(6):787–796. doi:10.1080/15402002.2019.1688153
46. Li G, Kong L, Zhou H, et al. Relationship between prenatal maternal stress and sleep quality in Chinese pregnant women: the mediation effect of resilience. Sleep Med. 2016;25:8–12. doi:10.1016/j.sleep.2016.02.015
47. Liu S, Huang M, Zhang F, et al. Family Support Moderates the Relationship Between Pregnancy Stress, Depressive Symptoms, and Insomnia. Nat Sci Sleep. 2025;17:261–270. doi:10.2147/nss.S496205
48. Yeşilkaya H, Gölbaşı Z. The Relationship Between Sleep Quality, Insomnia Severity, And Healthy Lifestyle Behaviours In Pregnant Women. Gazi Saglik Bilimleri Dergisi. 2025;10(2):40–51. doi:10.52881/gsbdergi.1714589
49. Kroeger EN, Carson TL, Baskin ML, et al. Reasons for Late-Night Eating and Willingness to Change:A Qualitative Study in Pregnant Black Women. J Nutr Educ Behav. 2019;51(5):598–607. doi:10.1016/j.jneb.2018.11.003
50. Ku CW, Loo RSX, Tiong MMY, et al. Nocturnal Lifestyle Behaviours and Risk of Poor Sleep during Pregnancy. Nutrients. 2022;14(11):2348. doi:10.3390/nu14112348
51. Barger MK, Caughey AB, Lee KA. Evaluating Insomnia During Pregnancy and Postpartum. In: Attarian HP, Viola-Saltzman M, editors. Sleep Disorders in Women: A Guide to Practical Management. Totowa, NJ: Humana Press; 2013:225–242.
52. Buman MP, Phillips BA, Youngstedt SD, et al. Does nighttime exercise really disturb sleep? Results from the 2013 National Sleep Foundation Sleep in America Poll. Sleep Med. 2014;15(7):755–761. doi:10.1016/j.sleep.2014.01.008
53. Stutz J, Eiholzer R, Spengler CM. Effects of Evening Exercise on Sleep in Healthy Participants: a Systematic Review and Meta-Analysis. Sports Med. 2019;49(2):269–287. doi:10.1007/s40279-018-1015-0
54. Mindell JA, Cook RA, Nikolovski J. Sleep patterns and sleep disturbances across pregnancy. Sleep Med. 2015;16(4):483–488. doi:10.1016/j.sleep.2014.12.006
55. O’Brien LM, Warland J. Typical sleep positions in pregnant women. Early Hum Dev. 2014;90(6):315–317. doi:10.1016/j.earlhumdev.2014.03.001
56. Shang X, Ye L, Wang MP, et al. A comprehensive insight on cognitive behavioral therapy for insomnia in pregnant women: a systematic review and meta-analysis. Sleep Med. 2023;112:322–332. doi:10.1016/j.sleep.2023.11.002
57. Sedov ID, Goodman SH, Tomfohr-Madsen LM. Insomnia Treatment Preferences During Pregnancy. J Obstet Gynecol Neonatal Nurs. 2017;46(3):e95–e104. doi:10.1016/j.jogn.2017.01.005
58. Felder JN, Epel ES, Neuhaus J, et al. Efficacy of Digital Cognitive Behavioral Therapy for the Treatment of Insomnia Symptoms Among Pregnant Women: a Randomized Clinical Trial. JAMA Psychiatry. 2020;77(5):484–492. doi:10.1001/jamapsychiatry.2019.4491
59. Kalmbach DA, Cheng P, O’Brien LM, et al. A randomized controlled trial of digital cognitive behavioral therapy for insomnia in pregnant women. Sleep Med. 2020;72:82–92. doi:10.1016/j.sleep.2020.03.016
60. Dolezal ML, Wielgosz J, Miller KE, et al. Investigating the Effectiveness of CBT-i Coach, a Free, Publicly Available mHealth App for Insomnia. J Technol Behav Sci. 2025;10(3):540–552. doi:10.1007/s41347-024-00459-x
61. Koffel E, Kuhn E, Petsoulis N, et al. A randomized controlled pilot study of CBT-I Coach: feasibility, acceptability, and potential impact of a mobile phone application for patients in cognitive behavioral therapy for insomnia. Health Informatics J. 2018;24(1):3–13. doi:10.1177/1460458216656472
62. Germain A, Buysse DJ. Chapter 15 - Brief Behavioral Treatment of Insomnia. In: Perlis M, Aloia M, Kuhn B, editors. Behavioral Treatments for Sleep Disorders. San Diego: Academic Press; 2011:143–150.
63. Bei B, Neemia D, Shen L, et al. 0396 A Brief, Automated Cognitive Behavioral Program Prevents Sleep Disturbance and Insomnia in Late Pregnancy: a Randomized Controlled Trial. Sleep. 2018;41(suppl_1):A151. doi:10.1093/sleep/zsy061.395
64. Lin YH, Chen MH, Chang YC, et al. Prevalence of exposure to benzodiazepines among pregnant women in Taiwan: a nationwide longitudinal study. J Sleep Res. 2022;31(6):e13678. doi:10.1111/jsr.13678
65. Estivill E, Bové A, García-Borreguero D, et al. Consensus on drug treatment, definition and diagnosis for insomnia. Clin Drug Investig. 2003;23(6):351–385. doi:10.2165/00044011-200323060-00001
66. Lee KA, Zaffke ME, Baratte-Beebe K. Restless legs syndrome and sleep disturbance during pregnancy: the role of folate and iron. J Womens Health Gend Based Med. 2001;10(4):335–341. doi:10.1089/152460901750269652
67. Okun ML, O’Brien LM. Concurrent insomnia and habitual snoring are associated with adverse pregnancy outcomes. Sleep Med. 2018;46:12–19. doi:10.1016/j.sleep.2018.03.004
68. Frawley J, Adams J, Sibbritt D, et al. Prevalence and determinants of complementary and alternative medicine use during pregnancy: results from a nationally representative sample of Australian pregnant women. Aust N Z J Obstet Gynaecol. 2013;53(4):347–352. doi:10.1111/ajo.12056
69. Foroughinia S, Hessami K, Asadi N, et al. Effect of Acupuncture on Pregnancy-Related Insomnia and Melatonin: a Single-Blinded, Randomized, Placebo-Controlled Trial. Nat Sci Sleep. 2020;12:271–278. doi:10.2147/nss.S247628
70. da Silva JB, Nakamura MU, Cordeiro JA, et al. Acupuncture for insomnia in pregnancy--a prospective, quasi-randomised, controlled study. Acupunct Med. 2005;23(2):47–51. doi:10.1136/aim.23.2.47
71. Levett KM, Sutcliffe KL, Betts D. Using Forbidden Points in Pregnancy: adverse Outcomes and Quality of Evidence in Randomized Controlled Trials-A Systematic Narrative Review. Med Acupunct. 2019;31(6):346–360. doi:10.1089/acu.2019.1391
72. Xiong Y, Liu C, Li M, et al. The use of Chinese herbal medicines throughout the pregnancy life course and their safety profiles: a population-based cohort study. Am J Obstet Gynecol MFM. 2023;5(5):100907. doi:10.1016/j.ajogmf.2023.100907
73. Gantner G, Spiess D, Randecker E, et al. Use of Herbal Medicines for the Treatment of Mild Mental Disorders and/or Symptoms During Pregnancy: a Cross-Sectional Survey. Front Pharmacol. 2021;12:729724. doi:10.3389/fphar.2021.729724
74. Illamola SM, Amaeze OU, Krepkova LV, et al. Use of Herbal Medicine by Pregnant Women: what Physicians Need to Know. Front Pharmacol. 2019;10:1483. doi:10.3389/fphar.2019.01483
75. Li X, Fang L, Guan L, et al. The effects of light therapy on depression and sleep in women during pregnancy or the postpartum period: a systematic review and meta-analysis. Brain Behav. 2023;13(12):e3339. doi:10.1002/brb3.3339
76. Zhao FY, Yue LP, Conduit R, et al. Development of a Stepped-Care Pathway for Managing Willis-Ekbom Disease/Restless Legs Syndrome During Pregnancy: a Best Evidence Synthesis. Nat Sci Sleep. 2026;18:591116. doi:10.2147/nss.S591116
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.