Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Transitioning from Once-Monthly to Once-Every-3-Months Paliperidone Palmitate Among Veterans with Schizophrenia
Authors El Khoury AC, Patel C, Mavros P, Huang A, Wang L, Bashyal R
Received 8 April 2021
Accepted for publication 21 September 2021
Published 19 October 2021 Volume 2021:17 Pages 3159—3170
DOI https://doi.org/10.2147/NDT.S313067
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Antoine C El Khoury,1 Charmi Patel,1 Panagiotis Mavros,1 Ahong Huang,2 Li Wang,2 Richa Bashyal2
1Janssen Scientific Affairs, LLC, Titusville, NJ, USA; 2STATinMED Research, Plano, TX, USA
Correspondence: Antoine C El Khoury
Janssen Scientific Affairs, LLC, 1125 Trenton-Harbourton Road, Titusville, NJ, 08560, USA
Tel +1 609-737-2699
Email [email protected]
Purpose: Compared to once-monthly paliperidone palmitate (PP1M), once-every-3-months paliperidone palmitate (PP3M) reportedly increases treatment adherence. The objective of this study was to compare treatment patterns, utilization, and costs among Veterans Health Administration (VHA) patients with schizophrenia who transitioned to PP3M versus those remaining on PP1M.
Patients and Methods: Adult VHA patients with ≥ 2 health care encounters (inpatient or outpatient) that included a schizophrenia diagnosis who initiated PP1M between January 1, 2015, and March 31, 2018 (identification period) were included in this exploratory retrospective cohort study. Propensity scores were used to match cases (PP1M users who transitioned to PP3M during the identification period) with controls (any patient initiating PP1M during the identification period). Data were assessed until death, health plan disenrollment, or study end. Outcomes were compared using chi-square and t-tests.
Results: A total of 257 eligible PP3M and 2973 eligible PP1M patients were identified among adult VHA patients; mean ages were 53.1 and 53.7 years, respectively. After propensity score matching, the PP3M and PP1M cohorts each held 111 patients. Comorbidities of patients treated with PP3M versus PP1M, respectively, included anxiety (12.5% vs 20%; standardized difference [STD] = 20.6), tobacco use (28.4% vs 43.2%; STD = 31.2), depressive disorder (26.5% vs 36.2%; STD = 21.1), and substance abuse (37.4% vs 44.2%; STD = 13.9). For the PP3M cohort, adherence (proportion of days covered ≥ 80%) to any antipsychotic agent was higher (78.4% vs 57.7%, P = 0.0009), and all-cause inpatient lengths of stay (LOS) were shorter (3.0 vs 8.3 days, P = 0.0354). Increased all-cause pharmacy costs with PP3M were offset by reduced all-cause medical costs, resulting in overall health care cost-neutrality.
Conclusion: Relative to those remaining on PP1M, VHA patients with schizophrenia who transitioned to PP3M experienced improved antipsychotic medication adherence and significantly shorter all-cause inpatient LOS; costs remained neutral.
Keywords: long-acting injectable antipsychotic, adherence, healthcare resource utilization, cost
Introduction
Schizophrenia is a chronic mental disorder affecting 1% of adults in the United States, characterized by a diminished capacity for learning, working, self-care, and interpersonal relationships.1–5 It is one of the top 20 leading causes of disability worldwide.6,7
A retrospective claims-based study using data from the Veterans Health Administration (VHA) system reported nearly 60,000 incident cases of schizophrenia during a 5-year period.8 The overall prevalence among veterans has been reported to be approximately 3%.9 Schizophrenia imposes a large economic burden and places a substantial burden on patients, caregivers, and the health care system.3,10–14 For example, in 2013, the estimated economic burden of schizophrenia in the United States was $155.7 billion.15
Antipsychotic (AP) agents such as oral AP therapies (OATs) and long-acting injectables (LAIs) serve as the treatment foundation for patients with schizophrenia.16,17 Patients with schizophrenia often have difficulty adhering to oral medication regimens despite the importance of long-term, continuous therapy.12,18–20 Nonadherence to regimens with medication such as OATs or oral atypical antipsychotics (OAAs) can lead to hospitalization and higher health care costs.19 For patients receiving atypical APs, relapse is particularly costly, incurring an incremental cost increase of $2459 per week.3 This additional cost is acquired through pharmacy, outpatient, and institutional visit costs, with institutional visits comprising over half of that additional weekly cost.3
Once-monthly paliperidone palmitate (PP1M) was approved by the US Food and Drug Administration (FDA) in 2009 for the treatment of adults with schizophrenia. Subsequent studies have shown that PP1M has improved adherence, lower inpatient and long-term health care resource utilization (HRU), and lower medical costs compared with oral therapies for patients with schizophrenia.18,21,22 In 2015, the FDA approved once-every-3-months paliperidone palmitate (PP3M) for the treatment of adults with schizophrenia. With reduced dosing frequency, PP3M treatment adherence was improved and caregiver burden was lessened.1,18,23,24 Additionally, a shift to PP3M showed a decrease in medical costs, mostly due to decreasing monthly inpatient costs.2
The current study evaluates the administration of PP3M after treatment with PP1M.25 Current literature comparing real-world outcomes between patients with schizophrenia taking PP3M and PP1M compares data before and after transition from PP1M to PP3M.1,2,19,26,27 This study design lacks risk factors that contributed to the use of PP1M before the start of PP3M. The current study design incorporates an analysis of balanced cohorts treated with either PP1M or PP3M. The PP3M cohort comprised patients who transitioned from PP1M to PP3M treatment during the study period, and the PP1M cohort comprised patients who initiated PP1M treatment during the study. The main objective of the study was to assess the potential benefits of either continuing treatment with PP1M or transitioning to PP3M by comparing treatment patterns (AP and mental health (MH)-related medication use and adherence), HRU, and costs among patients with schizophrenia who transitioned to PP3M versus patients who remained on PP1M treatment within the VHA.
Patients and Methods
Data Source
This retrospective cohort study utilized data from the VHA database from January 1, 2014, to March 31, 2018 (the study period).
According to the 2017 US Census, there are ~18.2 million veterans in the United States.28 The VHA is the largest integrated health care system in the United States and provides care to over 9 million veterans.29,30 The VHA Database consists of the Medical SAS Datasets, Decision Support System (DSS) data, and the Vital Status File. The Medical SAS Datasets are provided by fiscal year and include 4 inpatient datasets and 2 outpatient datasets. Demographic variables are found in both inpatient and outpatient datasets. Examples of variables in the inpatient datasets include date, date of diagnosis, discharge date, diagnoses, procedures, diagnostic and procedure codes, and death. Examples of variables in the outpatient datasets include information regarding outpatient service dates, clinic information, diagnoses, procedures, and diagnostic and procedure codes. The DSS data contain variables related to days of prescription supply and utilization and costs for pharmacy prescriptions, laboratory tests, radiologic procedures, and inpatient and outpatient services. The Vital Status File contains medical yearly enrollment indicators, veteran status, and birth and death information for each record.
Institutional Review Board (IRB) Exemption
Except in compliance with applicable law, no identifiable patient information or medical records were disclosed for the purposes of this study. Therefore, IRB approval to conduct this study was not required because the core study did not involve the collection, use, or transmittal of individual identifiable data.
Study Population
This study population was composed of 2 cohorts: PP1M and PP3M. VHA patients were included in the PP3M study group if they had transitioned from PP1M to PP3M treatment during the identification period (January 1, 2015, to March 31, 2018) and had no PP3M claims prior to the discontinuation of PP1M. The first dispensing date of PP3M was defined as the index date (ID) for the PP3M cohort.
The PP1M cohort was drawn from all those who initiated PP1M treatment during the identification period (January 1, 2015, to March 31, 2018), including those who might have switched to PP3M at a later time. The first dispensing of PP1M was defined as the PP1M date. The PP1M cohort was identified by assigning a random index date (RID) to all PP1M initiators during the period from PP1M initiation through discontinuation (≥45-day gap between injections), drug supply end date, disenrollment, or study period end date, whichever occurred first. The RID was assigned to ensure that cohort membership was based on current rather than future exposure to PP3M. This approach enabled selection of all those who had initiated PP1M and were at risk of transitioning to PP3M but had not done so by the RID. Patients from among all those initiating PP1M were matched to those in the PP3M cohort using propensity score matching. Propensity score matching was used to achieve balance in the baseline characteristics between the 2 cohorts because, due to the non-experimental nature of the study, patients in different study cohorts were likely to differ from one another. For those in the PP1M cohort who later initiated PP3M, the end of follow-up occurs when they discontinued PP1M.
Included patients in the PP1M and PP3M cohorts were also required to have had continuous health plan enrollment for 12 months before the ID (baseline period) and after the ID (follow-up period); ≥2 health care encounters (inpatient or outpatient) that included a schizophrenia diagnosis (International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9-CM] code 295.XX [excluding 295.7, schizoaffective disorder] or International Classification of Diseases, 10th Revision, Clinical Modification [ICD-10-CM] codes F20.XX or F21) during the study period; and age ≥18 years at ID. Patients were not excluded for having a diagnosis of schizoaffective disorder or bipolar disorder during the baseline period so long as they also had ≥2 health care encounters that included a schizophrenia diagnosis during the study period. Patients were excluded from the study if they had evidence of PP3M use during the baseline period. All patient data were assessed until death, health plan disenrollment, or the end of the study period.
Demographic and Baseline Clinical Characteristics
Patient demographics including age, sex, and race were assessed. Clinical characteristics such as the Quan-Charlson Comorbidity Index (CCI) score and other individual comorbidities were examined using ICD-9-CM codes (Appendix 1). Based on General Equivalence Mappings by the Centers for Medicare and Medicaid Services, all ICD-9 diagnostic and procedure codes were mapped to ICD-10 codes.31
Outcome Measures
Treatment patterns, HRU, and costs during baseline and follow-up were measured for the PP1M and PP3M cohorts. Outcome measures included the proportion of patients prescribed APs (including any oral, long-acting, and short-acting injectables (Appendices 2 and 3)) and other MH-related medication such as antidepressants, anxiolytics, and mood stabilizers (Appendix 4).
Adherence to medication was calculated using the proportion of days covered (PDC), defined as the number of days in the follow-up period covered by a medication divided by the follow-up time.32 The medication possession ratio (MPR) was defined as the number of days of supply within the entire exposure to therapy (defined as the number of days between the date of the first drug fill and the last drug refill plus the number of days of supply of the last refill). MPR was computed as the sum of days of supply divided by the exposure to therapy. PDC and MPR ≥80% was reported as adherent and <80% was reported as nonadherent.
HRU and costs were compared for all-cause, MH-related, and schizophrenia-related outcomes. Medical claims were considered MH-related if there was a schizophrenia diagnosis (as defined previously) or a MH disorder (Appendix 5) on any position of the claim. MH-related pharmacy costs included costs for any AP (Appendices 2 and 3) and/or other MH-related medications (Appendix 4). Medical costs were considered schizophrenia-related if there was a schizophrenia diagnosis on any position of the claim; schizophrenia-related pharmacy costs included costs for any AP (Appendices 2 and 3). Using the medical care component of the Consumer Price Index, all costs were adjusted to 2017 US dollars.
Statistical Analysis
Demographics and baseline clinical characteristics were assessed descriptively among patients in the PP1M and PP3M cohorts. To compare the follow-up outcomes between the PP1M and PP3M cohorts, t-test and chi-square tests were used for continuous and categorical variables, respectively. The level of significance was set at α = 0.05. Standardized differences (STD) were also calculated.
To create the comparison PP1M and PP3M cohorts, patients were matched on propensity score and duration of time from PP1M initiation date to either the ID (PP3M cohort) or RID (PP1M cohort) with an allowable difference of ±30 days. A multivariable logistic regression model controlling for all baseline demographics and clinical characteristics was used to predict the propensity of transitioning to PP3M. The model incorporated potential predictors of treatment as independent variables in the regression and group status as the outcome. It included the following covariates: age, sex, race, Quan-CCI score, other baseline individual comorbidities (MH-related and non–MH-related), and baseline all-cause total costs. Patients initiating PP1M were matched 1:1 to those transitioning to PP3M, based on the propensity score (nearest-neighbor matching without replacement, caliper distance = 0.01) and the time on PP1M (±30 days) prior to cohort entry.
Adequately treated patients were defined as patients who had ≥4 months of continuous PP1M use with no treatment gap of ≥45 days prior to the ID.
All analyses were conducted using SAS statistical software (version 9.3, SAS Institute, Cary, NC, 2012).
Results
A total of 257 PP3M and 2973 PP1M patients were included in the study after applying the inclusion and exclusion criteria; a total of 111 matched patients were included in the PP3M and PP1M cohorts after matching on propensity score and time on PP1M prior to ID (Figure 1).
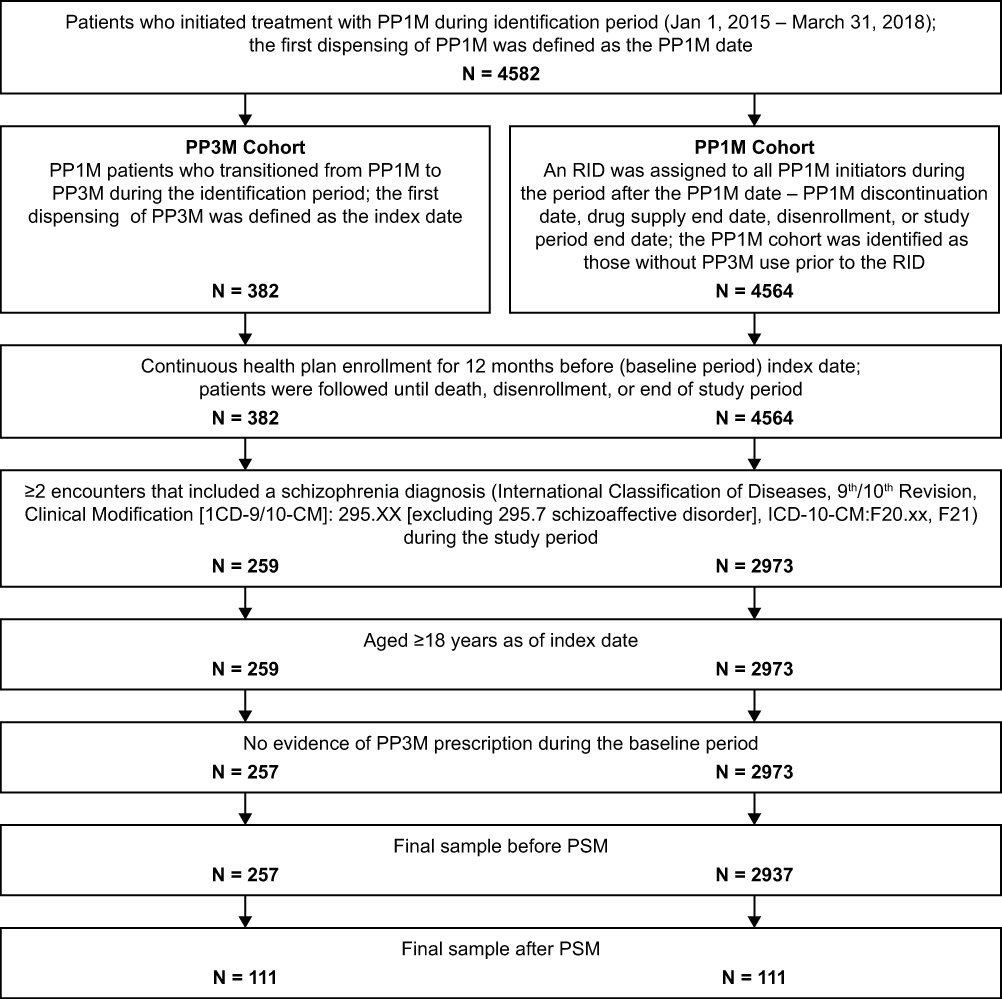 |
Figure 1 VHA patient selection criteria. Abbreviations: PP1M, once-monthly paliperidone palmitate; PP3M, once-every-3-months paliperidone palmitate; PSM, propensity score matching; RID, random index date. |
Demographic and Baseline Characteristics
The mean ages of the 257 PP3M and 2973 PP1M patients were 53.1 years (standard deviation [SD] = 13.5) and 53.7 years (SD = 13.4) (STD = 4.4), respectively. Most patients were male and White. Patients in the PP3M cohort had a lower mean Quan-CCI score compared with PP1M patients. Among patients who transitioned to PP3M, there were significantly lower rates of anxiety, tobacco use, depression, substance abuse, and other MH-related comorbidities. The most common non–MH-related comorbidities included cardiovascular disease (CVD)–hyperlipidemia, CVD–hypertension, and diabetes mellitus (Table 1).
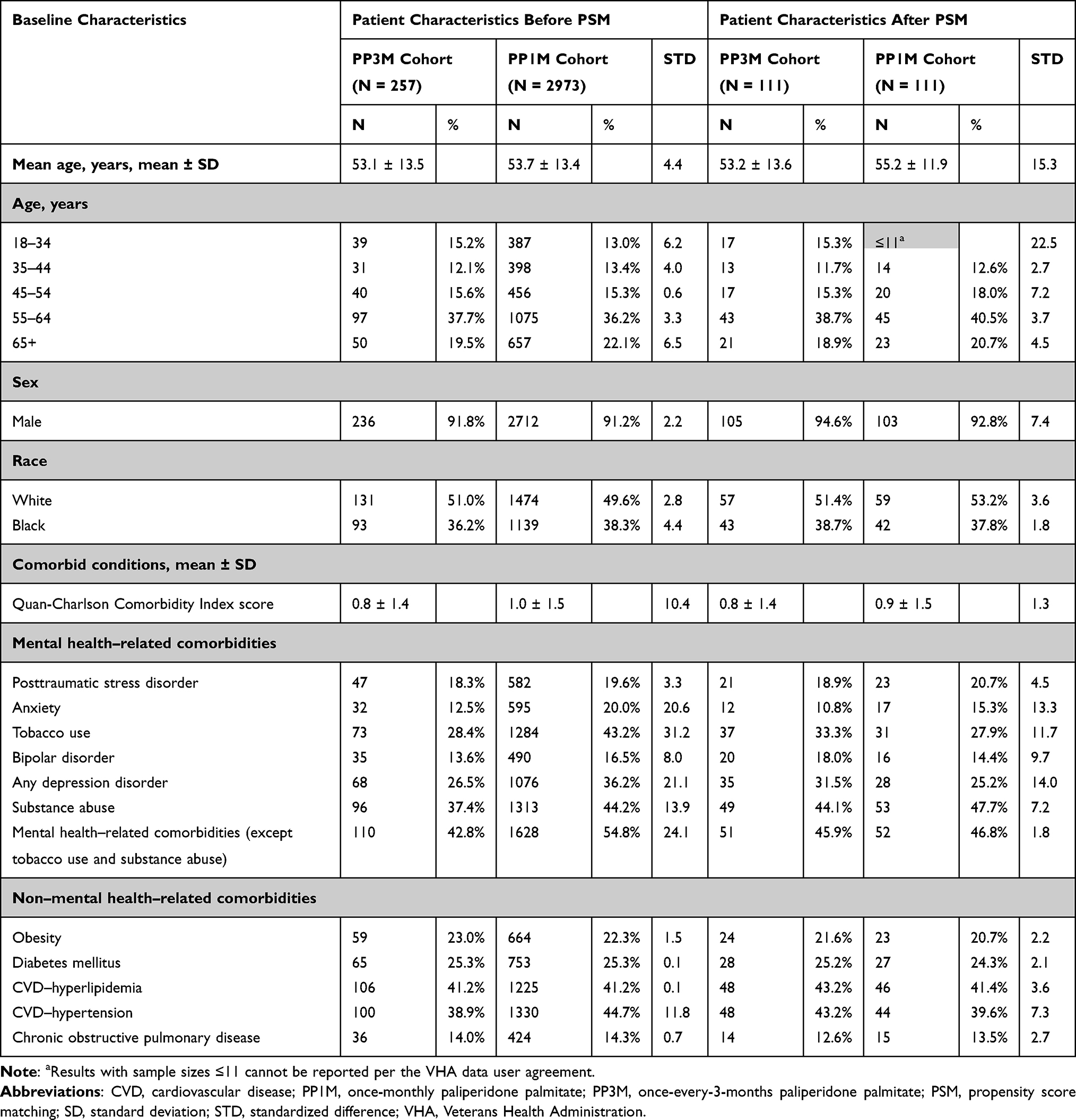 |
Table 1 Baseline Demographic and Clinical Characteristics Before PSM for VHA Patients with Schizophrenia Who Transitioned to PP3M versus Those Who Remained on PP1M |
After matching, imbalances between the PP3M and PP1M cohorts were observed in age, anxiety, tobacco use, and depression disorder. In particular, patients in the PP3M cohort were younger that those in the PP1M cohort (mean [SD] 53.2 [13.6] vs 55.2 [11.9], STD = 15.3), and a lower proportion of PP3M patients had anxiety (10.8% vs 15.3%, STD = 13.3), tobacco use (33.3% vs 27.9%, STD = 11.7), or any depression disorder (31.5% vs 25.2%, STD = 14.0) relative to PP1M patients.
Follow-Up Treatment Patterns
The mean time that patients received PP1M treatment prior to PP3M was 298.40 days. Patients in the PP1M cohort had been treated with PP1M for a mean of 299.57 days prior to the (randomly assigned) ID. Mean follow-up periods for the PP3M and PP1M groups were 496.48 days and 571.96 days, respectively. Compared to patients in the PP1M cohort, a significantly higher proportion of patients who transitioned to PP3M were adherent to their antipsychotic regimen (%PDC ≥80%: 78.4% vs 57.7%, P = 0.0009; %MPR ≥80%: 88.3% vs 72.1%, P = 0.0024). Patients who transitioned to PP3M had a significantly higher PDC (mean [SD] PDC: 0.9 [0.2] vs 0.7 [0.3], P < 0.0001) and MPR (mean [SD] MPR: 0.9 [0.2] vs 0.8 [0.3], P = 0.0016) compared with patients who remained on PP1M (Table 2).
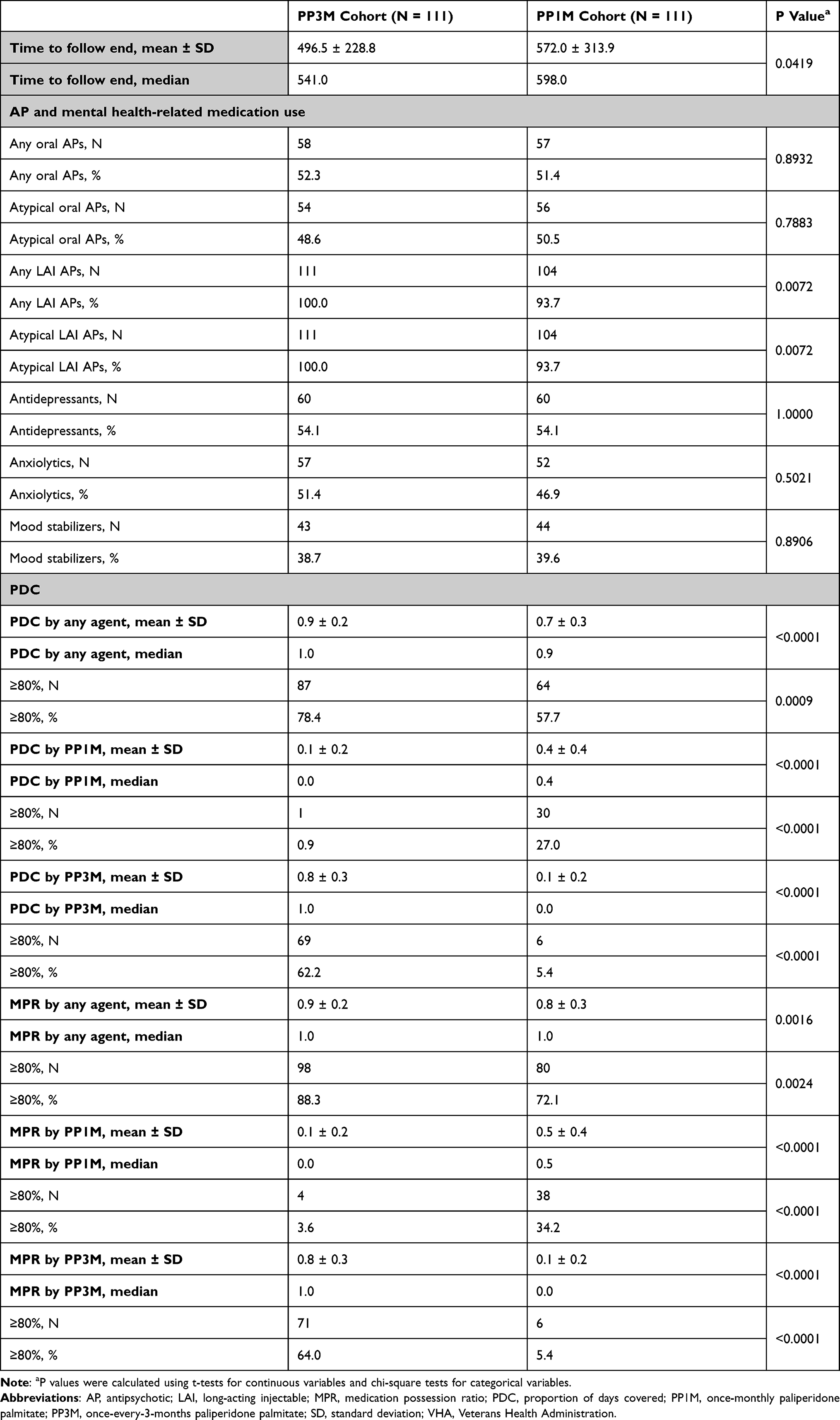 |
Table 2 PSM-Adjusted Comparison of Treatment Patterns Among VHA Patients with Schizophrenia Who Remained on PP1M versus Those Who Transitioned to PP3M |
HRU
During the follow-up period, patients with schizophrenia who transitioned to PP3M experienced a significantly shorter all-cause inpatient length of stay (LOS) per patient per year (PPPY) compared with patients who remained on PP1M (3.0 vs 8.3 days, P = 0.0354). There were no statistically significant differences in the number of all-cause inpatient stays (0.3 vs 0.7, P = 0.1471), outpatient visits (47.6 vs 48.6, P = 0.8335), or prescription fills PPPY (27.7 vs 30.6, P = 0.2893) (Figure 2). Results for MH- and schizophrenia-related HRU were directionally consistent with all-cause results. Sensitivity analysis among adequately treated patients yielded fewer all-cause inpatient stays (0.4 vs 1.0, P = 0.0818) and outpatient visits PPPY (45.1 vs 48.3, P = 0.5981). Similar trends for MH- and schizophrenia-related inpatient and outpatient stays PPPY were also observed. Significantly shorter all-cause (2.5 vs 14.1 days, P = 0.0176), MH-related (2.5 vs 13.7, P = 0.0214), and schizophrenia-related inpatient LOS PPPY (1.4 vs 11.3, P = 0.0362) was observed for patients who transitioned to PP3M.
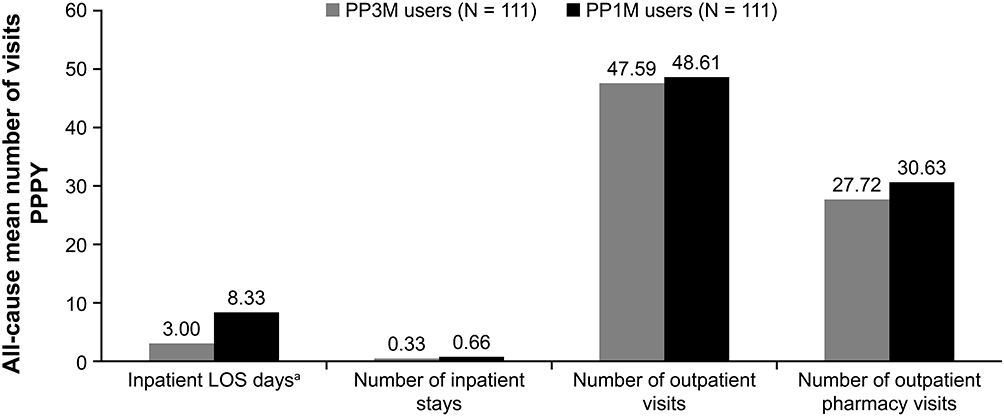 |
Figure 2 Comparison of all-cause HRU PPPY among VHA patients with schizophrenia who transitioned to PP3M versus those who remained on PP1M. Abbreviations: HRU, health care resource utilization; LOS, length of stay; PP1M, once-monthly paliperidone palmitate; PP3M, once-every-3-months paliperidone palmitate; PPPY, per patient per year; VHA, Veterans Health Administration. Note: aP < 0.05. P values were calculated using t-tests with the level of significance set at α = 0.05. |
Cost Comparison
Patients in the PP3M cohort incurred significantly higher all-cause pharmacy costs PPPY ($15,987 vs $11,381, P = 0.0004) compared with patients in the PP1M cohort. Although not statistically significant, there was a trend towards lower all-cause inpatient ($5518 vs $13,361, P = 0.0617) and total medical costs ($29,210 vs $38,297, P = 0.1010) among patients in the PP3M cohort relative to those in the PP1M cohort. There were no statistically significant differences in total costs PPPY ($45,198 vs $49,678, P = 0.4433) between the two patient cohorts (Figure 3). Similar cost trends were observed for MH- and schizophrenia-related costs. Sensitivity analysis among adequately treated patients showed that PP3M patients had significantly lower all-cause total medical ($25,645 vs $49,312, P = 0.0115) and total costs PPPY ($41,134 vs $61,127, P = 0.0378), MH-related total medical ($21,358 vs $44,748, P = 0.0115) and MH-related total costs PPPY ($36,370 vs $56,300, P = 0.0362), and schizophrenia-related total medical costs PPPY ($13,051 vs $30,324, P = 0.0287).
 |
Figure 3 Comparison of all-cause costs PPPY among VHA patients with schizophrenia who transitioned to PP3M versus those who remained on PP1M. Abbreviations: PP1M, once-monthly paliperidone palmitate; PP3M, once-every-3-months paliperidone palmitate; PPPY, per patient per year; VHA, Veterans Health Administration. Note: aP < 0.05. P values were calculated using t-tests with the level of significance set at α = 0.05. |
Discussion
Unlike previous publications, the current study compared PP1M patients who transitioned to PP3M with patients who, after accounting for person-time at risk, had not transitioned to PP3M. The time “at risk” was the person-time on PP1M treatment before the start of PP3M therapy. By accounting for this at-risk time, the comparator PP1M study cohort was selected from among all patients who initiated PP1M and were at risk of transitioning to PP3M. Therefore, the current study considered the dynamic and complex nature of medication therapy as opposed to treating medication as a time-fixed construct.33
The current study’s design includes an additional sensitivity analysis addressing adequately treated or stable patients within the main sample.27 Through propensity score matching, balanced cohorts receiving PP1M and PP3M treatment regimens enabled a comparison of the outcomes among PP1M patients who transitioned to PP3M versus those who continued to receive PP1M.
The study revealed that adherence, as measured by PDC and MPR, was significantly higher for patients who transitioned to PP3M compared with patients who remained on PP1M. These findings align with previous studies, which reported improved adherence upon transitioning patients to PP3M from PP1M.1,2,19,28,29 For example, in a retrospective longitudinal cohort study, Joshi et al17 reported a high proportion of patients who transitioned to PP3M as persistent and adherent to treatment (with >80% being adherent [PDC ≥80%]) and most patients having decreased HRU, possibly due to a lower dosing frequency. DerSarkissian et al1 reported that VHA patients with schizophrenia experienced an increase in PDC after transitioning to PP3M from PP1M as well as a decrease in HRU using a pre- and post-PP3M transition study design. Adherence plays a critical role in schizophrenia treatment because nonadherence to medication can lead to increased hospitalization, longer inpatient stays, and ultimately increased health care costs for patients.11,34–36 The opportunity for patients to receive treatment once every 3 months as opposed to once-monthly doses can contribute to improved adherence to PP3M, which can greatly affect patients’ recovery, quality of life, and HRU.
All-cause and MH-related inpatient LOS was significantly shorter for patients who transitioned to PP3M as opposed to those remaining on PP1M. DerSarkissian et al1 similarly reported a significantly shorter average LOS for any inpatient setting and MH care setting post-PP3M transition. Compared with the foundation treatment of OAAs, improved adherence to PP1M and PP3M has been reported; the even greater adherence to PP3M may further contribute to reduction in relapses and hospitalization and subsequently shorter inpatient LOS.26,36–39
Significantly higher all-cause pharmacy costs were observed for patients who transitioned to PP3M. The increased pharmacy costs among patients who transitioned to PP3M were offset by comparable inpatient and outpatient costs, resulting in cost neutrality for total costs. Comparable results for inpatient, outpatient, total medical, and total costs were confirmed by prior literature.1,2,29 Similarly, DerSarkissian et al1 observed significantly higher costs related to pharmacy costs but significantly lower health care costs related to inpatient, outpatient, and total costs. Whereas the current study has a patient population similar in age, sex distribution, and data source (VHA), the cost differences between patients who remained on PP1M and patients who transitioned to PP3M were not significantly different. These discrepancies could be explained by the differences in study design as well as the study period.
Whereas claims data can provide valuable real-world information to assess treatment patterns, HRU, costs, and health care outcomes, claims data come with limitations that may influence outcomes. These include coding errors, billing inaccuracies, and missing data; diagnoses entered as administrative processing as opposed to being linked to clinical outcomes; and certain information, such as clinical parameters, not being readily available in claims data. Further, the evaluation of adherence was based on the presence of a claim for a filled prescription, which does not indicate whether the medication was taken as prescribed.
A limitation of the current study’s matching algorithm may be incomplete matching that could affect the representativeness of the cohorts and the generalizability of the results. Because the study sample consisted of patients with schizophrenia enrolled in the VHA health care system, the findings may not be generalizable to the overall US population. Furthermore, due to the nature of claims data and the outcomes of this study, it is possible that not all utilizations for which mental health was coded were primarily used to discuss or treat mental health issues. Additionally, adherence before switching medications was measured through pharmacy claims and was only evaluated within 4 months before switching. Because patients were required to start on PP1M prior to transition to PP3M, initial treatment with PP1M may have contributed to the cost and healthcare resource utilization benefits observed with PP3M treatment. The study sample also consisted of a higher proportion of men aged ≥55 years, and this population of patients may have different comorbidities compared with the general population. Finally, a longer follow-up period may have produced more robust data and should be considered for future studies.
Conclusions
Compared with VHA patients who remained on PP1M treatment, patients who transitioned to PP3M experienced significantly shorter all-cause inpatient LOS and a lower average number of schizophrenia-related prescription fills PPPY. Although not statistically significant, results indicate that patients who transitioned to PP3M after PP1M experienced an overall reduction in all-cause medical costs. The reduction in all-cause medical costs offset the increased all-cause pharmacy costs for patients who transitioned to PP3M, resulting in overall health care cost-neutrality. In addition, patients who transitioned to PP3M experienced increased adherence in relation to schizophrenia treatment.
The findings from the current study demonstrate the potential improvement of clinical and economic outcomes associated with transition to PP3M from PP1M in comparison to remaining on PP1M treatment. The current study further validates the results of previous studies concerning real-world outcomes related to the transition from PP1M to PP3M for patients with schizophrenia.
Abbreviations
AP, antipsychotic; CCI, Quan-Charlson Comorbidity Index; CVD, cardiovascular disease; DSS, decision support system; FDA, US Food and Drug Administration; HRU, healthcare resource utilization; ICD-9, International Classification of Diseases, 9th Revision, Clinical Modification; ICD-10, International Classification of Diseases, 10th Revision, Clinical Modification; IRB, institutional review board; LAI, long-acting injectable; LOS, length of stay; MH, mental health; MPR, medication possession ratio; OAA, oral atypical antipsychotic; OAT, oral antipsychotic therapy; PDC, proportion of days covered; PP1M, once-monthly paliperidone palmitate; PP3M, once-every-3-months paliperidone palmitate; PPPY, per patient per year; RID, random index date; SD, standard deviation; STD, standardized difference; VHA, Veteran’s Health Administration.
Data Sharing Statement
The data sharing policy of Janssen Pharmaceutical Companies of Johnson & Johnson is available at https://www.janssen.com/clinical-trials/transparency. As noted on this site, requests for access to the study data can be submitted through Yale Open Data Access (YODA) Project site at https://yoda.yale.edu.
Acknowledgments
Analysis support, funded by Janssen Scientific Affairs, LLC, was provided by Jieni Li, PhD, of STATinMED Research. Editorial and medical writing support, funded by Janssen Scientific Affairs, LLC, was provided by Catherine Callan, MPH, and Emily Achter, MPH, of STATinMED Research and by Madeline Pfau, PhD, of ApotheCom (New York, NY).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Janssen Scientific Affairs, LLC. The study sponsor was involved in the design and conduct of the study; collection, management, analysis, and interpretation of data; preparation, review, and approval of the manuscript; and the decision to submit the manuscript for publication. All authors contributed to the development of the manuscript and approved the final version.
Disclosure
Dr. El Khoury, Mrs. Patel, and Dr. Mavros are employees of Janssen Scientific Affairs, LLC, and hold stock in Johnson & Johnson, Inc. Dr. Wang and Mr. Bashyal are employees of STATinMED Research, which received consulting fees from Janssen Scientific Affairs, LLC. At the time of the study, Ms. Huang was an employee of STATinMED Research, which received consulting fees from Janssen Scientific Affairs, LLC. The authors report no other conflicts of interest in this work.
References
1. DerSarkissian M, Lefebvre P, Joshi K, et al. Health care resource utilization and costs associated with transitioning to 3-month paliperidone palmitate among US veterans. Clin Ther. 2018;40(9):1496–1508. doi:10.1016/j.clinthera.2018.07.011
2. Emond B, Joshi K, El Khoury AC, et al. Adherence, healthcare resource utilization, and costs in Medicaid beneficiaries with schizophrenia transitioning from once-monthly to once-every-3-months paliperidone palmitate. Pharmacoecon Open. 2019;3(2):177–188. doi:10.1007/s41669-018-0089-9
3. Lafeuille MH, Gravel J, Lefebvre P, et al. Patterns of relapse and associated cost burden in schizophrenia patients receiving atypical antipsychotics. J Med Econ. 2013;16(11):1290–1299. doi:10.3111/13696998.2013.841705
4. American Psychiatric Association. What is schizophrenia?; July, 2017. Available from: https://www.psychiatry.org/patients-families/schizophrenia/what-is-schizophrenia.
5. National Institute of Mental Health. Schizophrenia; May, 2018. Available from: https://www.nimh.nih.gov/health/statistics/schizophrenia.shtml.
6. Lafeuille MH, Grittner AM, Fortier J, et al. Comparison of rehospitalization rates and associated costs among patients with schizophrenia receiving paliperidone palmitate or oral antipsychotics. Am J Health Syst Pharm. 2015;72(5):378–389. doi:10.2146/ajhp140219
7. Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382(9904):1575–1586. doi:10.1016/S0140-6736(13)61611-6
8. Xie L, Baser O Clinical and economic burden of U.S. veteran schizophrenia patients: a real-world evaluation.
9. Chwastiak LA, Rosenheck RA, Kazis LE. Association of psychiatric illness and obesity, physical inactivity and smoking among a national sample of veterans. Psychosomatics. 2011;52(3):230–236. doi:10.1016/j.psym.2010.12.009
10. Furiak NM, Ascher-Svanum H, Klein RW, et al. Cost-effectiveness of olanzapine long-acting injection in the treatment of patients with schizophrenia in the United States: a micro-simulation economic decision model. Curr Med Res Opin. 2011;27(4):713–730. doi:10.1185/03007995.2011.554533
11. Baser O, Xie L, Pesa J, et al. Healthcare utilization and costs of Veterans Health Administration patients with schizophrenia treated with paliperidone palmitate long-acting injection or oral atypical antipsychotics. J Med Econ. 2015;18(5):357–365. doi:10.3111/13696998.2014.1001514
12. Lafeuille MH, Tandon N, Tiggelaar S, et al. Economic impact in Medicaid beneficiaries with schizophrenia and cardiometabolic comorbidities treated with once-monthly paliperidone palmitate vs. oral atypical antipsychotics. Drugs Real World Outcomes. 2018;5(1):81–90. doi:10.1007/s40801-018-0130-4
13. Olivares JM, Sermon J, Hemels M, et al. Definitions and drivers of relapse in patients with schizophrenia: a systematic literature review. Ann Gen Psychiatry. 2013;12(1):32. doi:10.1186/1744-859X-12-32
14. Chong HY, Teoh SL, Wu DB, et al. Global economic burden of schizophrenia: a systematic review. Neuropsychiatr Dis Treat. 2016;12:357–373.
15. Cloutier M, Aigbogun MS, Guerin A, et al. The economic burden of schizophrenia in the United States in 2013. J Clin Psychiatry. 2016;77(6):764–771. doi:10.4088/JCP.15m10278
16. Pesa JA, Doshi D, Wang L, et al. Health care resource utilization and costs of California Medicaid patients with schizophrenia treated with paliperidone palmitate once monthly or atypical oral antipsychotic treatment. Curr Med Res Opin. 2017;33(4):723–731. doi:10.1080/03007995.2016.1278202
17. Joshi K, Lafeuille MH, Brown B, et al. Baseline characteristics and treatment patterns of patients with schizophrenia initiated on once-every-three-months paliperidone palmitate in a real-world setting. Curr Med Res Opin. 2017;33(10):1763–1772. doi:10.1080/03007995.2017.1359516
18. Furiak NM, Ascher-Svanum H, Klein RW, et al. Cost-effectiveness model comparing olanzapine and other oral atypical antipsychotics in the treatment of schizophrenia in the United States. Cost Eff Resour Alloc. 2009;7(1):4. doi:10.1186/1478-7547-7-4
19. Thieda P, Beard S, Richter A, Kane J. An economic review of compliance with medication therapy in the treatment of schizophrenia. Psychiatr Serv. 2003;54(4):508–516. doi:10.1176/appi.ps.54.4.508
20. Masand PS, Roca M, Turner MS, et al. Partial adherence to antipsychotic medication impacts the course of illness in patients with schizophrenia: a review. Prim Care Companion J Clin Psychiatry. 2009;11(4):147–154. doi:10.4088/PCC.08r00612
21. Joshi K, Lafeuille MH, Kamstra R, et al. Real-world adherence and economic outcomes associated with paliperidone palmitate versus oral atypical antipsychotics in schizophrenia patients with substance-related disorders using Medicaid benefits. J Comp Eff Res. 2018;7(2):121–133. doi:10.2217/cer-2017-0043
22. El Khoury A, Patel C, Huang A, et al. Transitioning from oral risperidone or paliperidone to once-monthly paliperidone palmitate: a real-world analysis among Veterans’ Health Administration patients with schizophrenia who have had at least one prior hospitalization. Curr Med Res Opin. 2019;35(12):2159–2168. doi:10.1080/03007995.2019.1651129
23. Einarson TR, Bereza BG, Garcia Llinares I, et al. Cost-effectiveness of 3-month paliperidone treatment for chronic schizophrenia in Spain. J Med Econ. 2017;20(10):1039–1047. doi:10.1080/13696998.2017.1351370
24. Brasso C, Bellino S, Bozzatello P, et al. Role of 3-monthly long-acting injectable paliperidone in the maintenance of schizophrenia. Neuropsychiatr Dis Treat. 2017;13:2767–2779. doi:10.2147/NDT.S150568
25. Daghistani N, Rey JA. Invega Trinza: the first four-times-a-year, long-acting injectable antipsychotic agent. P T. 2016;41(4):222–227.
26. Patel C, El Khoury A, Huang A, et al. Health outcomes among patients diagnosed with schizophrenia in the US Veterans Health Administration population who transitioned from once-monthly to once-every-3-month paliperidone palmitate: an observational retrospective analysis. Adv Ther. 2019;36(10):2941–2953. doi:10.1007/s12325-019-01039-9
27. Emond B, El Khoury AC, Patel C, et al. Real-world outcomes post-transition to once-every-3-months paliperidone palmitate in patients with schizophrenia within US commercial plans. Curr Med Res Opin. 2019;35(3):407–416. doi:10.1080/03007995.2018.1560220
28. US Census Bureau. 2018 American Community Survey Single-Year Estimates; September, 2019. Available from: https://www.census.gov/newsroom/press-kits/2019/acs-1year.html.
29. National Center for Veterans Analysis and Statistics. VA Utilization Profile FY 2016; March, 2020. Available from: https://va.gov/vetdata/docs/QuickFacts/VA_Utilization_Profile.PDF.
30. US Department of Veterans Affairs, Veterans Health Administration. About VHA; July, 2019. Available from: https://www.va.gov/health/aboutvha.asp.
31. Centers for Medicare & Medicaid Services. General Equivalence Mappings: ICD-9-CM to and from ICD-10-CM and ICD-10-PCS; March, 2009. Available from: https://www.cms.gov/Medicare/Coding/ICD10/downloads/ICD-10_GEM_fact_sheet.pdf.
32. Campagna EJ, Muser E, Parks J, et al. Methodological considerations in estimating adherence and persistence for a long-acting injectable medication. J Manag Care Pharm. 2014;20(7):756–766. doi:10.18553/jmcp.2014.20.7.756
33. Lund JL, Horvath-Puho E, Szepligeti SK, et al. Conditioning on future exposure to define study cohorts can induce bias: the case of low-dose acetylsalicylic acid and risk of major bleeding. Clin Epidemiol. 2017;9:611–626. doi:10.2147/CLEP.S147175
34. Zhang W, Amos TB, Gutkin SW, et al. A systematic literature review of the clinical and health economic burden of schizophrenia in privately insured patients in the United States. Clinicoecon Outcomes Res. 2018;10:309–320. doi:10.2147/CEOR.S156308
35. Higashi K, Medic G, Littlewood KJ, et al. Medication adherence in schizophrenia: factors influencing adherence and consequences of nonadherence, a systematic literature review. Ther Adv Psychopharmacol. 2013;3(4):200–218. doi:10.1177/2045125312474019
36. Ascher-Svanum H, Faries DE, Zhu B, et al. Medication adherence and long-term functional outcomes in the treatment of schizophrenia in usual care. J Clin Psychiatry. 2006;67(3):453–460. doi:10.4088/JCP.v67n0317
37. Savitz AJ, Xu H, Gopal S, et al. Efficacy and safety of paliperidone palmitate 3-month formulation for patients with schizophrenia: a randomized, multicenter, double-blind, noninferiority study. Int J Neuropsychopharmacol. 2016;19(7):pyw018. doi:10.1093/ijnp/pyw018
38. MacEwan JP, Forma FM, Shafrin J, et al. Patterns of adherence to oral atypical antipsychotics among patients diagnosed with schizophrenia. J Manag Care Spec Pharm. 2016;22(11):1349–1361.
39. Weiden PJ, Kim E, Bermak J, et al. Does half-life matter after antipsychotic discontinuation? A relapse comparison in schizophrenia with 3 different formulations of paliperidone. J Clin Psychiatry. 2017;78(7):e813–e820. doi:10.4088/JCP.16m11308
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.