Back to Journals » Journal of Pain Research » Volume 16
Transforaminal Epidural Steroid Injection for Patients with Lumbosacral Disc Herniation in the Absence of Spine Magnetic Resonance Imaging – Is Better Really the Enemy of the Best?
Authors Lee JH, Lee JH ![]() , Chang MC
, Chang MC ![]()
Received 6 January 2023
Accepted for publication 2 May 2023
Published 4 May 2023 Volume 2023:16 Pages 1477—1485
DOI https://doi.org/10.2147/JPR.S402405
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Dawood Sayed
Jung Hwan Lee,1 Jun Ho Lee,2 Min Cheol Chang3
1Namdarun Rehabilitation Clinic, Yongin-City, Gyeonggi-Do, South Korea; 2Department of Neurosurgery, Kyung Hee University Medical Center, Seoul, 02447, South Korea; 3Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Daegu, 705-717, Republic of Korea
Correspondence: Min Cheol Chang, Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, 317-1, Daemyungdong, Namku, Daegu, 705-717, Republic of Korea, Tel +82-53-620-4862, Email [email protected]
Purpose: This study aimed to evaluate the effect of transforaminal epidural steroid injection (TFESI) in patients with lumbosacral disc herniation by comparing its effect between those diagnosed by clinical evaluation and plain radiography only (X-ray group) and those by additional magnetic resonance imaging (MRI) (MRI group). Additionally, we investigated the accuracy of the preliminary clinical assumption in the X-ray group using confirmative post-injection MRI.
Patients and Methods: We retrospectively recruited 367 patients with back and radicular pain due to lumbosacral disc herniation from a single pain clinic. Among them, 201 and 166 patients were categorized into the X-ray and MRI groups, respectively. In the X-ray group, the pathological level assumed initially by clinical evaluation and plain radiography concurred with that confirmed later on post-injection MRI in 139 patients (corresponding group); the remaining 62 patients lacked this concurrence (non-corresponding group). The NRS scores and Macnab criteria results were compared between the X-ray and MRI groups as well as the corresponding and non-corresponding groups.
Results: Both the X-ray and MRI groups showed significant reductions in the NRS scores at 2 and 10 weeks post-injection when compared with the pretreatment scores. However, no significant difference was noted between the groups in terms of the magnitude of clinical improvement assessed by successful reduction in the NRS or Macnab scores. Furthermore, similar results were obtained in the comparison between the corresponding and non-corresponding groups of the X-ray group.
Conclusion: TFESI guarantees favorable clinical outcomes even in the absence of confirmative MRI in patients with back and radicular pain. The preemptive application of this procedure could be prioritized and justified in patients suspected of lumbosacral disc herniation based on clinical evaluation and plain radiography only without the preceding MRI verification.
Keywords: lumbosacral disc herniation, epidural injection, transforaminal, numeric rating scale, plain radiography
Introduction
Lumbosacral disc herniation refers to the displacement of the intervertebral disc beyond the boundaries of the disc space, causing lower back and radicular leg pain throughout the myotomal or dermatomal levels.1,2 Pain due to lumbosacral disc herniation is one of the most common causes of musculoskeletal pain.3,4 The prevalence of symptomatic lumbosacral disc herniation is 1–3%.1 The mechanisms of pain due to lumbosacral disc herniation include direct mechanical compression of the sinuvertebral nerve and nerve root and chemical inflammation around them.5–8 In most cases of lumbosacral disc herniation, chemical inflammation is the main cause of lower back and radicular leg pain.5–8 To control the inflammation around the herniated lumbosacral disc, transforaminal epidural steroid injection (TFESI) is commonly used in clinical practice.9 Its effectiveness in controlling pain due to lumbosacral disc herniation has been demonstrated in several previous clinical trials.9–11
Prior to TFESI, spine magnetic resonance imaging (MRI) is performed to diagnose herniated lumbosacral disc and to discern its location and severity.12–14 Based on the spine MRI findings, clinicians determine the exact location of TFESI administration. However, due to the high price and low accessibility of MRI in clinical practice, patients frequently refuse to undergo spine MRI or have to wait for a long time for appropriate treatment while awaiting MRI. Clinicians are usually reluctant to perform TFESI before confirming the diagnosis, location, and severity of the herniated lumbosacral disc on spine MRI, and many patients continue enduring pain without receiving symptomatic treatment with TFESI.
Based on this clinical reality, we speculated whether TFESI could be effectively administered based only on the clinical and spine radiography findings, without performing a spine MRI. If the effects of TFESI with and without confirming the diagnosis with MRI before TFESI are comparable, then TFESI could be administered without MRI as the second-best option in unavoidable circumstances wherein spine MRI cannot be performed.
To the best of our knowledge, no study has evaluated the effectiveness of TFESI after determining the level of injection administration based on the clinical and radiographic findings without a spine MRI prior to the procedure. Thus, we compared the effectiveness of TFESI between patients diagnosed by clinical evaluation and radiography only and those diagnosed by additional MRI. Additionally, we checked the accuracy of the preliminary clinical assumptions using confirmative post-injection MRI in the patients diagnosed only by clinical evaluation and radiography. The primary outcome assessed was pain using the numeric rating scale (NRS), and the secondary outcome was patient satisfaction using the MacNab criteria.
Materials and Methods
Patients
This study was approved by the Institutional Review Board of Wooridul Spine Hospital (WRDIRB-2021-03-004) after obtaining written informed consent from each patient. This study complied with the Declaration of Helsinki’s ethical standards. Data were retrospectively collected from January to December 2019 of consecutive patients with lower back and leg radicular pain, who were subsequently treated with TFESI at the pain clinic after being diagnosed with lumbosacral disc herniation clinically or using spine MRI for confirmation. Patients with prior lumbosacral spine surgical interventions or neurological deficits were excluded. Among the 367 patients finally recruited, 201 patients were empirically treated with TFESI based only on the clinical evaluation and spine radiography without MRI (X-ray group), and lumbosacral disc herniation was confirmed later on post-injection MRI. The spinal level with translational or angular instability, when compared with the adjacent disc level on spine radiography, was conventionally regarded as the main lesion segment15,16 (Figures 1 and 2). The remaining 166 patients were diagnosed with lumbosacral disc herniation using MRI prior to TFESI in addition to the routine clinical evaluation and spine radiography (MRI group). The X-ray group was subdivided into a corresponding group, which comprised patients in whom the lesion level determined by clinical evaluation or plain radiography concurred with that on the post-injection confirmation MRI, and a non-corresponding group, which comprised patients without this concurrence.
 |
Figure 1 Translational instability in the sagittal flexion (A) and extension (B) views on plain radiography. Black lines and arrows indicate the distances as a result of migration of adjacent upper vertebra upon lower lumbar vertebrae during flexion. |
 |
Figure 2 Angular instability in the sagittal flexion (A) and extension (B) views on plain radiography. Black line indicates the angular changes of adjacent upper and lower vertebra that occurs during flexion and extension. |
Transforaminal Epidural Steroid Injection
In our pain clinic, TFESI procedures have been conducted as described below. The patient is placed in a prone position. The fluoroscope is manipulated either in the caudal or cephalad direction until the superior endplate of the lower vertebra is projected as a single solid line, indicating true anteroposterior fluoroscopic view that is aligned parallel to the superior endplate of the lower vertebra. The fluoroscope is rotated by approximately 30–40° ipsilaterally toward the symptomatic side until the “Scotty dog” sign is visible.
The infraneural approach, also termed the retrodiscal or preganglionic approach, is routinely applied. This technique is advantageous in terms of proper access and administration of the injectate into the epidural space behind the targeted disc level as well as along the exiting nerve root. The needle is advanced directly into Kambin’s safe triangle behind the posterior annulus using a tunnel vision technique under fluoroscopic guidance. The operator avoids passing the needle medial to the mid-pedicle position in the oblique view to reduce the risk of incidental dural puncture. Contrast dye is injected to confirm that the flow is limited to the epidural space without intravascular, intrathecal, or soft tissue penetrative leakage. Additionally, a lateral view image is obtained to verify the presence of a contrast medium shadow over the ventral epidural space. Subsequently, a mixture of 4 mL of 0.5% lidocaine and 1 mL (5 mg) of dexamethasone is injected. Injections are routinely repeated at 1–2-week intervals for intended pain relief, either for the subjective satisfaction of the patients or for the objective flattening of the pain intensity to a plateau phase. However, these repetitions should not exceed four sessions, regardless of the degree of patient satisfaction.
Clinical Evaluation
The pain intensity of the participants in this study was evaluated using the NRS, ranging from 0 (no pain) to 10 (worst possible pain). Successful pain relief was defined as a more than 50% reduction in the NRS score when compared with the pretreatment score.17,18 Moreover, patient satisfaction was assessed using the MacNab criteria, which categorizes the treatment response as excellent, good, fair, or poor. Excellent and good responses were considered satisfactory results.19 Comparative evaluations were conducted before the treatment and 2 and 10 weeks after the final injection between the X-ray and MRI groups as well as the corresponding and non-corresponding groups of the X-ray group.
Sample Size Calculation
The sample size calculation was based on the literature comparing paramedian and midline approach groups for lumbar radicular pain.20 A sample size that could differentiate the proportion of clinical success by at least a 30% gap between the two groups was considered clinically relevant in our study. Considering a 0.05 two-sided significance level, power of 80%, and an allocation ratio of 1:1, at least 42 patients were required in each group.
Statistical Analysis
Statistical analyses were performed using Statistical Product and Service Solutions (version 14.0; SPSS Inc., Chicago, IL, USA). Paired t-test was used to evaluate the significance of the reduction in the NRS scores at 2 and 10 weeks posttreatment. Chi-square test was used to compare the sex ratio, main lesion level, main affected side, and improvement in the NRS scores and Macnab criteria results after treatment between the X-ray and MRI groups as well as the corresponding and non-corresponding groups. Student’s t-test was used to compare the age, symptom duration, number of injections, and NRS score before the treatment between the X-ray and MRI groups as well as the corresponding and non-corresponding groups. Results were considered statistically significant if the p-value was less than 0.05.
Results
Comparison of General Characteristics and Clinical Outcomes Between the X-Ray and MRI Groups
There were no significant differences in age, sex ratio, main lesion level, symptom duration, number of injections, affected side, and NRS scores at baseline between the X-ray and MRI groups. The NRS scores in both groups reduced significantly at 2 and 10 weeks after treatment when compared with the pretreatment scores (p<0.001). In the intergroup comparison, no significant difference was found in the improvement in the NRS scores and the Macnab criteria results (Table 1).
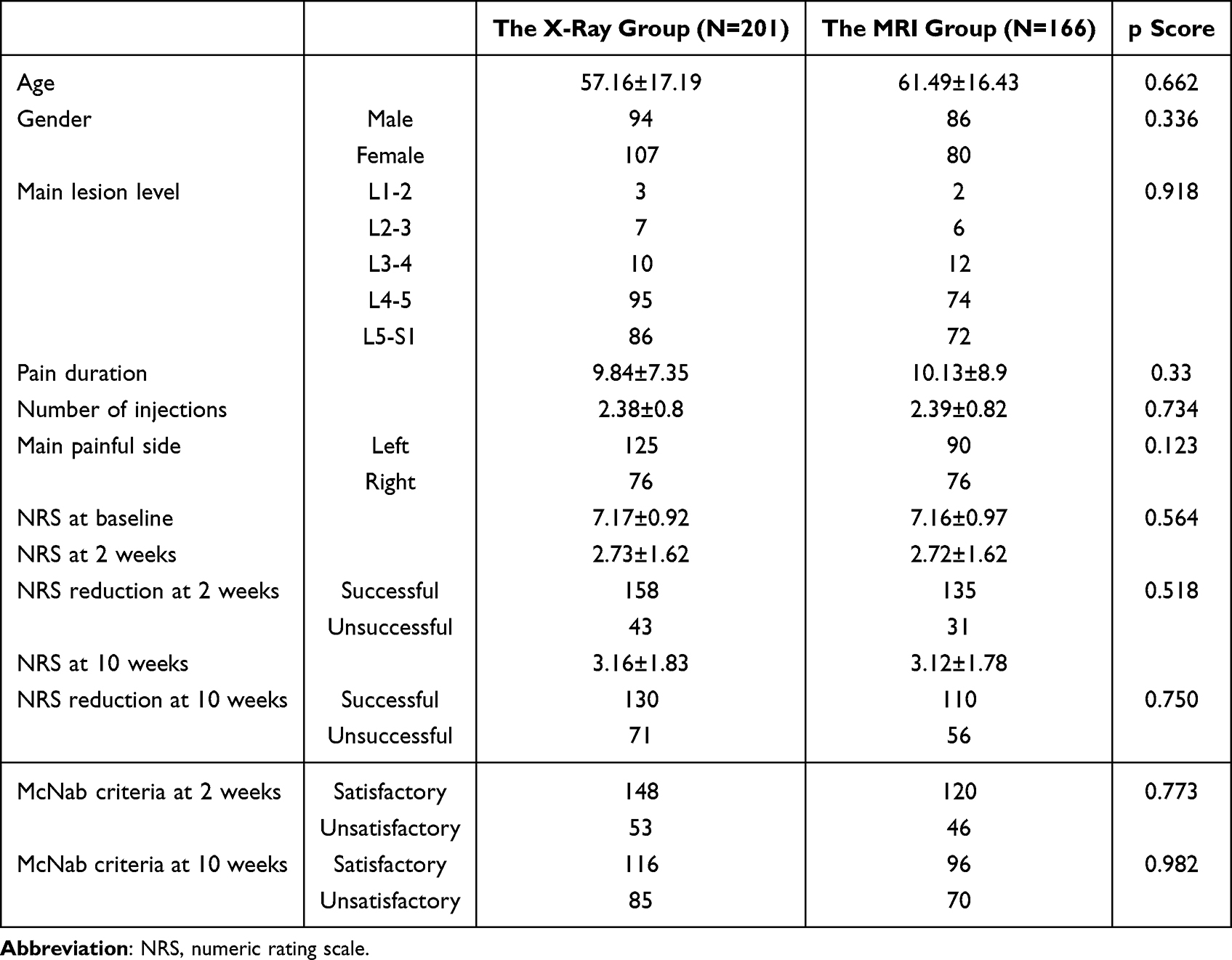 |
Table 1 Comparison of General Characteristics and Clinical Outcomes Between the X-Ray and MRI Groups |
Distribution of Main Lesion Levels as Determined on Radiography and Magnetic Resonance Imaging Post-Treatment in the X-Ray Group
In 62 out of 201 patients in the X-ray group, the spinal level to be treated changed on the post-procedural confirmative MRI. Out of the three patients with L1-2 herniation determined initially on plain radiography, one changed to L3-4 on the confirmative MRI. Among the seven patients preliminarily determined as having L2-3 herniation, one changed to L1-2, another to L3-4, and the remaining five to L4-5 level on the confirmative MRI. Moreover, of the 10 cases with L3-4 herniation, 3 patients were confirmed to have a lesion at L2-3, L4-5, and L5-S1, respectively. Among the 95 cases initially determined as having L4-5 lesions, 2 patients changed to L1-2, 3 to L2-3, 8 to L3-4, and 13 to L5-S1 lesions. Among the 86 patients initially determined as having L5-S1 lesions, 3 changed to L1-2, 3 to L2-3, 9 to L3-4, and 14 to L4-5 lesions (Table 2).
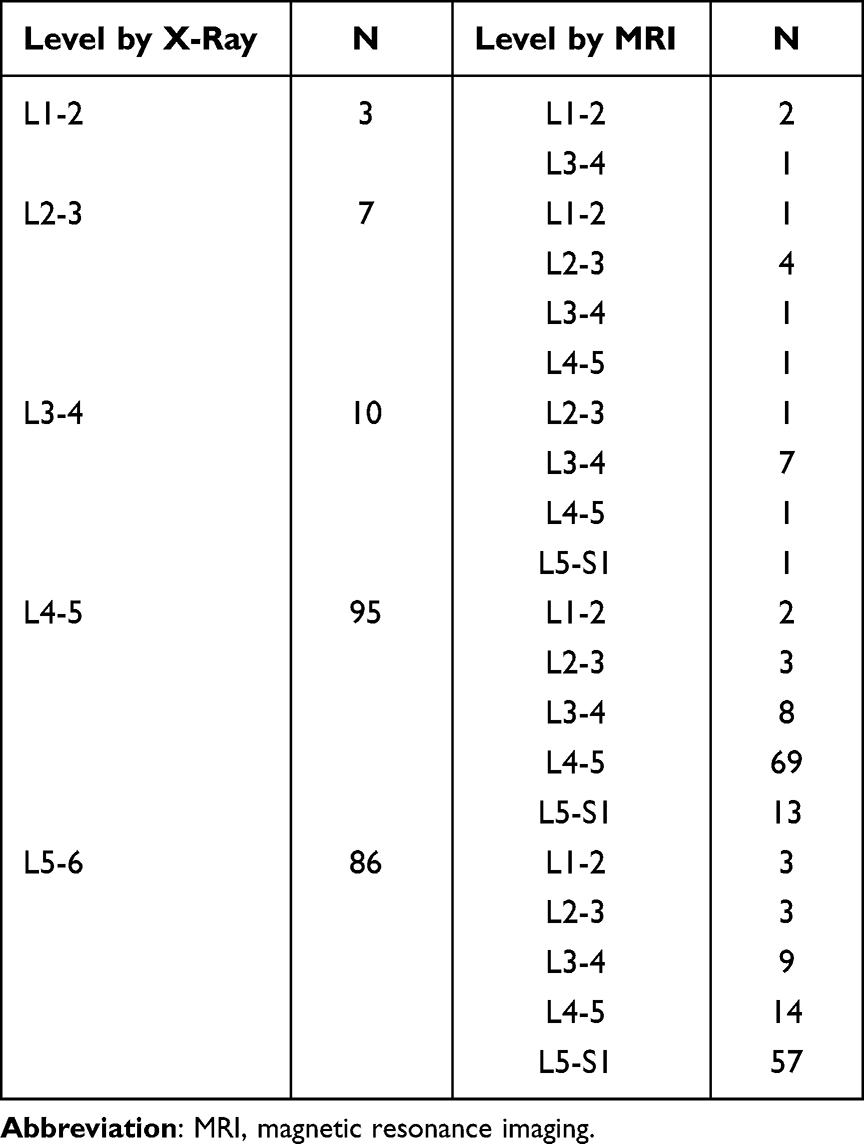 |
Table 2 Distribution of Main Lesion Levels Determined by X-Ray and MRI After Injection in the X-Ray Group |
Comparison of General Characteristics and Clinical Outcomes Between the Corresponding and Non-Corresponding Groups of the X-Ray Group
Within the X-ray group, the corresponding group and non-corresponding group included 139 patients and 62 patients, respectively. No significant differences in age, sex ratio, main lesion level, symptom duration, number of injections, affected side, and NRS scores at the baseline were observed between these two groups. The NRS score reduced significantly in both the groups at 2 and 10 weeks after treatment when compared with the pretreatment scores (p<0.001). However, no significant difference was found in the improvement in the NRS scores and the Macnab criteria results between the two groups (Table 3).
 |
Table 3 Comparison of General Characteristics and Clinical Outcomes Between the Corresponding and Non-Corresponding Groups in the X-Ray Group |
Discussion
TFESI, which is more target-specific for pain generators, such as the ventral epidural space and nerve root, is performed by advancing the needle through the neural foramen of the specific disc level that is considered the main source of pain.21
Since high levels of specificity and accuracy are mandatory during the spinal level designation before TFESI, pretreatment MRI is preferably requested for this injection method than for other methods, such as interlaminar or caudal injections.
However, due to the limited or non-availability of MRI, particularly in primary clinical settings, TFESI is frequently administered based on clinical evaluation and radiographic findings only, skipping the prerequisite lesion level determination. This study showed that clinical improvement with TFESI without the aid of MRI confirmation is non-inferior and comparable to treatment performed with MRI. This suggests that relevant clinical outcomes can be achieved without expensive and sophisticated tools, such as MRI, for accurate diagnosis. Therefore, in patients with pain originating from suspected disc herniation and in case of non-availability of spine MRI due to financial or logistic difficulties, TFESI could be conducted without confirmation of the spinal lesion level using MRI. However, the cause of lower back and radicular leg pain could be due to other spinal disorders, such as infection or tumor, and not due to lumbosacral disc herniation; therefore, it is necessary to explain this possibility to patients prior to performing TFESI without MRI.
In most countries, prior to TFESI, MRI is performed to confirm the presence, location, and severity of the lumbosacral disc herniation. In the Republic of Korea, TFESI can be performed even without the MRI findings, assuming the primary cause of pain is lumbosacral disc herniation and the pathological level is predicted by clinical evaluation and spine radiography only. Therefore, this study investigated the effects of TFESI in patients with lumbosacral herniated discs with and without confirmed diagnosis using MRI before TFESI.
Although TFESI is conducted after proper access to a specific neural foramen, it does not preclude the spread of the medication into a nerve root and may even involve the epidural area. A 5 mL dose of injectate administered during TFESI might be sufficient to include the epidural spaces at the adjacent disc levels. Furman et al demonstrated that 4 mL of contrast dye was sufficient for involving both the superior and inferior disc levels of the index lesion level in 93% of their TFESI cases.22 Therefore, this amount of medication could easily enter the epidural space and consequently lead to misdiagnosis and incorrect lesion-level decisions based on plain radiography.
In our study, the tentative diagnoses based on plain radiography and clinical evaluation presented almost 70% accuracy without the aid of MRI. This result suggests that a thorough clinical or radiographic assessment might be useful in providing clues for a relatively accurate diagnosis as well as the consequent optimal transforaminal injection. Among the 62 patients (30.8%) in whom the lesion level for treatment changed after the post-procedural MRI, only 21 patients (10.4%) showed a discrepancy of more than two levels between the initial and final diagnosis. In other words, 5 mL of transforaminal injectate was sufficient to relieve the pain in approximately 90% of the patients with a primarily correct diagnosis or with discrepancy within one level.
Notably, the actual source of pain does not always coincide with the prominent MRI findings.23,24 We frequently encountered the discrepancy between structural lesion and clinical or functional findings.25 Spinal pain could be due to chemical irritation other than mechanical compression of the neural tissues, such as the nerve root and sinuvertebral nerves that are broadly innervated over the epidural spaces, which justifies performing precedent epidural injection rather than direct surgical decompression.26,27
Paradoxically, the incorrect injection level, as later determined on MRI, could actually be correct. For instance, the most prominent disc protrusion at the L4-5 level on MRI might not be prioritized, or it could rule out the advanced degeneration or mild bulging phenomenon at the L3-4 level as the actual pain source. Thus, the L3-4 injection level designated superficially using plain radiography could incidentally be the actual affected level, although the L4-5 level was shown to be the main structural lesion later on MRI.
Another interpretation for these coincidental clinical improvements, regardless of the treatment level discrepancies, would be that the retrodiscal (infraneural) approach routinely performed might imitate the supraneural approach performed one level below, thus yielding similar relief. Retrodiscal transforaminal injection causes the medication to spill into the epidural space as well as the traversing root connected to the lower disc level.28,29 For example, a retrodiscal injection at the L4-5 level may not be topically restricted to the L4-5 ventral epidural segment and could involve the traversing L5 nerve root, mimicking the drug-spreading pattern observed in the L5-S1 supraneural approach. Therefore, a one-level discrepancy between the radiograph and MRI scan could readily be compensated by equivocal efficacy through the dual access of injections across adjacent levels.
This study has some limitations. The retrospective design in this study is predisposed to a selection bias since the patients undergoing post-procedural MRI were compared with those undergoing pre-procedural MRI. Second, the results and conclusions were established based on a relatively short-term follow-up period (10 weeks). However, this may be excused because the clinical course after each epidural injection usually declines over 2–3 months, along with diminishing steroid effects, and dexamethasone used in this study tended to last for a shorter duration than methylprednisolone or triamcinolone.30
Conclusion
TFESI seems to guarantee a favorable clinical outcome in patients with back and radicular pain, even in the absence of a confirmative MRI. In unavoidable circumstances where spine MRI cannot be performed, the preemptive performance of this procedure could be prioritized and justified as the second-best option in patients suspected of lumbosacral disc herniation based on clinical evaluation and radiographs only without the preceding MRI verification.
Funding
This study was supported by a National Research Foundation of Korea grant funded by the Korean government (grant no. NRF-2022R1F1A1072553).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jordan J, Konstantinou K, O’Dowd J. Herniated lumbar disc. BMJ Clin Evid. 2009;2009:1118.
2. Lee JH, Lee S-H. Clinical and radiological characteristics of lumbosacral lateral disc herniation in comparison with those of medial disc herniation. Medicine. 2016;95(7):e2733. doi:10.1097/MD.0000000000002733
3. Ruschel LG, Agnoletto GJ, Aragão A, et al. Lumbar disc herniation with contralateral radiculopathy: a systematic review on pathophysiology and surgical strategies. Neurosurg Rev. 2021;44:1071–1081. doi:10.1007/s10143-020-01294-3
4. Jang SH, Chang MC. Follow-up of at least five years after lumbar transforaminal epidural steroid injection for radicular pain due to lumbar disc herniation. Ann Palliat Med. 2020;9(1):116–118. doi:10.21037/apm.2020.01.05
5. Takahashi N, Yabuki S, Aoki Y, et al. Pathomechanisms of nerve root injury caused by disc herniation: an experimental study of mechanical compression and chemical irritation. Spine. 2003;28(5):435–441. doi:10.1097/01.BRS.0000048645.33118.02
6. Omarker K, Myers RR. Pathogenesis of sciatic pain: role of herniated nucleus pulposus and deformation of spinal nerve root and dorsal root ganglion. Pain. 1998;78(2):99–105. doi:10.1016/S0304-3959(98)00119-5
7. Manchikanti L, Buenaventura RM, Manchikanti KN, et al. Effectiveness of therapeutic lumbar transforaminal epidural steroid injections in managing lumbar spinal pain. Pain Physician. 2012;15:199–245. doi:10.36076/ppj.2012/15/E199
8. Schroeder GD, Guyre CA, Vaccaro AR. The epidemiology and pathophysiology of lumbar disc herniations. Semin Spine Surg. 2016;28:2–7. doi:10.1053/j.semss.2015.08.003
9. Kwak S, Jang SH, Chang MC. Long-term outcomes of transforaminal epidural steroid injection in patients with lumbosacral radicular pain according to the location, type, and size of herniated lumbar disc. Pain Pract. 2021;21(8):836–842. doi:10.1111/papr.13029
10. Sariyildiz MA, Batmaz İ, Yazmalar L, et al. The effectiveness of transforaminal epidural steroid injections on radicular pain, functionality, psychological status and sleep quality in patients with lumbar disc herniation. J Back Musculoskelet Rehabil. 2017;30(2):265–270. doi:10.3233/BMR-150438
11. Sencan S, Celenlioglu AE, Yazici G, et al. Transforaminal epidural steroid injection improves neuropathic pain in lumbar radiculopathy: a prospective, clinical study. Neurol India. 2021;69(4):910–915. doi:10.4103/0028-3886.323894
12. Herzog RJ. The radiologic assessment for a lumbar disc herniation. Spine. 1996;21:19s–38s. doi:10.1097/00007632-199612151-00004
13. Ghahreman A, Bogduk N. Predictors of a favorable response to transforaminal injection of steroids in patients with lumbar radicular pain due to disc herniation. Pain Med. 2011;12(6):871–879. doi:10.1111/j.1526-4637.2011.01116.x
14. Lee JH, Lee SH. Physical examination, magnetic resonance image, and electrodiagnostic study in patients with lumbosacral disc herniation or spinal stenosis. J Rehabil Med. 2012;44:845–850. doi:10.2340/16501977-1034
15. Zhang F, Wang H, Xu H, et al. Radiologic analysis of kinematic characteristics of Modic changes based on lumbar disc degeneration grade. World Neurosurg. 2018;114:e851–e856. doi:10.1016/j.wneu.2018.03.098
16. Kanemura A, Doita M, Kasahara K, et al. The influence of sagittal instability factors on clinical lumbar spinal symptoms. J Spinal Disord Tech. 2009;22(7):479–485. doi:10.1097/BSD.0b013e31818d1b18
17. Manchikanti L, Cash KA, Pampati V, et al. Two-year follow-up results of fluoroscopic cervical epidural injections in chronic axial or discogenic neck pain: a randomized, double-blind, controlled trial. Int J Med Sci. 2014;11(4):309–320. doi:10.7150/ijms.8069
18. Manchikanti L, Malla Y, Cash KA, et al. Comparison of effectiveness for fluoroscopic cervical interlaminar epidural injections with or without steroid in cervical post-surgery syndrome. Korean J Pain. 2018;31(4):277–288. doi:10.3344/kjp.2018.31.4.277
19. Ramirez Leon JF, Rugeles Ortiz JG, Martinez CR, et al. Surgical treatment of cervical radiculopathy using an anterior cervical endoscopic decompression. J Spine Surg. 2020;6(S1):S179–S185. doi:10.21037/jss.2019.09.24
20. Ghai B, Vadaje KS, Wig J, et al. Lateral parasagittal versus midline interlaminar lumbar epidural steroid injection for management of low back pain with lumbosacral radicular pain: a double-blind, randomized study. Anesth Analg. 2013;117(1):219–227. doi:10.1213/ANE.0b013e3182910a15
21. Carassiti M, Pascarella G, Strumia A, et al. Epidural steroid injections for low back pain: a narrative review. Int J Environ Res Public Health. 2021;19(1):231. doi:10.3390/ijerph19010231
22. Furman MB, Mehta AR, Kim RE, et al. Injectate volumes needed to reach specific landmarks in lumbar transforaminal epidural injections. PM & R. 2010;2(7):625–635. doi:10.1016/j.pmrj.2010.04.023
23. Dydyk AM, Khan MZ. Radicular back pain. In: StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2021, StatPearls Publishing LLC; 2021.
24. Fritz J, Niemeyer T, Clasen S, et al. Management of chronic low back pain: rationales, principles, and targets of imaging-guided spinal injections. Radiographics. 2007;27(6):1751–1771. doi:10.1148/rg.276065509
25. Lee JH, Lee SH, Seo IS. The characteristics of gait disturbance and its relationship with posterior tibial somatosensory evoked potentials in patients with cervical myelopathy. Spine. 2011;36(8):E524–E530. doi:10.1097/BRS.0b013e3181f412d9
26. Lee JH, Lee S-H. Comparison of clinical efficacy between interlaminar and transforaminal epidural injection in patients with axial pain due to cervical disc herniation. Medicine. 2016;95(4):e2568. doi:10.1097/MD.0000000000002568
27. Shayota B, Wong TL, Fru D, et al. A comprehensive review of the sinuvertebral nerve with clinical applications. Anat Cell Biol. 2019;52(2):128–133. doi:10.5115/acb.2019.52.2.128
28. Jeong HS, Lee JW, Kim SH, et al. Effectiveness of transforaminal epidural steroid injection by using a preganglionic approach: a prospective randomized controlled study. Radiology. 2007;245(2):584–590. doi:10.1148/radiol.2452062007
29. Lee JW, Kim SH, Choi J-Y, et al. Transforaminal epidural steroid injection for lumbosacral radiculopathy: preganglionic versus conventional approach. Korean J Radiol. 2006;7(2):139–144. doi:10.3348/kjr.2006.7.2.139
30. Kim D, Brown J. Efficacy and safety of lumbar epidural dexamethasone versus methylprednisolone in the treatment of lumbar radiculopathy: a comparison of soluble versus particulate steroids. Clin J Pain. 2011;27(6):518–522. doi:10.1097/AJP.0b013e31820c53e0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.