Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Transcranial Photobiomodulation For The Management Of Depression: Current Perspectives
Authors Askalsky P ![]() , Iosifescu DV
, Iosifescu DV ![]()
Received 4 July 2019
Accepted for publication 26 October 2019
Published 22 November 2019 Volume 2019:15 Pages 3255—3272
DOI https://doi.org/10.2147/NDT.S188906
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Paula Askalsky,1 Dan V Iosifescu1,2
1Department of Psychiatry, NYU Langone School of Medicine, New York, NY, USA; 2Clinical Research Division, Nathan Kline Institute for Psychiatric Research, Orangeburg, NY, USA
Correspondence: Dan V Iosifescu
Department of Psychiatry, NYU School of Medicine, One Park Avenue, 8th Floor, New York, NY 10016, USA
Tel +1 646-754-5156
Email [email protected]
Abstract: Major depressive disorder (MDD) is a prevalent condition associated with high rates of disability, as well as suicidal ideation and behavior. Current treatments for MDD have significant limitations in efficacy and side effect burden. FDA-approved devices for MDD are burdensome (due to repeated in-office procedures) and are most suitable for severely ill subjects. There is a critical need for device-based treatments in MDD that are efficacious, well-tolerated, and easy to use. In this paper, we review a novel neuromodulation strategy, transcranial photobiomodulation (t-PBM) with near-infrared light (NIR). The scope of our review includes the known biological mechanisms of t-PBM, as well as its efficacy in animal models of depression and in patients with MDD. Theoretically, t-PBM penetrates into the cerebral cortex, stimulating the mitochondrial respiratory chain, and also significantly increases cerebral blood flow. Animal and human studies, using a variety of t-PBM settings and experimental models, suggest that t-PBM may have significant efficacy and good tolerability in MDD. In aggregate, these data support the need for large confirmatory studies for t-PBM as a novel, likely safe, and easy-to-administer antidepressant treatment.
Keywords: low-level light therapy, photobiomodulation, near infrared radiation, major depressive disorder, depression
Introduction
Major depressive disorder (MDD) is prevalent (affecting 16.2% of the US population, lifetime) and disabling, being among the leading causes of years lived with disability worldwide.1,2 Existing antidepressants have burdensome side effects and are only partially effective; more than one-third of MDD patients do not achieve remission after several adequate antidepressant trials, and relapses are frequent.3 One option for individuals who do not respond to or tolerate antidepressant medications are neuromodulation strategies, which include the FDA-approved electroconvulsive therapy (ECT), transcranial magnetic stimulation (rTMS), and vagus nerve stimulation (VNS). Other neuromodulation options, such as transcranial direct current stimulation (tDCS), magnetic seizure therapy (MST), and deep brain stimulation (DBS), remain experimental.4 Despite their efficacy, FDA-approved neurostimulation strategies are complex procedures requiring multiple visits (ECT and rTMS), anesthesia (ECT), or surgical implantation (VNS). There is a clear need for a safe and effective neuromodulation strategy that may be well tolerated and potentially used by patients at home.
Transcranial photobiomodulation (t-PBM) is a novel form of neuromodulation, based on non-retinal exposure to light at specific wavelengths. t-PBM with near-infrared radiation (NIR) has yielded promising early results for the treatment of neuropsychiatric disorders.5 t-PBM has a low cost, good safety profile, and it is easy to self-administer. Therefore, it has the potential to become widely accessible.
We have reviewed in this paper the known biological mechanisms of t-PBM and its clinical efficacy data in MDD.
Transcranial Transmission Of NIR And Red Light
Before delving into the mechanics and potential effects of PBM, it is important to consider whether t-PBM can even reach the brain. After all, the light must pass through various layers of tissue and the skull, before reaching the cortex. An early study performed in a small cohort of patients undergoing neurosurgery postulated that out of all the layers between the scalp and cerebral tissue, the skull was the greatest impeder of light transmission.6 Others have pointed out that even 2mm of hair can absorb or reflect approximately 98% of NIR energy from a 10W laser.7
Thankfully, several studies have tried to answer this question directly. Jagdeo et al (2012) measured the transmission of NIR and red light with a piece of human cadaver skull and overlying tissue. They used a commercial LED device used in multiple clinical studies, the Omnilux New-U.8 They found that compared to red light (wavelength 633nm), NIR light (830nm) more appreciably penetrated the skull and soft tissue. Still, only 0.9–2.1% of NIR light penetrated through the cadaver skull and intact soft tissue in the frontal or temporal regions. Lapchak et al (2015) used a Class IV laser with a surface power density of 700mW/cm2 and found that more than 95% of the NIR light transmission was attenuated when applied to human cadaveric skulls.9 In a later study using a human cadaveric model, 808nm light, delivered by a transcranial laser system, penetrated to a brain depth of 40–50mm.10
Some have looked at the effect of wavelength, power, and delivery mode on transmission, as well. In the same study by Tedford et al (2015) mentioned earlier, the authors found that out of three tested wavelengths ranging from 660 to 940nm, 808nm showed superior penetration.10 Another study looking at the penetration depths of 675nm, 780nm, and 835nm in various human tissues, including post-mortem brain tissue, also argued that greater transmission was achieved with longer wavelengths.11 Henderson and Morries (2015) performed ex vivo studies of NIR penetration through 3cm of lamb skull, tissue, and brain.12 Two LED NIR emitters with lower energy (50 and 200mW) did not penetrate the 3cm of tissue. On the other hand, devices with power in the range 6–15W did penetrate the tissue. Further, the same 15W device reached variable depths, depending on wavelength used. With the 810nm setting, 2.9% of the power density was delivered to the cortex and with the 980nm setting, only 1.22% was delivered. This observation is consistent with the data presented earlier that transmission of t-PBM is likely dependent on wavelength and that 810nm may be preferable for this reason. Lastly, they reported that pulsed emission settings (10Hz) led to higher energy delivery, as seen in 2 of the 3 tested settings. However, those two settings also included longer wavelengths (980nm), while the third setting only had a wavelength of 810nm. Therefore, it is unclear if the increased energy delivery is due to pulsing alone or an interaction between wavelength and pulsing.
Two computation studies have also looked at ways to enhance penetration of light. Yue et al (2015) proposed using a multiunit emitter array, evenly distributed across the scalp, to take advantage of photon scattering properties in the brain.13 Using Monte Carlo simulations in a human head model to test this idea, they demonstrated that the multiunit emitter enhanced photon flux and improved uniformity of distribution. While this model is theoretically interesting, these results are likely not necessarily applicable to in vivo models, since little energy is absorbed through the skull and overlying tissues. Therefore, the photo-scattering of incident light described above is unlikely to be seen in the human brain. Another study looked at whether transcranial and transsphenoidal administration of red and NIR light could reach deep brain structures, and specifically, the substantia nigra.14 Both a cadaveric model and the Monte Carlo method were used. Ultimately, NIR light was felt to be more effective for transmission to the substantia nigra, due to less absorption and scattering; this was particularly true when the light was delivered via the sphenoid sinus.
Overall, studying the transcranial penetration of NIR and red light has several challenges. For one, only cadaveric models for humans can be used. Therefore, it is difficult to directly test the effect of blood flow and hydration status on attenuation of light. Though we are currently limited in our ability to study the full depths of t-PBM’s reach in the in vivo human brain, there are several measures that we can take to enhance penetration. Based on the data presented above, using wavelengths in the range of 808–835nm, laser devices, higher power densities, and pulsed parameters will likely increase efficacy. Practically speaking, we may also be limited to t-PBM application to the prefrontal cortex, unless patients are willing to shave their hair for the duration of treatment (which would be required to target other cortical brain areas). Further, while LED devices are less expensive and potentially more appealing to the average consumer, their clinical effectiveness is in question. Hopefully, future clinical studies utilize tools such as blood flow changes (measured by BOLD signal on fMRI) and bioenergetic metabolite changes (measured with magnetic resonance spectroscopy) to understand the depths of cortical effects in-vivo in humans.
Proposed Mechanisms Of t-PBM
Mitochondrial Function And Association With Depressive Symptoms
To understand the proposed mechanisms of t-PBM, we must first understand some basic principles of the mitochondria and the production of ATP. Oxidative phosphorylation, which takes place in the inner mitochondrial membrane, is one of the mechanisms by which ATP is generated. Substrates donate electrons to individual complexes (Complexes I-IV) and mobile components of the electron transport chain (ETC), such as coenzyme Q and cytochrome C oxidase (CCO), move electrons between the protein complexes. A proton gradient is established along the way, creating an electrochemical force. Ultimately, the energy stored by the proton gradient is captured by complex V and used to generate ATP.15
Multiple animal and human studies have found mitochondrial differences in depression, with specific changes seen in respiration and generation of ATP. In a rat model of depression, complexes I, III, and IV of the ETC were inhibited in the cerebral cortex and cerebellum.16 Changes in cytochrome oxidase activity have also been implicated in depression.17 Phosphorus magnetic resonance spectroscopy (31P-MRS) allows in vivo measurements of energy-rich compounds resulting from mitochondrial activity. For example, β-NTP is used to estimate the level of ATP.18 Phosphocreatine transfers high-energy phosphate groups to ATP, making it another useful marker.19 Using 31P-MRS, Harper et al (2016) found that decreased β-NTP levels correlated with executive dysfunction in depressed geriatric patients.20 Similarly, other 31P-MRS studies reported lower levels of β-NTP21 and compensatory higher levels of phosphocreatine (PCr)22 in non-geriatric adults with MDD. In both studies, these abnormalities related to mitochondrial function were associated with clinical response to antidepressants.
Changes in glucose metabolism have also been described in FDG PET studies in MDD. For example, MDD patients were shown to have increased mean glucose metabolism in the lateral orbital cortex, ventrolateral prefrontal cortex, left amygdala, and posterior cingulate cortex, as well as decreased metabolism in the subgenual ACC and dorsal medial/dorsal anterolateral PFC.23 Following treatment, metabolism in the left amygdala and left subgenual ACC decreased in these subjects. Another FDG PET study of MDD participants post-fluoxetine treatment showed that treatment responders had decreased glucose metabolism in limbic and striatal areas, as well as increased metabolism in brainstem and dorsal cortical regions.24
Changes in mitochondrial respiration in depression have been found outside of the central nervous system as well. Peripheral blood mononuclear cells of depressed patients were shown to have significantly impaired mitochondrial function. In fact, greater mitochondrial dysfunction correlated with severity of neurovegetative symptoms, including fatigue and poor concentration.25 Similarly, Hroudova et al (2013) found that the respiratory rate and maximal capacity of the ETC were significantly decreased in platelets of depressed patients.26 Muscle biopsy samples from depressed patients with physical symptoms had a decreased rate of ATP production and more frequent mitochondrial DNA deletions than controls.27 Treatment studies have yielded further evidence for the mitochondrial hypothesis of depression. After 21 days of treatment with desipramine and fluoxetine, somatic mitochondria in the rat frontal cortex had enhanced energy metabolism (though there was decreased energy production in synaptic mitochondria).28
Mitochondrial Effects Of PBM
Mitochondria are the main site of physiologic changes related to t-PBM. The cascade starts with CCO, which is a chromophore, a photoacceptor, and the terminal enzyme of the electron transport chain.29,30 t-PBM has been found to specifically increase CCO activity and expression.31–33 Studies have also shown increases in complex II, II, III, and IV activity,34,35 as well as upregulation of gene coding for subunits of complex I, complex IV, and ATP synthase.36 Additionally, PBM of complexes II and III still occurs with higher fluence lasers, despite previous concerns that the increased level of stimulation would be too strong.37 Though the focus has primarily been on enhanced effects of mitochondrial function, some have suggested that pulsed t-PBM may also increase the number of isolated mitochondria.38
Further, low-level laser therapy has been shown to increase levels of ATP, the rate of oxygen consumption, and cerebral oxygenation.31,33,39–42 In a mouse model, low-intensity NIR was able to ameliorate reduction of ATP that was previously induced by oxygen-glucose deprivation.43 Another study using two different depression mouse models showed increased ATP biosynthesis and mitochondrial complex IV expression following t-PBM in the prefrontal cortex specifically.44 While the time-to-effect of metabolic changes is unclear, Ferraresi et al (2015) suggest that the ATP levels are highest about six hours following treatment.45 On the other hand, another group found that bioenergetic changes were noticeable only after two weeks of repeated treatments.46
Effects Of Specific Wavelengths Of PBM On Mitochondria
Though t-PBM with red and NIR light can include wavelengths from 600 to 1070nm,47 specific wavelengths have been directly linked to mitochondrial activity. 810nm NIR activates CCO, increases mitochondrial oxygen consumption, and leads to higher levels of ATP.48,49 Further, a mouse model of TBI showed improvement in wavelength-dependent fashion - namely, 660nm and 810nm treatments led to improvement, while 730 and 980nm treatments did not.50 Subsequent analyses of 810nm and 980nm wavelengths propose that 810nm acts on CCO, but that 980nm works on temperature-gated calcium ion channels.51
Blood Flow And t-PBM
Several studies have looked at t-PBM’s ability to alter regional cerebral blood flow (CBF). In one animal study, NIR laser irradiation increased cerebral blood flow by 30%.52 Additionally, repeated NIR LED irradiation to the forehead increased regional CBF by 20% in a patient in persistent vegetative state.53 In a larger study of 25 healthy, elderly women, Salgado et al (2015) found that transcranial LED therapy in the red-wavelength spectrum also increased local CBF.54 Lastly, Dias et al (2012) showed dose-dependent modulation of vascular endothelial growth factor (VEGF), which stimulates angiogenesis,55 and VEGF Receptor-255 (VEGFR-2) in rat masseter muscles, following 10 laser irradiations with 780nm light.56
Nitric Oxide
Nitric oxide (NO) is an endogenous vasodilator that plays an important role in normal circulation. NO can also inhibit respiration by binding to cytochrome oxidase and displacing oxygen.57 Differences in nitric oxide levels have been seen in depressed versus non-depressed populations.58 Additionally, low-light level therapy has been shown to alter nitric oxide activity and may be a key in understanding the downstream effects of the treatment. Zhang et al (2009) showed that nitric oxide was directly implicated in the protective effects of NIR in an animal model of cardiomyocyte injury.59 In another study, NIR irradiation increased both NO concentration and local cerebral blood flow in mice.52 When nitric oxide synthase was blocked, cerebral blood flow and NO failed to increase. While this was used as evidence that NO played a role in regional CBF changes after irradiation, others have suggested that the effects of nitric oxide may be independent of nitric oxide synthase.60 Lastly, it has been proposed that PBM may work by releasing NO from CCO and therefore disinhibiting mitochondrial respiration.57
Reactive Oxygen Species (ROS) And Neuroinflammation
In 2007, Sarandol et al found that red blood cells (RBCs) were more susceptible to oxidation in depressed patients, compared to controls.61 Further, they saw that superoxide dismutase (SOD) activity was significantly higher in depressed patients and that the level of SOD activity positively correlated with disease severity. By the same token, PBM has been shown to effect oxidative stress and inflammation. An earlier study suggested that in vitro use of NIR could potentially protect the RBC membrane.62 Huang et al (2013) found that t-PBM actually increased ROS in normal neurons, but reduced ROS in oxidatively stressed neurons.63 Going even further, Salehpour et al (2018) demonstrated that NIR t-PBM could affect behavioral outcomes and oxidative stress in a mouse model.64 They used sleep deprivation to induce oxidative stress in the hippocampus and then looked at effects on spatial and episodic-like memories. When NIR was applied transcranially, antioxidants were enhanced in the hippocampus and cognitive impairment was ameliorated. In a mouse depression model, PBM decreased malondialdehyde levels and increased levels of antioxidants enzyme activity (i.e., GPx, SOD, TAC) in the prefrontal cortex and hippocampus. Additionally, t-PBM reduced pro-inflammatory cytokines.65
Apoptosis Mechanisms
In addition to the downstream effects already explained, t-PBM may have a role in preventing apoptosis, resulting in neuroprotection. In one study, apoptotic markers in the prefrontal cortex and hippocampus were elevated after five days of sub-chronic restraint stress.65 The authors found that t-PBM ameliorated the stress-induced pro-apoptotic response, as evidenced by a reduced Bax/Bcl-2 and cytosolic/mitochondrial CCO ratios. Other studies have similarly demonstrated a reduction in the Bax/Bcl-2 ratio following t-PBM.31,66 Additionally, NIR has been shown to protect against neuronal loss in the setting of ischemic insult.43,67,68
Some authors suggest that t-PBM can even help with neurogenesis. Tanka et al (2011) found that acute or chronic exposure to infrared radiation could increase the number of BrdU-positive cells in CA1 region of the hippocampus, suggesting increased proliferation.69 Similarly, exposure to a 810nm laser following controlled cortical impact in a mouse model of TBI led to significantly higher levels of brain-derived neurotrophic factors (BDNF) in some sub-regions of the hippocampus.70 In an animal model of stroke, t-PBM not only decreased the infarct size, but it also increased levels of biomarkers indicative of cell proliferation.71
Pre-Clinical Trials Of t-PBM Treatment For Depression (See Table 1)
One of the earliest studies compared acute and chronic exposure of infrared radiation against controls.69 Acutely exposed rats underwent infrared treatment for one session, while chronically exposed rats completed 10 sessions. During each treatment, the animals’ heads were immobilized and irradiated for 3 mins (highest emissivity values within 0.6–1.6μm, maximal irradiation intensity of 1800–2200mW). Twenty-four hours after the last irradiation treatment, the rats were subjected to behavioral testing, including the elevated plus maze, the light/dark test, and the forced swim test. Researchers found that chronic exposure of infrared radiation significantly and consistently ameliorated anxiety and depression-related behavior, compared to acutely exposed rats and controls. In addition, they found that both acute and chronic exposure to the treatment condition significantly increased the number of BrdU-positive cells in CA1 of the hippocampus, indicating neurogenesis. Since both acute and chronic exposures led to hippocampal neurogenesis, this finding could not explain the differences in behavioral outcomes between the two groups.
 |
Table 1 All Relevant Basic Research Studies That Utilized Photobiomodulation, With Wavelengths In The Red And/Or Near-Infrared Range, In Experimental Models Of Depression |
Xu et al (2017) also looked at the effects of chronic irradiation.44 (t-PBM) of the cerebral cortex was performed for 30 mins daily, for a total of 28 days. A diode laser, with a wavelength of 808nm, was used to deliver a power output density of 23mW/cm2 to the scalp. After 14 days of treatment, the t-PBM treated mice showed a significantly lower immobility time in the forced swim test and the tail suspension test (two behavioral assessments of depressive behavior), compared to sham-treated mice. Interestingly, this attenuation effect was stable after the 21st day of treatment. In an attempt to elucidate the underlying mechanism behind t-PBM’s therapeutic effect, they also measured the mitochondrial complex I-IV content and level of ATP biosynthesis in the prefrontal cortex, hippocampus, and hypothalamus. Following the full course of treatment, ATP biosynthesis and mitochondrial complex IV both significantly increased in the prefrontal cortex only. Taken together, this paper suggests that t-PBM reduces depressive symptoms via increased ATP and mitochondrial complex IV levels in the prefrontal cortex.
In another study using low-level infrared laser irradiation, several different power settings were tested to assess alterations in depressive behavior by dose.72 First, 80, 200, and 400 mW, all on continuous wave mode, were compared in their ability to improve mobility during the forced swim test in normal rats. Irradiation was performed daily for 1 week during this initial phase. A diode (GaAlAs) laser (Lasotronic Inc., Zug, Switzerland) with a wavelength of 804nm was used to irradiate the entire cortex via six different points, for 1 min per point. For the 3 powers listed above, the power densities were 0.64, 1.60, and 3.18W/cm2, respectively, and the three energy doses were 4.8, 12, and 24J/point. After 7 days of treatment, normal rats treated with the 400mW laser showed more depressive symptoms (significant increase in immobility, as well as decrease in both swimming and climbing during the forced swim test) compared to controls. On the other hand, those treated with 80 mW had significantly decreased immobility time, increased swimming, and increased climbing behavior. In the second phase of the study, rats were given reserpine to create an animal model of depression. A subgroup of the reserpinized rats were irradiated daily for 7 days, using the 80mW power setting. Treatment with 80mW was able to reverse the depression-like behaviors of reserpinized rats. Overall, these results show a biphasic response to irradiation, with higher power setting causing worsening depression-like behavior and lower power settings leading to amelioration of symptoms.
Another study compared two wavelengths of laser light against citalopram in a rat depression model.73 After undergoing chronic mild stress procedures over 4 weeks to induce a depressive phenotype, rats were divided into a stress group, a citalopram group, a red laser-group (630 nm), and an NIR laser group (810 nm). All t-PBM treatments were performed over the prefrontal region, using a GaAlAs diode laser (Mustang 2000þ, Moscow, Russia). The laser was set to 10-Hz pulsed wave with power densities of 89mW/cm2 for red beams and 562mW/cm2 for NIR beams. Both treatment settings had an average energy density of 1.18±0.01J/cm2 per each session. Following 3 weeks of treatment, rats in the NIR and citalopram treatment groups showed significantly less immobility and higher swimming times than the stress group. Interestingly, the red treatment group did not show a significant effect. On the other hand, only citalopram and red laser treatment effected anxiety-like behavior during the elevated plus maze task. Further, red laser and citalopram treatments lowered blood cortisol, while all treatment modalities lowered blood glucose levels.
In a similar study, Salehpour et al (2017) used rats who had undergone a standard chronic mild stress procedure to create an animal model of depression.74 Following the 4-week procedure, rats were randomly divided to receive NIR transcranial laser therapy and others were assigned to receive citalopram. Other animals acted as controls. Laser therapy sessions consisted of irradiation over the prefrontal region with a 810nm NIR probe derived by GaAlAs diode laser (Mustang 2000+, Russia; output power of 240±5mW, 10Hz pulsed wave, average energy density of 1.2J/cm2 per each treatment). After a series of 12 treatments, rats underwent testing with the forced swim test to assess depressive behaviors. Both NIR therapy and citalopram significantly increased swim time and decreased immobility compared to the depressive group. Curiously, only citalopram significantly decreased blood cortisol levels.
Wu et al (2012) also tested pulsed light and an antidepressant in a rat model of depression.75 After undergoing various mild stressors for 5 weeks, rats assigned to the drug group received daily injections of fluoxetine and those assigned to the t-PBM underwent treatment 3 times a week for 2 mins each session. All treatment paradigms lasted for 3 weeks, with concurrent, ongoing chronic mild stress. t-PBM was delivered to dorsal surface of the head, between the eyes and ears, using an 810nm, with pulsed parameters of 100Hz and an average power density of 15mW/cm2. At the completion of 3 weeks of treatment, both the fluoxetine and t-PBM groups had significantly higher swimming and lower immobility counts than the untreated group. Additionally, there was no significant difference between the fluoxetine group and TLT group.
More recently, Salehpour et al (2018) studied the effects of PBM and coenzyme Q10, an essential cofactor in the electron transport chain.15,65 NIR t-PBM and coenzyme Q10, alone or in combination, were given for 5 days in a mouse model of depression. During t-PBM sessions, an NIR GaA1As laser (Thor Photomedicine, Chesham, UK), with a wavelength of 810nm and a 10-Hz pulsed wave frequency, was used to irradiate the dorsal surface between the eyes and ears. Sessions lasted 5s and delivered a dose of 33.3J/cm2. Irradiance was 6.66W/cm2. Following a course of treatment, behavioral testing was performed. During the forced swim test, both CoQ10 and t-PBM significantly reduced immobility time on their own. However, the combination of the two treatment modalities lowered the immobility time even further. CoQ10 and t-PBM, both alone and in combination, also significantly reduced immobility time, as tested by the tail suspension test.
Another study directly compared the therapeutic benefits of pulsed vs continuous irradiation, but in a mouse model of TBI.76 Four-hours post TBI, three groups of mice were given a single irradiation treatment for a total of 12 mins. Mice were assigned to treatment on either continuous wave, 10-Hz, or 100-Hz wave settings. Laser treatments were conducted using a 810-nm Ga-Al-As diode laser (DioDent Micro 810, HOYA ConBio, Fremont, CA), with a total fluence of 36 J/cm2. The device was positioned over the left frontoparietal cortex (the region of the induced lesion) and delivered a power density of 50mW/cm2. Behavioral testing, using the forced swim test and tail suspension test, was performed 1 day after TBI, and again at 4 weeks. After 28 days, mice treated with 10-Hz pulsed wave laser had significantly increased mobility in the forced swim test, compared to untreated mice. In the tail suspension test, both pulsed wave laser-treated groups had significantly decreased immobility compared to untreated mice. There was also a significant difference between the 10-Hz group and the continuous wave group.
In conclusion, all the animal studies reviewed used a transcranial t-PBM approach, but their methodologies varied greatly. For example, some studies used chronic, while other used acute exposure to t-PBM. They also used different animal models of depression or TBI and different settings for the NIR radiation (power, wavelength, areas stimulated). As such, it is difficult to compare or aggregate the results. Despite the limitations, these studies provide significant support for the potential antidepressant effect of t-PBM.
Clinical Trials Of t-PBM Treatment For Depression (See Table 2)
In an early study, 10 patients with major depression (9 with co-morbid anxiety, 7 with past history of substance abuse, 3 with co-morbid PTSD) received four 4-min NIR treatments in random order at EEG sites F3 and F4, as well as placebo treatments at the same sites, using an LED array (Marubeni America Corp, Santa Clara, CA).77 The treatment parameters were as follows: peak wavelength of 810nm with a full-width half maximum of 40nm, irradiance of 250mW/cm2, and total delivered fluence per site of 60J/cm2. Overall, the study found significantly improved HAM-D scores at 2 weeks, with attenuation of effect at 4 weeks. At the 2-week follow-up point, 10 patients were “improvers” (at least a 20% reduction in HAM-D), 4 out of 10 patients were “responders” (>50% reduction in HAM-D) and 4 out of the 10 patients achieved “remission,” (HAM-D <8). By 4 weeks, only 5 out of 10 patients were “improvers,” 2 were “responders,” and none were in “remission”. These results suggest that one set of treatments was enough to yield significant improvement in a relatively short timeframe (2 weeks), but was not enough to sustain robust effects after 1 month. Parallel results were also found for changes on the HAM-A, a measure of anxiety.
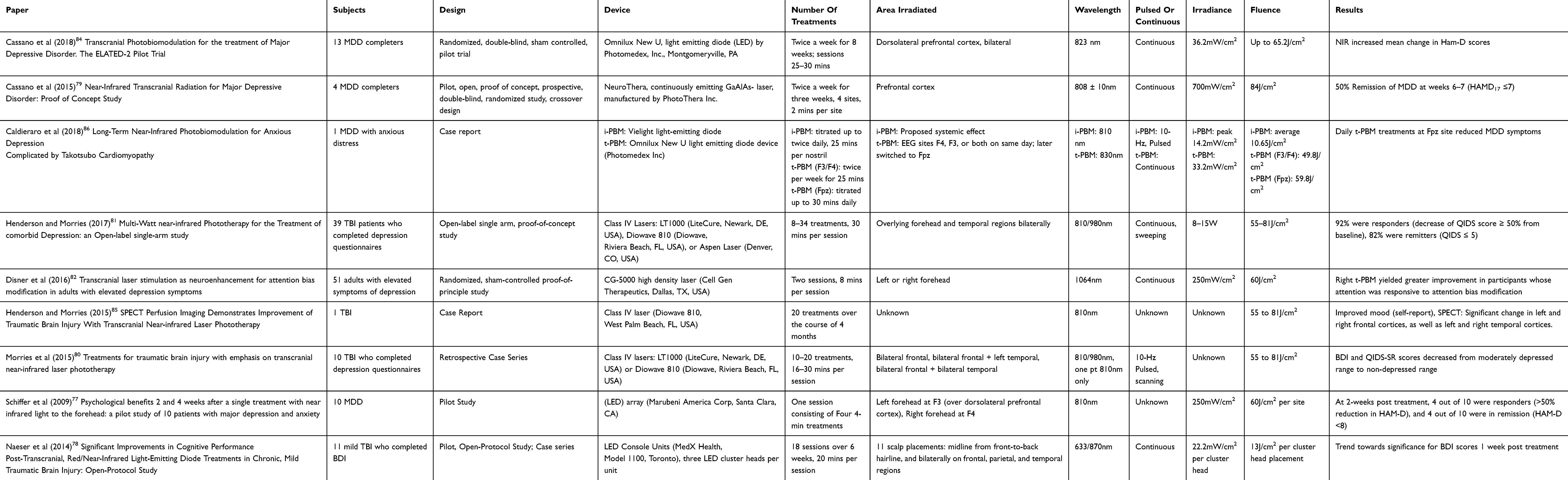 |
Table 2 All Available Clinical Research Studies And Case Reports That Utilized Transcranial Photobiomodulation, With Wavelengths In The Red And/Or Near-Infrared Range, For Treatment Of Depression |
Another study had a slightly longer follow-up period. In a pilot, open-protocol study of 11 participants with chronic, mild TBIs, 5 of the 10 participants were found to have moderate or severe depression scores on the Beck Depression Inventory (4 had PCL-C scores suggestive of PTSD, 3 had scores indicative of PTSD plus Depression).78 Each participant underwent 18 treatments (3 times/week) over the course of 6 weeks. During each session, an LED cluster head was applied for 10 mins to 11 scalp placements (midline from front-to-back hairline; bilaterally on frontal, parietal, and temporal areas) and one LED cluster was applied to the sole of the foot. In this paradigm, LED Console Units with three LED cluster heads each, were used (MedX Health, Model 1100, Toronto). Every LED cluster head contained 9 red diodes with wavelength of 633nm and 52 NIR diodes with wavelength of 870nm, as well as 22.2mW/cm2 power density and energy density of 13J/cm2. Of the 5 patients with BDI scores suggesting moderate-to-severe depression, 4 reported a reduced level of depression at 1 week post-LED treatment. Three of them continued to report reduction in symptoms at 1-month and 2-month follow-up visits. Similar to the prior study, 1 patient who had reported reduction in depression at 1 week and 1 month reverted back to severe depression at 2 months post-LED. These results suggest that a longer treatment course may lead to more sustained results.
In an open-pilot, proof of concept study, eight participants who met the criteria for at least moderate depression were enrolled. However, there were only four completers.79 Following a double-blind, sham-controlled model, subjects were randomized to 3 weeks of either NIR or sham, followed by crossover to 3 more weeks of the alternate treatment. Twice a week, subjects underwent treatment with a NeuroThera, continuously emitting GaAlAs-laser (PhotoThera Inc.) or the same device acting as a sham. Treatment involved irradiating the forehead bilaterally for 2 mins at 4 different sites. Parameters included a wavelength of 808 ± 10nm, irradiance of approximately 700mW/cm2, and a fluence of 84J/cm2. At the end of the study, 2 of the 4 participants achieved remission at weeks 6 and 7.
In a retrospective case series conducted by Morries et.al (2015), 10 patients with TBI (6 with co-morbid MDD) were enrolled to receive high-power NIR laser phototherapy with a Class IV laser.80 While the aim of this study was to target symptoms of TBI, over 90% of the patients complained of depression. Further, all subjects completed a baseline Quick Inventory of Depressive Symptomatology Self-Report (QIDS-SR) and seven completed the Beck Depression Inventory (BDI) before and after the course of treatment. Baseline scores fell in the moderate depression range. In this study, 6 participants received a single series of 10 treatments with the LT1000 Class IV laser (LiteCure, Newark, DE, USA; adjustable 10W NIR laser emitter with wavelengths of 810 and 980nm that can deliver continuous or pulsed light), 3 patients received a single series of 20 treatments with the LT1000 laser, and 1 patient underwent a series of 20 treatments with the Diowave 810-nm Class IV laser device (Diowave, Riviera Beach, FL, USA; up to 15W, wavelength of 810nm, can deliver continuous or pulsed NIR energy). Each treatment lasted 8–12 mins, depending on the subject, and fluence delivered to the skin ranged from 55 to 81J/cm2. The areas targeted for treatment included the bilateral frontal and temporal regions. Following the above-stated interventions, QIDS-SR and BDI scores significantly decreased to the non-depressed range.
A subsequent open-label, single-arm, proof-of-concept trial of 39 patients with TBI and co-morbid depression tested the effects of Multi-Watt t-PBM on depression.81 Each participant received NIR light therapy, applied to the forehead and temporal regions bilaterally, for a total of 30 mins per session. Depending upon individual improvement, subjects got anywhere from 8 to 34 treatments. (12 participants underwent 12 or fewer treatments, 27 had 13 or more treatments). The time course of treatments also varied, with 15 participants undergoing all treatments under 8 weeks and 6 completing the course in 4 weeks or less. Another factor increasing the variability in the study includes use of three different Class IV lasers [LT1000 (LiteCure, Newark, DE, USA), Diowave 810 (Diowave, Riviera Beach, FL, USA), or Aspen Laser (Denver, CO, USA)]. The power ranged from 8 to 15W and fluence delivered to the skin of patients ranged from 55 to 81J/cm2. To measure the effects of treatment on depressive symptoms, the Quick Inventory of Depression Symptomatology-Self Report (QIDS) was administered in all patients before and after. Overall, 92% of the patients responded to the treatment and 82% remitted from depression. Notably, patients who received ≥13 treatments had more significant results. Interestingly, some patients continued to show a response at 2, 6, 12, and 55 months follow-up points, indicating that the benefits were not transient.
The largest study to date had 45 total completers and data on 46 participants, all of whom came from a population of undergraduate students.82 The goal of this randomized, sham-controlled proof-of-principle study was to test the potential for transcranial laser stimulation to augment another type of intervention, attention bias modification (ABM). ABM is used to train individuals with a tendency towards negatively biased attention to shift their attention to more neutral or adaptive stimuli. The idea is that shifting attention away from negative attention bias may improve depressive symptoms.83 Therefore, in the above-mentioned study, participants with elevated depressive symptoms [based on Center for Epidemiologic Studies – Depression Scale (CES-D) scores] were randomized to undergo ABM training and augmentative t-PBM at the right forehead, left forehead, or sham. A repeat session of ABM and t-PBM was held 48 hrs later and CES-D scales were repeated at 1- and 2-week follow-ups. Each t-PBM treatment consisted of 8 consecutive minute-long applications, with 4 mins devoted to the medial region and 4 mins devoted to the lateral region of the forehead (left or right, depending on randomization). A CG-5000 high-density laser was used (Cell Gen Therapeutics, Dallas, TX, USA), with the following parameters: wavelength of 1064nm, irradiance of 250mW/cm2, and fluence of 60Joules/cm2. The authors found that CES-D scores decreased significantly each week. Further, for participants who were responsive to ABM, t-PBM applied to the right forehead only yielded greater reduction in depressive symptoms.
The ELATED-2 Pilot aimed to test the therapeutic benefit of t-PBM in patients with unipolar MDD.84 Twenty-one patients with at least moderate depression were randomized and 13 subjects completed 8 weeks of twice weekly t-PBM NIR treatment (or sham) with the Omnilux New U light-emitting diode (Photomedex, Inc., Montgomeryville, PA). During each session, light at a wavelength of 823nm was used to irradiate the dorsolateral prefrontal cortex at the F3 and F4 EEG placement sites, bilaterally. While sessions started off at 20 mins, the study clinician had the option to adjust the duration of light exposure after completion of weeks 3 and 5 to 25 and 30 mins. These adjustments increased the fluence from 40J/cm2 to 50J/cm2 and 60J/cm2, respectively. Compared to the sham group, those who underwent treatment with t-PBM had a significantly greater mean change in HAM-D17 score. Response and remission occurred in 50% of the subjects in the NIR arm. Comparatively, 27% of the sham group achieved response and 18% achieved remission.
In addition to the above-mentioned studies, there have been two case reports detailing the effects of longer-term repeated administrations of t-PBM on depressive symptoms. In the first, one male patient received 20 NIR treatments over the course of 4 months, using a class IV laser (Diowave 810, West Palm Beach, FL, USA; power density range 55 to 81 J/cm2).85 At baseline, this patient had a low mood and irritability, in addition to several other neurological and cognitive findings. Following treatment, depression, mood dysregulation, anxiety, and irritability improved. As part of his initial work up, the patient received a SPECT scan, which was repeated 2 months after completion of NIR treatments. In the post-treatment scan, areas of statistically significant change included the bilateral frontal cortices and the bilateral temporal cortices. In the second case report, a 76-year-old Caucasian female, who carried diagnoses of MDD with “anxious distress”, hypertrophic obstructive cardiomyopathy, and Takotsubo cardiomyopathy, underwent NIR t-PBM for a total of 31 months.86 Over the course of therapy, the patient performed weekly self-report assessments using the Quick Inventory of Depressive Symptomatology Self-Report version (QIDS-SR16) and the Anxiety Symptoms Questionnaire (ASQ). Interestingly, she received both intra-nasal PBM (i-PBM) and transcranial (t-PBM), alone and in combination at different points. Initially, she only underwent treatments with i-PBM (Vielight light-emitting diode, wavelength 810nm, peak irradiance, 14.2mW/cm2, average fluence 10.65J/cm2, 25 mins per nostril). The frequency of treatments was progressively increased from twice a week to twice daily. 22 months after starting i-PBM, t-PBM was added [Omnilux New U device (LED), at EEG sites F3, F4, or both, twice per week for 25 mins]. t-PBM parameters were wavelength of 830nm, irradiance of 33.2mW/cm2, and fluence of 49.8J/cm2. Five months later, the t-PBM treatment site was switched to Fpz and the length of sessions was increased to 30 mins. With these adjustments, fluence increased to 59.8J/cm2. The patient’s depressive symptoms only improved under the i-PBM plus t-PBM at site Fpz condition. Anxiety symptoms, on the other hand, steadily improved with the initiation of i-PBM, as well as the combination of i-PBM and t-PBM.
Comparison Of Animal And Clinical Studies
Several differences can be noted between the animal and clinical studies presented here. For one, almost all animal studies reviewed used laser devices. One used an infrared emitter and none of the eight studies used an LED device. Since rodent skulls are thinner than human skulls, NIR light can more easily penetrate the animal cortex and even subcortical structures.9 Therefore, the rodent and human studies may not be targeting the exact same cortical brain structures. Further, as is usually the case in initial pilot studies, the clinical trials were less well-controlled than the animal studies. In those reviewed earlier, several patient populations had co-morbid neuropsychiatric conditions, making it more difficult to measure antidepressant effects precisely. There was also some variability of the treatment paradigms (number of sessions, physical characteristics of the t-PBM devices) within the clinical trials themselves, complicating further a comparison.81,84 Lastly, the clinical studies used different measurements of depression (HAM-D, BDI, QIDS-SR, CES-D), making it challenging to compare patient populations as a whole.
Systemic PBM Clinical Trials
Although this is outside of the scope of this review, there is some evidence that PBM applied peripherally, not just transcranially, may have an effect in attenuating depressive symptoms. The studies reported are small and include a variety of treatment strategies.87–90 Most importantly, there is no clear mechanism proposed explaining the effect of peripheral PBM on the brain.
Safety And Tolerability
In the studies reviewed earlier, t-PBM was found to be relatively safe and well-tolerated. Of note, not all trials reported on adverse effects and safety data were frequently only assessed in the short term. Nonetheless, very few adverse effects were reported. Headaches were reported in three separate studies.81,84,86 Other potential side effects related to the active treatment mode were fatigue, localized skin warming, irritability, insomnia, illusions (i.e., “seeing vivid colors” or “tasting from an ashtray”), and abdominal bloating.81,84 Even larger studies of t-PBM in post-stroke patients, including a pooled sample of 1410 subjects, showed no significant difference in serious adverse effects or mortality between treatment and control groups.91–94
Discussion Of Optimal t-PBM Parameters
In this paper, we have reviewed the relevant basic and clinical studies on t-PBM for depression. Overall, the data are intriguing and open the door to a new treatment modality that may benefit a large cohort of patients. Though this field is promising, the clinical applications of this modality are still in the early stages and many questions remain.
For one, is an LED device sufficient for the delivery of therapeutic PBM? Lasers are currently the gold standard, but as Heiskanen and Hamblin (2018) have pointed out, LEDs cover more area at once, are less expensive, and are more readily used at home.95 In the first section of this paper, we discussed the relative lack of penetrance of light energy when delivered via LED, compared to lasers.12 One of the main reasons for this is likely coherence. Lasers have greater coherence of light compared to LED, by definition. Some have argued for the importance of coherent light, particularly when it comes to penetrating bulk tissue and providing therapeutic benefit.96 Others have shown that coherence of laser light is partially lost when fluid flows through tissue.97
There have been some clinical studies comparing lasers and LED light sources directly, but they involve NIR administration to other tissues and do not address the LED brain penetration concerns. In one small randomized, placebo-controlled, double-blind cross-over study, eight volleyball players had their rectus femoris muscle pre-treated with either an active LED cluster-probe (660/850 nm, 10/30 mW), a single-diode laser (810-nm 200-mW), or a placebo cluster-probe.98 After a standardized exercise test, it was found that the active LED group had significantly decreased creatinine kinase levels compared to the two other groups. Notably, the spot size and total energy delivered per muscle differed between the two active groups. Therefore, little can be concluded from this study about the effectiveness of laser vs LED t-PBM. On the other hand, in a near-infrared photoimmunotherapy study comparing LED and lasers in cell cultures and grafted tumors, lasers yielded better therapeutic results, in both in vitro and in vivo models.99 Though these studies are helpful, they do not involve transcranial application of PBM or the population of interest. In the clinical studies and case reports reviewed earlier, 4 out of 10 used LEDs. While it is tempting to generalize the clinical results of LEDs and lasers based on the current literature, there are too many differences between the patient populations, treatment paradigms, device settings, and brain regions targeted across these studies to come to definitive conclusions at this time. Since lasers remain the gold standard, we believe that future studies are needed to first prove conclusively the effectiveness of laser devices and then to secondly compare directly lasers and LED devices in the same patient population. If LED devices do prove to be effective, we must also consider a different mechanism of action, since, as discussed, LEDs might not provide sufficient irradiance in transcranial administration for the postulated mitochondrial enhancement in brain cells.
Another key parameter of t-PBM is whether the laser light is administered as continuous (CW) or pulsed wave (PW). While the animal and clinical literature presented here differ in this respect, most of the current data involved CW administration. Only one basic research study76 and one case report86 utilized both modalities. This begs the question: does it matter which mode is used and is one better than the other? While a complete analysis of this issue is beyond the scope of this review, there are a few key points to consider. In their 2010 review, Hashmi et al argue that pulsed lasers cause less heating, which is beneficial when higher power is needed to reach deeper layers of tissue.100 Because there is a potential ability to use higher power and cause less collateral damage, pulsing could potentially be safer and more effective, but this is a theoretical insight that would need to be proven in head-to-head studies. The few studies comparing the two modalities directly seem to suggest an advantage for PW. A study on laser t-PBM in a stroke model of rabbits showed improvement at 6 hrs post-embolization with PW, but not CW.101 On the other hand, when treatment was applied at 12 hrs post-embolization, no statistically significant improvement was seen with either setting. In an earlier study using the same rabbits model for stroke, PW leads to a greater increase in ATP production post-embolization than CW.102 Further, in a study comparing both power densities and frequencies (continuous and pulsed) in a rat model, PW produced much less heating and led to no tissue damage at the highest power tested (750mW/cm2).103 In contrast, both neurological deficits and histopathological damage were seen when CW was used at the same power. The authors attributed the damage to production of heat. Interestingly, some have shown better outcomes when the two are combined.104 Overall, PW t-PBM may be safer and more effective, but the most appropriate frequency of pulsing remains up for debate,100 which will require more exploratory studies with PW t-PBM.
As can be seen in the study summaries presented in Tables 1 and 2, both preclinical and clinical studies have used a wide spectrum of t-PBM parameters. While most of them appear to be safe, the studies are difficult to compare in terms of efficacy, and we can only speculate what the optimal treatment parameters for depression might be. To review, the penetration of t-PBM is greatly limited by hair, scalp, skull, and other overlying soft tissue. Skin color likely effects the level of attenuation as well,105 though only one of the trials accounted for skin tone.82 Despite these limitations, treatment may be optimized by using a laser device, NIR light in the 808–835nm range, higher power, and possibly pulsed wave (which may reduce brain heating for a given maximal irradiance). Of course, this must be balanced with the safety and tolerability of the treatment. In their study of 39 patients, Henderson and Morries (2017) utilized a power range of 8–15W and reported few adverse events, demonstrating that higher powers can be used safely.81 On the other hand, their earlier study demonstrated a more substantial temperature change in the brain with higher power (15W).12 The most effective power for treatment of depression is currently unknown, given the small breadth of clinical trials. Additionally, in terms of targetable regions, we may be limited to the prefrontal cortex, as patients are unlikely to comply with shaving their hair for the duration of treatment (which would be required for targeting temporal or parietal brain areas).
Conclusion
In conclusion, the studies reviewed here provide strong evidence for the mechanism of t-PBM (increasing mitochondrial energy production and increasing regional blood flow). The downstream effects of increased ATP production include not only increased cellular energy but also potentially increases in intercellular signaling.106
The animal and human studies reviewed are supportive of a likely t-PBM effect on depression. These studies have significant limitations. Both animal and human studies have used a variety of t-PBM parameters and settings. For example, studies used different radiation power, different wavelengths, continuous vs pulsed light, acute vs chronic treatment, and irradiation of the entire cortex vs prefrontal area. It is possible that a specific intensity of t-PBM radiation may be required for clinical efficacy; this may explain inconsistencies in the literature. Only one study controlled for skin color, although differences in skin color can theoretically impact level of light absorption and the eventual dose delivered to the brain.82 However, despite these limitations, the data support a likely effect of t-PBM in MDD and highlights the need for large confirmatory studies for t-PBM as a novel, likely safe and easy-to-administer antidepressant treatment. A study comparing the different t-PBM modalities to clarify the optimal antidepressant parameters is the critical next step in the development of this technology.
Disclosure
Over the last five years, DVI has received consulting fees from Axsome, Alkermes, Centers of Psychiatric Excellence, MyndAnalytics (CNS Response), Jazz, Lundbeck, Precision Neuroscience, Otsuka, and Sundovion; and has received research support (through his academic institutions) from Alkermes, Astra Zeneca, Brainsway, LiteCure, Neosync, Roche, and Shire. The authors report no other conflicts of interest in this work.
References
1. Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289(23):3095–3105. doi:10.1001/jama.289.23.3095
2. Ferrari AJ, Charlson FJ, Norman RE, et al. Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS Med. 2013;10(11):e1001547. doi:10.1371/journal.pmed.1001547
3. Rush AJ, Warden D, Wisniewski SR, et al. STAR*D: revising conventional wisdom. CNS Drugs. 2009;23(8):627–647. doi:10.2165/00023210-200923080-00001
4. Rosa MA, Lisanby SH. Somatic treatments for mood disorders. Neuropsychopharmacology. 2012;37(1):102–116. doi:10.1038/npp.2011.225
5. Hamblin MR. Shining light on the head: photobiomodulation for brain disorders. BBA Clin. 2016;6:113–124. doi:10.1016/j.bbacli.2016.09.002
6. Young AE, Germon TJ, Barnett NJ, Manara AR, Nelson RJ. Behaviour of near-infrared light in the adult human head: implications for clinical near-infrared spectroscopy. Br J Anaesth. 2000;84(1):38–42. doi:10.1093/oxfordjournals.bja.a013379
7. Henderson TA, Morries LD. Near-infrared photonic energy penetration—principles and practice. In: Hamblin MR, Ying-Ying H, editors. Photobiomodulation in the Brain. London: Elseveir; 2019:67–88.
8. Jagdeo JR, Adams LE, Brody NI, Siegel DM. Transcranial red and near infrared light transmission in a cadaveric model. PLoS One. 2012;7(10):e47460. doi:10.1371/journal.pone.0047460
9. Lapchak PA, Boitano PD, Butte PV, et al. Transcranial Near-Infrared Laser Transmission (NILT) Profiles (800 nm): systematic Comparison in Four Common Research Species. PLoS One. 2015;10(6):e0127580. doi:10.1371/journal.pone.0127580
10. Tedford CE, DeLapp S, Jacques S, Anders J. Quantitative analysis of transcranial and intraparenchymal light penetration in human cadaver brain tissue. Lasers Surg Med. 2015;47(4):312–322. doi:10.1002/lsm.v47.4
11. Stolik S, Delgado JA, Pèrez A, Anasagasti L. Measurement of the penetration depths of red and near infrared light in human “ex vivo” tissues. J Photochem Photobiol B. 2000;57(2–3):90–93. doi:10.1016/S1011-1344(00)00082-8
12. Henderson TA, Morries LD. Near-infrared photonic energy penetration: can infrared phototherapy effectively reach the human brain? Neuropsychiatr Dis Treat. 2015;11:2191–2208. doi:10.2147/NDT
13. Yue L, Humayun MS. Monte Carlo analysis of the enhanced transcranial penetration using distributed near-infrared emitter array. J Biomed Opt. 2015;20(8):088001. doi:10.1117/1.JBO.20.8.088001
14. Pitzschke A, Lovisa B, Seydoux O, et al. Red and NIR light dosimetry in the human deep brain. Phys Med Biol. 2015;60(7):2921–2937. doi:10.1088/0031-9155/60/7/2921
15. van der Bliek AM, Sedensky MM, Morgan PG. Cell Biology of the Mitochondrion. Genetics. 2017;207:843–871. doi:10.1534/genetics.117.300262
16. Rezin GT, Cardoso MR, Gonçalves CL, et al. Inhibition of mitochondrial respiratory chain in brain of rats subjected to an experimental model of depression. Neurochem Int. 2008;53(6–8):395–400. doi:10.1016/j.neuint.2008.09.012
17. Shumake J, Gonzalez-Lima F. Brain Systems Underlying Susceptibility to Helplessness and Depression. Behav Cogn Neurosci Rev. 2003;2(3):198–221. doi:10.1177/1534582303259057
18. Harper DG, Jensen JE, Renshaw PR. 31P MRS in psychiatric disorders. In: Bottomley PA, Griffiths JR, editors. Handbook of Magnetic Resonance Spectroscopy in Vivo. West Sussex, UK: Wiley; 2016:927–946.
19. Bessman SP. The creatine phosphate energy shuttle–the molecular asymmetry of a “pool”. Anal Biochem. 1987;161(2):519–523. doi:10.1016/0003-2697(87)90483-0
20. Harper DG, Joe EB, Jensen JE, Ravichandran C, Forester BP. Brain levels of high-energy phosphate metabolites and executive function in geriatric depression. Int J Geriatr Psychiatry. 2016;31(11):1241–1249. doi:10.1002/gps.v31.11
21. Renshaw PF, Parow AM, Hirashima F, et al. Multinuclear magnetic resonance spectroscopy studies of brain purines in major depression. Am J Psychiatry. 2001;158(12):2048–2055. doi:10.1176/appi.ajp.158.12.2048
22. Iosifescu DV, Bolo NR, Nierenberg AA, Jensen JE, Fava M, Renshaw PF. Brain bioenergetics and response to triiodothyronine augmentation in major depressive disorder. Biol Psychiatry. 2008;63(12):1127–1134. doi:10.1016/j.biopsych.2007.11.020
23. Drevets WC, Bogers W, Raichle ME. Functional anatomical correlates of antidepressant drug treatment assessed using PET measures of regional glucose metabolism. Eur Neuropsychopharmacol. 2002;12(6):527–544. doi:10.1016/S0924-977X(02)00102-5
24. Mayberg HS, Brannan SK, Tekell JL. Regional metabolic effects of fluoxetine in major depression: serial changes and relationship to clinical response. Biol Psychiatry. 2000;48(8):830. doi:10.1016/S0006-3223(00)01036-2
25. Karabatsiakis A, Böck C, Salinas-Manrique J, et al. Mitochondrial respiration in peripheral blood mononuclear cells correlates with depressive subsymptoms and severity of major depression. Transl Psychiatry. 2014;4(6):e397. doi:10.1038/tp.2014.44
26. Hroudová J, Fišar Z, Kitzlerová E, Zvěřová M, Raboch J. Mitochondrial respiration in blood platelets of depressive patients. Mitochondrion. 2013;13(6):795–800. doi:10.1016/j.mito.2013.05.005
27. Gardner A, Johansson A, Wibom R, et al. Alterations of mitochondrial function and correlations with personality traits in selected major depressive disorder patients. J Affect Disord. 2003;76(1–3):55–68. doi:10.1016/S0165-0327(02)00067-8
28. Villa RF, Ferrari F, Gorini A, Brunello N, Tascedda F. Effect of desipramine and fluoxetine on energy metabolism of cerebral mitochondria. Neuroscience. 2016;330:326–334. doi:10.1016/j.neuroscience.2016.05.051
29. Karu T, Afanas`eva NI. Cytochrome c oxidase acts as a primary photoacceptor in cell cultures subjected to visible and near IR laser irradiation. Dokl Biol Sci. 1995.
30. Pastore D, Greco M, Passarella S. Specific helium-neon laser sensitivity of the purified cytochrome c oxidase. Int J Radiat Biol. 2000;76(6):863–870. doi:10.1080/09553000050029020
31. Salehpour F, Ahmadian N, Rasta SH, Farhoudi M, Karimi P, Sadigh-Eteghad S. Transcranial low-level laser therapy improves brain mitochondrial function and cognitive impairment in D-galactose-induced aging mice. Neurobiol Aging. 2017;58:140–150. doi:10.1016/j.neurobiolaging.2017.06.025
32. Wang X, Tian F, Reddy DD, et al. Up-regulation of cerebral cytochrome-c-oxidase and hemodynamics by transcranial infrared laser stimulation: A broadband near-infrared spectroscopy study. J Cereb Blood Flow Metab. 2017;37(12):3789–3802. doi:10.1177/0271678X17691783
33. Gkotsi D, Begum R, Salt T, et al. Recharging mitochondrial batteries in old eyes. Near infra-red increases ATP. Exp Eye Res. 2014;122:50–53. doi:10.1016/j.exer.2014.02.023
34. Silveira PC, Streck EL, Pinho RA. Evaluation of mitochondrial respiratory chain activity in wound healing by low-level laser therapy. J Photochem Photobiol B. 2007;86(3):279–282. doi:10.1016/j.jphotobiol.2006.10.002
35. Silveira PC, Silva LA, Fraga DB, Freitas TP, Streck EL, Pinho R. Evaluation of mitochondrial respiratory chain activity in muscle healing by low-level laser therapy. J Photochem Photobiol B. 2009;95(2):89–92. doi:10.1016/j.jphotobiol.2009.01.004
36. Masha RT, Houreld NN, Abrahamse H. Low-Intensity Laser Irradiation at 660 nm Stimulates Transcription of Genes Involved in the Electron Transport Chain. Photomed Laser Surg. 2013;31(2):47–53. doi:10.1089/pho.2012.3369
37. Amaroli A, Ravera S, Parker S, Panfoli I, Benedicenti A, Benedicenti S. An 808-nm Diode Laser with a Flat-Top Handpiece Positively Photobiomodulates Mitochondria Activities. Photomed Laser Surg. 2016;34(11):564–571. doi:10.1089/pho.2015.4035
38. Giuliani A, Lorenzini L, Alessandri M, et al. In vitro exposure to very low-level laser modifies expression level of extracellular matrix protein RNAs and mitochondria dynamics in mouse embryonic fibroblasts. BMC Complement Altern Med. 2015;15:78. doi:10.1186/s12906-015-0593-8
39. Mochizuki-Oda N, Kataoka Y, Cui Y, Yamada H, Heya M, Awazu K. Effects of near-infra-red laser irradiation on adenosine triphosphate and adenosine diphosphate contents of rat brain tissue. Neurosci Lett. 2002;323(3):207–210. doi:10.1016/S0304-3940(02)00159-3
40. Begum R, Calaza K, Kam JH, Salt TE, Hogg C, Jeffery G. Near-infrared light increases ATP, extends lifespan and improves mobility in aged Drosophila melanogaster. Biol Lett. 2015;11(3):20150073. doi:10.1098/rsbl.2015.0073
41. Rojas JC, Bruchey AK, Gonzalez-Lima F. Low-level light therapy improves cortical metabolic capacity and memory retention. J Alzheimers Dis. 2012;32(3):741–752. doi:10.3233/JAD-2012-120817
42. Tian F, Hase SN, Gonzalez-Lima F, Liu H. Transcranial laser stimulation improves human cerebral oxygenation. Lasers Surg Med. 2016;48(4):343–349. doi:10.1002/lsm.22471
43. Yu Z, Liu N, Zhao J, et al. Near infrared radiation rescues mitochondrial dysfunction in cortical neurons after oxygen-glucose deprivation. Metab Brain Dis. 2015;30(2):491–496. doi:10.1007/s11011-014-9515-6
44. Xu Z, Guo X, Yang Y, et al. Low-level laser irradiation improves depression-like behaviors in mice. Mol Neurobiol. 2017;54(6):4551–4559. doi:10.1007/s12035-016-9983-2
45. Ferraresi C, Kaippert B, Avci P, et al. Low-level laser (light) therapy increases mitochondrial membrane potential and ATP synthesis in C2C12 myotubes with a peak response at 3–6 h. Photochem Photobiol. 2015;91(2):411–416. doi:10.1111/php.2015.91.issue-2
46. Mintzopoulos D, Gillis TE, Tedford CE, Kaufman MJ. Effects of near-infrared light on cerebral bioenergetics measured with phosphorus magnetic resonance spectroscopy. Photomed Laser Surg. 2017;35(8):395–400. doi:10.1089/pho.2016.4238
47. Chung H, Dai T, Sharma SK, Huang YY, Carroll JD, Hamblin MR. The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng. 2012;40(2):516–533. doi:10.1007/s10439-011-0454-7
48. Sanderson TH, Wider JM, Lee I, et al. Inhibitory modulation of cytochrome c oxidase activity with specific near-infrared light wavelengths attenuates brain ischemia/reperfusion injury [published correction appears in Sci Rep. 2018 Apr 25;8(1):6729]. Sci Rep. 2018;8(1):3481. doi:10.1038/s41598-018-21869-x
49. Oron U, Ilic S, De Taboada L, Streeter J. Ga-As (808 nm) laser irradiation enhances ATP production in human neuronal cells in culture. Photomed Laser Surg. 2007;25(3):180–182. doi:10.1089/pho.2007.2064
50. Wu Q, Xuan W, Ando T, et al. Low-level laser therapy for closed-head traumatic brain injury in mice: effect of different wavelengths. Lasers Surg Med. 2012;44(3):218–226. doi:10.1002/lsm.v44.3
51. Wang Y, Huang YY, Wang Y, Lyu P, Hamblin MR. Photobiomodulation of human adipose-derived stem cells using 810nm and 980nm lasers operates via different mechanisms of action. Biochim Biophys Acta Gen Subj. 2017;1861(2):441–449. doi:10.1016/j.bbagen.2016.10.008
52. Uozumi Y, Nawashiro H, Sato S, Kawauchi S, Shima K, Kikuchi M. Targeted increase in cerebral blood flow by transcranial near-infrared laser irradiation. Lasers Surg Med. 2010;42(6):566–576. doi:10.1002/lsm.v42:6
53. Nawashiro H, Wada K, Nakai K, Sato S. Focal increase in cerebral blood flow after treatment with near-infrared light to the forehead in a patient in a persistent vegetative state. Photomed Laser Surg. 2012;30(4):231–233. doi:10.1089/pho.2011.3044
54. Salgado AS, Zângaro RA, Parreira RB, Kerppers II. The effects of transcranial LED therapy (TCLT) on cerebral blood flow in the elderly women. Lasers Med Sci. 2015;30(1):339–346. doi:10.1007/s10103-014-1669-2
55. Byrne AM, Bouchier-Hayes DJ, Harmey JH. Angiogenic and cell survival functions of Vascular Endothelial Growth Factor (VEGF). J Cell Mol Med. 2005;9(4):777–794. doi:10.1111/jcmm.2005.9.issue-4
56. Dias FJ, Issa JP, Barbosa AP, de Vasconcelos PB, Watanabe IS, Mizusakiiyomasa M. Effects of low-level laser irradiation in ultrastructural morphology, and immunoexpression of VEGF and VEGFR-2 of rat masseter muscle. Micron. 2012;43(2–3):237–244. doi:10.1016/j.micron.2011.08.005
57. Hamblin MR. The role of nitric oxide in low level light therapy.
58. Moreno J, Gaspar E, López-Bello G, et al. Increase in nitric oxide levels and mitochondrial membrane potential in platelets of untreated patients with major depression. Psychiatry Res. 2013;209(3):447–452. doi:10.1016/j.psychres.2012.12.024
59. Zhang R, Mio Y, Pratt PF, et al. Near infrared light protects cardiomyocytes from hypoxia and reoxygenation injury by a nitric oxide dependent mechanism. J Mol Cell Cardiol. 2009;46(1):4–14. doi:10.1016/j.yjmcc.2008.09.707
60. Keszler A, Brandal G, Baumgardt S, et al. Far red/near infrared light-induced protection against cardiac ischemia and reperfusion injury remains intact under diabetic conditions and is independent of nitric oxide synthase. Front Physiol. 2014;5:305. doi:10.3389/fphys.2014.00305
61. Sarandol A, Sarandol E, Eker SS, Erdinc S, Vatansever E, Kirli S. Major depressive disorder is accompanied with oxidative stress: short-term antidepressant treatment does not alter oxidative–antioxidative systems. Hum Psychopharmacol. 2007;22(2):67–73. doi:10.1002/(ISSN)1099-1077
62. Chludzińska L, Ananicz E, Jarosławska A, Komorowska M. Near-infrared radiation protects the red cell membrane against oxidation. Blood Cells Mol Dis. 2005;35(1):74–79. doi:10.1016/j.bcmd.2005.04.003
63. Huang YY, Nagata K, Tedford CE, McCarthy T, Hamblin MR. Low-level laser therapy (LLLT) reduces oxidative stress in primary cortical neurons in vitro. J Biophotonics. 2013;6(10):829–838. doi:10.1002/jbio.201200157
64. Salehpour F, Farajdokht F, Erfani M, et al. Transcranial near-infrared photobiomodulation attenuates memory impairment and hippocampal oxidative stress in sleep-deprived mice. Brain Res. 2018;1682:36–43. doi:10.1016/j.brainres.2017.12.040
65. Salehpour F, Farajdokht F, Cassano P, et al. Near-infrared photobiomodulation combined with coenzyme Q10 for depression in a mouse model of restraint stress: reduction in oxidative stress, neuroinflammation, and apoptosis. Brain Res Bull. 2019;114:213–222. doi:10.1016/j.brainresbull.2018.10.010
66. Yin K, Zhu R, Wang S, Zhao RC. Low-level laser effect on proliferation, migration, and antiapoptosis of mesenchymal stem cells. Stem Cells Dev. 2017;26(10):762–775. doi:10.1089/scd.2016.0332
67. Wang R, Dong Y, Lu Y, Zhang W, Brann DW, Zhang Q. Photobiomodulation for Global Cerebral Ischemia: targeting Mitochondrial Dynamics and Functions. Mol Neurobiol. 2019;56(3):1852–1869. doi:10.1007/s12035-018-1191-9
68. Yang L, Dong Y, Wu C, et al. Photobiomodulation preconditioning prevents cognitive impairment in a neonatal rat model of hypoxia‐ischemia. J Biophotonics. 2019;12(6):e201800359. doi:10.1002/jbio.2019.12.issue-6
69. Tanaka Y, Akiyoshi J, Kawahara Y, et al. Infrared radiation has potential antidepressant and anxiolytic effects in animal model of depression and anxiety. Brain Stimul. 2011;4(2):71–76. doi:10.1016/j.brs.2010.04.001
70. Xuan W, Agrawal T, Huang L, Gupta GK, Hamblin MR. Low-level laser therapy for traumatic brain injury in mice increases brain derived neurotrophic factor (BDNF) and synaptogenesis. J Biophotonics. 2015;8(6):502–511. doi:10.1002/jbio.201400069
71. Yang L, Tucker D, Dong Y, et al. Photobiomodulation therapy promotes neurogenesis by improving post-stroke local microenvironment and stimulating neuroprogenitor cells. Exp Neurol. 2018;299(Pt A):86–96. doi:10.1016/j.expneurol.2017.10.013
72. Mohammed HS. Transcranial low-level infrared laser irradiation ameliorates depression induced by reserpine in rats. Lasers Med Sci. 2016;31(8):1651–1656. doi:10.1007/s10103-016-2033-5
73. Salehpour F, Rasta SH, Mohaddes G, Sadigh-Eteghad S, Salarirad S. Therapeutic effects of 10‐HzPulsed wave lasers in rat depression model: A comparison between near‐infrared and red wavelengths. Lasers Surg Med. 2016;48(7):695–705. doi:10.1002/lsm.v48.7
74. Salehpour F, Rasta SH, Mohaddes G, Sadigh-Eteghad S, Salarirad S. A comparison between antidepressant effects of transcranial near-infrared laser and citalopram in a rat model of depression. Clin Transl Neurophotonics. 2017;10050. Available from: https://www.spiedigitallibrary.org/conference-proceedings-of-spie/10050/100500G/A-comparison-between-antidepressant-effects-of-transcranial-near-infrared-laser/10.1117/12.2251598.full?SSO=1.
75. Wu X, Alberico SL, Moges H, De Taboada L, Tedford CE. Pulsed light irradiation improves behavioral outcome in a rat model of chronic mild stress. Lasers Surg Med. 2012;44(3):227–232. doi:10.1002/lsm.v44.3
76. Ando T, Xuan W, Xu T, et al. Comparison of therapeutic effects between pulsed and continuous wave 810-nm wavelength laser irradiation for traumatic brain injury in mice. PLoS One. 2011;6(10). doi:10.1371/journal.pone.0026212.
77. Schiffer F, Johnston AL, Ravichandran C, et al. Psychological benefits 2 and 4 weeks after a single treatment with near infrared light to the forehead: a pilot study of 10 patients with major depression and anxiety. Behav Brain Funct. 2009;5:46. doi:10.1186/1744-9081-5-46
78. Naeser MA, Zafonte R, Krengel MH, et al. Significant improvements in cognitive performance post-transcranial, red/near-infrared light-emitting diode treatments in chronic, mild traumatic brain injury: open-protocol study. J Neurotrauma. 2014;31(11):1008–1017. doi:10.1089/neu.2013.3244
79. Cassano P, Cusin C, Mischoulon D, et al. Near-Infrared Transcranial Radiation for Major Depressive Disorder: proof of Concept Study. Psychiatry J. 2015;2015:352979. doi:10.1155/2015/352979
80. Morries LD, Cassano P, Henderson TA. Treatments for traumatic brain injury with emphasis on transcranial near-infrared laser phototherapy. Neuropsychiatr Dis Treat. 2015;11:2159–2175. doi:10.2147/NDT.S65809
81. Henderson TA, Morries LD. Multi-watt near-infrared phototherapy for the treatment of comorbid depression: an open-label single-arm study. Front Psychiatry. 2017;8:187. doi:10.3389/fpsyt.2017.00187
82. Disner SG, Beevers CG, Gonzalez-Lima F. Transcranial Laser Stimulation as Neuroenhancement for Attention Bias Modification in Adults with Elevated Depression Symptoms. Brain Stimul. 2016;9(5):780–787. doi:10.1016/j.brs.2016.05.009
83. Yang W, Ding Z, Dai T, Peng F, Zhang JX. Attention Bias Modification training in individuals with depressive symptoms: A randomized controlled trial. J Behav Ther Exp Psychiatry. 2014;49:101–111. doi:10.1016/j.jbtep.2014.08.005
84. Cassano P, Petrie SR, Mischoulon D, et al. Transcranial Photobiomodulation for the Treatment of Major Depressive Disorder. The ELATED-2 Pilot Trial. Photomed Laser Surg. 2018;36:12. doi:10.1089/pho.2018.4490
85. Henderson TA, Morries LD. SPECT perfusion imaging demonstrates improvement of traumatic brain injury with transcranial near-infrared laser phototherapy. Adv Mind Body Med. 2015;29(4):27–33.
86. Caldieraro MA, Sani G, Bui E, Cassano P. Long-Term Near-Infrared Photobiomodulation for Anxious Depression Complicated by Takotsubo Cardiomyopathy. J Clin Psychopharmacol. 2018;38(3):268–270. doi:10.1097/JCP.0000000000000883
87. Zhang B, Wenyou M, Baoting Z, Shuling L. A control study of clinical therapeutic effects of laser acupuncture on depressive neurosis. World J Acupuncture Moxibustion. 1996;6(2):12–17.
88. Quah-Smith JI, Tang WM, Russell J. Laser acupuncture for mild to moderate depression in a primary care setting–a randomised controlled trial. Acupunct Med. 2005;23(3):103–111. doi:10.1136/aim.23.3.103
89. Quah-Smith I, Smith C, Crawford JD, Russell J. Laser acupuncture for depression: a randomised double blind controlled trial using low intensity laser intervention. J Affect Disord. 2013;148(2–3):179–187. doi:10.1016/j.jad.2012.11.058
90. Gabel CP, Petrie SR, Mischoulon D, et al. A case control series for the effect of photobiomodulation in patients with low back pain and concurrent depression. Laser Ther. 2018;27(3):167–173. doi:10.5978/islsm.27_18-OR-18
91. Caldieraro MA, Cassano P. Transcranial and systemic photobiomodulation for major depressive disorder: A systematic review of efficacy, tolerability and biological mechanisms. J Affect Disord. 2019;243(15):262–273. doi:10.1016/j.jad.2018.09.048
92. Huisa BN, Stemer AB, Walker MG, Rapp K, Meyer BC, Zivin JA. Transcranial laser therapy for acute ischemic stroke: a pooled analysis of NEST-1 and NEST-2. Int J Stroke. 2013;8(5):315–320. doi:10.1111/j.1747-4949.2011.00754.x
93. Lampl Y, Zivin JA, Fisher M, et al. Infrared laser therapy for ischemic stroke: a new treatment strategy. Stroke. 2007;38(6):1843–1849. doi:10.1161/STROKEAHA.106.478230
94. Hacke W, Schellinger PD, Albers GW. Transcranial laser therapy in acute stroke treatment: results of neurothera effectiveness and safety trial 3, a phase III clinical end point device trial. Stroke. 2014;45(11):3187–3193. doi:10.1161/STROKEAHA.114.005795
95. Heiskanen V, Hamblin MR. Photobiomodulation: lasers vs light emitting diodes? Photochem Photobiol Sci. 2018;17(8):1003–1017. doi:10.1039/C8PP00176F
96. Hode L. The importance of the coherency. Photomed Laser Surg. 2005;23(4):431–434. doi:10.1089/pho.2005.23.431
97. Fixler D, Duadi H, Ankri R, Zalevsky Z. Determination of coherence length in biological tissues. Lasers Surg Med. 2011;43(4):339–343. doi:10.1002/lsm.21047
98. Leal Junior EC, Lopes-Martins RA, Baroni BM, et al. Comparison between single-diode low-level laser therapy (LLLT) and LED multi-diode (cluster) therapy (LEDT) applications before high-intensity exercise. Photomed Laser Surg. 2009;27(4):617–623. doi:10.1089/pho.2008.2350
99. Sato K, Watanabe R, Hanaoka H, Nakajima T, Choyke PL, Kobayashi H. Comparative effectiveness of light emitting diodes (LEDs) and Lasers in near infrared photoimmunotherapy. Oncotarget. 2016;7(12):14324–14335. doi:10.18632/oncotarget.v7i12
100. Hashmi JT, Huang YY, Sharma SK, et al. Effect of pulsing in low-level light therapy. Lasers Surg Med. 2010;42(6):450–466. doi:10.1002/lsm.20950
101. Lapchak PA, Salgado KF, Chao CH, Zivin JA. Transcranial near-infrared light therapy improves motor function following embolic strokes in rabbits: an extended therapeutic window study using continuous and pulsed frequency delivery modes. Neuroscience. 2007;148(4):907–914. doi:10.1016/j.neuroscience.2007.07.002
102. Lapchak PA, De Taboada L. Transcranial near infrared laser treatment (NILT) increases cortical adenosine-5ʹ-triphosphate (ATP) content following embolic strokes in rabbits. Brain Res. 2010;1306:100–105. doi:10.1016/j.brainres.2009.10.022
103. Ilic S, Leichliter S, Streeter J, Oron A, DeTaboada L, Oron U. Effects of Power Densities, Continuous and Pulse Frequencies, and Number of Sessions of Low-Level Laser Therapy on Intact Rat Brain. Photomed Laser Surg. 2006;24(4):458–466. doi:10.1089/pho.2006.24.458
104. Gigo-Benato D, Geuna S, de Castro Rodrigues A, et al. Low-power laser biostimulation enhances nerve repair after end-to-side neurorrhaphy: a double-blind randomized study in the rat median nerve model. Lasers Med Sci. 2004;19(1):57–65. doi:10.1007/s10103-004-0300-3
105. Brondon P, Stadler I, Lanzafame RJ. Pulsing influences photoradiation outcomes in cell culture. Lasers Surg Med. 2009;41(3):222–226. doi:10.1002/lsm.v41:3
106. Karu T. Mitochondrial mechanisms of photobiomodulation in context of new data about multiple roles of ATP. Photomed Laser Surg. 2010;28(2):159–160. doi:10.1089/pho.2010.2789
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.