Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Transcranial Magnetic Stimulation Combined with Speech-Language Therapy for Post-Stroke Aphasia Recovery: A Systematic Review and Network Meta-Analysis
Authors Lin J, Bao Y ![]() , Fang M, Zhang H
, Fang M, Zhang H
Received 29 March 2026
Accepted for publication 18 May 2026
Published 5 June 2026 Volume 2026:22 597978
DOI https://doi.org/10.2147/TCRM.S597978
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Jine Lin,1 Yangjuan Bao,1 Min Fang,1 Huafang Zhang2
1Department of Rehabilitation Medicine, the Fourth Affiliated Hospital of School of Medicine, and International School of Medicine, International Institutes of Medicine, Zhejiang University, Yiwu, Zhejiang, 322000, People’s Republic of China; 2Department of Nursing, The Fourth Affiliated Hospital of School of Medicine, and International School of Medicine, International Institutes of Medicine, Zhejiang University, Yiwu, Zhejiang, 322000, People’s Republic of China
Correspondence: Huafang Zhang, Department of Nursing, the Fourth Affiliated Hospital of School of Medicine, and International School of Medicine, International Institutes of Medicine, Zhejiang University, No. N1, Shangcheng Avenue, Yiwu, Zhejiang, 322000, People’s Republic of China, Email [email protected]
Background: Speech-language therapy (SLT) is standard care for post-stroke aphasia (PSA), and adjunctive transcranial magnetic stimulation (TMS) may further improve language function. Which TMS protocol optimally complements SLT for which language domain at which time point remains unresolved, motivating this network meta-analysis.
Objective: To compare TMS protocols combined with SLT across immediate and long-term language outcomes in post-stroke aphasia.
Methods: Web of Science, EMBASE, PubMed, and the Cochrane Library were searched from inception to 24 January 2026 for randomized trials of TMS plus SLT in post-stroke aphasia. Bayesian network meta-analyses were run in R 4.4.2 with the gemtc and rjags packages, with outcomes grouped into seven immediate and four long-term language domains and effect sizes reported as standardized mean differences (SMDs) with 95% credible intervals (CrIs). Treatments were ranked by the surface under the cumulative ranking curve (SUCRA), and certainty of evidence was rated using GRADE (Grading of Recommendations Assessment, Development and Evaluation).
Results: Across 26 trials enrolling 1,136 patients, three protocols led across the language domains. LF-rTMS+Music+SLT ranked first for immediate aphasia severity (SUCRA = 96.86%), repetition (97.25%), naming (99.69%), and spontaneous speech (95.67%); LF-rTMS+SLT, for writing (87.73%); and Dual-rTMS+SLT, for immediate functional communication (91.49%) and comprehension (97.57%). Dual-rTMS+SLT was also optimal across all four long-term outcomes (overall aphasia severity 95.82%, comprehension 95.06%, naming 99.74%, repetition 97.90%). Heterogeneity was low-to-moderate (moderate-to-high for immediate aphasia severity), and all Bayesian models converged (PSRF < 1.05). Evidence was moderate-to-high for standard comparisons (LF-rTMS+SLT vs SLT) but low to very low for the highest-ranked novel combinations such as LF-rTMS+Music+SLT, driven by imprecision and indirectness.
Conclusion: The optimal TMS-plus-SLT protocol depends on which language domain and which time point matters. LF-rTMS+Music+SLT led the immediate domains, while Dual-rTMS+SLT led the long-term domains. Standard adjunctive comparisons (e.g. LF-rTMS+SLT vs SLT) rest on moderate-to-high certainty evidence, but the highest-ranked novel combinations rest on low-certainty evidence and require head-to-head confirmation. A text-heavy research infographic with a large title at the top, two text columns and a row of small network diagrams along the bottom. The layout uses section headings and table grids to present study background, methods, results and conclusion. Text is in English. Title: Transcranial Magnetic Stimulation Combined with Speech-Language Therapy for Post-Stroke Aphasia Recovery: A Network Meta-Analysis. Left column headings and text. Background: Post-stroke aphasia (PSA) affects approximately 30 percent stroke survivors. Speech-language therapy (SLT) is standard care. Optimal TMS plus SLT protocol remains unclear. Methods: Web of Science, EMBASE, PubMed and the Cochrane Library were searched from inception to January 24, 2026. Risk of bias was assessed using Cochrane RoB 2.0. A Bayesian NMA was performed using R 4.4.2 and Stata 18. Conclusion: Optimal TMS plus SLT depends on language domain and time point. Short-term: LF-rTMS plus Music plus SLT is best. Long-term: Dual-rTMS plus SLT is best. Head-to-head trials are needed for confirmation. Right column heading and tables. Results: 26 RCTs (1,136 patients). Two tables are labeled Immediate Outcomes (Post-treatment) and Long-term Outcomes (Follow-up). Each table has columns Language Domain, Most Effective Intervention and SUCRA. Immediate Outcomes (Post-treatment) rows and SUCRA values: Aphasia severity, LF-rTMS plus Music plus SLT, 96.86 percent. Repetition, LF-rTMS plus Music plus SLT, 97.25 percent. Naming, LF-rTMS plus Music plus SLT, 99.69 percent. Spontaneous speech, LF-rTMS plus Music plus SLT, 95.67 percent. Writing, LF-rTMS plus SLT, 87.73 percent. Comprehension, Dual-rTMS plus SLT, 97.57 percent. Functional communication, Dual-rTMS plus SLT, 91.49 percent. Long-term Outcomes (Follow-up) rows and SUCRA values: Aphasia severity, Dual-rTMS plus SLT, 95.82 percent. Repetition, Dual-rTMS plus SLT, 97.90 percent. Naming, Dual-rTMS plus SLT, 99.74 percent. Comprehension, Dual-rTMS plus SLT, 95.06 percent. Along the bottom edge, multiple small network meta-analysis diagrams show circular nodes connected by lines, with some connections drawn thicker than others.Infographic: TMS & Speech Therapy for Aphasia Recovery Post-Stroke.
Keywords: stroke, cerebrovascular accident, aphasia, transcranial magnetic stimulation, network meta-analysis
Introduction
Stroke is the second leading cause of death and disability-adjusted life years (DALYs) lost worldwide and represents a major public health burden.1,2 Aphasia, defined as partial or complete impairment of language function, affects approximately 30% of stroke survivors.3 This condition is associated with increased risks of anxiety and depression, reduced social participation, and diminished quality of life.4–7 Effective therapeutic strategies are therefore urgently needed.
Current rehabilitation approaches for PSA include pharmacological treatments, music therapy, speech-language therapy (SLT), and non-invasive brain stimulation (NIBS).8 Pharmacological interventions, including conventional drugs and herbal formulations, have shown limited and inconsistent efficacy.9,10 Their mechanisms remain unclear, and no agent has received regulatory approval specifically for the treatment of aphasia.11,12 Music therapy has shown potential benefits, but further validation is needed before broad clinical implementation.13,14 SLT remains the gold-standard behavioral intervention. However, its effectiveness often depends on intensive and sustained practice, which may not be feasible for all patients.15,16 More effective and individualized strategies are therefore needed.
Non-invasive brain stimulation (NIBS) techniques, particularly transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS), have emerged as neuromodulatory approaches that enhance cortical neuroplasticity and support language recovery.8,17,18 TMS comprises repetitive TMS (rTMS) and theta-burst stimulation (TBS); TBS subdivides into excitatory intermittent (iTBS) and inhibitory continuous (cTBS) forms.19 Combining NIBS with SLT is neurophysiologically motivated: transient modulation of cortical excitability primes the learning and reorganisation triggered by subsequent language training.20–22
Several meta-analyses18,22–24 reported beneficial effects of rTMS on language recovery in PSA, with preliminary evidence that rTMS combined with SLT yields greater improvements than SLT alone, particularly in auditory comprehension, naming, repetition, and spontaneous speech.25,26 The synthesis base is nonetheless limited. An AMSTAR 227 appraisal of existing rTMS reviews28 found multiple methodological shortcomings: unregistered review protocols, missing justifications for excluded studies, inadequate description of participants and stimulation parameters, neglected risk-of-bias when interpreting results, incomplete reporting of stimulation sites and coil types, and inconsistent data extraction across reviews. Three further constraints persist: (i) some syntheses evaluated rTMS without requiring concurrent SLT,29,30 however, given that SLT is the cornerstone of aphasia rehabilitation, such a requirement is essential for clinical applicability, and its absence limits the relevance of those syntheses; (ii) recent RCTs of newer protocols such as iTBS and cTBS31–34 have not been incorporated into existing networks.18,22–24,35,36 (iii) some reviews included non-randomized studies,29 provided focused syntheses of specific domains such as action naming37 rather than a comprehensive multi-domain comparison,or on restricted outcome selection,36 or omitted detailed stimulation parameters24 or long-term effects.38
This network meta-analysis addresses these gaps by restricting inclusion to randomized trials of TMS combined with concurrent SLT, incorporating recent TBS trials, evaluating 11 outcome measures across 7 language domains, and assessing both immediate and follow-up effects. The certainty of each ranking was rated under the GRADE framework.
Methods
Design and Registration
This network meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Network Meta-Analyses (PRISMA-NMA).39 The protocol was prospectively registered in PROSPERO (CRD42024602404).
Search Strategy
Two independent reviewers (J.E.L. and Y.J.B.) searched Web of Science, EMBASE, PubMed, and the Cochrane Library from inception to January 24, 2026. No restrictions were applied to date, publication status, or document type. The search strategy combined Medical Subject Headings (MeSH) and free-text terms for keywords such as “stroke,” “cerebrovascular accident,” “transcranial magnetic stimulation,” “rTMS,” “cTBS,” and “aphasia,” along with related variants (see Table S1 for the full search strategies).
Inclusion and Exclusion Criteria
Eligibility followed the Population, Intervention, Comparison, Outcome, and Study Design (PICOS) framework, restricted to English-language randomized controlled trials (RCTs). Eligible participants were adults aged ≥18 years with PSA diagnosed by standardized clinical assessment. Eligible interventions were any TMS protocol (LF-rTMS, high-frequency rTMS (HF-rTMS), iTBS, cTBS, or Dual-rTMS) combined with SLT, provided that identical adjuvant treatments were used in both groups. Comparators were sham or placebo TMS combined with SLT, SLT alone, or other conventional therapies. Outcomes were immediate and long-term language improvement plus adverse events, assessed using validated instruments: the Montreal-Toulouse Protocol,40 Western Aphasia Battery (WAB),41 Aachen Aphasia Test (AAT),42 Concise Chinese Aphasia Test (CCAT),43 Boston Diagnostic Aphasia Examination (BDAE),44,45 WAB-Revised,46 Hemispheric Stroke Scale (HSS),47 Standard Language Test of Aphasia (SLTA),48 Boston Naming Test (BNT),49 semantic verbal fluency tasks,50–52 36-item Token Test (TT),53 Test of Language Assessment in Aphasia (ADD),54 Picture Naming Test-Turkish (T-RAT),55 International Picture Naming Database,56 Functional Independence Measure (FIM),57 Amsterdam-Nijmegen Everyday Language Test (ANELT),58 and the Snodgrass-Vanderwart picture inventory.59 These instruments mapped to seven outcome domains: aphasia severity, naming, repetition, spontaneous speech, comprehension, functional communication, and writing. Immediate and long-term effects were analyzed separately within each domain. Where multidomain scales were used (eg., WAB, AAT, BDAE), subscale scores were assigned to prespecified domains following the original test structure and prior literature.
Because very small studies are susceptible to small-study effects and yield unstable estimates, we excluded those with fewer than 20 participants60–62 (one study was excluded on this basis). Studies were also excluded for unclear diagnostic or efficacy criteria, non-extractable data, or TMS combined with medications or acupuncture. Non-original studies (reviews, meta-analyses, case reports, animal studies, conference abstracts, guidelines, letters) were also excluded.
Study Selection
After duplicates were removed in EndNote 21, two reviewers (J.E.L. and Y.J.B.) independently screened titles and abstracts. Full texts of potentially eligible studies were then assessed. Disagreements were resolved through discussion or consultation with a third reviewer (M.F). The selection process is shown in the PRISMA flow diagram (Figure 1).
 |
Figure 1 PRISMA flow diagram for search and selection of eligible studies included in the NMA. |
Data Extraction and Quality Assessment
Data were extracted using standardized Cochrane forms, capturing study characteristics (title, author, year, and country), participant characteristics (sample size, age, sex, handedness, stroke type, aphasia type, and time post-stroke), intervention details (TMS protocol and parameters, stimulation site, content and timing of SLT relative to TMS, treatment duration, and follow-up period), and outcome data (means, standard deviations, numbers of adverse events, and measurement scales). For multi-arm trials with both eligible and ineligible neuromodulation arms, only the arms relevant to the TMS-based network were extracted. One reviewer (J.E.L.) extracted the data, a second (Y.J.B.) verified them, and a third (M.F.) adjudicated discrepancies.
Risk of bias for each included RCT was assessed independently by two reviewers (J.E.L. and Y.J.B.) using the Cochrane Risk of Bias tool for randomized trials (RoB 2.0).63 Each study was evaluated across five domains and assigned a judgment of “low risk,” “some concerns,” or “high risk.” An overall high risk of bias was assigned if any domain was rated as high risk, whereas an overall low risk required all domains to be rated as low risk. Disagreements were resolved through discussion or consultation with a third reviewer (M.F).
Certainty of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.64,65 For each comparison and outcome, certainty was rated as high, moderate, low, or very low,66,67 based on risk of bias, inconsistency, indirectness, imprecision, publication bias, intransitivity, and incoherence. Imprecision was rated following GRADE guidance.68 Where incoherence occurred, the estimate with higher certainty between direct and indirect evidence was adopted.
Statistical Analysis
A Bayesian framework was applied using JAGS through the gemtc (version 0.8–2) and rjags (version 4–10) packages in R (version 4.4.2). Continuous outcomes were expressed as standardized mean differences (SMDs) with 95% credible intervals (CrIs). Random-effects models were used to account for clinical and methodological heterogeneity across studies. The surface under the cumulative ranking curve (SUCRA) and mean ranks were calculated to rank the interventions. Higher SUCRA values, ranging from 0% to 100%, indicated a greater probability that an intervention was the most effective or safest option. Consistency between direct and indirect comparisons was assessed using the deviance information criterion (DIC), with a difference of less than 5 indicating acceptable consistency. Publication bias was assessed visually using comparison-adjusted funnel plots in Stata 18.0.
Prior distributions and model implementation: Non-informative priors were used for all model parameters to let the data dominate the posterior. The relative effect parameters were assigned a normal distribution with mean 0 and SD = 15 x om.scale, where om.scale is a data-derived scale parameter defining the prior range for continuous outcomes. The between-study heterogeneity SD (τ) followed a uniform prior on [0, om.scale] (τ ~ Uniform(0, om.scale)). Markov chain Monte Carlo (MCMC) simulations used four independent chains with 5,000 burn-in and 20,000 sampling iterations. Heterogeneity, convergence, and visual diagnostics: Heterogeneity was assessed using tau values categorised by established guidelines: low (<0.04), low-to-moderate (0.04–0.16), moderate-to-high (0.16–0.36), and high (>0.36).69,70 Uncertainty of the heterogeneity estimate was quantified by the 95% credible interval (CrI) for τ2. Model convergence was assessed by the Brooks-Gelman-Rubin diagnostic, with PSRF < 1.05 indicating adequate convergence for all parameters.71 Diagnostic plots provided visual validation: trace plots confirmed adequate chain mixing and the absence of trends, and posterior density plots characterised the shape and variability of the posterior distribution.
Results
Search Results
The initial database search identified 1,900 records. After removal of 474 duplicates, 1,426 studies underwent title and abstract screening according to predefined criteria, and 1,341 were excluded. A total of 85 full-text articles were sought for retrieval; 28 could not be obtained, and the remaining 57 were assessed for eligibility. Of these, 31 were excluded because the total number of participants was less than 20 (n=1), the article was not in English (n=2), the intervention was not relevant (n=1), the study was a case report (n=4), the study was not an RCT (n=8), the target population was not eligible (n=1), the data were not extractable (n=9), or the intervention was not combined with SLT (n=5). Ultimately, 26 RCTs were included in the network meta-analysis. The PRISMA flow diagram is shown in Figure 1.
 |
Table 1 Characteristics of the Included Studies |
Study Characteristics
Twenty-six RCTs published between 2012 and 2026 were included (Table 1): 2 multinational (Canada/United States/Germany),72,73 1 in the United States,87 3 in Germany,78,84,91 1 in Turkey,74 1 in Canada,86 15 in China,25,31–34,75,76,79–82,85,88,89,92 2 in Poland,77,90 and 1 in Egypt.83 The trials enrolled 1,136 patients with PSA; sample sizes ranged from 28 to 96 (mean 43.7, median 41), mean ages from 45.3 to 71.2 years, and follow-up from 1 to 180 days.
Across the included trials, the network comprised the following nodes: LF-rTMS alone;74 LF-rTMS with SLT (n=19);34,72–79,81,82,84–88,90–92 LF-rTMS with SLT and music (n=1);80 dual-hemisphere rTMS with SLT (n=2)25,83 iTBS with SLT (n=5);31–34,89 and cTBS with SLT (n=3).31–33 The intensity of rTMS ranged from 80% to 110% of resting motor threshold (RMT), and the mean duration of illness from 15.9 days to 6.25 years. A detailed breakdown of stimulation parameters (intensity, frequency, and total pulses per session) is provided in Table 1.
Risk of Bias and GRADE Evidence Grading
Overall, 18 studies (69.2%) were low risk, 5 (19.2%) had some concerns, and 3 (11.5%) were high risk (Figure 2).
 |
Figure 2 Summary of risk of bias for the included studies. |
Most studies showed a low risk of bias across domains: outcome reporting (100%), missing data (88.5%), outcome measurement (96.2%), randomization (76.9%), and protocol deviations (88.5%). Unclear risk was noted for inadequate reporting of missing data (7.7%), protocol deviations (11.5%), and randomization methods (19.2%). High risk was identified for poorly described randomization (3.8%), missing outcome data (3.8%), and outcome measurement (3.8%). Studies failing to report relevant information were classified as unclear risk. Three trials were rated high risk for specific reasons: Yaşa et al74 for insufficient randomization description allowing prediction of group assignment; Bai et al85 for not reporting outcome-assessor blinding (possible detection bias); and Dresang et al87 for missing outcome data with evidence that missingness depended on the true value (attrition bias).
The certainty of evidence varied substantially across comparisons. Conventional protocols, notably LF-rTMS+SLT versus SLT alone, had moderate-to-high certainty across several domains (eg., immediate naming, comprehension, and writing), reflecting narrow credible intervals and direct robust comparisons. However, network estimates involving novel or multi-component interventions (eg., LF-rTMS+Music+SLT) had predominantly low to very low certainty. Downgrades were driven by inconsistency (larger upper bound of tau-squared), indirectness (sparse network connections), and imprecision (wide credible intervals crossing the null). Risk of bias was generally not downgraded, as approximately 70% of studies showed low overall risk per the Cochrane RoB 2.0 assessment. A detailed GRADE summary for all network estimates is provided in Table S2.
Heterogeneity and Model Convergence Assessment
The between-study heterogeneity variance (τ2) varied across outcomes, with posterior medians ranging from 0.0033 (95% CrI: 0.00001 to 0.0404) for immediate comprehension to 0.1728 (95% CrI: 0.0057 to 0.6349) for immediate aphasia severity. Most τ2 estimates were small, although long-term repetition showed greater uncertainty (τ2 = 0.0673, 95% CrI: 0.00013 to 1.7868). Overall model convergence was satisfactory, with all PSRF values < 1.05 (Table S3). Trace plots showed adequate mixing without drift, and posterior density plots were generally unimodal and stable, supporting model convergence and stability (Figure S1). These findings were consistent with the Brooks-Gelman-Rubin diagnostic plots (Figure S2).
NMA
Immediate Improvement in Aphasia Severity
Twenty studies31–34,72,75,76,78–86,88,89,91,92 Involving seven interventions reported immediate aphasia severity outcomes (Figure 3A). LF-rTMS+Music+SLT was significantly more effective than several alternatives (Figure 3B): compared with LF-rTMS+SLT (SMD =1.48, 95% CrI [0.21, 2.73]); music+SLT (SMD = 1.77, 95% CrI [0.43, 3.14]); iTBS+SLT (SMD = 1.51, 95% CrI [0.18, 2.82]); and SLT alone (SMD = 2.05, 95% CrI [0.84, 3.29]). SUCRA ranked LF-rTMS+Music+SLT highest (96.86%) (Figure 3C).
 |
Figure 3 NMA of immediate improvement in aphasia severity: (A) network plot; (B) comparative effectiveness; (C) SUCRA rankings. SMDs with 95% CrIs; significant results are shown in bold. |
The certainty of evidence for this outcome is shown in Table S2; heterogeneity and convergence diagnostics are summarized in Table S3.
Immediate Improvement in Repetition
Twenty studies25,32–34,74,76–86,88,89,91,92 involving eight protocols assessed immediate repetition improvement (Figure 4A). LF-rTMS+Music+SLT was superior to cTBS+SLT (SMD = 1.07, 95% CrI [0.12, 1.98]), iTBS+SLT (SMD = 1.38, 95% CrI [0.53, 2.21]), LF-rTMS (SMD = 1.68, 95% CrI [0.49, 2.86]), LF-rTMS+SLT (SMD = 1.29, 95% CrI [0.49, 2.08]), music+SLT (SMD = 1.06, 95% CrI [0.05, 2.05]), and SLT (SMD = 1.63, 95% CrI [0.86, 2.39]) (Figure 4B). SUCRA ranked LF-rTMS+Music+SLT highest (97.25%) (Figure 4C).
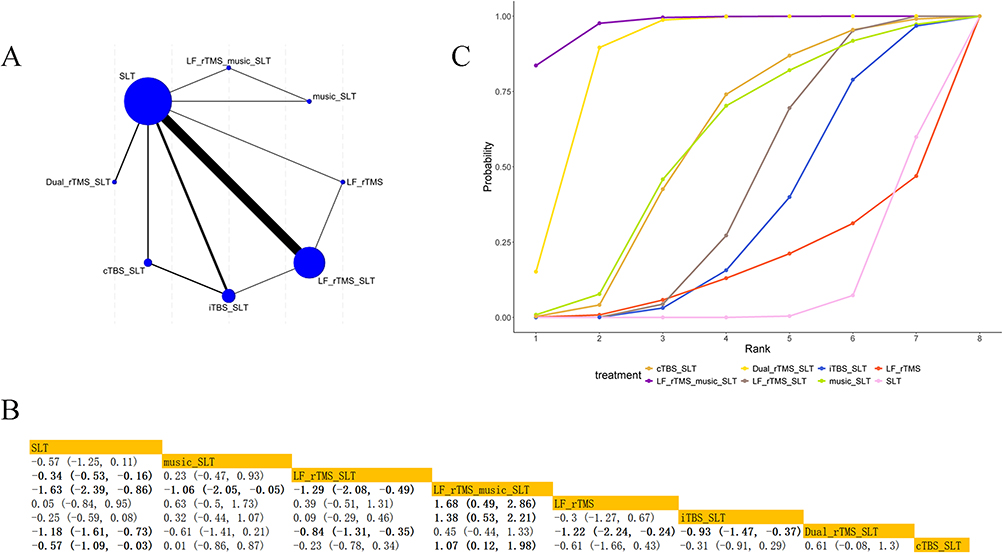 |
Figure 4 NMA of immediate repetition: (A) Network plot; (B) Comparative effects; (C) SUCRA rankings. SMD with 95% CrI; significant results in bold. |
The certainty of evidence for this outcome is shown in Table S2; heterogeneity and convergence diagnostics are summarized in Table S3.
Immediate Improvement in Comprehension
Twenty25,32–34,72–74,77–86,89,91,92 studies involving eight interventions evaluated immediate comprehension outcomes (Figure 5A). Dual-rTMS+SLT was superior to iTBS+SLT (SMD = 0.84, 95% CrI [0.35, 1.30]), LF-rTMS (SMD = 1.38, 95% CrI [0.39, 2.37]), LF-rTMS+SLT (SMD = 0.91, 95% CrI [0.48, 1.33]), music+SLT (SMD = 1.1, 95% CrI [0.34, 1.859]), cTBS+SLT (SMD = 0.72, 95% CrI [0.06, 1.37]), and SLT (SMD = 1.18, 95% CrI [0.77, 1.57]) (Figure 5B). Dual-rTMS+SLT had the highest SUCRA (97.57%) (Figure 5C).
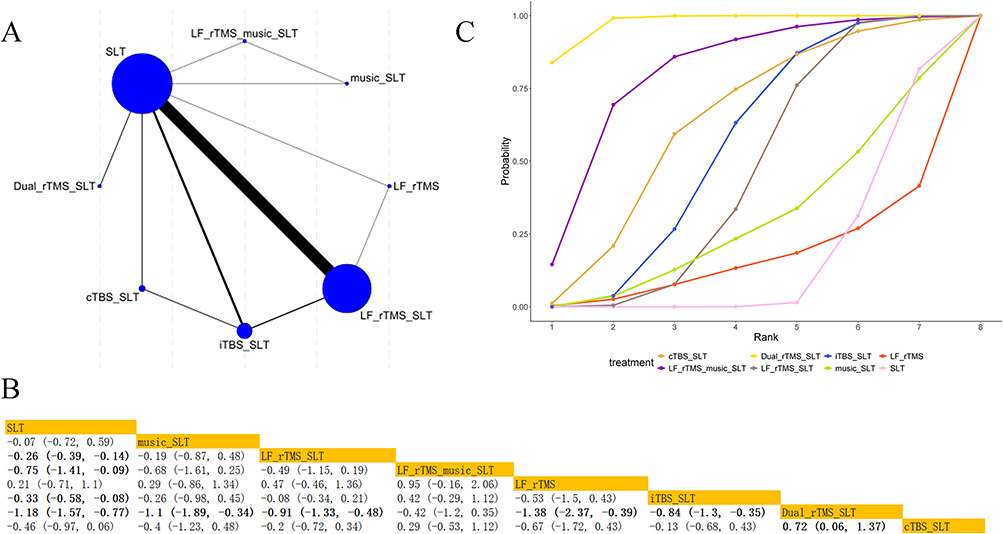 |
Figure 5 NMA of immediate comprehension: (A) Network plot; (B) Comparative effectiveness; (C) SUCRA rankings. SMD with 95% CrI; significant results in bold. |
The certainty of evidence for this outcome is shown in Table S2; heterogeneity and convergence diagnostics are summarized in Table S3.
Immediate Improvement in Naming
Twenty-two studies32,33,72–91 involving eight interventions evaluated immediate naming outcomes (Figure 6A). LF-rTMS+Music+SLT was superior to cTBS+SLT (SMD = 1.51, 95% CrI [0.53, 2.46]), Dual-rTMS+SLT (SMD = 1.21, 95% CrI [0.10, 2.41]), iTBS+SLT (SMD = 1.56, 95% CrI [0.65, 2.47]), LF-rTMS (SMD = 2.59, 95% CrI [1.53, 3.61]), LF-rTMS+SLT (SMD = 1.55, 95% CrI [0.72, 2.36]), music+SLT (SMD = 1.38, 95% CrI [0.36, 2.38]), and SLT (SMD = 1.96, 95% CrI [1.15, 2.76]) (Figure 6B). LF-rTMS+Music+SLT ranked first by SUCRA (99.69%) (Figure 6C).
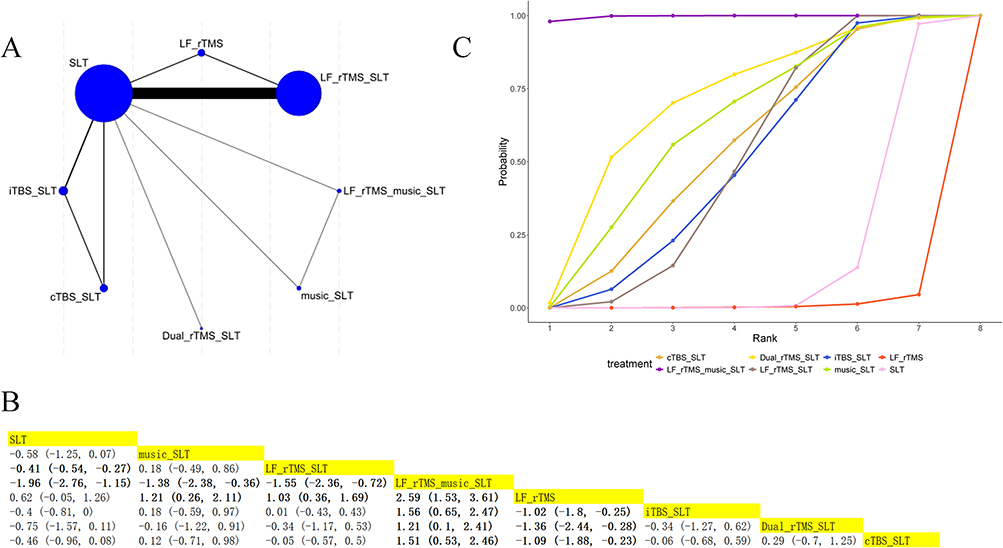 |
Figure 6 NMA of immediate naming: (A) Network plot; (B) Comparative effects; (C) SUCRA rankings. SMD with 95% CrI; significant results in bold. |
The certainty of evidence for this outcome is shown in Table S2; heterogeneity and convergence diagnostics are summarized in Table S3.
Immediate Improvement in Spontaneous Speech
Sixteen studies25,32–34,75,76,78–82,85,86,88,89,92 involving seven interventions reported immediate spontaneous speech outcomes (Figure 7A). LF-rTMS+Music+SLT significantly outperformed cTBS+SLT (SMD = 2.53, 95% CrI [1.4, 3.7]), iTBS+SLT (SMD = 1.23, 95% CrI [0.24, 2.21]), LF-rTMS+SLT (SMD = 1.05, 95% CrI [0.1, 1.99]), music+SLT (SMD = 1.27, 95% CrI [0.17, 2.36]), and SLT (SMD = 1.48, 95% CrI [0.57, 2.4]) (Figure 7B). SUCRA for LF-rTMS+Music+SLT was 95.67% (Figure 7C).
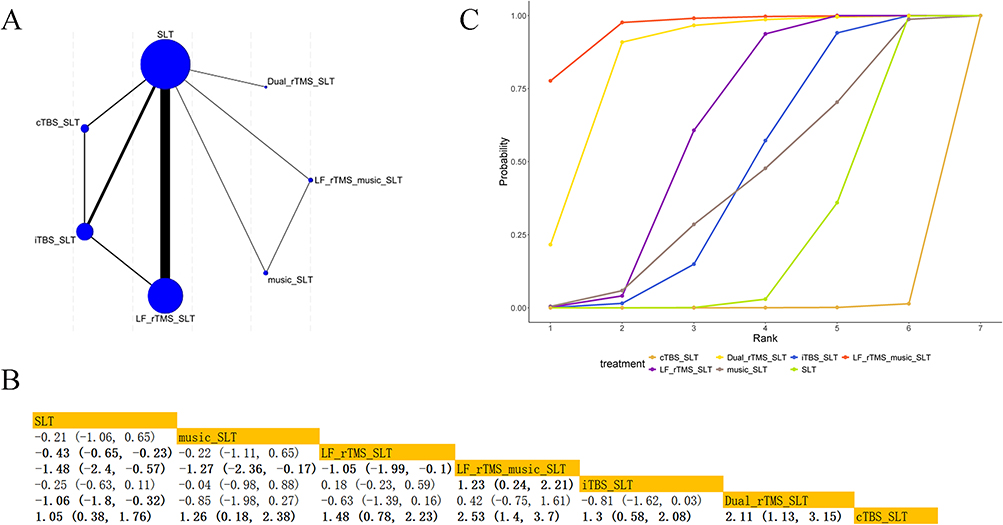 |
Figure 7 NMA of immediate spontaneous speech: (A) Network plot; (B) Comparative effectiveness; (C) SUCRA rankings. SMD with 95% CrI; significant results in bold. |
The certainty of evidence for this outcome is shown in Table S2; heterogeneity and convergence diagnostics are summarized in Table S3.
Immediate Improvement in Functional Communication
Seven studies25,34,75,76,78,86,92 involving four interventions assessed immediate improvement in functional communication (Figure 8A). Dual-rTMS+SLT was significantly more effective than SLT alone (SMD = 0.62, 95% CrI [0.06, 1.17]) (Figure 8B). SUCRA ranked Dual-rTMS+SLT highest (91.49%) (Figure 8C).
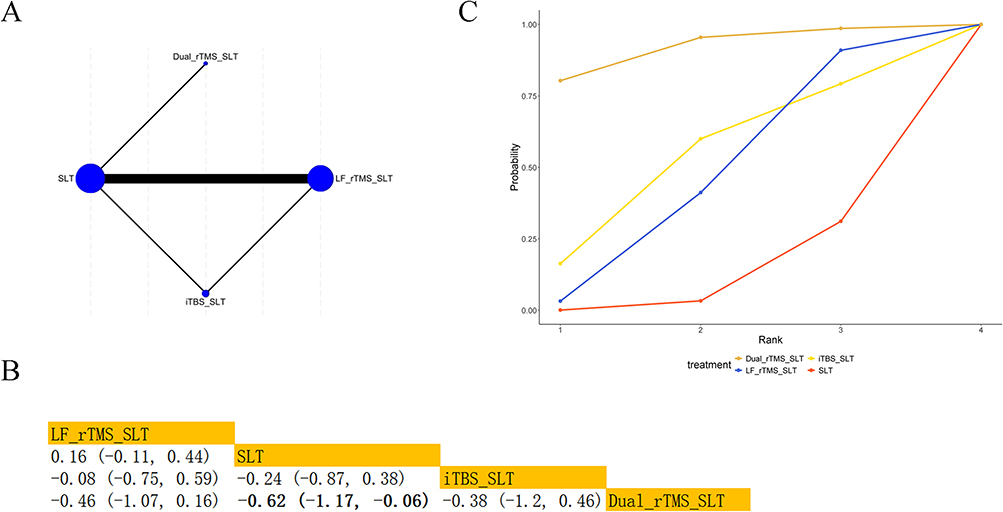 |
Figure 8 NMA of immediate functional communication: (A) Network plot; (B) Comparative effectiveness; (C) SUCRA rankings. SMD with 95% CrI; significant results in bold. |
The certainty of evidence for this outcome is shown in Table S2; heterogeneity and convergence diagnostics are summarized in Table S3.
Immediate Improvement in Writing
Seven studies34,78,81,82,84,91,92 involving three interventions evaluated immediate writing outcomes (Figure 9A). LF-rTMS+SLT was significantly more effective than SLT (SMD = 0.34, 95% CrI [0.10, 0.58]) (Figure 9B). SUCRA for LF-rTMS+SLT was 87.73% (Figure 9C).
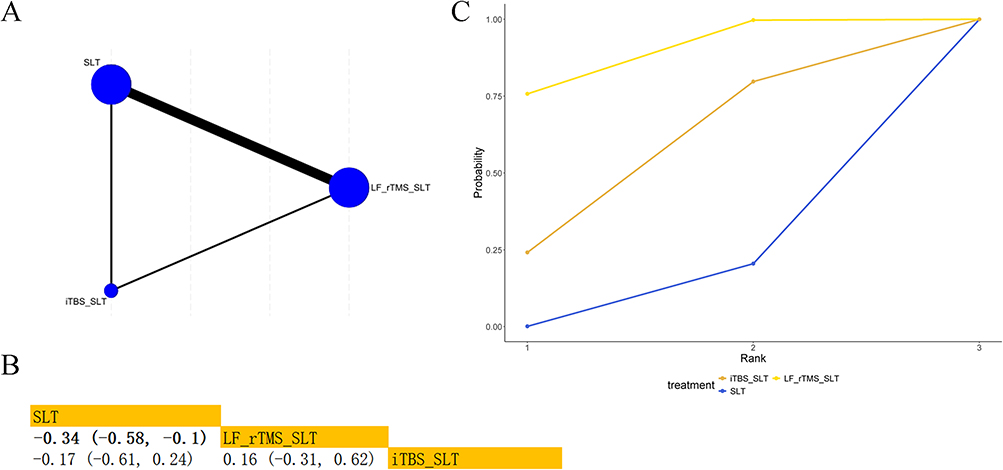 |
Figure 9 NMA of immediate writing: (A) Network plot; (B) Comparative effectiveness; (C) SUCRA rankings. SMD with 95% CrI; significant results in bold. |
The certainty of evidence for this outcome is shown in Table S2; heterogeneity and convergence diagnostics are summarized in Table S3.
Long-Term Improvement in Aphasia Severity
Five studies72,75,76,83,86 involving three interventions reported long-term aphasia severity outcomes (Figure 10A). Dual-rTMS+SLT showed a larger improvement than SLT (SMD = 1.23, 95% CrI [0.10, 2.36]) (Figure 10B). Although the credible interval did not cross the null, the lower bound was close to zero and the interval was wide. This imprecision, largely attributable to the limited number of studies informing this comparison, contributed to the evidence being rated low certainty in the GRADE assessment. SUCRA ranked Dual-rTMS+SLT highest (95.82%) (Figure 10C).
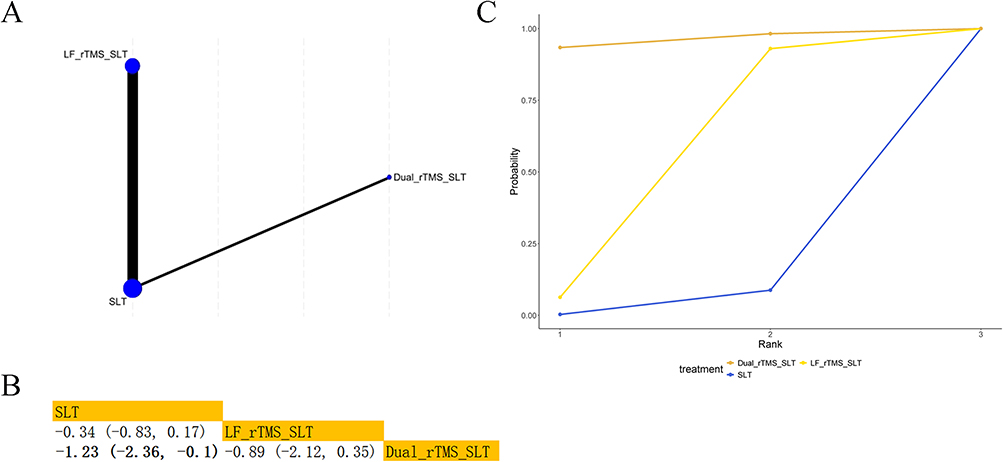 |
Figure 10 NMA of long-term severity of aphasia: (A) Network plot; (B) Comparative effectiveness; (C) SUCRA rankings. SMD with 95% CrI; significant results in bold. |
The certainty of evidence for this outcome is shown in Table S2; heterogeneity and convergence diagnostics are summarized in Table S3.
Long-Term Improvement in Repetition
Five studies74,76,83,86,91 involving four interventions assessed long-term repetition improvement (Figure 11A). Dual-rTMS+SLT was superior to SLT (SMD = 1.82, 95% CrI [0.44, 3.17]) (Figure 11B). Dual-rTMS+SLT had the highest SUCRA (97.90%) (Figure 11C).
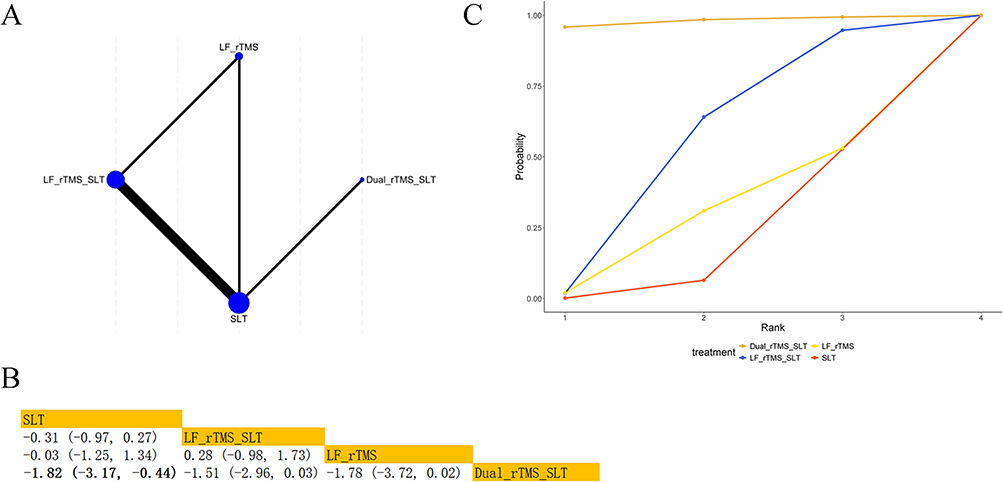 |
Figure 11 NMA of long-term repetition: (A) Network plot; (B) Comparative effects; (C) SUCRA rankings. SMD with 95% CrI; significant results in bold. |
The certainty of evidence for this outcome is shown in Table S2; heterogeneity and convergence diagnostics are summarized in Table S3.
Long-Term Improvement in Comprehension
Six studies72–74,77,83,86 involving four interventions assessed long-term comprehension outcomes (Figure 12A). Pairwise comparisons showed no statistically significant differences among the interventions, as all 95% credible intervals crossed the null value (Figure 12B). Although Dual-rTMS+SLT had the highest SUCRA value (95.06%) (Figure 12C), this ranking reflects relative probability rather than statistically confirmed superiority. Therefore, these long-term comprehension results should be interpreted cautiously.
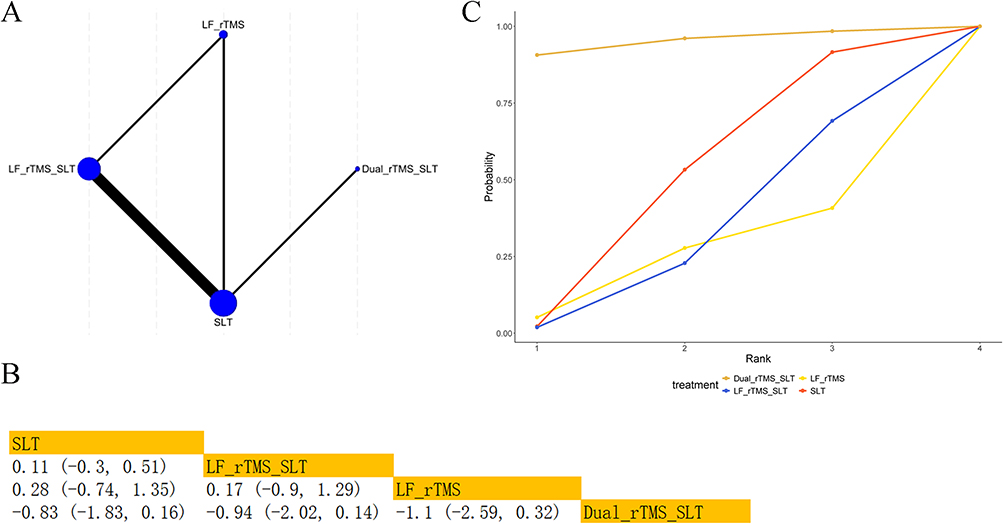 |
Figure 12 NMA of long-term comprehension: (A) Network plot; (B) Comparative effects; (C) SUCRA rankings. SMD with 95% CrI; significant results in bold. |
The certainty of evidence for this outcome is shown in Table S2; heterogeneity and convergence diagnostics are summarized in Table S3.
Long-Term Improvement in Naming
Ten studies72–77,83,86,87,90 involving four interventions assessed long-term naming outcomes (Figure 13A). Dual-rTMS+SLT was significantly more effective than LF-rTMS (SMD = 1.99, 95% CrI [0.82, 3.07]), LF-rTMS+SLT (SMD = 1.23, 95% CrI [0.29, 2.15]), and SLT (SMD = 1.47, 95% CrI [0.55, 2.37]) (Figure 13B). SUCRA ranked Dual-rTMS+SLT highest (99.74%) (Figure 13C).
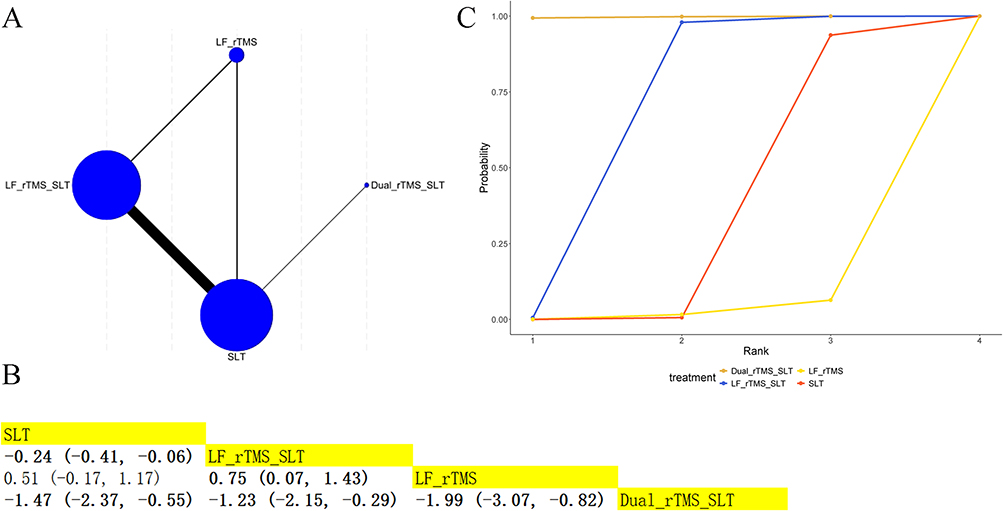 |
Figure 13 NMA of long-term naming: (A) Network plot; (B) Comparative effects; (C) SUCRA rankings. SMD with 95% CrI; significant results in bold. |
The certainty of evidence for this outcome is shown in Table S2; heterogeneity and convergence diagnostics are summarized in Table S3.
Adverse Events
The reporting of adverse events was inconsistent across studies: some trials reported the number of affected participants, while others reported the total number of events or sessions during which events occurred. We therefore present the data as originally described, without pooling, and highlight relevant limitations. Among the 26 included studies, seven studies31,34,72,73,75,80,86 documented at least one treatment-related adverse event, all occurring during or shortly after the TMS procedure. Headache was reported in four studies: Ren et al31 (1 participant), Zumbansen et al72 (1 participant), Zumbansen et al73 (1 participant), and Low et al86 (10 episodes across sessions; affected participants not specified). Dysesthesia was reported in Zumbansen et al72 (1 participant) and Zumbansen et al73 (1 participant). Dizziness was reported in Chou et al34 (2 participants) and Liu et al80 (2 participants). Ren et al31 also reported seizure (2 participants) and involuntary movement (1 participant), and Wang et al75 reported dull pain (1 participant). No serious adverse events were reported. Because reporting formats were heterogeneous, the true number of participants experiencing adverse events may differ from the figures above.
Consistency and Publication Bias
Model consistency was assessed using DIC, with all closed-loop models showing differences <5, indicating adequate consistency. Node-splitting analysis was conducted for outcomes with available closed loops in the network. Only four outcomes (immediate aphasia severity, immediate repetition, immediate comprehension, and immediate spontaneous speech) had sufficient closed loops for this assessment; the remaining outcomes lacked closed loops and were therefore not amenable to node-splitting (Table 2). No significant inconsistency was detected in any of the assessable comparisons (all P > 0.05). Comparison-adjusted funnel plots detected potential publication bias (Figure S3).
 |
Table 2 Local Inconsistency Assessment for Outcomes with Available Closed Loops |
Discussion
Across 26 randomized trials, no single TMS protocol led every language domain. Three protocols partitioned the leadership: LF-rTMS+Music+SLT produced the largest immediate gains in aphasia severity, repetition, naming, and spontaneous speech; Dual-rTMS+SLT led short- and long-term comprehension and the long-term outcomes for aphasia severity, naming, and repetition plus immediate functional communication; LF-rTMS+SLT topped immediate writing. Whether these domain-specific advantages survive critical appraisal of the underlying evidence is the focus of the remainder of this Discussion.
The ranking hierarchy carries an interpretive ceiling. Trials varied in aphasia subtype, time since stroke, lesion characteristics, stimulation targets, and co-intervention details, so apparently direct protocol contrasts often draw on quite different study settings. The ceiling tightens further for nodes informed by a single trial or only by indirect comparisons; those rankings should be read as hypothesis-generating, not confirmatory.
LF-rTMS+Music+SLT ranked first for immediate aphasia severity, This finding is broadly consistent with prior studies supporting LF-rTMS-based approaches in post-stroke aphasia.30,80,93 However, this estimate rests on a single trial and should be treated as hypothesis-generating. The mechanism is plausible, with neuromodulation likely facilitating transient cortical reorganization while structured language therapy plus music-based input reinforces engagement and language processing,14,94–96 yet head-to-head replication is needed before this protocol can be positioned ahead of established LF-rTMS+SLT for severity recovery.
LF-rTMS+Music+SLT led immediate repetition, contradicting Li et al38 who identified iTBS as the optimal protocol. Two non-exclusive explanations apply. Mechanistically, repetition draws primarily on frontal language regions including Broca’s, Wernicke’s, and Geschwind’s territories and their associated pathways,97,98 and although iTBS spreads dynamic neurophysiological effects from the stimulation site to distributed fronto-limbic circuits,99 pairing LF-rTMS+SLT with music input may amplify repetition recovery through synergistic neuromodulation and intensive language engagement. Methodologically, Li et al38 did not require concurrent SLT as an inclusion criterion, whereas the present network restricted comparators to TMS+SLT, which can shift the relative ranking. Head-to-head trials are needed to clarify the comparative efficacy of LF-rTMS– and iTBS-based combinations.
Dual-rTMS combined with SLT was the most effective intervention, not only for short- and long-term improvement in comprehension, but also for long-term improvement in aphasia severity, naming, and repetition. This finding is consistent with Li et al38 Khedr et al83 Dang et al25 and supports the relevance of bilateral neuromodulation for auditory–semantic processing. Comprehension is largely mediated by a ventral neural pathway.100,101 In the dual-hemisphere protocol, low-frequency stimulation is applied to the right Broca’s homologue to reduce transcallosal inhibition, while high-frequency stimulation is delivered to the left Broca’s area to enhance connectivity in metabolically compromised regions. Sequential bilateral stimulation, first targeting the unaffected hemisphere and then the affected hemisphere, may reduce pathological right-hemisphere hyperactivity. This approach restores interhemispheric balance and creates favorable conditions for excitatory stimulation.83 The dependence of comprehension on coordinated bilateral networks may explain the pronounced benefit of Dual-rTMS+SLT.
Immediate naming improved most with LF-rTMS, SLT, and music therapy. This contrasts with Ding et al30 who identified Dual-rTMS as optimal and cTBS as ineffective, and with Li et al38 who reported cTBS as superior. Variability in adjunctive interventions may partly explain these differences. Naming outcomes are also influenced by the duration of therapy and the first language of participants,30 and environmental factors such as background noise may affect performance.101 The phase of stroke recovery represents a critical moderator. During the subacute phase, contralesional hyperexcitability may increase transcallosal inhibition of perilesional networks. Inhibitory LF-rTMS targeting the right inferior frontal gyrus may mitigate this maladaptive effect.102 In the chronic phase, when structural reserve in the left hemisphere is diminished, compensatory recruitment of right-hemisphere homologues may become the primary recovery pathway. In such cases, facilitatory stimulation, including HF-rTMS within dual-mode protocols or iTBS, may provide greater benefit.103 Differences in cohort composition across trials likely influenced pooled estimates and may explain why studies with a higher proportion of chronic patients30 reported stronger effects for bilateral stimulation.
For immediate spontaneous speech, LF-rTMS+Music+SLT demonstrated the most favorable outcomes, consistent with Ding et al30 Beyond direct modulation at the stimulation site, LF-rTMS may suppress maladaptive activation in frontal and temporal regions of the right hemisphere while facilitating functional engagement of corresponding areas in the left dominant hemisphere. This coordinated modulation promotes restoration of interhemispheric balance and supports functional reorganization within preserved language networks.81
Dual-rTMS combined with SLT was most effective for long-term naming. This finding agrees with Ding et al30 but differs from Li et al38 who reported cTBS as optimal. Differences in adjunctive therapy and follow-up duration may account for the discrepancy. Importantly, SLT remains the essential behavioral component across all protocols. Structured and goal-directed language practice is necessary to guide and consolidate neuroplastic changes.104 The failure of some studies38 to distinguish between immediate and long-term outcomes may further contribute to inconsistent conclusions. Future trials should analyze short- and long-term effects separately across language domains.
Consistent with the findings of Lee et al92 LF-rTMS+SLT produced the greatest immediate improvement in writing. One possible explanation is that LF-rTMS promotes language recovery by modulating neural activity in the right hemisphere, particularly in the right frontotemporal cortex, caudate nucleus, and insular cortex.102 These neuroadaptive changes have been linked to enhanced language production.
Strengths and Limitations
This network’s principal strength is comparing multiple TMS protocols head-to-head while holding SLT as a concurrent co-intervention, which keeps the clinical question intact. Separating language domains and distinguishing immediate from follow-up outcomes further yielded a treatment-effect picture that conventional pairwise meta-analysis cannot produce.
Five limitations bound the inferences. First, included trials varied in patient characteristics, stroke chronicity, stimulation targets, treatment intensity, and SLT content, which limits cross-study comparability and likely shaped the rankings. Second, several nodes (particularly newer or combined protocols) rested on sparse or single-trial evidence, so any node-level claim is provisional. Third, the top-ranked combinations (notably LF-rTMS+Music+SLT) carry low to very low certainty driven by imprecision and indirectness, even though standard TMS-vs-SLT-alone comparisons reached moderate-to-high certainty. Fourth, long-term outcomes drew on fewer studies than immediate outcomes, making follow-up estimates less stable Fifth, inconsistent adverse-event reporting precluded reliable cross-protocol safety comparison. Together, these constraints place the protocol hierarchy on hypothesis-generating rather than confirmatory footing, with adequately powered head-to-head trials of the top three combinations as the most informative next step.
Conclusions
This NMA suggests that the optimal TMS protocol depends on the rehabilitation goal in post-stroke aphasia. LF-rTMS combined with music therapy and SLT showed the most favorable short-term pattern across several language outcomes, whereas Dual-rTMS+SLT ranked highest for most follow-up outcomes. LF-rTMS+SLT appeared to offer the clearest short-term benefit for writing. These findings may guide targeted rehabilitation strategies, but remain uncertain because most comparisons rest on low-certainty, largely indirect evidence. Direct comparative trials are needed to inform firm clinical recommendations.
Abbreviations
DALYs, disability-adjusted life years; SLT, speech-language therapy; NIBS, non-invasive brain stimulation; TMS, transcranial magnetic stimulation; tDCS, transcranial direct current stimulation; rTMS, repetitive TMS; TBS, theta-burst stimulation; iTBS, intermittent TBS; cTBS, continuous TBS; PSA, post-stroke aphasia; PICOS, Population/Patients, Intervention, Comparison, Outcome, and Study Design; WAB, Western Aphasia Battery; AAT, Aachen Aphasia Test; CCAT, Concise Chinese Aphasia Test; BDAE, Boston Diagnostic Aphasia Examination; HSS, Hemispheric Stroke Scale; SLTA, Standard Language Test of Aphasia; BNT, Boston Naming Test; TT, Token Test; T-RAT, Picture Naming Test-Turkish; FIM, Functional Independence Measure; ANELT, Amsterdam-Nijmegen Everyday Language Test; RCTs, randomized controlled trials; SMD, Standardized mean differences; RR, risk ratios; SUCRA, surface under the cumulative ranking curve; DIC, deviance information criterion.
Data Sharing Statement
Data available from corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This article does not contain any studies with human or animal participants.
Consent for Publication
There are no human participants in this article and informed consent is not required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Health Medicine and Hygiene Science and Technology Program of Zhejiang Province (2023KY839, 2023KY837).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. WHO. DALY estimates, 2000–2016. Available from: https://www.who.int/data/global-health-estimates.
2. WHO. Summary tables of mortality estimates by cause, age and sex, globally and by region, 2000–2016. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates.
3. Flowers HL, Skoretz SA, Silver FL, et al. Poststroke Aphasia Frequency, Recovery, and Outcomes: a Systematic Review and Meta-Analysis. Arch Phys Med Rehabil. 2016;97(12):2188–2201.e8. doi:10.1016/j.apmr.2016.03.006
4. Blonski DC, Covert M, Gauthier R, et al. Barriers to and Facilitators of Access and Participation in Community-Based Exercise Programmes from the Perspective of Adults with Post-stroke Aphasia. Physiother Can. 2014;66(4):367–26. doi:10.3138/ptc.2013-70
5. Baker C, Worrall L, Rose M, Ryan B. Stroke health professionals’ management of depression after post-stroke aphasia: a qualitative study. Disabil Rehabil. 2021;43(2):217–228. doi:10.1080/09638288.2019.1621394
6. Shehata GA, El Mistikawi T, Risha AS, Hassan HS. The effect of aphasia upon personality traits, depression and anxiety among stroke patients. J Affect Disord. 2015;172:312–314. doi:10.1016/j.jad.2014.10.027
7. Hilari K, Needle JJ, Harrison KL. What are the important factors in health-related quality of life for people with aphasia? A systematic review. Arch Phys Med Rehabil. 2012;93(1 Suppl):S86–95. doi:10.1016/j.apmr.2011.05.028
8. Vitti E, Hillis AE. Treatment of post-stroke aphasia: a narrative review for stroke neurologists. Int J Stroke. 2021;16(9):1002–1008. doi:10.1177/17474930211017807
9. Zhang X, Shu B, Zhang D, Huang L, Fu Q, Du G. The Efficacy and Safety of Pharmacological Treatments for Post-stroke Aphasia. CNS Neurol Disord Drug Targets. 2018;17(7):509–521. doi:10.2174/1871527317666180706143051
10. Fridriksson J, Hillis AE. Current Approaches to the Treatment of Post-Stroke Aphasia. J Stroke. 2021;23(2):183–201. doi:10.5853/jos.2020.05015
11. Berthier ML. Ten key reasons for continuing research on pharmacotherapy for post-stroke aphasia. Aphasiology. 2021;35(6):824–858. doi:10.1080/02687038.2020.1769987
12. Stockbridge MD. Better language through chemistry: augmenting speech-language therapy with pharmacotherapy in the treatment of aphasia. Handb Clin Neurol. 2022;185:261–272. doi:10.1016/b978-0-12-823384-9.00013-x
13. Leonardi S, Cacciola A, De Luca R, et al. The role of music therapy in rehabilitation: improving aphasia and beyond. Int J Neurosci. 2018;128(1):90–99. doi:10.1080/00207454.2017.1353981
14. Liu Q, Li W, Yin Y, et al. The effect of music therapy on language recovery in patients with aphasia after stroke: a systematic review and meta-analysis. Neurol Sci. 2022;43(2):863–872. doi:10.1007/s10072-021-05743-9
15. Brady MC, Kelly H, Godwin J, Enderby P, Campbell P. Speech and language therapy for aphasia following stroke. Cochrane Database Syst Rev. 2016;2016(6):Cd000425. doi:10.1002/14651858.CD000425.pub4
16. Health and Social Care Delivery Research, Brady MC, Ali M, VandenBerg K, et al. Complex Speech-Language Therapy Interventions for Stroke-Related Aphasia: The RELEASE Study Incorporating a Systematic Review and Individual Participant Data Network Meta-Analysis. 2022. National Institute for Health and Care Research Copyright © King’s Printer and Controller of HMSO 2022. This work was produced by Brady et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health and Care Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK
17. Jin L, Zhang L, Zheng X, Zhao J, Yao B, Zhang X. Efficacy and safety profile of tDCS (Transcranial direct current stimulation) alongwith speech therapy in stroke patients with aphasia: a meta-analysis. Conference Abstract. In: Wiener Klinische Wochenschrift. 2024;136:S377. doi: 10.1007/s00508-024-02383-9
18. Hong Z, Zheng H, Luo J, et al. Effects of Low-Frequency Repetitive Transcranial Magnetic Stimulation on Language Recovery in Poststroke Survivors With Aphasia: an Updated Meta-analysis. Neurorehabil Neural Repair. 2021;35(8):680–691. doi:10.1177/15459683211011230
19. Goldsworthy MR, Pitcher JB, Ridding MC. A comparison of two different continuous theta burst stimulation paradigms applied to the human primary motor cortex. Clin Neurophysiol. 2012;123(11):2256–2263. doi:10.1016/j.clinph.2012.05.001
20. Hamilton RH, Chrysikou EG, Coslett B. Mechanisms of aphasia recovery after stroke and the role of noninvasive brain stimulation. Brain Lang. 2011;118(1–2):40–50. doi:10.1016/j.bandl.2011.02.005
21. Schlaug G, Marchina S, Wan CY. The use of non-invasive brain stimulation techniques to facilitate recovery from post-stroke aphasia. Neuropsychol Rev. 2011;21(3):288–301. doi:10.1007/s11065-011-9181-y
22. Ren CL, Zhang GF, Xia N, et al. Effect of low-frequency rTMS on aphasia in stroke patients: a meta-analysis of randomized controlled trials. PLoS One. 2014;9(7):e102557. doi:10.1371/journal.pone.0102557
23. Kielar A, Patterson D, Chou YH. Efficacy of repetitive transcranial magnetic stimulation in treating stroke aphasia: systematic review and meta-analysis. Clin Neurophysiol. 2022;140:196–227. doi:10.1016/j.clinph.2022.04.017
24. Gholami M, Pourbaghi N, Taghvatalab S. Evaluation of rTMS in patients with poststroke aphasia: a systematic review and focused meta-analysis. Neurol Sci. 2022;43(8):4685–4694. doi:10.1007/s10072-022-06092-x
25. Dang H, Chen J, Li J, Wu Y, Zeng Z. Effects of speech rehabilitation training combined with repetitive transcranial magnetic stimulation on patients with post-stroke aphasia. Clin Neurol Neurosurg. 2025;252:108833. doi:10.1016/j.clineuro.2025.108833
26. Xie L, Diao Y, Gong C, Huang J, Huang M, Dong Z. Efficacy and safety of repetitive transcranial magnetic therapy for post-stroke aphasia: a systematic review and meta-analysis of randomized controlled trials. Front Neurol. 2025;16:1614586. doi:10.3389/fneur.2025.1614586
27. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
28. Georgiou AM, Lada E, Kambanaros M. Evaluating the quality of conduct of systematic reviews on the application of transcranial magnetic stimulation (TMS) for aphasia rehabilitation post-stroke. Aphasiology. 2020;34(5):540–556.
29. Wang C, Nie P, Wang P, Wang Y, Zang Y, Zhang Y. The Therapeutic Effect of Transcranial Magnetic Stimulation on Post-stroke Aphasia and the Optimal Treatment Parameters: a Meta-analysis. Arch Phys Med Rehabil. 2024;105(7):1388–1398. doi:10.1016/j.apmr.2023.11.006
30. Ding X, Zhang S, Huang W, et al. Comparative efficacy of non-invasive brain stimulation for post-stroke aphasia: a network meta-analysis and meta-regression of moderators. Neurosci Biobehav Rev. 2022;140:104804. doi:10.1016/j.neubiorev.2022.104804
31. Ren J, Ren W, Zhou Y, et al. Personalized functional imaging-guided rTMS on the superior frontal gyrus for post-stroke aphasia: a randomized sham-controlled trial. Brain Stimul. 2023;16(5):1313–1321. doi:10.1016/j.brs.2023.08.023
32. Dai Y, Wang H, Fang Q, et al. Randomized controlled trial of theta burst stimulation modalities in severe post-stroke aphasia: examining the right hemisphere’s role. Neuroscience. 2025;585:198–205. doi:10.1016/j.neuroscience.2025.08.003
33. Dai Y, Fang Q, Wang H, et al. Impact of Right Cerebellar Theta Burst Stimulation on Post-Stroke Aphasia: a Randomized Controlled Trial. Arch Phys Med Rehabil. 2026. doi:10.1016/j.apmr.2025.12.012
34. Chou TY, Wang JC, Lin MY, Tsai PY. Low-Frequency vs. Theta Burst Transcranial Magnetic Stimulation for the Treatment of Chronic Non-fluent Aphasia in Stroke: a Proof-of-Concept Study. Front Aging Neurosci. 2021;13:800377. doi:10.3389/fnagi.2021.800377
35. Han C, Tang J, Tang B, Han T, Pan J, Wang N. The effectiveness and safety of noninvasive brain stimulation technology combined with speech training on aphasia after stroke: a systematic review and meta-analysis. Medicine. 2024;103(2):e36880. doi:10.1097/md.0000000000036880
36. Han C, Pan J, Du J, Feng L, Ma H, Tang J. Efficacy of different rehabilitation therapies on post-stroke aphasia patients: a network meta-analysis. Medicine. 2024;103(21):e38255. doi:10.1097/md.0000000000038255
37. Spigarelli M, Lalancette A, Massé-Alarie H, Wilson MA. Repetitive Transcranial Magnetic Stimulation for Action Naming in Aphasia Rehabilitation: a Systematic Review and Meta-Analysis. Brain Sci. 2024;14(7):665. doi:10.3390/brainsci14070665
38. Li P, Xiao R, Gong M, Jia P, Jin S. Efficacy of different types of transcranial magnetic stimulation on post-stroke aphasia patients: a network meta-analysis. Front Neurol. 2025;16:1597504. doi:10.3389/fneur.2025.1597504
39. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/m14-2385
40. Nespoulous JLA, Lafond D, Lemay A, Puel M, Joannette Y. Protocole Montréal-Toulouse d’examen linguistique de l’aphasie. 1992.
41. Turkstra LS. Western Aphasia Battery. 2018.
42. Huber W, Poeck K, Willmes K. The Aachen Aphasia Test. Adv Neurol. 1984;42:291–303.
43. Chung LS, Chang MH, Hsu TC. The Concise Chinese Aphasia Test and its application. J Speech Language Hearing Assoc. 1998;13:119–137.
44. Draper I. The assessment of aphasia and related disorders. J Neurol Neurosurg. 1973;36(5):894. doi:10.1136/jnnp.36.5.894-b
45. Kertesz A, Poole E. The aphasia quotient: the taxonomic approach to measurement of aphasic disability. Can J Neurol Sci. 1974;1(1):7–16. doi:10.1017/S031716710001951X
46. Kertesz A. Western Aphasia Battery--Revised. 2006.
47. Adams RJ, Meador KJ, Sethi KD, Grotta JC, Thomson DS. Graded neurologic scale for use in acute hemispheric stroke treatment protocols. Stroke. 1987;18(3):665–669. doi:10.1161/01.str.18.3.665
48. Hasegawa T, Kishi H, Shigeno K, et al. A study on aphasia rating scale: a method for overall assessment of SLTA results. High Brain Funct Res. 1984;4(2):638–646. doi:10.2496/apr.4.638
49. Tombaugh TN, Hubley AM. The 60-item Boston Naming Test: norms for cognitively intact adults aged 25 to 88 years. J Clin Exp Neuropsychol. 1997;19(6):922–932. doi:10.1080/01688639708403773
50. Tombaugh TN, Kozak J, Rees L. Normative data stratified by age and education for two measures of verbal fluency: FAS and animal naming. Arch Clin Neuropsychol. 1999;14(2):167–177.
51. Cardebat D, Doyon B, Puel M, Goulet P, Joanette Y. Formal and semantic lexical evocation in normal subjects. Performance and dynamics of production as a function of sex, age and educational level. Acta Neurol Belg. 1990;90(4):207–217. Evocation lexicale formelle et sémantique chez des sujets normaux. Performances et dynamiques de production en fonction du sexe, de l’âge et du niveau d’étude.
52. Aschenbrenner TSO, Lange KW. Regensburger Wort-flüssigkeits-Test. Hogrefe: Verlag für Psychologie; 2020.
53. De Renzi E, Faglioni P. Normative data and screening power of a shortened version of the Token Test. Cortex. 1978;14(1):41–49. doi:10.1016/s0010-9452(78)80006-9
54. Toğram IMB. Afazi Dil Değerlendirme Testi (ADD) Kullanım Yönergesi. Detay Yayıncılık; 2009.
55. Maviş İ, Tuncer AM, Selvi-Balo S, et al. The Adaptation of Comprehensive Aphasia Test (CAT) Into Turkish and the Development of Other Aphasia Assessment Tools in Turkish. 2020.
56. Szekely A, Jacobsen T, D’Amico S, et al. A new on-line resource for psycholinguistic studies. J Mem Lang. 2004;51(2):247–250. doi:10.1016/j.jml.2004.03.002
57. Granger CV, Hamilton BB, Linacre JM, Heinemann AW, Wright BD. Performance profiles of the functional Independence measure. Am J Phys Med Rehabil. 1993;72(2):84–89. doi:10.1097/00002060-199304000-00005
58. Blomert L. The Amsterdam — Nijmegen Everyday Language Test (ANELT). Berlin Heidelberg: Springer; 1992:121–127.
59. Snodgrass JG, Vanderwart M. A standardized set of 260 pictures: norms for name agreement, image agreement, familiarity, and visual complexity. J Exp Psychol Hum Learn. 1980;6(2):174–215. doi:10.1037//0278-7393.6.2.174
60. Hsiao V, Fernandes-Taylor S, Francis DO. Concerns Over Diagnostic Accuracy of Fine-Needle Biopsy in Thyroid Nodule Diagnosis-Reply. JAMA Surg. 2023;158(8):889–890. doi:10.1001/jamasurg.2023.0569
61. Sterne JA, Sutton AJ, Ioannidis JP, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343(jul22 1):d4002. doi:10.1136/bmj.d4002
62. Beets MW, Weaver RG, Ioannidis JPA, et al. Influence of pilot and small trials in meta-analyses of behavioral interventions: a meta-epidemiological study. Syst Rev. 2023;12(1):21. doi:10.1186/s13643-023-02184-7
63. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
64. Puhan MA, Schünemann HJ, Murad MH, et al. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2014;349:g5630. doi:10.1136/bmj.g5630
65. Brignardello-Petersen R, Bonner A, Alexander PE, et al. Advances in the GRADE approach to rate the certainty in estimates from a network meta-analysis. J Clin Epidemiol. 2018;93:36–44. doi:10.1016/j.jclinepi.2017.10.005
66. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
67. Brignardello-Petersen R, Mustafa RA, Siemieniuk RAC, et al. GRADE approach to rate the certainty from a network meta-analysis: addressing incoherence. J Clin Epidemiol. 2019;108:77–85. doi:10.1016/j.jclinepi.2018.11.025
68. Zeng L, Brignardello-Petersen R, Hultcrantz M, et al. GRADE Guidance 34: update on rating imprecision using a minimally contextualized approach. J Clin Epidemiol. 2022;150:216–224. doi:10.1016/j.jclinepi.2022.07.014
69. Turner RM, Davey J, Clarke MJ, Thompson SG, Higgins JP. Predicting the extent of heterogeneity in meta-analysis, using empirical data from the Cochrane Database of Systematic Reviews. Int J Epidemiol. 2012;41(3):818–827. doi:10.1093/ije/dys041
70. da Costa BR, Juni P. Systematic reviews and meta-analyses of randomized trials: principles and pitfalls. Eur Heart J. 2014;35(47):3336–3345. doi:10.1093/eurheartj/ehu424
71. Gelman A, Rubin DB. Inference from iterative simulation using multiple sequences. Stat Sci. 1992;7(4):457–472. doi:10.1214/ss/1177011136
72. Zumbansen A, Kneifel H, Lazzouni L, et al. Differential Effects of Speech and Language Therapy and rTMS in Chronic Versus Subacute Post-stroke Aphasia: results of the NORTHSTAR-CA Trial. Neurorehabil Neural Repair. 2022;36(4–5):306–316. doi:10.1177/15459683211065448
73. Zumbansen A, Black SE, Chen JL, et al. Non-invasive brain stimulation as add-on therapy for subacute post-stroke aphasia: a randomized trial (NORTHSTAR). Eur Stroke J. 2020;5(4):402–413. doi:10.1177/2396987320934935
74. Yaşa IC, Maviş I, Şalçini C, Midi I. Comparing the efficiency of speech and language therapy and transcranial magnetic stimulation for treating Broca’s aphasia. J Stroke Cerebrovasc Dis. 2023;32(6):107108. doi:10.1016/j.jstrokecerebrovasdis.2023.107108
75. Wang CP, Hsieh CY, Tsai PY, Wang CT, Lin FG, Chan RC. Efficacy of synchronous verbal training during repetitive transcranial magnetic stimulation in patients with chronic aphasia. Stroke. 2014;45(12):3656–3662. doi:10.1161/strokeaha.114.007058
76. Tsai PY, Wang CP, Ko JS, Chung YM, Chang YW, Wang JX. The persistent and broadly modulating effect of inhibitory rTMS in nonfluent aphasic patients: a sham-controlled, double-blind study. Neurorehabil Neural Repair. 2014;28(8):779–787. doi:10.1177/1545968314522710
77. Seniów J, Waldowski K, Leśniak M, Iwański S, Czepiel W, Członkowska A. Transcranial magnetic stimulation combined with speech and language training in early aphasia rehabilitation: a randomized double-blind controlled pilot study. Top Stroke Rehabil. 2013;20(3):250–261. doi:10.1310/tsr2003-250
78. Rubi-Fessen I, Hartmann A, Huber W, et al. Add-on Effects of Repetitive Transcranial Magnetic Stimulation on Subacute Aphasia Therapy: enhanced Improvement of Functional Communication and Basic Linguistic Skills. A Randomized Controlled Study. Arch Phys Med Rehabil. 2015;96(11):1935–44.e2. doi:10.1016/j.apmr.2015.06.017
79. Ren C, Zhang G, Xu X, et al. The Effect of rTMS over the Different Targets on Language Recovery in Stroke Patients with Global Aphasia: a Randomized Sham-Controlled Study. Biomed Res Int. 2019;2019:4589056. doi:10.1155/2019/4589056
80. Liu Q, Li W, Chen Y, et al. Effects of repetitive transcranial magnetic stimulation combined with music therapy in non-fluent aphasia after stroke: a randomised controlled study. Int J Lang Commun Disord. 2024;59(3):1211–1222. doi:10.1111/1460-6984.12991
81. Lin BF, Yeh SC, Kao YJ, Lu CF, Tsai PY. Functional Remodeling Associated With Language Recovery After Repetitive Transcranial Magnetic Stimulation in Chronic Aphasic Stroke. Front Neurol. 2022;13:809843. doi:10.3389/fneur.2022.809843
82. Lin BF, Hon F, Lin MY, Tsai PY, Lu CF. Right arcuate fasciculus as outcome predictor after low-frequency repetitive transcranial magnetic stimulation in nonfluent aphasic stroke. Eur J Neurol. 2023;30(7):2031–2041. doi:10.1111/ene.15808
83. Khedr EM, Abo El-Fetoh N, Ali AM, et al. Dual-hemisphere repetitive transcranial magnetic stimulation for rehabilitation of poststroke aphasia: a randomized, double-blind clinical trial. Neurorehabil Neural Repair. 2014;28(8):740–750. doi:10.1177/1545968314521009
84. Heiss WD, Hartmann A, Rubi-Fessen I, et al. Noninvasive brain stimulation for treatment of right- and left-handed poststroke aphasics. Cerebrovasc Dis. 2013;36(5–6):363–372. doi:10.1159/000355499
85. Bai G, Jiang L, Huan S, et al. Study on Low-Frequency Repetitive Transcranial Magnetic Stimulation Improves Speech Function and Mechanism in Patients With Non-fluent Aphasia After Stroke. Front Aging Neurosci. 2022;14:883542. doi:10.3389/fnagi.2022.883542
86. Low TA, Lindland K, Kirton A, et al. Transcranial Magnetic Stimulation Combined With Multimodality Aphasia Therapy for Chronic Poststroke Aphasia: a Randomized Clinical Trial. Neurology. 2025;104(6):e213424. doi:10.1212/wnl.0000000000213424
87. Dresang HC, Harvey DY, Vnenchak L, et al. Semantic and Phonological Abilities Inform Efficacy of Transcranial Magnetic Stimulation on Sustained Aphasia Treatment Outcomes. Neurobiol Lang. 2025;6:160. doi:10.1162/nol_a_00160
88. Bai G, Jiang L, Ma W, et al. Effect of Low-Frequency rTMS and Intensive Speech Therapy Treatment on Patients With Nonfluent Aphasia After Stroke. Neurologist. 2020;26(1):6–9. doi:10.1097/nrl.0000000000000303
89. Bai G, Jiang L, Li Q, Qiu P. Study on Intermittent Theta Burst Stimulation Improves Expression Function and Mechanism in Patients With Aphasia After Stroke. Neurologist. 2025;30(4):204–211. doi:10.1097/nrl.0000000000000622
90. Waldowski K, Seniów J, Leśniak M, Iwański S, Członkowska A. Effect of low-frequency repetitive transcranial magnetic stimulation on naming abilities in early-stroke aphasic patients: a prospective, randomized, double-blind sham-controlled study. ScientificWorldJournal. 2012;2012:518568. doi:10.1100/2012/518568
91. Thiel A, Hartmann A, Rubi-Fessen I, et al. Effects of noninvasive brain stimulation on language networks and recovery in early poststroke aphasia. Stroke. 2013;44(8):2240–2246. doi:10.1161/strokeaha.111.000574
92. Lee IT, Huang CC, Hsu PC, Lin CP, Tsai PY. Resting-State Network Changes Following Transcranial Magnetic Stimulation in Patients With Aphasia-A Randomized Controlled Study. Neuromodulation. 2022;25(4):528–537. doi:10.1016/j.neurom.2021.10.004
93. Zhang L, Lin B, Huang Y, et al. Speech and Language Therapy Plus Electroacupuncture or Non-Invasive Brain Stimulation for Post-Stroke Aphasia: a Systematic Review and Network Meta-Analysis. NeuroRehabilitation. 2025;56(3):302–314. doi:10.1177/10538135241312600
94. Peretz I, Vuvan D, Lagrois M, Armony JL. Neural overlap in processing music and speech. Philos Trans R Soc Lond B Biol Sci. 2015;370(1664):20140090. doi:10.1098/rstb.2014.0090
95. Ramaswamy M, Philip JL, Priya V, et al. Therapeutic use of music in neurological disorders: a concise narrative review. Heliyon. 2024;10(16):e35564. doi:10.1016/j.heliyon.2024.e35564
96. Naeser MA, Martin PI, Treglia E, et al. Research with rTMS in the treatment of aphasia. Restorat Neurol Neurosci. 2010;28(4):511–529. doi:10.3233/RNN-2010-0559
97. Berthier ML, Lambon Ralph MA. Dissecting the function of networks underpinning language repetition. Front Hum Neurosci. 2014;8:727. doi:10.3389/fnhum.2014.00727
98. Forkel SJ, Rogalski E, Drossinos Sancho N, et al. Anatomical evidence of an indirect pathway for word repetition. Neurology. 2020;94(6):e594–e606. doi:10.1212/wnl.0000000000008746
99. Tang Y, Jiao X, Wang J, et al. Dynamic Functional Connectivity Within the Fronto-Limbic Network Induced by Intermittent Theta-Burst Stimulation: a Pilot Study. Front Neurosci. 2019;13:944. doi:10.3389/fnins.2019.00944
100. Chang EF, Raygor KP, Berger MS. Contemporary model of language organization: an overview for neurosurgeons. J Neurosurg. 2015;122(2):250–261. doi:10.3171/2014.10.Jns132647
101. Crinion JT, Lambon-Ralph MA, Warburton EA, Howard D, Wise RJ. Temporal lobe regions engaged during normal speech comprehension. Brain. 2003;126(Pt 5):1193–1201. doi:10.1093/brain/awg104
102. Tilton-Bolowsky V, Stockbridge MD, Hillis AE. Remapping and reconnecting the language network after stroke. Brain Sci. 2024;14(5):419. doi:10.3390/brainsci14050419
103. Hartwigsen G, Saur D. Neuroimaging of stroke recovery from aphasia - Insights into plasticity of the human language network. Neuroimage. 2019;190:14–31. doi:10.1016/j.neuroimage.2017.11.056
104. Sheppard SM, Sebastian R. Diagnosing and managing post-stroke aphasia. Expert Rev Neurother. 2021;21(2):221–234. doi:10.1080/14737175.2020.1855976
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Efficacy of Various Acupuncture-Related Therapies for Post-Stroke Sleep Disorders: A Network Meta-Analysis of Randomized Controlled Trials
Lian J, Jiang Y, Kong L, Zhou M
Nature and Science of Sleep 2025, 17:1217-1229
Published Date: 9 June 2025