Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Transcranial Magnetic Stimulation Combined with Nursing Intervention in Children with Autism Spectrum Disorder and Its Effects on Developmental Quotient and Serum Neurotransmitters
Authors Chen X, Xia Y, Zhang M, Xie Y, Chen S, Hou F
Received 8 December 2025
Accepted for publication 21 February 2026
Published 17 March 2026 Volume 2026:19 587415
DOI https://doi.org/10.2147/JMDH.S587415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Xili Chen,1 Yun Xia,1 Mingyue Zhang,1 Ying Xie,1 Shuaimei Chen,1 Fang Hou2
1Pediatric Rehabilitation Department, Acupuncture, Massage and Rehabilitation Center, the First Affiliated Hospital of Hunan University of Chinese Medicine, Changsha, 410007, People’s Republic of China; 2Emergency Medicine Center, the First Affiliated Hospital of Hunan University of Chinese Medicine, Changsha, 410007, People’s Republic of China
Correspondence: Fang Hou, Email [email protected]
Objective: To evaluate the clinical efficacy and potential biological effects of transcranial magnetic stimulation (TMS) combined with rehabilitation nursing in children with autism spectrum disorder (ASD).
Methods: This retrospective controlled study included 90 children with ASD admitted between January 2023 and January 2025. Participants were divided into a control group (rehabilitation nursing only, n = 45) and an observation group (TMS combined with rehabilitation nursing, n = 45). Outcomes included Developmental Quotient assessed by the Gesell Developmental Schedules, autism-related behaviors assessed by the Autism Behavior Checklist, symptom severity assessed by the Autism Treatment Evaluation Checklist, quality of life assessed by the Pediatric Quality of Life Inventory, and serum neurotransmitter levels [glutamate (Glu) and γ-aminobutyric acid (GABA)].
Results: After intervention, both groups showed significant improvements in developmental quotient and quality of life, along with reductions in autism-related behaviors and symptom severity (all P < 0.05). Improvements were consistently greater in the observation group compared with the control group. In addition, serum Glu and GABA levels increased significantly after intervention in both groups, with a greater magnitude of change observed in the observation group (P < 0.05).
Conclusion: TMS combined with rehabilitation nursing may effectively promote developmental progress, alleviate behavioral symptoms, and improve quality of life in children with ASD, accompanied by increased serum Glu and GABA levels. These findings suggest that TMS may serve as a promising adjunctive intervention. Further multicenter randomized controlled trials with long-term follow-up are warranted to confirm efficacy, optimize stimulation parameters, and explore underlying mechanisms.
Keywords: transcranial magnetic stimulation, rehabilitation nursing, autism spectrum disorder, children, developmental quotient, serum neurotransmitters
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder with onset in early childhood, characterized primarily by deficits in social communication and interaction, restricted and repetitive patterns of behavior and interests, abnormal emotional responses, and sensory processing abnormalities.1 Epidemiological surveys2 indicate that the prevalence of ASD is increasing year by year, and it has become one of the common and far-reaching developmental disorders among children worldwide. The etiology and pathogenesis of ASD are complex. Studies3–5 suggest that genetic susceptibility, neurodevelopmental abnormalities, immune dysfunction, environmental factors, and imbalances in neurotransmitter metabolism jointly contribute to the occurrence and development of ASD. Currently, there is no cure for ASD; clinical interventions focus on rehabilitation training and behavioral therapy, including language rehabilitation, sensory integration training, social skills training, cognitive behavioral therapy, and parent education and guidance. These rehabilitation nursing measures, through systematic training stimulation, can to some extent promote neural plasticity in affected children and improve communication and social adaptation.6,7 However, due to the high heterogeneity of ASD in children, single rehabilitation nursing approaches often act slowly, have limited durability, and some children respond poorly to conventional rehabilitation. Therefore, exploring more effective adjunctive interventions has become a focus in clinical and research fields.Transcranial magnetic stimulation (TMS) is a non-invasive brain modulation technique that induces local currents via magnetic fields to alter cortical excitability and plasticity.8 Depending on the stimulation frequency, TMS can enhance or suppress activity in specific brain regions and thereby partially reorganize neural network connections. In recent years, TMS has been widely applied as an adjunctive treatment for depression, anxiety disorders, post-stroke functional impairment, and attention deficit hyperactivity disorder, showing good safety and feasibility.9–11 Some studies12,13 have found that TMS can improve language function, attention control, and social interaction abilities in children with ASD, possibly by modulating neurotransmitter balance, promoting synaptic plasticity, and improving neural circuit synchrony. When combined with rehabilitation nursing, TMS may achieve synergistic improvements in neural function and behavioral function through physiological neuromodulation and behavioral training. Especially during the developmental stage when the pediatric nervous system exhibits strong plasticity, TMS combined with rehabilitation nursing may exert more pronounced synergistic effects on cognitive, language, and social development. Based on these considerations, this study retrospectively analyzed 90 children with ASD treated at our hospital to systematically evaluate the comprehensive effects of adding TMS to routine rehabilitation nursing. We aim to provide new clinical evidence for multimodal intervention strategies for ASD and to offer reference directions for future individualized application and parameter optimization of TMS.
Materials and Methods
Study Design and Participants
This study adopted a retrospective controlled design to systematically evaluate the effects of TMS combined with rehabilitation nursing on developmental levels, autism-related behavioral symptoms, quality of life, and serum neurotransmitter levels in children with ASD. The study followed principles of scientific rigor, objectivity, and ethics. All data were obtained from the hospital’s electronic medical record system and rehabilitation assessment records. All assessments were conducted by certified evaluators who had received standardized training. A total of 90 children with ASD diagnosed and treated in the Department of Rehabilitation Medicine of our hospital from January 2023 to January 2025 were included. According to the intervention methods, the participants were divided into two groups: Control group (n = 45): Received conventional rehabilitation nursing only. Observation group (n = 45): Received TMS intervention in addition to the same conventional rehabilitation nursing as the control group. (1) Diagnostic criteria: Diagnosis was based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria for ASD,14 which require persistent deficits in social communication and interaction, restricted and repetitive patterns of behavior, and symptoms present in the early developmental period that impair daily functioning. Diagnoses were made by pediatric psychiatrists with an associate chief physician title or higher and were confirmed through consultation with two additional experts. (2) Inclusion criteria: ① Meeting the above diagnostic criteria; ② Age between 2 and 12 years, no restriction on sex; ③ Cognitive ability adequate for scale-based evaluation; ④ Completed a full 12-week rehabilitation program at our hospital; ⑤ Guardians provided informed consent and cooperated with the study procedures. (3) Exclusion criteria: ① Coexisting epilepsy or other organic neurological diseases; ② Severe sensory impairments (eg., hearing or visual deficits); ③ Presence of significant psychiatric disorders, genetic metabolic diseases, or structural brain abnormalities; ④ Use of antipsychotics or drugs affecting neurotransmitter levels; ⑤ Incomplete clinical data or poor treatment compliance. This study was approved by the Ethics Committee of the First Affiliated Hospital of Hunan University of Chinese Medicine (Approval No.: JSKXE25-LC04). Informed consent was obtained from all participants’ guardians. The research was conducted in accordance with the Declaration of Helsinki and relevant medical ethical standards. All patient information was anonymized during data collection and analysis to ensure privacy protection.
Intervention Methods
Control Group Intervention
Children in the control group received systematic conventional rehabilitation training, conducted by experienced rehabilitation therapists in a standardized rehabilitation setting. The entire intervention adhered to the principles of gradual progression and individualization, comprising the following modules: (1) Language training: Conducted one-on-one in a quiet and familiar environment. Therapists used picture cards, situational simulations, video demonstrations, and role-playing to stimulate the child’s interest in language. The training included basic vocalization, word imitation, phoneme recognition, and oral-motor coordination exercises. For children with articulation disorders, mirror imitation techniques were used to enhance awareness of speech production, gradually progressing to phrase and sentence expression. (2) Sensory integration training: Multisensory stimulation was applied to improve perception and response to external stimuli. Exercises involved stepping, rolling, crawling, and balancing on tactile mats, balance boards, and uneven surfaces to enhance vestibular and proprioceptive functions. Supplementary methods such as soft-brush tactile stimulation, alternating hot and cold exposure, and tactile ball massage were used to improve tactile sensitivity. Therapists also employed play-based activities such as ball passing, catching, and balance walking to strengthen hand-eye coordination and body balance. (3) Auditory and music training: For children with reduced auditory responsiveness or poor sound discrimination, an auditory stimulation system was used to play sounds of varying frequencies, rhythms, and directions, guiding the child to identify sound sources and tonal changes. When necessary, an auditory training device was employed for auditory correction. Additionally, music therapy was incorporated—therapists played upbeat or soothing music to encourage rhythmic imitation through clapping or nodding, promoting emotional relaxation and attention enhancement. (4) Social interaction and emotional expression training: A combined “music–movement–expression” approach was adopted to reinforce social communication. Therapists used song-based interaction, eye contact, and gesture imitation to enhance social responsiveness. Expression cards were used to help children recognize and express basic emotions such as happiness, anger, sadness, and fear, improving emotional understanding and interpersonal communication. (5) Behavioral analysis and individualized correction: Based on parent questionnaires, behavioral observation scales, and interview data, therapists analyzed behavioral issues, adaptive difficulties, and cognitive deficits to establish individualized intervention goals. Training began with single-skill exercises—such as maintaining attention or imitation training—and gradually transitioned to integrated multi-skill exercises, enabling children to generalize learned abilities to daily-life contexts. All training sessions were conducted by the same rehabilitation team, with each session lasting approximately 60 minutes, five times per week, for 12 consecutive weeks. Parents accompanied the children throughout each session to ensure compliance and safety.
Observation Group Intervention Measures
Children in the observation group received the same routine rehabilitation training as the control group, combined with rTMS therapy. (1) Equipment and parameter settings: Intervention was performed using an rTMS system produced by Nanjing Weisi Medical Technology Co., Ltd., Nanjing, China. The stimulation intensity was determined by a professional rehabilitation physician prior to the first session. The motor threshold (MT) was measured by placing surface electrodes on the skin over the abductor pollicis brevis (APB) muscle, with TMS stimulation applied to the contralateral motor cortex hand area (around C3 or C4). If at least 5 of 10 single-pulse stimulations evoked a motor evoked potential (MEP) amplitude ≥50 μV, the corresponding minimum output power was defined as the resting motor threshold (RMT). Unless otherwise specified, MT in this study refers to RMT. (2) Stimulation site and procedure: The dorsolateral prefrontal cortex (DLPFC) was selected as the stimulation target. After identifying the site that elicited the maximal MEP, the DLPFC location was determined by moving 4–5 cm forward horizontally. During treatment, the center of the circular stimulation coil was positioned over the DLPFC, with the coil parallel to the scalp surface. A low-frequency inhibitory protocol was used: frequency 1 Hz, stimulation intensity at 90% of RMT, 900 pulses per side of the DLPFC, with a total stimulation time of approximately 20 minutes per session. All treatments were administered by trained rehabilitation physicians to ensure accurate coil placement and uniform stimulation. (3) Treatment cycle and management: Each child received one session per day, with seven sessions comprising one treatment course. A 7-day interval was scheduled between courses, for a total of six courses (12 weeks). Throughout treatment, a dedicated staff member continuously monitored the child’s behavior and device output. In cases of discomfort, fear, or poor cooperation, a psychologist and the child’s parents jointly provided reassurance and behavioral guidance to ensure smooth treatment completion. (4) Safety and compliance management: During treatment, close observation was maintained for any transient discomfort such as scalp tingling, mild headache, or fatigue. If symptoms persisted, the treatment interval was extended or the stimulation intensity adjusted. No treatment interruptions or dropouts occurred during the study period, and all participants successfully completed the scheduled intervention cycles.
Observation Indicators and Evaluation Methods
The internal consistency indices (Cronbach’s α) reported for each scale were derived from previously validated studies and were not recalculated after each questionnaire administration in the present retrospective analysis.
- Developmental quotient: Before and after 12 weeks of intervention (after intervention), the Gesell Developmental Schedules (GDS; Cronbach’s α = 0.87, test-retest reliability = 0.82, content validity = 0.91)15 were used to assess the developmental quotient. The scale includes five dimensions—fine motor, gross motor, social, language, and adaptive abilities—each scored out of 100, with higher scores indicating better developmental function.
- Autistic behavior: Before and after intervention, the Autism Behavior Checklist (ABC; Cronbach’s α = 0.91, test-retest reliability = 0.86, content validity = 0.89)16 was used to assess autism-related behaviors. The scale includes five dimensions—language, sensory, self-care, social interaction, and physical movement—with 57 items in total. The total score ranges from 0 to 175, with higher scores indicating more severe autistic behaviors.
- Autism symptoms: Before and after intervention, the Autism Treatment Evaluation Checklist (ATEC; Cronbach’s α = 0.94, test-retest reliability = 0.88, content validity = 0.92)17 was used to assess autism-related symptoms. The scale includes four dimensions—health/physical/behavior, speech/language/communication, sensory/cognitive/awareness, and social—with 77 items in total. The total score ranges from 0 to 179, with higher scores indicating more severe symptoms.
- Quality of life: Before and after intervention, the Pediatric Quality of Life Inventory (PedsQL; Cronbach’s α = 0.89, test-retest reliability = 0.84, content validity = 0.95)18 was used to evaluate quality of life. The scale includes four dimensions—physical function, social function, role function, and emotional function—each scored out of 100, with higher scores indicating better quality of life.
- Serum neurotransmitters: Before and after intervention, 5 mL of fasting venous blood was collected from each child in the morning, centrifuged (3000 r/min, 10 min) to obtain serum, and stored at −80°C. Enzyme-linked immunosorbent assay (ELISA) kits for glutamate (Glu; catalog no. S11714) and γ-aminobutyric acid (GABA; catalog no. S10880) were obtained from Wuhan Saite Sen Biotechnology Co., Ltd., Wuhan, China. Each assay was performed strictly according to the manufacturer’s instructions, using 50 μL of serum per reaction. Standard curves were generated for each plate. Both positive and negative controls were included, and all samples were analyzed in duplicate to ensure assay reliability. Serum neurotransmitter measurements were used as peripheral biomarkers to reflect neurochemical changes, acknowledging that they may not fully represent central nervous system levels due to the presence of the blood–brain barrier.
Quality Control
All evaluators underwent standardized training and passed consistency testing (Kappa ≥ 0.80). Evaluation and data entry were performed in a double-blind manner to minimize subjective bias. All TMS procedures strictly followed safety guidelines, and contraindications were assessed prior to treatment.
Statistical Analysis
GraphPad Prism 8 was used for data visualization, and SPSS 25.0 was used for statistical analysis. Measurement data were tested for normality (Shapiro–Wilk test) and found to conform to a normal distribution, expressed as mean ± standard deviation ( ). Independent-samples t-test was used for between-group comparisons, and paired t-test was used for within-group comparisons before and after intervention. Categorical data were expressed as counts or percentages, and between-group comparisons were conducted using χ2-test or Fisher’s exact test. To account for multiple comparisons, Bonferroni correction was applied where appropriate. Adjusted P values < 0.05 were considered statistically significant.
). Independent-samples t-test was used for between-group comparisons, and paired t-test was used for within-group comparisons before and after intervention. Categorical data were expressed as counts or percentages, and between-group comparisons were conducted using χ2-test or Fisher’s exact test. To account for multiple comparisons, Bonferroni correction was applied where appropriate. Adjusted P values < 0.05 were considered statistically significant.
Results
Comparison of Baseline Data Between the Two Groups
There were no statistically significant differences between the two groups in terms of sex distribution, age, disease duration, or baseline disease severity (all P > 0.05, χ2-test or independent-samples t test), indicating good baseline comparability (Table 1).
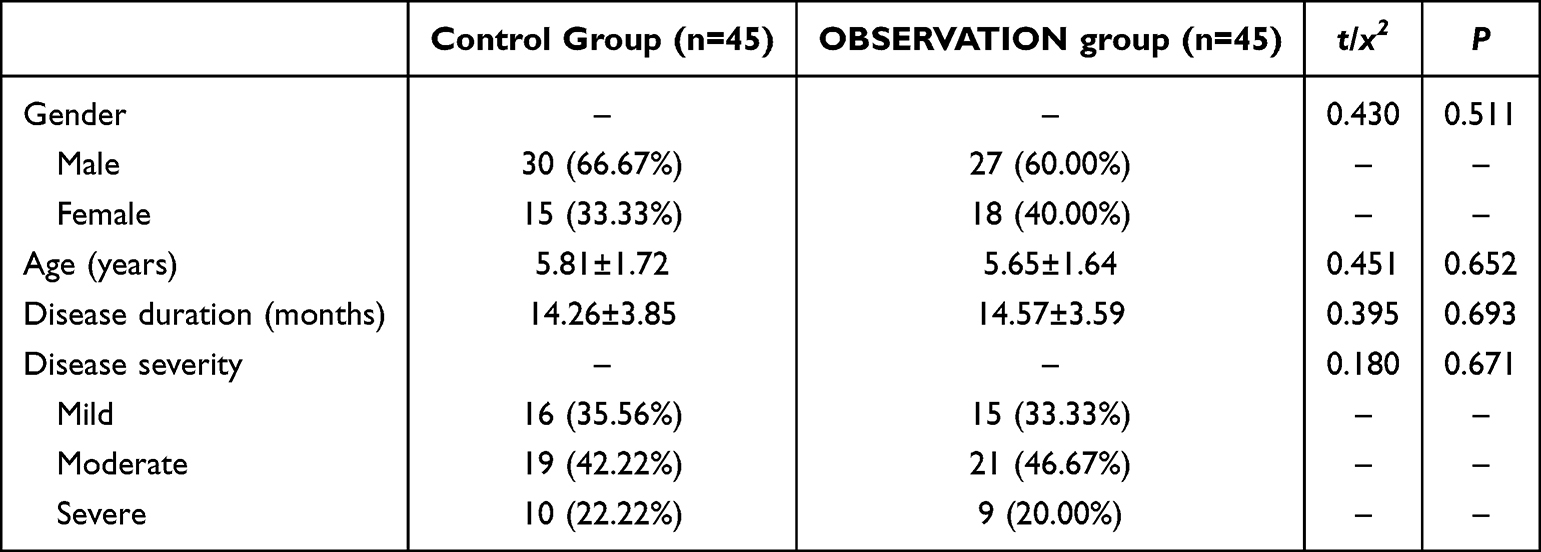 |
Table 1 Comparison of Baseline Data Between the Two Groups ( |

Comparison of Developmental Quotient Between the Two Groups
After intervention, both groups showed significant improvements in fine motor, gross motor, social, language, and adaptive behavior scores compared with baseline (paired t test, all Bonferroni-adjusted P < 0.05). Intergroup comparisons demonstrated significantly greater post-intervention improvements in the observation group than in the control group across all developmental domains (independent-samples t test, df = 88; fine motor: P = 0.030; gross motor: P = 0.001; social: P = 0.023; language: P = 0.032; adaptive behavior: P = 0.012; Table 2).
 |
Table 2 Comparison of Developmental Quotient Between the Two Groups ( |

Comparison of Autistic Behavior Between the Two Groups
Significant reductions in language, sensory, self-care, communication, and physical movement scores were observed in both groups after intervention (paired t test, all Bonferroni-adjusted P < 0.05). The observation group exhibited significantly greater reductions than the control group in all behavioral domains (independent-samples t test, df = 88; language: P < 0.001; sensory: P = 0.008; self-care: P < 0.001; communication: P < 0.001; physical movement: P < 0.001; Table 3).
 |
Table 3 Comparison of Autistic Behavior Between the Two Groups ( |

Comparison of Autism Symptoms Between the Two Groups
After intervention, scores for health/physical/behavior, speech/language/communication, sensory/cognitive/awareness, and socialization domains decreased significantly in both groups (paired t test, Bonferroni-adjusted P < 0.05). Post-intervention scores in the observation group were significantly lower than those in the control group for all symptom dimensions: health/physical/behavior (18.10 ± 3.54 vs. 21.71 ± 3.76, P < 0.001), speech/language/communication (13.41 ± 2.67 vs. 17.46 ± 2.89, P < 0.001), sensory/cognitive/awareness (16.51 ± 2.97 vs. 18.32 ± 3.12, P = 0.012), and socialization (15.46 ± 2.75 vs. 18.21 ± 3.24, P < 0.001) (all independent-samples t test, df = 88; Bonferroni-adjusted; Figure 1).


Comparison of Quality of Life Between the Two Groups
Both groups demonstrated significant post-intervention improvements in physical, social, role, and emotional functioning (paired t test, Bonferroni-adjusted P < 0.05). Compared with the control group, the observation group showed significantly higher post-intervention scores in physical functioning (77.02 ± 17.15 vs. 68.53 ± 15.39, P = 0.006), social functioning (58.94 ± 12.46 vs. 52.36 ± 11.62, P = 0.018), role functioning (52.59 ± 10.33 vs. 47.35 ± 9.46, P = 0.021), and emotional functioning (70.24 ± 16.43 vs. 62.19 ± 15.74, P = 0.010) (independent-samples t test, df = 88; Bonferroni-adjusted; Figure 2).


Comparison of Serum Neurotransmitters Between the Two Groups
After intervention, serum Glu and GABA levels increased significantly in both groups (paired t test, Bonferroni-adjusted P < 0.05). Post-intervention Glu levels were significantly higher in the observation group than in the control group (120.12 ± 4.93 vs. 101.52 ± 3.98 μmol/L, P < 0.001), as were GABA levels (2705.36 ± 223.86 vs. 2298.94 ± 360.73 pg/mL, P < 0.001) (independent-samples t test, df = 88; Bonferroni-adjusted; Figure 3).


Discussion
This study demonstrated that the Observation group receiving TMS combined with rehabilitation nursing achieved significantly greater improvement in multiple outcome indicators compared with the group receiving rehabilitation alone. Firstly, regarding developmental quotient, the Observation group exhibited markedly higher post-intervention scores in fine motor, gross motor, language, social, and adaptive abilities. This suggests that the addition of TMS can facilitate multidimensional developmental recovery in children within a short period. Mechanistically, TMS may transiently alter local cortical excitability and induce neuroplasticity, thereby enhancing functional connectivity in brain regions associated with sensorimotor coordination, language processing, and social cognition. Consequently, it may improve learning efficiency and the transfer effect of behavioral training. These findings are consistent with previous studies,19,20 which reported that rTMS targeting the prefrontal or parietal cortex improved attention and motor control, indirectly promoting motor skills and fine motor development. The observed enhancement in both language and social functions may be related to TMS-induced modulation of cortical networks involved in left-lateralized or bilateral language processing. The simultaneous improvement across all GDS domains in this study indicates that TMS may not act solely on a single functional module but rather promote a global reorganization of neural networks, amplifying the benefits of rehabilitation training. This aligns with the theoretical model of “low-dose neuromodulation plus behavioral training” as synergistic enhancers of neural plasticity.21
Regarding changes in autistic behaviors and symptoms, the Observation group showed more significant reductions in scores across the ABC and ATEC subscales (including language/communication, sensory response, somatic movement, and social interaction) compared with the Control group. This finding may be explained from two perspectives: (1) the direct regulatory effect of TMS on cortical excitability and subcortical circuits; and (2) the enhancement of behavioral intervention efficacy, allowing the behavioral changes consolidated through repetitive training to generalize more effectively to real-world contexts. Specifically, for sensory abnormalities and stereotyped behaviors, TMS may rebalance the regulatory interaction between sensory cortices and the prefrontal cortex, reducing hypersensitivity to external stimuli or compulsive repetitive patterns—reflected in decreased sensory and motor subscale scores. Previous studies22,23 reported that low- or medium-frequency rTMS targeting the prefrontal or parietal cortex can alleviate stereotyped behavior and emotional agitation. The improvement observed in this study supports those findings and provides new evidence on the combined use of TMS and systematic rehabilitation in children with ASD.
An equally important finding was the significant improvement in quality of life. The Observation group exhibited higher PedsQL scores across all dimensions (physical, emotional, social, and role functioning) compared with the Control group. These improvements not only reflect alleviation of functional symptoms but also enhancement of family and social participation. Mechanistically, TMS may mitigate core ASD symptoms such as social and language impairments, allowing children greater engagement and autonomy in daily life—thereby improving both subjective and objective measures of quality of life. Consistent with previous findings,24 behavioral improvements often parallel enhancements in quality of life, emphasizing that clinical outcomes should go beyond scale scores to focus on functional and family-level benefits.
Another key result was that serum Glu and GABA levels increased after intervention in both groups, with greater elevations in the Observation group. Although simultaneous upregulation of excitatory (Glu) and inhibitory (GABA) neurotransmitters may appear paradoxical, it likely reflects an overall enhancement of neural metabolic activity or a remodeling of the excitatory/inhibitory (E/I) balance system. TMS can modulate neuronal firing patterns, strengthen synaptic transmission, and induce plastic responses, leading to dynamic adjustments in neurotransmitter metabolism both locally and systemically. Prior studies25–27 have shown that rTMS can influence Gluergic and GABAergic balance, with effects depending on stimulation parameters and target regions; for example, low-frequency rTMS tends to suppress overexcited cortical regions, while high-frequency stimulation enhances cortical activity. Both mechanisms may ultimately drive Glu and GABA levels toward a more coordinated state. The concurrent elevation of both neurotransmitters in this study suggests that in children—a population characterized by high neuroplasticity—TMS may activate more neurons and metabolic pathways, reflected as increased serum neurotransmitter concentrations. Moreover, if the Glu/GABA ratio trends toward stabilization or reduction, it would further support the hypothesis of E/I balance restoration. Although peripheral serum levels may not directly mirror central neurotransmitter concentrations, their changes provide a quantifiable biological signal that, together with behavioral outcomes, strengthens the evidence that TMS exerts its effects via neurobiological mechanisms.
Beyond mechanism, integration of the present results with previous literature revealed several meaningful similarities and differences. In terms of language and social function improvement, our findings align with studies reporting rTMS-enhanced language ability in children with ASD;28,29 however, other studies30 have failed to find significant effects. Such discrepancies may arise from differences in sample characteristics, stimulation parameters (frequency, intensity, pulse number, target area), intervention duration, or whether behavioral training was combined. Our study applied short daily stimulation (seven sessions per course, twelve weeks total) alongside intensive conventional rehabilitation, and this “parallelized” design might have amplified TMS’s clinical efficacy. Thus, design variability should be considered when interpreting heterogeneous findings across studies. Similarly, in terms of sensory integration and stereotyped behavior, the positive outcomes observed here are consistent with certain studies,31–33 while more comprehensive improvements compared with studies using TMS alone highlight the clinical feasibility of the “neuromodulation plus behavioral training” synergistic model. Regarding safety and feasibility, no severe adverse events, treatment dropouts, or major compliance issues were observed, consistent with most pediatric rTMS reports. This suggests that, under strict screening and monitoring, low-frequency rTMS can be a well-tolerated adjunctive intervention. Nevertheless, the long-term safety of TMS in children requires further investigation with larger samples and extended follow-up, particularly given the developmental nature of the pediatric brain. Any long-term neuromodulatory intervention must be carefully evaluated for potential delayed effects.
Clinically, this study provides empirical support for integrated ASD interventions: incorporating appropriately parameterized TMS into conventional rehabilitation may amplify short-term therapeutic gains, enhance multidimensional developmental outcomes, and improve quality of life, accompanied by measurable neurobiological changes. These findings offer a reference for designing intervention protocols in clinical practice, suggesting that applying TMS during critical rehabilitation windows could enhance training sensitivity and learning generalization. However, individualized optimization of TMS parameters and coordination with rehabilitation schedules remain essential to achieve maximal benefits. Finally, several limitations should be noted. As a single-center retrospective study, potential selection bias and confounding factors cannot be excluded. The limited sample size and short follow-up restrict evaluation of long-term efficacy and delayed effects. Although serum Glu and GABA serve as valuable peripheral biomarkers, they cannot fully represent central neurotransmitter levels. Future studies should combine TMS with neuroimaging techniques such as magnetic resonance spectroscopy (MRS), functional MRI (fMRI), or electroencephalography (EEG) to more directly map the effects of TMS on brain function and network connectivity. Moreover, randomized, double-blind, placebo-controlled trials are needed to systematically compare the efficacy of different stimulation parameters, target combinations, and rehabilitation arrangements, as well as to identify patient subgroups most likely to benefit from TMS, thereby advancing precision rehabilitation.
Conclusion
This study demonstrates that short-term TMS combined with rehabilitation nursing yields multidimensional benefits in children with ASD, potentially mediated by modulation of neurotransmitter levels and enhancement of neural plasticity. These findings provide practical evidence supporting the integration of neuromodulation into ASD rehabilitation. However, to translate this approach into a long-term, safe, and widely applicable clinical strategy, further high-quality prospective studies and interdisciplinary mechanistic investigations are warranted.
Disclosure
The authors report no conflicts of interest in this work.
References
1. He YY, Wen CM, Yan YY, et al. Study on primary screening technique for children with autism spectrum disorder. Zhonghua Yu Fang Yi Xue Za Zhi. 2024;58(1):81–11. doi:10.3760/cma.j.cn112150-20230412-00285 Wolof
2. Du JB, Ding Y, Huang L, et al. The autism spectrum disorder cohort-the sub-cohort of China national birth cohort. Zhonghua Liu Xing Bing Xue Za Zhi. 2021;42(4):591–596. doi:10.3760/cma.j.cn112338-20201211-01405 Danish
3. Huang K, Zhang Y, Zhao R, et al. Advances in genetic research on autism spectrum disorders. Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2022;39(1):103–107. doi:10.3760/cma.j.cn511374-20201012-00710 Polish
4. Zhou YY, Fu QH. Advance in pathogenesis of oligodendrocytes-associated autism spectrum disorder. Zhonghua yu fang yi xue za zhi. 2022;56(9):1232–1237. doi:10.3760/cma.j.cn112150-20220529-00541
5. Liu X, Guo C, Zou M-Y, et al. Association between maternal gestational diabetes mellitus and the risk of autism spectrum disorder in offspring. Zhongguo Dang Dai Er Ke Za Zhi. 2023;25(8):818–823. doi:10.7499/j.issn.1008-8830.2301021 Xhosa
6. Franck N, Bon L, Dekerle M, et al. Satisfaction and needs in serious mental illness and autism spectrum disorder: the REHAbase psychosocial rehabilitation project. Psychiatr Serv. 2019;70(4):316–323. doi:10.1176/appi.ps.201800420
7. Zhang L, Liu Y, Zhou Z, et al. A follow-up study on the long-term effects of rehabilitation in children with autism spectrum disorders. NeuroRehabilitation. 2019;44(1):1–7. doi:10.3233/NRE-182502
8. Wang HX, Liu XL. Strategies for applying noninvasive brain stimulation techniques to treat psychiatric disorders. Zhonghua Yi Xue Za Zhi. 2024;104(41):3785–3791. doi:10.3760/cma.j.cn112137-20240524-01185
9. Qi C, Zhao JH, Wei YR, et al. Observation on the efficacy of different targets low-frequency repetitive transcranial magnetic stimulation for the treatment of tremor-dominant subtypes of Parkinson’s disease. Zhonghua Yi Xue Za Zhi. 2023;103(39):3112–3118. doi:10.3760/cma.j.cn112137-20230629-01102 Danish
10. Yang YF, Jin B, Liu LZ, et al. Changes of brain network characteristics in patients with depression before and after precise repetitive transcranial magnetic stimulation. Zhonghua Yi Xue Za Zhi. 2022;102(43):3449–3456. doi:10.3760/cma.j.cn112137-20220415-00813 Danish
11. Wu S, Zhang J, Zhang F, et al. Effect of MEP-oriented scalp acupuncture combined with transcranial magnetic stimulation on limb motor ability in patients with ischemic stroke hemiplegia. Zhongguo Zhen Jiu. 2024;44(3):251–254. doi:10.13703/j.0255-2930.20230520-k0003
12. Masuda F, Nakajima S, Miyazaki T, et al. Motor cortex excitability and inhibitory imbalance in autism spectrum disorder assessed with transcranial magnetic stimulation: a systematic review. Transl Psychiatry. 2019;9(1):110. doi:10.1038/s41398-019-0444-3
13. Casanova MF, Sokhadze EM, Casanova EL, et al. Transcranial magnetic stimulation in autism spectrum disorders. Neuropathologic Underpinning Clin Correlations Semin Pediatr Neurol. 2020;35:100832. doi:10.1016/j.spen.2020.100832
14. Kaba D, Soykan Aysev A. Evaluation of autism spectrum disorder in early childhood according to the DSM-5 diagnostic criteria. Turk Psikiyatri Derg. 2020;31(2):106–112. doi:10.5080/u23735
15. Wang LJ, Wang HM, Meng YQ, et al. Association between cord blood BPDE-DNA and neurodevelopment of children aged 0 and 2 years: a birth cohort study. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. 2022;40(6):412–418. doi:10.3760/cma.j.cn121094-20210413-00202 Dutch
16. Huang MX, Yu Q, Li YY. A prospective randomized controlled study of neurofeedback combined with learning style profile intervention training in children with high-functioning autism. Zhongguo Dang Dai Er Ke Za Zhi. 2024;26(10):1066–1071. doi:10.7499/j.issn.1008-8830.2405054 Xhosa
17. Netson R, Schmiedel Fucks A, Schmiedel Sanches Santos A, et al. A comparison of parent reports, the mental synthesis evaluation checklist (MSEC) and the autism treatment evaluation checklist (ATEC), with the childhood autism rating scale (CARS). Pediatr Rep. 2024;16(1):174–189. doi:10.3390/pediatric16010016
18. Katsiana A, Strimpakos N, Ioannis V, et al. Health-related quality of life in children with autism spectrum disorder and children with down syndrome. Mater Sociomed. 2020;32(2):93–98. doi:10.5455/msm.2020.32.93-98
19. Li JM, Huang JP, Liu JH. Effect of electroacupuncture combined with motor training on motor learning and motor cortex excitability. Zhongguo Zhen Jiu. 2021;41(12):1365–1369. doi:10.13703/j.0255-2930.20210303-k0007 Dutch
20. Yin ZL, Ge S, Huang L-H, et al. Acupuncture combined with repetitive transcranial magnetic stimulation for post-stroke depression: a randomized controlled trial. Zhongguo Zhen Jiu. 2022;42(11):1216–1220. doi:10.13703/j.0255-2930.20211221-0002 Dutch
21. Sheng Y, Wang J, Tan G, et al. Muscle synergy plasticity in motor function recovery after stroke. IEEE Trans Neural Syst Rehabil Eng. 2024;32:1657–1667. doi:10.1109/TNSRE.2024.3389022
22. Smilovich AA, Nelyubova ES, Kolsanov AV, et al. Comprehensive treatment of adynamic depression with the combined use of traditional psychopharmacotherapy, transcranial magnetic stimulation and virtual reality technologies. Zh Nevrol Psikhiatr Im S S Korsakova. 2023;123(11):75–81. doi:10.17116/jnevro202312311175 Hungarian
23. Aftanas LI, Brack IV, Kulikova KI, et al. Clinical and neurophysiological effects of dual-target high-frequency rTMS over the primary motor and prefrontal cortex in Parkinson’s disease. Zh Nevrol Psikhiatr Im S S Korsakova. 2020;120(5):29–36. doi:10.17116/jnevro202012005129 Hungarian
24. Zhang -J-J, Wang E-N. Enhancing autism care through remote support: a family-centered approach. World J Psychiatry. 2025;15(4):102645. doi:10.5498/wjp.v15.i4.102645
25. Pecsok MK, Mordy A, Cristancho MA, et al. The glutamatergic effects of clinical repetitive transcranial magnetic stimulation in depressed populations: a preliminary meta-analysis of proton magnetic resonance spectroscopy studies. Psychopathology. 2024;57(4):318–33.
26. Gonsalves MA, White TL, Barredo J, et al. Repetitive transcranial magnetic stimulation-associated changes in neocortical metabolites in major depression: a systematic review. Neuroimage Clin. 2022;35:103049. doi:10.1016/j.nicl.2022.103049
27. Vural G, Soldini A, Padberg F, et al. Exploring the effects of prefrontal transcranial direct current stimulation on brain metabolites: a concurrent tDCS-MRS study. Hum Brain Mapp. 2024;45(18):e70097. doi:10.1002/hbm.70097
28. Savino R, Davinelli S, Polito AN, et al. Repetitive transcranial magnetic stimulation in children and adolescents with autism spectrum disorder: study protocol for a double-blind, sham-controlled, randomized clinical trial. Trials. 2025;26(1):240. doi:10.1186/s13063-025-08946-z
29. Minghui Q, Wang Y, Chen B, et al. The effects of rTMS and tDCS on repetitive/stereotypical behaviors, cognitive/executive functions in intellectually capable children and young adults with autism spectrum disorder: a systematic review and meta-analysis of randomized controlled trials. Res Dev Disabil. 2025;164:105076. doi:10.1016/j.ridd.2025.105076
30. Luckhardt C, Boxhoorn S, Schuetz M, et al. Brain stimulation by tDCS as treatment option in autism spectrum disorder-a systematic literature review. Prog Brain Res. 2021;264:233–257.
31. Zemestani M, Hoseinpanahi O, Salehinejad MA, et al. The impact of prefrontal transcranial direct current stimulation (tDCS) on theory of mind, emotion regulation and emotional-behavioral functions in children with autism disorder: a randomized, sham-controlled, and parallel-group study. Autism Res. 2022;15(10):1985–2003. doi:10.1002/aur.2803
32. Molavi P, Aziziaram S, Basharpoor S, et al. Repeated transcranial direct current stimulation of dorsolateral-prefrontal cortex improves executive functions, cognitive reappraisal emotion regulation, and control over emotional processing in borderline personality disorder: a randomized, sham-controlled, parallel-group study. J Affect Disord. 2020;274:93–102. doi:10.1016/j.jad.2020.05.007
33. Quirke T, Sleator RD. A beginner’s guide to genomics in complex neurological disorders. Innov Discov. 2024;1(4):29. doi:10.53964/id.2024029
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Sandplay Therapy on Children with Autism Spectrum Disorder: A Systematic Review and Meta-Analysis
Wu X, Zhao X, Meng Y, Huang L, Xie L, Huang S, Yang J, Song Y
Neuropsychiatric Disease and Treatment 2026, 22:579433
Published Date: 26 March 2026