Back to Journals » Journal of Pain Research » Volume 16
Transcranial Magnetic Stimulation as a Therapy for Migraine: An Overview of Systematic Reviews
Authors Shen M, Li C, Wei X, Zhang L, Li Y, Wu H, Zhang X, Dong Z, Gao S, Ma Y, Ma Y
Received 13 April 2023
Accepted for publication 5 September 2023
Published 13 September 2023 Volume 2023:16 Pages 3133—3144
DOI https://doi.org/10.2147/JPR.S416993
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Alexandre F DaSilva
Min Shen,1 Chunjing Li,1 Xiaocen Wei,1 Linlin Zhang,1 Yang Li,1 Hongxue Wu,2 Xiaobin Zhang,1 Zhibin Dong,1 Shuzhong Gao,1 Yuning Ma,1 Yuxia Ma1
1Department of Acupuncture and Massage College, Shandong University of Traditional Chinese Medicine, Jinan, People’s Republic of China; 2Department of Rehabilitation, The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
Correspondence: Yuning Ma; Yuxia Ma, Email [email protected]; [email protected]
Introduction: This overview of systematic reviews (SRs) systematically collected, evaluated, and combined the evidence for migraine treatment with transcranial magnetic stimulation (TMS).
Methods: We conducted a systematic literature search in various databases, such as PubMed, The Cochrane Library, Web of Science, Embase, the China National Knowledge Infrastructure, Wanfang, VIP, and China Biomedical Literature. Two reviewers independently assessed the methodological quality, risk of bias, reporting quality, and strength of evidence of the included studies using AMSTAR-2, ROBIS, the PRISMA checklist, and the GRADE system.
Results: We performed an overview of 7 relevant SRs, of which 4 were of moderate quality and 3 were of low quality according to AMSTAR 2. All SRs had low risk of bias in Phase 1 (Assessing relevance), Domain 1 (Study eligibility criteria), and Domain 4 (Synthesis and findings) as evaluated by ROBIS. In Domain 2 (Identification and selection of studies), 4 SRs (57.1%) had low risk of bias, while in Domain 3 (data collection and study appraisal) and Risk of Bias in the Review Phase 3, 4 SRs (57.1%) had low risk of bias. The PRISMA reporting standards were generally comprehensive, but some limitations were observed in the assessments, pooled results, evidence reliability, registration and protocols, and funding sources. The GRADE levels ranged from moderate to low, with 10 outcomes of moderate quality and 6 outcomes of low quality. The main reason for the low quality of evidence was the small sample size and high heterogeneity of the available studies.
Conclusion: TMS may improve migraine severity and frequency, but the evidence is limited due to methodological flaws and heterogeneity. Future studies should standardize use, assess side effects, and compare with other treatments.
Keywords: transcranial magnetic stimulation, migraine, evidence, overview, systematic reviews
Introduction
Migraine is a common neurological disorder characterized by recurrent moderate to severe headaches and is often accompanied by other symptoms, such as nausea, vomiting, and sensitivity to light and sound.1 Such symptoms affect approximately 12% of general population and are more prevalent in females than males.2,3 The pathophysiology of migraine is complex, with cortical spreading depression (CSD) as a key event leading to central and peripheral sensitization.4 CSD involves a depolarization wave followed by a slower neural inhibition wave, which typically develops in the occipital cortex and spreads to other cortical areas at a speed of 3–6 mm/minute.5 TMS is a technique that uses brief magnetic pulses on the scalp to stimulate the brain tissue below.6 This technique is non-invasive, meaning it does not require surgery or implants. A variation of TMS, called rTMS, delivers repeated pulses that can change the activity and adaptability of the brain area being stimulated.7 TMS and rTMS may affect CSD by altering the balance of excitation and inhibition in the brain’s cortex. The most common side effects of TMS and rTMS are mild headache, scalp discomfort, and temporary hearing impairment.8,9
In recent years, neuroregulation devices, such as transcranial magnetic stimulation (TMS) has gained wide recognition as an option for treating migraines.10–12 In order to suppress or alleviate migraine symptoms, TMS has been developed to target CSD through disrupting the propagation of electrical activity during migraine attacks via magnetic field stimulation of specific areas of the brain.13 Considering its role in inhibiting CSD, there is growing interest in using TMS to treat migraines.14–17 This overview of SRs/MAs is, to the best of our knowledge, the first one to systematically collect, appraise, and synthesize the evidence on the efficacy and safety of TMS for migraine treatment, while addressing the methodological quality and heterogeneity of the included SRs/MAs.
Several SRs and MAs have been conducted to assess the effectiveness and safety of TMS for migraine management.18–24 However, not all SRs can provide reliable evidence, and low-quality evidence can mislead clinical decision-making. Therefore, an overview that summarizes the current evidence on the efficacy and safety of TMS for migraine treatment is needed. Moreover, this overview can serve as a user-friendly tool for healthcare professionals and patients with migraine by presenting the results of SRs/MAs in a unified format and minimizing information redundancy. The results of this overview can inform clinical decision-making and guideline development for the use of TMS in migraine management, as well as identify knowledge gaps and research priorities for future studies.
Methods
Registration and Protocol
The methodology of this study followed the Cochrane manual.25 The PROSPERO database had this protocol listed as registered (CRD42021287635).
Inclusion and Exclusion Criteria
The inclusion criteria for the SRs/MAs were as follows: (1) SRs/MAs that synthesized the evidence from RCTs on TMS treatment for migraine prevention, regardless of the type, site, frequency, or intensity of TMS stimulation; (2) Migraine of any type that met the diagnostic criteria in the included RCTs; (3) TMS as an intervention of interest for migraine treatment, with a control group consisting of placebo or conventional medication; and (4) Clinical outcomes that measured headache intensity, headache frequency, clinical effectiveness, and adverse events.
The exclusion criteria were as follows: (1) Reviews including non-RCTs; (2) Reviews involving patients with Tension headache; (3) Reviews that were not efficacy evaluations; and (4) Studies without complete data, such as conference abstracts, letters or comments.
Search Methods for Identification of Reviews
From the inception of each database to February 28, 2023, searches were conducted on various databases including The China National Knowledge Infrastructure (CNKI), Wanfang, VIP, China Biomedical Literature (CBM), PubMed, the Cochrane Library, Web of Science and Embase. Systematic reviews related to the subject were also retrieved in order to locate more relevant studies. Specific search strategies were modified in different databases. Table 1 displays the Medicine database search strategy employed in this study.
 |
Table 1 Search Strategy for the Medicine Database |
Evaluation of Eligibility and Data Extraction
Two authors conducted literature review and independently extracted data. The retrieved literature was imported into Endnote X9 after eliminating duplicates. Titles and abstracts of the literature were read to determine whether the studies those met the inclusion criteria. For final inclusion, full texts of the selected literature were carefully read and analyzed. Information such as author name, publication year, country, enrolled trials, sample size, quality assessment techniques used, interventions and comparisons made in each study along with primary outcomes and data synthesis techniques employed were extracted from all the included studies.
Quality Assessment
The Assessment of Multiple Systematic Reviews 2 (AMSTAR2) tool,26 the Risk of Bias in Systematic Reviews (ROBIS),27 the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist,28 and the Grading of Recommendations Assessment, Development and Evaluation (GRADE)29 system were independently applied by the two authors to evaluate methodological quality, Risk of bias, reporting quality, and evidence quality. Seven of the 16 items in AMSTAR-2 were considered to be key items (2, 4, 7, 9, 11, 13, and 15). ROBIS includes 3 phases with Phase 2 containing 4 domains. Each of the 27 items in PRISMA is given a rating of “not reported”, “completely reported”, or “partially reported”. The GRADE system evaluates evidence quality from five aspects: limitations, imprecision, indirectness, inconsistency, and publication bias for SRs/MAs results.
Graphical Representation of Overlap for OVErviews
We used Excel spreadsheets to extract the studies contained in each summary to explore literature overlap and conduct evaluations. The Graphical Overview of Evidence (GROOVE)30 is an easy-to-use tool and its calculation of evidence matrix and corrected covered area (CCA) may be one of the most comprehensive methods for measuring overlap. GROOVE uses statistical methods to calculate CCA coverage area and provides an overall interpretation of overlap assessment, which is considered slight if CCA <5%, moderate if it is between 5% and <10%, high if it is between 10% and <15%, and very high if CCA is 15% or higher.30
Results
Results on Literature Selection
A total of 103 literature papers were found, of which 84 were excluded after reviewing their abstracts and titles. The remaining studies were carefully read in full, and 12 of them were subsequently excluded. Finally, 7 studies were considered as meeting our inclusion criteria.18–24 A flow chart of literature selection is shown in Figure 1.
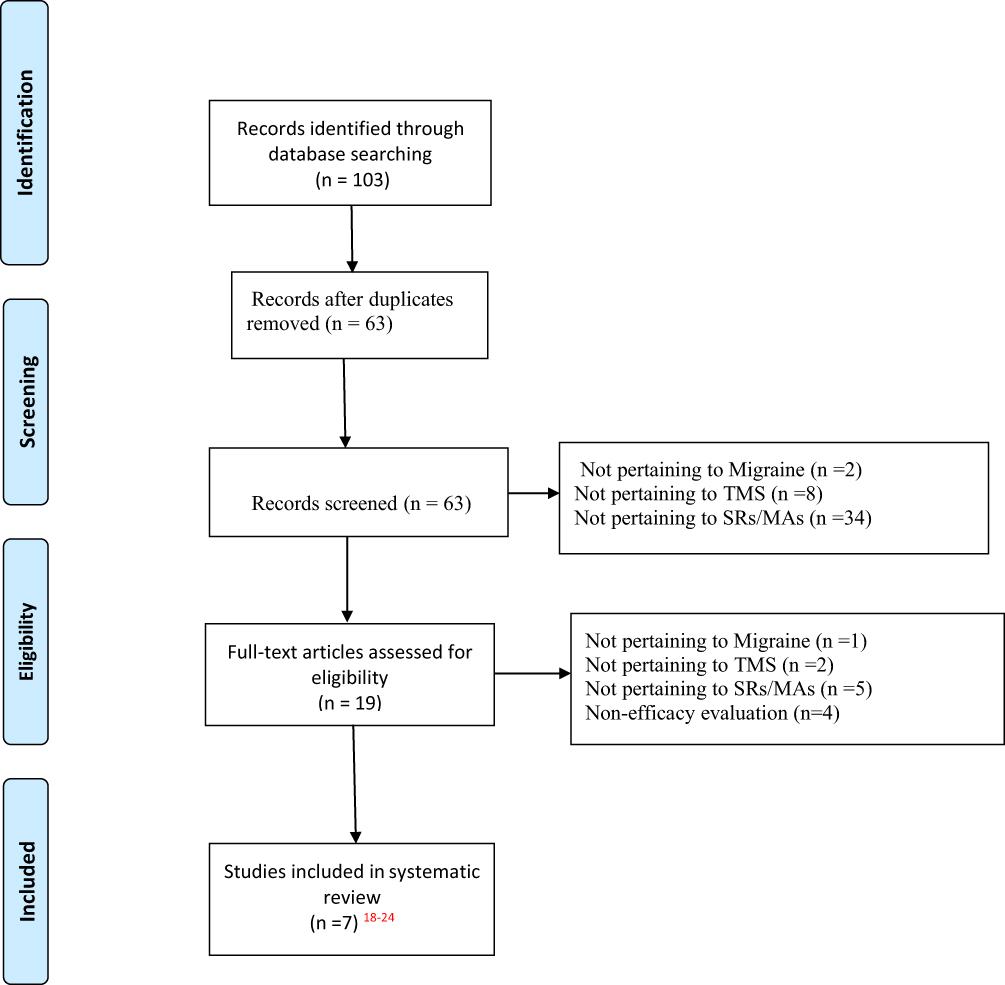 |
Figure 1 Flow-chart of study selection. |
Characteristics of the Included Studies
This overview includes research published from 2016 to 2022. In all the SRs/MAs, the search scope was limited to RCT design. The SRs/MAs contained 3 to 9 RCTs, and the sample sizes ranged from 39 to 452. Regarding the nationality of the first author, 5 articles were published by Chinese authors, 1 article was published by a Finnish author, and 1 article was published by a Malaysian author. The interventions varied slightly. Six articles used rTMS technology, while 1 article used TMS (not specifically classified). For the control group, all the literature was compared using sham stimulation. When evaluating original literature quality, 5 articles used Cochrane bias risk standards, 1 article used PEDro method, and another article used an unknown method. For specific details please refer to Table 2.
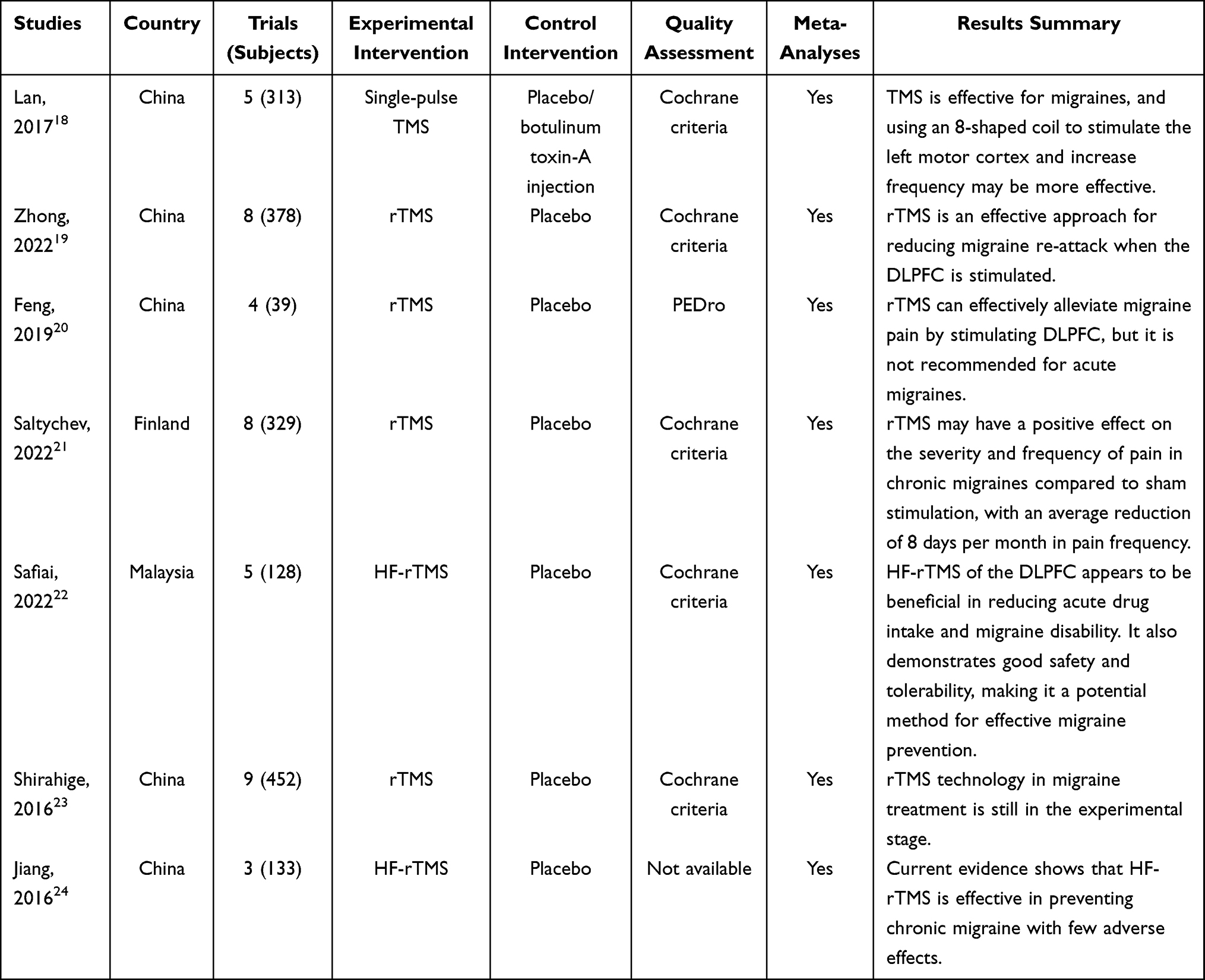 |
Table 2 Characteristics of the Included Reviews |
Methodological Quality of the Included SRs
Table 3 displays the results of evaluating methodological quality using the AMSTAR 2 tool. Among the 7 SRs, 4 were rated as moderate quality19,21–23 and 3 were rated as low quality18,20,24 It was worth noting that items 2 and 7 received poor ratings. All the SRs included PICO components and 419,21–23 reported study protocols in advance. However, none of them provided a comprehensive list of excluded studies with exclusion reasons. Additionally, 1 SR24 did not report funding source for the included studies.
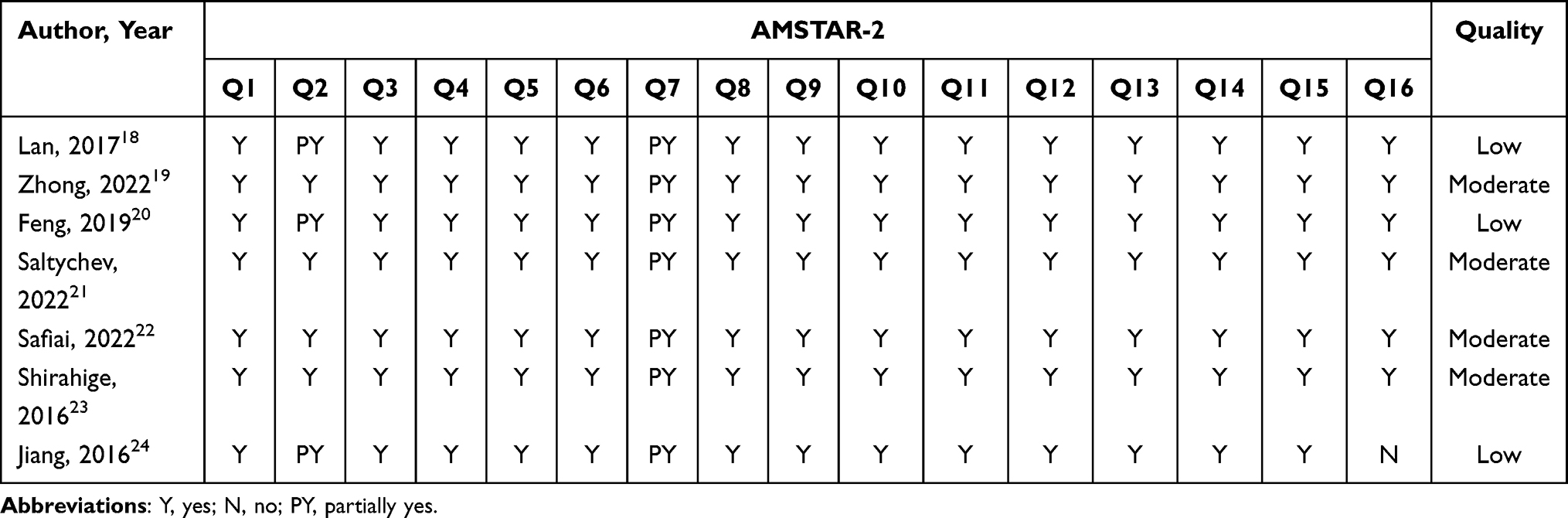 |
Table 3 Quality Assessment of the Included Reviews by the AMSTAR-2 Tool |
Risk of Bias of the Included SRs
According to ROBIS, all systematic reviews (100%) were assessed as low risk in Phase 1 (assessment of relevance), Domain 1 (eligibility criteria), and Domain 4 (synthesis and findings) as shown in Table 4. For Domain 2, 4 systematic reviews (57.1%), which focus on the identification and selection of studies, were classified as low risk. Similarly, 4 systematic reviews (57.1%), which focus on data gathering and study evaluation, were rated as low risk for Domain 3. Finally, four systematic reviews (57.1%) were considered as low risk (Table 4) and belonged to the Phase 3 (Risk of bias in the review).
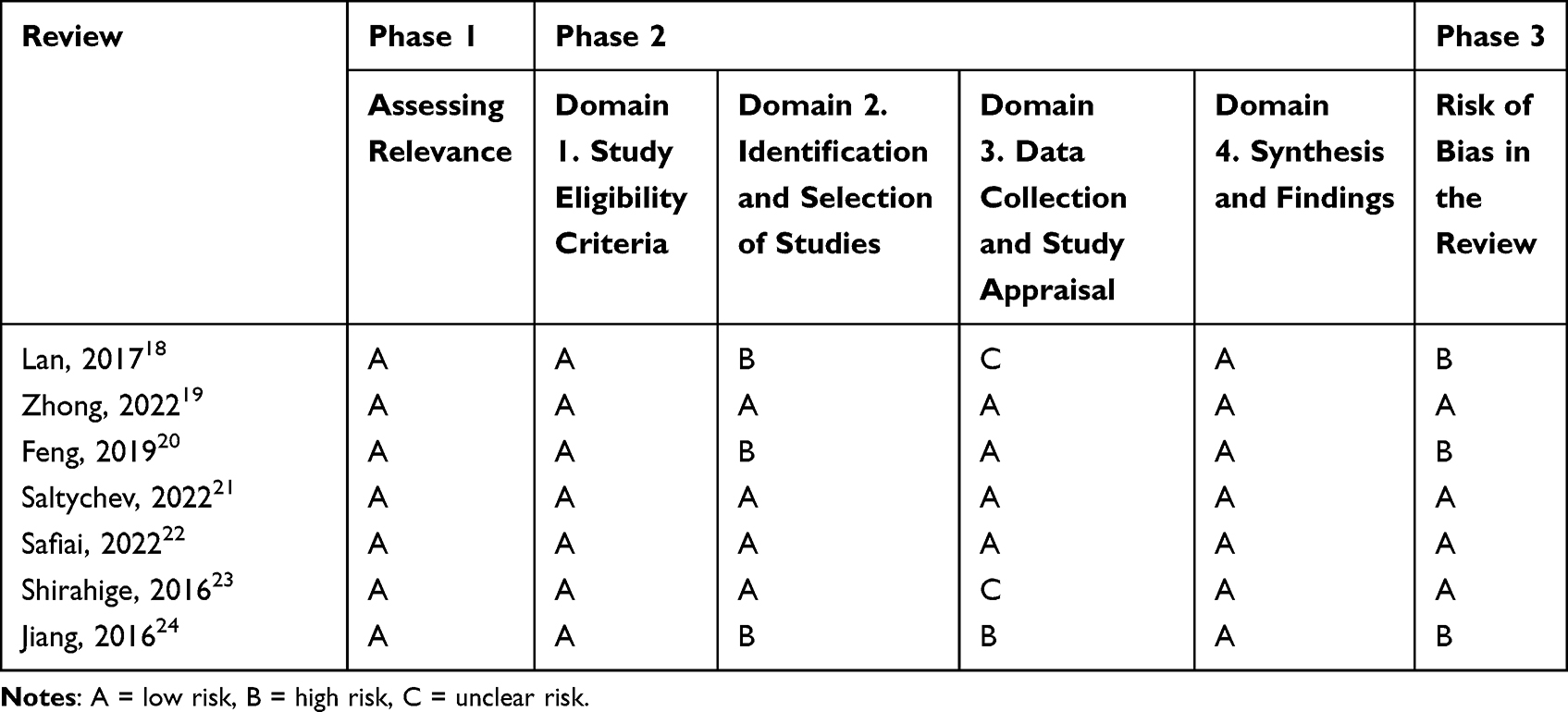 |
Table 4 Results of Risk of Bias in Systematic Reviews (ROBIS) |
Reporting Quality of the Included SRs
The reports included in the study met satisfactory standards for all 27 items on the PRISMA checklist. Only 3 studies met all the requirements for every item. Most of the included studies adequately reported on most items, with over a half achieving a completion rate of 100%. However, some specific details were more challenging to achieve. For instance, only 4 studies completed review protocols and provided registration information and numbers (item 24a). Additionally, item 20d (synthesis of results) had a lower completion rate at 57.1% when compared to retrieval completion rates. Some other items, such as items 15, 22 and 25 did not reach a completion rate of 100% (Table 5).
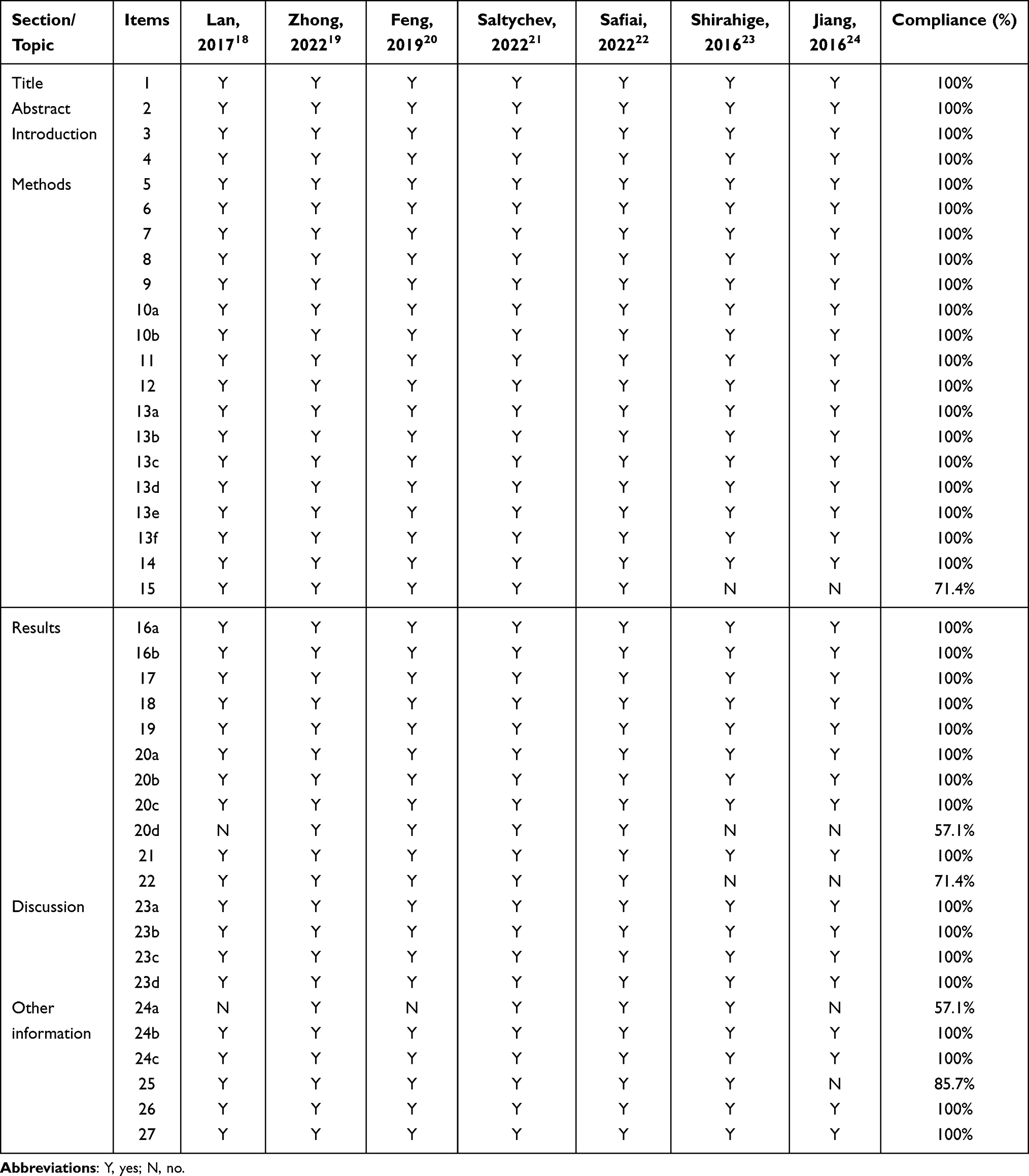 |
Table 5 Results of the Reporting Quality |
Results of the Evidence Quality Assessment
Table 6 summarizes the quality of evidence in the research results using the GRADE system. Out of 16 outcome indicators, none were rated as high-quality confidence, while 10 (62.5%) were rated as moderate-quality confidence and the remaining 6 (37.5%) were rated as low-quality confidence. The primary reasons for downgrading the quality of evidence were small sample sizes and a high level of consistency among the existing studies.
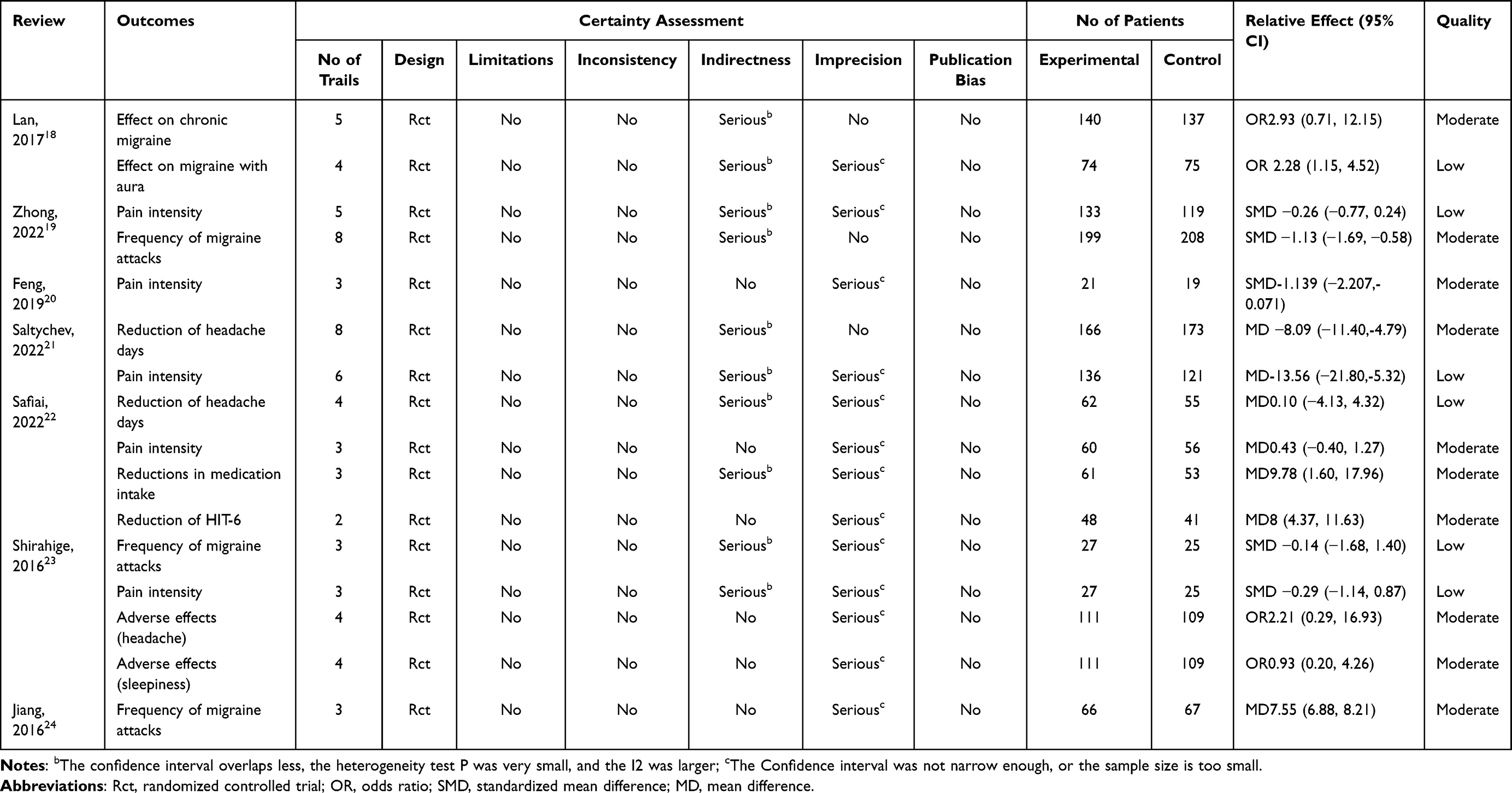 |
Table 6 Results of Evidence Quality |
Overlap Between the Included Reviews
The OVErviews visuals highlighted potential overlaps between each pair of SR/MA in addition to computing the overall CCA. With a total of 21 nodes and considerable overlap throughout the contained comments, we discovered that 7 showed slightly overlapping, 1 showed moderately overlapping, 2 showed highly overlapping, and 11 showed heavily overlapping. For more detailed information please refer to Figure 2.
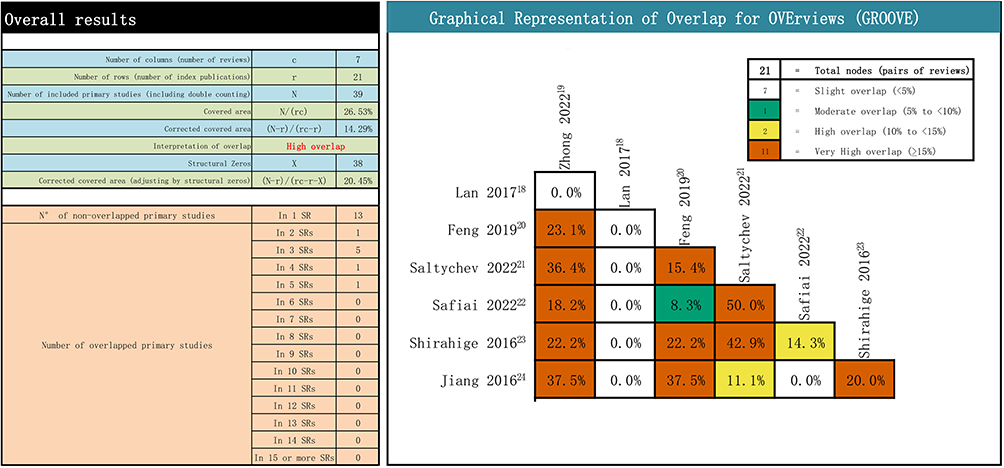 |
Figure 2 Overlapping of the included reviews. |
Efficacy and Safety of Interventions
One SRs18 evaluated the acute relief effect of TMS compared to sham stimulation on migraine patients (OR 2.28 (1.15, 4.52)), while there was no significant improvement in chronic migraine (OR2.93 (0.71, 12.15)). Five SRs19–23 assessed pain intensity with TMS compared to sham stimulation, with 2 showing significant improvement (SMD-1.139 (−2.207, −0.071); MD-13.56 (−21.80, −5.32)) and 3 showed no significant improvement (SMD-0.26 (−0.77, 0.24), MD 0.43 (−0.40, 1.27), SMD −029 (−114, 0.87)). 3 SRs19,23,24 evaluated the frequency of migraine attacks with TMS compared to sham stimulation, and two showed a significant improvement (SMD −1.13 (−1.69, −0.58); MD7.55 (6.88, 8.21)). One SRs showed no significant improvement (SMD −0.14 (−1.681.40)). There were 2 studies21,22 reporting shorter headache days, specifically, 1 indicated that compared to sham stimulation, TMS can reduce headache days (MD-8.09 (−11.40, −4.79)), while another indicated no difference (MD0.10 (−4.13, 4.32)). One SR22 reported changes in medication intake and HIT-6 score after TMS treatment, which demonstrated that TMS reduced medication intake for migraine patients (MD9.78 (1.60, 17.96)) and HIT-6 scores (MD8 (4.37, 11.63)). One SRs23 reported adverse reactions of TMS compared to sham stimulation, which showed that TMS did not induce headaches (OR2.21 (0.29, 16.93)) or cause sleep disturbances (OR0.93 (0.20, 4.26)).
Discussion
According to the philosophy of evidence-based medicine, evidence derived from SRs is considered to have the highest level of credibility.31,32 Many SRs have been carried out recently to assess the efficacy and safety of TMS in treating migraines.18–24 However, the PRISMA statement has recommended by only a few SRs, and GRADE could evaluate their quality of evidence. Therefore, it is preferable to have a thorough understanding of these SRs rather than using a large number of low-quality SRs with dubious conclusions or meta-analyses.33 Additionally, an overview can provide valuable insight for enhancing and guiding future high-quality SRs.34 By evaluating the data from 7 SRs, our review investigated the use of TMS for migraines and proposed 3 key conclusions.
Firstly, due to the uncertainty of the results, caution should be taken when recommending TMS as an alternative treatment for migraines. The included SRs evaluated the effectiveness of TMS in improving pain intensity, reducing migraine frequency and decreasing headache days, however, all these evaluations were greatly underestimated by AMSTAR 2 methodological quality standards, especially items 2 and 7. Some were rated as high risk during ROBIS stage 2, which covers key review processes that may introduce bias into SR process transparency as an important domain to introduce SR bias. Therefore, it is necessary to confirm the effectiveness of TMS in improving pain intensity, frequency of migraine attacks, and reduction of headache days with high-quality methodology without risk biases. Such evidence came from one systemic review,23 which demonstrates that TMS can reduce medication intake and migraine attacks patients with migraines. However, the GRADE level evidence quality was low due to the limited sample size, heterogeneity, and sample size. Promoting the use of TMS among patients with migraines is not recommended due to limited sample sizes and related safety indicators. Further large-scale clinical trials are needed to draw more convincing conclusions.
Secondly, there was sample opportunity within systematic review (SR) processes to address risks associated with bias, methodology, and reporting quality. Methodological flaws limit the validity of SRs, while the possibility of bias in SRs could affect the validity of the data. Improper reporting in SRs may omit to mention adverse reactions or inflate the impact of interventions, thereby reducing their design value. Our examination of 7 SRs using AMSTAR 2 revealed common deficiencies such as a lack of pre-published protocols or explanations for study design choices and exclusion of some SRs and funding sources. Based on the PRISMA results, all the 7 included SRs had varying degrees of reporting deficiencies, particularly in protocol and registration, synthesis results, certainty assessment, evidence reliability and funding. Future systematic reviews should adhere to both AMSTAR 2 and PRISMA guidelines. During stage two (identification and selection of studies) and stage three (reviewing risks associated with bias), ROBIS identified some low-risk assessments and result quality varied depending on GRADE results.
Thirdly, we extracted and analyzed every original RCT for TMS therapy of migraines in SRs/MAs using the GROOVE tool. Overall, there was a relatively high overlap between the included SRs/MAs. A majority of the overlaps (>5%) occurred among the studies, as shown in the overlapping distribution area in Figure 2. Therefore, current published systematic reviews had similar results that can explain why there were 3 SRs on TMS treatment for migraines in 2022. Further systematic review research is not necessary unless new double-blind and multicenter RCTs emerge.
Implications for Future Study
Reviewers should adhere to the guidelines of AMSTAR 2, ROBIS, and PRISMA when conducting SRs. In particular, during the transparent process, research plans should be registered or published in PROSPERO (http://www.crd.york.ac.uk/prospero) or Cochrane beforehand, and gray literature should be considered. At the same time, conflicts of interest or funding sources should be stated, along with a list of eliminated studies and the reasons for elimination. To improve the quality of original research evidence on TMS treatment for migraine with aura, it is recommended to increase sample size. If significant heterogeneity exists, subgroup analysis or meta-regression analysis is needed for further improving evidence quality.
The AMSTAR 2 tool is widely used for assessing the quality of systematic reviews (SRs)26 but does not assess the possibility of bias in SRs. To address this gap, the ROBIS tool was developed specifically for conducting overviews. The ROBIS instrument contains 3 stages, the second of which consists of 4 domains, each with signaling questions and a determination of the domain’s bias risk.27 Even though some aspects in AMSTAR 2 and ROBIS may be similar, these tools have diverse functions that work well together to give a more complete picture. The 7 SRs have several shortcomings, yet TMS could still reduce the severity and frequency of migraine patients’ headache. Future research should pay more attention to standardizing TMS operations, such as localization, current intensity, operation frequency and time. In addition, we do not have enough evidence to show that TMS would produce adverse reactions, therefore further investigation is needed to determine its safety. It is worth noting that TMS has advantages such as non-invasiveness, repeatability and personalized treatment methods.
Limitations
Our review has several limitations. Firstly, we might have overlooked a few studies in other languages as we only included SRs written in English and Mandarin. Secondly, the sample size of SRs that included RCTs was relatively small. Due to the GRADE level was in the moderate to low range, no definite conclusions can be made.
Conclusion
TMS may have a beneficial effect on the severity and frequency of migraine episodes and has a good safety profile, but the evidence is limited and inconclusive due to the methodological flaws and heterogeneity of the existing studies. Some of the major limitations include small sample size, lack of blinding, heterogeneity of intervention parameters, variability of outcome measures, and risk of bias and publication bias in the included studies. Therefore, future studies should address these issues by carefully selecting patients, standardizing the use of TMS and rTMS, assessing side effects, and comparing with other treatments. This would provide more reliable and consistent evidence for the efficacy and safety of TMS in migraine management, as well as inform clinical decision-making and guideline development.
Funding
The general program of Shandong Natural Science Foundation (No. ZR2021MH373), the Joint Fund of Natural Science Foundation of Shandong Province (No. ZR2021LZY044), Jinan “GaoXiao 20 Tiao” Funding Project Contract (No. 2020GXRC005), Qilu Health Leading Talent Project, Lu Wei Talent Word [2020] No. 3, and the fifth batch of National Research and Training Program for Outstanding Clinical Talents of Traditional Chinese Medicine (National Letter of TCM Practitioners No. 1 (2022)).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Perenboom MJ, van de Ruit M, Zielman R, et al. Enhanced pre-ictal cortical responsivity in migraine patients assessed by visual chirp stimulation. Cephalalgia. 2020;40(9):913–923. doi:10.1177/0333102420912725
2. Pohl H, Streit AC, Neumeier MS, Merki-Feld GS, Ruch W, Gantenbein AR. Migraine and Happiness. Women’s Health Rep. 2022;3(1):155–161. doi:10.1089/whr.2021.0122
3. Maraia Z, Ricci D, Rocchi MBL, et al. Real-life analysis with erenumab: first target therapy in the episodic and chronic Migraine’s prophylaxis. J Clin Med. 2021;10(19):4425. doi:10.3390/jcm10194425
4. Nie L, Ma D, Quinn JP, Wang M. Src family kinases activity is required for transmitting purinergic P2X7 receptor signaling in cortical spreading depression and neuroinflammation. J Headache Pain. 2021;22(1):146. doi:10.1186/s10194-021-01359-8
5. Schaefer SM, Gottschalk CH, Jabbari B. Treatment of chronic migraine with focus on botulinum neurotoxins. Toxins. 2015;7(7):2615–2628. doi:10.3390/toxins7072615
6. Cirillo G, Pepe R, Siciliano M, et al. Long-term neuromodulatory effects of Repetitive Transcranial Magnetic Stimulation (rTMS) on Plasmatic Matrix Metalloproteinases (MMPs) levels and visuospatial abilities in Mild Cognitive Impairment (MCI). Int J Mol Sci. 2023;24(4):3231. doi:10.3390/ijms24043231
7. Tian D, Izumi SI. Interhemispheric facilitatory effect of high-frequency rTMS: perspective from intracortical facilitation and inhibition. Brain Sci. 2022;12(8):970. doi:10.3390/brainsci12080970
8. McClintock SM, Reti IM, Carpenter LL, et al; National Network of Depression Centers rTMS Task Group, & American Psychiatric Association Council on Research Task Force on Novel Biomarkers and Treatments. Consensus Recommendations for the Clinical Application of Repetitive Transcranial Magnetic Stimulation (rTMS) in the Treatment of Depression. J Clin Psychiatry. 2018;79(1):16cs10905. doi:10.4088/JCP.16cs10905
9. Rubio B, Boes AD, Laganiere S, Rotenberg A, Jeurissen D, Pascual-Leone A. Noninvasive brain stimulation in Pediatric Attention-Deficit Hyperactivity Disorder (ADHD): a Review. J Child Neurol. 2016;31(6):784–796. doi:10.1177/0883073815615672
10. Mohamad Safiai NI, Amir NA, Basri H, et al. Effectiveness and tolerability of repetitive transcranial magnetic stimulation for preventive treatment of episodic migraine: a single-centre, randomised, double-blind, sham-controlled phase 2 trial (Magnet-EM). Trials. 2020;21(1):923. doi:10.1186/s13063-020-04832-y
11. Aamir A, Girach A, Sarrigiannis PG, et al. Repetitive magnetic stimulation for the management of peripheral neuropathic pain: a systematic review. Adv Ther. 2020;37(3):998–1012. doi:10.1007/s12325-020-01231-2
12. Mykland MS, Uglem M, Neverdahl JP, et al. Sleep restriction alters cortical inhibition in migraine: a transcranial magnetic stimulation study. Clin Neurophysiol. 2022;139:28–42. doi:10.1016/j.clinph.2022.04.004
13. Monteith TS, Goadsby PJ. Acute migraine therapy: new drugs and new approaches. Curr Treat Options Neurol. 2011;13(1):1–14. doi:10.1007/s11940-010-0105-6
14. Mykland MS, Uglem M, Stovner LJ, et al. Insufficient sleep may alter cortical excitability near the migraine attack: a blinded TMS crossover study. Cephalalgia. 2023;43(3):3331024221148391. doi:10.1177/03331024221148391
15. Cosentino G, Di Marco S, Ferlisi S, et al. Intracortical facilitation within the migraine motor cortex depends on the stimulation intensity. A paired-pulse TMS study. J Headache Pain. 2018;19(1):65. doi:10.1186/s10194-018-0897-4
16. Kalita J, Kumar S, Singh VK, Misra UK. A randomized controlled trial of high rate rTMS versus rTMS and amitriptyline in chronic migraine. Pain Physician. 2021;24(6):E733–E741.
17. Leahu P, Bange M, Ciolac D, et al. Increased migraine-free intervals with multifocal repetitive transcranial magnetic stimulation. Brain Stimul. 2021;14(6):1544–1552. doi:10.1016/j.brs.2021.10.383
18. Lan L, Zhang X, Li X, Rong X, Peng Y. The efficacy of transcranial magnetic stimulation on migraine: a meta-analysis of randomized controlled trails. J Headache Pain. 2017;18(1):86. doi:10.1186/s10194-017-0792-4
19. Zhong J, Lan W, Feng Y, et al. Efficacy of repetitive transcranial magnetic stimulation on chronic migraine: a meta-analysis. Front Neurol. 2022;13:1050090. doi:10.3389/fneur.2022.1050090
20. Feng Y, Zhang B, Zhang J, Yin Y. Effects of non-invasive brain stimulation on headache intensity and frequency of headache attacks in patients with migraine: a systematic review and meta-analysis. Headache. 2019;59(9):1436–1447. doi:10.1111/head.13645
21. Saltychev M, Juhola J. Effectiveness of high-frequency repetitive transcranial magnetic stimulation in migraine: a systematic review and meta-analysis. Am J Phys Med Rehabil. 2022;101(11):1001–1006. doi:10.1097/PHM.0000000000001953
22. Mohamad Safiai NI, Mohamad NA, Basri H, et al. High-frequency repetitive transcranial magnetic stimulation at dorsolateral prefrontal cortex for migraine prevention: a systematic review and meta-analysis. Cephalalgia. 2022;42(10):1071–1085. doi:10.1177/03331024221092423
23. Shirahige L, Melo L, Nogueira F, Rocha S, Monte-Silva K. Efficacy of noninvasive brain stimulation on pain control in migraine patients: a systematic review and meta-analysis. Headache. 2016;56(10):1565–1596. doi:10.1111/head.12981
24. Jiang C, Yu N, Li F, Shi J. Systematic evaluation of the efficacy and safety of repetitive transcranial magnetic stimulation for the prevention of chronic migraine. J Clin Neurol. 2016;06:421–424.
25. Higgins J, Green S, Collaboration C. Cochrane handbook for systematic reviews for interventions. In: Cochrane Database of Systematic Reviews. Bristol: The Cochrane Collaboration; 2011:S38.
26. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
27. Whiting P, Savović J, Higgins JP, et al; ROBIS group. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol. 2016;69:225–234. doi:10.1016/j.jclinepi.2015.06.005
28. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;71. doi:10.1136/bmj.n71
29. Pollock A, Farmer SE, Brady MC, et al. An algorithm was developed to assign GRADE levels of evidence to comparisons within systematic reviews. J Clin Epidemiol. 2016;70:106–110. doi:10.1016/j.jclinepi.2015.08.013
30. Pérez-Bracchiglione J, Meza N, Bangdiwala SI, et al. Graphical representation of overlap for overviews: GROOVE tool. Res Synth Methods. 2022;13(3):381–388. doi:10.1002/jrsm.1557
31. Pan M, Lan Y, Wang Z. Wrist-ankle acupuncture has a positive effect on chronic pain: a systematic review and meta-analysis. Acupunct Herbal Med. 2023;3(1):7–19. doi:10.1097/HM9.0000000000000059
32. Yang K, Zhang J, Zhao L. An umbrella review of Lianhua Qingwen combined with Western medicine for the treatment of coronavirus disease 2019. Acupunct Herbal Med. 2022;2(3):143–151. doi:10.1097/HM9.0000000000000041
33. Huang J, Zhang J, Wang Y, et al. Scientific evidence of Chinese herbal medicine (Gegen Qinlian Decoction) in the treatment of ulcerative colitis. Gastroenterol Res Pract. 2022;2022:7942845. doi:10.1155/2022/7942845
34. Shen M, Huang J, Qiu T. Quality of the evidence supporting the role of acupuncture for stable angina pectoris: an umbrella review of systematic reviews. Front Cardiovasc Med. 2021;8:732144. doi:10.3389/fcvm.2021.732144
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Breathing Exercises in the Treatment of COPD: An Overview of Systematic Reviews
Li Y, Ji Z, Wang Y, Li X, Xie Y
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:3075-3085
Published Date: 7 December 2022