Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Transcranial direct current stimulation for Obsessive-Compulsive Disorder: patient selection and perspectives
Authors da Silva RMF, Brunoni AR ![]() , Miguel EC
, Miguel EC ![]() , Shavitt RG
, Shavitt RG
Received 8 May 2019
Accepted for publication 22 August 2019
Published 16 September 2019 Volume 2019:15 Pages 2663—2669
DOI https://doi.org/10.2147/NDT.S184839
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Video abstract presented by Renata de Melo Felipe da Silva.
Views: 1523
Renata de Melo Felipe da Silva,1 Andre Russowsky Brunoni,2 Eurípedes Constantino Miguel,1 Roseli Gedanke Shavitt3
1Department and Institute of Psychiatry, Obsessive-Compulsive Spectrum Disorders Program and Service of Interdisciplinary Neuromodulation (SIN), Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo, SP, Brazil; 2Department and Institute of Psychiatry, Department of Internal Medicine, Laboratory of Neurosciences (LIM-27), Service of Interdisciplinary Neuromodulation (SIN), Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo, SP, Brazil; 3Department and Institute of Psychiatry and Director of the Obsessive-Compulsive Spectrum Disorders Program, Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo, SP, Brazil
Correspondence: Roseli Gedanke Shavitt
Instituto de Psiquiatria – HC-FMUSP, R. Dr Ovidio Pires de Campos 785 3o Andar Ala Norte, São Paulo, SP CEP 05403-000, Brazil
Email [email protected]
Abstract: Transcranial direct current stimulation (tDCS) is a non-invasive neuromodulation technique that has been increasingly examined as an alternative treatment modality for Obsessive-Compulsive Disorder (OCD), due to its low costs, ease of use, and portability. Previous studies have suggested that tDCS may achieve a reasonably good response and present a safe tolerability profile. However, at this point there is not strong evidence for the use of this modality of treatment. Considering that OCD is very heterogeneous with regard to clinical presentation, clinical severity and comorbidities, we have conducted a systematic review of studies on tDCS for OCD aiming to evaluate the clinical characteristics of the selected patients and to discuss perspectives for future studies. A literature search was conducted from inception until March 2019 at PubMed/MedLine and Scielo using the following keywords: “tdcs” or “transcranial direct current stimulation” and “obsessive compulsive disorder”. Out of 45 manuscripts, twelve were included. Most of the included studies are uncontrolled. A few controlled studies reported improvement of OCD, but some limitations need to be considered. Our main findings were that the selected patients were adults with severe OCD and psychiatric comorbidities, medicated at the time of assessment and resistant to at least one previous conventional treatment. We could not find any studies including specific populations such as adolescents, elderly, pregnant and breastfeeding participants. Similarly, the potential use of tDCS has not been tested in patients with less severe OCD, as a first treatment option, or for those who do not tolerate pharmacological treatments. These opportunities should be explored in future controlled trials.
Keywords: obsessive-compulsive disorder, transcranial direct current stimulation, neuromodulation
Introduction
Obsessive-Compulsive Disorder (OCD) is a neuropsychiatric disorder with a prevalence of 2% in the general population.1 It is a chronic, potentially disabling condition that is characterized by the presence of recurrent and uncontrollable thoughts (obsessions) and repetitive behaviors (compulsions) that the subject feels compelled to repeat.2 Subjects with OCD may suffer a great amount of interference from their obsessions and compulsions with their regular activities. Besides the obsessions, the compulsions may also be triggered by sensory experiences like incompleteness or the not-just-right perceptions.3 First-line treatments for OCD include the selective serotonin-reuptake inhibitors (SSRIs) and cognitive-behavioral therapy (CBT).4 Augmentation strategies with antipsychotics have been studied, which showed a limited capacity to increase treatment success. Therefore, about one-third of the patients remain symptomatic after one or more evidence-based treatments.5 In OCD, there is usually the need to achieve the higher recommended doses of the medications, which may be associated with the occurrence of various side.6–8 Thus, treatment alternatives for patients with OCD who do not respond to or do not tolerate the adverse effects of the standard medications are still lacking.
The growing knowledge of the neurobiology of OCD, especially about the cortical-striatum-thalamus-cortical (CSTC) circuits, has facilitated the development of treatments involving neuromodulation.9 Recently, a few case reports and clinical trials reporting the use of transcranial direct current stimulation (tDCS) as a treatment for OCD have been reported. tDCS is a non-invasive neuromodulation technique that consists of applying a low voltage current to the brain using electrodes placed on the scalp.10 This technique has been studied on the treatment of different psychiatric disorders due to its good tolerability, with no serious adverse effects.11
In the initial case reports involving tDCS and OCD, Narayanaswamy 201512 described 2 patients with OCD that showed a good response to tDCS. These patients had failed to two or more pharmacological treatments. Most of the subsequent case reports and clinical trials have reported a mixed, although positive response to treatment.13–15
Considering that OCD is a very heterogeneous disorder with regard to clinical presentation, clinical severity and comorbidities, we have conducted a systematic review of studies on tDCS for OCD aiming to evaluate the clinical characteristics of the selected patients and to discuss perspectives for future studies.
Methods
Literature search strategy
We conducted a systematic review following the steps established in the PRISMA guidelines.16 Our search strategy included the main electronic databases (PubMed/MedLine and Scielo) from the first data available to March 2019, using the keywords “tdcs” or “transcranial direct current stimulation” and “obsessive compulsive disorder”. We then reviewed the references of selected manuscripts.
Manuscript selection criteria
Inclusion criteria for the available studies were: a) original articles published in English; b) case reports, open trials, randomized clinical trials; c) patients: subjects diagnosed with OCD in accordance to the 4th or 5th versions of the Diagnostic and Statistical Manual of Mental Disorders – DSM;2 d) intervention type: tDCS for the improvement of OCD symptoms. We have excluded studies with incomplete data regarding the patients’ profile or describing a poor quality of patient selection.
Quality assessment
To assess quality we have used the PEDRo scale17 for the assessment of clinical trials. The PEDro scale has 11 items, designed for rating the methodological quality of clinical trials. Scores greater or equal to 9 are considered “excellent”, from 6 to 8 are considered “good”, from 4 to 5 are considered “fair” and scores below 4 are considered “poor” methodological quality. We included only manuscripts with good or excellent methodological quality. For uncontrolled studies (case report, case series, open trial) we measured the quality by evaluating the presence of a complete description of the data of interest for this review, such as the description of the participants’ age, and a validated measure of OCD severity. Open trials should contain a diagram or appropriate description of the included patients.
Data extraction
For each selected manuscript we have extracted the study characteristics such as design, author, year and clinical and demographic data of patients (such as sample size, sex, age, psychiatric comorbidities, medication status, initial YBOCS and OCD severity), tDCS parameters and response to treatment.
Results
The search strategy described above resulted in 45 manuscripts. After having reviewed the title, abstracts and having applied the eligibility criteria, we excluded 31 manuscripts for the following reasons: 20 manuscripts were reviews or comments of this topic, 8 evaluated different diagnoses and treatment modalities and 3 manuscripts did not evaluate improvement based on YBOCS scores. Figure 1 displays the flowchart.
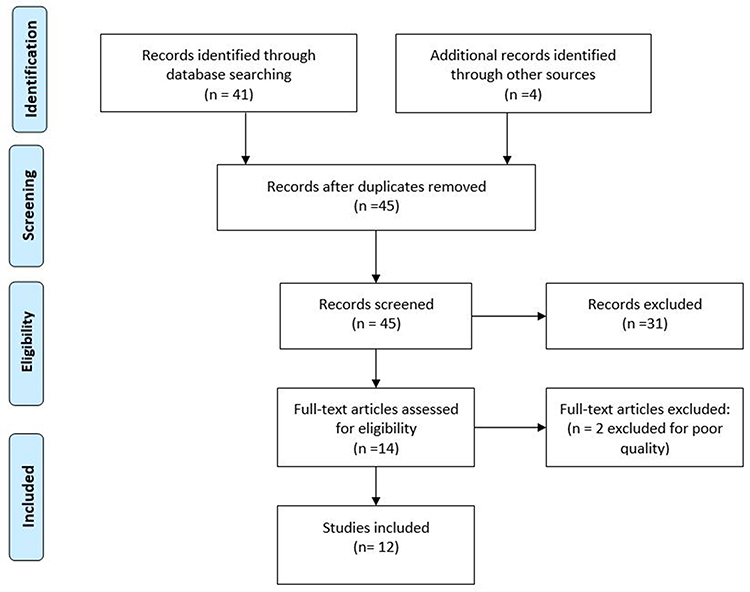 |
Figure 1 Flowchart of the selection of studies according to PRISMA. |
At this step 14 full-text manuscripts that met our inclusion criteria were included for review. Three RCTs and 11 uncontrolled studies (open trials and case reports) were assessed for quality and 2 were excluded: one clinical trial (Yekta, 2015)18 that was classified as having poor methodological quality and one uncontrolled trial (Najafi, 2016)19 was excluded due to the absence of a diagram or an appropriate description of the patients included. Finally, 12 manuscripts were selected.
Overview of the selected studies
Uncontrolled studies (case reports, case series, open-label trials)
Uncontrolled studies of tDCS in OCD reported on adult patients, both men and women, with a primary diagnosis of OCD and presenting with psychiatric comorbidities (Table 1). Most patients were on medication and had failed at least one first-line treatment. Regarding treatment parameters, the number of sessions ranged from 10 to 20, once or twice a day. The anode was positioned over the neck, the pre-SMA, right occipital cortex, cerebellum, deltoid muscle, FP1 and F3 (according 10–20 EEG system), whereas the cathode was positioned over the F3, FP1, FP2, F4, pre-SMA, deltoid muscle, left OFC and right supra-orbital area. Response to treatment ranged from no change in baseline YBOCS scores to 80% of improvement.
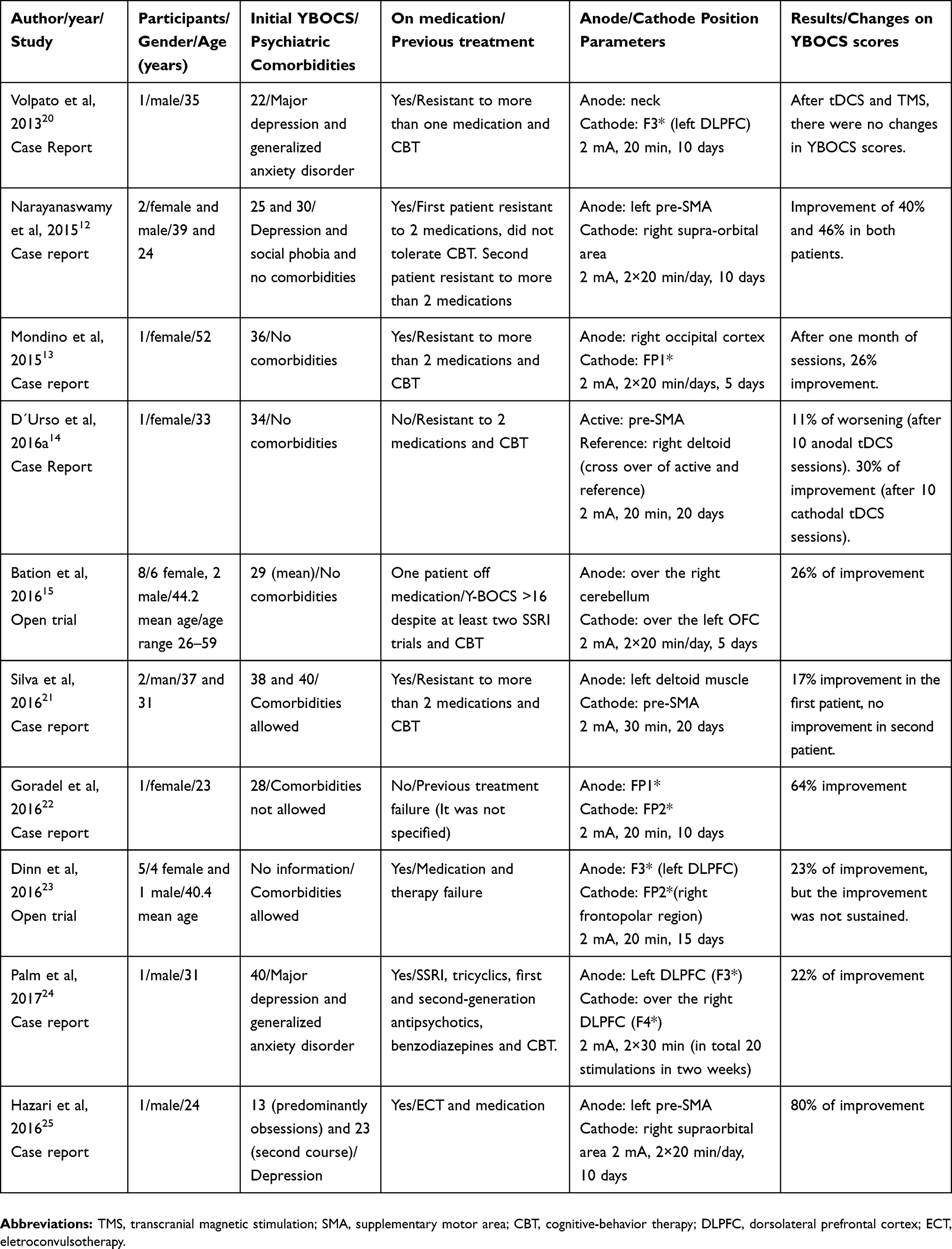 |
Table 1 Demographic and clinical characteristics of the uncontrolled selected studies (case reports, case series, open-label trials) |
Randomized clinical trials
Two RCTs have been selected as demonstrated in Table 2. The first one is a crossover trial,26 evaluating the cathode versus the anode on the pre-SMA of adult patients with a primary diagnosis of OCD. Psychiatric comorbidities were allowed. This trial included men and women, aged 25–65, with previous failure to respond to at least one SRI. The patients received 20 min of 2 mA tDCS sessions during 20 days of cathodal or anodal stimulation over the pre-SMA, and the other electrode placed over the right deltoid. If patients showed improvement or no change in OCD symptoms after 10 sessions, they were maintained on the same current polarity for 10 additional sessions. In case of worsening after the first 10 sessions, subjects were switched to the other polarity for 10 additional sessions. The authors found that cathodal, but not anodal tDCS over the pre-SMA was associated with improvement of OCD symptoms. After 10 sessions, 100% of patients that had started on the cathodal stimulation continued on the same polarity, while 50% of patients who had started receiving anodal stimulation were switched to the cathodal stimulation. At the end of the study (4 weeks), the mean YBOCS scores of patients who underwent cathodal tDCS has decreased, while there was no difference between pre-post stimulation in the anodal tDCS.
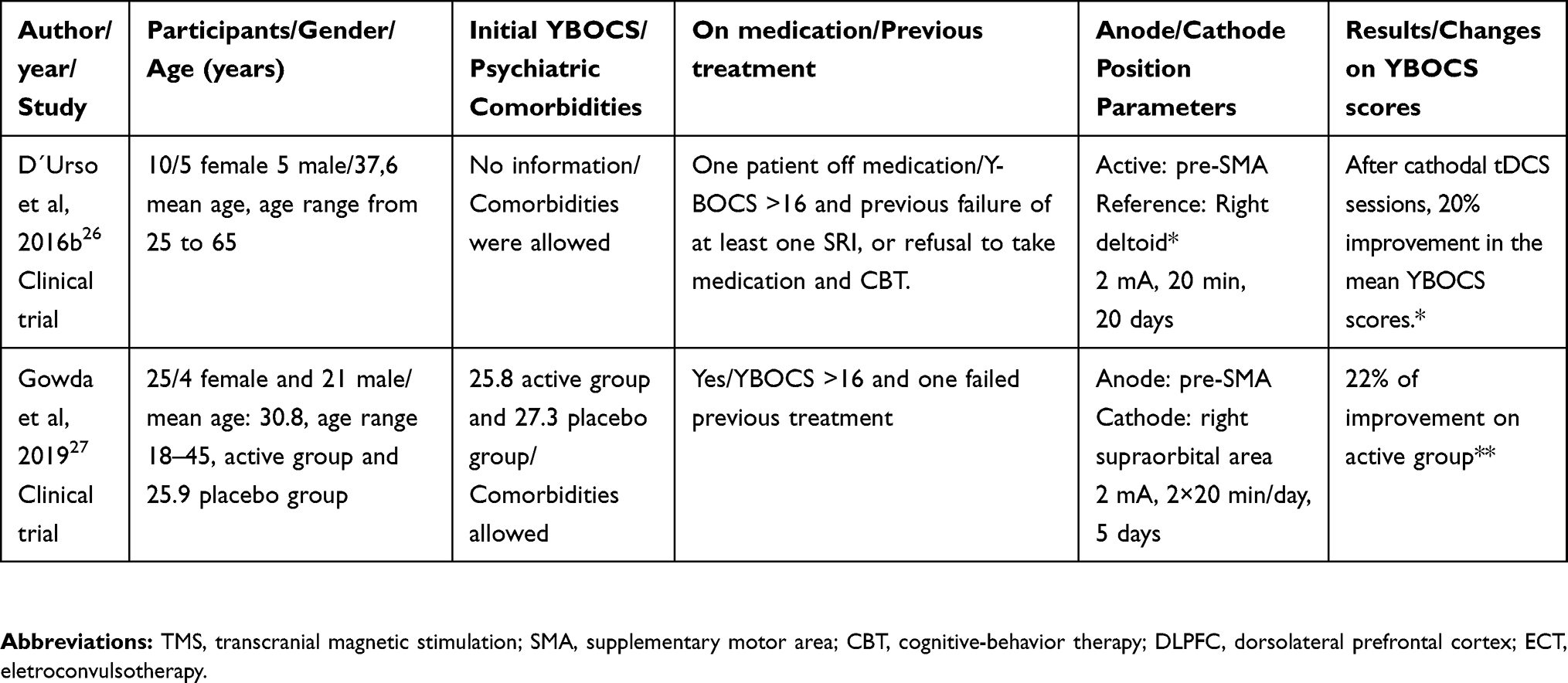 |
Table 2 Demographic and clinical characteristics of the selected randomized clinical trials |
The second study27 was a randomized, double blind, sham-controlled trial evaluating the efficacy of anodal tDCS over the pre-SMA and the cathode over the right supra-orbital area. Twenty-five adult patients that had not responded to at least one SSRI were randomized to receive a sham stimulation or active tDCS. The sessions were conducted twice a day, on 5 consecutive days during 20 mins. On this study, psychiatric comorbidities were allowed, except for the lifetime presence of substance dependence, psychosis, bipolar disorder, neurological disease or psychiatric emergency. Patients could be on medication since dosages were stable for at least 3 months. The authors found that the active treatment was superior to sham based on an international expert consensus of response criteria (35% reduction in the baseline YBOCS total score with a CGI-I score of 1 (very much improved) or 2 (improved)). After 10 days of follow-up (from baseline to primary outcome), the authors found that 4 of 12 in the active tDCS group versus 0 in the sham group had sustained their response status.
Discussion
Our systematic review revealed 12 manuscripts, 10 uncontrolled and 2 controlled studies. Regarding the uncontrolled studies, the case reports and open trials included adults, both female and male, on medication and presenting with psychiatric comorbidities. Subjects had failed at least one previous treatment. The electrode montages of these studies varied considerably. However, considering a computer simulation of the electric fields, these montages concentrated the EF on the prefrontal cortex.28 Most of these case reports and open trials related positive response to treatment. It is important to evaluate the limitations of these studies, considering sample size and bias publication.
Considering the controlled studies, the profile of the selected patients was very similar to the uncontrolled studies: adults, male and female, with a more severe disorder (non-responders to at least one previous treatment), presenting with psychiatric comorbidities and on medication. D´Urso et al26 found that the cathodal, but not anodal tDCS on the pre-SMA were related to improvement of OCD symptoms, sustained at 4-weeks follow-up. On the other hand, Gowda et al27 reported a positive response to treatment after anodal tDCS over the pre-SMA and the cathode over the right supra-orbital area, sustained at 10-days follow-up. As limitations of these trials we could consider the small sample sizes and a short period of the follow-up assessments. The majority of the studies (controlled and uncontrolled) reported improvement of OCD. However, as stated above, these results should be considered preliminary and need replication.
The age profile of patients admitted to the tDCS studies reported so far did not include children, adolescents or elderly adults. The latter constitute a particularly interesting population to be studied. Evidence suggests that the elderly present more clinical comorbidities, leading to the use of several medications with potential pharmacological interactions; they tend to be more concerned about taking medications, to be more sensitive to side effects and to have high dropout rates.29 In addition, elderly patients are more sensitive to the anticholinergic, hypotensive, and cardiac effects of tricyclic antidepressants.30 Thus, further studies evaluating non invasive neuromodulation treatments for this population are timely and needed to improve the rates of treatment success.
Another population that is not represented among the available studies refers to pregnant and lactating women with OCD. Although some psychoactive drugs offer greater safety in pregnancy and lactation, some patients refuse to take medication on those occasions. The literature dealing with tDCS during pregnancy is still sparse, which merits attention since tDCS has a favorable safety profile during pregnancy.31
In terms of OCD severity, most patients had failed 1 or more pharmacological treatments and some of them had also failed one CBT trial. This means that less severe or treatment-naïve patients have not been evaluated in tDCS trials. Studies with untreated patients are needed to inform us about the role of tDCS as a first-line treatment alternative, since the current recommendations of SSRIs in high doses and CBT4 may not be tolerated by a considerable number of subjects.
In this review, most studied patients were on medication. Psychiatric and non-psychiatric medications may influence tDCS treatment, but at this point this effect is not clear.32 Especially regarding the use of SSRIs, one study with 12 subjects suggested that citalopram seemed to influence the cortical excitability of the subjects studied.33 While the effect of medications on tDCS is unclear, it is important that patients are properly screened for illicit drugs, nicotine, and medication use in tDCS trials.32
To conclude, future trials are needed to determine the efficacy of tDCS in OCD and investigate the best electrode position, with larger samples and longer periods of follow-up. Regarding the selection of subjects for future tDCS trials, we point out the need to include subjects with the following profiles: a) elderly patients; b) subjects with less severe OCD; c) treatment-naïve patients; d) tDCS in combination with CBT. The relative paucity of available studies of tDCS for OCD constituted a limitation to our review. Thus, the evaluation of the selected patient profile was performed based on a small number of manuscripts.
Conclusion
tDCS is a neuromodulation technique that has only recently been studied for the treatment of OCD. At present, there is not a strong evidence for this modality of treatment in OCD patients. Published studies are mostly uncontrolled, and very few controlled studies suggest that tDCS may be efficacious for this disorder. Our review included, mostly, samples of adults with severe OCD and on medication. There are no studies evaluating the efficacy and safety of tDCS in populations such as the elderly, adolescents, infants, pregnant or lactating women, patients with less severe OCD or treatment-naive patients. Future studies are needed to determine the efficacy of tDCS in OCD, including these populations, given the good tolerability profile of tDCS, its low cost and the need for alternative treatment modalities when medication or CBT cannot be delivered.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the national comorbidity survey replication. Mol Psychiatry. 2010;15:53–63. doi:10.1038/mp.2008.94
2. American Psychiatric Association. DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington, DC: American Psychiatric Association; 2013.
3. Shavitt RG, de Mathis MA, Oki F, et al. Phenomenology of OCD: lessons from a large multicenter study and implications for ICD-11. J Psychiatr Res. 2014;57:141–148. doi:10.1016/j.jpsychires.2014.06.010
4. Hirschtritt ME, Bloch MH, Mathews CA. Obsessive-compulsive disorder. JAMA. 2017;317(13):1358. doi:10.1001/jama.2017.2200
5. Simpson HB, Huppert JD, Petkova E, Foa EB, Liebowitz MR. Response versus remission in obsessive-compulsive disorder. J Clin Psychiatry. 2006;67(2):269–276. doi:10.4088/JCP.v67n0214
6. Pedro Franz A, Paim M, Moreno de Araújo R, et al. Treating Refractory Obsessive-Compulsive Disorder: What to Do When Conventional Treatment Fails? Vol. 35; 2013. Available from: http://www.scielo.br/pdf/trends/v35n1/a04v35n1.pdf.
7. Kellner M. Drug treatment of obsessive-compulsive disorder. Dialogues Clin Neurosci. 2010;12(2):187–197. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20623923.
8. Pittenger C, Bloch MH. Pharmacological treatment of obsessive-compulsive disorder. Psychiatr Clin North Am. 2014;37(3):375–391. doi:10.1016/j.psc.2014.05.006
9. van Den Heuvel OA, van Wingen G, Soriano-Mas C, et al. Brain circuitry of compulsivity. Eur Neuropsychopharmacol. 2016;26(5):810–827. doi:10.1016/j.euroneuro.2015.12.005
10. Brunoni AR, Sampaio-Junior B, Moffa AH, et al. Noninvasive brain stimulation in psychiatric disorders: a primer. Braz J Psychiatry. 2018. doi:10.1590/1516-4446-2017-0018
11. Brunoni AR, Moffa AH, Fregni F, et al. Transcranial direct current stimulation for acute major depressive episodes: meta-analysis of individual patient data. Br J Psychiatry. 2016;208(6):522–531. doi:10.1192/bjp.bp.115.164715
12. Narayanaswamy JC, Jose D, Chhabra H, et al. Successful Application of Add-on Transcranial Direct Current Stimulation (tDCS) for Treatment of SSRI Resistant OCD. Brain Stimul. 2015;8(3):655–657. doi:10.1016/j.brs.2014.12.003
13. Mondino M, Haesebaert F, Poulet E, Saoud M, Brunelin J. Efficacy of cathodal transcranial direct current stimulation over the left orbitofrontal cortex in a patient with treatment-resistant obsessive-compulsive disorder. J Ect. 2015;31(4):271–272. doi:10.1097/YCT.0000000000000218
14. D’Urso G, Brunoni AR, Anastasia A, Micillo M, de Bartolomeis A, Mantovani A. Polarity-dependent effects of transcranial direct current stimulation in obsessive-compulsive disorder. Neurocase. 2016;22(1):60–64. doi:10.1080/13554794.2015.1045522
15. Bation R, Poulet E, Haesebaert F, Saoud M, Brunelin J. Transcranial direct current stimulation in treatment-resistant obsessive-compulsive disorder: an open-label pilot study. Prog Neuro-Psychopharmacol Biol Psychiatry. 2016;65:153–157. doi:10.1016/j.pnpbp.2015.10.001
16. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–341. doi:10.1016/J.IJSU.2010.02.007
17. de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother. 2009;55(2):129–133. doi:10.1016/S0004-9514(09)70043-1
18. Yekta M, Rostami R, Fayyaz E. Transcranial direct current stimulation of dorsolateral prefrontal cortex in patients with obsessive compulsive disorder to improve decision making and reduce obsession symptoms. Pract Clin Psychol. 2015;3(3):185–194. http://jpcp.uswr.ac.ir/browse.php?a_code=A-10-259-2&slc_lang=en&sid=1.
19. Najafi K, Fakour Y, Zarrabi H, et al. Efficacy of transcranial direct current stimulation in the treatment: resistant patients who suffer from severe obsessive-compulsive disorder. Indian J Psychol Med. 2017;39(5):573–578. doi:10.4103/IJPSYM.IJPSYM_388_16
20. Volpato C, Piccione F, Cavinato M, et al. Modulation of affective symptoms and resting state activity by brain stimulation in a treatment-resistant case of obsessive–compulsive disorder. Neurocase. 2013;19(4):360–370. doi:10.1080/13554794.2012.667131
21. da Silva RMF, Brunoni AR, Miguel EC, Shavitt RG. Transcranial direct current stimulation for treatment-resistant obsessive-compulsive disorder: report on two cases and proposal for a randomized, sham-controlled trial. Sao Paulo Med J. 2016;134(5):446–450. doi:10.1590/1516-3180.2016.0155010716
22. Goradel JA, Pouresmali A, Mowlaie M, Movahed FS. The effects of transcranial direct current stimulation on obsession-compulsion, anxiety, and depression of a patient suffering from obsessive-compulsive disorder. J Pract Clin Psychol. 2016;4(2):75–80. doi:10.15412/J.JPCP.06040201
23. Dinn WM, Aycicegi-Dinn A, Göral F, et al. Treatment-resistant obsessive-compulsive disorder: insights from an open trial of transcranial direct current stimulation (tDCS) to design a RCT. Neurol Psychiatry Brain Res. 2016;22(3–4):146–154. doi:10.1016/j.npbr.2016.08.003
24. Palm U, Leitner B, Kirsch B, et al. Prefrontal tDCS and sertraline in obsessive compulsive disorder: a case report and review of the literature. Neurocase. 2017;23(2):173–177. doi:10.1080/13554794.2017.1319492
25. Hazari N, Narayanaswamy JC, Chhabra H, Bose A, Venkatasubramanian G, Reddy YCJ. Response to transcranial direct current stimulation in a case of episodic obsessive compulsive disorder. J ECT. 2016;32(2):144–146. doi:10.1097/YCT.0000000000000309
26. D’Urso G, Brunoni AR, Mazzaferro MP, Anastasia A, de Bartolomeis A, Mantovani A. Transcranial direct current stimulation for obsessive–compulsive disorder: a randomized, controlled, partial crossover trial. Depress Anxiety. 2016;33(12):1132–1140. doi:10.1002/da.22578
27. Gowda SM, Narayanaswamy JC, Hazari N, et al. Efficacy of pre-supplementary motor area transcranial direct current stimulation for treatment resistant obsessive compulsive disorder: a randomized, double blinded, sham controlled trial. Brain Stimul. 2019;12:922–929. doi:10.1016/j.brs.2019.02.005
28. da Silva RMF, Batistuzzo MC, Shavitt RG, et al. Transcranial direct current stimulation in obsessive-compulsive disorder: an update in electric field modeling and investigations for optimal electrode montage. Expert Rev Neurother. 2019:1–11. doi:10.1080/14737175.2019.1637257
29. Nowshin I, Kabir F. The silent geriatric giant- anxiety disorders in late life. Bangladesh J Physiol Pharmacol. 2014;29(1–2):29–31. doi:10.3329/bjpp.v29i1-2.20065
30. Subramanyam AA, Kedare J, Singh OP, Pinto C. Clinical practice guidelines for Geriatric Anxiety Disorders. Indian J Psychiatry. 2018;60(Suppl 3):S371–S382. doi:10.4103/0019-5545.224476
31. Kurzeck A, Kirsch B, Weidinger E, Padberg F, Palm U. Transcranial Direct Current Stimulation (tDCS) for depression during pregnancy: scientific evidence and what is being said in the media—a systematic review. Brain Sci. 2018;8(8):155. doi:10.3390/brainsci8080155
32. McLaren ME, Nissim NR, Woods AJ. The effects of medication use in transcranial direct current stimulation: a brief review. Brain Stimul. 2018;11(1):52–58. doi:10.1016/j.brs.2017.10.006
33. Nitsche MA, Kuo M-F, Karrasch R, Wächter B, Liebetanz D, Paulus W. Serotonin affects transcranial direct current–induced neuroplasticity in humans. Biol Psychiatry. 2009;66(5):503–508. doi:10.1016/j.biopsych.2009.03.022
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.