Back to Journals » OncoTargets and Therapy » Volume 11
Transcatheter hepatic arterial chemoembolization plus cinobufotalin injection adjuvant therapy for advanced hepatocellular carcinoma: a meta-analysis of 27 trials involving 2,079 patients
Authors Guo N, Miao YY, Sun MZ
Received 6 August 2018
Accepted for publication 14 November 2018
Published 7 December 2018 Volume 2018:11 Pages 8835—8853
DOI https://doi.org/10.2147/OTT.S182840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leo Jen-Liang Su
Na Guo,* Yanyan Miao,* Mingzhong Sun
Department of Hepatopathy, The Sixth People’s Hospital of Qingdao, Qingdao 266033, Shandong Province, China
*These authors contributed equally to this work
Objective: The aim of this study was to systematically investigate the safety and efficacy of the combination of transcatheter hepatic arterial chemoembolization (TACE) and cinobufotalin injection for advanced hepatocellular carcinoma (HC).
Methods: Clinical trials were searched from Web of Science, Cochrane Library, PubMed, Embase, Chinese Medical Citation Index (CMCI), China National Knowledge Infrastructure (CNKI), Chinese Scientific Journal Database (VIP), and Wanfang database. Outcome measures including therapeutic efficacy, quality of life, liver function, immune function, and adverse events were extracted and evaluated.
Results: After final assessment, 27 studies including 2,079 advanced HC patients were involved in this study. Compared with TACE alone, the combination of TACE with cinobufotalin injection adjuvant therapy significantly prolonged the patients’ 1-, 1.5-, 2-, and 3-year overall survival (OS) rate (1-year OS, OR=2.84, 95% CI=2.20–3.67, P<0.00001; 1.5-year OS, OR=3.57, 95% CI=1.92–6.66, P<0.0001; 2-year OS, OR=3.17, 95% CI=2.36–4.25, P<0.00001; 3-year OS, OR=2.88, 95% CI=1.82–4.57, P<0.00001). The combined therapy also improved patients’ overall response rate (ORR; OR=1.86, 95% CI=1.54–2.24, P<0.00001), disease control rate (DCR; OR=2.05, 95% CI=1.59–2.64, P<0.00001), and quality of life improved rate (QIR; OR=3.45, 95% CI=2.52–4.72, P<0.00001). Moreover, the immune function and liver function of HC patients were all significantly enhanced after the combined therapy of TACE and cinobufotalin injection (CD3+, P=0.001; CD4+, P=0.0006; CD4+/CD8+, P=0.03; natural killer [NK] cell, P=0.01; total bilirubin [TBIL], P=0.003; alanine aminotransferase [ALT], P<0.00001; aspartate aminotransferase [AST], P<0.00001). No serious adverse events occurred during cinobufotalin injection-mediated therapy.
Conclusion: The combination of TACE and cinobufotalin injection adjuvant therapy is safe and more effective for end-stage HC treatment than TACE alone.
Keywords: hepatocellular carcinoma, cinobufotalin injection, transcatheter hepatic arterial chemoembolization, meta-analysis
Introduction
Hepatocellular carcinoma (HC) is a major threat to human health. It is the fifth most common malignancy and caused more than 600,000 deaths every year.1–3 Over the past 20 years, the number of HC-related deaths has increased by 62%.4 China is a high-risk area for HC and accounts for more than half of the HC cases worldwide.4,5 Despite the development of diagnostic methods, early detection of HC is still difficult.2 In most patients, HC progressed to the intermediate and advanced stage, and the 5-year survival rate was <17% at this stage.1 Therefore, only a small proportion of early-stage HC patients are suitable for radical treatment.
Transcatheter hepatic arterial chemoembolization (TACE) is the current standard locoregional treatment for advanced HC.2,6 Several studies reported that TACE significantly increased the survival time in HC patients compared to supportive treatments.7,8 However, TACE also has its own limitations, as it can further influence the liver functions and damage the hepatic arterial system of patients.2,9 In addition, its clinical application was also limited by drug resistance and toxic side effects.1 In view of these limitations of TACE therapy for HC, complementary and alternative medicine has been increasingly used for the treatment of advanced HC.
In recent years, traditional Chinese medicine has become an important source for novel chemotherapeutic agents and was considered as a powerful method for the cancer treatment.4,10–12 Cinobufotalin, a cardiotonic steroid or bufadienolide, is extracted from the skin secretions of the traditional Chinese medicinal giant toads.12–15 Many studies have shown that cinobufotalin has anti-tumor activity and can enhance the treatment effect of chemotherapeutics for malignancies.12,15,16 It can inhibit the growth of vascular endothelial cells by inhibiting the expression of vascular endothelial growth factor and EGF receptor and then inhibit the growth and metastasis of the tumor.17 In addition, it can also induce tumor cells apoptosis through decreasing ROS production and by destroying the structure of DNA in cancer cells.14,16
Up to now, several clinic trials have been conducted to evaluate the therapeutic effects between TACE and TACE+cinobufotalin injection in advanced HC patients.18–44 Despite the wide use of cinobufotalin injection in HC treatment for many years, its clinical efficacy was still not well established and recognized. Therefore, we conducted a meta-analysis to investigate the treatment effect and safety of cinobufotalin injection adjuvant therapy combined with TACE in comparison with TACE alone for end-stage HC, to provide scientific reference for the design of future clinical trials.
Materials and methods
Search strategy and selection criteria
Original articles published after 2000 were searched across eight databases, including Web of Science, Cochrane Library, PubMed, Embase, Chinese Medical Citation Index (CMCI), China National Knowledge Infrastructure (CNKI), Chinese Scientific Journal Database (VIP), and Wanfang database, with key terms “huachansu” or “cinobufotalin” “cinobufagin” or “cinobufacini” combined with “hepatocellular carcinoma” or “liver cancer”. No language limits were applied. The initial search was performed in May 2018 and updated in July 2018.
Selection criteria of this study are as follows: 1) controlled trials concerning advanced HC patients; 2) literatures comparing the clinical outcomes of TACE plus cinobufotalin injection adjuvant therapy (experimental group) with TACE treatments alone (control group); and 3) articles involving more than 30 HC patients. Exclusion criteria of this study are as follows: 1) non-contrast articles, case studies, and review papers and 2) patients with mixed malignancies.
Data extraction and quality assessment
Data were extracted by two reviewers (Na Guo and Yanyan Miao) independently; disagreements were adjudicated by the third investigator (Mingzhong Sun). The extracted characteristics were summarized as follows: 1) first author’s names; 2) years of publication; 3) study locations; 4) tumor stages; 5) number of cases; 6) patient ages; 7) study parameter types; 8) therapeutic regimens; 9) enrollment period and expected survival time of patients; 10) application sequence of cinobufotalin injection; and 11) manufacturer of cinobufotalin injection. The included trial’s quality was evaluated according to the Cochrane Handbook.45
Outcome definition
Clinical outcomes include therapeutic effect and adverse events. Therapeutic effect was assessed in terms of the overall survival (OS) rates, complete response (CR) rates, partial response (PR) rates, stable disease (SD) rates, progressive disease (PD) rates, overall response rate (ORR; ORR=CR rate+PR rate), disease control rate (DCR; DCR=CR rate+PR rate+SD rate), and quality of life improved rate (QIR). The immune function indicators (CD3+, CD4+, and natural killer (NK) cells percentage and CD4+/CD8+ ratio) and liver function indexes including total bilirubin (TBIL), alanine aminotransferase (ALT), aspartate aminotransferase (AST), and serum albumin (ALB) of HC patients were determined and compared between the two groups. Moreover, adverse events including leukopenia, thrombocytopenia, nausea and vomiting, fever, hepatotoxicity, and myelosuppression were also taken for assessment.
Statistical analyses
The analyses were performed using Review Manager 5.3 and Stata 12.0. Between-study heterogeneity was assessed using the chi-squared statistic and quantified by I2. I2<50% indicated that the studies were homogenous.46 A fixed effects model was conducted when the heterogeneity did not exist; otherwise, a random effects model was performed. OR was the principal measurement for therapeutic effects and is presented with a 95% CI. We further investigated potential sources of between-study heterogeneity by subgroup analyses based on the some baseline variables (study design and sample sizes). Publication bias was assessed visually by funnel plots and quantified in Egger’s test and Begg’s regression test.47,48 When publication bias existed, trim-and-fill method was applied to adjust the pooled estimates of potentially unpublished studies.
Results
Search results
A total of 1,291 articles were identified with the initial retrieve. 717 papers were excluded due to duplication. After title and abstract review, 468 articles were further excluded because they did not include clinical trials (n=344), were reviews or meta-analysis (n=7), were unrelated studies (n=104), or were case reports (n=13), leaving 106 studies as potentially relevant. After detailed assessment of full texts, articles without the control group (n=15), patients not treated by cinobufotalin injection (n=24) or TACE (n=19), studies with insufficient data (n=7), and studies published before 2000 (n=14) were excluded. Finally, 27 trials19–37 involving 2,079 advanced HC patients were included in this analysis (Figure 1).
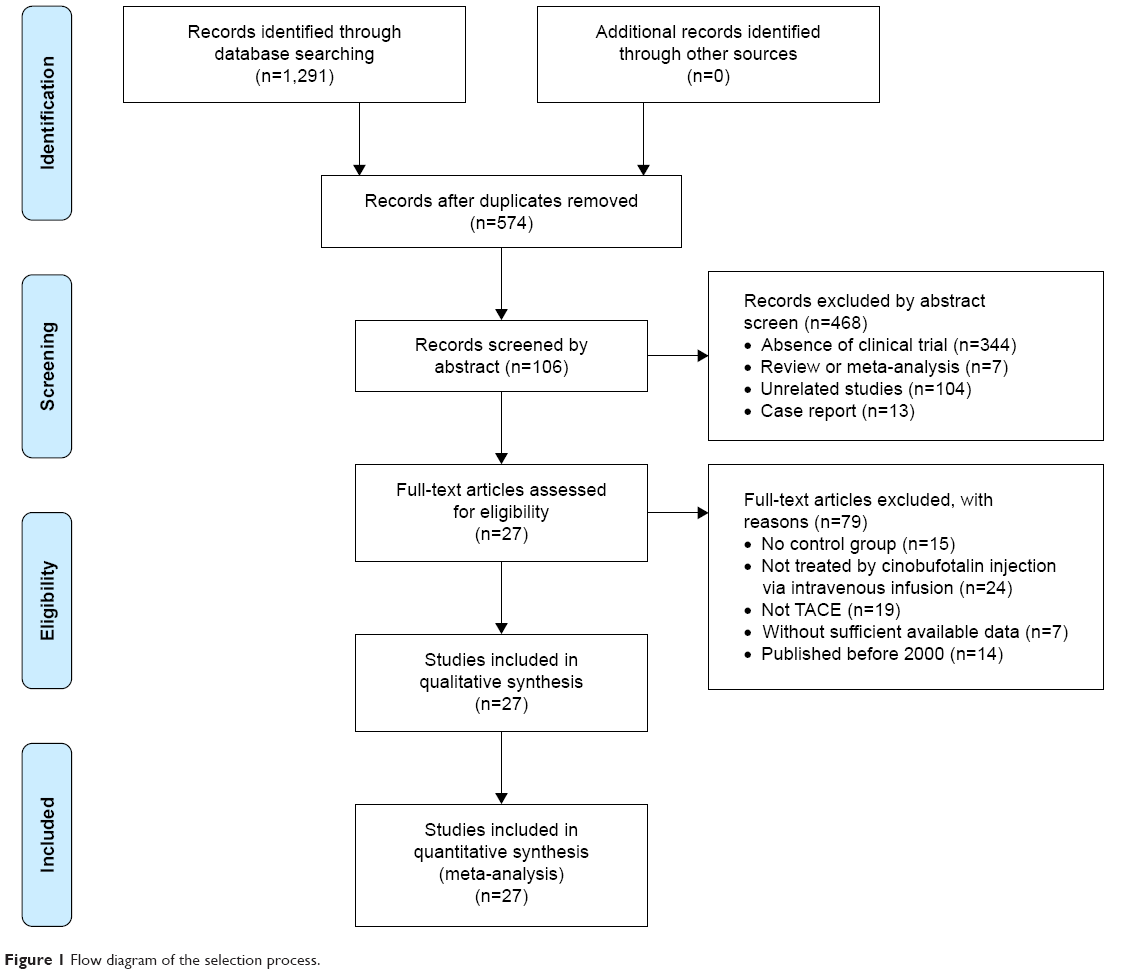 | Figure 1 Flow diagram of the selection process. |
Patients’ characteristics
After selection, all studies were carried out in the hospitals in China since 2000. In total, 1,045 advanced HC patients were treated by TACE in combination with cinobufotalin injection adjuvant therapy, while 1,034 patients were treated by TACE alone. Among all included studies, cinobufotalin injection and TACE were used simultaneously in the 16 trials,19–21,23,24,26,27,29–31,34,37–40,42 whereas cinobufotalin injection was used after TACE in nine articles18,22,25,28,32,33,35,36,44 and was used before TACE in two studies.41,43 Detailed information of the studies involved and HC patients is shown in Tables 1, 2, and S1.
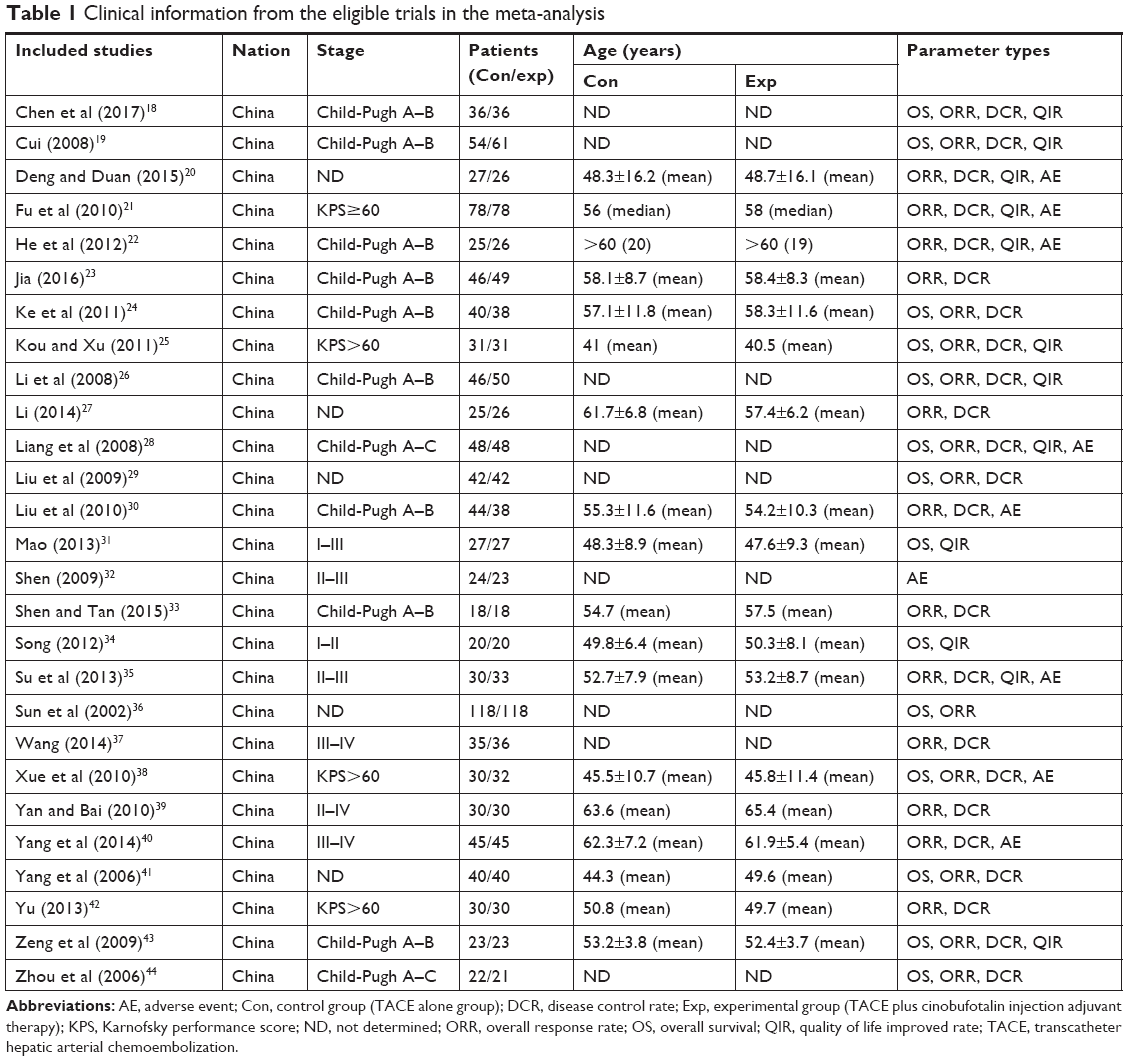 | Table 1 Clinical information from the eligible trials in the meta-analysis |
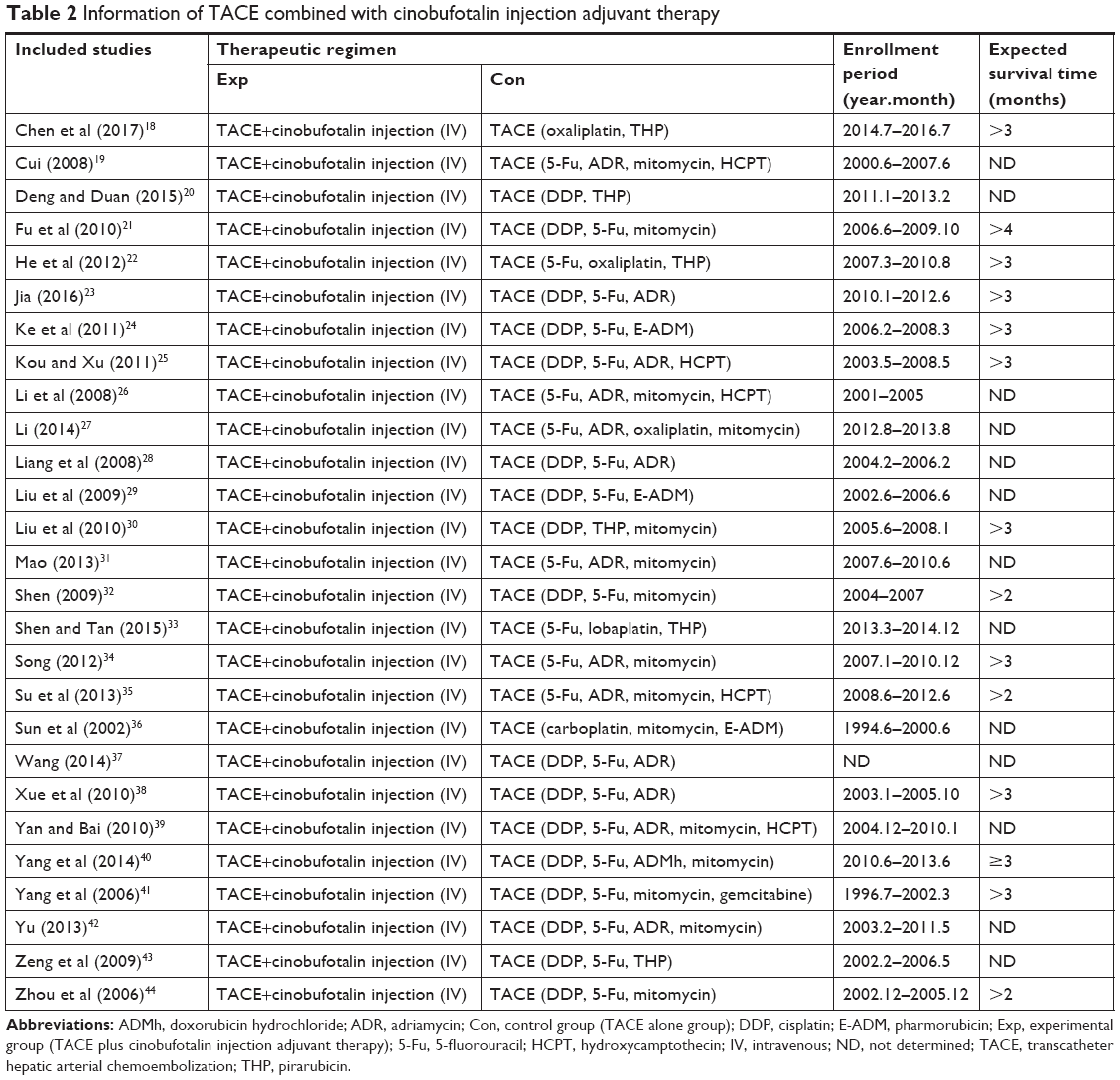 | Table 2 Information of TACE combined with cinobufotalin injection adjuvant therapy |
Quality assessment
The evaluation of bias risk is presented in Figure 2. Twenty-five studies had low risk and the other two studies did not have a clear description of randomization process. All included trials did not provide clear description of performance and detection risks. One study was regarded as a high risk due to the absence of follow-up, and 20 trials were considered as unclear risk owing to selective reporting.
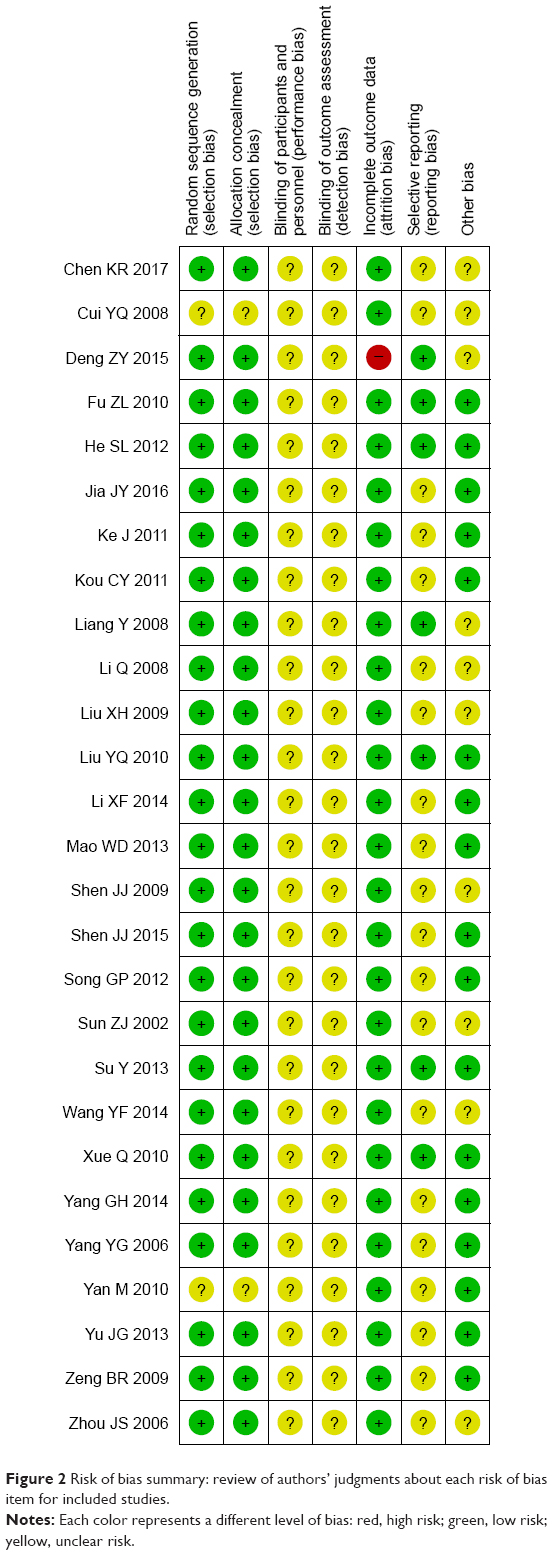 | Figure 2 Risk of bias summary: review of authors’ judgments about each risk of bias item for included studies. |
Therapeutic efficacy assessments
As shown in Figures 3 and 4 and Table 3, the analysis results showed that patients underwent combined therapy had significantly improved 1-, 1.5-, 2-, and 3-year OS (1-year OS, OR=2.84, 95% CI=2.20–3.67, P<0.00001; 1.5-year OS, OR=3.57, 95% CI=1.92–6.66, P<0.0001; 2-year OS, OR=3.17, 95% CI=2.36–4.25, P<0.00001; 3-year OS, OR=2.88, 95% CI=1.82–4.57, P<0.00001), CR rate (OR=1.73, 95% CI=1.04–2.87, P=0.03), PR rate (OR=1.61, 95% CI=1.31–1.97, P<0.00001), ORR (OR=1.86, 95% CI=1.54–2.24, P<0.00001), and DCR (OR=2.05, 95% CI=1.59–2.64, P<0.00001) and significantly decreased PD rate (OR=0.46, 95% CI=0.35–0.59, P<0.00001), whereas the 0.5-year OS and SD rate (0.5-year OS, OR=1.40, 95% CI=0.97–2.01, P=0.07; SD rate, OR=0.88, 95% CI=0.72–1.09, P=0.25) did not show significant difference from patients who received TACE alone.
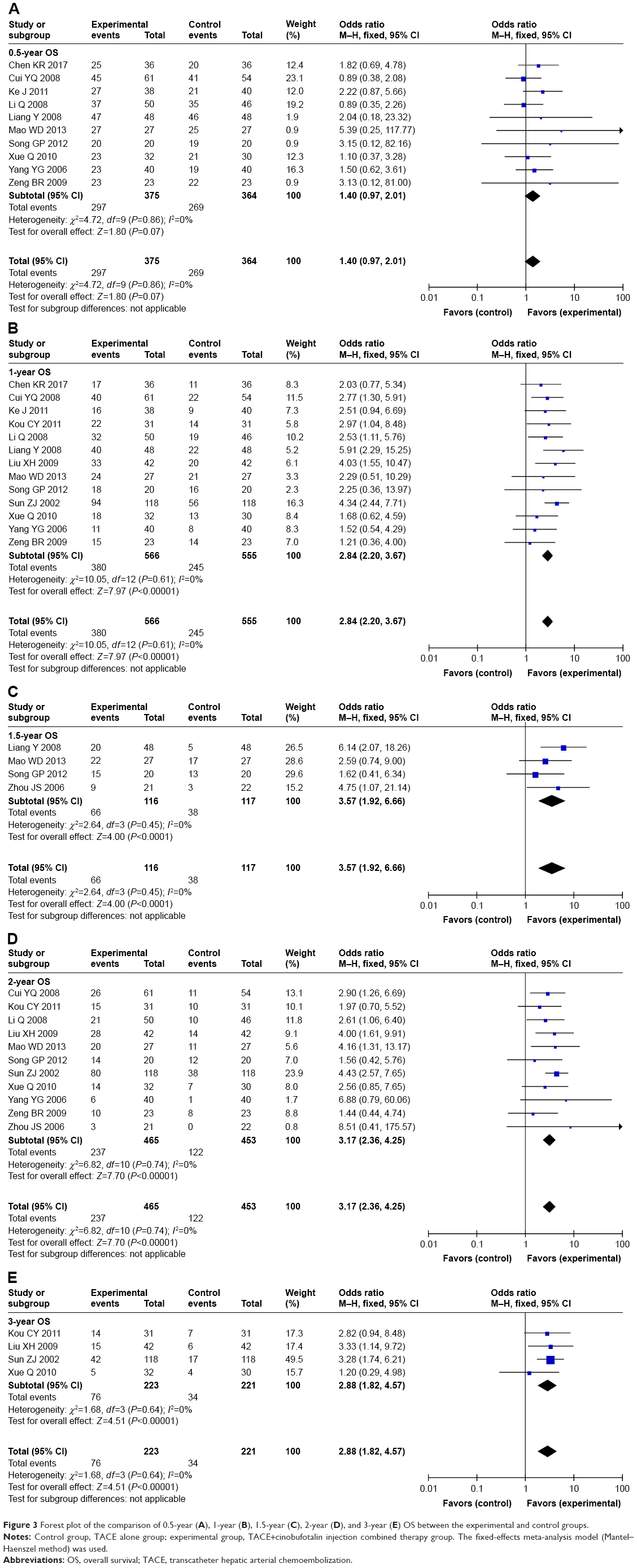 | Figure 3 Forest plot of the comparison of 0.5-year (A), 1-year (B), 1.5-year (C), 2-year (D), and 3-year (E) OS between the experimental and control groups. |
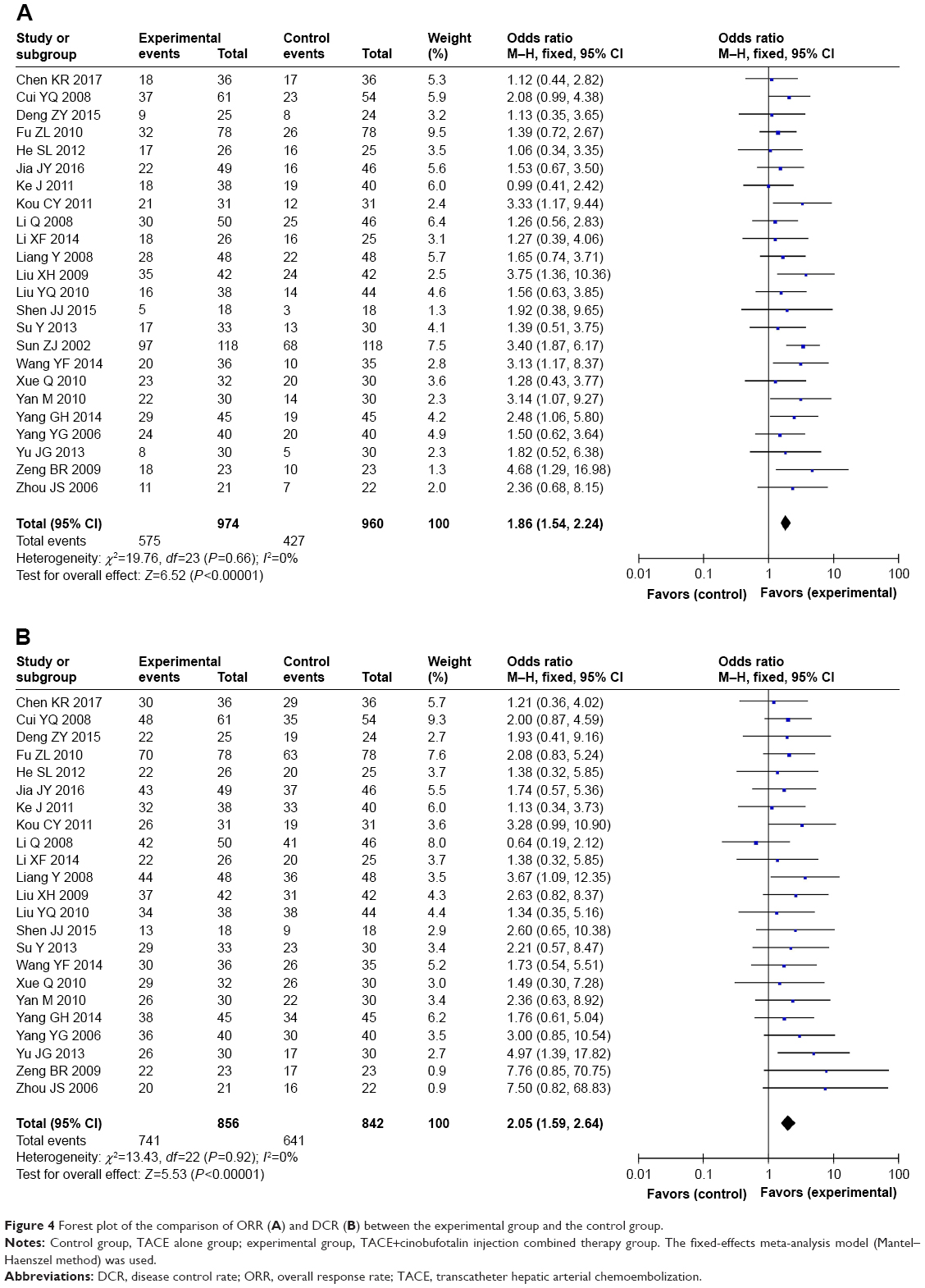 | Figure 4 Forest plot of the comparison of ORR (A) and DCR (B) between the experimental group and the control group. |
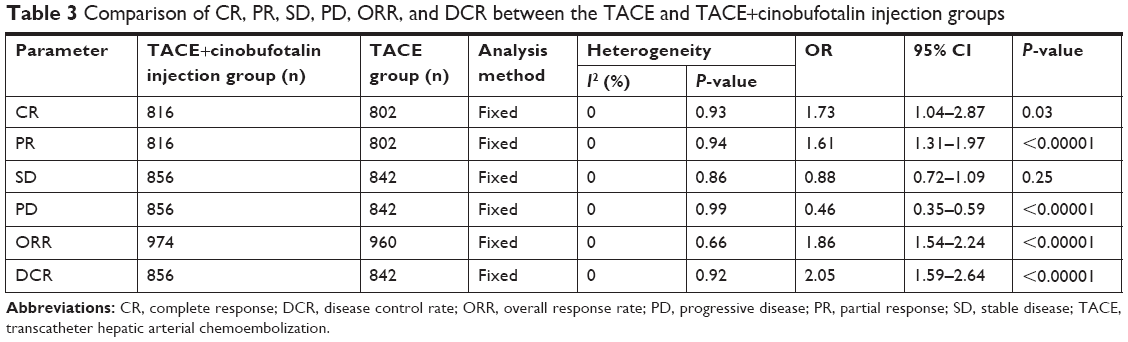 | Table 3 Comparison of CR, PR, SD, PD, ORR, and DCR between the TACE and TACE+cinobufotalin injection groups |
Quality of life assessment
Thirteen studies18–22,25,26,28,31,34,35,43,44 assessed the quality of life of advanced HC patients between the TACE+cinobufotalin injection and TACE alone groups. Results showed that quality of life of patients in the combined group was significantly better than that of the control group, indicated by significantly improved QIR (Figure 5; OR=3.45, 95% CI=2.52–4.72, P<0.00001).
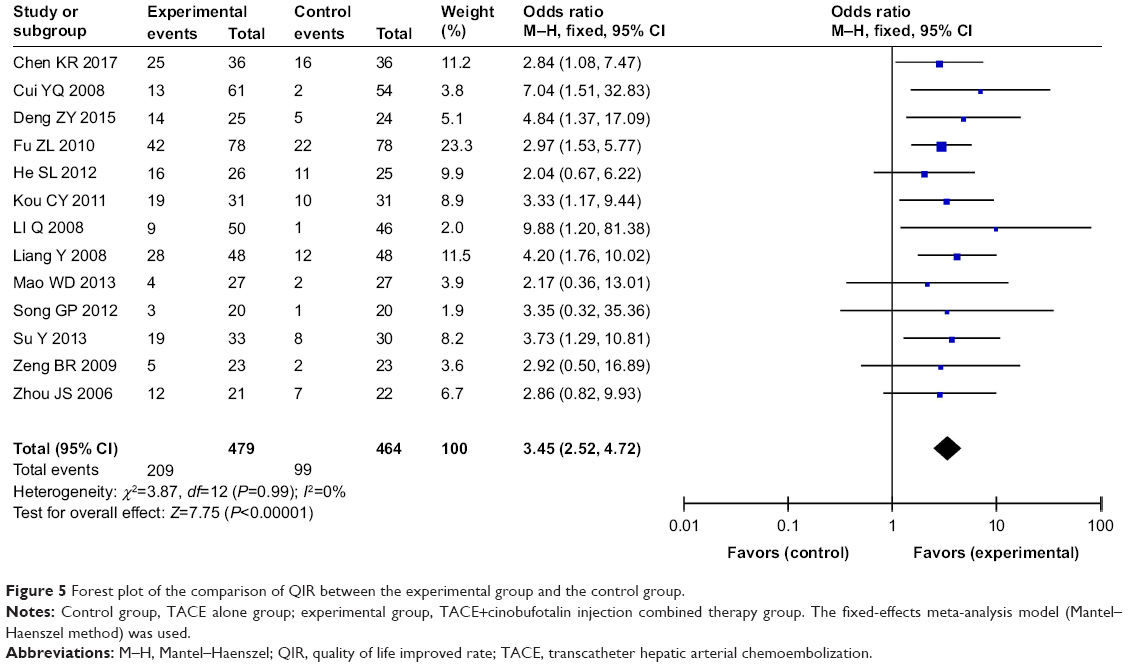 | Figure 5 Forest plot of the comparison of QIR between the experimental group and the control group. |
Liver function evaluation
Five clinical trials24,26,32,42,44 evaluated the liver function of advanced HC patients between the two groups. As shown in Figure 6, the liver function of HC patients who received combined therapy was significantly improved compared with TACE alone, indicated by obviously reduced TBIL, AST, and ALT (TBIL, OR=−9.21, 95% CI=−15.14 to −3.10, P=0.003; ALT, OR=−30.76, 95% CI=−41.65 to −19.88, P<0.00001; AST, OR=−30.66, 95% CI=−42.36 to −18.97, P<0.00001; ALB, OR=2.46, 95% CI=−2.75 to 7.67, P=0.35).
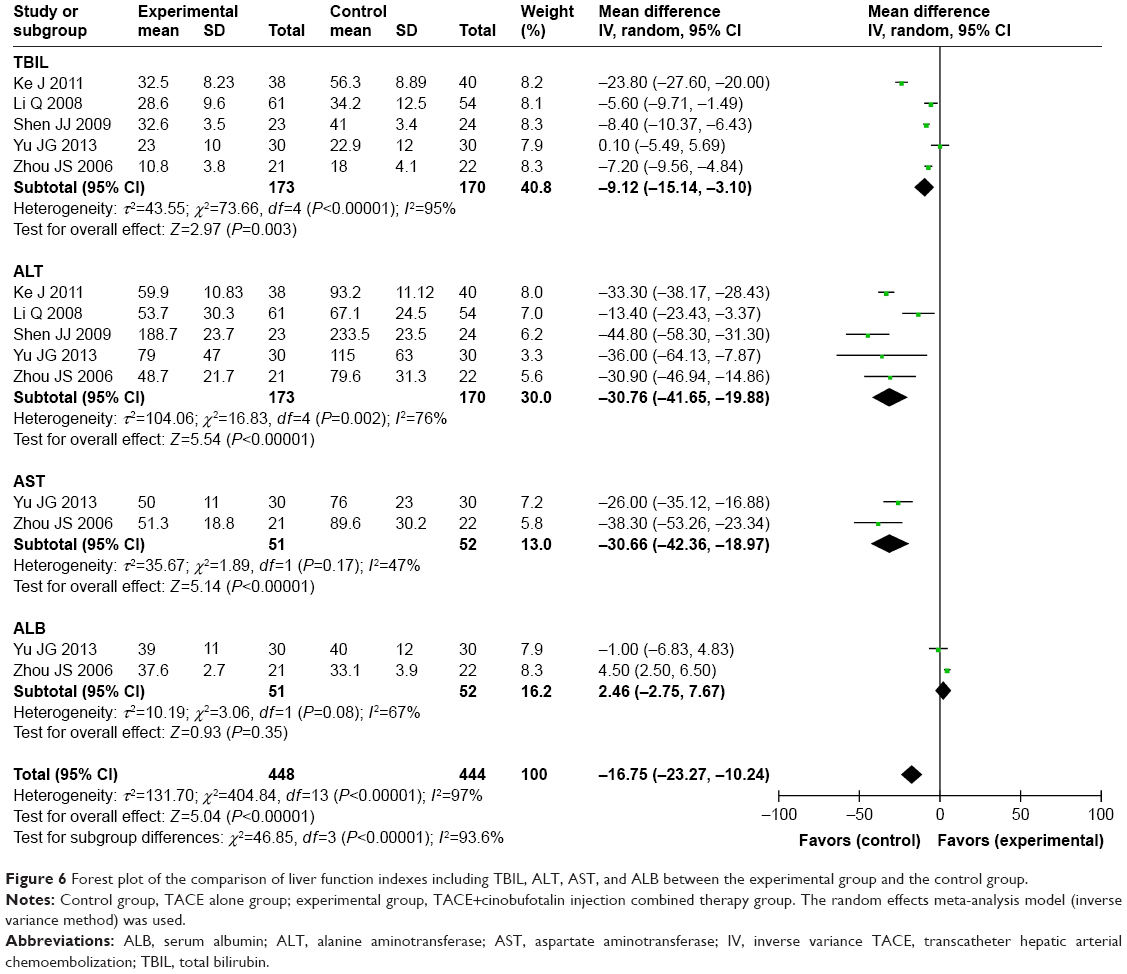 | Figure 6 Forest plot of the comparison of liver function indexes including TBIL, ALT, AST, and ALB between the experimental group and the control group. |
Immune function evaluation
The immune status of patients was examined between TACE and TACE+cinobufotalin injection group in five controlled studies.23,26,29,36,43 Compared with TACE alone, the percentages of CD3+, CD4+, and NK cells, and CD4+/CD8+ ratio in the combined treatment group were significantly increased (Figure 7; CD3+, OR=9.05, 95% CI=3.62–14.49, P=0.001; CD4+, OR=7.42, 95% CI=3.20–11.63, P=0.0006; NK, OR=10.00, 95% CI=2.08–17.92, P=0.01; CD4+/CD8+, OR=0.33, 95% CI=0.03–0.62, P=0.03).
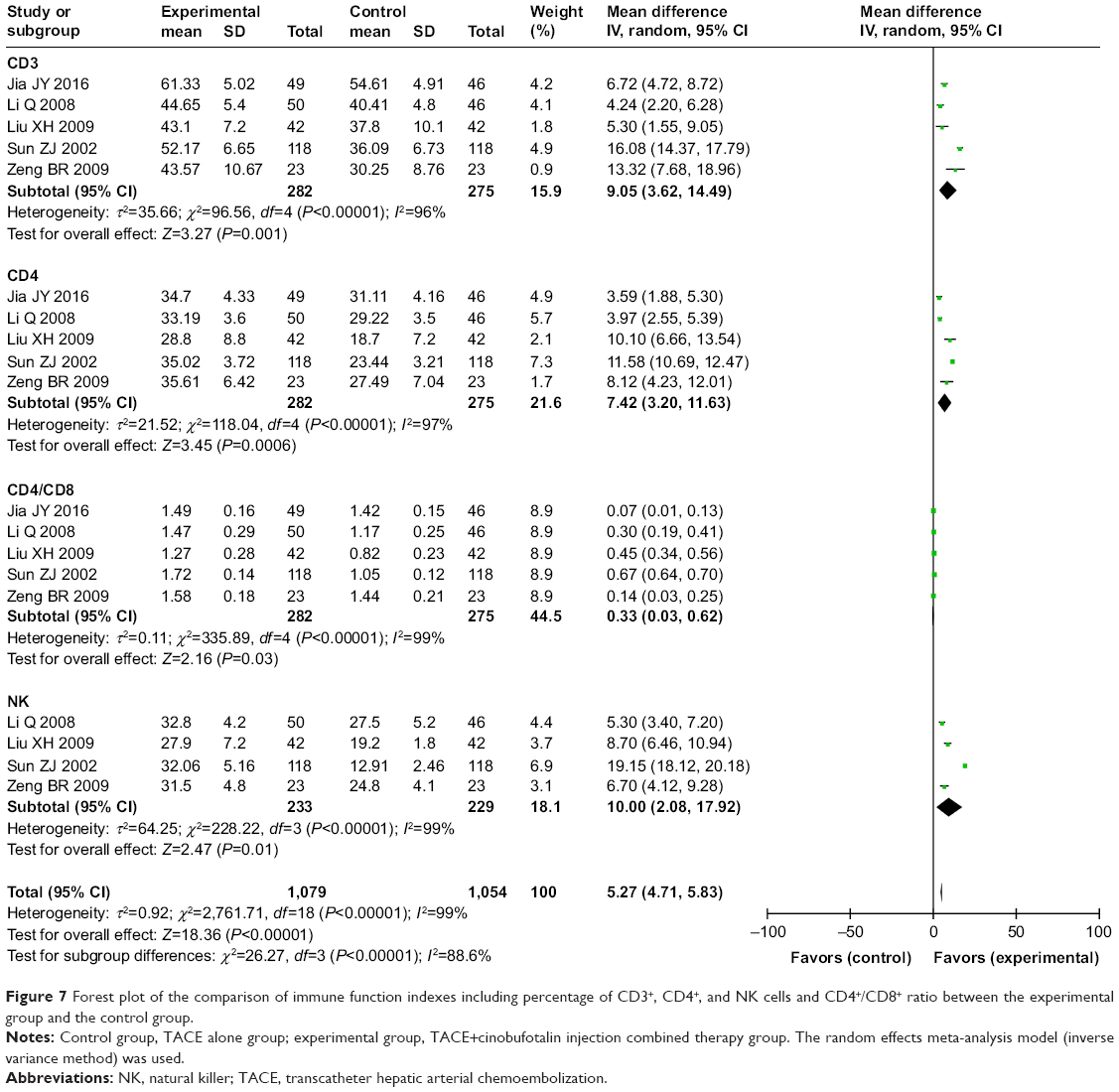 | Figure 7 Forest plot of the comparison of immune function indexes including percentage of CD3+, CD4+, and NK cells and CD4+/CD8+ ratio between the experimental group and the control group. |
Adverse events assessment
Safety of cinobufotalin injection-mediated therapy was evaluated in eight studies.20–22,28,30,32,35,38 As shown in Figure 8, no serious adverse events were reported during cinobufotalin injection-mediated therapy. The group that received TACE plus cinobufotalin injection had lower rates of myelosuppression (OR=0.29, 95% CI=0.15–0.57, P=0.0003), whereas analysis on other adverse events did not show significant difference (leukopenia, OR=2.74, 95% CI=0.25–30.43, P=0.41; thrombocytopenia, OR=1.08, 95% CI=0.46–2.52, P=0.86; nausea and vomiting, OR=0.57, 95% CI=0.21–1.57, P=0.28; fever, OR=1.23, 95% CI=0.16–9.78, P=0.84; hepatotoxicity, OR=0.83, 95% CI=0.22–3.13, P=0.79).
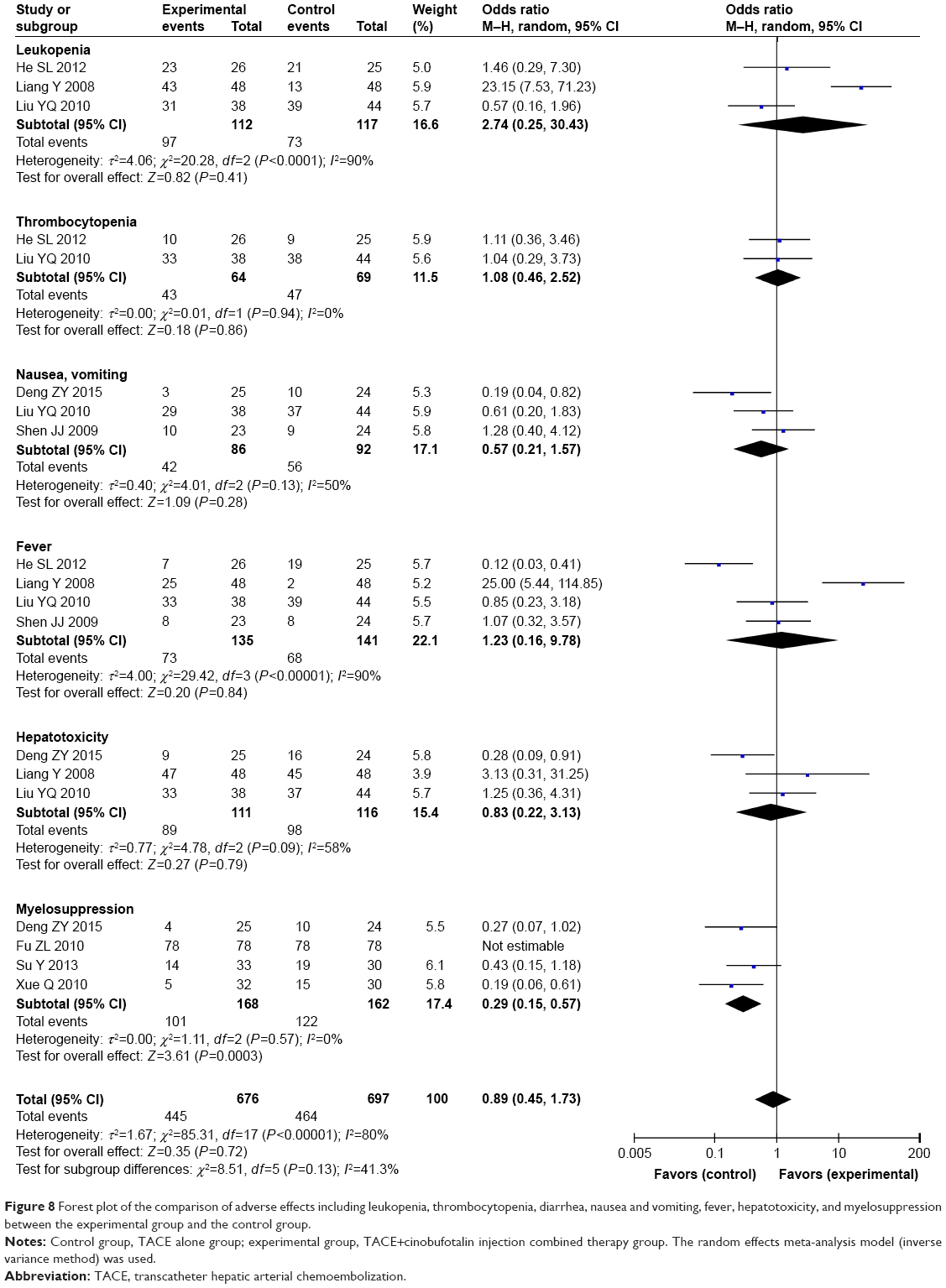 | Figure 8 Forest plot of the comparison of adverse effects including leukopenia, thrombocytopenia, diarrhea, nausea and vomiting, fever, hepatotoxicity, and myelosuppression between the experimental group and the control group. |
Publication bias
Publication bias was assessed visually by funnel plots and quantified in Egger’s test and Begg’s regression test. As shown in Figures 9 and 10 and Table 4, no significant publication bias for OS rate, CR rate, PR rate, SD rate, PD rate, and QIR was observed in these analyses, which confirmed the reliability of our primary conclusions.
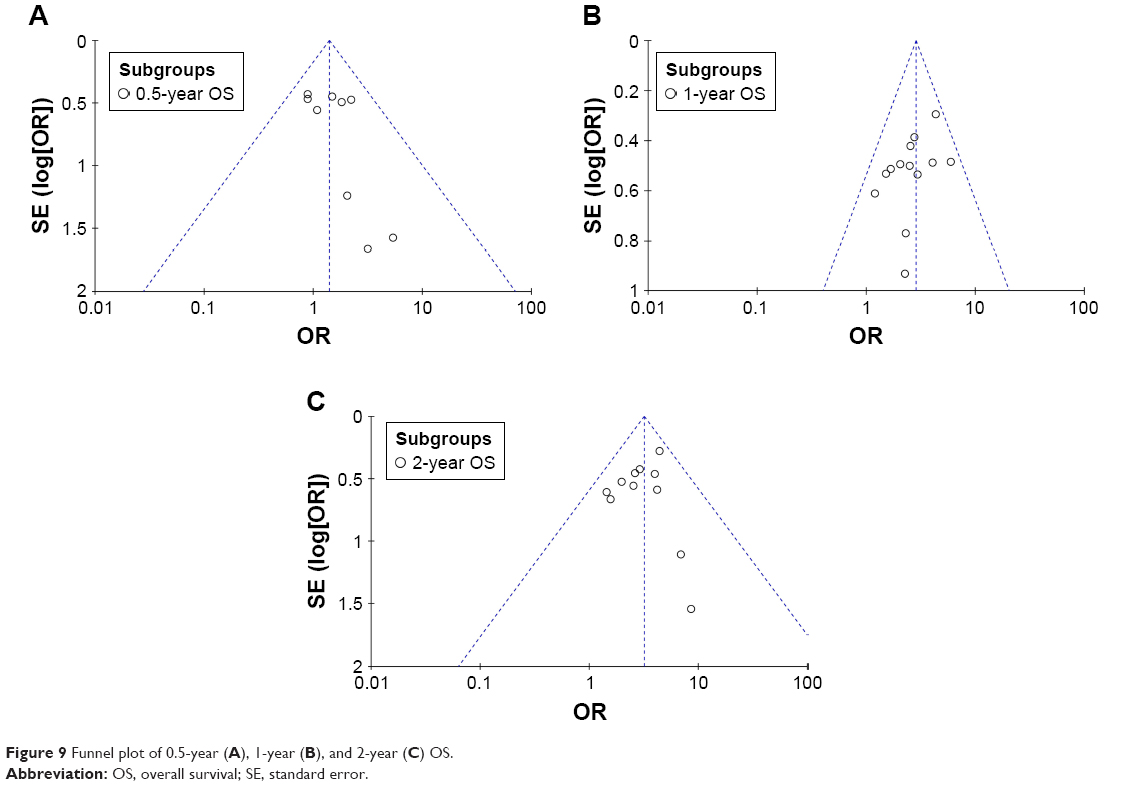 | Figure 9 Funnel plot of 0.5-year (A), 1-year (B), and 2-year (C) OS. |
 | Figure 10 Funnel plot of ORR (A) and DCR (B). |
 | Table 4 Publication bias on OS, CR, PR, SD, PD, ORR, DCR, and QIR |
Sensitivity analysis
We conducted subgroup analysis to explore the source of heterogeneity in OS rate, ORR, DCR, and QIR with respect to the study design and sample sizes of involved studies. As shown in Table 5, our analysis results showed that no significant difference was found between different study designs and sample sizes of studies in most of the primary indicators except 0.5-year OS.
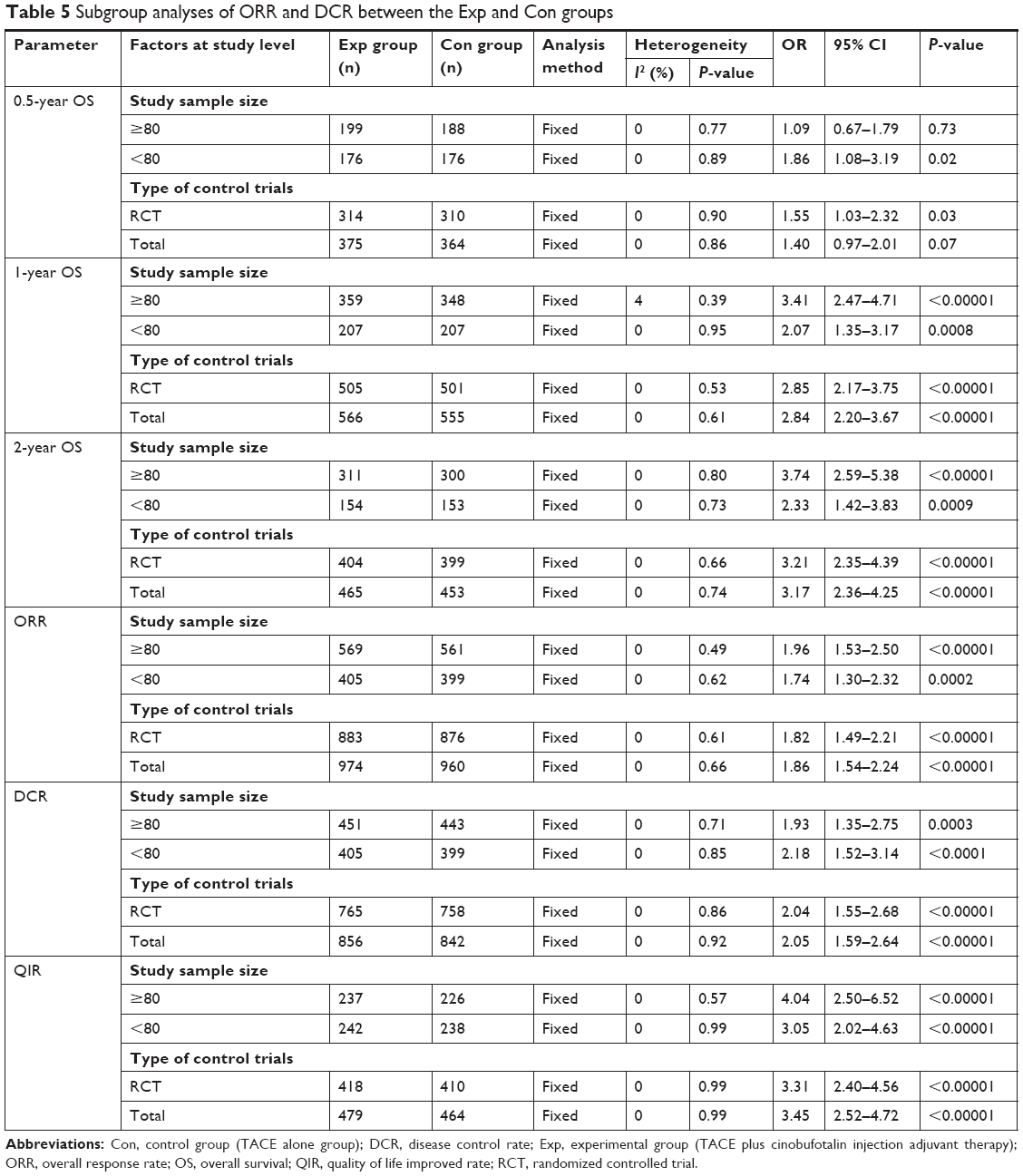 | Table 5 Subgroup analyses of ORR and DCR between the Exp and Con groups |
Discussion
In view of the limitations such as drug resistance and toxic side effects of the current chemotherapy for malignancies, more and more physicians are trying to find more adjunctive or auxiliary therapies to improve patients’ survival time or quality of life and to reduce side effects caused by chemotherapy. Traditional Chinese medicine has been utilized as an adjuvant method to treat HC for a long time. Several studies have been reported that the addition of cinobufotalin injection could be beneficial to patients with advanced HC. Even though there were statistical analyses of published clinical trials, the exact therapeutic effects were still not systematically evaluated because of small sample sizes and different applied protocols in different studies. In this analysis, we conducted a wide range of online search according to the strict inclusion and exclusion criteria, by which to provide clear and systematical conclusion.
Our meta-analysis revealed that TACE combined with cinobufotalin injection adjuvant therapy is associated with a favorable efficacy compared to HC patients treated by TACE alone. Compared to patients treated by TACE alone, patients treated with combined therapy showed markedly increased 1- to 3-year OS, CR rate, PR rate, ORR, DCR, and QIR (P<0.05). Moreover, after TACE and cinobufotalin injection combined treatment, the liver function of HC patients was obviously improved, indicated by increased ALB and decreased TBIL, ALT, and AST, although changes in ALB did not show statistical significance. These results indicated that intravenous infusion of cinobufotalin injection could increase the curative effect of TACE.
The immunosuppressed status of cancer patients has been reported previously.47 Therefore, immune system reconstruction is one of the critical factors to effectively treat malignancies.47 Many studies reported that cinobufotalin injection can enhance the ability of body’s immunity and resistance to tumors by increasing the IL-2 and interferon (IFN)-γ secretion of T cells and the activities of NK cells and by promoting the maturation of dendritic cells and upregulating the expression of costimulatory molecules in dendritic cells. Our analysis showed significantly increased percentages of CD3+, CD4+, NK, and CD3+CD56+ T cells and CD4+/CD8+ ratio, indicating that immune function of HC patients was improved after cinobufotalin injection-mediated therapy.
Safety is the top priority of the clinical treatment, and it is also a key factor for the development of cinobufotalin injection-mediated therapy. Our analysis showed no significant difference in most adverse events between the two groups, while the myelosuppression caused by TACE was obviously alleviated (P<0.05), which proves the safety of cinobufotalin injection treatment for advanced HC.
Some factors may have influence on the therapeutic effects of cinobufotalin injection treatment. In our study, subgroup analysis was used for evaluating the impact of study design and sample size on therapeutic effects of cinobufotalin injection-mediated therapy. Our results found no difference between different study designs and sample sizes of studies in most indexes, except 0.5-year OS. However, currently, studies probing the impact of these factors on treatment effects of cinobufotalin injection adjuvant therapy are still insufficient, and these should be further researched and explored.
There are a few limitations in our study. First, all included researches were performed in different medical institutions in China, which may bring in regional bias and influence the clinical application of cinobufotalin injection-mediated therapy worldwide. In addition, different trials evaluated the treatment efficacy with different outcomes, resulting in a reduction in the size of the statistical sample, making it difficult to summarize the results at the same scale. Finally, the therapeutic effects of the combined therapy may be influenced by numerous variables such as chemotherapeutics types, tumor stage, tumor size, and patient’s age. Due to the above limitations, future studies and generated data will be valuable to further verify the safety and efficacy of cinobufotalin injection-mediated therapy.
In summary, our study confirmed that TACE combined with cinobufotalin injection adjuvant therapy was an effective treatment for advanced HC patients. Intravenous infusion of cinobufotalin injection markedly enhanced the treatment efficacy of TACE for advanced HC. Moreover, cinobufotalin injection-mediated therapy can effectively improve the quality of life, immune function, and liver function of HC patients. Therefore, cinobufotalin injection-mediated therapy could be recommended as an adjuvant treatment method for end-stage HC.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Zhang Y, Hui F, Yang Y, et al. Can Kushen injection combined with TACE improve therapeutic efficacy and safety in patients with advanced HCC? a systematic review and network meta-analysis. Oncotarget. 2017;8(63):107258–107272. | ||
Liu X, Wang Z, Chen Z, et al. Efficacy and safety of transcatheter arterial chemoembolization and transcatheter arterial chemotherapy infusion in hepatocellular carcinoma: a systematic review and meta-analysis. Oncol Res. 2018;26(2):231–239. | ||
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. | ||
Ma X, Li RS, Wang J, et al. The therapeutic efficacy and safety of compound kushen injection combined with transarterial chemoembolization in unresectable hepatocellular carcinoma: an update systematic review and meta-analysis. Front Pharmacol. 2016;7:70. | ||
Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. | ||
Cho WC, Chen HY. Transcatheter arterial chemoembolization combined with or without Chinese herbal therapy for hepatocellular carcinoma: meta-analysis. Expert Opin Investig Drugs. 2009;18(5):617–635. | ||
Llovet JM, Real MI, Montaña X, et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. 2002;359(9319):1734–1739. | ||
Oliveri RS, Wetterslev J, Gluud C, Transarterial GC. Transarterial (chemo)embolisation for unresectable hepatocellular carcinoma. Cochrane Database Syst Rev. 2011;3(3):CD004787. | ||
Sergio A, Cristofori C, Cardin R, et al. Transcatheter arterial chemoembolization (TACE) in hepatocellular carcinoma (HCC): the role of angiogenesis and invasiveness. Am J Gastroenterol. 2008;103(4):914–921. | ||
Zhai XF, Chen Z, Li B, et al. Traditional herbal medicine in preventing recurrence after resection of small hepatocellular carcinoma: a multicenter randomized controlled trial. J Integr Med. 2013;11(2):90–100. | ||
Tian HQ, Li HL, Wang B, et al. Treatment of middle/late stage primary hepatic carcinoma by Chinese medicine comprehensive therapy: A prospective randomized controlled study. Chin J Integr Med. 2010;16(2):102–108. | ||
Meng Z, Yang P, Shen Y, et al. Pilot study of huachansu in patients with hepatocellular carcinoma, nonsmall-cell lung cancer, or pancreatic cancer. Cancer. 2009;115(22):5309–5318. | ||
Kai S, Lu JH, Hui PP, Zhao H. Pre-clinical evaluation of cinobufotalin as a potential anti-lung cancer agent. Biochem Biophys Res Commun. 2014;452(3):768–774. | ||
Emam H, Zhao QL, Furusawa Y, et al. Apoptotic cell death by the novel natural compound, cinobufotalin. Chem Biol Interact. 2012;199(3):154–160. | ||
Chen KK, Anderson RC, Henderson FG. Comparison of cardiac action of bufalin, cinobufotalin, and telocinobufagin with cinobufagin. Proc Soc Exp Biol Med. 1951;76(2):372–374. | ||
Cheng L, Chen YZ, Peng Y, et al. Ceramide production mediates cinobufotalin-induced growth inhibition and apoptosis in cultured hepatocellular carcinoma cells. Tumour Biol. 2015;36(8):5763–5771. | ||
Li QW, Sun T, Hu KW. Research progress on anti-tumor mechanism of cinobufagin. China J Tradit Chin Med Pharm. 2010;25(12):2075–2078. | ||
Chen KR, Zhang HW, Ma JL. Clinical efficacy of TACE combined with cinobufotalin injection and Entecavir dispersible tablets for liver cancer. J Clin Med Lit. 2017;4(56):11021–11022. | ||
Cui YQ. Clinical analysis of 61 cases of liver cancer patients treated by cinobufotalin combined with TACE. J Binzhou Med Univ. 2008;31(6):463–464. | ||
Deng ZY, Duan HB. Clinical observation of cinobufacini injection combined with TACE in the treatment of hepatocellular carcinoma. Tianjin J Tradit Chin Med. 2015;32(5):275–278. | ||
Fu ZL, Qu ZH, Wang Y. The clinical research of huachansu injection combined with interventional therapy for middle and advanced stages of hepatocellular carcinoma. China Pract Med. 2010;5(34):107–108. | ||
He SL, Liu LM, Sun XJ, Shen J. Effect of huachansu injection sequence TACE including oxaliplatin regimen for advanced hepatocelluler carcinoma. Chin J Clin. 2012;6(14):3880–3883. | ||
Jia JY. Clinical effect of cinobufagin combined with transhepatic arterial chemotherapy and embolization in the treatment of primary hepatocellular carcinoma. China Mod Med. 2016;23(8):52–57. | ||
Ke J, Lu K, Li Y. Clinical observation of patients with primary liver cancer treated by cinobufagin Injection combined with transcatheter arterial chemoembolization (TACE). China Pract Med. 2011;6(34):1–2. | ||
Kou CY, Xu Z. The clinical analysis of huachansu injection combines with transcatheter arterial chemoembolization for middle and advanced stages of hepatocellular carcinoma treatment. Chin J Misdiagnostics. 2011;11(25):6151–6152. | ||
Li Q, Sun BM, Peng YH, Fan ZZ, Sun J. Clinical study on the treatment of primary liver cancer by cinobufotain combined with transcatheter arterial chemoembolization. Acta Universitatis Traditionis Medicalis Sinensis Pharmacologiaeque Shanghai. 2008;22(2):32–34. | ||
Li XF. Clinical observation of cinobufacini injection combined with transcatheter hepatic arterial chemoembolization for primary hepatocellular carcinoma. China Health Care Nutr. 2014;7:3728. | ||
Liang Y, Long JZ, Liu H, Feng J. Study of cinobufotalin and interferon combined with transcatheter hepatic arterial chemoembolization on primary hepatocellular carcinoma. Modern J Integr Tradit Chin West Med. 2008;17(11):1628–1630. | ||
Liu XH, Fu H, Zhu QH, Pan PS, Yang L. The clinical study of cinobufotalin injection combined with transcatheter hepatic arterial chemoembolization on hepatocellular carcinoma. Chin J Mod Drug Appl. 2009;3(23):134–135. | ||
Liu YQ, Zh Y, Shao ZH, Jiang ZY, Liu XW. The clinical study of cinobufotalin injection combined with transcatheter arterial chemoembolization for hepatocellular carcinoma treatment. Chin Rural Health Serv Admin. 2010;30(5):402–404. | ||
Mao WD. Clinical study of cinobufotalin injection intervention on the postoperative recurrence of primary liver cancer. Anhui Med Pharm J. 2013;17(12):2144–2145. | ||
Shen JJ. The clinical effect of Cinobufagin injection by transcatheter arterial chemoembolization (TACE) combined with intravenous on treating primary liver cancer (PLC). J Clin Hepatol. 2009;25(3):207–209. | ||
Shen JJ, Tan SZ. Transcatheter arterial embolization with cinobufacini on terminal stage of hepatocellular carcinoma. Jilin J Tradit Chin Med. 2015;35(7):678–680. | ||
Song GP. Effect of cinobufagin injection on prevention of recurrence of primary liver cancer with radical resection. Chin J Exp Tradit Med Formulae. 2012;18(22):307–309. | ||
Su Y, Yang JQ, Guo CQ. The cinobufotalin injection in combination with transcatheter arterial chemoembolization for advance hepatocellular carcinoma treatment. J Basic Clin Oncol. 2013;26(3):245–246. | ||
Sun ZJ, Pan CN, Wang GJ. Clinical observation on cinobufotain in treating hepatocellular carcinoma after transcather arterial chemoembolization. Cancer Res Prevent Treat. 2002;29(1):67–68. | ||
Wang YF. TACE combined with cinobufotalin in the treatment of primary liver cancer. J Basic Clin Oncol. 2014;27(5):417–418. | ||
Xue Q, Lu LQ, Yuan GR, Zhao TW. Clinical study of cinobufotalin combined with TACE for the treatment of 32 cases patients with middle and advanced liver cancer. Jiangsu J Tradit Chin Med. 2010;42(2):22–24. | ||
Yan M, Bai XJ. Clinical observation of 30 cases of advanced liver cancer treated by cinobufotalin injection and chemotherapy. J Pract Tradit Chin Med. 2010;26(8):554–555. | ||
Yang GH, Xue T, Li P, Yu XM, Mo JM, Xu LP. Study of cinobufacini injection intervention on serum prealbumin and vascular endothelial growth factor in patients with primary liver cancer. Chin Arch Tradit Chin Med. 2014;32(5):1086–1088. | ||
Yang YG, Li J, Ma YH, Liu JS. Clinical observation of cinobufacini injection intervention combined with chemotherapy for the treatment of advanced liver cancer. J Pract Tradit Chin Med. 2006;22(1):20. | ||
Yu JG. Clinical observation of cinobufotalin injection combined with transcatheter hepatic arterial chemoembolization for the treatment of primary liver cancer. Modern Digestion Interv. 2013;18(1):32–33. | ||
Zeng BR, He X, Li P. The clinical research on the treatment of primary liver cancer by sequential therapy of cinobufotalin intravenous and transcathether arterial infusion. J Emerg Tradit Chin Med. 2009;18(4):525–527. | ||
Zhou JS, Lu H, Wu XD, Xu S. Effects of huachansu injection combined with transcatheter arterial chemoembolization on patients with advanced unresectable hepatocelluler carcinoma. Chin J Prim Med Pharm. 2006;13(4):571–572. | ||
Zeng X, Zhang Y, Kwong JS, et al. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: a systematic review. J Evid Based Med. 2015;8(1):2–10. | ||
Jackson D, White IR, Riley RD. Quantifying the impact of between-study heterogeneity in multivariate meta-analyses. Stat Med. 2012;31(29):3805–3820. | ||
Zhang L, Mu Y, Zhang A, et al. Cytokine-induced killer cells/dendritic cells-cytokine induced killer cells immunotherapy combined with chemotherapy for treatment of colorectal cancer in China: a meta-analysis of 29 trials involving 2,610 patients. Oncotarget. 2017;8(28):45164–45177. | ||
Liang M, Chen Q, Zhang Y, et al. Impact of diabetes on the risk of bedsore in patients undergoing surgery: an updated quantitative analysis of cohort studies. Oncotarget. 2017;8(9):14516–14524. |
Supplementary materials
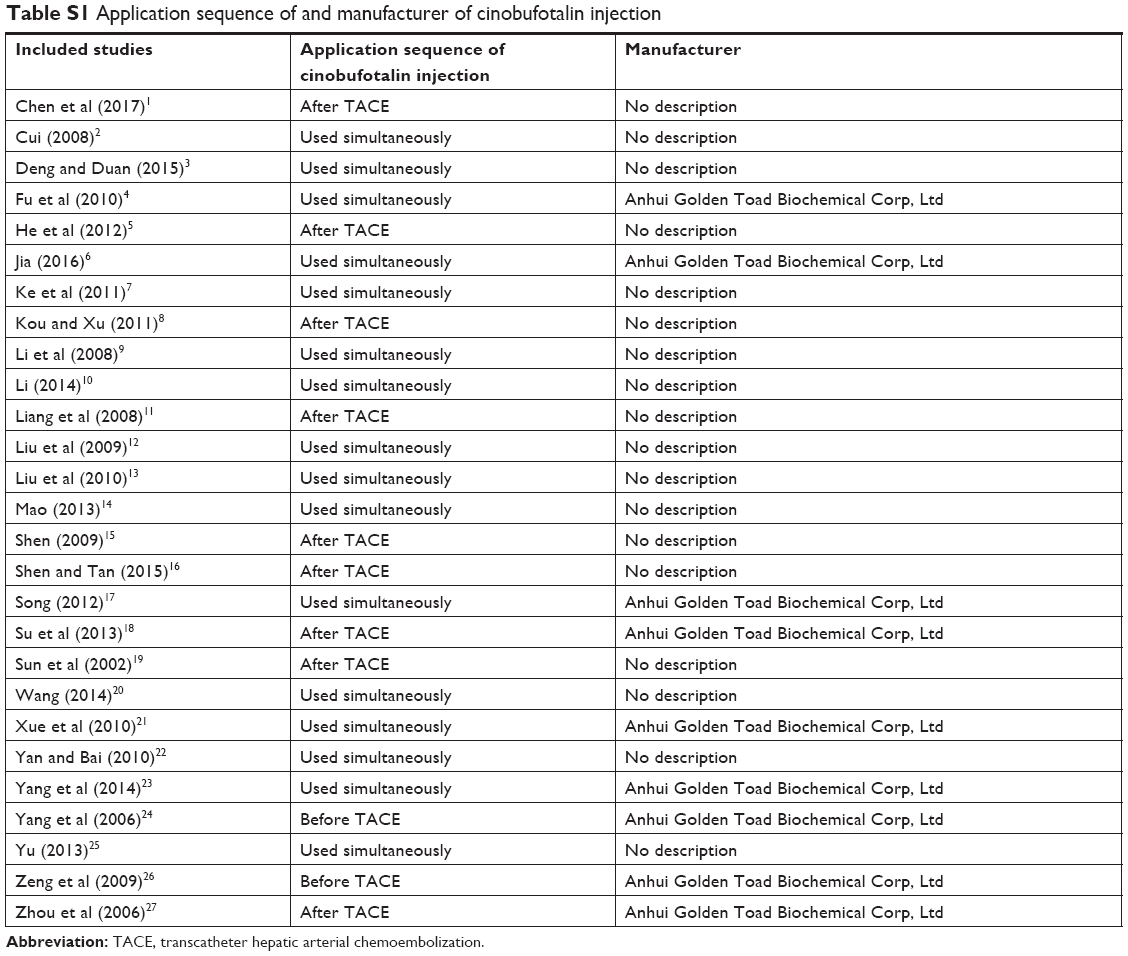 | Table S1 Application sequence of and manufacturer of cinobufotalin injection |
References
Chen KR, Zhang HW, Ma JL. Clinical efficacy of TACE combined with cinobufotalin injection and Entecavir dispersible tablets for liver cancer. J Clin Med Lit. 2017;4(56):11021–11022. | ||
Cui YQ. Clinical analysis of 61 cases of liver cancer patients treated by cinobufotalin combined with TACE. J Binzhou Med Univ. 2008;31(6):463–464. | ||
Deng ZY, Duan HB. Clinical observation of cinobufacini injection combined with TACE in the treatment of hepatocellular carcinoma. Tianjin J Tradit Chin Med. 2015;32(5):275–278. | ||
Fu ZL, Qu ZH, Wang Y. The clinical research of huachansu injection combined with interventional therapy for middle and advanced stages of hepatocellular carcinoma. China Pract Med. 2010;5(34):107–108. | ||
He SL, Liu LM, Sun XJ, Shen J. Effect of huachansu injection sequence TACE including oxaliplatin regimen for advanced hepatocelluler carcinoma. Chin J Clin. 2012;6(14):3880–3883. | ||
Jia JY. Clinical effect of cinobufagin combined with transhepatic arterial chemotherapy and embolization in the treatment of primary hepatocellular carcinoma. China Mod Med. 2016;23(8):52–57. | ||
Ke J, Lu K, Li Y. Clinical observation of patients with primary liver cancer treated by cinobufagin Injection combined with transcatheter arterial chemoembolization (TACE). China Pract Med. 2011;6(34):1–2. | ||
Kou CY, Xu Z. The clinical analysis of huachansu injection combines with transcatheter arterial chemoembolization for middle and advanced stages of hepatocellular carcinoma treatment. Chin J Misdiagnostics. 2011;11(25):6151–6152. | ||
Li Q, Sun BM, Peng YH, Fan ZZ, Sun J. Clinical study on the treatment of primary liver cancer by cinobufotain combined with transcatheter arterial chemoembolization. Acta Universitatis Traditionis Medicalis Sinensis Pharmacologiaeque Shanghai. 2008;22(2):32–34. | ||
Li XF. Clinical observation of cinobufacini injection combined with transcatheter hepatic arterial chemoembolization for primary hepatocellular carcinoma. China Health Care Nutr. 2014;7:3728. | ||
Liang Y, Long JZ, Liu H, Feng J. Study of cinobufotalin and interferon combined with transcatheter hepatic arterial chemoembolization on primary hepatocellular carcinoma. Modern J Integr Tradit Chin West Med. 2008;17(11):1628–1630. | ||
Liu XH, Fu H, Zhu QH, Pan PS, Yang L. The clinical study of cinobufotalin injection combined with transcatheter hepatic arterial chemoembolization on hepatocellular carcinoma. Chin J Mod Drug Appl. 2009;3(23):134–135. | ||
Liu YQ, Zh Y, Shao ZH, Jiang ZY, Liu XW. The clinical study of cinobufotalin injection combined with transcatheter arterial chemoembolization for hepatocellular carcinoma treatment. Chin Rural Health Serv Admin. 2010;30(5):402–404. | ||
Mao WD. Clinical study of cinobufotalin injection intervention on the postoperative recurrence of primary liver cancer. Anhui Med Pharm J. 2013;17(12):2144–2145. | ||
Shen JJ. The clinical effect of Cinobufagin injection by transcatheter arterial chemoembolization (TACE) combined with intravenous on treating primary liver cancer (PLC). J Clin Hepatol. 2009;25(3):207–209. | ||
Shen JJ, Tan SZ. Transcatheter arterial embolization with cinobufacini on terminal stage of hepatocellular carcinoma. Jilin J Tradit Chin Med. 2015;35(7):678–680. | ||
Song GP. Effect of cinobufagin injection on prevention of recurrence of primary liver cancer with radical resection. Chin J of Exp Tradit Med Formulae. 2012;18(22):307–309. | ||
Su Y, Yang JQ, Guo CQ. The cinobufotalin injection in combination with transcatheter arterial chemoembolization for advance hepatocellular carcinoma treatment. J Basic Clin Oncol. 2013;26(3):245–246. | ||
Sun ZJ, Pan CN, Wang GJ. Clinical observation on cinobufotain in treating hepatocellular carcinoma after transcather arterial chemoembolization. Cancer Res Prevent Treat. 2002;29(1):67–68. | ||
Wang YF. TACE combined with cinobufotalin in the treatment of primary liver cancer. J Basic Clin Oncol. 2014;27(5):417–418. | ||
Xue Q, Lu LQ, Yuan GR, Zhao TW. Clinical study of cinobufotalin combined with TACE for the treatment of 32 cases patients with middle and advanced liver cancer. Jiangsu J Tradit Chin Med. 2010;42(2):22–24. | ||
Yan M, Bai XJ. Clinical observation of 30 cases of advanced liver cancer treated by cinobufotalin injection and chemotherapy. J Pract Tradit Chin Med. 2010;26(8):554–555. | ||
Yang GH, Xue T, Li P, Yu XM, Mo JM, Xu LP. Study of cinobufacini injection intervention on serum prealbumin and vascular endothelial growth factor in patients with primary liver cancer. Chin Arch Tradit Chin Med. 2014;32(5):1086–1088. | ||
Yang YG, Li J, Ma YH, Liu JS. Clinical observation of cinobufacini injection intervention combined with chemotherapy for the treatment of advanced liver cancer. J Pract Tradit Chin Med. 2006;22(1):20. | ||
Yu JG. Clinical observation of cinobufotalin injection combined with transcatheter hepatic arterial chemoembolization for the treatment of primary liver cancer. Modern Digestion Interv. 2013;18(1):32–33. | ||
Zeng BR, He X, Li P. The clinical research on the treatment of primary liver cancer by sequential therapy of cinobufotalin intravenous and transcathether arterial infusion. J Emerg Tradit Chin Med. 2009;18(4):525–527. | ||
Zhou JS, Lu H, Wu XD, Xu S. Effects of huachansu injection combined with transcatheter arterial chemoembolization on patients with advanced unresectable hepatocelluler carcinoma. Chin J Prim Med Pharm. 2006;13(4):571–572. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.