Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Transarterial Chemoembolization in Hepatocellular Carcinoma: Lessons from a 10-Year Real-World Retrospective Study
Authors von Schoen-Angerer G, Pesola G, Garo ML ![]() , Marini G, Cappio S, Cerny A, Magenta L, Majno-Hurst P, Bernardi L, Cefalì M, Cristaudi A, Terziroli Beretta-Piccoli B, Trevisi E, De Dosso S
, Marini G, Cappio S, Cerny A, Magenta L, Majno-Hurst P, Bernardi L, Cefalì M, Cristaudi A, Terziroli Beretta-Piccoli B, Trevisi E, De Dosso S
Received 25 January 2026
Accepted for publication 14 May 2026
Published 15 June 2026 Volume 2026:13 598858
DOI https://doi.org/10.2147/JHC.S598858
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Mohamed Shaker
Gayane von Schoen-Angerer,1,* Guido Pesola,2,* Maria Luisa Garo,3 Gianluigi Marini,2,4 Stefano Cappio,4 Andreas Cerny,5 Lorenzo Magenta,5 Pietro Majno-Hurst,1,6 Lorenzo Bernardi,6 Marco Cefalì,2 Alessandra Cristaudi,6 Benedetta Terziroli Beretta-Piccoli,1,7 Elena Trevisi,2 Sara De Dosso1,2
1Faculty of Biomedical Sciences, University of Southern Switzerland (USI), Lugano, Switzerland; 2Medical Oncology Department, Oncology Institute of Southern Switzerland (IOSI), Ente Ospedaliero Cantonale (EOC), Bellinzona, Switzerland; 3Mathsly Research, Biostatistics Unit, Rome, Italy; 4Clinic of Radiology, Imaging Institute of Southern Switzerland, Ente Ospedaliero Cantonale (EOC), Bellinzona, Switzerland; 5Epatocentro Ticino, Lugano, Switzerland; 6Department of Surgery, Ente Ospedaliero Cantonale (EOC), Lugano, Switzerland; 7Division of Gastroenterology and Hepatology, Ente Ospedaliero Cantonale (EOC) Lugano, Lugano, Switzerland
*These authors contributed equally to this work
Correspondence: Sara De Dosso, Medical Oncology Department, Oncology Institute of Southern Switzerland (IOSI), Ente Ospedaliero Cantonale (EOC), c/o Ospedale San Giovanni, Via A. Gallino 12, Bellinzona, CH-6500, Switzerland, Tel +41 091 811 9410, Email [email protected]
Introduction: Transarterial chemoembolization, TACE continues to be the primary treatment option for patients diagnosed with intermediate-stage (BCLC B) hepatocellular carcinoma, HCC. However, emerging real-world evidence suggests that it may also be applicable for selected early-stage patients (BCLC A) who are not candidates for surgical resection or thermal ablation. This study aimed to evaluate the long-term outcomes of TACE within a large single-centre cohort.
Methods: This retrospective observational cohort study included patients with HCC treated with TACE at Ente Ospedaliero Cantonale, EOC in Ticino, Switzerland between 2013 and 2023. The study was conducted and reported in accordance with the STROBE guidelines. Overall survival, OS and progression-free survival, PFS were estimated using Kaplan–Meier analysis and compared across Barcelona Clinic Liver Cancer, BCLC stages.
Results: A total of 195 patients were included, with a median follow-up of 56 months. Most patients were classified as BCLC stage A (55.4%) or B (43.6%). Median OS for the entire cohort was 56 months. PFS was significantly longer in stage A compared with stage B patients (15 vs 9 months, p=0.003). Early modification of treatment within one month was associated with inferior outcomes, whereas patients who subsequently underwent curative-intent therapies achieved markedly prolonged survival.
Conclusion: In this retrospective study, TACE demonstrated sustained tumour control and prolonged survival, exceeding the survival durations reported in previous studies (20– 42 months), particularly among early-stage HCC patients who were initially deemed unsuitable for resection or ablation. These findings emphasise the value of centralisation, multidisciplinary evaluation, tailored therapeutic approaches, and systematic periodic reassessment to optimise patient outcomes.
Plain Language Summary: Hepatocellular carcinoma, HCC is the most common type of primary liver cancer. Many patients are not eligible for surgery, transplantation, or heat-based tumour ablation. In such situations, transarterial chemoembolization, TACE is frequently used. TACE delivers chemotherapy directly into the liver arteries supplying the tumour and blocks these blood vessels to reduce tumour blood flow.
In this retrospective study, we evaluated real-world outcomes of TACE in a Swiss referral centre over a 10-year period (2013– 2023). We analysed medical records of 195 patients with HCC treated with TACE and followed them for a median of 56 months. Most patients had early-stage (BCLC A) or intermediate-stage (BCLC B) disease.
Median overall survival for the entire cohort was 56 months. Cancer control lasted longer in early-stage disease: median progression-free survival was 15 months in BCLC A compared with 9 months in BCLC B. Patients requiring an early change of treatment within the first month after TACE tended to have worse outcomes. Importantly, patients who later received more effective treatments, including curative-intent options such as transplantation, surgery, or ablation, achieved very long survival.
These findings suggest that TACE can provide durable tumour control and long-term survival, especially in carefully selected early-stage patients, and highlight the value of multidisciplinary care and regular reassessment over time.
Keywords: hepatocellular carcinoma, HCC, transarterial chemoembolization, TACE, progression-free survival, PFS, stage migration
Introduction
Hepatocellular carcinoma, HCC, is a prevalent malignancy worldwide, ranking fifth in terms of incidence and third in cancer-related mortality.1–3 The primary aetiological factors include cirrhosis and chronic liver diseases, which are largely caused by infections such as hepatitis B virus, HBV, or hepatitis C virus, HCV, along with alcoholic-associated liver disease, ALD, and metabolic dysfunction-associated steatotic liver disease, MASLD, exposure to dietary toxins, haemochromatosis, and various genetic metabolic disorders.4,5 Unlike other carcinomas, HCC has shown an upward trend in recent years.6 The Barcelona Clinic Liver Cancer, BCLC staging system, serves as the Western standard for HCC classification, taking into account tumour characteristics (size, number, vascular invasion, extrahepatic spread), liver function, and performance status.7 In the early stage (BCLC 0–A), interventions such as thermal ablation or resection are employed depending on the anatomical location and size of the tumour. For well-defined tumours with preserved portal flow in the intermediate stage (BCLC B), transarterial chemoembolization, TACE, is the standard treatment. Systemic therapies are reserved for diffuse, infiltrative growth in BCLC stage B, as well as BCLC stage C. Best supportive care is recommended for BCLC stage D.7 The allocation for liver transplantation is determined using various criteria, although limited organ availability and competition with other indications pose significant challenges.8
TACE, which has been established since the 1980s,9 exploits the predominant arterial vascularisation of HCC, in contrast to the dual arterial and portal supply to the liver parenchyma. TACE consists of two modalities: conventional TACE, cTACE and drug-eluting bead TACE, DEB-TACE. Retrospective studies, clinical trials, and meta-analyses comparing cTACE and DEB-TACE indicate similar overall survival, OS and progression-free survival, PFS, with DEB-TACE associated with higher hepatic artery and biliary injury but reduced post-procedural pain.10,11 Consequently, international guidelines do not recommend DEB-TACE over cTACE as the standard treatment.12
The role of TACE in intermediate-stage (BCLC B) HCC is well established and incorporated into the guidelines,13 with numerous studies and meta-analyses validating its efficacy and safety. However, the evidence concerning early-stage patients (BCLC A) remains sparse and inconsistent.14,15 Specifically, there is a scarcity of data regarding the application and results of TACE in patients who are not candidates for immediate surgical intervention or ablation. The present study offers a comprehensive real-world evaluation of TACE in both BCLC A and B patients, with the objective of providing clinically relevant background for patient counselling and multidisciplinary decision-making.
The primary aim of this study was to assess OS and PFS across HCC stages in a cohort treated with TACE over a 10-year period at a single institution, Ente Ospedaliero Cantonale, EOC, located in Ticino, Switzerland. The secondary objectives including detailing recurrences (local and systemic), identifying predictive factors for survival (alpha-fetoprotein, tumour size, multifocality, and doxorubicin/epirubicin dose), and determining whether routine radiological evaluations at one and three months influenced therapeutic decisions or follow-up strategies. Additionally, we sought to explore potential changes in HCC aetiology, particularly the transition from alcohol-related causes to MASLD throughout the study period.
Methods
Study Design
This investigation was a retrospective observational cohort study involving patients with HCC who underwent TACE between 2013 and 2023 at EOC, Ticino, Switzerland. Data were extracted from patient records stored in the hospital’s internal medical software system. The final follow-up for all patients occurred on 1 September, 2024. The study was designed and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology, STROBE guidelines.16
Participants
Eligible patients were those aged 18 years or older who had received at least one TACE procedure. Exclusions were made for patients who opted out of data usage for research purposes, those who had received TACE at a different centre, or individuals who had the procedure prior to the designated observation period. Each patient was reviewed during the weekly multidisciplinary team meeting at the time of diagnosis and whenever a relevant clinical or radiological change occurred. Treatment decisions were guided by the contemporary BCLC guidelines, with modifications made as necessary to accommodate particular anatomical or clinical features. The protocol received approval from the local ethical commission on human research regarding the use of retrospective data.
Variables
The study variables encompassed a range of baseline demographic, clinical, tumour-related, laboratory, treatment, and survival parameters. Demographic and risk factors included sex, date of birth, HCC risk profile, presence of cirrhosis, and the date of HCC diagnosis. Clinical stage and functional reserve were assessed using the Child–Pugh score, Model for End-Stage Liver Disease, MELD score, Eastern Cooperative Oncology Group, ECOG performance status, BCLC stage, and albumin-bilirubin, ALBI score. Additional clinical factors considered included comorbidities, American Society of Anesthesiologists, ASA classification, and requirement for renal replacement therapy. Tumour-specific characteristics encompassed maximum lesion diameter, number and intrahepatic distribution of nodules, vascular invasion, extrahepatic dissemination, tumoral vein thrombosis, portal hypertension, and hepatic encephalopathy. Laboratory variables comprised serum alpha-fetoprotein, AFP, aspartate aminotransferase, AST, alanine aminotransferase, ALT, sodium, albumin, bilirubin, creatinine, and international normalized ratio, INR. Treatment-related variables included the type, intention, and technical details of TACE, the presence and severity of adverse events, treatment completion or failure (defined according to JSH-LCSGJ criteria17), radiological lipiodol accumulation, and any subsequent therapeutic interventions. Tumour response assessment was performed using modified Response Evaluation Criteria in Solid Tumors, mRECIST. Accordingly, imaging response on contrast-enhanced CT and/or MRI was evaluated based on the viable tumour component, defined by the presence of arterial phase enhancement. Complete response, CR was for example defined as the disappearance of any intratumoural arterial enhancement in all target lesions, irrespective of residual mass.18 The hospital’s senior radiologists were responsible for the radiological assessments. Outcome variables included OS, PFS, and the cause of death.
Data Sources/Measurement
All baseline demographic and clinical data were sourced from institutional patient records and electronic health databases. Clinical scores (Child–Pugh, MELD, ECOG, BCLC, ALBI, and ASA) were calculated at the time of HCC diagnosis and prior to the initiation of TACE, adhering to standard definitions and criteria. Tumour burden and vascular involvement were assessed through baseline cross-sectional imaging (computed tomography, CT or magnetic resonance imaging, MRI) and confirmed by a multidisciplinary review. Treatment decisions were made within a multidisciplinary tumour board in accordance with BCLC guidelines. Due to the retrospective design, detailed information on the decision-making process was limited to tumour board documentation. Laboratory parameters were measured using standardised methods in the institutional clinical chemistry laboratory. Procedural information regarding TACE – including technical modality, drug dosing, number of sessions, and hospitalisation – were extracted from procedural reports archived in the radiology information system. Adverse events were retrospectively graded according to the Common Terminology Criteria for Adverse Events, CTCAE. Tumour response was evaluated according to mRECIST criteria on CT or MRI at one, three, and six months, with lipiodol accumulation specifically assessed on non-contrast CT after one month. Subsequent therapies were documented from institutional treatment records and verified through cross-referencing pharmacy and radiology registries. Survival data (OS, PFS, cause of death) were obtained from follow-up documentation.
Statistical Analysis
Descriptive statistics are expressed as mean ± standard deviation, SD and median with interquartile range, IQR, given the non-normal distribution of several continuous variables. The Shapiro–Wilk test was utilized to assess normality. Categorical variables are reported as absolute frequencies and percentages. No imputation was performed; analyses were conducted on available cases only, and the number of missing values, if present, is reported in the legends of the tables.
OS was defined as the interval from diagnosis to death from any cause, while PFS was defined as the interval from the first TACE to first documented progression or death, whichever occurred first. Survival functions were estimated using the Kaplan–Meier method. Differences between strata – specifically baseline BCLC stage and early treatment modification within one month – were compared using the Log rank test. Subgroup analyses examined the prognostic effect of baseline BCLC stage (A vs B) on OS and PFS. Exploratory analyses evaluated whether an early change in treatment following the first TACE session influenced long-term outcomes. To quantify effect size, hazard ratios, HR and 95% confidence intervals, CI were derived from unadjusted Cox proportional hazards regression models, provided the proportional hazards assumption was satisfied (verified using Schoenfeld residuals). In cases where this assumption was not met, alternative survival models based on a Weibull distribution were applied. Tumour response was assessed according to mRECIST criteria at one, three, and six months, with the best response during follow-up recorded. The association between baseline BCLC stage and radiographic response was tested using Fisher’s exact test. All tests were two-sided, with statistical significance set at a p-value < 0.05. Analyses were performed using STATA19 software (StataCorp., College Station, TX, USA).
Results
Participants
From an initial sample of 214 patients, 195 individuals with HCC who underwent TACE were included in the analysis. Nineteen patients were excluded for various reasons: TACE was performed before the study period or at another centre (n = 5), absence of radiological data (n = 5), TACE deemed unfeasible (n = 3), simple embolisation (TAE) performed instead of TACE (n = 1), TACE performed for cholangiocarcinoma or metastatic disease (n = 3), and refusal to participate in the study (n = 2). The exclusion flow diagram illustrating the patient selection pathway is reported in Figure 1.
 |
Figure 1 Exclusion flow diagram showing the number of patients assessed for eligibility, excluded, and finally included in the study. |
Descriptive Data
The median age of the cohort was 71 years (IQR: 66–76), with a predominance of male patients (81%). The mean body mass index, BMI was 26.8 ± 5.1 kg/m2. A substantial number of patients (93.8%) had cirrhosis, primarily due to alcohol-related liver disease (56.4%), followed by HCV infection (26.7%), MASLD (27.7%), and HBV infection (12.8%), with some patients exhibiting multiples aetiologies (34.4%). The distribution of aetiologies showed no significant change throughout the study period.
Cardiovascular comorbidities were frequent (76.9%), and 44.1% of the cohort had diabetes mellitus, indicating a population at high metabolic and vascular risk (Table 1). The mean number of HCC nodules was 2.2 ± 1.8, with a median largest diameter of 28 mm (IQR: 20–44.5). Multifocal disease was present in 59.5% of patients. The majority were classified as BCLC stage A (55.4%) or B (43.6%); two patients (1%) were stage C and were excluded from further analyses. Within stage A, most had an ASA score of 3 (70.8%). Segment VIII was the most frequently involved liver segment (37%). Twenty-five patients (23.1%) with stage A had prior local therapy, with one-fifth having undergone surgical resection. Portal vein thrombosis was observed in 3.1% of cases and ascites (subclinical) were present in 17.4% of patients. Three patients had a previous episode of hepatic encephalopathy (1.5%). Detailed information regarding tumour burden and staging is provided in Table 2.
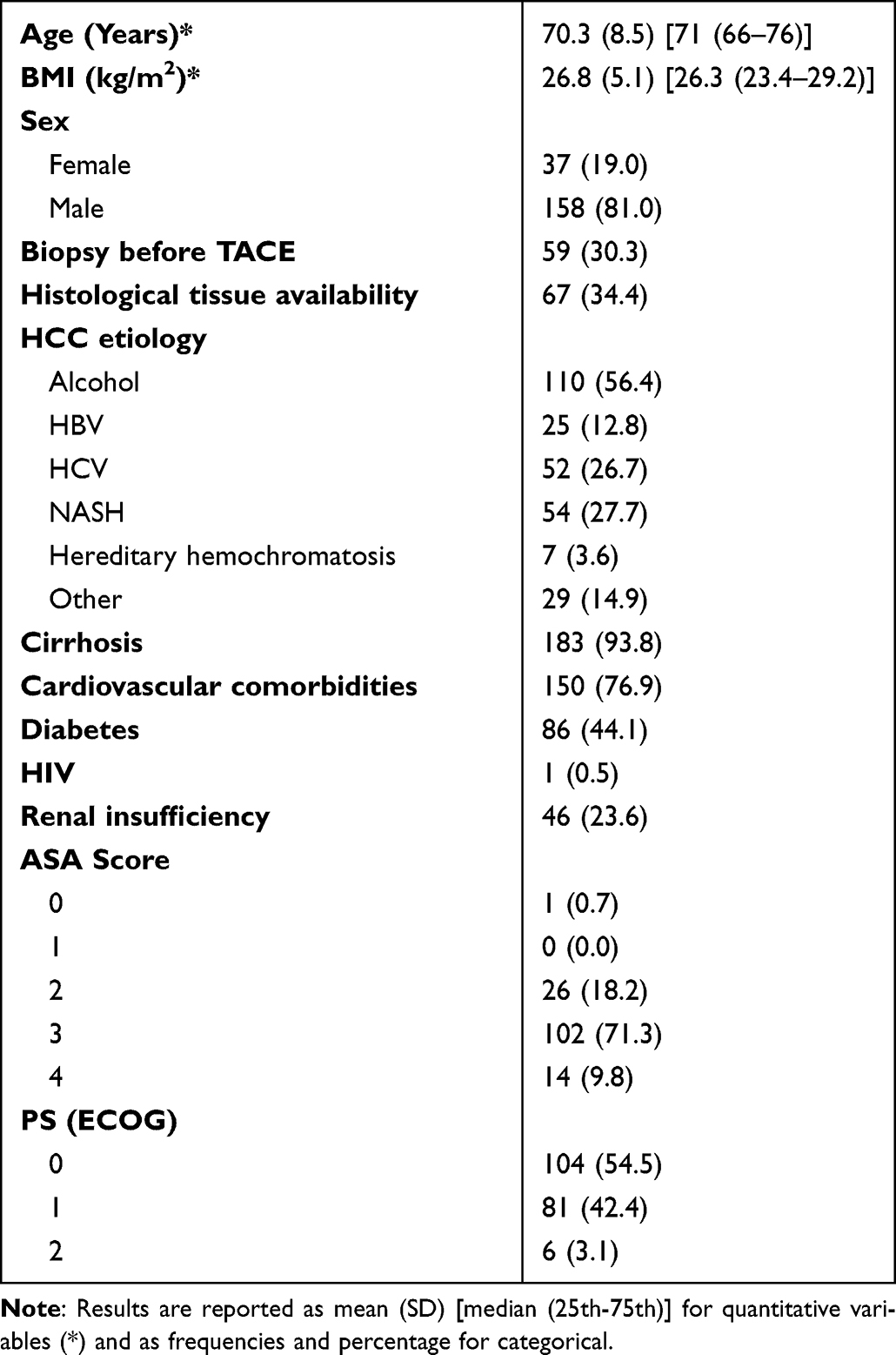 |
Table 1 Demographic (n = 195) |
 |
Table 2 HCC Characteristics |
Baseline AFP levels exhibited considerable variability (565.4 ± 4710 ng/mL; median 8.4 ng/mL, IQR: 4–49.7), reflecting tumour heterogeneity. The median MELD score was recorded at 8.5 (IQR: 8.2–8.8). Most patients were classified as Child–Pugh class A (85.1%), and 52.6% as ALBI grade 2. Further details are provided in Table 3.
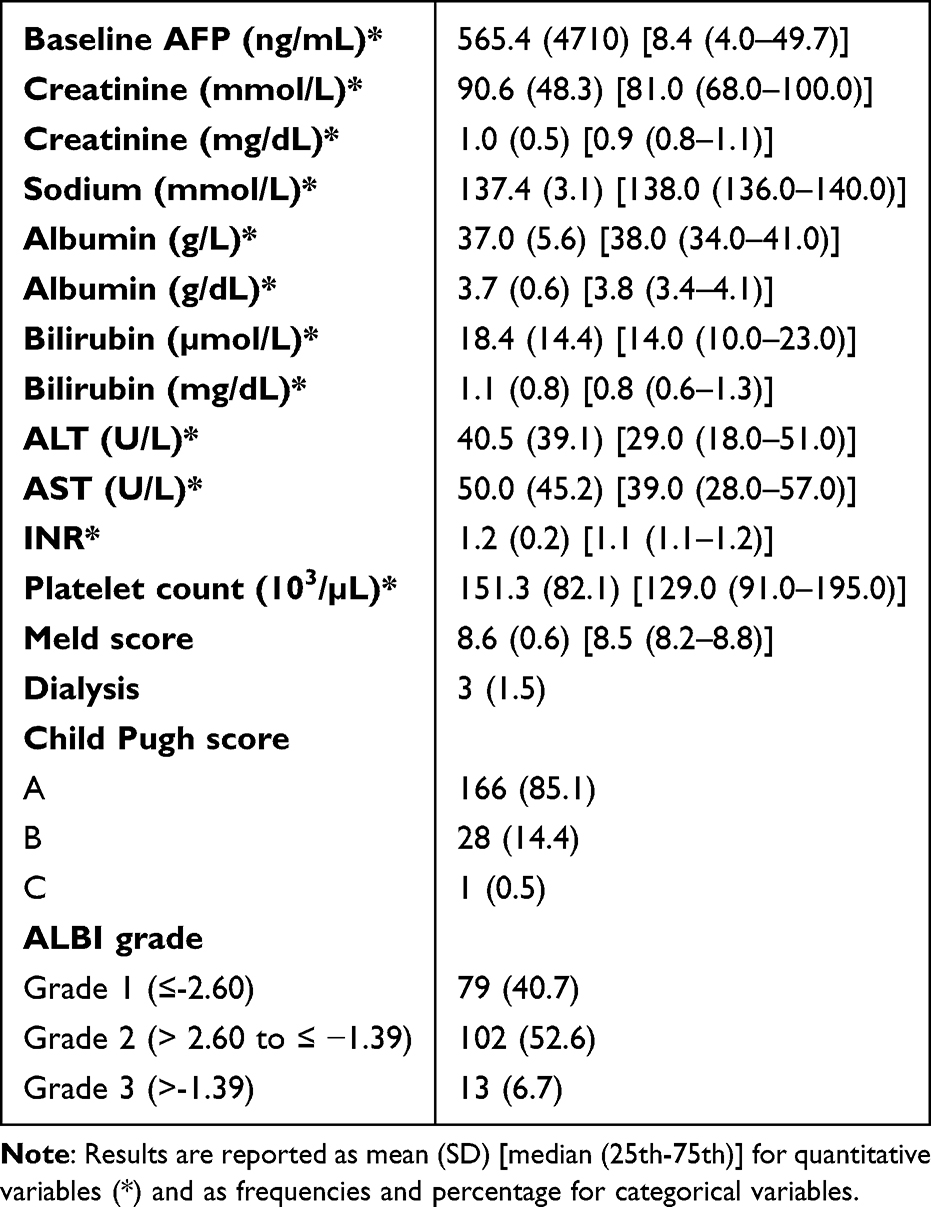 |
Table 3 Lab Values and Liver Function Parameters |
Thirty-five patients (17.9%) had previously undergone local therapies prior to TACE. The majority (80.0%) had received a single treatment; 8.6% had two or three, and 2.9% had four. Among these patients, the most recent previous procedure was thermal ablation (n = 18), followed by Selective Internal Radiation Therapy, SIRT (n = 7), arterial embolisation (n = 4), surgical resection (n = 5), and portal vein embolisation (n = 1). None had received systemic therapy prior to TACE. The results are presented in Table 4.
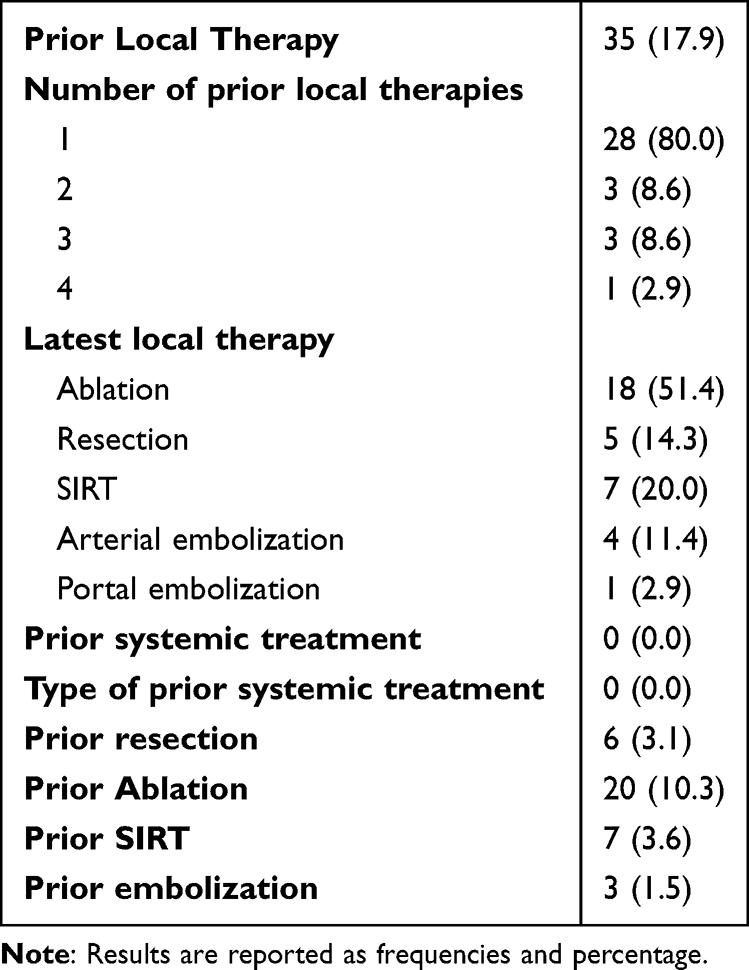 |
Table 4 Prior Treatment |
TACE was administered as the first-line therapy in 72.8% of cases (Table 5).
 |
Table 5 TACE Procedure |
Epirubicin was the predominant chemotherapeutic agent (80.2%) used, with a mean dose of 50.9 ± 16.8 mg/mL. Superselective delivery was achieved in 71.9%, with vascular mapping in 78.8%. The median hospital stay was three days (IQR: 3–5). Adverse events occurred in 15.4% of patients, primarily classified as grade 1 (71.4%) or grade 2 (25%).
Follow-Up and Tumour Response
During follow-up, serum AFP levels decreased significantly (Table 6). The median AFP fell to 5.7 ng/mL at one month (IQR: 3.2–24.4), remaining stable at 5.6 ng/mL at three months and 5.5 ng/mL at six months. The large SD at one month (2844.7 ng/mL) was attributed to outliers with advanced disease.
 |
Table 6 Follow-Up |
Radiological assessment at one month was available for 96.8% of patients. Lipiodol accumulation was complete in 51.8%, partial in 35.7%, and absent in 12.5%. Throughout the first month, most patients (69.8%) had no complications. The most frequent adverse event was ascites (14.0%), followed by portal vein thrombosis (6.7%). Severe complications, such as abscess formation (2.2%) and pancreatitis (0.6%), were rare. After one month, no further treatment was considered necessary in 81.9% of patients, while 18.1% (n = 34) required additional TACE or other treatments. At the three-month mark, MRI was used more often than CT (63.6% vs 36.4%).
At the final follow-up, TACE failure (defined as the absence of a therapeutic effect within the first one to two months post-procedure and is characterised by intrahepatic, vascular, or extrahepatic invasion of HCC accordingly with the JSH-LCSGJ criteria17) was observed in 50% of cases, while relapse or progression occurred in 77.4%. Among those who had experienced progression, local recurrence was the most common (62.3%; 48.2% of the whole cohort), followed by the emergence of new intrahepatic nodules (31.1%); however, extrahepatic spread was rare (6.6%).
One month subsequent to TACE, the overall complete response, CR rate was recorded at 65.8%, with a higher rate in stage A (84.2%) than in stage B (43.9%, p < 0.001). This difference persisted at three months (CR: 76.1% vs 41.3%, p < 0.001) and six months (63.0% vs 40.3%, p = 0.007). The best response during the follow-up period was a CR in 73% of cases overall, with a marked advantage for stage A (88.2%) vs stage B (54.3%, p < 0.001). An early modification of the treatment regimen at one month was more common in BCLC stage B (27.4%) than in stage A (9.8%, p = 0.002). The complete results are presented in Table 7. The distribution of best radiological responses by BCLC stage is illustrated in Figure 2.
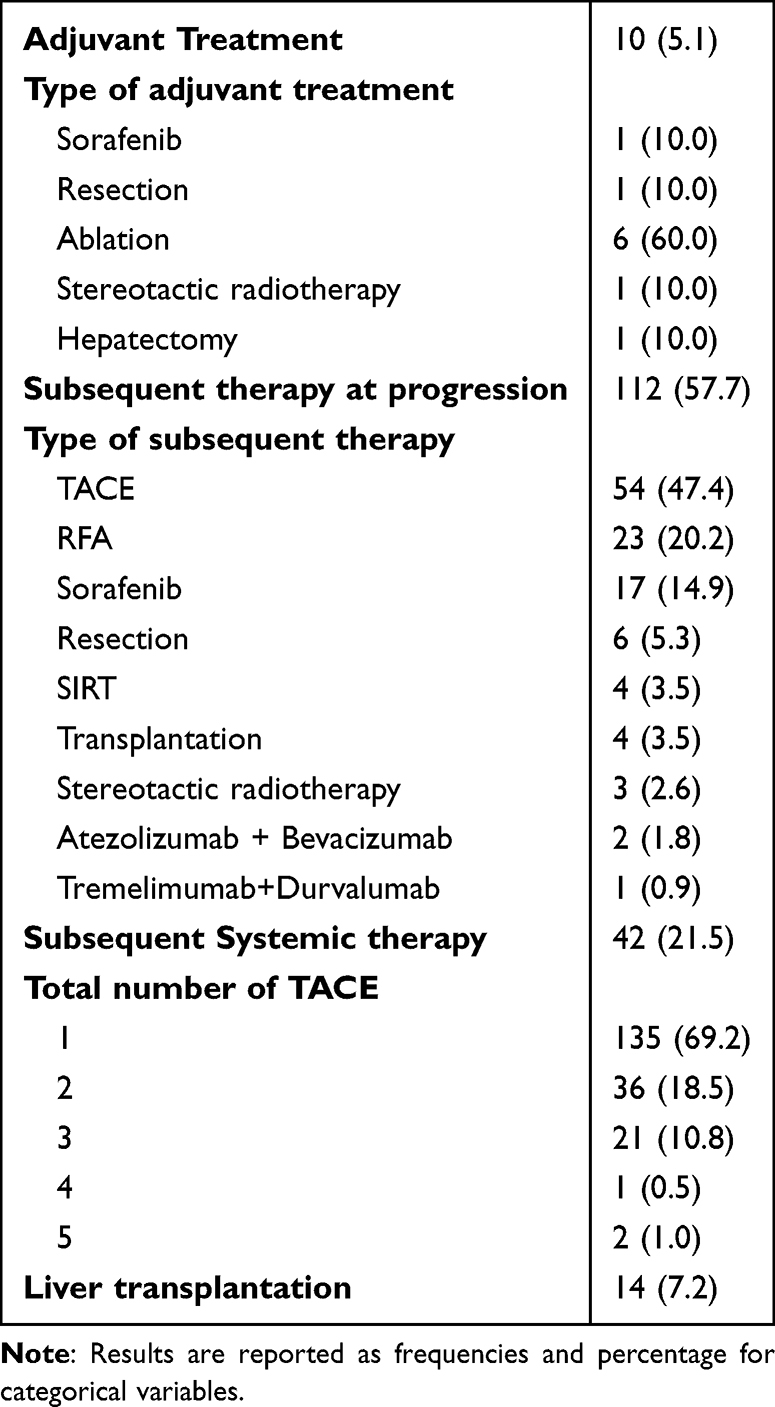 |
Table 7 Adjuvant/Subsequent Therapy |
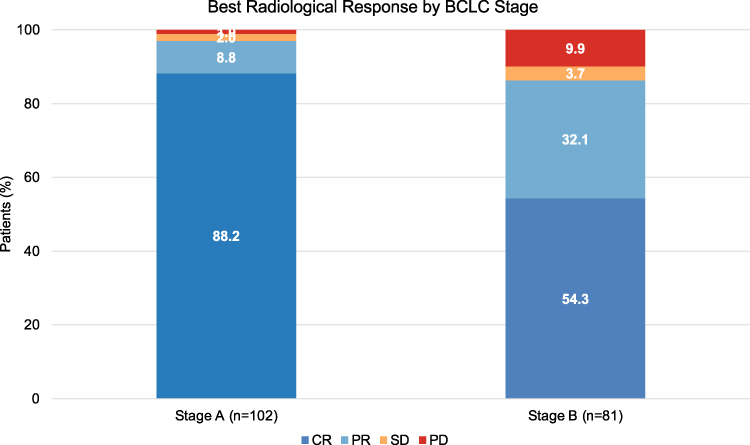 |
Figure 2 Distribution of best radiological response by BCLC stage. Stacked bar chart showing the proportion of patients achieving complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD) as best overall response during follow-up, stratified by baseline BCLC stage (Stage A, n=102; Stage B, n=81). Two BCLC stage C patients are excluded from the analysis. |
Complementary treatments following the first TACE procedure were performed in 10 patients (5.1%). Thermal ablation was used in six, two underwent resections, one received sorafenib, and one had stereotactic radiotherapy. A documented second-line treatment was performed in 57.7% of the patients who experienced progression. The most common intervention was repeated TACE (47.4%). Other locoregional therapies included Radiofrequency ablation, RFA (20.2%), SIRT (3.5%), and stereotactic radiotherapy (2.6%). Sorafenib was the most commonly used systemic agent (14.9%), while immune checkpoint inhibitors were only administered during the later stages of the cohort: atezolizumab plus bevacizumab in 1.8% and tremelimumab plus durvalumab in 0.9%. Overall, systemic therapy was provided to 42 patients (21.5%).
The total number of TACE sessions per patient varied, with the majority (69.2%) undergoing a single session, 18.5% (n = 36) receiving two, and 10.8% (n = 21) having three. Only three patients (1.5%) required four or more sessions. In total, 14 patients (7.2%) underwent liver transplantation. The complete results are illustrated in Table 8.
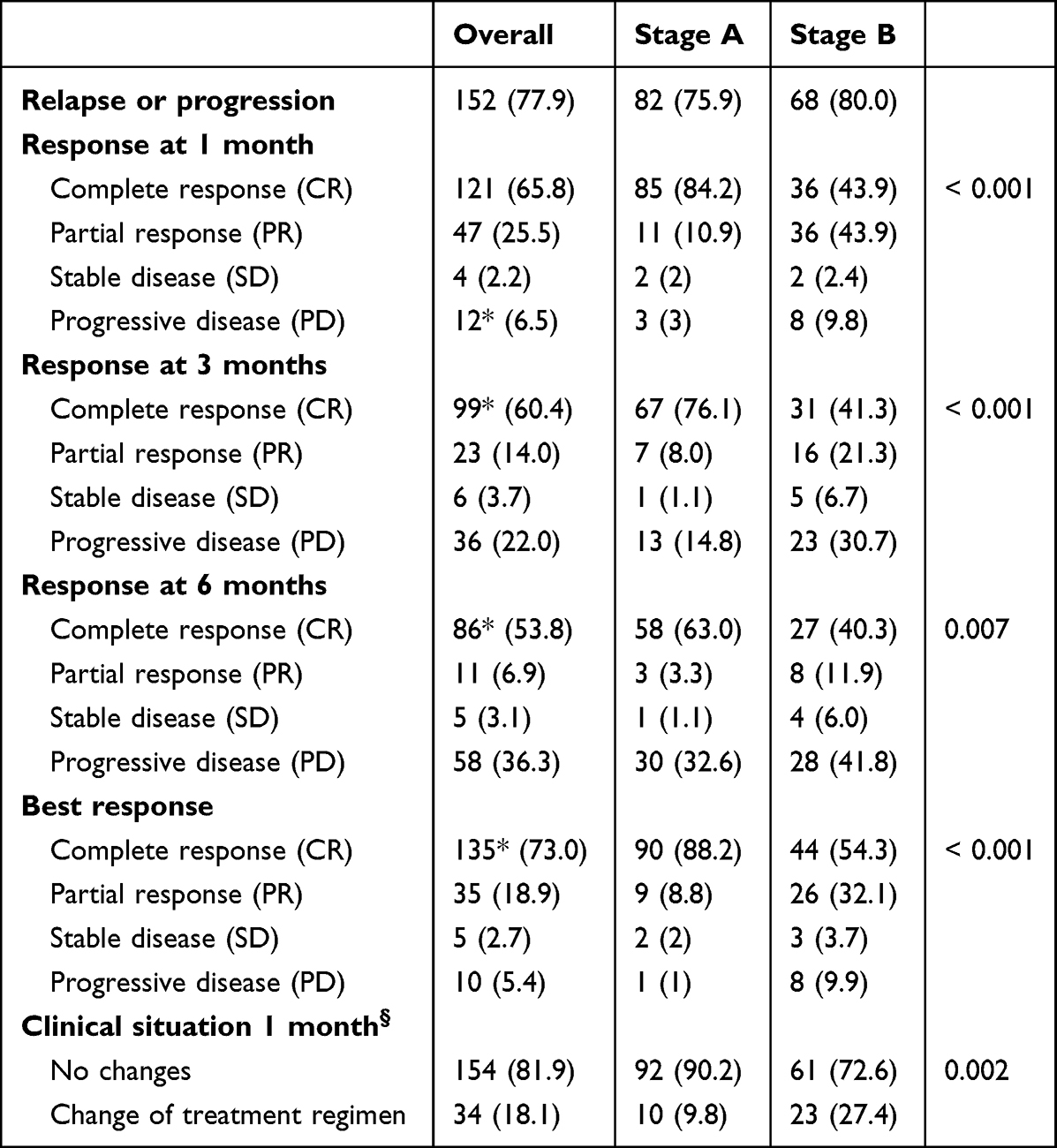 |
Table 8 Response by Baseline BCLC |
Overall Survival and Progression-Free Survival
The median follow-up was 56 months (IQR: 26–85.8). The median OS for the cohort was 56 months (IQR: 26.3–86), while the median PFS was 11 months (IQR: 5.2–24.9) (Figure 3A–C). When stratified by baseline BCLC stage, patients in stage A exhibited significantly longer PFS (15 months, 95% CI: 11–25) in comparison to those in stage B (9 months, 95% CI: 7–11) (log-rank p = 0.003); consequently, patients in Stage B faced a significantly higher risk of progression (HR = 1.62, 95% CI: 1.17–2.25, p = 0.004) (Figure 3D). The difference in OS remained non significative (Figure 3B).
 |
Figure 3 Overall Survival (OS) and Progression-Free Survival (PFS). Kaplan–Meier curves show (A) OS in the overall cohort, (B) OS stratified by BCLC stage, (C) PFS in the overall cohort, and (D) PFS stratified by BCLC stage. PFS estimates were 15 months [95% CI: 11–25] for stage A and 9 months [95% CI: 7–11] for stage B. The bottom row shows OS (E) and PFS (F) according to the variable “Clinical Change of Treatment After 1 Month”. Shaded areas indicate 95% confidence intervals. Notes: Kaplan–Meier survival plots arranged in six panels. (A) shows overall survival for the entire cohort. (B) displays overall survival curves separated by BCLC stages. (C) shows progression-free survival for the overall cohort. (D) presents progression-free survival curves stratified by BCLC stage, with confidence-interval shading. (E and F) show overall survival and progression-free survival, respectively, grouped by the variable “Clinical Change of Treatment After 1 Month”. Each curve includes shaded 95% confidence intervals. |
An analysis of patients who required treatment modification (n = 34) revealed that those who underwent an early change (within one month) experienced substantially poorer outcomes compared to those who continued their initial regimen. These patients demonstrated poorer PFS (HR = 3.14, 95% CI: 2.07–4.78, p < 0.001), while the difference in OS did not reach statistical significance, although there was a trend towards reduced survival (HR = 1.57, 95% CI: 0.92–2.71, p = 0.096) (Figure 3E and F).
Patients who received a more effective treatment hierarchy after TACE had better survival: median OS of 113 months (95% CI: 73–152) for transplanted patients (n = 4), 79 months (95% CI: 35–114) for resected patients (n = 5), and 62 months (95% CI: 47–74) for patients treated with radiofrequency thermal ablation (n = 18).
Univariate analysis did not identify significant associations between established prognostic factors (tumour size, multifocality, doxorubicin/epirubicin dose, or AFP level) and OS or PFS. At the final follow-up, 43.1% of patients had died, primarily due to cancer-related causes (34.5%) or liver failure (23.8%) (Table 9).
 |
Table 9 OS/PFS |
Discussion
The therapeutic landscape for HCC has expanded due to the introduction of effective systemic therapies and multimodal strategies that prolong patient survival.3,4 TACE remains the standard treatment for patients with intermediate-stage HCC, with historically reported median OS ranging from approximately 20 to 42 months in cohort studies and randomised trials.15,19 In comparison, our study reports a median OS of 56 months, surpassing both historical controlled and contemporary real-world estimates. With a median follow-up of 56 months and nearly 200 patients treated at a referral centre, these results demonstrate the remarkable effectiveness of TACE. The favourable outcomes can be attributed to careful patient selection (mainly stage A), the specialised treatment setting, and the consistency of the operators and techniques employed. The absence of treatment-related mortality and the low rates of complications further reinforce the notion that TACE, when performed or supervised by experts, is safe in the short term and effective in the long term. Furthermore, even though approximately one in two patients may be refractory or experience progression after TACE, the possibility of offering subsequent treatment in most cases could be another factor contributing to improved outcomes.
The high proportion of stage A patients in our study can be accounted for by the relatively high prevalence of patients with a single nodule initially deemed unfit for resection (due to comorbidities), those unsuitable for RFA because of the superficial position of the nodules, or patients with two or three nodules who were not candidates for transplantation (generally due to age or comorbidities). The elevated number of these patients may represent a distinctive feature of our population; however, we propose that in other centres, they may be more prevalent than their seemingly minor representation on the BCLC algorithm. Regardless, these patients have shown favourable responses to TACE.
As expected, PFS was remarkably longer in stage A compared to stage B, which reflects the more aggressive biology of intermediate-stage disease.20 Conversely, no significant difference was observed in OS between the two groups. It is crucial to highlight that the median OS for BCLC B patients could not be determined, as fewer than 50% of the patients had succumbed to death at the time of analysis. Rather than representing a limitation of the dataset, this finding suggests that our cohort of BCLC B patients performed substantially better than anticipated based on historical benchmarks.
This favourable survival outcome likely reflects the benefits of structured multidisciplinary care and seamless collaboration across specialties, which facilitated consistent and individualised treatment sequencing. Moreover, integration within a robust referral network ensured timely access to advanced locoregional and systemic therapies, minimising delays and maximising the therapeutic window for each patient.21,22 Collectively, these elements may have contributed to attenuating the prognostic disadvantage traditionally associated with intermediate-stage HCC.
This comparable survival rates also imply that numerous early-stage patients eventually progressed to advanced disease. The early initiation of TACE in selected BCLC A patients (who are unsuitable for surgery or thermal ablation) may help delay this transition. This indicates that staging should be viewed as a therapeutic opportunity to optimise timing and maximise long-term benefits, rather than merely interpreting it as a natural course of tumour biology.
An analysis of the proportion of BCLC A and B patients receiving TACE over time revealed no significant year-dependent trends, with the exception of 2021, when a higher proportion of stage A patients underwent TACE, likely due to the impact of COVID-19 restrictions and reduced surgical capacity, although this remains a speculative assertion.23 A descriptive analysis of subgroups provided further insight into the rationale for choosing TACE in early-stage disease. A significant proportion of stage A patients exhibited an ASA score of 3, which signifies a heightened surgical risk, thereby favouring a non-surgical approach.22 In addition, many tumours were located in segment VIII, a site that poses technical challenges for both resection and ablation procedures.24 Approximately 20% of stage A patients had also received prior local therapy, indicating possible recurrence or progression, thus supporting TACE as a reasonable option for this subgroup.19,21
In light of the high response rates observed in stage A patients, another clinically relevant aspect concerns radiological follow-up and the potential for imaging de-escalation. Within our cohort, almost all patients underwent a CT scan at the one-month mark, in accordance with EASL and EORTC guidelines that recommend Modified Response Evaluation Criteria in Solid Tumors (mRECIST)-based assessment at this time point.25
Notably, 84.2% of stage A patients achieved CR at one month, with only 9.8% requiring a change in treatment. These findings raise the question of whether routine one-month CT, as suggested by guidelines, is necessary for all patients, or whether imaging could safely be deferred to three months in selected low-risk cases, balancing the benefits of early detection against the risks and costs of repeated imaging. While a reduction in imaging frequency could lead to decreased radiation exposure and lower healthcare costs, it also carries the risk of missing early identification of the small subset of patients who fail to benefit from treatment and who, in our cohort, exhibited significantly worse outcomes. Consequently, future studies should examine the safety and cost-effectiveness of modified follow-up protocols, employing a selective imaging strategy that targets patients with specific risk factors (eg, elevated AFP, multifocal disease). As an example, the 2026 BCLC update marks a shift towards a more adaptive precision medicine by integrating the CUSE (Complexity, Uncertainty, Subjectivity, Emotion) framework and the BCLCCUSE. AI digital tool, designed to standardize multidisciplinary and personalized decision-making in contexts of clinical uncertainty.26
All these factors, together with patient preference in the shared decision-making process, may explain the use of TACE in early-stage HCC. In this specific subgroup, our analysis demonstrated favourable response rates and prolonged PFS, suggesting a sustained probability of tumour control and supporting TACE as an effective therapeutic option for patients who are not eligible for upfront curative treatments. These findings emphasise the need for the refined stratification of early-stage patients who are unsuitable for resection or ablation. This subgroup, often characterised by anatomical complexity, clinical frailty, or a history of prior treatments, requires tailored management strategies that transcend standard curative algorithms.
In line with these observations, another noteworthy finding from our analysis was the markedly prolonged OS in patients who subsequently received a hierarchically more effective treatment after TACE. This highlights the importance of adopting a dynamic, stage-adapted therapeutic strategy in HCC, where TACE can serve not only as a stand-alone treatment but also as a bridging or enabling intervention that facilitates access to potentially curative options. These results reinforce the value of continuous reassessment within multidisciplinary tumour boards to ensure timely transition of eligible patients to higher-intent therapies whenever feasible. However, given the limited number of patients in this subgroup, these findings should be interpreted with caution and considered hypothesis-generating, warranting validation in future dedicated studies.
Finally, with nearly half of the patients experiencing TACE failure despite high early response rates, our data highlights the need for a more dynamic and clinically meaningful definition of failure. This finding has direct clinical implications, as early identification of patients unlikely to benefit from repeated TACE may facilitate timely treatment modification and transition to systemic therapy, in line with the concept of TACE refractoriness and a stage-adapted, multimodal treatment strategy.18 In such cases, timely transition to systemic therapy is essential to preserve liver function and optimise outcomes.27 Moreover, increasing evidence supports the integration of TACE with systemic therapies, particularly with immune checkpoint inhibitors and antiangiogenic agents.28 Although the use of modern systemic therapies was limited in our cohort due to the study period, our findings support a dynamic, stage-adapted treatment strategy with early consideration of treatment escalation in non-responders. Therefore, incorporating early radiological and clinical patterns may better guide post-TACE strategies.
This study presents some limitations. First, the single-centre retrospective design carries an inherent risk of selection bias and limits the generalisability of our results. Second, although a comprehensive dataset was drawn from the electronic patient records, it is important to note that the residual confounding due to unmeasured clinical factors cannot be excluded. Additionally, missing values were neither calculated nor corrected, and analyses were performed using only the available cases, which may have introduced bias if the data were not missing at random. Third, tumour response was assessed at predefined imaging time points, and heterogeneity in radiological evaluation might have influenced response classification. Fourth, although the overall sample size is adequate for the primary survival analyses, statistical power for subgroup analyses is limited. Findings from these subgroups should therefore be interpreted as exploratory and hypothesis-generating, and warrant confirmation in larger prospective cohorts. Fifth, a potential immortal time bias cannot be excluded in the subgroup of patients who received curative-intent therapies following TACE. By definition, these patients must have survived long enough to become eligible for and undergo subsequent treatment, which may have contributed to the markedly prolonged OS observed in this subgroup. Accordingly, the survival estimates reported for this group should be interpreted with caution and regarded as descriptive rather than attributable to a treatment sequencing effect per se. Sixth, formal multivariable survival analyses were not included among the reported results. Although exploratory models were computed for both endpoints, their inclusion was deemed methodologically inappropriate. For OS, the multivariable Cox model was structurally underpowered: the event-to-variable ratio is at the minimum threshold conventionally considered acceptable, and the marked imbalance in key categorical predictors further limited the reliability of stratum-specific effect estimates, as confirmed by a globally non-significant model (LR χ2 = 8.66, p = 0.372). For PFS, a multivariable Cox regression model was computed, but also in this the overall model did not reach statistical significance (LR χ2 = 12.10, p = 0.097), and no individual covariate was significantly associated with PFS after adjustment. Future prospective studies with larger and more heterogeneous patient populations, pre-specified multivariable models, and systematic collection of potential confounders would be needed to formally assess independent prognostic factors for OS and PFS in patients treated with TACE across BCLC stages. Finally, as in most real-world studies, treatment decisions, including the intent and selectivity of TACE, were made at the discretion of the multidisciplinary team, which could lead to variability that is difficult to fully account for.
Conclusion
In conclusion, our study suggests that the role of TACE may extend beyond its conventional position in the HCC therapeutic algorithm, encompassing concepts such as therapeutic stage migration and selective imaging de-escalation. Moreover, the markedly prolonged OS observed in patients who subsequently underwent curative treatment after TACE underscores its potential not only as a palliative therapy but also as a bridging or enabling strategy within a dynamic, stage-adapted continuum of care. These findings should be interpreted in the context of the retrospective design and the characteristics of the study population. Collectively, these findings highlight the enduring value of TACE in optimising outcomes for carefully selected patients and support the need for further investigation in prospective, real-world contexts.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Statement of Ethics
Every patient either signed a general informed consent for data collection or was deceased at the time of data analysis. Written informed consent was obtained from the patient for the publication of their medical case details and any accompanying images prior to their death. If informed consent had not been obtained before their death, an exemption was obtained from the Swiss Ethics Committee in accordance with Article 34 of the Human Research Act. This study was performed in accordance with the Declaration of Helsinki. As this retrospective study did not involve organ procurement or transplantation, no organs were donated or used for research, and requirements related to the Declaration of Istanbul are not applicable. This human study was approved by Comitato Etico Cantonale, Bellinzona (CH), approval number 024-01101 CE 4616.
Acknowledgment
The authors acknowledge Mrs. Cinzia Marini for her valuable contribution in initiating this work through systematic case recording and constructive encouragement.
Author Contributions
Guido Pesola, Gianluigi Marini, Maria Luisa Garo, Sara De Dosso contributed to study concept and design. Gayane von Schoen-Angerer, Guido Pesola contributed to data acquisition.
Maria Luisa Garo conducted the statistical analysis. Gayane von Schoen-Angerer, Guido Pesola, Maria Luisa Garo, Sara De Dosso contributed to data analysis and interpretation, and drafting of the manuscript. Andreas Cerny, Lorenzo Magenta, Stefano Cappio, Pietro Majno-Hurst, Lorenzo Bernardi, Marco Cefali, Alessandra Cristaudi, Benedetta Terziroli Beretta-Piccoli, Elena Trevisi critically reviewed the article. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any sponsor or funder.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wong MCS, Xu RH, Singh AK, et al. International incidence and mortality trends of liver cancer: a global profile. Sci Rep. 2017;7(1):45846. doi:10.1038/srep45846
2. Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, Roberts LR. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol. 2019;16(10):589–17. doi:10.1038/s41575-019-0186-y
3. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
4. Kulik L, El-Serag HB. Epidemiology and management of hepatocellular carcinoma. Gastroenterology. 2019;156(2):477–91.e1. doi:10.1053/j.gastro.2018.08.065
5. Fitzmaurice C, Akinyemiju TF, Lami FH, et al. The burden of primary liver cancer and underlying aetiologies from 1990 to 2015: results from the global burden of disease study 2015. JAMA Oncol. 2017;3(12):1683–1691. doi:10.1001/jamaoncol.2017.3055
6. Ryerson AB, Eheman CR, Altekruse SF, et al. Annual report to the nation on the status of cancer, 1975–2012, featuring the increasing incidence of liver cancer. Cancer. 2016;122(9):1312–1337. doi:10.1002/cncr.29936
7. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
8. Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for hepatocellular carcinoma. Ann Surg Oncol. 2008;15(4):1001–1007. doi:10.1245/s10434-007-9559-5
9. Suzuki K, Kaneko T, Nakamura S, et al. Arterial chemo-embolization for humoral hypercalcemia of hepatocellular carcinoma. Jpn J Clin Oncol. 1989;19(2):146–151.
10. Golfieri R, Giampalma E, Renzulli M, et al. Randomised controlled trial of doxorubicin-eluting beads vs conventional chemoembolisation for hepatocellular carcinoma. Br J Cancer. 2014;111(2):255–264. doi:10.1038/bjc.2014.199
11. Zou JH, Zhang L, Ren ZG, Ye SL. Efficacy and safety of cTACE versus DEB-TACE in patients with hepatocellular carcinoma: a meta-analysis. J Dig Dis. 2016;17(8):510–517. doi:10.1111/1751-2980.12380
12. Sangro B, Sarobe P, Hervás-Stubbs S, Melero I. EASL clinical practice guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82(2):315–374. doi:10.1016/j.jhep.2024.08.028
13. Vogel A, Chan SL, Dawson LA, et al. Hepatocellular carcinoma: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2025;36(5):491–506. doi:10.1016/j.annonc.2025.02.006
14. Titano J, Noor A, Kim E. Transarterial chemoembolization and radioembolization across Barcelona clinic liver cancer stages. Semin Intervent Radiol. 2017;34(2):109–115. doi:10.1055/s-0037-1602709
15. Arizumi T, Ueshima K, Minami T, et al. Overall survival of patients with hepatocellular carcinoma correlates with the newly defined time to progression after transarterial chemoembolization. Liver Cancer. 2017;6(3):227–235. doi:10.1159/000475777
16. von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
17. Kudo M, Kawamura Y, Hasegawa K, et al. Management of hepatocellular carcinoma in Japan: JSH 2014 update &2017 update. Liver Cancer. 2021;10(3):181–223. doi:10.1159/000514174
18. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
19. Haak F, Karli T, Takes M, Zech CJ, Kollmar O, Soysal SD. A retrospective cohort analysis of transarterial chemoembolization for hepatocellular cancer at a tertiary center in Switzerland. J Clin Med. 2024;13(11):3279. doi:10.3390/jcm13113279
20. Ogunwobi OO, Harricharran T, Huaman J, et al. Mechanisms of hepatocellular carcinoma progression. World J Gastroenterol. 2019;25(19):2279–2293. doi:10.3748/wjg.v25.i19.2279
21. Bernardi L, Balzano E, Roesel R, et al. Recurrence and survival after robotic vs laparoscopic liver resection in very-early to early-stage (BCLC 0-A) hepatocellular carcinoma. Surg Endosc. 2025;39(3):2116–2128. doi:10.1007/s00464-025-11553-3
22. Balzano E, Bernardi L, Roesel R, et al. Robotic versus laparoscopic liver resections: propensity-matched comparison of two-center experience. Surg Endosc. 2023;37(10):8123–8132. doi:10.1007/s00464-023-10358-6
23. Hoffmann K, Müller-Bütow V, Hinz U, et al. Risk assessment for liver resection. Surgery. 2018;164(5):998–1005. doi:10.1016/j.surg.2018.06.024
24. Ishizawa T, Gumbs AA, Kokudo N, Gayet B. Laparoscopic segmentectomy of the liver: from segment I to VIII. Ann Surg. 2012;256(6):959–964. doi:10.1097/SLA.0b013e31825ffed3
25. European Association For The Study Of The Liver. European organisation for research and treatment of cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56(4):908–943. doi:10.1016/j.jhep.2011.12.00
26. Reig M, Sanduzzi-Zamparelli M, Forner A, et al. BCLC strategy for prognosis prediction and treatment recommendations: the 2026 update. J Hepatol. 2026;84:631–654. doi:10.1016/j.jhep.2025.10.020
27. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922–1965. doi:10.1097/HEP.0000000000000466
28. Kudo M, Ren Z, Guo Y, et al. Transarterial chemoembolisation combined with lenvatinib plus pembrolizumab versus dual placebo for unresectable, non-metastatic hepatocellular carcinoma (LEAP-012): a multicentre, randomised, double-blind, Phase 3 study. Lancet. 2025;405(10474):203–215. doi:10.1016/S0140-6736(24)02575-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.