")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Trans-Regional Medical Support in Public Health Emergencies: A Case Study of Wuhan in the Early COVID-19 Pandemic in China
Authors Li T
Received 28 October 2021
Accepted for publication 28 March 2022
Published 15 April 2022 Volume 2022:15 Pages 677—683
DOI https://doi.org/10.2147/RMHP.S346556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kent Rondeau
Tao Li
School of Law, Hebei University of Economics and Business, Shijiazhuang, Hebei, People’s Republic of China
Correspondence: Tao Li, School of Law, Hebei University of Economics and Business, Xuefu Road No. 47, Shijiazhuang, 050061, People’s Republic of China, Tel +86 18034167013, Fax +86 311 87655560, Email [email protected]
Abstract: In the occurrence of public health emergency events, such as the ongoing COVID-19 pandemic, the most severely affected areas may face various problems due to insufficient medical staff and materials. These problems can be solved by the adequate supply of trans-regional medical support. However, due to the Chinese government’s hierarchical and segmented administrative system, the provision of such support to fight against the COVID-19 epidemic in China met several challenges, including insufficient coordination and weak integration. This article summarizes four aspects of fragmentation related to the holistic management of this situation: cooperation from local government officials, supply of medical resources, support from logistical services, and incentive mechanisms. Furthermore, suggestions for improving the holistic management of trans-regional medical support are provided.
Keywords: public health emergency, COVID-19, trans-regional medical support, holistic management
Introduction
The outbreak of the coronavirus epidemic in Wuhan in late 2019 has been considered the most severe public health event in China in recent decades. In the following months, how to cope with the surge of COVID-19 patients within a short time became the top concern for Chinese governments at various levels. Under the directive of the Chinese central government, from January to March 2020, about 42,000 medical personnel from other provinces gathered in Wuhan,1 and massive amounts of medical materials donated by the Chinese people at home and abroad were sent to Hubei, thus giving rise to the phenomenon of trans-regional medical support (TRMS). Trans-regional support is a feasible approach to cope with medical capacity insufficiency during major public health events.2 However, this temporal and comprehensive management of rapidly rising numbers of medical staff and materials may also face problems, such as support fragmentation and collaboration inefficiency.
A Review of TRMS During the COVID-19 Pandemic in China
TRMS is a kind of emergency management that is initiated when a public health event occurs. In China, governments at different levels have already established their respective medical emergency plans. However, the COVID-19 pandemic still brought unprecedented challenges as a public health emergency with the fastest transmission speed and the widest range of infections in the country since 1949.3 In the early pandemic, Wuhan was in urgent need of medical staff and materials, thus requiring the central government to secure medical resources from elsewhere to maintain the normal operation of Wuhan’s medical system. This process of providing TRMS includes three key steps.
The Paralysis of Wuhan’s Medical System
Public health emergencies pose a massive challenge to the medical response capacity of a region’s hospital system. It is no exaggeration to say that no area or region can successfully respond to large-scale public health emergencies based only on its own medical system. When COVID-19 first emerged, Hubei Province in China was the most severely hit region, with Wuhan as the center of the epidemic. At the end of 2020, Hubei Province reported a total of 68,147 confirmed cases, of which over 50,000 were found in Wuhan from January to March 2020, exceeding half of the confirmed cases nationwide.4 At the end of 2019, a total of 117,100 medical staff were performing medical-related tasks in Wuhan, including 43,100 practicing physicians and 57,700 nurses.5 However, the available medical resources cannot meet the rapidly growing needs of COVID-19 patients. At the peak of the epidemic, a large number of suspected cases in Wuhan could not be tested, and it was difficult to find a bed if they wanted to be hospitalized.6 Furthermore, after Wuhan implemented a city-wide lockdown on January 23, 2020, suspected cases could not leave the city to find treatment elsewhere; thus, all people at home and in hospitals faced increased risks of infection. The imbalance between a sharply rising demand and the limited supply of medical resources almost led to the collapse of the local hospital system. Eventually, when officials had already exhausted all possible medical resources locally, seeking external assistance became the only option to restart Wuhan’s hospital system.
Coordination by the Central Government
Trans-regional medical assistance involves the mobilization and movement of medical staff, equipment, and other types of resources across various places, directed under the supervision of higher-level authorities. The unitary system implemented in China provides convenience in coordinating different regions and deploying TRMS. Under the direction of the central government, members of the Senior Expert Group of the National Health Commission (hereafter referred to as the “Health Commission”) traveled to Wuhan many times to provide guidance during the early days of the epidemic. On January 24, 2020, Shanghai, Guangdong, and other provinces sent the first batch of medical support staff to Wuhan. In the following days, more medical support teams from different provinces traveled to the city. On February 10, 2020, the Health Commission initiated a paring-assistance program, whereby 16 cities of Hubei Province, aside from Wuhan, obtained assistance from partner cities located in 19 other provinces. As of March 1, 2020, nearly 42,000 medical personnel had been dispatched to Hubei, among which about 30,000 were sent to Wuhan (Figure 1). Without the coordination and deployment of the Chinese central government, such large-scale TRMS would have been impossible to achieve.
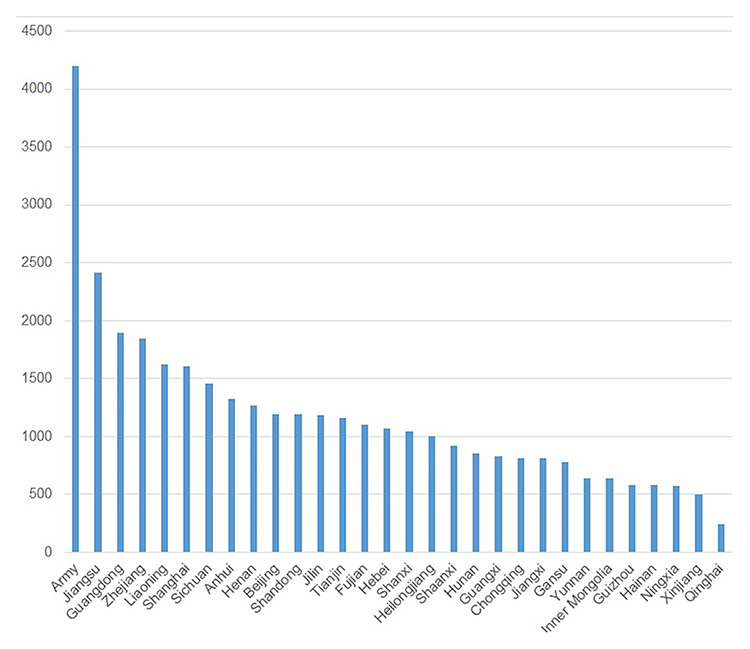 |
Figure 1 Numbers of medical personnel dispatched from outside Hubei to Wuhan (Jan. 24 to Mar. 1, 2020). Note: Adapted with permission from BjNews.com.cn. Available from: https://www.bjnews.com.cn/detail/158426496615591.html.18 |
Responses from Local Governments and Society
China’s one-party system in which the Communist Party of China leads all levels of government ensures that government leaders at lower levels follow instructions from those at higher levels. This system has largely facilitated the smooth implementation of TRMS. Notably, the medical staff who traveled to Wuhan to provide such support came from regions where there were fewer coronavirus cases. Apart from Hubei, only four other provinces had reported more than 1000 cases for 2020. Therefore, the provinces providing such assistance were not adversely affected by their act of sending out medical staff. Moreover, thanks to the historical tradition of mutual aid, TRMS was considered acceptable among the Chinese people.7
Generally, sufficient funds and materials are required to cope with a public health emergency. Specifically, a lack of protective materials may impede medical treatment work once a highly infectious disease breaks out. When experts announced at the end of January 2020 that the coronavirus could spread through small liquid particles and contact, masks, goggles, and protective clothing soon became scarce resources in China, and even medical personnel at the forefront faced shortages of these protective materials. In response, various organizations and kind people do their best to raise funds and collect protective materials for Wuhan, thus alleviating such shortages to some degree.
Fragmentation of TRMS
A public health emergency response is a systematic project. The Chinese government’s administrative system, which is organized into higher and lower levels, as well as different departments and regions, should be adjusted to improve its ability to respond to public health emergencies. If all units engaged in the provision of TRMS maintain separate approaches, this can lead to fragmentation and inefficiency.
Fragmentation in Cooperation Among Local Government Officials
The ability of government officials to respond quickly and correctly is crucial in the effective management of a public health emergency. The key to emergency response is to identify possible risks and nip them in the bud. For example, if the circulation of a known virus can be controlled at an early stage of an infectious disease outbreak, the medical system will be confronted with less pressure in patient treatment. However, in the aftermath of a public health event, Chinese government officials, many of whom do not have sufficient professional knowledge or act based solely on self-interest, are unable to act appropriately in the areas of problem identification, risk assessment, and information communication. For example, near the end of 2019,8 the novel coronavirus disease was already reported by Dr. Jixian Zhang to the local government, but no attention was given to this matter until late January 2020. At this early stage, the local government neither paid enough attention to the epidemic nor guided the public properly, resulting in a sharp increase in cases in a short time. Furthermore, some government officials did not fulfil their duty to prevent and control the disease, as required by higher authorities. By February 22, 2020, over 630 officials were held accountable for breaching epidemic prevention and control disciplines. The incompetency of some government officials further added difficulties in the effective and timely implementation of TRMS.
Fragmentation in the Supply of Medical Resources
When a public health emergency event occurs, the response often falls into a dilemma: on the one hand, the medical staff, medical materials, and professional volunteers are woefully inadequate; on the other hand, substandard medical materials donated by the public and the presence of incompetent staff may hinder the treatment of patients. The mismatch between medical supply and demand gives birth to “redundant forces” in medical assistance. In fighting the coronavirus pandemic in China, these redundant forces mainly consisted of substandard medical materials donated to Hubei from all around the world. As no technical standards were released at the beginning of the epidemic, many of the donated materials included face masks and diving goggles that did not meet medical standards, complicating the task of choosing suitable materials, which reduced the efficiency of medical materials allocation.9
Fragmentation in Logistics Support
Fulfilling the basic needs of food, clothing, housing, transportation, and so on, for the medical staff is crucial in the smooth implementation of TRMS. However, facing the social turmoil caused by a public health emergency, the local government, which is busy settling local inhabitants, may be incapable of providing good logistical services for the medical staff engaged in such medical support. In late January 2020, some medical staff sent from elsewhere did not have adequate food due to the lack of coordination and cooperation among the relevant departments responsible for managing logistics support. In February 2020, there was a shortage of non-medical materials, such as adult diapers and female sanitary products.10 In the current administrative system of China, the convening and delivery of trans-regional medical staff and the logistical service for them were arranged by various government departments at various levels. Due to the lack of emergency plans and relevant experience, some government departments, which were accustomed to fulfilling their regular obligations without proper communication regarding the unique situation caused by the pandemic, failed to meet the basic living needs of trans-regional medical staff.
Fragmentation in the Incentive Mechanism
Incentives are a vital management tool for guiding human resources. In the aftermath of a public health emergency event, ideological education or organizational pressure may play a role in motivating medical staff to participate in trans-regional support. Nevertheless, these management tools are not sustainable when facing a pandemic with unknown risks and indefinite durations. As stated by former Chinese leader Xiaoping Deng, it would be a kind of idealism to emphasize the spirit of sacrifice while neglecting the possible material benefits.11 As such, an institutionalized incentive mechanism is required in the mobilization of TRMS staff, as this can help achieve better results. However, the majority of doctors and nurses participated in the trans-regional support program for Hubei owing to their sense of responsibility or as a result of organizational motivation. In this case, relevant incentive measures did not produce a direct motivating effect because they were mostly issued after the TRMS was already underway or had already concluded.
TRMS from the Perspective of Holistic Management
A public health emergency endangers people’s lives, health, and safety, thus requiring prompt action from all relevant social entities. Thus, the response to such an event has an all-encompassing nature. For this reason, public health emergency management in China is no longer the exclusive responsibility of the Health Commission at all levels; instead, it follows a systemic cooperative mechanism that emphasizes the participation of all social units under the leadership of distinct government departments. This is in accordance with the proposition of holistic management theory.
Holistic management emerged as a correction to the concept of “new public management” (NPM), which was developed during the 1980s.12 While NPM was developed to meet increasing public service demand, it also led to the fragmentation of public institutions and difficulties in reaching public decisions.13 The rapid development of digital technology requires government departments to transition from a state of separation to that of constant coordination and cooperation and to provide technical support for inter-departmental coordination and integration. In this sense, holistic management can be achieved without drastic reforms in government institutions.
Coordination and integration are considered as the basic principles of holistic management.14 Coordination, which is not a novel concept in management practice, is regarded by advocates of holistic management as a process involving dialogues, joint planning, and joint decision-making among government agencies. Integration refers to the internal cooperation among all government departments and between government and external institutions. The holistic management of TRMS aims to eliminate deficiencies in staff recruitment, medical materials supply, logistical service, and incentive mechanisms caused by the segmentation of an existing governance system. Thus, its goal is to improve the overall outcome of TRMS.
First, the holistic management of TRMS should integrate the differentiated objectives of the participating subjects into an overlapping consensus. Multiple subjects, including physicians and nurses, medical materials manufacturers, and transportation enterprises, are mobilized to participate in TRMS, even though their respective goals might be diversified. Whether it is to improve their own reputation or to obtain reasonable economic benefits, these objectives are acceptable. However, compared to improving the efficiency of TRMS, these objectives are not imperative. As the first principle, the holistic management of TRMS should strive to improve overall efficiency in epidemic response. It should guide the participating subjects in cooperating together based on their common goals. However, the diverse demands of the participating subjects should also be properly recognized.
Second, the holistic management of TRMS should eliminate separation and segmentation across all the involved units and highlight cooperation among government agencies, the market, and civil organizations. Specifically, the focus should shift from relying one-sidedly on government departments to integrating the government and all non-governmental subjects. Indeed, the process of integration under holistic management is not a mechanical patchwork at a single center. It is also not a random collision under decentralized command nor a fragmentation under multiple authorities. Rather, it should be a deliberative coalition in an open, cooperative, and inclusive environment.
Third, the holistic management of TRMS should bring information technologies (IT) into full play. With IT, various stakeholders can deal with vast and complex information and respond to various resources, thus laying a solid foundation for TRMS by connecting different subjects and resources to achieve a common goal. In addition, IT, especially 5G technology, makes it possible for medical personnel to take part in medical support online. In fact, during the epidemic in Wuhan, many hospitals launched online consultation clinics whereby patients could communicate with doctors by sending pictures or making video calls.
Suggestions for Improving the Holistic Management of TRMS
Almost every crisis contains within itself the seeds of success as well as the roots of failure. Finding, cultivating, and harvesting that potential success is the essence of crisis management.15
Therefore, summarizing the lessons obtained from efforts to overcome the COVID-19 pandemic is an important way to improve the efficiency of public health emergency management. TRMS as an important strategic measure can also be improved through the following suggestions that are based on holistic management theory.
Upholding a Decision-Making Mechanism That Prioritizes Efficiency and Responsibility
TRMS results from decision-making under emergent conditions; thus, decisions must be made more decisively and rapidly than regular management decisions. However, emergency decisions must also be made based on a scientific method while ensuring accountability. First, professionals should play a more critical role in decision-making, with assistance from information transmission platforms. The Health Commission, which is also the central government department responsible for disease prevention and control in the country, is advised by a group of senior experts consisting of five epidemiologists. Further, an online direct report system has been established since the outbreak of the SARS epidemic in 2003. If necessary, the Health Commission will send members of the senior expert group to help local governments make scientific decisions. Such decisions must be based on detailed, objective, and comprehensive information. Accordingly, the responsibility of local governments in information disclosure should be enhanced by strengthening the punishment of information concealment in public health emergencies, thus ensuring the smooth flow of information necessary for decision-making. Second, once a decision is made, it must be implemented immediately to alleviate the shortage of medical resources in regions requiring medical support. However, the medical assistance task should be assigned to an aiding region according to its medical therapy capacity and the situation affected by a public health emergency.
Improving the Accuracy of Trans-Regional Medical Aid
Improving the accuracy of trans-regional medical aid can also improve the efficiency of public health emergency response in the long run. First, the need for medical staff and materials can be estimated by evaluating the trends in public health emergencies based on data modeling. Second, the medical staff engaged in trans-regional support should have professional expertise consistent with the required assistance. Furthermore, their ability to work under intense pressure and their cooperative attitude should also be considered. Third, the role of the Internet can be broadened in TRMS. For instance, doctors can participate in group consultation using cloud technology, thus reducing the barrier of distance in providing TRMS. Finally, the demand for medical materials should be more precisely released. Any medical institution urgently needing materials support should be adept at using various media to accurately express its demand. In this way, point-to-point donations can be realized immediately without any intermediate steps.
Improving Logistical Service by Integrating Planning and Market Measures
The primary living needs of medical staff should not be ignored when conducting TRMS. Due to several reasons, including business interruption, poor logistics, social distancing, and other restrictive conditions that may sometimes occur in response to infectious diseases, medical staff staying away from home could face difficulties obtaining daily necessities. To alleviate their anxiety in this regard, leading agencies in public health emergency response must arrange the unified procurement of those daily necessities and distribute them according to the needs of the medical staff. Smooth communication between medical staff undertaking TRMS and the logistics support department should also be ensured so that any demand from the former can be met in a timely manner. If some goods cannot be supplied immediately, good explanations should be provided to help the medical support staff understand the situation. Meanwhile, private enterprises, especially those with a sense of social responsibility, can be summoned to contribute to the provision of logistical products and services with reasonable prices.16
Creating Fair and Effective Incentives
Public health emergencies are unpredictable events. Launching large-scale TRMS implies that the medical staff will work in high-pressure and high-risk environments for an indefinite period.17 In this case, incentives must be established to affirm their contribution and improve their willingness to work under such conditions. Local government units sending out medical staff can set out institutionalized incentives in terms of remuneration, job promotion, and other forms of support. At the same time, the local governments receiving medical support can compensate for such expenditures assumed by the units providing medical staff. Nevertheless, incentives are not to be considered universal welfare. They must be realized according to the performance of the supporting medical staff, and the adverse effects of unfair incentives must be reduced.
Concluding Remarks
TRMS is a response to insufficiencies in regional medical resources during public health emergencies and is provided under the direction of higher authorities. Given that this is usually initiated in emergency situations, effective TRMS has significant value in overcoming pandemics or other types of catastrophes. The holistic management of TRMS can motivate all sectors of society to sustain the work of medical staff. It can also integrate the medical strengths of different regions and thus improve the overall efficiency of public health emergency responses. Generally, the medical groups engaged in trans-regional support are formed temporarily, and the members do not have much experience working in difficult environments. Thus, improving their ability to deal with public health emergencies remains an issue that should be discussed at a later time.
Acknowledgments
The author is grateful to the anonymous reviewers for their insightful comments to improve the quality of this article.
Funding
This work was supported by the Scientific Research and Development Program of Hebei University of Economics and Business (grant number 2021YB06).
Disclosure
The author reports no conflicts of interest in this work.
References
1. Sajid I. Medical support team workers leave Wuhan for hometowns; 2020. Available from: https://www.aa.com.tr/en/asia–pacific/medical–support–team–workers-leave-wuhan-for–hometowns/1786716.
2. Yao Y, Tian Y, Zhou J, Diao X, Di L, Wang S. Impact of population emigration from Wuhan and medical support on COVID-19 infection in China. J Epidemiol Glob Health. 2020;11:178–185. doi:10.2991/jegh.k.201121.001
3. The State Council Information Office of China. Fighting COVID-19: China in action; 2020. Available from: https://www.fmprc.gov.cn/ce/ceke/eng/gdxw/t1787011.htm.
4. Heath Commission of Hubei Province. Report of Hubei Province on the COVID-19 pandemic; 2020. Available from: http://wjw.hubei.gov.cn/bmdt/dtyw/202101/t20210101_3194761.shtml.
5. Wuhan Bureau of Statistics. Statistical bulletin on economic and social development in Wuhan; 2019. Available from: http://tjj.wuhan.gov.cn/tjfw/tjgb/202004/t20200429_1191417.shtml.
6. Hu Y. Does Wuhan have enough hospital beds for coronavirus patients? CGTN; 2020. Available from: https://news.cgtn.com/news/2020-02-18/Coronavirus–Does–Wuhan–have–enough–hospital–beds–ObxZUAhuJG/index.html.
7. Zhong K, Lu X. Exploring the administrative mechanism of China’s paired assistance to disaster-affected areas programme. Disasters. 2017;42(3):590–612. doi:10.1111/disa.12262
8. Li X, Cui W, Zhang F. Who was the first doctor to report the COVID-19 outbreak in Wuhan, China? J Nucl Med. 2020;61(6):782–783. doi:10.2967/jnumed.120.247262
9. Wuhan hospitals still desperate for supplies, but what happened to donations? CGTN; 2020. Available from: https://news.cgtn.com/news/2020-02-01/Hubei-Red-Cross-faces-scrutiny-over-whereabouts-of-donations-NJGbCJxb9u/index.html.
10. The Women’s Federation supported female medical workers at the frontline of the fight against the coronavirus with sanitary products; 2020. Available from: http://cpc.people.com.cn/n1/2020/0214/c64387-31587046.html.
11. Deng X. Selected Works of Deng Xiaoping. Vol 2. Beijing: People’s Publishing House; 1994.
12. Leat D, Seltzer K, Stoker G. Towards Holistic Governance: The New Reform Agenda. Houndmills, UK: Palgrave Macmillan; 2002.
13. Dunleavy P, Margetts H, Bastow S, Tinkler J. New public management is dead: long live digital-era governance. J Public Adm Res Theory. 2005;16(3):467–494. doi:10.1093/jopart/mui057
14. Zhu Q. From new public management to holistic management. Chin Administrat Manage. 2008;10:52–58.
15. Augustine NR. Managing the crisis you tried to prevent. Harv Bus Rev. 1995;73:147.
16. Waugh WL. Terrorism, homeland security and the national emergency management network. Public Organ Rev. 2003;3:373–385. doi:10.1023/B:PORJ.0000004815.29497.e5
17. Zeng Y, Zhen Y. Chinese medical staff request international medical assistance in fighting against COVID-19. Lancet Global Health. 2020. doi:10.1016/S2214-109X(20)30065-6.
18. BJ News. 30,000 Medical Staff, 20 Million Masks...This is how everyone supports Wuhan. 2022. Available from: https://www.bjnews.com.cn/detail/158426496615591.html.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.