Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Training and Subjective Confidence in CTG Interpretation in Germany: A National Cross-Sectional Survey
Authors Schäffler H, Dimpfl M, Hüner B, Janni W, Reister F, Andres S ![]()
Received 6 December 2025
Accepted for publication 24 April 2026
Published 3 June 2026 Volume 2026:19 586934
DOI https://doi.org/10.2147/JMDH.S586934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Henning Schäffler,1 Moritz Dimpfl,2 Beate Hüner,1 Wolfgang Janni,1 Frank Reister,1 Sophia Andres1
1Department of Gynecology and Obstetrics, University Hospital Ulm, Ulm, Germany; 2Department of Gynecology and Obstetrics, University Hospital Mannheim, Mannheim, Germany
Correspondence: Sophia Andres, Department of Gynecology and Obstetrics, University Hospital Ulm, Ulm, Germany, Email [email protected]
Purpose: Cardiotocography (CTG) is widely used for intrapartum fetal surveillance, but interpretation remains heterogeneous and prone to interobserver variation. This study explored which CTG classification systems are used in German maternity care, how CTG interpretation is taught, and how confident midwives and obstetricians feel when interpreting CTG traces and fetal scalp blood sampling results.
Patients and Methods: We conducted a national pilot exploratory online cross-sectional survey among midwives, obstetricians, and trainees in Germany. The questionnaire covered workplace characteristics, professional experience, CTG education, onboarding, current use of CTG classification systems, and self-rated confidence using an intuitive 0– 100 scale. The survey was developed by the research team for this exploratory project and was not formally validated or pilot tested. Analyses were descriptive only.
Results: A total of 1,132 respondents completed the questionnaire, including 60.4% midwives, 30.5% obstetricians, and 9.6% students. CTG was routinely used by 95.5% of respondents, and FIGO was the most commonly reported classification system (85.3%). CTG education during formal professional training was reported by 79.7% of midwives but by only 9.5% of junior doctors. Among physicians, CTG knowledge was commonly acquired from colleagues or through workplace experience. Only 39.7% of junior doctors reported systematic onboarding in the delivery room. More than half of junior doctors and 39.4% of specialists had not attended CTG training in the previous five years. Across professional groups, respondents reported only moderate confidence in CTG interpretation. Nearly all participants (99%) expressed a need for structured CTG training in Germany.
Conclusion: This exploratory survey suggests considerable variation in CTG education, onboarding, and self-reported confidence among maternity care professionals in Germany. The findings support the need for more structured and recurring CTG education, while underscoring that the present data reflect subjective perceptions rather than objective competence or clinical outcomes.
Keywords: cardiotocography, CTG training, fetal monitoring, subjective confidence, survey, Germany
Introduction
Cardiotocography (CTG) has been an established component of intrapartum care for decades and remains part of routine obstetric practice in Germany.1,2 In everyday delivery-room care, CTG findings contribute to communication, escalation, and clinical decision-making, rendering their interpretation highly relevant to routine practice.
At the same time, CTG interpretation is not based on a single universally applied framework. Multiple scoring and classification systems have been used in obstetric care, including older national approaches as well as international systems such as FIGO-, NICE-, and ACOG-based classifications.3–8 Where different interpretative frameworks coexist, differences in terminology, thresholds, and management implications may hinder consistent communication and limit comparability across institutions.
In Germany, greater harmonization of specialist training, a shared professional language, and more standardized decision pathways are important goals in obstetric care. These aims also require comparable teaching content, consistent documentation, and a common basis for multicenter data collection and future research.9 However, before such structures can be developed, the current state of practice must first be understood. An exploratory national assessment is therefore needed to identify how CTG is currently interpreted in German delivery units, which scoring or classification systems are used in routine care, and to what extent practice may differ between professional groups or institutions. This baseline is essential for informing structured curricula, standardization efforts, and targeted continuing education.
Subjective confidence in CTG interpretation is another relevant aspect in this context, because labor often requires rapid decision-making under conditions of uncertainty, with potentially far-reaching consequences. Feeling insufficiently secure in CTG assessment may increase reliance on additional diagnostic measures, senior support, or intervention-oriented decision-making. Moreover, persistent uncertainty in the emotionally demanding environment of obstetric care may contribute to stress and reduce professional confidence. Although self-reported confidence does not measure objective competence, it may still help identify perceived educational needs and areas in which support structures are lacking.10
This question is especially relevant in Germany, since the current S3 guideline on vaginal birth at term recommends use of the FIGO 2015 classification for intrapartum CTG interpretation.1 However, implementation is not necessarily uniform across institutions, and local routines, departmental culture, and available teaching structures may continue to shape clinical practice.11
In parallel, professional training pathways in Germany differ between midwives and physicians. Midwives usually receive profession-specific training with structured curricular content, whereas physicians commonly acquire delivery-room competencies during postgraduate specialist training in obstetrics and gynecology.12,13 This workplace-based training may vary considerably between hospitals with regard to supervision, onboarding, and formal CTG teaching. At the same time, the specialist training catalogue requires experience in the interpretation of 300 antepartum and intrapartum CTGs, underlining the central role of CTG in obstetric training.13
Despite this clinical and educational relevance, little national information is available on which CTG interpretation systems are used in Germany, how CTG interpretation is taught and learned across professional groups, and how secure professionals feel when applying CTG in practice. The aim of this study was therefore to provide a national cross-sectional description of current CTG practice in Germany by assessing which classification systems are used in routine care, how CTG interpretation is taught and learned, and how confident midwives and obstetricians feel when applying CTG in clinical care.
Materials and Methods
This pilot exploratory study was based on an online cross-sectional survey targeting midwives, obstetricians, and trainees involved in intrapartum care in Germany. The questionnaire was developed by the research team based on clinical experience and covered workplace characteristics, level of care, support options during labor, professional experience, CTG education, onboarding, CTG application, interpretation systems in use, perceived confidence in CTG interpretation, perceived confidence in fetal scalp blood sampling, and perceived need for further training.
The questionnaire comprised 29 items, including single-choice questions, multiple-choice questions, yes/no questions, and self-rating items on an intuitive visual 0–100 scale. Open text fields were not included. The instrument was created for this exploratory project and was neither formally validated nor pilot tested before dissemination. This limits the interpretability, comparability, and measurement precision of the results.
The survey was implemented using SurveyMonkey. Participants were approached through two distribution channels. First, an Email invitation was sent through the CoBRA program, a filtered address database of maternity clinics in Germany, with a request that clinic administrators forward the survey invitation to staff involved in peripartum care. Second, the survey link was distributed online in connection with a CTG training course attended by 3,300 participants. Because the invitation could have been forwarded internally and because overlap between both recruitment channels could not be quantified, the exact number of individuals who received the survey remains unknown. Consequently, an exact response rate and the representativeness of the sample cannot be determined with certainty.
This study was planned as a purely descriptive, exploratory, and hypothesis-generating pilot study. No a priori sample size calculation or statistical power analysis was performed, and only descriptive analyses were used. Results are therefore intended to characterize patterns in the sample rather than to support formal hypothesis testing or causal inference. Mean values of the 0–100 confidence ratings are presented descriptively and should not be interpreted as validated interval-scale measurements.
This study was conducted in accordance with the Declaration of Helsinki. Participation was voluntary and anonymous. Before accessing the questionnaire, participants were informed about the purpose of the study, the voluntary nature of participation, the anonymous handling of data, and their right to discontinue participation at any time. Proceeding to the online survey was considered to indicate informed consent. According to the local ethics committee policy, formal ethical approval was not required for this anonymous survey of healthcare professionals. A full list of questionnaire items is provided separately as Supplement Table 1. Participants were allowed to skip questions, and denominators therefore vary across items.
Results
A total of 1,132 respondents completed the questionnaire. Of these, 60.4% were midwives, 30.5% were obstetricians, and 9.6% were students in medicine or midwifery.
Overall, 95.5% of respondents reported using CTG for fetal monitoring during labor. The FIGO classification was the most commonly reported interpretation system and was used by 85.3% (960/1125) of respondents, whereas 4.9% (55/1125) reported using physiological CTG interpretation. Respondents with more than 10 years of professional experience more often reported use of the Fischer score than those with less experience (Supplement Figure 1 and Supplement Table 2).
Marked differences were observed in reported CTG education. Among midwives, 79.7% (498/625) stated that CTG had been taught during formal training, whereas only 9.5% (14/147) of junior doctors reported this. Among physicians, CTG knowledge was commonly reported to be acquired from colleagues, and 25.0% (86/344) described on-the-job learning in clinical practice as an important source of CTG training (Figure 1).
 |
Figure 1 CTG training among midwives and obstetricians. Abbreviation: CTG, cardiotocography. Notes: A total of 79.7% of midwives (498/625) reported having received CTG education during training or studies, whereas only 9.5% of resident physicians reported the same. Among physicians, CTG training was mainly acquired through experiential learning and instruction from colleagues. |
Among junior doctors, 80.8% (118/147) reported that they had already managed births independently during their first year of specialist training. When respondents were asked to rate how secure they had felt during their first independently managed birth on a 0–100 scale, the mean reported values were 36 among junior doctors, 41 among specialists, and 62 among midwives (Figure 2). These values describe subjective perceptions and were not compared inferentially.
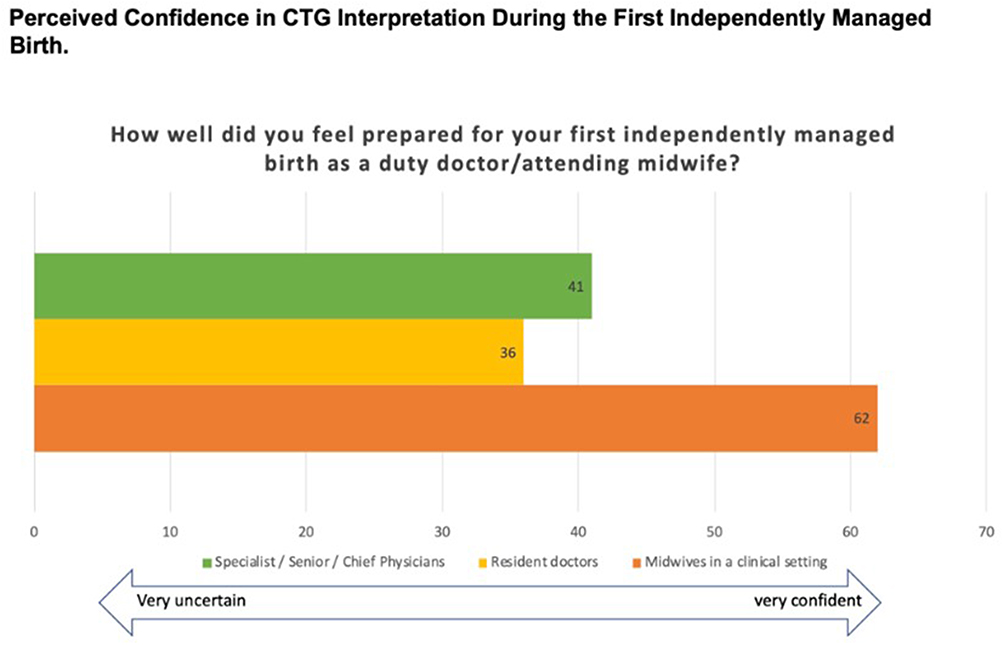 |
Figure 2 Perceived confidence in CTG interpretation during the first independently managed birth. Abbreviations: n, number; M, median; SD, standard deviation. Notes: Participants provided an intuitive rating on a scale from 0 to 100, where 100 indicates “very confident” and 0 indicates “very uncertain.” The data show lower mean self-reported confidence among physicians than among midwives during the first independently managed birth. Total sample: n = 1,024; resident physicians n = 147 (M = 36.1, SD = ±23.0); senior physicians (specialists, senior consultants, and department heads) n = 198 (M = 41.0, SD = ±24.1); midwives n = 679 (M = 61.9, SD = ±24.1). |
Self-rated confidence in CTG interpretation for fetal well-being was moderate overall, with mean values between 65 and 72 out of 100 across professional groups. Reported confidence in fetal scalp blood sampling was of a similar magnitude (Figure 3 and Supplement Figure 2).
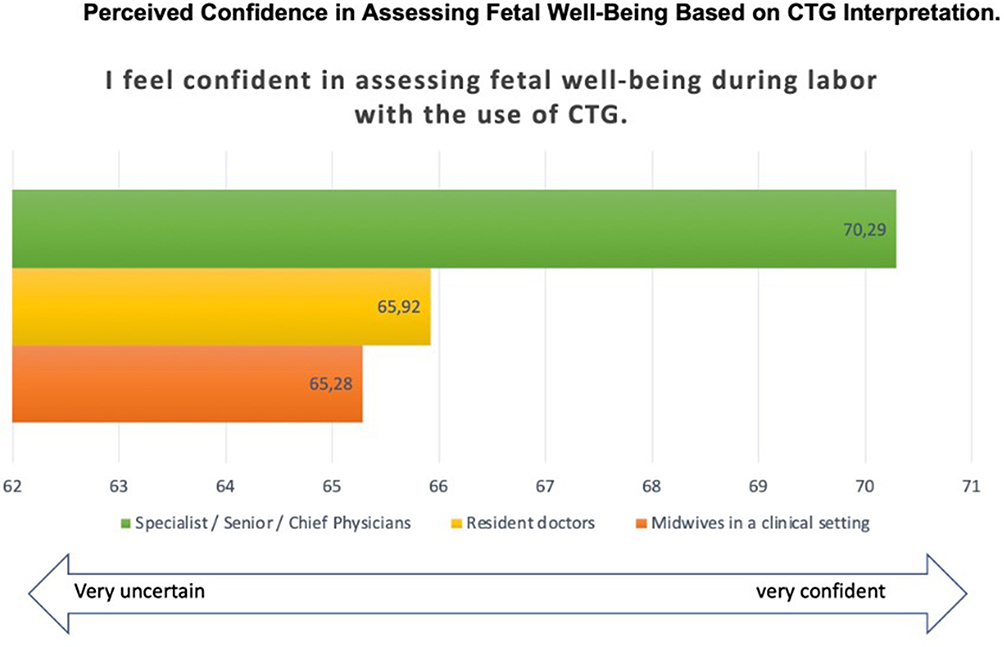 |
Figure 3 Perceived confidence in assessing fetal well-being based on CTG interpretation. Abbreviations: CTG, cardiotocography; n, number; M, median; SD, standard deviation. Notes: Participants provided an intuitive rating on a scale from 0 to 100, where 100 indicates “very confident” and 0 indicates “very uncertain.” Overall, the results suggest uncertainty in CTG interpretation for assessing fetal well-being during labour. Senior physicians reported higher mean self-reported confidence than resident physicians and midwives. Senior physicians: n = 156 (M = 70.3, SD = ±18.1); resident physicians: n = 118 (M = 65.9, SD = ±19.1); midwives: n = 532 (M = 64.8, SD = ±19.4). |
Systematic onboarding in the delivery room was reported by 67.5% of specialists but by only 39.7% of junior doctors (Figure 4). Reported duration of onboarding also varied by level of training. Less than 1 week of orientation was reported by 55.1% of junior doctors and 26.9% of specialists, whereas 16.8% of junior doctors and 40.0% of specialists reported an onboarding phase lasting more than 4 weeks (Supplement Figure 3).
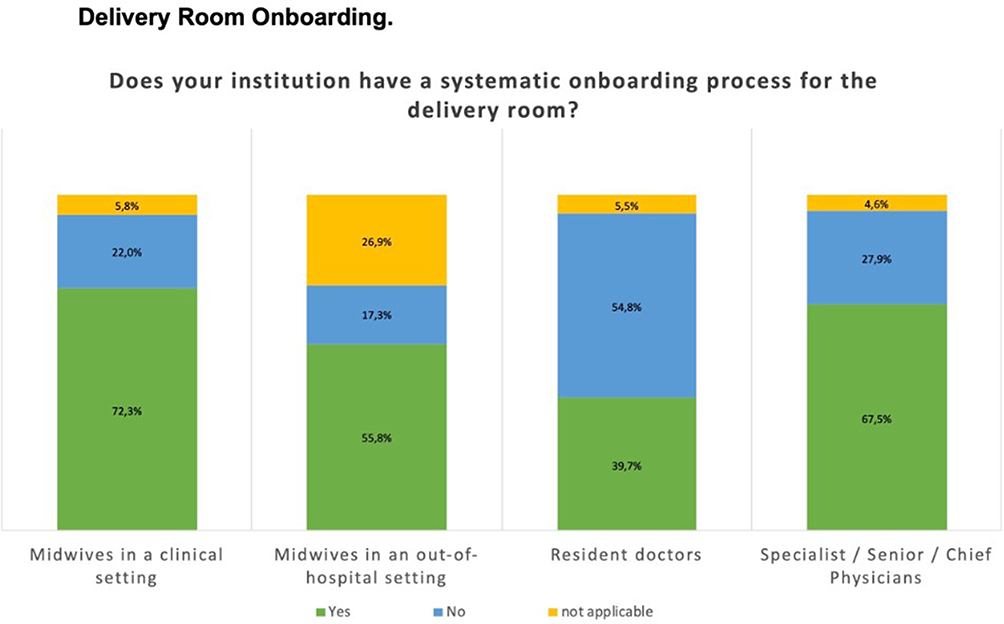 |
Figure 4 Delivery room onboarding. Notes: Reported delivery room onboarding varied according to level of training. Overall, most respondents indicated a systematic onboarding process. Among physicians, responses differed according to stage of training. |
CTG training was often described as a minor component of delivery-room orientation. Approximately half of junior doctors and one-third of specialists reported that CTG played no major role during onboarding (Supplement Figure 4). In addition, 55.8% of junior doctors and 39.4% of specialists stated that they had not attended CTG training during the previous 5 years, whereas around two-thirds of midwives reported attending 1–4 CTG courses in the same period (Figure 5). Only 17.7% of junior doctors and midwives reported regular CTG training within their own institution (Figure 6).
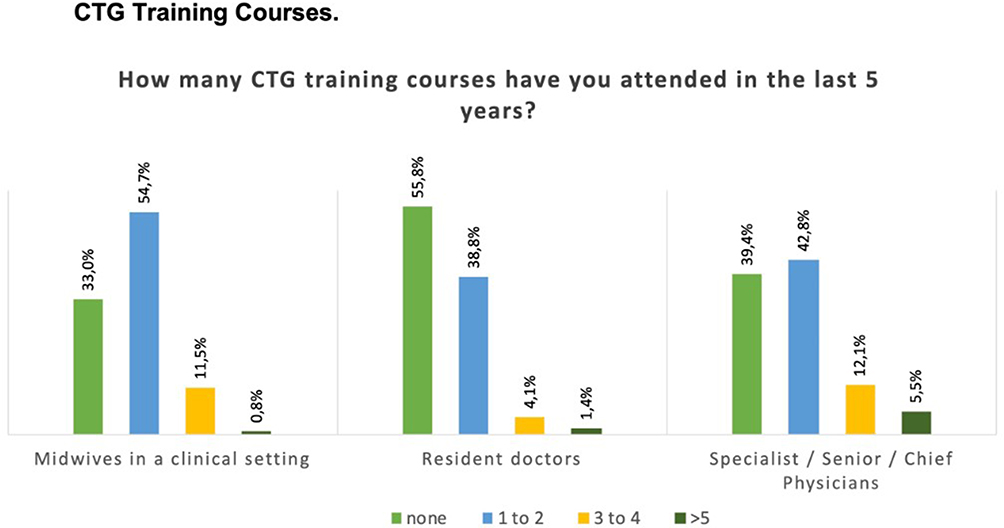 |
Figure 5 CTG training courses during the previous five years. Abbreviation: CTG, cardiotocography. Notes: Attendance at CTG training courses during the previous five years differed by professional group and level of training among obstetric care providers. Approximately one-third of midwives and more than half of resident physicians reported not having attended any CTG training during this period. |
 |
Figure 6 In-house CTG training courses. Abbreviations: CTG, cardiotocography; n, number. Notes: Regular in-house CTG training was reported infrequently across professional groups and levels of training among obstetric care providers. Only about 18% of resident physicians and midwives reported regular CTG training at their institution (total n = 968, including senior physicians n = 197, resident physicians n = 147, and midwives n = 624). |
Across the sample, 99% of respondents reported a need for structured CTG training in Germany.
Discussion
To our knowledge, this survey provides one of the first broad national descriptions of CTG education, onboarding, and self-reported confidence among midwives and obstetricians in Germany. The findings suggest substantial heterogeneity in how CTG interpretation is learned and supported in practice. FIGO was the most frequently reported classification system, yet structured teaching and regular refreshers appeared to be inconsistent, particularly among physicians in early postgraduate training.
A central finding is the contrast between the routine clinical use of CTG and the limited degree of formalized training reported by many respondents. Midwives more often described CTG as part of formal education, whereas physicians frequently reported learning CTG through colleagues or workplace exposure. This pattern is compatible with the structure of German postgraduate obstetric training, which is strongly workplace-based and may differ between departments regarding staffing, supervision, protected teaching time, and curriculum implementation. Such structural variation may help explain why onboarding and recurring CTG training were experienced so differently across respondents.
The present study assessed subjective confidence rather than objective competence. The reported scores should therefore not be interpreted as evidence that one professional group performs better or worse in CTG interpretation. However, the results still matter because they illustrate how professionals experience this important area of intrapartum decision-making. Departments in which junior staff feel insufficiently prepared may be more likely to face uncertainty, frequent escalation, or inconsistent responses to the same tracing, especially when local teaching structures are informal.
Our findings align with international literature showing that CTG interpretation is difficult and that educational interventions may improve knowledge and interobserver agreement, although effects vary by format and context. Previous reviews and observational studies suggest that repeated and multimodal training can be beneficial, including combinations of web-based teaching, case-based discussion, and on-site education.14–18 At the same time, this literature does not justify strong causal conclusions from the present survey. Our data cannot demonstrate that training deficits directly worsen clinical outcomes, nor can they show that structured training would reduce operative intervention rates in Germany.
The discussion of CTG education also needs to be situated within the broader clinical context. CTG interpretation does not occur in isolation but depends on labor stage, the overall clinical picture, and access to senior support and adjunctive tests.19,20 In particular, the second stage of labor deserves attention, as the risk of neonatal acidemia increases with longer duration and may rise further when pathological CTG patterns are present.21–23 Although our questionnaire did not explore stage-specific interpretation practices, this aspect should be considered in future research and training concepts.
Several structural barriers may contribute to the training gaps described by respondents, including limited protected teaching time, variable local curricula, staffing pressures in delivery rooms, and the absence of a nationwide mandatory CTG recertification framework. In some other healthcare systems, recurring fetal monitoring training has been implemented more formally.24,25 Germany currently lacks comparable mandatory national structures for all professional groups involved in intrapartum care.
A major strength of this study is the large sample size and the inclusion of respondents from different professional backgrounds. However, several limitations must be emphasized. The questionnaire was not formally validated or pilot tested. Recruitment occurred partly in connection with a CTG training course, which may have introduced selection bias toward respondents with a particular interest in CTG. The exact denominator for all invited participants is unknown because forwarding through institutions could not be tracked and overlap between recruitment channels could not be quantified. As a result, representativeness and response rate remain uncertain. In addition, all confidence data were self-reported and measured on a non-validated 0–100 scale, so the results reflect subjective impressions rather than objective competency.
Taken together, the findings support the view that CTG education in Germany could benefit from clearer structures, recurring training opportunities, and more explicit onboarding standards. Future studies should combine survey data with objective assessments of CTG knowledge or performance and should evaluate whether different educational formats improve self-reported confidence, consistency, and clinically meaningful outcomes.
Conclusion
In this exploratory national survey, CTG interpretation was reported to be routine practice in Germany, but CTG education, onboarding, and self-reported confidence varied considerably across professional groups and workplaces. The results support the need for more structured and recurring educational strategies for professionals involved in intrapartum care. Because the present study was descriptive and based on subjective ratings, its findings should be interpreted as an overview of perceived training needs rather than as evidence of objective competence or outcome effects.
Use of Generative AI Tools
Generative AI tools were used only for language editing and rewording. Study conception, questionnaire development, data collection, analysis, and interpretation were performed by the authors.
Data Sharing Statement
The data that support the findings of this study are available in the Uni Ulm CloudStore: https://cloudstore.uni-ulm.de/s/rBomWeAFAgtbHgc.
Ethics Statement
According to the guidance of the local ethics committee at Ulm University, formal ethics approval was not required for this anonymous survey of healthcare professionals. Participation was voluntary and anonymous, and proceeding to the survey after reading the study information was considered informed consent.
Acknowledgments
The authors thank all midwives, obstetricians, and trainees who participated in this survey.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Prof. Dr. Frank Reister reports that he is a coauthor for the german guideline vaginal delivery at term, I conduct classes and workshops for physiological CTG Interpretation. Dr Sophia Andres reports that she is a lecturer for physiological CTG Interpretation on workshops and congresses and have written content for Ambos learning platform.The authors report no conflicts of interest in this work.
References
1. Abou-Dakn M, Schäfers R, Peterwerth NVGAT. S3 Leitlinie AWMF. 2020;245.
2. Beard RW, Filshie GM, Knight CA, Roberts GM. The significance of the changes in the continuous fetal heart rate in the first stage of labour. BJOG. 1971;78:865–9. doi:10.1111/j.1471-0528.1971.tb00198.x
3. Richter R, Brun Del Re R, De Grandi P, Hammacher K, Hindemann P. Klinische Bedeutung der Reifegradbestimmung bei kardiotokographischem Hinweis auf eine fetale Gefährdung. Gynakol Geburtshilfliche Rundsch. 1974;14:64–66.
4. Schneider K, Butterwegge M, Daumer M, et al. Leitlinien-Detailansicht Anwendung des CTG während Schwangerschaft und Geburt. Available from: http://www.awmf.org/leitlinien/detail/ll/015-036.html. Registernu. 2013.
5. Fischer WM, Stude I, Brandt H. A suggestion for the evaluation of the antepartal cardiotocogram (author’stransl). Z Geburtshilfe Perinatol. 1976;180:117–123.
6. NICE Guideline: fetal monitoring in labour. (2022). Available from: https://www.nice.org.uk/guidance/ng229/documents/draft-guideline.
7. ACOG Committee Opinion No. 348: umbilical Cord Blood Gas and. Obstetrics & Gynecology. 2006. Available from https://journals.lww.com/greenjournal/citation/2006/11000/acog_committee_opinion_no__348__umbilical_cord.58.aspx.
8. Ayres-De-Campos D, Arulkumaran S. FIGO consensus guidelines on intrapartum fetal monitoring: physiology of fetal oxygenation and the main goals of intrapartum fetal monitoring. Int J Gynecol Obstet. 2015;131:5–8. doi:10.1016/j.ijgo.2015.06.018
9. Lovers A, Daumer M, Frasch MG, et al. Advancements in fetal heart rate monitoring: a report on opportunities and strategic initiatives for better intrapartum care. BJOG. 2025;132:853–866. doi:10.1111/1471-0528.18097
10. Miller S, Abalos E, Chamillard M, et al. Beyond too little, too late and too much, too soon: a pathway towards evidence-based, respectful maternity care worldwide. Lancet. 2016;388:2176–2192. doi:10.1016/S0140-6736(16)31472-6
11. Fast ein Drittel aller Geburten im Jahr 2021 durch Kaiserschnitt - Statistisches Bundesamt. (2023). Available from: https://www.destatis.de/DE/Presse/Pressemitteilungen/2023/02/PD23_N009_231.html.
12. Plappert C, Graf J, Simoes E, Schönhardt S, Abele H. The academization of midwifery in the context of the amendment of the german midwifery law: current developments and challenges. Geburtshilfe Frauenheilkd. 2019;79:854–862. doi:10.1055/a-0958-9519
13. Lermann J, Schulmeyer CE, Beckmann MW. Weiterbildungsmöglichkeiten im Fach Frauenheilkunde und Geburtshilfe. Frauenheilkunde up2date. 2020;14:451–465.
14. Pehrson C, Sorensen JL, Amer-Wåhlin I. Evaluation and impact of cardiotocography training programmes: a systematic review. BJOG. 2011;118:926–935. doi:10.1111/j.1471-0528.2011.03021.x
15. Thellesen L, Sorensen JL, Hedegaard M, et al. Cardiotocography interpretation skills and the association with size of maternity unit, years of obstetric work experience and healthcare professional background: a national cross-sectional study. Acta Obstet Gynecol Scand. 2017;96:1075–1083. doi:10.1111/aogs.13171
16. Froc E, Philip C-A, Rudigoz R-C, et al. Fetal heart rate analysis: evaluation of an in situ training program oncardiotocography interpretation during labor in the Auvergne-Rhône-Alpes region (France). Gynecol Obstet Fertil Senol. 2018;46:645–652. doi:10.1016/j.gofs.2018.06.007
17. Zhu L-A, Blanc J, Heckenroth H, et al. Fetal physiology cardiotocography training, a regional evaluation. J Gynecol Obstet Hum Reprod. 2021;50:102039. doi:10.1016/j.jogoh.2020.102039
18. Gyllencreutz E, Hulthén Varli I, Lindqvist PG, Holzmann M. Reliability in cardiotocography interpretation - impact of extended on-site education in addition to web-based learning: an observational study. Acta Obstet Gynecol Scand. 2017;96:496–502. doi:10.1111/aogs.13090
19. Afors K, Chandraharan E. Use of continuous electronic fetal monitoring in a preterm fetus: clinical dilemmas and recommendations for practice. J. Pregnancy. 2011;1–7. doi:10.1155/2011/848794
20. Pinas A, Chandraharan E. Continuous cardiotocography during labour: analysis, classification and management. Best Pract Res Clin Obstet Gynaecol. 2016;30:33–47. doi:10.1016/j.bpobgyn.2015.03.022
21. Nurani R, Chandraharan E, Lowe V, Ugwumadu A, Arulkumaran S. Misidentification of maternal heart rate as fetal on cardiotocography during the second stage of labor: the role of the fetal electrocardiograph. Acta Obstet Gynecol Scand. 2012;91:1428–1432. doi:10.1111/j.1600-0412.2012.01511.x
22. Cavoretto PI, Seidenari A, Farina A. Hazard and cumulative incidence of umbilical cord metabolic acidemia at birth in fetuses experiencing the second stage of labor and pathologic intrapartum fetal heart rate requiring expedited delivery. Arch Gynecol Obstet. 2022;307:1225–1232. doi:10.1007/s00404-022-06594-1
23. Cavoretto PI, Seidenari A, Amodeo S, et al. Quantification of posterior risk related to intrapartum figo 2015 criteria for cardiotocography in the second stage of labor. Fetal Diagn Ther. 2021;48:149–157. doi:10.1159/000512658
24. NHS England » Saving babies’ lives: version 3. https://www.england.nhs.uk/long-read/saving-babies-lives-version-3/#element-4-effective-fetal-monitoring-during-labour. (2023).
25. Bundle E. of the Saving Babies Lives Care. Evaluation of the Implementation of the Saving Babies’ Lives Care Bundle in Early Adopter NHS Trusts in England. 2018.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.