")
Back to Journals » International Journal of General Medicine » Volume 17
Traditional Chinese Medicine is Associated with the Reduction in Endpoint Events in Patients with Gouty Arthritis: Cohort Study and Association Rule Analysis
Authors Chen Y , Liu J , Cong C, Li Y , Hu Y
Received 6 December 2023
Accepted for publication 6 February 2024
Published 13 February 2024 Volume 2024:17 Pages 525—539
DOI https://doi.org/10.2147/IJGM.S451097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Yiming Chen,1,2 Jian Liu,1,2 Chengzhi Cong,1 Yang Li,1 Yuedi Hu1
1The First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, Anhui, 230038, People’s Republic of China; 2Anhui Key Laboratory of Application and Development of Internal medicine of Modern Chinese Medicine, Hefei, Anhui, 230038, People’s Republic of China
Correspondence: Jian Liu, Email [email protected]
Objective: This study aimed to evaluate the effect of traditional Chinese medicine (TCM) on endpoint events in patients with gouty arthritis (GA).
Methods and Materials: A total of 2091 hospitalized GA patients were followed up by telephone, and propensity score matching (PSM) was used to reduce potential bias in the study design. Cox proportional risk model and Kaplan-Meier survival curve were utilized to analyze the impact and time effect of factors on the readmission of GA patients. The differences of laboratory indexes before and after treatment between the low and high exposure groups were compared, and the types and frequencies of medicines in all patients were counted. Association rule analysis was performed to investigate the association between TCM and test indexes or endpoint events.
Results: After 1:1 PSM, 187 patients were enrolled in the TCM group and 187 patients in the non-TCM group. The incidence of readmission, new tophus, and all-cause death was lower in the TCM group than that in the non-TCM group (P < 0.05). Cox proportional risk regression analysis showed that TCM, NSAIDs and uric acid lowering drug were independent protective factors for GA readmission. The protective effect was enhanced by the prolongation of TCM treatment and the drug combinations. Kaplan-Meier survival curves indicated a significantly lower readmission rate in the high exposure group than in the low exposure group (P < 0.01). Compared with before treatment, NLR, hs-CRP, UA, TC and other laboratory indexes of the low and high exposure groups were improved after treatment (P < 0.01); The improvement of TG and TC in the high exposure group was more significant than the low exposure group (P < 0.01). The analysis of medicines used by all patients identified the top 20 Chinese herbal medicines and the top 2 Chinese patent medicines. The core drugs identified through association rule analysis that can improve test index and reduce the incidence of endpoint events include Yiyiren, Danshen, and HQC, among others. The network diagram of association rule analysis intuitively shows the relationship between core drugs and “improvement of indicators” and “the absence of endpoint events”.
Conclusion: TCM is associated with a reduced incidence of endpoint events in patients with GA.
Keywords: gouty arthritis, cohort study, traditional Chinese medicine, Chinese patent medicine, neutrophil to lymphocyte ratio
Introduction
Gouty arthritis (GA) is the most common form of Crystal arthritis associated with diet, obesity, and genetics. Pathologically, GA is triggered by the deposition of sodium urate crystals in joints due to excessive production or impaired excretion of uric acid (UA).1,2 GA typically presents with painful redness, swelling, and even restricted movement of joints.3 The incidence of GA is on the rise in the past 10 years and shows a younger trend, and men are more prone to GA onset than women.4,5 Moreover, GA patients at the advanced stage are vulnerable to severe complications such as cardio-cerebrovascular disease, kidney disease, and liver disease, which significantly compromise the quality of life and pose heavy economic burdens.6
Encouragingly, traditional Chinese medicine (TCM) has shown promising efficacy in alleviating the clinical symptoms of GA. A randomized controlled trial of Qingre Lishi Decoction(QLRD)7 demonstrated that the QLRD group was outperformed the control group (basic treatment and colchicine tablets) in improving joint symptom, effective rate, uric acid (UA), erythrocyte sedimentation rate (ESR), interleukin-1β(IL-1β), NALP3. Some researchers8 have found that GA patients receiving the external application of compound Qingbi granules combined with basic medicine exhibited better joint pain and swelling relief, CRP and UA level, onset time, and efficacy duration than those treated with basic medicine alone, and no significant difference was found in the incidence of adverse events between the groups. Many scholars believe that the application of TCM can inhibit inflammatory responses, promote the dissolution and excretion of urate crystals, and prevent liver and kidney damage in GA patients.9–11 Since long-term use of Western medicine alone may cause damage to liver and kidney function, it is of great practical significance to explore the advantages of TCM application in GA and seek the possibility of TCM as a complementary or even alternative therapy for GA.
The real-world observational cohort study is particularly suitable for exploring the effects of TCM in managing chronic refractory diseases in the clinic.12–14 Therefore, we employed a cohort study to obtain evidence-based medical proof of TCM for GA. This cohort study followed up 2091 GA patients at the First Affiliated Hospital of Anhui University of Chinese Medicine and statistically analyzed the occurrence of endpoint events and medication. We then used association rule analysis to find the core drugs of TCM in the treatment of GA and confirm the relationship between TCM and the occurrence of GA endpoint events.
Methods and Materials
Data Collection
Diagnostic Criteria
The diagnostic criteria of GA referred to the gout classification criteria developed by the American College of Rheumatology and the European League Against Rheumatism in collaboration in 2015 and the guidelines for the combined diagnosis and treatment of gout and hyperuricemia developed by the Chinese Academy of Traditional Chinese Medicine in 2021.15,16 All patients with GA were admitted by a senior rheumatologist in our hospital according to the above two guidelines.
Inclusion Criteria
(1) Inpatients eligible for GA diagnosis between May 2012 and October 2022 at the First Affiliated Hospital of Anhui University of Chinese Medicine;
(2) Age of 18–85 years old.
Exclusion Criteria
(1) Patients requiring frequent use of high-dose hormone for combined diseases;
(2) Patients complicated with severe primary diseases involving the respiratory system and hematopoietic system;
(3) Patients unable to cooperate (eg, suffering from mental illness);
(4) Patients with important items missing or massive items missing from the medical case data.
Therapeutic Drugs
Referring to the guidelines for diagnosis and treatment of gout and hyperuricemia with integrated traditional Chinese and Western medicine, the drugs used were recorded during the follow-up period.17 The conventional Western medicine included colchicine, diclofenac sodium, celecoxib, febuxostat, allopurinol, etc. The commonly used TCM included Chinese patent medicine (CPM) and Chinese herbal medicine decoction (TCM decoction). (1) CPM: Huangqin Qingre Chubi Capsule (HQC), Xinfeng Capsule (XFC), Xinhuang Tablet, etc.; (2) TCM decoction: Simiao San, Dangguiniantong Decoction, Guizhi Shaoyao Zhimu Decoction, Shuanghe Decoction, Xuanbi Decoction, Qinpi Gout Formula, etc.; (3) Drugs for treating other diseases.
Collection of Data
A questionnaire was designed for the GA patient. The patients discharged with a primary diagnosis of GA were retrieved through the medical case information management system of the hospital and strictly screened according to inclusion and exclusion criteria. The general information of eligible cases was entered into the questionnaire, including name, gender, age, and telephone number.
Through telephone follow-up, the patient’s concurrent diseases (including the disease name, onset time, and change of condition), other diseases, drug use after discharge (including the drug name, dosage, and time), and occurrence of endpoint events (including the type, time and frequency) were inquired and recorded. Subsequently, the test indexes of all patients with successful follow-up at the time of admission and during the follow-up period were retrieved from the case information management system, including erythrocyte sedimentation rate (ESR), platelet count (PLT), neutrophil-to-lymphocyte ratio (NLR), white blood cell (WBC), complement C3, complement C4, high sensitive C-reactive protein (hs-CRP), uric acid (UA), creatinine (Cr), blood urea nitrogen (BUN), triglycerides (TG), and total cholesterol (TC). If a patient’s hs-CRP exceeded 20mg/L, the corresponding value was supplemented using that patient’s CRP.
All follow-up visits were done by our specialized physicians, and at least two physicians were involved in the supervision and verification of the data. The following flowchart depicts the screening and grouping process of GA patients (Figure 1).
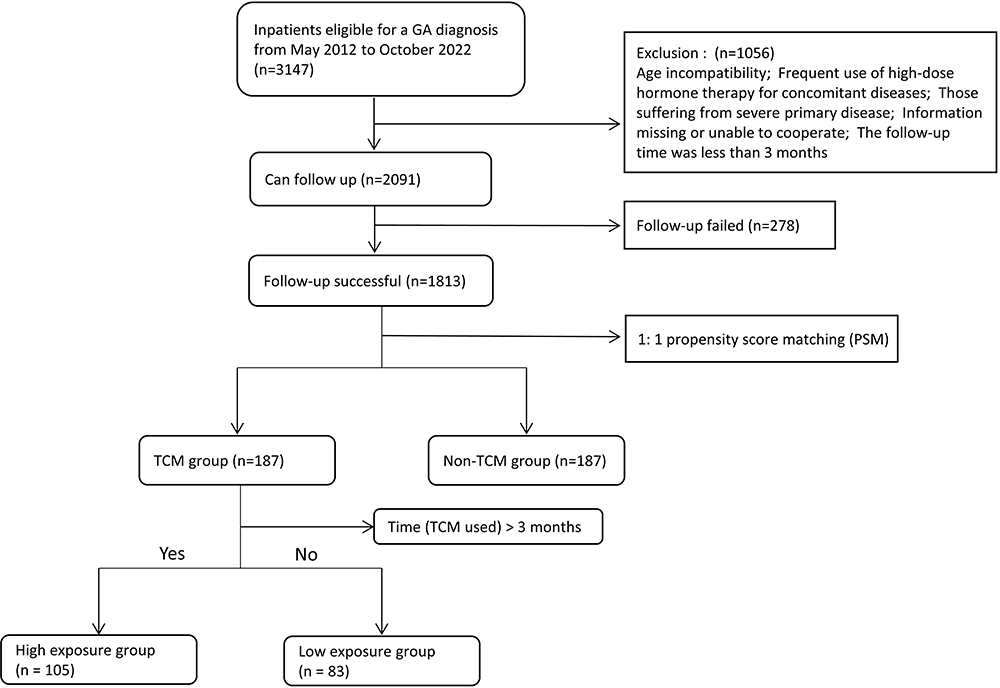 |
Figure 1 Flowchart of the study population. Abbreviations: GA, gouty arthritis; TCM, traditional Chinese medicine. |
Data Processing
Definition
Patients who did not receive TCM decoction and CPM during the follow-up period were defined as the non-TCM group, while patients who received TCM decoction or CPM as the TCM group. Further, the patients with a duration of TCM decoction or CPM for ≤ 3 months were assigned to the low exposure group, while those with a duration of TCM decoction or CPM for > 3 months were assigned to the high exposure group.
The combined diseases of GA were hypertension, kidney disease, hyperlipidemia, and diabetes mellitus. The basic medicines of GA were mainly non-steroidal anti-inflammatory drugs (NSAIDs), colchicine, glucocorticoids, and uric acid-lowering drugs. The endpoint events were defined as (1) readmission, (2) new tophus (tophus appears in body regions where tophus has not previously formed), (3) surgery (joint cavity irrigation, tophi excision, Joint repair or replacement, etc), (4) extra-articular lesions (gouty nephropathy, cardiovascular diseases, metabolic diseases, etc) and (5) all-cause death. Among them, (1) was the primary endpoint, and (2), (3), (4), (5) were the secondary endpoints.
Propensity Score Matching (PSM)
Since the number of GA cases who did not receive TCM decoction and CPM in our institution was small and the baseline status of GA patients might be an influential factor of endpoint events, we used propensity score matching (PSM) to eliminate baseline differences. The variables used for matching included gender, age, previous combined diseases (hypertension, kidney disease, hyperlipidemia, and diabetes mellitus), and basic medicines (NSAIDs, colchicine, glucocorticoids, and uric acid-lowering drugs). The grouping variables were TCM group and non-TCM group. The above covariates were used to generate scores for each patient using a multivariate logistic regression model with a 1:1 nearest-neighbor algorithm (caliper = 0.2). Each eligible patient was matched according to the score to obtain a matched cohort and perform baseline statistics.
Cox Proportional Risk Regression Analysis
Univariate and multivariate Cox regression models were constructed with the covariates including age, gender, hypertension, kidney disease, diabetes mellitus, hyperlipidemia, NSAIDs, colchicine, glucocorticoids, uric acid lowering drug, TCM treatment, duration of TCM treatment and drug combinations. The time effect of each covariate on the target variable “readmission” was analyzed to identify the independent influencing factors.
Kaplan-Meier Survival Curves
The cumulative risk of readmission events in patients in the TCM and non-TCM groups was compared using Kaplan-Meier survival curves. The TCM group was further divided into low and high exposure groups according to the duration of exposure to analyze the effect of the duration of TCM intervention on the risk of readmission events.
Association Rule Analysis and Network Diagram
The association between drugs and GA clinical indexes was analyzed using the Apriori module in SPSS Modeler 18.0. The use of a single herbal medicine or CPM was recorded as T, otherwise as F; the improvement of test indexes was recorded as T, otherwise as F. In addition, the use of a single herbal medicine or CPM was set as the antecedent (LHS, X) and the test index as the consequent (RHS, Y). The minimum Support was set at 20%, the minimum Confidence was 80%, and the Lift was greater than 1.
Similarly, the association between drugs and endpoint events was analyzed. The use of a single herbal medicine or CPM was recorded as T, otherwise as F; the absence of endpoint events was recorded as T, otherwise as F. The remaining settings were as before.
The association rule formula18 is as follows.



Finally, the most representative associations were listed according to the results of Support, Confidence, and Lift, and the network diagram of the above associations was drawn.
Statistical Methods
Since some of the variables in this study contained missing values, the method of multiple imputations was used to fill the missing values to maximize the statistical power and reduce the bias. Continuous variables conforming to normal distribution were expressed as mean ± standard deviation and compared using the t-test. Continuous variables that did not conform to normal distribution were expressed as median (interquartile spacing) [M (P25, P75)] and compared using the Mann–Whitney U-test. Categorical variables were expressed as frequencies (percentages) and compared using the chi-square test or Fisher’s test. A value of P<0.05 was considered statistical significance.
Processing Tools
All data were imported into Excel 2019, SPSS Statistics 26.0, and SPSS Modeler 18.0 for analysis. The images were visualized using Cytoscape 3.9.1.
Results
Inclusion, Exclusion and Follow-Up Results
The data of 3147 patients with a primary diagnosis of GA discharged between May 2012 and October 2022 were retrieved from the medical case information management system. According to the inclusion and exclusion criteria, 184 patients with age incompatibility were excluded; 138 patients who required frequent high-dose hormone for combined diseases were excluded; 432 patients with severe primary diseases were excluded; 211 patients with incomplete information or unable to cooperate were excluded; 91 patients with less than 3 months of follow-up were excluded. A total of 2091 patients were finally included for follow-up, and 1813 cases were successfully followed up, with a failure rate of 13.2%.
Among the 1813 patients, there were 1737 (95.8%) male and 76 (4.2%) female, aged 18–85 years [mean (54.89±15.14) years], and the duration of follow-up ranged from 3.0 months to 10.5 years [mean (50.58±30.26) months]. There were 188 cases in the non-TCM group and 1625 cases in the TCM group.
Baseline Characteristics of GA Patients in the TCM and Non-TCM Groups Before and After PSM Matching
There were significant differences in the use of some basic drugs such as NSAIDs, colchicine, and uric acid-lowering drugs between the two groups before matching (P < 0.05). To avoid bias caused by the baseline, we used the 1:1 PSM to balance the bias between the two groups in terms of general conditions, combined diseases, and basic medicines. After matching, there were 187 cases in each of the two groups, with no statistically significant differences in age, gender, combined diseases, and basic medicines (P > 0.05). In terms of endpoint events, the incidence of recurrent and newly-onset tophus and all-cause death was significantly lower in the TCM group than that in the non-TCM group (P < 0.05). In addition, surgery and extra-articular lesions were not statistically different between the two groups (P > 0.05; Table 1).
 |
Table 1 Baseline Characteristics of GA Patients Before and After PSM in the TCM Group and Non-TCM Group |
Influential Factors of GA Readmission
We defined five endpoint events, of which “readmission” best represented the disease progression. Therefore, we used a Cox proportional risk model to analyze the risk factors for readmission in patients with GA. Univariate analysis showed that the risk of GA readmission was significantly lower in the TCM group compared with that in the non-TCM group [hazard ratio (HR) = 0.65, 95% confidence interval (95% CI)= 0.41–0.71, P < 0.01]. The risk of readmission was also significantly lower in patients taking NSAIDs (HR = 0.69, 95% CI = 0.37–0.91, P = 0.04) and uric acid-lowering drugs (HR = 0.57, 95% CI = 0.39–0.94, P = 0.01). In contrast, the risk of readmission was significantly higher in patients with combined hypertension (HR = 3.31, 95% CI = 2.23–3.97, P = 0.03) and kidney disease (HR = 2.23, 95% CI = 1.85–2.81, P < 0.01) (Table 2).
 |
Table 2 The Cox Proportional Hazards Model for the Readmission of GA Patients |
The results of multivariate analysis showed that combined kidney disease, NSAIDs, uric acid lowering drug, TCM treatment, duration of TCM treatment, and drug combinations were independent influencing factors for readmission. Among them, combined kidney disease (HR=2.04, 95% CI=1.66–2.79, P < 0.01) was a risk factor, while NSAIDs (HR=0.54, 95% CI=0.32–0.81, P=0.01), uric acid-lowering drugs (HR=0.64, 95% CI=0.34–1.57, P=0.02), and TCM treatment (HR=0.59, 95% CI=0.38–0.82, P=0.02) were protective factors. Notably, TCM treatment significantly reduced the risk of readmission by 41% in patients with GA.
Based on the above results, we further analyzed the impact of the duration of TCM treatment on readmission in GA. Similarly, we also examined the effects of TCM in combination with uric acid-lowering drugs or NSAIDs on readmission in GA. The results showed that compared to the low exposure group, the high exposure group (HR=0.80, 95% CI=0.78–0.84, P < 0.01) could reduce the readmission risk in GA by 20%. Moreover, drug combinations such as low exposure & uric acid-lowering drug, high exposure & uric acid-lowering drug, low exposure & NSAIDs, and high exposure & NSAIDs all demonstrated varying degrees of reduced readmission risk in GA compared to those using only TCM (all P values ≤0.01) (Table 2).
Kaplan–Meier Survival Curve Analysis of the Time Effect of TCM on GA Readmission
Kaplan-Meier survival curves were used to compare the readmission risk between the TCM group and the non-TCM group. And we further explore the effect of TCM duration on the readmission risk. In the TCM group, GA patients treated with TCM decoction or CPM for ≤ 3 months were defined as the low exposure group, and those with > 3 months of TCM decoction or CPM as the high exposure group. The curves demonstrated that GA patients usually experienced readmission within a relatively short period of time after an episode, and approximately 50% of patients experienced readmission within three years. The risk of readmission was significantly lower in the TCM group than that in the non-TCM group (log-rank P < 0.01; (Figure 2a)). Also, the risk of readmission was significantly lower in the high exposure group than that in the low exposure group (log-rank P < 0.01; (Figure 2b)). There was also a significant difference in the readmission rate between the high and low exposure groups (P < 0.01; Table 3).
 |
Table 3 The Incidence of Readmission in the Low Exposure Group and High Exposure Group |
 |
Figure 2 The K-M survival curve of readmission in GA patients. (a) The K-M survival curve was used to analyze the effect of TCM on the risk of readmission. (b) The K-M survival curve was utilized to assess the effect of TCM intervention duration on the risk of readmission. Abbreviations: TCM, traditional Chinese medicine; HR, hazard ratio. |
Effect of TCM Intervention Duration on the Test Indexes of GA Patients
ESR, PLT, NLR, C3, C4, CRP, UA, and TC levels were reduced in the low exposure group after treatment compared to those before treatment (P < 0.01). Similarly, ESR, PLT, NLR, C3, C4, CRP, UA, Cr, TG, and TC levels were reduced in the high exposure group after treatment compared to those before treatment (P < 0.01). Moreover, the changes of the above indexes before and after treatment in the low and high exposure groups were compared, and the results showed that the decrease in TG and TC levels was more pronounced in the high exposure group than that in the low exposure group (P < 0.01; Table 4).
 |
Table 4 Effect of TCM Intervention Duration on Test Indexes in GA Patients |
Use Frequency of Herbal Medicines and CPMs in GA Patients
We analyzed the drug prescriptions of 1625 GA patients in the TCM group before PSM matching and calculated the use frequency of drugs. The top 20 herbal medicines used frequently could be divided into five major categories, namely, diuretic and dehumidifying medicine, heat-clearing and detoxifying medicine, blood-activating and stasis-removing medicine, spleen-strengthening and qi-invigorating medicine, and wind-dispelling and dehumidification medicine, as shown in Table 5. Similarly, the top 2 CPMs in the use frequency were HQC and XFC (Table 6).
 |
Table 5 The Use Frequency of Chinese Herbal Medicines |
 |
Table 6 The Use Frequency of Chinese Patent Medicines |
Association Rule Analysis of TCM Treatment and Test Indexes in GA Patients
Association rule analysis was performed with herbal medicines and CPMs as the antecedent and test indexs improvement as the postecedent. Specifically, the use of herbal medicines and CPMs was defined as T and the non-use as F. The decrease of ESR, PLT, NLR, WBC, C3, C4, hs-CRP, UA, Cr, BUN, TG, and TC was recorded as T and the non-decrease was defined as F. The results showed that the use of Yiyiren, Cheqiancao, Tufuling, Huangbai, Chuanniuxi, and HQC was strongly associated with the improvement of NLR, hs-CRP, TG, ESR, C3, and C4 (Table 7). The diagram of the association network for all terms also demonstrated similar results (Figure 3).
 |
Table 7 The Association Between the Use of TCM and the Improvement of Test Indexes |
 |
Figure 3 The network diagram of associations between TCM and test indexes. Abbreviations: NLR, neutrophil-lymphocyte ratio; hs-CRP, high-sensitive C-reactive protein; HQC, Huangqin Qingre Chubi capsule; ESR, erythrocyte sedimentation rate; C3, complement component 3; C4, complement component 4; TG, triglyceride; TC, total cholesterol. Notes: Circles represent terms, and larger circles and darker colors represent terms that occur more often. The line represents the association between two items, and the thicker line and darker color represent the stronger association between the two items. |
Association Rule Analysis of TCM Treatment and Endpoint Events in GA Patients
Association rule analysis was performed with herbal medicines and CPMs as the antecedent and the absence of endpoint events as the postecedent. Specifically, the use of herbal medicines and CPMs was defined as T and the non-use as F. The absence of endpoint events was defined as T, otherwise as F. The results showed that the use of Danshen, Chenpi, HQC, and Taoren was more associated with no readmission (Figure 4a); the use of Fuling and HQC was associated with no new tophus (Figure 4b); Shancigu and Tufuling were associated with no extra-articular lesions (Figure 4c; Table 8). Surgery and all-cause death had very few cases in this study and were not significantly associated with any of the antecedents.
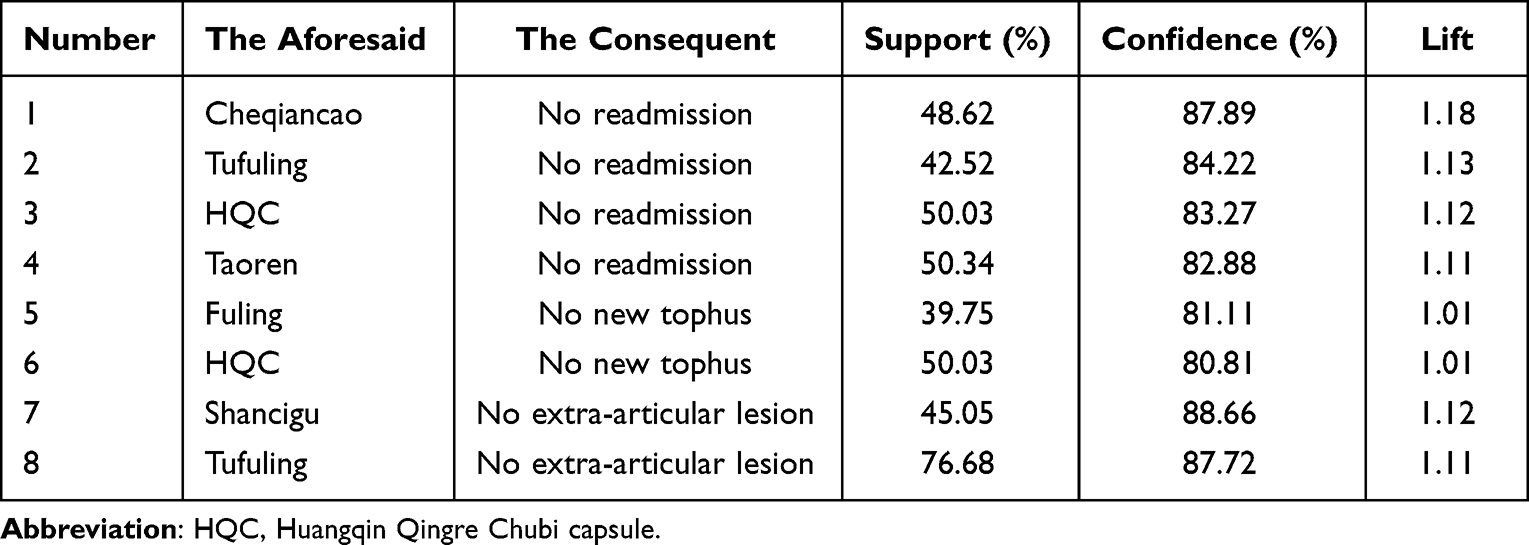 |
Table 8 The Association Between the Use of TCM and the Absence of Endpoint Events |
 |
Figure 4 The network diagram of association rule analysis between TCM and endpoint events in GA patients. (a) The network diagram of associations between TCM and no readmission. (b) The network diagram of associations between TCM and no new tophus. (c) The network diagram of associations between TCM and no extra-articular lesions. Abbreviations: HQC, Huangqin Qingre Chubi capsule; XFC, Xinfeng capsule. |
Discussion
GA is a common inflammatory joint disease with a high readmission rate.2,19 In our study, the readmission rate of GA patients reached 76.45% (1386/1813), and some patients had at least three readmissions within one year. In ancient China, GA was once called the disease of wealth and empire, indicating that the etiology of GA was more related to lifestyle. As productivity grows, people are prone to high-protein and high-fat diets in their daily life, eventually leading to a high intake of purines.20 As a result, the prevalence of GA increases constantly, especially in economically developed areas.21,22
The existing therapeutic drugs such as NSAIDs, colchicine, and glucocorticoids provide rapid pain relief in GA patients but also cause significant side effects.23–25 Uric acid-lowering drugs such as febuxostat and allopurinol can inhibit uric acid production, but long-term use tends to overwhelm the liver and kidney.26,27 GA patients may experience liver and kidney function reduction after years of recurrent attacks and medications.
To our knowledge, the present study is the first retrospective cohort study to evaluate the effect of TCM on GA patients. TCM holds great promise for complex chronic diseases with the advantages of multi-target, multi-component, and less adverse effects. Modern pharmacological studies have also found that some ingredients in these TCM decoctions can ameliorate GA symptoms, reduce inflammatory responses, and promote uric acid excretion. Accordingly, this study recruited 2091 GA patients with a follow-up period of up to 10 years, aiming to find evidence-based medical evidence for TCM in the treatment of GA.
This study had a rigorous follow-up plan design, which recorded the disease and medication status of each GA patient in detail and objectively. For the subsequent data analysis, PSM was used to eliminate bias, with age, gender, previous relevant diseases, and basic medicines used as matching variables. After matching, we found that the TCM group had an approximately 14% reduction in readmission rate, an approximately 10% reduction in new tophus, and an approximately 5% reduction in all-cause mortality compared to the non-TCM group.
Readmission is the most common endpoint event for rheumatic diseases, which can reflect the progress of GA patients to some extent. Further cox proportional risk regression analysis identified TCM treatment, NSAIDs, uric acid-lowering drugs, and drug combinations were independent protective factor for readmission. With the prolonged duration of TCM treatment, the protective performance of the high exposure group increased by 20% compared to the low exposure group. When TCM is combined with uric acid lowering drug or NSAIDs, it exhibits a superior effect compared to the sole use of TCM. We therefore concluded that TCM has a positive effect on delaying GA readmission, especially when it is used in combination with uric acid lowering drug or NSAIDs, in consistence with the findings found in previous studies.28
The duration of TCM treatment also affects the risk of disease readmission. The results of the K-M survival curve showed that the high exposure group had a lower risk of readmission than the low exposure group. Then the test indexes of the low exposure group and high exposure group before and after treatment were compared. We found that TCM reduced some indexes of inflammation, immunity, lipid metabolism, and renal function in GA patients, and that the high exposure group had an advantage over the low exposure group in reducing lipid metabolism. These results suggest that long-term use of TCM decoction and CPM contributed to delaying the progression of GA, improving the related indexes, and causing little or no renal damage.
We counted the top 20 herbal medicines and top 2 CPMs used in this study, correlated the use of these drugs with the improvement of test indexes and the absence of endpoint events, and plotted the association network using the Apriori algorithm. Apriori algorithm, a novel association analysis method based on big data, is an important component of data mining and can be used to determine combined patterns and correlations of target events and treatments.29,30 Our association rule analysis revealed that Tufuling, Chenqiancao, Yiyiren, Huangbai, Danshen, Chenpi, and HQC were the core drugs for improving test indexes and delaying endpoint events in GA patients. Modern pharmacological studies have shown that the total flavonoids of C. glabra in Tufuling can inhibit xanthine oxidase activity and upregulate the expression of uric acid-related transporter protein and its mRNA in renal tissues, thereby reducing uric acid significantly.31 The extract of Yiyiren can treat rheumatoid arthritis by inhibiting pro-inflammatory factors and reducing oxidative stress.32 The HQC developed by our team has shown favorable efficacy in the acute exacerbation of many rheumatic diseases. Our in vitro study found that HQC suppressed inflammatory responses of T cells in the serum of GA patients by downregulating miR-23a-3p and upregulating PTEN.33 Animal studies found that HQC ameliorated inflammatory responses in RA through the FZD8-Wnt/β-catenin signaling axis.34 In brief, clarifying the core drugs in GA treatment is conducive to guiding the clinical medication or developing new CPMs.
CPM as a new form of TCM combines modern pharmaceutical technology and traditional Chinese medicine theory, but in essence, it still belongs to the category of TCM.35 Therefore, this study allocated GA patients receiving HQC treatment to the TCM group for analysis. HQC (patent number ZL201110095718.X) is a characteristic CPM developed by our team, consisting of Huangqin, Zhizi, Yiyiren, Taoren and Weilingxian. We found a strong association between the use of HQC and the reduction of NLR in GA patients, with a support of 50.03%, a confidence of 82.01%, and a lift of 1.52. NLR is a composite inflammatory index that has received more attention in recent years in rheumatic diseases,36 immune diseases,37 inflammation,38 and tumors.39 NLR is defined as the ratio of the absolute number of neutrophils to the absolute number of lymphocytes in blood routine, which dynamically reflects the relative relationship between neutrophils and lymphocytes, thus suggesting inflammatory changes in patients.40 Some researchers41 found that NLR was higher in GA patients compared to healthy adults and that NLR was positively correlated with ESR and CRP, suggesting the ability of NLR to assess the disease activity of GA. In this study, we found that HQC effectively reduced NLR in GA patients, indicating that HQC may contribute to repressing immune inflammatory reactions in GA. Further animal and cellular experiments are warranted to validate the pharmacological effects and therapeutic mechanisms of HQC in GA.
The strengths of this study are: first, it is the first retrospective, large-sample, and long-term cohort study on TCM for GA; second, the protocol of this cohort study is derived from our team’s previous studies and further improved, making the protocol more mature and reliable; third, this study also emphasizes the analysis of CPM while analyzing TCM decoction, and the patients who used CPM or TCM decoction were included in the TCM group.
This study also has several limitations. Firstly, all patients included were from one medical institution, which may lead to selection bias. Secondly, merely 76 female patients were included. Due to the small sample size, the data should be interpreted with caution in female GA patients. Finally, we failed to record as many baseline characteristics of the patients as possible before hospitalization. Although we used PSM to control for these biases, the variables we used for matching did not include all baseline characteristics. In the future, we need to conduct large sample randomized controlled trials to further clarify the efficacy of TCM on GA. Animal experiments and cell experiments are also necessary, and we need to explore the molecular mechanisms of TCM in the treatment of GA.
Conclusions
To sum up, TCM can improve test indexes and delay endpoint events in GA patients. This study provides a reference for the comprehensive treatment of GA in the clinic. Further, we need to explore the pharmacological effects and molecular mechanisms of TCM on GA or conduct a large sample of randomized controlled trials to determine whether the findings revealed in this study are generalizable.
Data Sharing Statement
The data used in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent Statement
The present study was approved by the Ethics Committee of the First Affiliated Hospital of Anhui University of Chinese Medicine (2023AH-52). Verbal consent was obtained from all study participants after they were fully informed of the purpose of the study, the Ethics Committee of the First Affiliated Hospital of Anhui University of Chinese Medicine approved the verbal informed consent process. All the procedures were conducted according to all applicable institutional and governmental regulations concerning the ethical use of human volunteers in compliance with the Declaration of Helsinki.
Consent for Publication
This paper is our original work. We certify that this manuscript has not been published in part or whole elsewhere in any language, and it has not been submitted to any other journal for reviews.
We certify that all authors named deserve authorship, and that all authors have agreed to be so listed and have read and approved the manuscript and its submission to International Journal of General Medicine.
Acknowledgments
We thank Ling Xin, a senior Information Engineer, for his contributions to the statistical methods and data review of this paper.
Funding
The study was supported by grants from Anhui Provincial Laboratory of Applied Basis and Development of Internal Medicine of Modern Traditional Chinese Medicine (2016080503B041); The 12th batch of “115” Innovation team of Anhui Province (Anhui Talent Office [2019] No. 1); Anhui Famous Traditional Chinese Medicine Liu Jian Studio Construction Project (Traditional Chinese Medicine Development Secret [2018] No. 11); and Anhui Province Traditional Chinese Medicine Leading Talent Project(Traditional Chinese Medicine Development Secret [2018] No. 23).
Disclosure
The authors declare that they have no conflicts of interest regarding the publication of this paper.
References
1. Shi Y, Mucsi AD, Ng G. Monosodium urate crystals in inflammation and immunity. Immunol Rev. 2010;233(1):203–217. doi:10.1111/j.0105-2896.2009.00851.x
2. Navrátilová A, Voclonová V, Hulejova H, et al. Pos1142 interleukin-37: associations of plasma levels and genetic variants in gout. Ann Rheumatic Dis. 2021;80(Suppl 1):850–852. doi:10.1136/annrheumdis-2021-eular.3217
3. Dong L, Zhang S, Chen L, et al. In vivo anti-hyperuricemia and anti-gouty arthritis effects of the ethanol extract from amomum villosum lour. Biomed. Pharmacother. 2023;161:114532. doi:10.1016/j.biopha.2023.114532
4. Song J, Jin C, Shan Z, et al. Prevalence and risk factors of hyperuricemia and gout: a cross-sectional survey from 31 provinces in mainland China. J Transl Int Med. 2022;10(2):134–145. doi:10.2478/jtim-2022-0031
5. Mattiuzzi C, Lippi G. Recent updates on worldwide gout epidemiology. Clin Rheumatol. 2020;39(4):1061–1063. doi:10.1007/s10067-019-04868-9
6. Huang C, Liu J, Huang H, et al. Longitudinal transition trajectory of gouty arthritis and its combined diseases: a population-based study. Rheumatol Int. 2017;37(2):313–322. doi:10.1007/s00296-016-3634-9
7. Yu J, Li L, Liu J, et al. Influence of intervention treatment by “heat-clearing and diuresis-promoting” prescription on NALP3, an inflammatory factor in acute gouty arthritis. J Orthopaedic Surg Res. 2022;17(1):1. doi:10.1186/s13018-022-03046-z
8. Ren S, Meng F, Liu Y, et al. Effects of external application of compound Qingbi granules on acute gouty arthritis with dampness-heat syndrome: a randomized controlled trial. ChinMed. 2020;15(1):1. doi:10.1186/s13020-020-00398-8
9. Chi X, Zhang H, Zhang S, et al. Chinese herbal medicine for gout: a review of the clinical evidence and pharmacological mechanisms. ChinMed. 2020;15(1):1. doi:10.1186/s13020-020-0297-y
10. Li X, Han M, Wang Y, et al. Chinese herbal medicine for gout: a systematic review of randomized clinical trials. Clin Rheumatol. 2013;32(7):943–959. doi:10.1007/s10067-013-2274-7
11. Wang X, Long H, Chen M, et al. Modified Baihu decoction therapeutically remodels gut microbiota to inhibit acute gouty arthritis. Front Physiol. 2022;2:4.
12. Taur S. Observational designs for real-world evidence studies. Perspect Clin Res. 2022;13(1):12. doi:10.4103/picr.picr_217_21
13. Li Y, Liu Y, Cui J, et al. Cohort studies on chronic non-communicable diseases treated with traditional Chinese medicine: a bibliometric analysis. Front Pharmacol. 2021;1:2.
14. Wang X, Kattan MW. Cohort studies: design, analysis, and reporting. Chest. 2020;158(1):S72–S78. doi:10.1016/j.chest.2020.03.014
15. Jiang Q, Tang XP. Guidelines for diagnosis and treatment of gout and hyperuricemia with integrated traditional Chinese and Western medicine. J Traditional Chin Med. 2021;62(14):1276–1288.
16. Neogi T, Jansen TLTA, Dalbeth N, et al. 2015 gout classification criteria: an American College of rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheumatol. 2015;67(10):2557–2568. doi:10.1002/art.39254
17. Liu W. Guidelines for diagnosis and treatment of gout and hyperuricemia with integrated traditional Chinese and Western medicine. J Traditional Chin Med. 2023;64(01):98–106.
18. Yang J, Li Y, Liu Q, et al. Brief introduction of medical database and data mining technology in big data era. J Evid Based Med. 2020;13(1):57–69. doi:10.1111/jebm.12373
19. Galozzi P, Bindoli S, Doria A, et al. Autoinflammatory Features in Gouty Arthritis. J Clin Med. 2021;10(9):1880. doi:10.3390/jcm10091880
20. Zhang Y, Chen S, Yuan M, et al. Gout and diet: a comprehensive review of mechanisms and management. Nutrients. 2022;14(17):3525. doi:10.3390/nu14173525
21. Butler F, Alghubayshi A, Roman Y. The epidemiology and genetics of hyperuricemia and gout across major racial groups: a literature review and population genetics secondary database analysis. J Personal Med. 2021;11(3):231. doi:10.3390/jpm11030231
22. Dehlin M, Jacobsson L, Roddy E. Global epidemiology of gout: prevalence, incidence, treatment patterns and risk factors. Nat Rev Rheumatol. 2020;16(7):380–390. doi:10.1038/s41584-020-0441-1
23. Tan MS, Gomez-Lumbreras A, Villa-Zapata L, et al. Colchicine and macrolides: a cohort study of the risk of adverse outcomes associated with concomitant exposure. Rheumatol Int. 2022;42(12):2253–2259. doi:10.1007/s00296-022-05201-5
24. Al-Azayzih A, Al-Azzam SI, Alzoubi KH, et al. Nonsteroidal anti-inflammatory drugs utilization patterns and risk of adverse events due to drug-drug interactions among elderly patients: a study from Jordan. Saudi Pharm J. 2020;28(4):504–508. doi:10.1016/j.jsps.2020.03.001
25. Wang H, Zhou J, Guo X, et al. Use of glucocorticoids in the management of immunotherapy-related adverse effects. Thorac Cancer. 2020;11(10):3047–3052. doi:10.1111/1759-7714.13589
26. Yokose C, Lu N, Xie H, et al. Heart disease and the risk of allopurinol-associated severe cutaneous adverse reactions: a general population–based cohort study. Can. Med. Assoc. J. 2019;191(39):E1070–E1077. doi:10.1503/cmaj.190339
27. Zhang S, Xie Q, Xie S, et al. The association between urate‐lowering therapies and treatment‐related adverse events, liver damage, and major adverse cardiovascular events (MACE): a network meta‐analysis of randomized trials. Pharmacotherapy. 2021;41(9):781–791. doi:10.1002/phar.2609
28. Zhang Q, Li R, Liu J, et al. Efficacy and tolerability of Guizhi-Shaoyao-Zhimu decoction in gout patients: a systematic review and Meta-analysis. Pharm Biol. 2020;58(1):1023–1034. doi:10.1080/13880209.2020.1823426
29. Nishtala PS, Chyou T, Held F, et al. Association rules method and big data: evaluating frequent medication combinations associated with fractures in older adults. Pharmacoepidemiol Drug Saf. 2018;27(10):1123–1130. doi:10.1002/pds.4432
30. Huang L, Yuan J, Yang Z, et al. Patterns exploration on patterns of empirical herbal formula of Chinese medicine by association rules. Sci World J. 2015;2015:1–7. doi:10.1155/2015/148948
31. Huang L, Deng J, Chen G, et al. The anti-hyperuricemic effect of four astilbin stereoisomers in Smilax glabra on hyperuricemic mice. J Ethnopharmacol. 2019;238:111777. doi:10.1016/j.jep.2019.03.004
32. Zhang C, Zhang W, Shi R, et al. Coix lachryma-jobi extract ameliorates inflammation and oxidative stress in a complete Freund’s adjuvant-induced rheumatoid arthritis model. Pharm Biol. 2019;57(1):792–798. doi:10.1080/13880209.2019.1687526
33. Sun GH, Liu J, Wan L, et al. Effect of Huangqin Qingre Chubi Capsule-containing serum on the expression of miR-23a-3p/PTEN after co-culture of CD4+T cells and cardiomyocytes in gouty arthritis. J Beijing Univ Trad Chin Med. 2021;44(08):735–743.
34. Zhou W, Wang Y, Huang Y, et al. Huangqin Qingre Qubi Capsule inhibits RA pathology by binding FZD8 and further inhibiting the activity of Wnt/β-catenin signaling pathway. J Ethnopharmacol. 2023;302:115886. doi:10.1016/j.jep.2022.115886
35. Yin WX, Qu CH, Dong XX, et al. Preparation regularity of Chinese patent medicine in Chinese Pharmacopoeia(2020 edition,Vol.I). China J Chin Materia Medica. 2022;47(16):4529–4535. doi:10.19540/j.cnki.cjcmm.20220419.601
36. Targońska-Stępniak B, Grzechnik K, Kolarz K, et al. Systemic Inflammatory Parameters in Patients with Elderly-Onset Rheumatoid Arthritis (EORA) and Young-Onset Rheumatoid Arthritis (YORA)—An Observational Study. J Clin Med. 2021;10(6):1204. doi:10.3390/jcm10061204
37. Olsson A, Gustavsen S, Gisselø Lauridsen K, et al. Neutrophil‐to‐lymphocyte ratio and CRP as biomarkers in multiple sclerosis: a systematic review. Acta Neurol Scand. 2021;143(6):577–586. doi:10.1111/ane.13401
38. Pan R, Ren Y, Li Q, et al. Neutrophil–lymphocyte ratios in blood to distinguish children with asthma exacerbation from healthy subjects. Inter j Immuno Pharmacol. 2023;2:1042695850.
39. Li P, Li H, Ding S, et al. NLR, PLR, LMR and MWR as diagnostic and prognostic markers for laryngeal carcinoma. Am J Transl Res. 2022;14(5):3017–3027.
40. Chen YM, Liu J, Li Y, et al. The independent value of neutrophil to lymphocyte ratio in gouty arthritis: a narrative review. J Inflamm Res. 2023;16:4593–4601. doi:10.2147/JIR.S430831
41. Wu H, Zhou H, Chen P. Correlation of neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), and mean platelet volume (MPV) with gout activity: a monocentric and retrospective study. Medicine. 2022;101(35):e30242. doi:10.1097/MD.0000000000030242
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.