Back to Journals » OncoTargets and Therapy » Volume 17
Traditional Chinese Medicine in Regulating Tumor Microenvironment
Authors Wang Z, Li M ![]() , Bi L, Hu X
, Bi L, Hu X ![]() , Wang Y
, Wang Y
Received 31 October 2023
Accepted for publication 15 March 2024
Published 10 April 2024 Volume 2024:17 Pages 313—325
DOI https://doi.org/10.2147/OTT.S444214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Lukas Hawinkels
Ziwei Wang, Mengyao Li, Ling Bi, Xueqing Hu, Yan Wang
Department of Medical Oncology, Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China
Correspondence: Yan Wang; Xueqing Hu, Department of Medical Oncology, Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, Rd528 Zhangheng, Shanghai, 201203, People’s Republic of China, Email [email protected]; [email protected]
Abstract: Tumor microenvironment (TME) is a complex and integrated system containing a variety of tumor-infiltrating immune cells and stromal cells. They are closely connected with cancer cells and influence the development and progression of cancer. Traditional Chinese medicine (TCM) is an important complementary therapy for cancer treatment in China. It mainly eliminates cancer cells by regulating TME. The aim of this review is to systematically summarize the crosstalk between tumor cells and TME, and to summarize the research progress of TCM in regulating TME. The review is of great significance in revealing the therapeutic mechanism of action of TCM, and provides an opportunity for the combined application of TCM and immunotherapy in cancer treatment.
Keywords: cancer, tumor microenvironment, traditional Chinese medicine, anti-tumor effects
Background
Cancer is currently one of the leading causes of human mortality. According to the latest statistics from Global Cancer in 2020, there are approximately 19.3 million new cancer cases and nearly 10 million cancer deaths worldwide.1 Cancer treatment has always been a challenge for researchers. Since the beginning of the 20th century, researchers have come to realize that the interaction between cancer cells and tumor microenvironment (TME) plays an important role in promoting tumorigenesis and its progression, and that the TME consists of an immune microenvironment, mainly composed of immune cells, and a non-immune microenvironment, mainly composed of fibroblasts, which are both anti-tumorigenic, but also promote tumorigenesis and progression.2,3 Targeting the balance of immune cells in the microenvironment and enhancing tumor immunity have been the focus of tumor immunotherapy. Current therapeutic approaches, like chemotherapy and targeted therapy, have also achieved remarkable results and prolonged patient survival time, but the adverse effects and drug resistance have limited their clinical use.4–7
Traditional Chinese medicine (TCM) has been applied in clinical as an adjuvant therapy for anti-tumor treatment, which can reduce the adverse effects of radiotherapy/chemotherapy, and have synergistic effects with anti-tumor drugs to prolong the survival of tumor patients. The occurrence and development of tumor diseases are closely related to the low immune function of the human body. Especially after surgery, radiotherapy and chemotherapy, the immune system of the body is seriously damaged.8 More and more studies have confirmed that TCM can enhance anti-tumor effects by regulating the immune system.9,10 The aim of this study is to introduce how immune cells and non-immune cells in TME promote tumor progression, and to summarize the research progress of TCM in regulating TME.
Crosstalk Between Cancer Cells and TME
The TME mainly consists of innate and adaptive immune cells, as well as stromal cells,including T and B lymphocytes, tumor-associated macrophages (TAMs), myeloid-derived suppressor cells (MDSCs), tumor-associated neutrophils (TANs), natural killer cells (NKs), and dendritic cells (DCs).11 In TME, several types of cells are closely associated with the promotion of tumorigenesis and progression (Figure 1 and Table 1).
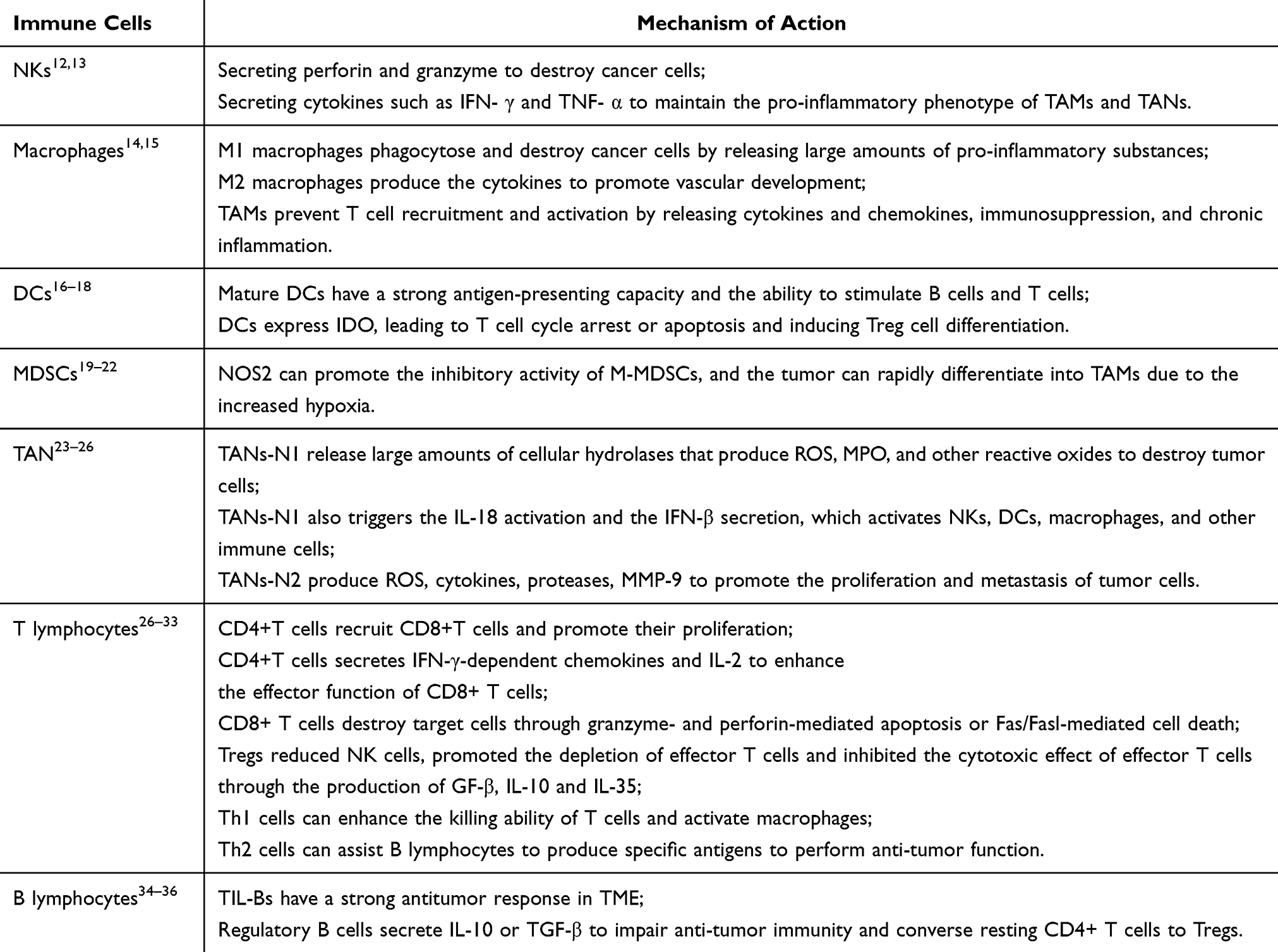 |
Table 1 Mechanisms of Action of Immune Cells |
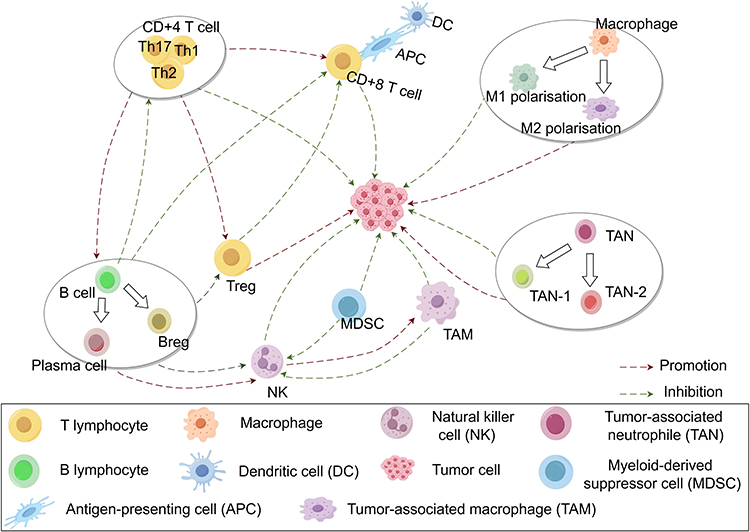 |
Figure 1 Crosstalk between cancer cells and TME cells. T lymphocytes mainly include CD4+ T cells, CD8+ T cells and Tregs, of which CD4+ T cells can differentiate into T helper 1 (Th1 cells) and T helper 2 (Th2 cells). Th1 cells can enhance the killing ability of T lymphocytes and activate macrophages; Th2 cells can assist B lymphocytes (B cells) to produce specific antigens and exert anti-tumor function; meanwhile, CD4+ T cells can recruit CD8+ T cells and promote tumor growth. Regulatory T cells (Tregs) can reduce NK cells and promote the depletion of effector T cells. TIL-Bs can reduce NK cells and promote the depletion of effector T cells. Secretion of IL-10 or TGF-β by regulatory B cells impairs antitumor immunity and converts quiescent CD4+ T cells into Tregs. NK cells secrete proinflammatory phenotypes that maintain tumor-associated macrophages (TAMs) and tumor-associated neutrophils (TANs). TANs differentiate into TAN-1 and TAN-2, of which TAN-1 inhibits tumor growth and TAN-2 promotes tumor cell proliferation and metastasis. Mature cells (DC cells) have strong antigen-presenting ability, and can block T cell cycle or apoptosis, and induce Treg cell differentiation. Macrophages are mainly polarized into M1 and M2 macrophages, most of which have antigen-presenting capacity. |
Crosstalk Between Innate Immune Cells and Cancer Cells
Dual Roles of Nature Killer Cells (NK cells)
NK cells, mainly derived from thymic bone marrow lymphoid stem cells, act on TIME-associated cells by secreting cytokines such as IFN- γ and TNF- α to maintain the pro-inflammatory phenotype of TAMs and TANs. In addition, NK cells secrete perforin and granzyme, which target and destroy cancer cells through antibody-dependent cell-mediated cytotoxicity. In addition, they trigger an immune response by releasing of immunomodulatory cytokines, thereby inhibiting cancer cell metastasis.12,13 However, it has been shown that TAMs and MDSCs release inhibitory cytokines such as TGF-β and IL-10, which prevent NK cells from migrating to TME and have anti-tumor effects.
Macrophages Subtypes and Their Opposite Roles
Macrophages are the most numerous group of immune cells in the TME, derived from monocytes, the progenitor monocytes in the bone marrow, and are present in almost all tissues with strong phagocytosis, killing ability, and pro-inflammatory responses.14 They mainly contains M1 macrophages and M2 macrophages. The former can phagocytose and destroy cancer cells by releasing large amounts of proinflammatory substances, while the latter mainly produce vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), transforming growth factor--β (TGF-β), platelet derived growth factor (PDGF), and other vasculature-promoting cytokines.14 TAMs, which are mainly composed of M2 macrophages, are immunosuppressive cells in TME.15 These TAMs prevent T cell recruitment and activation by releasing cytokines and chemokines, and participate in multiple signaling pathways that promote angiogenesis, immunosuppression, and chronic inflammation. Thus, they contribute to tumor development.15
Dual Roles of Dendritic Cells (DCs)
DCs are the primary effector cells in the immune response. In the resting state, DC cells are usually immature with reduced level of expression of MHC and stimulatory molecules, and are therefore unable to activate T cells.16 Mature DCs have a strong antigen-presenting capacity and the ability to stimulate B cells and T cells.17 In tumor immunity, DCs cannot kill tumor cells directly, but monitor and kill tumors by recognizing tumor cell-specific antigens and presenting them to T cells.18
Immunosuppressive Effects of Myeloid-Derived Suppressor Cells (MDSCs)
MDSCs are immature populations of DCs, macrophages, and granulocytes that significantly suppress immune cell responses.19 It has been found that MDSCs can be classified into different subtypes based on their specific functions. These subtypes include polymorphonuclear (PMN-MDSCs) and Monocyte-like MDSCs (M-MDSCs).20,21 PMN-MDSCs account for more than 70% of the total number of MDSCs in peripheral lymphoid organs, whereas M-MDSCs account for a much higher proportion of tumors. Interferon-γ (IFN-γ) has been shown to stimulate the inhibitory activity of M-MDSCs by activating the transcription factor STAT1, which in turn promotes the transcription of NOS2, one of the main enzymes responsible for the inhibitory activity of M-MDSCs. Differentiation of M-MDSCs toward macrophages depends on tissue. M-MDSCs differentiate slowly into macrophages in spleen, but rapidly into TAMs in tumors, a phenomenon that is regulated by hypoxia.20,22
Dual Roles of Tumor-Associated Neutrophils (TANs)
Neutrophils are myeloid progenitor cells of the human body and are important component of peripheral blood cells and TME. They play an important role in promoting and inhibiting tumor cell growth.23 TANs have a dual nature, and their functional diversity determines functional heterogeneity. In the early stages of tumor growth, TANs-N1 release large amounts of cellular hydrolases that produce reactive oxygen species (ROS), myeloperoxidase (MPO), and other reactive oxides to destroy tumor cells. It also triggers the activation of IL-18 and the secretion of interferon-β (IFN-β), which activates NKs, DCs, Macrophages, and other immune cells in the immune system and exert cellular immunity.24,37 As the tumor develops, TANs gradually change into N2 phenotype and produce various products such as ROS, cytokines, proteases, and matrix metalloproteinase-9 (MMP-9), thus promoting the proliferation and metastasis of tumor cells.25
Crosstalk Between Adaptive Immune Cells and Cancer Cells
T Lymphocyte Subtypes with Different Functions
In TME, T cells are one of the most important tools against tumor. Depending on the surface antigen, they mainly include CD4+T and CD8+T lymphocytes.CD4+T cells recruit CD8+T cells and promote their proliferation. In addition, it secretes IFN-γ-dependent chemokines and IL-2, which enhances the effector function of CD8+ T cells. They mainly differentiate into helper T cells (Th), which mainly include Th1 and Th2, as well as regulatory T cells (Tregs). Th1 cells enhance the killing ability of T cells, and activate macrophages, which exert significant anti-tumor effects. Th2 cells exert anti-tumor functions mainly by assisting B lymphocytes in the production of specific antigens.26,27
The classical phenotype of Tregs is CD4+CD25+Foxp3+, which belongs to the CD4+ T cell subpopulation, has low proliferative capacity, secretes cytokines such as IL-4, IL-10 and TGF-β, and acts mainly by suppressing immune response, maintaining immune homeostasis, and inducing immune tolerance, which is opposite to the role of helper T cells.28 Based on their products and biological characteristics, Tregs can be categorized into natural regulatory T cells (nTregs) and induced regulatory T cells (iTregs). Compared with nTregs, iTregs are more closely related to tumorigenesis and progression than nTregs.29,30 TGF-β, IL-10, and IL-35 produced by Tregs block anti-tumor immune response. TGF-β secreted by Tregs inhibits the cytotoxic effects of NK cells and cytotoxic T cells (CTLs), and promotes tumor growth. It also promotes depletion of effector T cells and inhibits the cytotoxic effects of effector T cells by producing IL-10 and IL-35.29,30 CD8+ T cells differentiate into CTL and memory T cells (Tm). Through antigen presentation, the T cell receptor (TCR) binds to MHC expressed by cancer cells, thereby specifically recognizing cancer cells. Upon binding to the TCR, CD8+ T cells eliminate target cells through granzyme- and perforin-mediated apoptosis or Fas/Fasl-mediated cell death.31 Nanotechnology promotes the expansion and infiltration of T cells, which significantly enhances the antitumor effect of T cells.32,33
B Lymphocyte Subtypes with Different Functions
B lymphocytes are the primary mediators of humoral immunity. In TME, B cells exert anti-tumor effects through antibody-dependent cytotoxicity and complement activation.34 Many studies have shown that B cells reside in the tertiary lymphoid structures (TLSs) of TME. Infiltrating B cells and plasma cells (PCs) have been referred to as tumor-infiltrating B lymphocytes (TIL-B), which have a strong anti-tumor response in TME.34,35 However, TIL-B rarely act alone, but are closely associated with T cells and promote T cell activation through antigen presentation.36 In addition, B cells over-secrete anti-inflammatory and pro-angiogenic mediators that promote inflammation and immunosuppression, thereby supporting tumor growth. TIL-Bs are mainly composed of effector and regulatory B cells, where regulatory B cells are an important cell population in the immunosuppressive microenvironment, either directly impairing anti-tumor immunity through the secretion of IL-10 or indirectly destroying tumorigenic immunity through the production of TGF-β and the conversion of resting CD4+ T cells into Tregs.36,38,39
Regulation of tumor microenvironment (TME) by TCM
The immune system is a natural defense against tumorigenesis and development. We have described in detail how immune cells defend against tumorigenesis and development above. Therefore, targeted regulation of the balance of immune cells in the microenvironment has always been the focus of tumor immunotherapy. As an important adjunct to antitumor therapy, a number of previous clinical studies have shown that TCM can alleviate the adverse effects of radiotherapy, improve quality of patients’ life, and work synergistically with anti-tumor drugs to prolong the survival time of cancer patients.40,41 In addition, studies have demonstrated that TCM herbs and thier active ingredients (polysaccharides, alkaloids, flavonoids, terpenoids, etc.) can enhance anti-tumor efficacy by modulating the immune system.42 In this section, the anti-tumor immunomodulatory mechanisms of representative TCM formulae (Table 2, Supplementary Table 1) and compounds (Table 3) will be discussed.
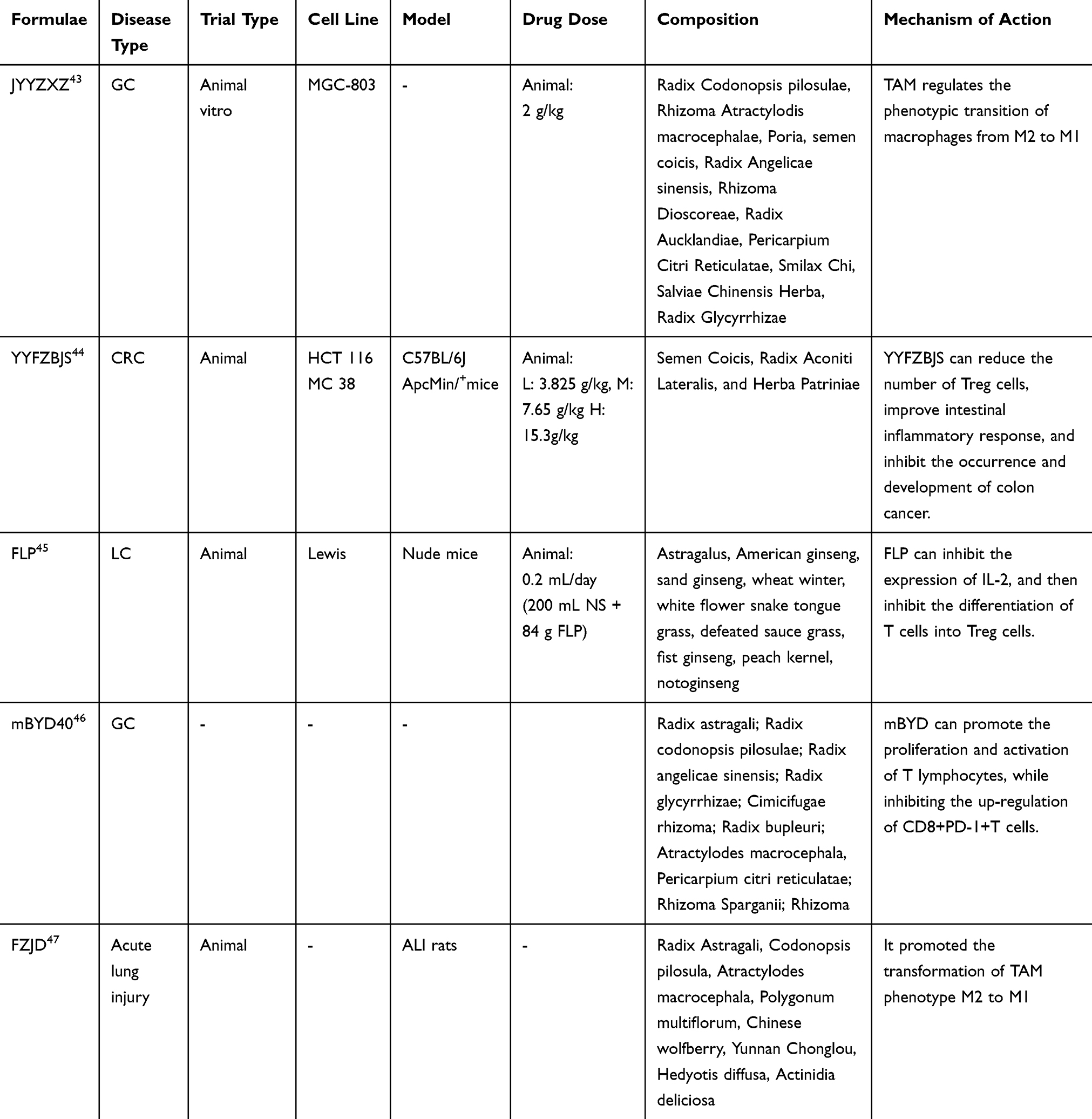 |
Table 2 TCM Formulae in Regulating Tumor Microenvironment |
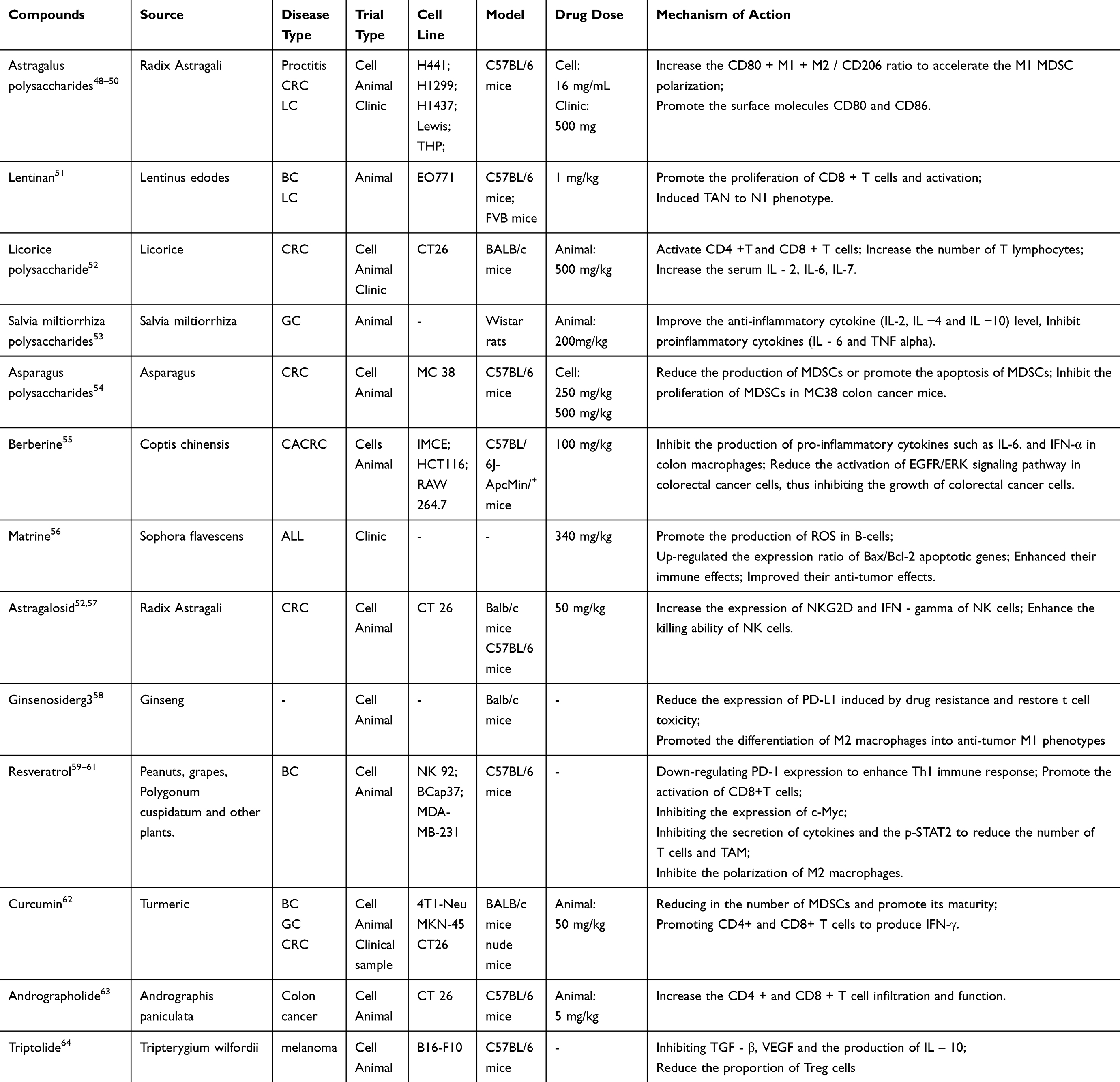 |
Table 3 Herbal Compounds in Regulating Tumor Microenvironment |
TCM Formulae
Jianpi Yangzhen Xiaozheng Decoction (JYYZXZ) Converts M2 Macrophages into M1 Macrophages
JYYZXZ is composed of Radix Codonopsis pilosulae, Rhizoma Atractylodis macrocephalae, Poria, semen coicis, Radix Angelicae sinensis, Rhizoma Dioscoreae, Radix Aucklandiae, Pericarpium Citri Reticulatae, Smilax Chi, Salviae Chinensis Herba, and Radix Glycyrrhizae. Sun et al analyzed the effects of JYYZXZ and its disassembled prescription on postoperative patients with gastric cancer. The results showed that JPYZXZ and its components could prevent the progression of gastric cancer. Compared with JPYZ (Radix Codonopsis pilosulae, Rhizoma Atractylodis macrocephalae, Poria, semen coicis, Radix Glycyrrhizae) and XZSJ (Radix Paeoniae Alba, Radix Angelicae sinensis, Rhizoma Dioscoreae, Pericarpium Citri Reticulatae, Smilax Chi, Salviae Chinensis Herba), JYYZXZ inhibits the Epithelial-Mesenchymal Transition (EMT) of gastric cancer more effectively, but JPYZ mainly regulated the phenotypic changes of macrophages from M2 subtype to M1 subtype.43
Fei Liu Ping (FLP) Inhibits the Differentiation of T Cells into Treg Cells
FLP is composed of astragalus, American ginseng, sand ginseng, wheat winter, white flower snake tongue grass, defeated sauce grass, fist ginseng, peach kernel, notoginseng. Fan et al discovered that FLP combined with cyclophosphamide chemotherapy reduced the proportion of localized Treg cells in the tumor and the expression of IL-2, which in turn inhibited the differentiation of T cells into Treg cells and immune escape of the tumor.45
Yi-Yi-Fu-Zi-Bai-Jiang-San (YYFZBJS) Reduced the Accumulation of CD4+CD25+Foxp3-Positive Treg Cells
YYFZBJS, as an important ancient formula, is mainly composed of Semen coicis, Radix Aconiti Lateralis, and Herba Patriniae. In intestinal adenomas, YYFZBJS can reduce the number of intestinal lymphatic vessels and mesenteric lymph nodes (MLN) and accumulate CD4+CD25+Foxp3-positive Treg cells, as well as improve the intestinal inflammatory response and inhibit the occurrence and development of colon cancer.44
mBYD40 Enhances the Cytotoxicity of T Cells
mBYD, composed of Radix astragali, Radix codonopsis pilosulae, Radix angelicae sinensis, Radix glycyrrhizae, Cimicifugae rhizome, Radix bupleuri, Atractylodes macrocephala, Pericarpium citri reticulatae, Rhizoma Sparganii and Rhizoma, has been shown to directly promote the proliferation, activation and cytotoxicity of T lymphocytes. Meanwhile, the upregulation rate of CD8+PD-1+T cells was decreased. In addition, this study confirmed that the PI3K/AKT pathway inhibited PD-L1 expression in gastric cancer tissues.46
Fu Zheng Jie Du Formula (FZJD) Reversed M2 Macrophage to M1 Macrophage
FZJD (Radix Astragali, Codonopsis pilosula, Atractylodes macrocephala, Polygonum multiflorum, Lycium barbarum, Yunnan leafy rhizome, tapeworm, and Aguta kiwifruit) not only reduced the expression of IL-10 and TGF- β, but also raised the ratio of iNOS/Arg2, which represents the ratio of M1/M2, which reversed TAM’s phenotype from M2 to M1 of TAM, thereby suppressing tumor cells.47
Herbal Compounds
Polysaccharides increase the number of T cells and the maturation of DCs, and promote conversion of MDSCs to M1 macrophages
Astragalus-contained herbs are commonly used in TCM. Its main components are astragalus polysaccharide (APS), astragalus polysaccharide glycoside (AS-IV) and flavonoids. APS is a water-soluble heteropolysaccharide composed of hexanedioic acid, glucose, galacturonic acid and glucuronic acid. It has various health benefits such as enhancing the immune system, modulating anti-tumor, anti-stress and antioxidant effects. Studies have shown that APS can increase the ratio of CD80+M1/CD206+M2, promote MDSCs polarization towards M1, and activate CTL to exert anti-tumor effects. In addition, APS prevented the recruitment of SDF-1 Treg cells through CXCR4/CXCL12 axis, activated the TLR4 signaling pathway, and reduced the number of Treg cells.48–50 Glycyrrhiza glabra is an important ingredient in many complementary and alternative medicine prescriptions, and is also commonly used in TCM for the treatment of various diseases. Licorice polysaccharide (Glycyrrhiza polysaccharide, GPS) is one of the main active components of licorice, which consists of rhamnose, glucan, arabinose and galactose.52 Recent studies have shown that Glycyrrhiza increased the expression ratio of CD3+CD8+ and CD3+CD4+T lymphocytes, promoted the maturation and phagocytosis of DCs, and enhance the cytokine production of IL-4 and IFN-γ.65 Lentinan (LNT), a kind of polysaccharides extracted from Lentinus edodes, has been widely used in clinic to enhance patients’ immunity. It was found to inhibit the growth of breast cancer and lung cancer, and promoted the proliferation and activation of CD8+ T cells and induced the polarization of TANs toward the N1 phenotype, resulting in an anti-tumor effect.51 He et al explored the mechanism of Salvia miltiorrhiza Bunge polysaccharides to improve the immune function of rats with gastric cancer. It was found that compared with the gastric cancer model group, Salvia miltiorrhiza Bunge polysaccharides enhanced the killing ability of NK cells and CTLs, increased the expression levels of IL-2, IL-4, IL-10, IgA, IgG and IgM in serum, and decreased the levels of IL-6 and TNF-α, which enhanced the immune function of rats with gastric cancer.53 Zhang et al found APS inhibited the migration, invasion and angiogenesis of HCC cells by down-regulating the HIF-1α/VEGF signaling pathway under normoxic conditions in vitro.54
Alkaloid inhibits the production of inflammatory factors and up-regulates apoptotic genes
A study on berberine for prevention and treatment of colitis-associated colorectal cancer (CACRC) found that berberine inhibits CACRC by inhibiting the production of pro-inflammatory cytokines (eg, IL-6 and IFN-α) in colon macrophages, leading to a reduced activation of the EGFR/ERK signaling pathway in colorectal cancer cells, and inhibited their proliferation.55 Matrine is a unique tetracyclic quinoline alkaloid derived from Robinia pseudoacacia with anti-inflammatory properties. Aghvami M et al found that it promoted the production of ROS in B-cells, up-regulated the expression ratio of Bax/Bcl-2 apoptotic genes, enhanced thier immune effects and improved thier anti-tumor effects.56
Glycosides Balance Th1/Th2 Ratio and Promote M1 Polarization
Astragalus saponin inhibited the proliferation of tumor cells, increased the protein levels of IL-12, IL-12R and pSTAT4, activated the IL-12/STAT4 pathway, increased the expression of IL-12, IL-12R and STAT4 genes, and thus induced the transformation of Th1/Th2 to Th1 cells.52 Xu et al also found that astragalus saponins inhibited M2 polarization of macrophages through the AMP-activated protein kinase (AMPK) signaling pathway, increased the proportion of M1 cells in TME, alleviated immunosuppression, and reduced the proliferation of lung cancer A549 cells and H1299 cells.57 In another study, ginsenosideRg3, an active ingredient of Radix Ginseng reduced drug resistance-induced PD-L1 expression, restored T-cell cytotoxicity, and inhibited proliferation and cisplatin resistance in A549/DDP cells. Moreover, Rg3 regulated the differentiation of pro-tumor M2 macrophages into the anti-tumor M1 phenotype when used in combination with chemotherapy.58
Phenols Enhance the Killing Ability of NK Cells and Reduce the Number of MDSCs
Phenolic compounds are widely found in the human diet and plant foods, and their use in human health has been extensively studied. Resveratrol is a plant-derived phytoantitoxin widely found in berries, peanuts, mulberries, grapes and other fruits. However, resveratrol attenuated CTL response to PD-L1, thereby preventing suppression and exhaustion of antitumor immunity.59 Another study showed that resveratrol induced mammalian target of rapamycin protein complex 2 (mTORC2)/Akt/cMyb signaling pathway to act on NK cells, which then exerted an anti-tumor effect.60 In addition, it was found that the activation of NK cells required the upregulation of c-Myb.60 In addition, resveratrol increased the expression of NKp30a, NKp30b and other ligands, which enhanced the cancer-killing ability of NK cells.61 Curcumin reduced the number of MDSCs, promoted their maturation, and facilitated the production of IFN-γ by CD4+T and CD8+T cells. In addition, curcumin inhibited the activation of Stat3 and NF-κB pathway (activation of Stat3 and NF-κB regulated the expression of anti-apoptotic, pro-proliferative, and immune response genes) and reduced the level of IL-6 in MDSCs, thus exerting anti-tumor effects.62
Other Compounds Involved in T Cell Activation and Inhibition of Pro-Inflammatory Factors
Yang et al found that the combination of Andrographolide with PD-1 inhibitors resulted in greater therapeutic efficacy in a mouse CT26 colon cancer xenograft model.63 Studies have shown that andrographolide combined with PD-1 blockade immunotherapy enhanced the infiltration of CD4+ and CD8+ T cells and co-activated T cell function.63 In addition, Andrographolide inhibited the expression of inflammation-related genes and limited the immunostimulatory activity of cells by inducing COX2 gene transcription to increase PGE2 production.63 Triptolide is a diterpene lactone with a variety of bioactive diterpene lactone extracted from the roots of Tripterygium wilfordii. It is the main active ingredient in preparations such as therapeutic rheumatoid tablets and wilfordii polyglucoside tablets. Triptolide inhibited the production of IL-2 and IFN- γ, as well as activation of Naïve T cells and effector T cells, such as Tregs. Triptolide-treated DCs have also been reported to down-regulate the expression of Th1 cells and inhibited the maturation and migration of DCs.64 In addition, studies have shown that glycyrrhizic acid (GL) and glycyrrhetinic acid (GA) modulated a variety of components involved in immune regulation and inflammation, such as inflammatory factor and acidophilic chemotactic protein secretion.66
Discussion
In 1889, Paget et at. first proposed the theory of “soil and seed”, which suggested that tumor cells are equivalent to “seeds”, and their unbridled proliferation is predicated on the need for “soil” with a suitable environment67. TME is a complex network of interactions that affect tumorigenesis and development. The significance of the immunosuppressive microenvironment lies in the fact that it can evade tumor-suppressing immune cells and molecules, escape immune surveillance, and promote the occurrence and development of tumor cells, and leaving the organism in a state of immunosuppression.68 Since entering the 21st century, tumor immunotherapy has achieved remarkable results, but through the actual feedback from clinicians and patients, it has been found that its adverse reactions and drug resistance may be an important factor affecting its long-term efficacy. A single therapeutic target may not be enough to prevent and treat tumor progression, but also requires the combined application of multiple targets. TCM can improve the tumor immunosuppressive microenvironment and the progression of chronic inflammation from various aspects.
The mechanism of immunotherapy is to activate immune cells by lifting the “braking” effect of the immune system, restarting and maintaining the “tumor-immunity” cycle, restoring the normal anti-tumor immune response of the body, and controlling the occurrence and development of tumors. it is common with the “holistic concept” of TCM. TCM is a systematic means of treatment, characterized by the combination of multiple targets and pathways. Currently, doctors believe that TCM works on both “seeds” and “soil”. The effects on tumor cells are mainly reflected in the following aspects: (1) Inhibiting tumor cell proliferation, inducing tumor cell differentiation and apoptosis. Among them, Lentinan is a potential drug expected to be used in clinic in the future51. (2) Reducing oncogene expression and inhibiting tumor angiogenesis. Among TCM compounds, Triptolide and Its derivatives have good therapeutic efficacy and deserve further study.64 (3) Reversing the drug resistance of tumor cells. Andrographolide and ginsenosideRg3 are able to sensitize cancer cells to immunotherapy and platinum drugs, respectively, indicating their combined application to enhance the efficiency and reduce the toxicity.58,63 The effects of TCM on TME are mainly manifested in two ways: to improving blood rheology index, activate blood circulation; and to improve the immune function and indirectly inhibit cancer cells.
Adjuvant alternative therapy is a form of medicine that combines TCM with other anti-tumor therapies to increase the sensitivity of tumor cells to radiotherapy, reduce adverse reactions, lower the risk of drug resistance and recurrence of tumors, and promote the reduction of toxicity and increase in efficacy. As we know, TCM is affordable, safe and reliable, and therefore favored by tumor patients. It helps reduce the economic burden of patients and is a widely accepted treatment option. However, according to the current literature review, the following problems still exist: 1) Most of the studies only verified the effects of TCM on immune cells, and the specific binding targets are not clarified. We can explore the mechanism of TCM intervention in TME from multiple perspectives and levels, such as protein expression, signal transduction, metabolomics, etc. 2) The effects of various TCM combinations/single formulas on immune cells tend to focus on T cells, MDSCs and DCs. However, the immune system includes innate and adaptive immunity. The body’s defense system consists of many cells, and there are interrelationships among these cells. Therefore, it is important to study other immune cells as well. 3) In most studies, the molecular mechanisms of the efficacy of TCM formulae remains largely unknow. 4) The research of TCM on TME has been based on basic research, with a low rate of translation of the results, and its clinical efficacy has not yet been further verified. In addition, although TCM formulae or single herb have been proven to bring benefits to patients, the time of benefit has not been tracked, which should also be the research focus in the future.
Abbreviations
TME, Tumor microenvironment; TCM, Traditional Chinese medicine; TAM, Tumor-associated macrophages; MDSCs, Myeloid-derived suppressor cells; TAN, Tumor-associated neutrophils; NK, Natural killer cells; DCs, Dendritic cells; VEGF, Endothelial growth factor; EGF, Epidermal growth factor; TGF-β, Transforming growth factor-β; PDGF, Platelet derived growth factor; PMN-MDSCs, Polymorphonuclear MDSCs; M-MDSC, Monocyte-like MDSC; ROS, Reactive oxygen species; MPO, Myeloperoxidase; IFN-β, Interferon-β; MMP-9, Matrix metalloproteinase-9; Th, Helper T cell; nTregs, Regulatory T cell; iTregs, Induced regulatory T cell; CTL, Cytotoxic T cell; Tm, Memory T cell; TCR, T cell receptor; TLSs, Tertiary lymphoid structures; PCs, Plasma cell; APS, Astragalus polysaccharide; LNT, Lentinan; CACRC, Colitis-associated colorectal cancer; AMPK, AMP-activated protein kinase; GC, Gastric cancer; CRC, colorectal cancer; LC, Lung cancer; ALL, acute lymphoblastic leukemia; BC, Breast cancer.
Funding
This work was supported by the National Natural Science Foundation of China (82122075, 82074232), Shanghai Pujiang Program (23PJ1412400), “Shu Guang” project supported by Shanghai Municipal Education Commission and Shanghai Education Development Foundation (21SG43), Shanghai Frontier Research Base of Disease and Syndrome Biology of Inflammatory Cancer Trans-formation (2021KJ03-12), Three-year Plan Project of Shanghai Traditional Chinese Medicine (ZY(2021-2023)-0208) and Shanghai Youth Talent Support Program.
Disclosure
The authors declare no conflict of interest, financial or otherwise.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Wang S, Long S, Wu W. Application of Traditional Chinese Medicines as Personalized Therapy in Human Cancers. Am J Chin Med. 2018;46(5):953–970. doi:10.1142/S0192415X18500507
3. Lin S, An X, Guo Y, et al. Meta-Analysis of Astragalus-Containing Traditional Chinese Medicine Combined With Chemotherapy for Colorectal Cancer: efficacy and Safety to Tumor Response. Front Oncol. 2019;9:749. doi:10.3389/fonc.2019.00749
4. Chesney J, Lewis KD, Kluger H, et al. Efficacy and safety of lifileucel, a one-time autologous tumor-infiltrating lymphocyte (TIL) cell therapy, in patients with advanced melanoma after progression on immune checkpoint inhibitors and targeted therapies: pooled analysis of consecutive cohorts of the C-144-01 study. J Immunother Cancer. 2022;10(12). doi:10.1136/jitc-2022-005755
5. Maio M, Ascierto PA, Manzyuk L, et al. Pembrolizumab in microsatellite instability high or mismatch repair deficient cancers: updated analysis from the Phase II KEYNOTE-158 study. Ann Oncol. 2022;33(9):929–938. doi:10.1016/j.annonc.2022.05.519
6. Diaz LA, Shiu KK, Kim TW, et al. Pembrolizumab versus chemotherapy for microsatellite instability-high or mismatch repair-deficient metastatic colorectal cancer (KEYNOTE-177): final analysis of a randomised, open-label, Phase 3 study. Lancet Oncol. 2022;23(5):659–670. doi:10.1016/S1470-2045(22)00197-8
7. Oh DY, Lee KH, Lee DW, et al. Gemcitabine and cisplatin plus durvalumab with or without tremelimumab in chemotherapy-naive patients with advanced biliary tract cancer: an open-label, single-centre, Phase 2 study. Lancet Gastroenterol Hepatol. 2022;7(6):522–532. doi:10.1016/S2468-1253(22)00043-7
8. Hiam-Galvez KJ, Allen BM, Spitzer MH. Systemic immunity in cancer. Nat Rev Cancer. 2021;21(6):345–359. doi:10.1038/s41568-021-00347-z
9. Miao K, Liu W, Xu J, et al. Harnessing the power of traditional Chinese medicine monomers and compound prescriptions to boost cancer immunotherapy. Front Immunol. 2023;14:1277243. doi:10.3389/fimmu.2023.1277243
10. Jia R, Liu N, Cai G, et al. Effect of PRM1201 Combined With Adjuvant Chemotherapy on Preventing Recurrence and Metastasis of Stage III Colon Cancer: a Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Front Oncol. 2021;11:618793. doi:10.3389/fonc.2021.618793
11. Lv B, Wang Y, Ma D, et al. Immunotherapy: reshape the Tumor Immune Microenvironment. Front Immunol. 2022;13:844142. doi:10.3389/fimmu.2022.844142
12. Russick J, Joubert PE, Gillard-Bocquet M, et al. Natural killer cells in the human lung tumor microenvironment display immune inhibitory functions. J Immunother Cancer. 2020;8(2):e001054. doi:10.1136/jitc-2020-001054
13. Gaggero S, Witt K, Carlsten M, et al. Cytokines Orchestrating the Natural Killer-Myeloid Cell Crosstalk in the Tumor Microenvironment: implications for Natural Killer Cell-Based Cancer Immunotherapy. Front Immunol. 2020;11:621225. doi:10.3389/fimmu.2020.621225
14. Güç E, Pollard JW. Redefining macrophage and neutrophil biology in the metastatic cascade. Immunity. 2021;54(5):885–902. doi:10.1016/j.immuni.2021.03.022
15. Yuan R, Li S, Geng H, et al. Reversing the polarization of tumor-associated macrophages inhibits tumor metastasis. Int Immunopharmacol. 2017;49:30–37. doi:10.1016/j.intimp.2017.05.014
16. Sabado RL, Balan S, Bhardwaj N. Dendritic cell-based immunotherapy. Cell Res. 2017;27(1):74–95. doi:10.1038/cr.2016.157
17. Kim MK, Kim J. Properties of immature and mature dendritic cells: phenotype, morphology, phagocytosis, and migration. RSC Adv. 2019;9(20):11230–11238. doi:10.1039/C9RA00818G
18. Mestrallet G, Sone K, Bhardwaj N. Strategies to overcome DC dysregulation in the tumor microenvironment. Front Immunol. 2022;13:980709. doi:10.3389/fimmu.2022.980709
19. Veglia F, Sanseviero E, Gabrilovich DI. Myeloid-derived suppressor cells in the era of increasing myeloid cell diversity. Nat Rev Immunol. 2021;21(8):485–498. doi:10.1038/s41577-020-00490-y
20. Wu Y, Yi M, Niu M, et al. Myeloid-derived suppressor cells: an emerging target for anticancer immunotherapy. Mol Cancer. 2022;21(1):184. doi:10.1186/s12943-022-01657-y
21. Li K, Shi H, Zhang B, et al. Myeloid-derived suppressor cells as immunosuppressive regulators and therapeutic targets in cancer. Signal Transduct Target Ther. 2021;6(1):362. doi:10.1038/s41392-021-00670-9
22. Grover A, Sanseviero E, Timosenko E, et al. Myeloid-Derived Suppressor Cells: a Propitious Road to Clinic. Cancer Discov. 2021;11(11):2693–2706. doi:10.1158/2159-8290.CD-21-0764
23. Gungabeesoon J, Gort-Freitas NA, Kiss M, et al. A neutrophil response linked to tumor control in immunotherapy. Cell. 2023;186(7):1448–1464.e20. doi:10.1016/j.cell.2023.02.032
24. Muqaku B, Pils D, Mader JC, et al. Neutrophil Extracellular Trap Formation Correlates with Favorable Overall Survival in High Grade Ovarian Cancer. Cancers. 2020;12(2):505. doi:10.3390/cancers12020505
25. Huo X, Li H, Li Z, et al. Transcriptomic profiles of tumor-associated neutrophils reveal prominent roles in enhancing angiogenesis in liver tumorigenesis in zebrafish. Sci Rep. 2019;9(1):1509. doi:10.1038/s41598-018-36605-8
26. Meitei HT, Lal G. T cell receptor signaling in the differentiation and plasticity of CD4(+) T cells. Cytokine Growth Factor Rev. 2023;69:14–27. doi:10.1016/j.cytogfr.2022.08.001
27. Borst J, Ahrends T, Bąbała N, et al. CD4(+) T cell help in cancer immunology and immunotherapy. Nat Rev Immunol. 2018;18(10):635–647. doi:10.1038/s41577-018-0044-0
28. Kang JH, Zappasodi R. Modulating Treg stability to improve cancer immunotherapy. Trends Cancer. 2023;9(11):911–927. doi:10.1016/j.trecan.2023.07.015
29. Nishikawa H, Koyama S. Mechanisms of regulatory T cell infiltration in tumors: implications for innovative immune precision therapies. J Immunother Cancer. 2021;9(7):456.
30. Li C, Jiang P, Wei S, et al. Regulatory T cells in tumor microenvironment: new mechanisms, potential therapeutic strategies and future prospects. Mol Cancer. 2020;19(1):116. doi:10.1186/s12943-020-01234-1
31. Zhou H, Wang Y, Xu H, et al. Noninvasive interrogation of CD8+ T cell effector function for monitoring early tumor responses to immunotherapy. J Clin Invest. 2022;132(16). doi:10.1172/JCI161065
32. Li Z, Chu Z, Yang J, et al. Immunogenic Cell Death Augmented by Manganese Zinc Sulfide Nanoparticles for Metastatic Melanoma Immunotherapy. ACS Nano. 2022;16(9):15471–15483. doi:10.1021/acsnano.2c08013
33. Chen B, Xiao L, Wang W, et al. Bi(2-x)Mn(x)O(3) Nanospheres Engaged Radiotherapy with Amplifying DNA Damage. ACS Appl Mater Interfaces. 2023;15(28):33903–33915. doi:10.1021/acsami.3c06838
34. Laumont CM, Banville AC, Gilardi M, et al. Tumour-infiltrating B cells: immunological mechanisms, clinical impact and therapeutic opportunities. Nat Rev Cancer. 2022;22(7):414–430. doi:10.1038/s41568-022-00466-1
35. Fridman WH, Meylan M, Petitprez F, et al. B cells and tertiary lymphoid structures as determinants of tumour immune contexture and clinical outcome. Nat Rev Clin Oncol. 2022;19(7):441–457. doi:10.1038/s41571-022-00619-z
36. Tokunaga R, Naseem M, Lo JH, et al. B cell and B cell-related pathways for novel cancer treatments. Cancer Treat Rev. 2019;73:10–19. doi:10.1016/j.ctrv.2018.12.001
37. Parekh A, Das S, Parida S, et al. Multi-nucleated cells use ROS to induce breast cancer chemo-resistance in vitro and in vivo. Oncogene. 2018;37(33):4546–4561. doi:10.1038/s41388-018-0272-6
38. Rosser EC, Mauri C. Regulatory B cells: origin, phenotype, and function. Immunity. 2015;42(4):607–612. doi:10.1016/j.immuni.2015.04.005
39. Catalán D, Mansilla MA, Ferrier A, et al. Immunosuppressive Mechanisms of Regulatory B Cells. Front Immunol. 2021;12:611795. doi:10.3389/fimmu.2021.611795
40. Youn BY, Kim JH, Jo YK, et al. Current Characteristics of Herbal Medicine Interventions for Cancer on Clinical Databases: a Cross-Sectional Study. Integr Cancer Ther. 2023;22:15347354231218255. doi:10.1177/15347354231218255
41. Park CR, Lee JS, Son CG, et al. A survey of herbal medicines as tumor microenvironment-modulating agents. Phytother Res. 2021;35(1):78–94. doi:10.1002/ptr.6784
42. Guo Q, Li J, Lin H. Effect and Molecular Mechanisms of Traditional Chinese Medicine on Regulating Tumor Immunosuppressive Microenvironment. Biomed Res Int. 2015;2015:261620. doi:10.1155/2015/261620
43. Wu J, Zhang XX, Zou X, et al. The effect of Jianpi Yangzheng Xiaozheng Decoction and its components on gastric cancer. J Ethnopharmacol. 2019;235:56–64. doi:10.1016/j.jep.2019.02.003
44. Sui H, Zhang L, Gu K, et al. YYFZBJS ameliorates colorectal cancer progression in Apc(Min/+) mice by remodeling gut microbiota and inhibiting regulatory T-cell generation. Cell Commun Signal. 2020;18(1):113. doi:10.1186/s12964-020-00596-9
45. Geng L, Lv J, Fan J. Effect of Fei-Liu-Ping ointment combined with cyclophosphamide on lung cancer cell proliferation and acidic microenvironment. Beijing Da Xue Xue Bao Yi Xue Ban. 2020;52(2):247–253. doi:10.19723/j.issn.1671-167X.2020.02.009
46. Xu R, Wu J, Zhang X, et al. Modified Bu-zhong-yi-qi decoction synergies with 5 fluorouracile to inhibits gastric cancer progress via PD-1/PD- L1-dependent T cell immunization. Pharmacol Res. 2020;152:104623. doi:10.1016/j.phrs.2019.104623
47. Lu Y, Wu Y, Huang M, et al. Fuzhengjiedu formula exerts protective effect against LPS-induced acute lung injury via gut-lung axis. Phytomedicine. 2024;123:155190. doi:10.1016/j.phymed.2023.155190
48. Bamodu OA, Kuo KT, Wang CH, et al. Astragalus polysaccharides (PG2) Enhances the M1 Polarization of Macrophages, Functional Maturation of Dendritic Cells, and T Cell-Mediated Anticancer Immune Responses in Patients with Lung Cancer. Nutrients. 2019;11(10). doi:10.3390/nu11102264
49. Sha W, Zhao B, Wei H, et al. Astragalus polysaccharide ameliorates vascular endothelial dysfunction by stimulating macrophage M2 polarization via potentiating Nrf2/HO-1 signaling pathway. Phytomedicine. 2023;112:154667. doi:10.1016/j.phymed.2023.154667
50. Tsao SM, Wu TC, Chen J, et al. Astragalus Polysaccharide Injection (PG2) Normalizes the Neutrophil-to-Lymphocyte Ratio in Patients with Advanced Lung Cancer Receiving Immunotherapy. Integr Cancer Ther. 2021;20:1534735421995256. doi:10.1177/1534735421995256
51. Xu H, Qi Z, Zhao Q, et al. Lentinan enhances the antitumor effects of Delta-like 1 via neutrophils. BMC Cancer. 2022;22(1):918. doi:10.1186/s12885-022-10011-w
52. Song W, Wang Y, Li G, et al. Modulating the gut microbiota is involved in the effect of low-molecular-weight Glycyrrhiza polysaccharide on immune function. Gut Microbes. 2023;15(2):2276814. doi:10.1080/19490976.2023.2276814
53. Wang N, Yang J, Lu J, et al. A polysaccharide from Salvia miltiorrhiza Bunge improves immune function in gastric cancer rats. Carbohydr Polym. 2014;111:47–55. doi:10.1016/j.carbpol.2014.04.061
54. Cheng W, Cheng Z, Weng L, et al. Asparagus Polysaccharide inhibits the Hypoxia-induced migration, invasion and angiogenesis of Hepatocellular Carcinoma Cells partly through regulating HIF1α/VEGF expression via MAPK and PI3K signaling pathway. J Cancer. 2021;12(13):3920–3929. doi:10.7150/jca.51407
55. Li D, Zhang Y, Liu K, et al. Berberine inhibits colitis-associated tumorigenesis via suppressing inflammatory responses and the consequent EGFR signaling-involved tumor cell growth. Lab Invest. 2017;97(11):1343–1353. doi:10.1038/labinvest.2017.71
56. Aghvami M, Ebrahimi F, Zarei MH, et al. Matrine Induction of ROS Mediated Apoptosis in Human ALL B-lymphocytes Via Mitochondrial Targeting. Asian Pac J Cancer Prev. 2018;19(2):555–560. doi:10.22034/APJCP.2018.19.2.555
57. Xu F, Cui WQ, Wei Y, et al. Astragaloside IV inhibits lung cancer progression and metastasis by modulating macrophage polarization through AMPK signaling. J Exp Clin Cancer Res. 2018;37(1):207. doi:10.1186/s13046-018-0878-0
58. Zhu Y, Wang A, Zhang S, et al. Paclitaxel-loaded ginsenoside Rg3 liposomes for drug-resistant cancer therapy by dual targeting of the tumor microenvironment and cancer cells. J Adv Res. 2023;49:159–173. doi:10.1016/j.jare.2022.09.007
59. Verdura S, Cuyàs E, Cortada E, et al. Resveratrol targets PD-L1 glycosylation and dimerization to enhance antitumor T-cell immunity. Aging. 2020;12(1):8–34. doi:10.18632/aging.102646
60. Lee YJ, Kim J. Resveratrol Activates Natural Killer Cells through Akt- and mTORC2-Mediated c-Myb Upregulation. Int J Mol Sci. 2020;21(24):9575. doi:10.3390/ijms21249575
61. Lee Y, Shin H, Kim J. In vivo Anti-Cancer Effects of Resveratrol Mediated by NK Cell Activation. J Innate Immun. 2021;13(2):94–106. doi:10.1159/000510315
62. Lee J, Han Y, Wang W, et al. Phytochemicals in Cancer Immune Checkpoint Inhibitor Therapy. Biomolecules. 2021;11(8):1107. doi:10.3390/biom11081107
63. Liu W, Fan T, Li M, et al. Andrographolide potentiates PD-1 blockade immunotherapy by inhibiting COX2-mediated PGE2 release. Int Immunopharmacol. 2020;81:106206. doi:10.1016/j.intimp.2020.106206
64. Noel P, Von Hoff DD, Saluja AK, et al. Triptolide and Its Derivatives as Cancer Therapies. Trends Pharmacol Sci. 2019;40(5):327–341. doi:10.1016/j.tips.2019.03.002
65. Wu Y, Zhou H, Wei K, et al. Structure of a new glycyrrhiza polysaccharide and its immunomodulatory activity. Front Immunol. 2022;13:1007186. doi:10.3389/fimmu.2022.1007186
66. Richard SA. Exploring the Pivotal Immunomodulatory and Anti-Inflammatory Potentials of Glycyrrhizic and Glycyrrhetinic Acids. Mediators Inflamm. 2021;2021:6699560. doi:10.1155/2021/6699560
67. Paget S. The distribution of secondary growths in cancer of the breast. 1889. Cancer Metastasis Rev. 1989;8(2):98–101.
68. Zhang Y, Han X, Nie G. Responsive and activable nanomedicines for remodeling the tumor microenvironment. Nat Protoc. 2021;16(1):405–430. doi:10.1038/s41596-020-00421-0
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.