Back to Journals » Drug Design, Development and Therapy » Volume 15
Toxicities and Associated Factors in Patients Receiving Temozolomide-Containing Regimens: A 12-Year Analysis of Hospital Data
Authors Shi C, Wang X, Diao C, Zhu H, Yuan Q, Liu J, Li S, Gu M, Zhang Y
Received 7 February 2021
Accepted for publication 3 May 2021
Published 20 May 2021 Volume 2021:15 Pages 2151—2159
DOI https://doi.org/10.2147/DDDT.S305792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Chen Shi,1,2 Xiong Wang,1,2 Changdong Diao,1,2 Haixia Zhu,1,2 Qi Yuan,1,2 Jinmei Liu,1,2 Shijun Li,1,2 Ming Gu,1,2 Yu Zhang1,2
1Department of Pharmacy, Union Hospital, Tongji Medical College, Huazhong University of Science & Technology (HUST), Wuhan, People’s Republic of China; 2Hubei Province Clinical Research Center for Precision Medicine for Critical Illness, Wuhan, 430022, People’s Republic of China
Correspondence: Ming Gu; Yu Zhang
Department of Pharmacy, Union Hospital, Tongji Medical College, Huazhong University of Science & Technology (HUST), Wuhan, People’s Republic of China
Email [email protected]; [email protected]
Objective: Although temozolomide has been extensively used to treat various tumors, there is a lack of large-cohort studies on temozolomide’s toxicity profile. The toxicity profiles and associated factors in patients treated with temozolomide-containing regimens were analyzed.
Patients and Methods: Patients treated with temozolomide-containing regimens in the Affiliated Union Hospital of Huazhong University of Science and Technology from January 2008 to December 2019 were included. A retrospective analysis of the clinical data of patients treated with temozolomide-containing regimens was performed. Univariate chi-square test and multivariate logistic regression analysis were employed to identify factors associated with the occurrence of toxicities.
Results: Among the 1057 patients received temozolomide-containing regimens, 922 patients were included in our analyses. Of the 922 patients, 484 patients (52.5%) experienced toxicities. Univariate analysis revealed that radiotherapy, chemotherapy cycle, chemotherapy regimen, and clinical stage were significantly associated with the toxicity during temozolomide treatment (P < 0.05). The chemotherapy regimen, chemotherapy cycle, and clinical stage were significantly associated with the overall occurrence of toxicities (P < 0.05). A chemotherapy regimen, chemotherapy cycle, and clinical stage were associated with the hematological system’s toxicities, whereas gender, age, clinical diagnosis, and clinical stage were related to gastrointestinal toxicities (P < 0.05). Clinical diagnosis, chemotherapy regimen, and age were associated with liver toxicity (P < 0.05).
Conclusion: Toxicities are common among patients receiving temozolomide-containing regimens. Clinicians should be aware of factors associated with toxicities to minimize the impact of the toxicity.
Keywords: temozolomide, toxicity, hematological system, gastrointestinal system, liver toxicity
Introduction
Temozolomide is an imidazotetrazine derivative and a second-generation alkylating agent with antitumor effects. Orally administered temozolomide capsules are fully absorbed and well distributed in tissues; hence, the drug crosses the blood-brain barrier resulting in predictable adverse reactions.1 Temozolomide’s toxic profile and side effects are relatively mild and tolerable in patients receiving six or more cycles of treatment.2 Temozolomide has been associated with anemia, lymphopenia, neutropenia, and severe thrombocytopenia.2 In clinical practice, temozolomide has been extensively used to treat glioma, non-small cell lung cancer, leukemia, melanoma, lymphoma, and certain solid tumors. Among other chemotherapeutics, temozolomide provides the most potent antitumor effects in glioblastoma.3 In China, temozolomide has been on the market for nearly 20 years. Due to its sound curative effects in glioma patients, temozolomide has become the first-line treatment for malignant brain tumors.4,5
Temozolomide’s efficacy and therapeutic regimen have been extensively studied in various tumors.6–11 However, there is a lack of large-cohort studies on the toxicity profile of temozolomide. In this study, we retrospectively analyzed clinical data in patients treated with temozolomide in our hospital during the past 12 years. The in-depth analysis of the temozolomide-related toxicities can guide the clinical use of temozolomide to prevent toxicities.
Methods
Study Population
This study was approved by the Ethics Committee of Union Hospital of Tongji Medical College of Huazhong University of Science and Technology (reference number: 2019-S893). This retrospective study analyzed the toxicity profiles of cancer patients treated with temozolomide-containing regimens from January 1, 2008, to December 31, 2019, at the Union Hospital of Tongji Medical College of Huazhong University of Science and Technology. The hospital is a 5000 - bed comprehensive university teaching hospital in Wuhan, a megacity in China. The exclusion criteria were 1) patients with poor treatment adherence (irregular use, discontinuation or change of medication), which might have affected the evaluation of temozolomide’s safety and efficacy, and 2) patients with incomplete data.
Study Design
A “Temozolomide Safety Reassessment Research Card” was designed to collect demographic data, medication status, and toxicity occurrence. Additional information gathered included Karnofsky Performance Status Scale (KPS scale), body-mass index (BMI), drug manufacturer, radiotherapy, chemotherapy cycle, chemotherapy regimen, clinical diagnosis, and clinical tumor stage. Data were retrieved from the hospital electronic health records (EHR).
Chemotherapy regimens were divided into five categories: (1) concurrent chemoradiotherapy with adjuvant chemotherapy (usually six cycles of adjuvant chemotherapy with temozolomide alone); (2) mono-chemotherapy (only temozolomide); (3) combined chemotherapy with two drugs (temozolomide combined with capecitabine, cisplatin, irinotecan, apatinib, bevacizumab, recombinant human endostatin, gemcitabine, methotrexate, or rituximab); (4) complex chemotherapy regimen, including multidrug chemotherapy involving three or more drugs and concurrent chemoradiotherapy followed by combined chemotherapy; (5) adjuvant chemotherapy after radiotherapy. In this analysis, the chemotherapy cycle was regarded as the total cycle number with clear examination results during the patient’s hospitalization. Usually, temozolomide was used for five days in a cycle, and each cycle lasted for 28 days. However, in concurrent chemoradiotherapy, temozolomide was employed for 42 consecutive days, and this was regarded as one chemotherapy cycle due to the continuous use of temozolomide in concurrent chemoradiotherapy.
The severity of toxicities was assessed based on the Common Terminology Criteria for Adverse Events (CTCAE) v4.0.12 The CTCAE displays Grades 1 through 5 with unique clinical descriptions of severity for each adverse event. Grade 1- mild: asymptomatic or mild symptoms; clinical or diagnostic observations only; intervention not indicated. Grade 2 - moderate: minimal, local, or noninvasive intervention indicated; limiting age-appropriate instrumental activities of daily living (ADL). Grade 3 - severe or medically significant but not immediately life-threatening: hospitalization or prolongation of hospitalization indicated; disabling; limiting self-care ADL. Grade 4 - life-threatening consequences; urgent intervention indicated. Grade 5 - death related to an adverse event.
Statistical Analysis
Data were recorded using Microsoft Excel®, and SPSS 25.0 was used for statistical analyses. Normally distributed data were expressed as means ± standard deviation (SD), whereas categorical data were expressed as percentages. The chi-square test was used to compare groups, and the influencing factors were analyzed by multivariate logistic regression analysis. Significant factors in univariate analysis were used in multivariate logistic regression analysis. P-values < 0.05 were considered statistically significant.
Results
Characteristics of Patients and Analysis of Toxicities
A total of 1057 patients were treated with temozolomide-containing regimens within the analysis period, and 922 met the inclusion and exclusion criteria. Among the 922 patients, 558 were males, and the average age was 45.25 years (ranged from 1 to 93 years). Toxicities were reported in 484 of the 922 patients, with an overall toxicity rate of 52.5% (Table 1).
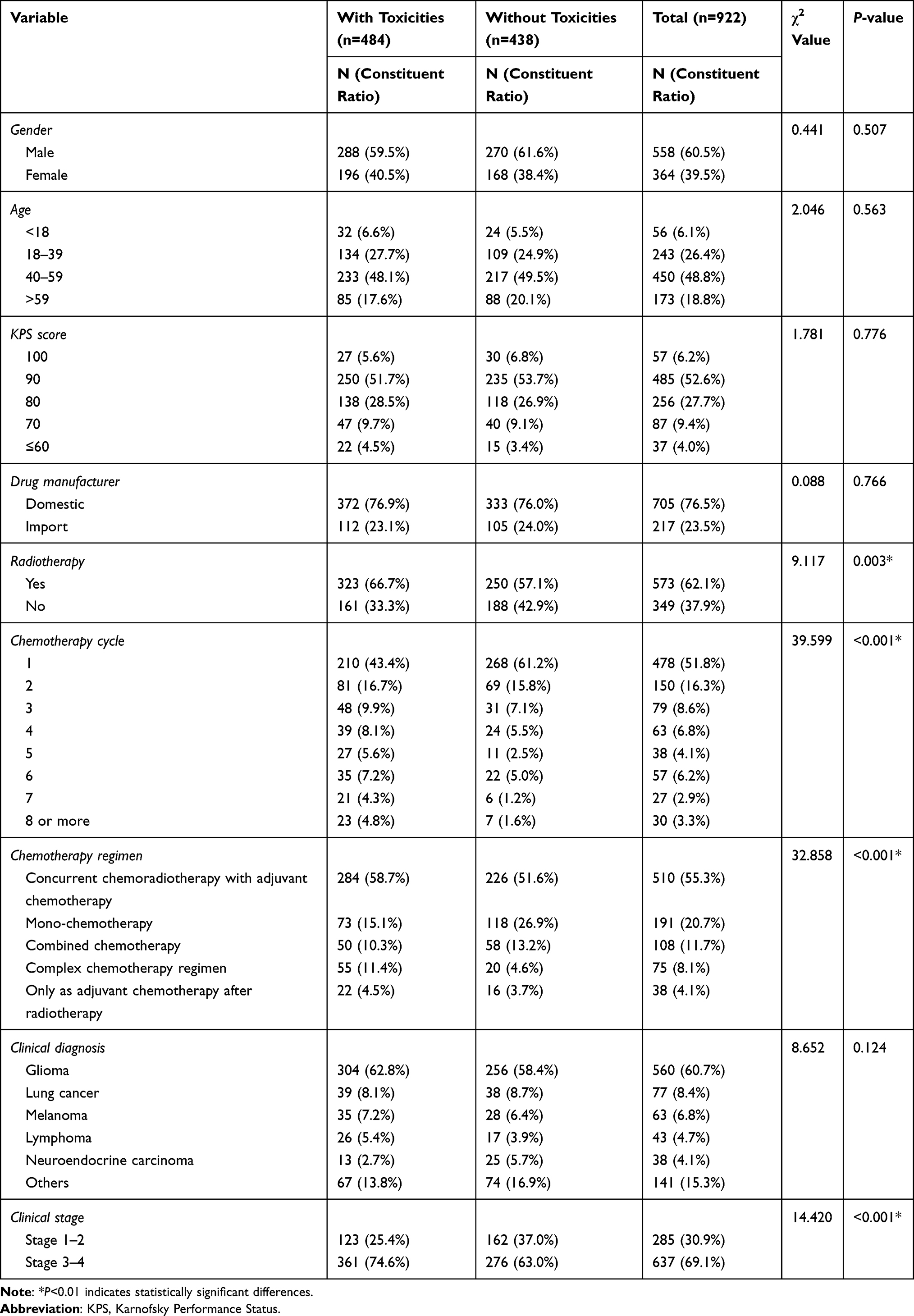 |
Table 1 Univariate Analysis of Factors Affecting the Overall Occurrence of Toxicities |
As a retrospective study, we have observed differences in the dosage of temozolomide in different chemotherapy regimens. Concurrent chemoradiotherapy is 75mg/m2/d for 42 days (some patients do not use it for 42 days, and some patients only use temozolomide from Monday to Friday each week), and this was regarded as one chemotherapy cycle due to the continuous use of temozolomide in concurrent chemoradiotherapy. In the adjuvant treatment period or in combination with other chemotherapy regimens, the dosage of temozolomide is usually 150mg/m2/d or 200mg/m2/d for 5 days, and each cycle lasted for 28 days. Different temozolomide-containing regimens in our study were listed in Supplemental Table 1.
A total of 787 toxic cases were recorded in patients treated with temozolomide-containing regimens. The most common cases involved the hematological system (34.9%, 275/787), followed by the gastrointestinal system (24.8%, 195/787) (Supplemental Table 2). When cases were analyzed based on chemotherapy regimens, the concurrent chemoradiotherapy with adjuvant chemotherapy accounted the most, 55.3% (435/787), followed by temozolomide mono-therapy (17%, 134/787) (Table 2).
 |
Table 2 Different Chemotherapy Regimens and the Associated Toxicities |
Among the 922 patients who were treated with temozolomide, 183 patients concurrently received other chemotherapeutic agents. The toxicity occurrence based on the concurrent drugs used in more than ten patients is listed in Table 3. The most common combination drug used was capecitabine (31.7%, 58/183), followed by cisplatin (23.5%, 43/183).
 |
Table 3 Occurrence of Toxicities in Combined Temozolomide Chemotherapy |
Among the 922 patients analyzed, 285 (30.9%) were classified as clinical stages 1–2, and 637 (69.1%) as stages 3–4. The occurrence of toxicities in patients with different clinical diagnoses and at different stages is listed in Table 4. In patients at clinical stages of 1 and 2, patients with glioma (n = 192) experienced the highest rate of toxicities (47.9%, 92/192), followed by patients with lymphoma (46.7%, 7/15). This pattern was also observed in patients at clinical stages 3 and 4, patients with glioma (n = 368) had the highest rate of toxicities (77.7%, 286/368), followed by patients with lymphoma (67.9%, 19/28). The rates of toxicity occurrence were higher in stages 3–4 than stages 1–2 regardless of cancer types. Due to the large gap in the number of toxicity occurrence of different severities, no statistically significant factors affecting toxicity severity are identified.
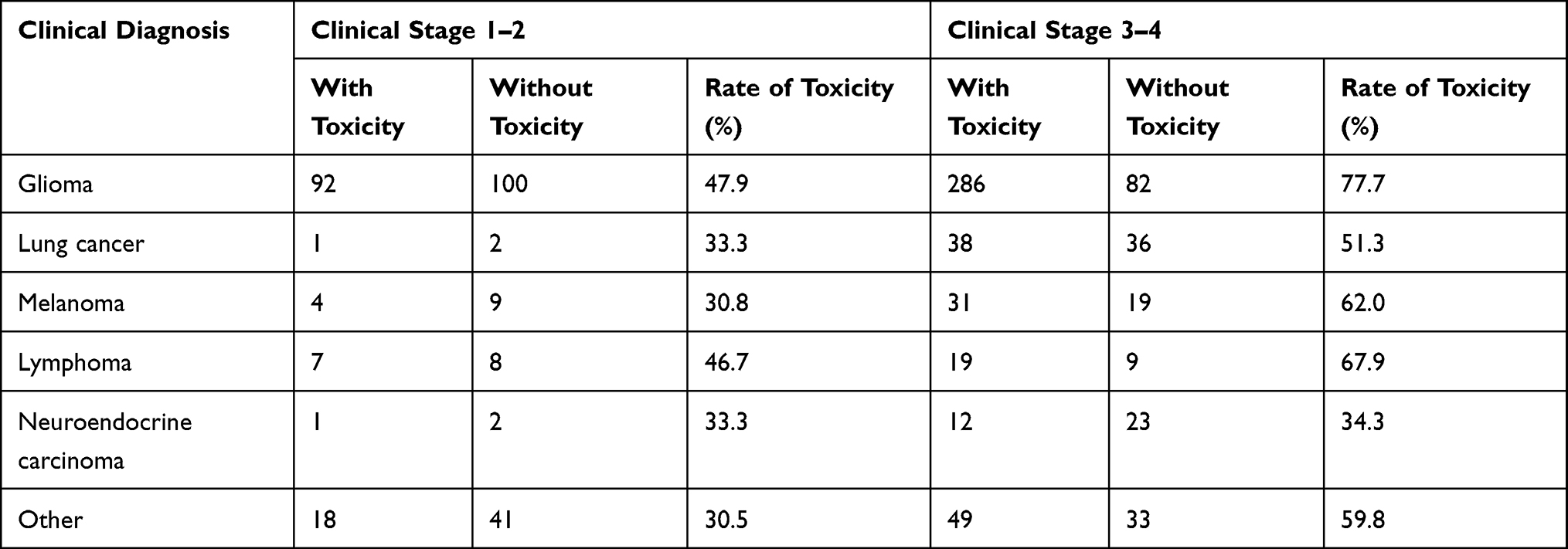 |
Table 4 Occurrence of Toxicities at Different Clinical Tumor Stages |
The case toxicity severities were assessed using the CTCAE rating scale. A total of 726 cases (92.2%) were rated at grades 1–2, and 61 (7.8%) were rated grade 3 or above. Within the grades 1–2 categories, the hematological system accounted for 249 cases (34.3%, 249/726), followed by the gastrointestinal system (25.9%, 188/726). Within the grades 3 or above category, the hematological system accounted for the most, 26 cases (42.6%, 26/61), followed by the other type (37.7%, 23/61) (Table 5).
 |
Table 5 Severity of Toxicity |
Factors Affecting the Toxicity Occurrence of Temozolomide-Containing Regimens
Univariate analysis indicates that radiotherapy, chemotherapy cycle, chemotherapy regimen, and clinical stage were significant factors affecting the toxicity occurrence (P < 0.05) (Table 1). Among the 922 patients, 616 had BMI recorded in EHR. Univariate analysis revealed that BMI was not associated with the overall toxicity occurrence (P = 0.082) (Supplemental Table 3).
The variables that showed statistical significance in univariate analysis were used as independent variables in logistic multivariate regression analysis. The overall toxicity and toxicities in the hematological system, gastrointestinal system, and liver were used as dependent variables. A chemotherapy regimen, chemotherapy cycle, and clinical stage were identified as factors significantly affecting the overall occurrence of toxicity (P<0.05) (Table 6).
 |
Table 6 Multivariate Analysis of Factors Affecting the Overall Occurrence of Toxicities |
A chemotherapy regimen, chemotherapy cycle, and clinical stage were identified as factors significantly affecting the occurrence of toxicities in the hematological system (P<0.05) (Supplemental Table 4). Gender, age, clinical diagnosis, and clinical stage were factors significantly associated with toxicity in the gastrointestinal system (P<0.05) (Supplemental Table 5). Clinical diagnosis, chemotherapy regimen, and age were factors significantly affecting the occurrence of toxicity in the liver (P<0.05) (Supplemental Table 6).
Among the 922 cases, 21 cases were observed to be active discontinuation of the drug, except for 3 cases due to economic reasons and 1 case due to switching chemotherapy regimens, the other 17 cases were reported in Supplemental Table 7. It can be observed that of the 17 cases of discontinuation, 16 cases of discontinuation occurred in the first cycle, and only 1 case occurred in the third cycle. 13 cases of drug discontinuation occurred during concurrent radiotherapy and chemotherapy. 7 cases continued to complete the treatment of temozolomide after the toxicity was reduced or disappeared. 5 cases of drug discontinuation indicated related hematological system toxicity, 5 cases of drug discontinuation indicated related gastrointestinal system toxicity, 4 cases of drug discontinuation accompanied with liver injury. Multiple toxicity were also observed in 7 cases occurred in the first chemotherapy cycle. Cases of multiple toxicity were analyzed based on chemotherapy regimens, the concurrent chemoradiotherapy with adjuvant chemotherapy accounted the most, 57.1% (4/7), followed by combined chemotherapy (28.6%, 2/7) and temozolomide mono-therapy (14.3%, 1/7).(Supplemental Table 7).
Discussion
This retrospective analysis reveals that in patients receiving temozolomide-containing regimens, the toxicity occurrence rate is high, around 50%. A chemotherapy regimen, chemotherapy cycle, and clinical stage are significant factors affecting the overall toxicity occurrence. Factors affecting the toxicity occurrence varies among organ systems.
Evaluation of Toxicity Occurred in the Combination Therapy
When combined with the orally-administered chemotherapeutic agent capecitabine, the toxicity rate in temozolomide-treated patients is 25.9% (15/58), lower than that of patients receiving temozolomide mono-chemotherapy (38.2%, 73/191). However, why the combination of temozolomide with capecitabine has a favorable safety profile remains unclear. The combination of temozolomide with injectable chemotherapeutics increases the toxicity rate occurrence except for the combination with bevacizumab, which exhibits a comparable rate to temozolomide mono-chemotherapy.
Evaluation of Factors Associated with Temozolomide-Containing Therapies
A chemotherapy regimen and chemotherapy cycle are significant factors affecting the overall toxicity occurrence. The risk of toxicity in complex chemotherapy regimens and concurrent chemoradiotherapy with adjuvant chemotherapy is 4.06 and 3.37 times higher than that of temozolomide mono-chemotherapy. Hematological toxicity incidence was 275/922 (29.8%) and only 26/922 (2.8%) for grade 3 or higher. Gastrointestinal system toxicity incidence was 195/922 (21.3%), and only 7/922 of grade 3 or higher. Abnormal liver function incidence was 139 of 922 (15.1%), and the incidence of grade 3 or higher toxicity was only 5 of 922 (0.5%). Results of retrospective analysis revealed that the chemotherapy regimen containing temozolomide was found to be safe with a low overall incidence of grade 3 or 4 toxicity.
The toxicity of different chemotherapy regimens containing temozolomide was also investigated in other studies. Brada reported that incidences of grade 3–4 hematological and grade 3–4 non-hematological toxicity in the temozolomide monotherapy for glioblastoma were the same as 25%.13 Chua reported a higher incidences of grade 3–4 hematological toxicity (36.4%) and grade 3–4 non-hematological toxicity (40.9%) in chemotherapy regimens containing temozolomide.14 However, a low incidence of toxicity in the temozolomide monotherapy for glioblastoma was also reported that the incidence of grade 3–4 hematological toxicity was 2.4% and no grade 3–4 non-hematological toxicity was observed.15 It should be noted that the toxicity evaluations were based on the specific chemotherapy regimens.
Notably, patients receiving more treatment cycles exhibit a significantly higher rate of toxicity occurrence. In patients receiving temozolomide for eight cycles or above, the risk is 4.04 times higher than patients receiving one treatment cycle (P < 0.05). The risk of toxicity in patients at clinical stages 1–2 is only 0.56 times higher than that of patients at stages 3–4 (P < 0.001). Interestingly, the factors affecting the toxicity occurrence varies among different organ systems.
A chemotherapy regimen, chemotherapy cycle, and clinical stage are significant factors affecting the hematological system’s toxicity. In patients undergoing concurrent chemoradiotherapy with adjuvant chemotherapy, adjuvant chemotherapy after radiotherapy, and complex chemotherapy, the risk of toxicity is 6.42, 5.31, and 4.79 times higher, respectively, than patients receiving mono-chemotherapy (P < 0.05). A study on the risks of toxicity in patients receiving temozolomide-containing regimens for glioma treatment also indicates a higher risk of concurrent chemoradiotherapy with adjuvant chemotherapy than mono-chemotherapy.16 The number of chemotherapy cycles is also associated with the risk of toxicity. Importantly, patients receiving temozolomide for eight cycles or above exhibit a six times higher toxicity rate than patients receiving one cycle (P < 0.05). Gender is not a significant factor associated with the risk of hematological toxicity occurrence in our analysis. This is different from a retrospective analysis of 680 patients with malignant glioma, which reveals that temozolomide’s hematological toxicity is higher in women than in men.14 This discrepancy could be attributed to the fact that we included all cancer patients treated with temozolomide, not just glioma patients. The risk of hematological toxicities in patients at clinical stages 1–2 is only 0.64 times higher than that in patients at stages 3–4 (P < 0.05).
Clinical diagnosis, clinical stage, gender, and age are significant factors affecting the gastrointestinal system’s toxicity occurrence. In lung cancer patients, the risk of the gastrointestinal system toxicity is 6.2 times higher than that in patients with neuroendocrine tumors (P < 0.01). The risk of gastrointestinal toxicity in patients at clinical stages 1–2 is only 0.59 times higher than that in patients at stages 3–4 (P < 0.05). Our analysis is consistent with another study, which indicates that the risk of gastrointestinal toxicity is 1.88 times higher in women than in men (P < 0.01).17
Clinical diagnosis, chemotherapy regimen, and age are significant factors contributing to treatment-related liver dysfunction. The risk of abnormal liver function in lymphoma patients is 6.01 times higher than that in patients with neuroendocrine tumors (P < 0.05). The risk of liver toxicity in patients undergoing concurrent chemoradiotherapy with adjuvant chemotherapy, complex chemotherapy, and combined chemotherapy is 6.75, 4.33, and 3.37 times higher, respectively, compared with the risk in patients receiving temozolomide mono-chemotherapy (P < 0.05). The risk of liver dysfunction in patients under 18 is only 0.09 times higher than that in patients aged over 59 (P < 0.05). Notably, out of 56 patients aged under 18, only one patient (1.79%) exhibited liver toxicity instead of the 15.1% overall incidence of treatment-related liver dysfunction.
Our study analyzed patients who received temozolomide-containing regimens over 12 years using data from real-world clinical practice. The findings may help clinicians better design temozolomide-containing chemotherapies and monitor at-risk patients to develop treatment-related toxicities. The study has the following limitations 1) the analysis is a single-center study, and 2) the study is retrospective in nature. We did not assess the clinical outcome of the patients.
Conclusion
In patients treated with temozolomide-containing regimens, toxicities present commonly in the hematological and gastrointestinal systems and the liver. Clinicians should pay particular attention to the significant factors associated with the toxicity occurrence, such as the chemotherapy regimen, chemotherapy cycle, and the patient’s clinical stage.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Union Hospital of Tongji Medical College of Huazhong University of Science and Technology (reference number: 2019-S893). The requirement for informed consent was waived by the ethics committee due to the retrospective nature of the study. The patient data that was collected will be treated with confidentiality and in compliance with Declaration of Helsinki.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 82073402) and National Key Research and Development Plan of China (2017YFC0909900).
Disclosure
All authors declare that they have no conflicts of interest.
References
1. Friedman HS, Kerby T, Calvert H. Temozolomide and treatment of malignant glioma. Clin Cancer Res. 2000;6(7):2585–2597.
2. Grieco A, Tafuri MA, Biolato M, et al. Severe cholestatic hepatitis due to temozolomide: anadverse drug effect to keep in mind. Case report and review of literature. Medicine(Baltimore). 2015;94(12):e476. doi:10.1097/MD.0000000000000476
3. He J, Ch H. Research progress on resistance mechanism of temozolomide in treatment of glioblastoma(in Chinese). Chin J Mod Appl Pharm. 2019;36(23):3001–3007. doi:10.13748/j.cnki.issn1007-7693.2019.23.024
4. Niu XD, Ma DW, Tian HL, et al. Efficacy of temozolomide versus traditional Chemotherap- -eutic drugs in the treatment of glioma: a systematic review(in Chinese). J Int Neuro Neurosurg. 2014;41(1):1–6.
5. Bai Y, Chen Y, Hong X, et al. Newcastle disease virus enhances the growth-inhibiting and proapoptotic effects of temozolomide on glioblastoma cells in vitro and in vivo. Sci Rep. 2018;8(1):11470. doi:10.1038/s41598-018-29929-y
6. Roger S, Monika EH, Warren PM, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised Phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10(5):459–466. doi:10.1016/S1470-2045(09)70025-7
7. Sastre-Gallego S, Fernández-Lizarbe E, Martín-Sánchez M, et al. EP-1204: limited margin radiotherapy and temozolomide for glioblastoma multiforme: pattern of failure. Radiother Oncol. 2018;127:S671. doi:10.1016/S0167-8140(18)31514-7
8. Silke BN, Gabi S, Hendrik B, et al. Temozolomide during radiotherapy of glioblastoma Multiforme:Dailyadministration improves survival. Strahlenther Onkol. 2017;193(11):890–896. doi:10.1007/s00066-017-1110-4
9. Wee CW, Kim E, Kim TM, et al. Impact of interim progression during the surgery-to-radiotherapy interval and its predictors in glioblastoma treated with temozolomide-based radiochemotherapy. J Neurooncol. 2017;134(1):169–175. doi:10.1007/s11060-017-2505-x
10. Brachman DG, Wang M, Ashby LS, et al. Phase II Trial of Temozolomide (TMZ), Motexafin Gadolinium (MGd), and 60 Gy Fractionated Radiation (RT) for Newly Diagnosed Supratentorial Glioblastoma (GBM): results of RTOG 0513. Int J Radiat Oncol Bio Phys. 2011;81(2):S129–S130. doi:10.1016/j.ijrobp.2011.06.267
11. Brada M, Stenning S, Gabe R, et al. Temozolomide versus procarbazine, lomustine, and vincristine in recurrent high-grade glioma. J Clin Oncol. 2010;28(30):4601–4608. doi:10.1200/JCO.2009.27.1932
12. CTCAE v4.0, Common terminology criteria for adverse events [EB/OL]; 2011. Available from: http://www.calgb.org/Public/meetings/presentations/2009/summer_group/cra_cont_ed/06a_CTCAE-Setser_062009.pdf.
13. Brada M, Hoang-Xuan K, Rampling R, et al. Multicenter phase II trial of temozolomide in patients with glioblastoma multiforme at first relapse. Ann Oncol. 2001;12(2):259–266. doi:10.1023/a:1008382516636
14. Chua SL, Rosenthal MA, Wong SS, et al. Phase 2 study of temozolomide and Caelyx in patients with recurrent glioblastoma multiforme. Neuro Oncol. 2004;6(1):38–43. doi:10.1215/S1152851703000188
15. Brandes AA, Ermani M, Basso U, et al. Temozolomide in patients with glioblastoma at second relapse after fifirst line nitrosourea-procarbazine failure: a phase II study. Oncol. 2002;63(1):38–41. doi:10.1159/000065718
16. Zhou B, Mao Q, Wang P, et al. The Adverse Effects Analysis of Temozolomide in Glioma Chemotherapy(in Chinese). Chin J Neurooncol. 2012;10(1):14–18.
17. Armstrong TS, Cao Y, Scheurer ME, et al. Risk analysis of severe myelotoxicity with temozolomide: the effects of clinical and genetic factors. Neuro Oncol. 2009;11(6):825–832. doi:10.1215/15228517-2008-120
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.