Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Towards a Sub-Acute Cardiorespiratory Physiotherapy Service Within a Hospital-at-Home Model: A Descriptive Qualitative Study
Authors Pereira E, Taylor G, Johnston KN
Received 14 March 2026
Accepted for publication 11 June 2026
Published 22 June 2026 Volume 2026:19 606364
DOI https://doi.org/10.2147/JMDH.S606364
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Elisio Pereira,1– 3 Grant Taylor,4 Kylie N Johnston1
1School of Allied Health and Human Performance, Adelaide University, Adelaide, South Australia, Australia; 2School of Health and Biomedical Sciences, RMIT University, Melbourne, Victoria, Australia; 3Shanghai University of Health and Medical Sciences, Shanghai, People’s Republic of China; 4PhysioWest, Adelaide, South Australia, Australia
Correspondence: Elisio Pereira, School of Allied Health and Human Performance, Adelaide University, Adelaide, South Australia, Australia, Email [email protected]
Purpose: To identify the perceived needs of healthcare providers prior to the implementation of a physiotherapy-led sub-acute home-care service integrated into an existing home hospital service (HSS) in South Australia.
Patients and Methods: A qualitative descriptive study was conducted using semi-structured interviews with one HHS management representative and seven private practice physiotherapists in South Australia. Data were analysed using qualitative content analysis, and findings were reported in accordance with the Consolidated Criteria for Reporting Qualitative Research COREQ guidelines.
Results: Participants identified uncertainty regarding patient selection, referral criteria, and role of physiotherapy within the HHS. Physiotherapists reported limited recent experience in community-based cardiorespiratory practice and expressed concerns related to perceived clinical risk in the home setting despite recognition that HHS patients are generally clinically stable. Willingness to engage with the service varied and was influenced by professional interest, operational feasibility, workload integration and clarity of governance structures. Key implementation needs include targeted training, clinical protocols, access to equipment, supervision, and streamlined documentation systems.
Conclusion: Successful integration of physiotherapy into HHS requires clear referral logic, role definition, and alignment with private practice operational realities. Future research should evaluate post-implementation outcomes, patient perspectives, and refined referral criteria in order to inform scalable physiotherapy-inclusive HHS models.
Keywords: early discharge, hospital in the home, home-care physiotherapy
Introduction
Prolonged hospitalisation represents a substantial financial burden the healthcare system1 and is associated with adverse patient outcomes.2,3 In Australia, public and private hospitals accounted for approximately 40% of the total national health expenditure in 2021–22, amounting to 96 billion.4 Extended hospitalisation also increases the risk of hospital-acquired complications (eg., pneumonia, sepsis), prolonged length of hospital stay, functional decline, and mortality.2,3
Home hospital services (HHS) have been developed as an alternative model of care that delivers hospital-level treatment within a person’s home.5 These services typically include vital sign monitoring, diagnostic testing, medication prescription and administration (including intravenous therapies), advanced life support and face-to-face or virtual clinical review by physicians and nurses.2,6 HHS models have been shown to support early discharge, improve patient outcomes, reduce long-term care admissions and decrease the overall health system costs.2,6
Internationally, hospital-at-home models have expanded as alternatives to inpatient care for selected patients requiring acute or sub-acute management.5 While these models commonly emphasise medical and nursing governance, monitoring, diagnostics, and escalation processes, the role of allied health professionals is less consistently described.2,6 Physiotherapy may be particularly relevant for patients experiencing functional decline, breathlessness-related activity limitation, secretion retention, post-operative mobility limitations, or deconditioning. However, safe integration of physiotherapy into HHS requires more than evidence of potential clinical benefit. It also requires attention to workforce capability, professional role clarity, referral criteria, escalation pathways, and compatibility with the local service model.2,6
In South Australia, one such HHS model is delivered by a private hospital and provides treatment for conditions, such as infections, exacerbations of respiratory disease, heart failure, gastrointestinal conditions, and postoperative care. The service is predominantly nurse-led with limited input from other health professionals. The hospital is currently exploring the expansion of this service through collaboration with a local private physiotherapy practice in Adelaide, which already provides home-based rehabilitation for musculoskeletal conditions under a separate model of care. The proposed expansion would involve incorporating physiotherapists into HHS to support the management of postoperative patients and individuals with chronic cardiorespiratory conditions. However, most physiotherapists in partnering practice have musculoskeletal-focused training, and there is limited understanding of the equipment, clinical competencies, and training required to safely deliver physiotherapy within a subacute home hospital context.
Although previous research has explored health professionals’ perceptions of HHS,7–9 there is a lack of evidence addressing local implementation needs and profession-specific requirements in the South Australian context. To address this gap, the present study sought to establish a framework for integrating physiotherapy into the existing HHS model. By capturing the perspectives of hospital management and physiotherapists from the partnering private practice, this examined how physiotherapists could contribute to the care of individuals requiring postoperative or subacute cardiorespiratory management in their homes.
Therefore, this study aimed to identify the perceived needs of healthcare providers, hospital management, and private practice-based physiotherapists prior to the potential implementation of a physiotherapy-led subacute home-care service for people with cardiorespiratory and/or post-surgical conditions in Adelaide, South Australia.
Materials and Methods
This qualitative descriptive study was approved by the University of South Australia Human Research Ethics Committee (Application ID 206469, approved 9/12/2024) and reported according to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.10
The research team consisted of (a) two physiotherapists with PhD qualifications and extensive experience in acute, subacute, and community cardiorespiratory physiotherapy (EP and KJ). Both researchers have previously undertaken qualitative research and are skilled in interview techniques, data coding, and content analysis; and (b) one physiotherapist with clinical experience in musculoskeletal physiotherapy and professional expertise in business models integrating private practice and hospital services (GT).
Given the prior professional relationships between some members of the research team and the clinic, reflexivity was considered throughout the study. EP had previously worked at the clinic but ceased employment approximately 18 months before data collection. GT was the clinic director but did not conduct interviews or lead coding of staff interviews. KJ had no prior clinical relationship with the clinic. Independent coding, consensus discussions, and the use of direct participant quotations were employed to support analytic rigour and minimise the influence of researcher assumptions.
Methodological Framework
Qualitative description was selected as the methodological approach because it supports an exploration of the phenomenon in its natural context and avoids imposing interpretive or theoretical structures on participants’ accounts.11,12 This approach is well-suited to the aims of the study, which sought to generate a clear and pragmatic summary of the “facts of the case in everyday terms”.12,13 By emphasising low-inference interpretation, qualitative description enabled us to focus on stakeholders’ perspectives of the proposed sub-acute physiotherapy home hospital service (HHS), rather than developing abstract concepts or theorising meaning. Consistent with this methodology, findings were presented using language that remained close to participants’ own words and the surface of events.11–13
Participant Recruitment
For this descriptive study, we adopted a purposive sampling approach, whereby participants were intentionally selected based on their anticipated ability to provide information relevant to the planned implementation of a physiotherapy-integrated home hospital service (HHS). We initially recruited a private hospital representative who was responsible for HHS management. This allowed the research team to gain a clearer understanding of what the planned service would look like and what the private hospital would require at the clinic. Secondly, we sought to recruit all physiotherapists at the clinic who had been or could potentially be involved in HHS services. These included clinicians from a range of career stages and different periods of employment with the clinic, who were likely to have personal knowledge and direct experience of the needs of healthcare providers prior to the potential implementation of the sub-acute physiotherapy HHS. This purposive approach ensured representation of the key stakeholder groups most directly involved in the planning and potential delivery of the proposed service.
For participant recruitment, GT contacted the HHS manager to seek approval to share their Email address with the broader research team. The physiotherapists’ Email addresses were obtained from their professional public pages on the clinic website. An invitation to participate in the research was then sent by EP to target participants via email, detailing the background of the research project, study aims, anonymity, data management, and process for informed consent. Written consent, which included publication of anonymised responses/direct quotes, was provided by all participants via reply to the invitation Email prior to data collection. Interested participants contacted EP to arrange a time and date for the online interview, and they were sent a survey link with the participant information sheet to collect informed consent and demographic characteristics (eg., age and years of practice).
Sample adequacy was considered using the concept of information power. As the study addressed a narrow and applied research question, participants were selected because of their direct involvement in the existing or proposed service, and the sample was highly specific to the implementation context. Consistent with information power principles, a relatively small sample was therefore considered sufficient to generate meaningful insights relevant to local service planning.11,12
Data Collection
Individual online interviews were conducted using EP and planned for 30 min. The facilitators and participants were the only individuals present in the interviews. A semi-structured guide (Supplemental Material 1) for the physiotherapist interviews was developed based on the aims of the study to explore their needs prior to the implementation of sub-acute HHS. The guide was piloted with a PhD candidate in Health Sciences (ET) who had previous experience conducting interviews and qualitative research. The HHS representative was purposefully interviewed first with questions exploring current HHS eligibility criteria, referral sources, service delivery processes, allied health referral pathways, perceived role of physiotherapy and anticipated requirements for implementing physiotherapy within the service, as this would provide further details on the proposed HHS. Following feedback from the pilot session and the HHS interview, a semi-structured guide was adapted with specific questions and prompts. The physiotherapist interview guide included questions about participants’ previous exposure to HHS and cardiorespiratory physiotherapy, perceived preparedness to manage post-operative and cardiorespiratory patients at home, perceived clinical and operational concerns, training and supervision needs, equipment and resource requirements, documentation processes, and anticipated integration with existing clinic-based workloads. The interviews were then audio recorded.
Data Analysis
Demographic data were descriptively summarised. Transcripts were read multiple times. Condensed meaning units are highlighted in the transcripts. Open coding was conducted by assigning labels to condensed meaning units identified in the data.14 Codes were organised into subcategories and main categories, with direct quotations aligned with each subcategory provided as examples.14 The one HHS management representative interview was independently analysed first (meaning units, codes and preliminary categories).14 Next, the seven physio staff interviews were independently analysed. Analysis was subsequently combined using categories and sub-categories common to both.
Content analysis was conducted independently by two investigators (KJ and EP) for trustworthiness purposes.15 Preliminary sub-categories and categories identified were highly similar between reviewers.14,15 Category and subcategory labels were refined, and final analysis agreed on through discussion with consensus achieved.14,15 Coding was primarily inductive, with codes generated directly from the data rather than from a pre-existing theoretical framework. Meaning units relevant to the study aim were identified, condensed and assigned open codes. Similar codes were grouped into subcategories, which were then organised into broader descriptive categories. Consistent with qualitative description, categories were developed to provide a pragmatic summary of participants’ perspectives rather than generate abstract theoretical interpretations.14,15
Several strategies were used to enhance trustworthiness.14,15 Credibility was supported through independent coding by two researchers, discussion of coding decisions and use of direct quotations. Dependability was supported through a documented analytic process moving from meaning units to codes, subcategories and categories. Transferability was supported through detailed description of the service context, participant groups and local implementation setting.
Results
Participants represented two stakeholder groups: one HHS management representative from the private hospital service and seven physiotherapists (five men/two women) from the partnering private practice. All physiotherapists worked in private practice, identified musculoskeletal/sports physiotherapy as their primary area of practice, and varied in career stage from recent graduate to experienced clinician (median of 2.8 years of experience ranging from three months to nine years). Prior exposure of physiotherapist to the HHS physiotherapy was limited, with only two participants having previously seen a small number of HHS patients and six reporting no recent community-based cardiorespiratory physiotherapy experience. Content analysis resulted in six main categories of data, each with several subcategories (Table 1). Consistent with the study aim, the descriptive categories generated through content analysis were subsequently examined to identify the underlying implementation needs reflected within participants’ accounts (Table 1).
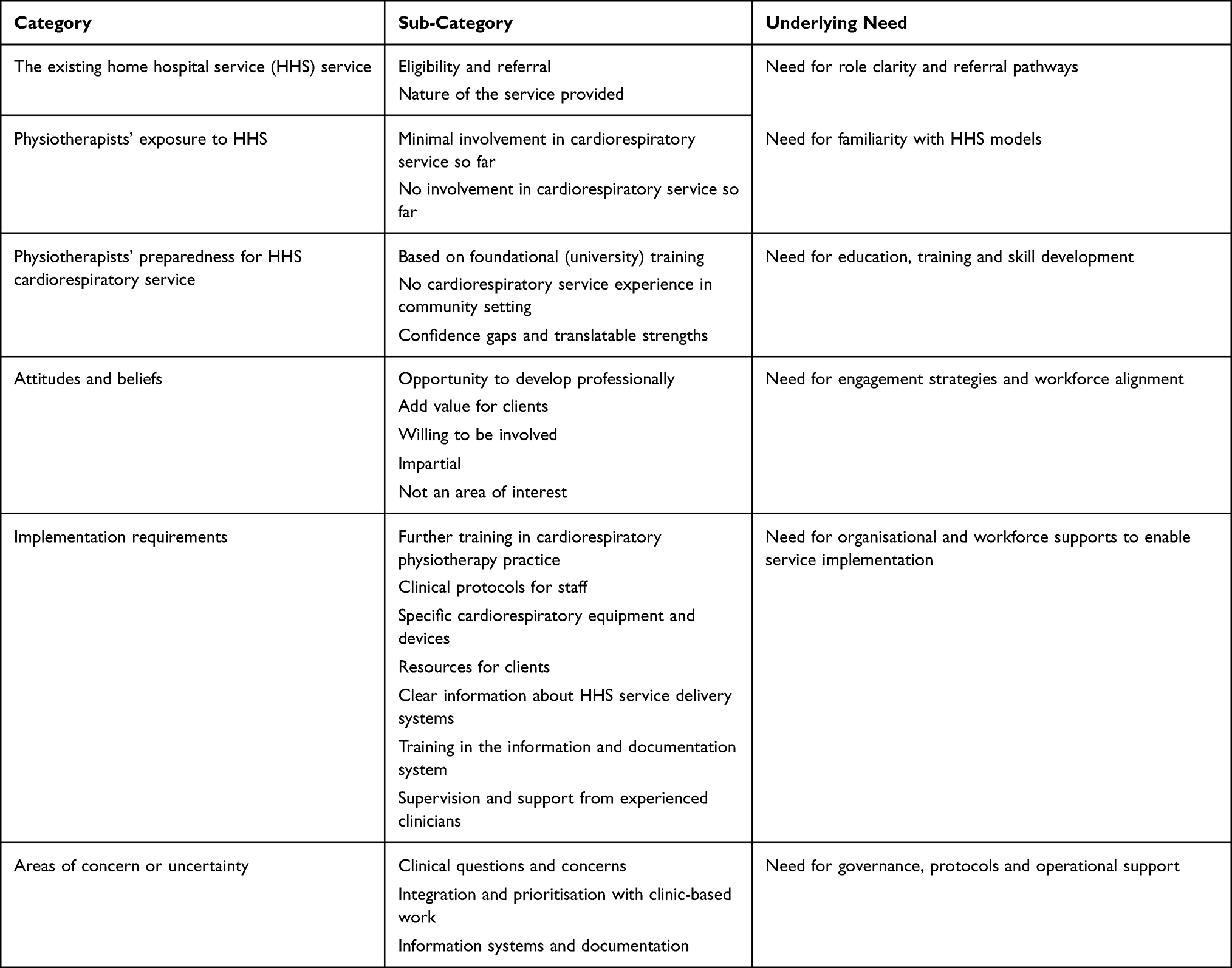 |
Table 1 Data Categories and Subcategories |
The Existing HHS: Need for Role Clarity and Referral Pathways
The HHS management representative spoke about eligibility for patients entering the existing HHS service (Medicare eligible, patients already safe to go home) and referral sources – ie., paramedics, general practitioners, private care centres, hospital and emergency department and registered nurses in aged care facilities. In-home service was mostly provided 1–4 times a day for usually 3–4 days by nursing and other providers, with delivery of equipment and consumables including medication by courier. The remote service included virtual monitoring of vital signs, and phone/video consultations by medical and nursing staff. Once in the service, doctors provided a referral for allied health if required. A private practice physiotherapist would see the patient within 24 hours (by the next working day). Referrals for HHS physiotherapy services had been mostly for people following orthopaedic surgical procedures, with only a few for people with cardiorespiratory conditions.
Now we service up to 150 different diagnostic groups…. branching out to a lot of planned surgeries, working with an orthopaedic surgeon and doing some potential day surgery cases. Then with physios available for an assessment, which we do on admission anyway we then put the referral. Physio can go out the following day to see them as well. There’s research out there that people heal so much better. They heal quicker. They recover quicker in their own environment. if we can get physio in their home and monitor their pain and I think they have a better outcome. M1
I can only probably recall maybe one there may have been two for the chest physio. We wait for those referrals to come from the doctor. And I suppose if the patient wasn’t recovering, what do we need, you know? And then I suppose it would be a referral to physios. M1
Physiotherapists’ Exposure to the HHS: Need for Familiarity with HHS and Cardiorespiratory Service Delivery
Physiotherapy staff had either minimal or no involvement with providing cardiorespiratory services through the HHS service. Those with minimal involvement had seen a few (three or less) clients for conditions of pneumonia or deconditioning. Documentation of the services provided had taken the form of a written letter.
I saw him two or three times in the first three or four days P1
so they do write a report after they’ve reviewed a patient, and we upload that report into the patient’s file M1
Physiotherapists’ Preparedness for HHS Cardiorespiratory Service: Need for Workforce Capability Development
Physiotherapists had a foundational level of knowledge and skill in cardiorespiratory practice gained from their university training. This provided them with sound basics, but they had not practiced or kept up with developments in the area since then.
I remember the basics from uni(versity) like airway clearance, breathing techniques, mobility with shortness of breath but I haven’t used those skills much since then P3
Most of the cardiorespiratory patients seen previously had been in the hospital, not community, setting. Physiotherapists recognised cardiorespiratory physiotherapy was not their usual area of practice, compared with high familiarity with exercise, musculoskeletal and sports fields. They expressed confidence with managing non-complicated cardiorespiratory cases. While not yet fully confident in all areas (deep knowledge and skills, techniques, devices), existing ability to “think on your feet” (P7) in home visit situations was valued.
I’ve always been more confident with exercise type stuff, so I’d want to refresh my knowledge of respiratory techniques P5
I wouldn’t feel confident managing more complex things or knowing what devices are available for home care P3
Attitudes and Beliefs About Providing Cardiorespiratory Service: Need for Workforce Engagement and Role Alignment
Some participants regarded providing cardiorespiratory services through HHS as an opportunity to develop professionally, to enjoy the challenge of learning new skills, see different presentations, and gain valuable experience.
I think it would be a really good learning opportunity for me, and it makes sense to build those skills early in my career P3
Cardiorespiratory practice could add value to the services that physiotherapists provided to clients, integrating with existing expertise.
I think it definitely plays a role and it can often intertwine with other medical conditions. P1
The HHS management representative expressed potential value for their clients from cardiorespiratory physiotherapy.
So I suppose what would I like to see? I would probably like to say see a shorter length of stay.I would like to see …an increased positive experience for the patient, like feeling better quicker M1
Some participants were impartial, willing to take part in this new role. Others indicated it was not an area of interest for them.
I think if the service is going to run, it should probably be done by people who are actually interested in that area. I don’t think forcing it across the board makes sense. P4
Implementation Requirements: Need for Organisational, Educational and Resource Supports to Enable Implementation
The management representative expressed interest in what the upskilling physiotherapists would need to implement the service. Physiotherapists expressed a need for further training in cardiorespiratory physiotherapy practice, including knowledge of clinical presentations, skills, interventions, devices; hands on experience; work shadowing opportunities; and training (eg., simulation) for managing deteriorating patients/emergency situations. Clinical protocols and guidelines for conditions, equipment and emergency procedures were needed.
some structured training or maybe a set of guidelines for common conditions what to look for, red flags, when to escalate that would really help. I think structured sessions on assessment and treatment of common respiratory issues like airway clearance, oxygen monitoring, safe exercise prescription. Also, maybe simulation training for emergencies, like what to do if someone desat(urate)s suddenly. P5
Access to specific cardiorespiratory equipment and devices, and the process for obtaining these, were needed to prepare for the service, along with resources for clients (eg., about exercise, devices and information) specific to cardiorespiratory physiotherapy. Physiotherapists needed clear information about HHS service delivery arrangements and expectations, for themselves and to communicate with clients, and training in the documentation systems. Supervision from a physiotherapist experienced in the field at least initially, and in some cases, ongoing support (someone to call if needed) was expressed as a need.
I’d just want to know that I had enough support to not feel out of my depth. ….As a new grad physio, I’d really like having someone I could check in with like a senior physio to call if I was unsure P3
Areas of Concern or Uncertainty: Need for Governance, Risk Management and Operational Clarity
Concerns related to implementation were raised in three interrelated areas: clinical questions, integration with clinic-based work, and information systems and documentation. There was a lack of clarity about the medical stability of clients who would be seen by physiotherapists in the HHS service. Participants had concerns about how to proceed if clients deteriorated (emergency procedures and possible transfer to hospital setting) and timing of HHS physiotherapy to deliver effective care and prevent deconditioning or deterioration.
if they’re discharged from hospital, you’d think they’d be stable enough I suppose. But if an emergency happens while we’re there we need to know what to do. P1
it’s the logistics of driving as well. Of getting the allied health there. So I think …if a patient urgently needed a physio review, that’s where us as a virtual hospital would have to weigh up the pros and cons and do we need to up transfer them to a hospital if they’re not safe? M1
I think at the end of the day like if they were quite unwell then they’d be sitting in a bricks and mortar hospital and that’s probably why you gonna see probably a lot more of your chest physio coming into that space. M1
The management representative expressed interest in evidence and criteria about which clients would benefit from cardiorespiratory physiotherapy in this service.
Just like some general points of these sort of type of people with these co-morbidities …because I’m just thinking …probably last month I had quite a few …. sitting on a long length of stay that we just couldn’t wean the oxygen. Well maybe …going out there doing better chest physio or/and educating that patient on some deep breathing exercise. The community nurses that go out there they probably like me, have that basic nursing assessment to say, hey, practise your deep breathing. You know, if you’re feeling short of breath, stop, sit down. ….but it’s not the same as a physio coming in and giving that …bit more education. M1
Another clinical question raised was options for care on discharge from the HHS service. Concerns around integration of HHS visits with clinic-based physiotherapist workload were raised by most participants. Fitting HHS clients in to be seen with less than 24 hours’ notice, to meet HHS service delivery expectations and client needs, would be a challenge and require flexibility and changes to the current physiotherapy practice diary system. For some, this potentially clashed with their preference for seeing clinic-based clients and for others it was an acceptable situation.
That would be challenging but doable if it’s planned. If it’s too last-minute, it might clash with existing bookings. P6
But if the service is a priority, I think we’d just have to find ways to make space maybe swapping some patients around or blocking a slot for urgent cases. P5
If you are on the road you don’t have that availability for clients in the clinic, and particularly if that’s a therapist preference to be seeing those sort of clients in the clinic it’s then harder to build and maintain a list if you’re out on the road half the day. P2
Concern was expressed regarding learning a new system for information access and documentation; learning and staying familiar with the systems if the volume of clients was relatively low, extra work and complexity involved. For some this was a source of frustration and others felt it could work if it was well organised, time was allocated and training provided.
I’d be a bit concerned about the portal and filling in notes… I suppose it would be a difficult learning process to learn a whole new software system and note system just for this smaller subset of clients we see. P1
Discussion
This study explored perceived needs and considerations prior to the implementation of a physiotherapy-led sub-acute home-care service within an existing home hospital service (HHS). The findings highlight several interrelated challenges and enablers relevant to the integration of physiotherapy into predominantly nurse-led HHS models, including uncertainty regarding patient selection and referral processes, perceptions of clinical risk in the home setting, and the feasibility of delivering such services within a private practice context. Hospital management and physiotherapists recognised potential value in physiotherapy input but lacked shared operational frameworks to support consistent and confident practice. Interpreting these perspectives together provides insight into how clinical, professional and organisational factors intersect when extending physiotherapy practice into sub-acute home hospital care.
Physiotherapy Value, Referral Criteria and Patient Selection in HHS
HHS models are increasingly adopted internationally as alternatives to inpatient care, with robust evidence demonstrating comparable or improved outcomes for selected patient populations when compared with conventional hospitalization.16,17 However, the role of allied health, and physiotherapy in particular, remains inconsistently defined within these models. Much of the existing literature focuses on medical and nursing components, with physiotherapy often positioned as an adjunct rather than an integrated element of care.16,17
Findings from this study suggest that uncertainty about the value of physiotherapy does not arise from scepticism but from a lack of operational clarity regarding which patients benefit and when referral should occur. Whilst there was expressed interest in patient improved recovery and reduced length of stay from the HHS management, it lacked explicit criteria for identifying appropriate referrals, particularly for cardiorespiratory presentations. This mirrors broader implementation literature indicating that unclear role definition and referral pathways are key barriers to allied health integration in novel care models.18
Clarifying patient selection is therefore central to translating perceived benefit into practice. Evidence from early supported discharge and home-based rehabilitation suggests that physiotherapy is most beneficial for patients with functional decline, mobility limitation, breathlessness-related activity restriction or deconditioning following acute illness.16,19 Applying these principles to HHS requires explicit articulation of referral triggers, rather than reliance on individual clinician judgement. Without such clarity, physiotherapy referrals may become reactive,17,18 infrequently utilised18 or reserved for orthopaedic cases, as observed in the HHS explored in the present study. Establishing shared referral logic across medical, nursing and physiotherapy stakeholders may therefore be a foundational step in embedding physiotherapy as a meaningful contributor to HHS rather than an optional add-on.
Perceived Patient Risk in an HHS Context
A key aspect identified in this study was the apparent contradiction between eligibility for home hospital care, implying clinical stability, and physiotherapists’ concerns regarding deterioration and emergency management in the home. Although HHS patients are selected on the basis that their care can be safely delivered at home, physiotherapists expressed uncertainty about escalation processes and their responsibilities should a patient’s condition worsen, which may be a reflection of professional identity and clinical training. Physiotherapists trained in inpatient environments may implicitly associate “hospital care” with higher acuity, and the term “hospital in the home” may therefore inherit symbolic risk despite a different clinical reality.7,8,18 Limited exposure to community-based cardiorespiratory physiotherapy during university training further intensifies this uncertainty, particularly when clinicians are unfamiliar with home-based monitoring, escalation pathways and shared governance arrangements.
The perceived risk described by physiotherapists may therefore reflect not only the objective acuity of HHS patients but also the symbolic meaning of “hospital-level care” being delivered in a non-hospital environment. For clinicians whose recent professional identity has been shaped by musculoskeletal private practice, the proposed model requires a shift from familiar clinic-based assessment and treatment towards shared responsibility for patients with recent acute illness, cardiorespiratory symptoms, monitoring needs, and potential deterioration.7,8,18 This may explain why participants requested not only clinical training but also clear escalation pathways, senior support and role boundaries.
Implementation research in virtual and home hospital models suggests that such concerns are common during early adoption phases and can be mitigated through clear escalation protocols, defined clinical boundaries and access to senior support.20,21 Addressing perceived risk through governance and support structures may therefore be as important as clinical upskilling in building physiotherapist confidence and engagement with the HHS model.
Implementation Implications
Beyond clinical considerations, feasibility emerged as a major determinant of physiotherapists’ willingness to engage with the HHS service. Participants described competing priorities between routine existing activities, such as clinic-based care and home visits, particularly when referrals required rapid response, travel time and diary flexibility. Additionally, documentation and information systems emerged as potential barriers, with concerns about learning new platforms for a small caseload. These challenges are well recognised in studies examining integration of community-based services into private practice contexts, where workload balance and documentation burden significantly influence clinician engagement and sustainability.22,23 Operational design of the HHS must account for the reality of the private practice, including protected capacity for home visits, geographic planning and streamlined documentation processes. Piloting the service with a defined cohort and agreed outcome measures such as acceptability, feasibility, and clinician confidence would enable iterative refinement of the program, consistent with contemporary implementation frameworks.24
Interest in participation varied across clinicians. Some physiotherapists viewed involvement as an opportunity for skill development and professional growth, while others expressed neutrality or lack of interest, reflecting differences in professional identity, career stage and perceived alignment with the private practice. These findings suggest that implementation strategies should not assume universal participation. Targeted staffing models, where interested clinicians receive dedicated training, protected capacity and ongoing support, may be more sustainable than distributing HHS responsibilities across all staff.22,25 Such approaches align with broader evidence indicating that clinician engagement is strongest when new roles are voluntary, supported and congruent with existing professional practice.25,26
Participants consistently identified the need for structured preparation prior to implementation, including targeted training in cardiorespiratory physiotherapy, access to appropriate equipment, and clear clinical protocols. Supervision and access to experienced clinicians were identified as particularly important, especially for less experienced physiotherapists. Evidence from early supported discharge and home-based rehabilitation programs indicates that clinician preparedness and clarity of scope are essential to ensuring safety and effectiveness in non-hospital settings.6,19,27 Implementation science literature emphasises that mentoring and accessible senior support not only enhance clinical decision-making but also reduce perceived risk and improve uptake of new care models.28
Practical Considerations for Implementation
Practically, implementation should begin with a defined cohort of patients and explicit referral triggers, such as breathlessness limiting function, reduced mobility or exercise tolerance following acute illness, secretion retention, oxygen weaning needs, post-operative functional decline or deconditioning. A targeted staffing model may be preferable, whereby interested physiotherapists receive dedicated training, protected HHS capacity, access to equipment and supervision from an experienced cardiorespiratory physiotherapist. Service protocols should specify inclusion and exclusion criteria, escalation processes, documentation requirements, and communication pathways between the HHS team and the private practice.
Strengths and Limitations
By capturing perspectives from multiple stakeholder groups within the same service context, the study offers a nuanced understanding of how clinical, professional and operational considerations intersect when integrating physiotherapy into an HHS. The use of a qualitative descriptive approach enabled findings to remain close to participants’ accounts, enhancing their relevance for service planning and implementation. This study has several limitations. The inclusion of a single management participant limits the breadth of organisational perspectives. The specificity of the study also limits the transferability of the findings to other contexts (eg., different state/country, public sector).
Conclusion
While physiotherapy was viewed as having potential value for supporting post-operative and selected cardiorespiratory patients within a sub-acute home-care service, uncertainty regarding referral criteria, operational feasibility, workforce readiness, patient selection and perceived clinical risk in the home setting emerged as key challenges. These findings suggest that effective integration of physiotherapy into home hospital care requires clear role definition, shared referral logic, structured training and supervision and service models that align with private practice operational realities. Future research should evaluate physiotherapy-inclusive home hospital services following implementation, incorporating patient outcomes, service utilisation and clinician experience will be essential to inform scalable and evidence-based models of sub-acute physiotherapy care in the home.
Acknowledgments
The authors would like to acknowledge the assistance provided by Miss Esther Tian (ET) from Adelaide University in participating in the pilot interview and providing feedback on the semi-structured interview guide. The authors would also like to acknowledge the assistance from clinical and administrative staff at facilities where recruitment was conducted: PhysioWest and Calvary Private Hospital, both located in Adelaide, South Australia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Friedman B, Jiang HJ, Elixhauser A. Costly hospital readmissions and complex chronic illness. Inquiry. 2008;45:408–11. doi:10.5034/inquiryjrnl_45.04.408
2. Arsenault-Lapierre G, Henein M, Gaid D, et al. Hospital-At-home interventions vs in-hospital stay for patients with chronic disease who present to the emergency department. JAMA Network Open. 2021;4:E2111568. doi:10.1001/jamanetworkopen.2021.11568
3. Vasilevskis EE, Han JH, Hughes CG, Ely EW. Epidemiology and risk factors for delirium across hospital settings. Best Pract Res Clin Anaesth. 2012;26:277–287. doi:10.1016/j.bpa.2012.07.003
4. Australian Institute of Health Welfare. Health Expenditure Australia 2021-22; 2023.
5. Leff B, Montalto M. Home hospital-toward a tighter definition. J Am Geriatr Soc. 2004;52:2141. doi:10.1111/j.1532-5415.2004.52579_1.x
6. Gonçalves-Bradley DC, et al. Early discharge hospital at home. Cochrane Database Syst Rev. 2017
7. Chua CMS, Ko SQ, Lai YF, Lim YW, Shorey S. Perceptions of hospital-at-home among stakeholders: a meta-synthesis. J Gen Intern Med. 2022;37:637–650. doi:10.1007/s11606-021-07065-0
8. Cox R, Kyle G, Suzuki A, et al. Patient and multidisciplinary health professional perceptions of an Australian geriatric evaluation and management and rehabilitation hospital in the home service. Journal of Health Services Research & Policy. 2024;29(1):31–41. doi:10.1177/13558196231193863
9. Karacaoglu K, Leask CF. Staff views of a hospital at home model implemented in a Scottish care setting. AIMS Public Health. 2021;8:467–478. doi:10.3934/publichealth.2021036
10. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19:349–357. doi:10.1093/intqhc/mzm042
11. Colorafi KJ, Evans B. Qualitative descriptive methods in health science research. Health Env Res Design J. 2016;9:16–25. doi:10.1177/1937586715614171
12. Neergaard MA, Olesen F, Andersen RS, Sondergaard J. Qualitative description-the poor cousin of health research? BMC Med. Res. Method. 2009;9
13. Sandelowski M. Focus on research methods: whatever happened to qualitative description? Res Nurs Health. 2000;23:334–340. doi:10.1002/1098-240X(200008)23:4<334::AID-NUR9>3.0.CO;2-G
14. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107–115. doi:10.1111/j.1365-2648.2007.04569.x
15. Elo S, Kääriäinen M, Kanste O, et al. Qualitative content analysis: a focus on trustworthines. SAGE Open. 2014;4:215824401452263. doi:10.1177/2158244014522633
16. Edgar K, Iliffe S, Doll HA, et al. Admission avoidance hospital at home. Cochrane Database Syst Rev. 2024;3
17. Leong MQ, Lim CW, Lai YF. Comparison of Hospital-at-Home models: a systematic review of reviews. BMJ Open. 2021;11:e043285. doi:10.1136/bmjopen-2020-043285
18. ShahAli S, Shahabi S, Etemadi M, et al. Barriers and facilitators of integrating physiotherapy into primary health care settings: a systematic scoping review of qualitative research. Heliyon. 2023;9:e20736. doi:10.1016/j.heliyon.2023.e20736
19. Langhorne P, Baylan S, Trialists ESD. Early supported discharge services for people with acute stroke. Cochrane Database Syst Rev. 2017;2017
20. Bamgboje-Ayodele A, Boscolo A, Newton N, et al. Detection and management of clinical deterioration in a virtual hospital: a work system analysis. Appl Ergon. 2025;127:104530. doi:10.1016/j.apergo.2025.104530
21. Wallis JA, Shepperd S, Makela P, et al. Factors influencing the implementation of early discharge hospital at home and admission avoidance hospital at home: a qualitative evidence synthesis. Cochrane Database Syst Rev. 2024
22. Miller-Jenkins A, Lewis AK, Pryde K, Dennett AM. “The right people at the right time”: process evaluation of a novel allied health hospital in the home service for people with cancer. Support Care Cancer. 2025;33
23. Melman A, Vella SP, Dodd RH, et al. Clinicians’ perspective on implementing virtual hospital care for low back pain: qualitative study. JMIR Rehabil Assist Technol. 2023;10:e47227. doi:10.2196/47227
24. Proctor E, Silmere H, Raghavan R, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health Ment Health Serv Res. 2011;38:65–76. doi:10.1007/s10488-010-0319-7
25. Urquhart R, Kendell C, Cornelissen E, et al. Defining sustainability in practice: views from implementing real-world innovations in health care. BMC Health Serv Res. 2020;20
26. Greenhalgh T, Wherton J, Papoutsi C, et al. Beyond adoption: a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J Med Internet Res. 2017;19:e367. doi:10.2196/jmir.8775
27. Michaelchuk W, Oliveira A, Marzolini S, et al. Design and delivery of home-based telehealth pulmonary rehabilitation programs in COPD: a systematic review and meta-analysis. Int J Med Inform. 2022;162:104754. doi:10.1016/j.ijmedinf.2022.104754
28. Nilsen P, Bernhardsson S. Context matters in implementation science: a scoping review of determinant frameworks that describe contextual determinants for implementation outcomes. BMC Health Serv Res. 2019;19
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.