Back to Journals » Drug Design, Development and Therapy » Volume 20
Toward Optimized Platinum Therapy: A Risk Prediction Model for Toxicity Based on Platinum Accumulation and Its Impact on Treatment Outcomes
Authors Huang X ![]() , Chen C, Zheng J, Lai Y, Yang Y, Zhang Y, Fang L
, Chen C, Zheng J, Lai Y, Yang Y, Zhang Y, Fang L
Received 25 February 2026
Accepted for publication 5 June 2026
Published 10 June 2026 Volume 2026:20 600037
DOI https://doi.org/10.2147/DDDT.S600037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Xiaoting Huang,1,* Chen Chen,1,* Jieting Zheng,2 Yier Lai,3 Yi Yang,4 Yuling Zhang,5 Ling Fang2
1Pharmacy Intravenous Admixture Service, Cancer Hospital of Shantou University Medical College, Shantou, Guangdong, People’s Republic of China; 2Pharmacy Department, Cancer Hospital of Shantou University Medical College, Shantou, Guangdong, People’s Republic of China; 3Shantou University Medical College, Shantou, Guangdong, People’s Republic of China; 4Shantou University College of Science, Shantou, Guangdong, People’s Republic of China; 5Research Institute of Clinical Pharmacy, Shantou University Medical College, Shantou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuling Zhang, Email [email protected] Ling Fang, Email [email protected]
Background: Platinum-based chemotherapeutic agents are fundamental in the treatment of various malignancies, yet their long-term efficacy is often compromised by cumulative toxicity. This study investigates the association between platinum accumulation and length of hospital stay (LOS), and develops a predictive tool to optimize individualized platinum therapy.
Methods: A total of 300 cancer patients receiving platinum-based chemotherapy were enrolled. Serum platinum concentration was measured on day 21 ± 3 after drug administration. The LOS and adverse events were recorded. Mediation analysis explored underlying mechanisms, and a classification and regression tree (CART) model was constructed for risk prediction.
Results: Elevated serum platinum concentration significantly prolonged LOS, primarily mediated through reduced red blood cell count (mediation effect accounted for 32.3%). The CART model identified serum platinum concentration > 534.40 μg/L as a key threshold and major predictor of adverse reactions, alongside age > 60.5 years, serum creatinine > 94.50 μmol/L, and use of cisplatin or carboplatin. The model demonstrated an AUC of 0.782 and accuracy of 75.7%.
Conclusion: A serum platinum concentration > 534.40 μg/L serves as a clinically meaningful cutoff for identifying patients at high risk of platinum‑related toxicity. The proposed decision‑tree model offers a clinically actionable framework for the early recognition of these high‑risk individuals, facilitating timely dose management and treatment optimization in clinical practice.
Keywords: platinum, accumulation, length of stay, risk prediction, decision tree model, cancer
Introduction
Chemotherapy remains a cornerstone of clinical oncology. Among various antitumor treatment regimens, platinum-based therapies are widely used in the management of multiple malignancies, including lung, colorectal, and ovarian cancers.1,2 Platinum-based agents have become indispensable components of numerous first-line antitumor regimens. However, their extensive use is associated with significant clinical challenges. Platinum compounds exert cytotoxic effects that result in well-documented adverse reactions and dose-limiting toxicities, such as nephrotoxicity, neurotoxicity, and gastrointestinal toxicity.3,4 Nevertheless, persistent discomfort following treatment completion and potential long-term adverse effects are often overlooked in clinical practice. Our previous research has uncovered this underestimated phenomenon: months after chemotherapy—when the drugs are theoretically fully metabolized—patients commonly continue to experience symptoms such as nausea, fatigue, and skin rashes. Some patients even develop Mees’ lines, a characteristic sign of heavy metal poisoning.5 More importantly, these persistent symptoms show a significant correlation with the level of platinum accumulation in the body. Further studies indicate that platinum accumulation is positively correlated with concurrent white blood cell and platelet counts, and increases the risk of anemia, other adverse reactions, and fatigue.5,6 These observations cannot be adequately explained by conventional theories of chemotherapy-induced adverse effects, suggesting that residual platinum following platinum-based drug administration may mediate deeper, sustained pathophysiological processes.
Platinum-based chemotherapeutic agents differ from other conventional antitumor drugs in that their core active component is the metallic element platinum (Pt). As a heavy metal, platinum shares physicochemical properties with toxic metals such as lead (Pb), cadmium (Cd), and mercury (Hg). Although the toxicity of these metals has been extensively studied and confirmed in the context of occupational and environmental exposure,7–12 studies have reported detectable platinum accumulation in patients even up to 20 years after completion of platinum-based chemotherapy.13 However, the administration of platinum-based drugs as antitumor agents differs fundamentally from environmental or occupational heavy metal exposure in two key aspects. First, the intensity of exposure significantly exceeds that of typical environmental or occupational settings. When administered intravenously, platinum bypasses the dermal barrier entirely. For example, following a 2-hour intravenous infusion of oxaliplatin at a dose of 130 mg/m2, the peak plasma concentration of total platinum reaches 5.1 ± 0.8 μg/mL, with an area under the curve (AUC) as high as 189 ± 45 μg·h/mL.14 Second, due to the necessity and continuity of cancer treatment, clinical management cannot abruptly discontinue platinum administration to terminate exposure. This leads to persistent accumulation of platinum in the body, which may eventually exceed the threshold for human detoxification and excretion, resulting in significant deposition in critical organs such as the liver and kidneys.
The implications of such high-concentration, sustained platinum infusion cannot be overlooked. In clinical practice, we have observed that patients often report persistent symptoms such as fatigue and nausea during follow-up visits even after the completion of chemotherapy. Similar to this often neglected aspect of potential toxicity, clinical discussions frequently focus on efficacy and economic costs, while neglecting the quantification of time costs.15 Hospitalization accounts for 66% to 80% of the patient’s total medical time, exerting a substantial impact on their quality of life. Examining length of hospital stay (LOS) aims to more authentically and comprehensively reflect the overall impact of cancer treatment on patients’ lives.15,16 Therefore, we consider both LOS and adverse reactions to be important factors in treatment outcomes.
This study aims to measure residual serum platinum concentrations in patients and employ mediation analysis to explore potential mechanisms influencing the LOS. Additionally, a decision tree model will be applied to identify thresholds for adverse reactions induced by platinum accumulation. The resulting risk prediction model may ultimately be integrated into clinical medication management to contribute to improved quality of life for patients.
Methods
Study Design
This study will measure the serum platinum concentration and hematological parameters of patients receiving platinum-based chemotherapy, and record and analyze related adverse reactions and hospitalization duration. A mediation effect model will be constructed to explore the potential mechanisms by which platinum accumulation affects hospitalization duration. Additionally, a predictive model for adverse reactions related to platinum accumulation will be developed to identify high-risk factors and determine clinical intervention thresholds.
Based on the half-life theory, drugs are completely eliminated from the human body after 5.5 half-lives. Clinically, chemotherapy cycles are generally set to be more than three weeks. Therefore, blood samples will be collected on the day before the next round of chemotherapy to measure the serum platinum concentration, which represents the residual platinum accumulation in the body from the previous chemotherapy.
Inclusion and exclusion criteria were established for the study, and patients receiving platinum-based treatment at the Cancer Hospital Affiliated to Shantou University Medical College were recruited. The inclusion and exclusion criteria are shown in Table 1.
 |
Table 1 Patient Recruitment Criteria |
Ethical Approval
The study was approved by the Ethics Committee of the Affiliated Cancer Hospital of Shantou University Medical College (Approval No. 2024023). The committee confirmed that the study complies with the Declaration of Helsinki and ICH-GCP guidelines, and all participants provided informed consent.
Treatment Regimens
All patients received standard platinum-based chemotherapy. Doses were BSA-adjusted: cisplatin (75–100 mg/m2, q3w), carboplatin (AUC 5–6 via Calvert formula, q3w), or oxaliplatin (85–130 mg/m2, q2-3w). Dose modifications or delays occurred for ≥ grade 2 toxicities or renal dysfunction (creatinine clearance < 60 mL/min), per guideline recommendations. Each patient completed at least two full treatment cycles.
Clinical Data Collection
Clinical data were collected and recorded through electronic medical records. After enrollment, demographic characteristics (including age, name, gender, and disease type) and treatment parameters (including regimen, dosage, and administration route) were collected.
Blood Sample Collection
Baseline blood samples were collected before the use of platinum-based drugs after patient enrollment. Blood samples were also collected after the elimination time of platinum-based drugs (considering clinical feasibility, the sampling window was set before the patient’s next admission for treatment).
Serum Platinum Measurement
On day 21 ± 3 following cisplatin/oxaliplatin/carboplatin chemotherapy (ie, on the morning prior to the next cycle), 1 mL of fasting peripheral venous blood was collected using heparin-anticoagulated vacuum tubes.
For serum separation, whole blood samples were centrifuged at 3500 rpm for 10 minutes. Approximately 0.5 mL of supernatant serum was aspirated and stored in 1.5 mL platinum-free EP tubes at −80 °C.
For sample digestion and dilution, A 100 μL aliquot of serum was mixed with 900 μL of a 0.5% nitric acid solution, resulting in a final volume of 1 mL. The mixture was vortexed for 3 minutes to ensure thorough mixing and digestion, followed by standing for 20 minutes. The supernatant was then collected for the determination of platinum concentration using graphite furnace atomic absorption spectrometry (Jena ZEEnit 650, Germany).17
Treatment Outcome Evaluation
Adverse reactions after drug administration: Adverse reactions persisting after drug elimination were recorded and evaluated. The occurrence of adverse reactions was recorded as “No (0)” or “Yes (1)” and graded strictly according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 (grades 1–5).
Single hospitalization duration: The LOS for a single hospitalization was recorded. Situations where the LOS could not be determined or where other factors influenced the LOS were also recorded, such as when a single hospitalization included two drug administrations or when surgery or radiotherapy was performed during the hospitalization.
Statistical Methods
Statistical analysis was performed using SPSS Statistics 27.0, which was employed to run decision tree and mediation effect analyses. Mediation analysis was applied to explore factors mediating the relationship between platinum accumulation and LOS. This was conducted using the Process macro (Version 4.1, Model 4) with bootstrap resampling repeated 5000 times to calculate the 95% confidence interval for the indirect effect.
The Classification and Regression Tree (CART) algorithm is a universal binary tree-based algorithm. Its core principle involves recursively partitioning the data space. At each node, the optimal feature and split point are identified based on the principle of Gini impurity minimization, dividing the data into two subsets to construct a binary tree and ultimately generate interpretable decision rules.
The occurrence of adverse reactions was defined as the outcome variable of the prediction model, while indicators potentially influencing the occurrence of adverse reactions were included as independent variables for decision tree construction. The risk prediction model was developed using the CART algorithm, with the Gini impurity serving as the node splitting criterion and cost-complexity pruning applied as a built-in regularization strategy. The hyperparameters for tree growth were configured as follows: the maximum tree depth was set to 5, the minimum number of cases in parent nodes was set to 20, the minimum number of cases in child nodes was set to 10, and independent variables with a normalized importance greater than 5% were retained. A 10-fold cross-validation approach was employed for model training and validation, wherein the dataset was partitioned into 10 equally sized folds. During each iteration, 9 folds were used for training and the remaining fold for testing, with the average performance across all iterations taken as the final result. Model performance was evaluated using the receiver operating characteristic (ROC) curve and the area under the curve (AUC). Based on established methodological practice, this approach is recognized as an effective means of obtaining a decision tree model with reduced overfitting risk and enhanced generalization capability.
Results
Patient Characteristics
Following the application of predefined inclusion and exclusion criteria, a total of 300 eligible patients were ultimately enrolled in this study, with baseline characteristics summarized in Table 2. The cohort included 151 males (50.33%) and 149 females (49.67%). A history of surgery was reported in 127 patients (42.33%), while 173 (57.67%) had no surgical history. Treatment regimens consisted of cisplatin (129 patients), carboplatin (100 patients), and oxaliplatin (71 patients), with specific regimens and doses determined by the clinicians. Lung cancer was the most common diagnosis (54 patients, 18.00%), followed by cervical and ovarian cancer (29 patients each, 9.67%). Other cancer types included nasopharyngeal, breast, colon, esophageal, rectal, endometrial, and gastric cancers (see Figure 1).
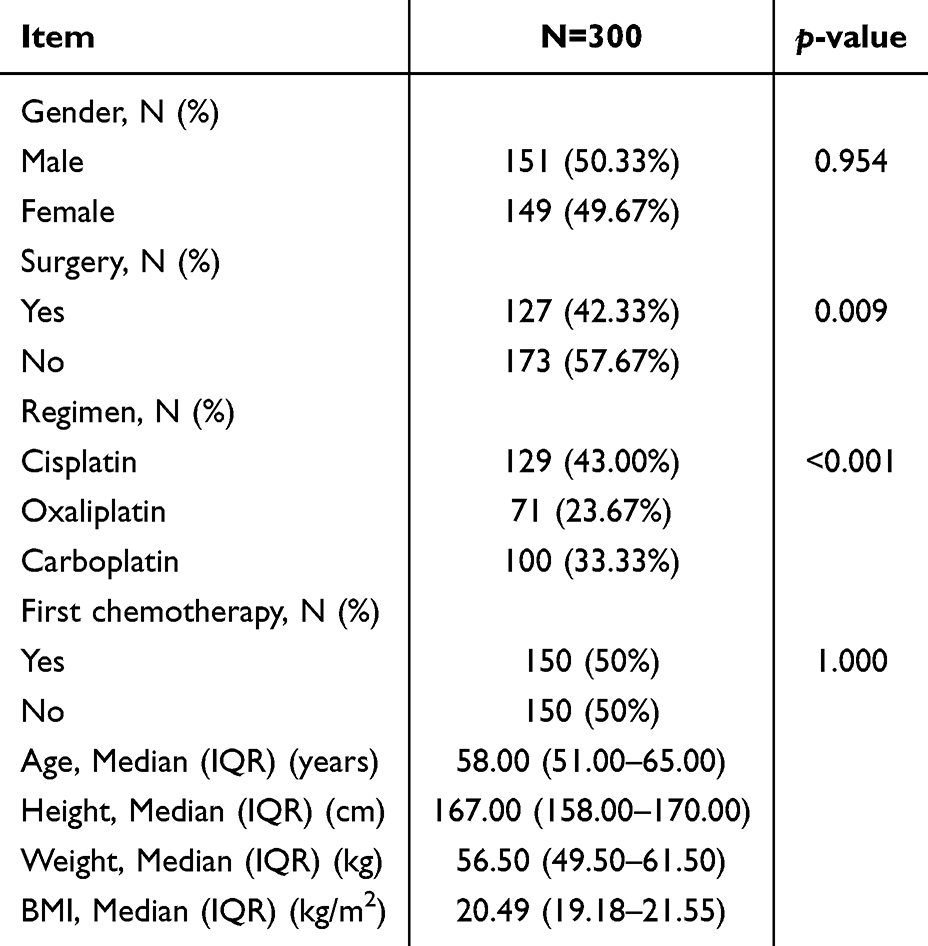 |
Table 2 Patient Baseline Characteristics |
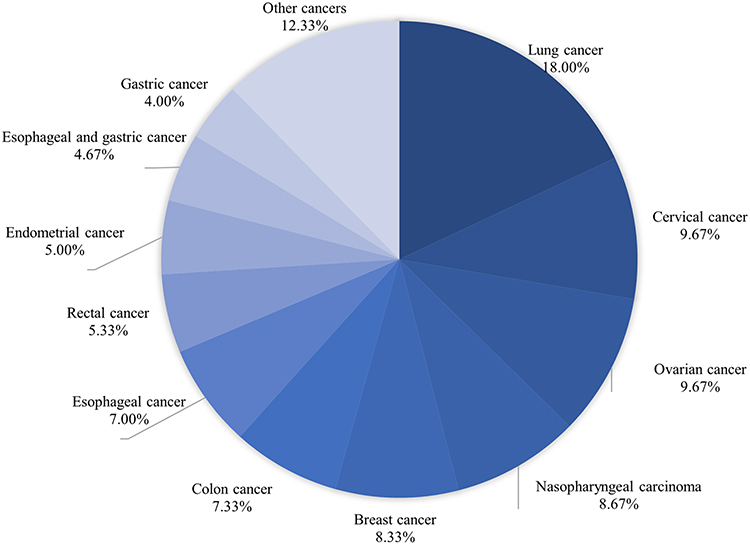 |
Figure 1 Cancer Type Distribution. |
Impact of Platinum Accumulation on LOS
A systematic analysis was conducted on the single LOS following medication. After excluding cases in which LOS was affected by surgery or radiotherapy or could not be accurately determined, 269 samples remained. The median LOS was 5.08 days (IQR: 4.00–8.04). A mediation effect analysis was conducted using the Bootstrap method.
The results (Figure 2) indicated a significant total effect of serum platinum concentration on LOS (β = 0.064, p < 0.05). However, after introducing the mediator (red blood cell count), the direct effect became non-significant (β = 0.043, p > 0.05), while the indirect effect through the mediator was significant (effect value = 0.0207, 95% CI: 0.0056–0.0424). Notably, both path coefficients were negative (Path a: β = –0.001, p < 0.001; Path b: β = –27.211, p < 0.01), indicating that higher serum platinum concentration reduces red blood cell count, which in turn prolongs LOS. This indirect effect accounted for approximately 32.3% of the total effect.
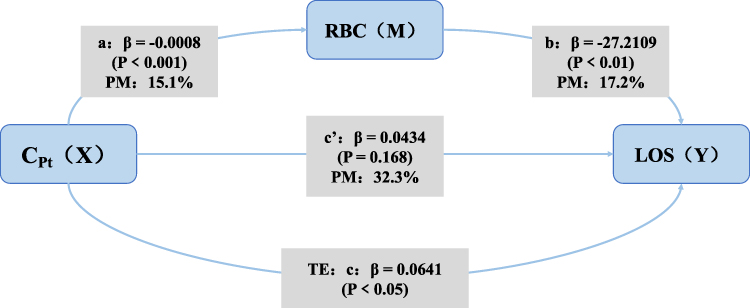 |
Figure 2 Mediation Effect Analysis of Platinum Accumulation and LOS. Abbreviations: CPt, Serum Platinum Concentration; RBC, Erythrocyte; LOS, Length of Stay; PM, Proportion Mediated; TE, Total Effect. |
Statistical power analysis demonstrated that the current sample size (n=300) provided over 99% statistical power (α=0.05) to detect the observed mediation effect size (f2=0.3232≈0.48), confirming the adequacy of the sample.
Construction and Validation of the Platinum Accumulation Risk Prediction Model
Basic Information of the Decision Tree Model
The risk prediction model, constructed with the CART algorithm, ultimately formed a stable and interpretable tree structure after parameter optimization and variable screening. The final model consisted of 12 nodes (including 5 decision nodes and 7 terminal nodes), had a depth of 5, and contained 12 decision paths (see Figure 3).
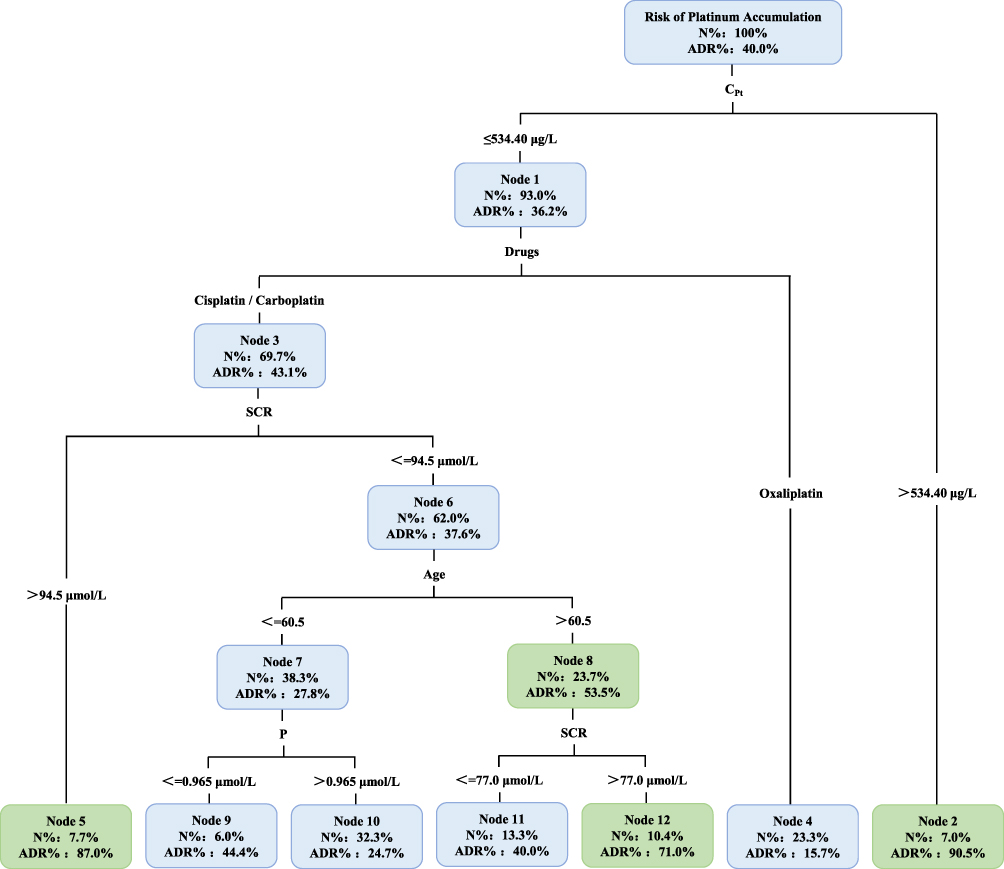 |
Figure 3 Decision Tree Model for Platinum Accumulation Risk Prediction. Abbreviations: CPt, Serum Platinum Concentration; SCR, Serum Creatinine; P, Serum Phosphorus. |
Initially, 14 potential independent variables were included: gender, age, serum platinum concentration, RBC count, hemoglobin, ALT, AST, serum creatinine, platelet count, absolute lymphocyte count, absolute neutrophil count, serum phosphorus, drug type, and number of treatment cycles. Following screening based on “minimum node cases” and “normalized importance > 5%”, five core predictors were retained: serum platinum concentration, serum creatinine, age, drug type, and serum phosphorus. Detailed model parameters are presented in Table 3.
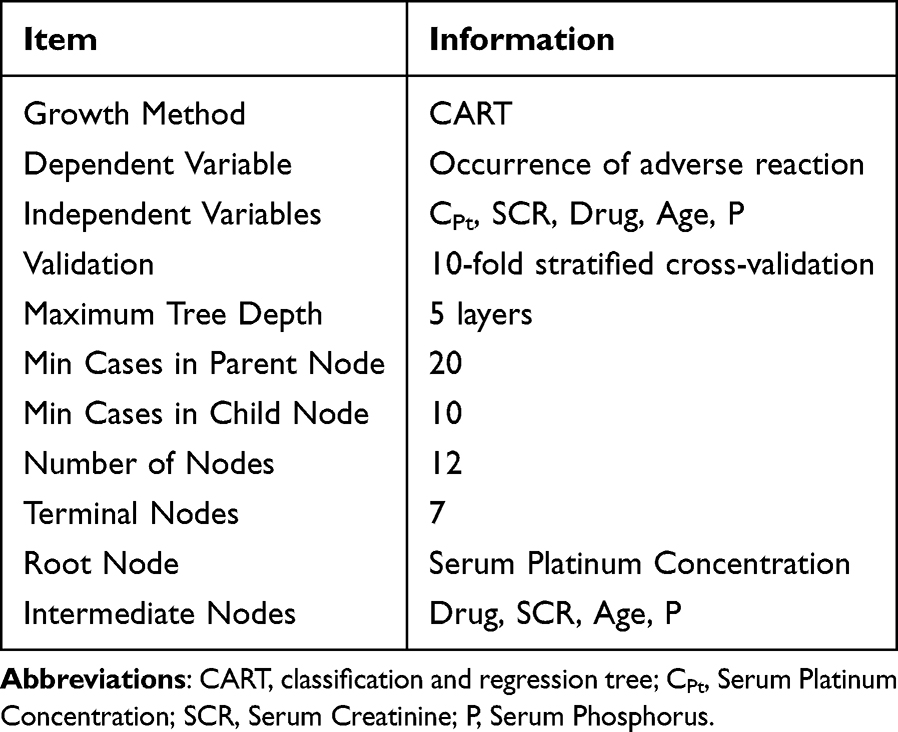 |
Table 3 Decision Tree Model Information |
As shown in Figure 3, in the decision tree model developed in this study, serum platinum concentration served as the root node. This indicates that a serum platinum concentration (CPt > 534.40 μg/L) was the most critical decision factor in this prediction model for determining the occurrence of adverse drug reactions, directly reflecting the level of platinum accumulation in the body. The second-level decision node was the medication category, with cisplatin/carboplatin conferring a higher risk of platinum accumulation toxicity than oxaliplatin. The third-level node was serum creatinine (SCR), a key indicator for renal function assessment. When SCR > 94.50 μmol/L, the risk of platinum accumulation toxicity increased significantly. Subsequent nodes, including age and serum phosphorus, were also identified as important factors in predicting platinum accumulation risk. The decision nodes were ranked in descending order of importance as follows: Serum platinum concentration, SCR, Platinum-based agent category, Age, and serum phosphorus (see Table 4 for the importance ranking of key independent variables in the model).
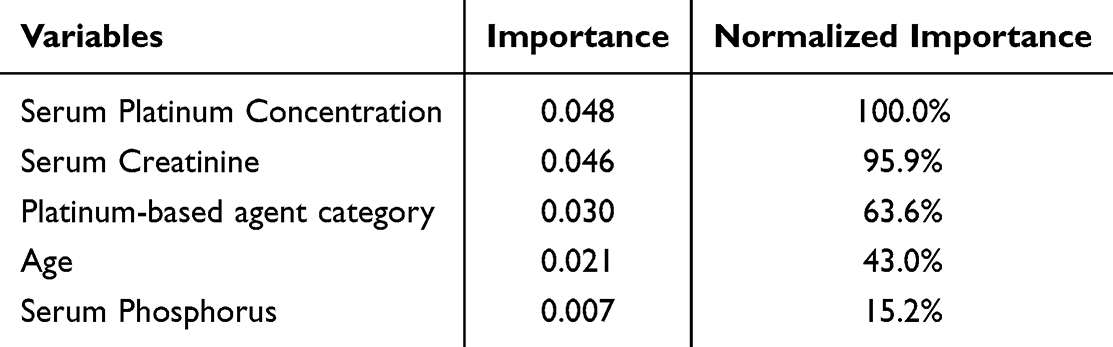 |
Table 4 Key Independent Variable Importance Ranking |
Performance Evaluation of the Risk Prediction Model
Confusion Matrix and Prediction Accuracy
The confusion matrix (Table 5) showed an overall prediction accuracy of 75.7%, preliminarily validating the model’s utility.
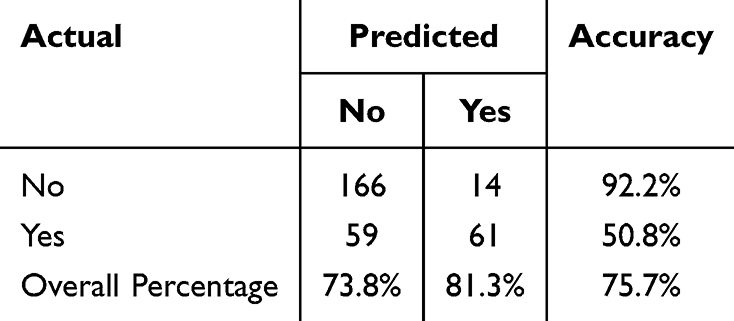 |
Table 5 Confusion Matrix of the Risk Prediction Model |
Model Risk Assessment
To further evaluate the model’s stability and applicability, risk was assessed from the perspectives of both training set fit and cross-validation generalization (K = 10 folds) (Table 6). The cross-validation error was 27.3% (SE ± 0.027), slightly higher than the resubstitution error (difference 3.0%; comparison: 24.3% ± 2.5% vs. 27.3% ± 2.7%), indicating mild overfitting.
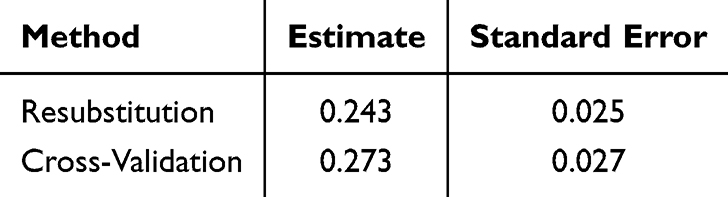 |
Table 6 Risk Estimation of the Prediction Model |
Model Predictive Performance Evaluation
The CART model developed in this study exhibited a sensitivity of only 50.8% at the default threshold, indicating a high risk of missed diagnosis. This is attributed to the CART algorithm’s default classification threshold of 0.5. Adjusting the classification threshold can significantly improve this situation. We used the ROC curve to further evaluate the model’s discriminatory ability (Figure 4). When the threshold was lowered from 0.57 to 0.32 (the point of maximum Youden index), the maximum Youden index was 0.461, corresponding to a sensitivity of 70.8% and a specificity of 75.3%. Compared to the threshold of 0.5, this adjustment allows for the identification of 20% more high‑risk patients while maintaining clinically acceptable specificity. The area under the ROC curve was 0.782 (95% CI: 0.727–0.837), significantly greater than 0.5 (p < 0.001), indicating moderate to good predictive discrimination.
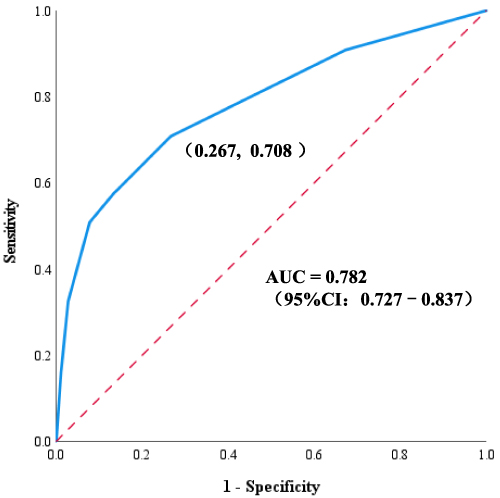 |
Figure 4 ROC Curve of the Risk Prediction Model. |
Discussion
Serum platinum concentration was used to reflect the extent of platinum accumulation in the body after drug clearance. The accumulation mechanism is primarily related to the pharmacokinetic properties of platinum drugs:18 (1) Irreversible binding: Platinum drugs can form covalent bonds with proteins, DNA, or other molecules, resulting in platinum-protein complexes; (2) DNA cross-linking: For example, cisplatin forms intra- or inter-strand cross-links with DNA bases, which are difficult to repair; (3) Metabolic inertia: Platinum drugs mainly exist in their original or monohydrated form in vivo, lacking effective metabolic degradation pathways. These properties collectively lead to sustained platinum accumulation.
We aimed to explore the impact of this chronic toxicity induced by platinum accumulation on patients’ quality of life. LOS served as a key and multidimensional indicator, reflecting not only healthcare quality and resource utilization but, more importantly, the economic and time burden on patients. A retrospective study showed that each additional day of hospitalization increased average costs by 1399 yuan,19 highlighting the importance of controlling LOS to reduce economic burden. Our previous research demonstrated that platinum accumulation is associated with an increased risk of anemia,5 and other studies have linked anemia to prolonged LOS.20 The present mediation analysis connects these findings: RBC count significantly mediates the relationship between serum platinum concentration and LOS. This reveals a clear clinical pathological mechanism: increased serum platinum concentration significantly suppresses RBC count, and lower RBC levels are closely associated with longer hospitalization. Therefore, monitoring and timely intervention for platinum-induced erythrocytopenia are crucial for improving patient outcomes and shortening LOS.
Factors influencing LOS are complex and include disease type, cancer stage, age, adverse reactions, transfusions, and surgery.21,22 In our preliminary investigation, serum platinum concentration was found to be correlated with several hematologic indices, as well as with the incidence of adverse events, cancer-related fatigue, and the category of medications used.5 However, in the present study, we did not identify an association between these factors and LOS. Yet multiple studies15,16,23 have indicated that chemotherapy regimens (eg, Nivolumab + FOLFOX), adverse events, and chemotherapy-induced adverse reactions all increase patients’ length of hospital stay. These factors may also serve as potential mediators between serum platinum concentration and LOS, which warrants further investigation.
In the decision tree model, serum platinum concentration served as the root node, indicating it is the most critical factor for predicting adverse reactions (threshold: CPt ≥ 534.40 μg/L). When serum platinum exceeds this threshold, the risk of adverse reactions increases significantly (90.5%). Our previous study also found that for every 1 μg/L increase in serum platinum concentration, the risk of adverse reactions increased by 0.7%.5 Other studies have reported that oxaliplatin-induced neurotoxicity is reversible at low doses but becomes irreversible at high doses, potentially affecting quality of life.24 Thus, serum platinum concentration holds value for guiding clinical individualized dosing. When a patient’s measured serum platinum level is high, vigilance for adverse events and timely interventions are warranted. In preventing adverse reactions to platinum-based drugs, common clinical approaches include pre‑chemotherapy pretreatment and post‑chemotherapy accelerated elimination. However, there is currently a lack of effective intervention strategies for the long‑term toxicity issues induced by platinum accumulation after drug administration. Based on the general principle of promoting the excretion of water‑soluble substances, hydration and diuresis remain the most classic method.25 When the serum platinum concentration exceeds the threshold (CPt ≥ 534.40 μg/L), aggressive fluid infusion and diuresis can accelerate renal excretion of platinum.
The risk associated with oxaliplatin was significantly lower than that of cisplatin/carboplatin (15.7% vs. 43.1%), which may be attributed to differences in pharmacokinetics and toxicity profiles. First, unlike cisplatin, oxaliplatin enters cells primarily via organic cation transporters (OCT1-3)-mediated active transport and passive diffusion, reducing renal accumulation and consequent nephrotoxicity.26 Second, the DNA adducts formed by oxaliplatin differ from those produced by cisplatin and carboplatin. Its DACH ligand enables specific hydrogen bonding and structural distortions on DNA strands, potentially leading to differences in apoptosis pathways. In contrast, cisplatin and carboplatin generate high levels of DNA intrastrand cross-links, readily triggering oxidative stress and inflammatory responses, thereby increasing the risk of renal tubular damage.27 Furthermore, oxaliplatin’s structure was optimized to reduce toxicity risk. Stable leaving groups diminish off-target organ damage and significantly lower systemic toxicity, although a shift in the toxicity profile is unavoidable. Neurotoxicity remains common and requires specific management strategies (eg, avoiding cold stimuli).27
Age is another important factor in the risk prediction model. The higher risk of adverse drug reactions in elderly patients is not limited to platinum drugs and is related to age-dependent changes in kidney structure: after age 60, the number of nephrons decreases by 30–50%, and the proportion of sclerotic glomeruli increases from 0.5% to 36% between ages 50–60, resulting in reduced glomerular filtration area and permeability. As the glomerular filtration rate declines, the risk of drug accumulation toxicity increases.28 Data from platinum drug applications show that patients over 50 have a higher rate of chemotherapy termination due to infection risk, and elderly patients exhibit an increased need for transfusions.29 Among cisplatin-treated patients, those over 65 have a 2.96 times higher risk of acute kidney injury compared to those under 25.30 Therefore, age should be considered a core variable for renal toxicity risk when using cisplatin or carboplatin.
Serum creatinine and serum phosphorus, both related to renal function, were also included in the model. The risk of adverse reactions increased significantly when serum creatinine exceeded 94.50 μmol/L. In patients under 60.5 years, serum phosphorus also influenced the incidence of adverse reactions. This aligns with our other study on platinum accumulation risk modeling: platinum accumulation level was positively correlated with serum phosphorus, and accumulation led to increased serum creatinine, partially mediating (5.2%) the occurrence of adverse reactions,31 underscoring the value of renal function indicators in the prediction model. Notably, these variables appeared as sub-nodes under the cisplatin/carboplatin branch, not under oxaliplatin, indicating that the metabolism of cisplatin and carboplatin highly depends on renal clearance, and their toxicity risk is closely tied to renal function. The decision tree did not reveal distinct risk markers for oxaliplatin; its key monitoring indicators require further exploration using real-world data.
We previously used mediation analysis to explore the biological mechanisms behind platinum accumulation-induced toxicity and calculated cutoff values to predict the risk of adverse reactions when indicators are abnormal.31 Individual cutoff values can serve for preliminary screening and dynamic warning based on single indicators. However, clinical decision-making often requires integrating multiple variables.
From the decision tree model, it is evident that serum platinum concentration is a critical indicator in clinical individualized dosing of platinum-based drugs, providing feedback on platinum accumulation levels and predicting accumulation risks. When using carboplatin or cisplatin, a monitoring system centered on renal function should be established, and indicators such as age, serum creatinine levels, and serum phosphorus levels should be given high attention in assessing the risk of platinum accumulation. This study focuses on the fundamental pharmacokinetic phenomenon of platinum metal accumulation and integrates multiple clinical indicators through a decision tree to form a clear stratified decision pathway. This approach is better suited to the complex clinical data encountered in practical applications. The predictive results can be directly used to guide dynamic adjustments to treatment plans, reflecting a shift in perspective from “toxicity management” to “treatment optimization.”
In contrast to existing predictive models for platinum-based agents—such as the model for cisplatin-induced nephrotoxicity developed by Zhang et al32 and the model for myelosuppression following platinum-based chemotherapy established by Li et al33 which focus on predicting risks of specific adverse drug reactions—this study introduces a distinct approach by incorporating the cumulative platinum concentration after complete metabolic elimination following each administration as the fundamental decision factor for risk assessment. Furthermore, the study establishes clear clinical intervention thresholds for key variables (eg, CPt > 534.40 μg/L, Age > 60.5 years), thereby constructing a transparent and actionable clinical decision pathway with demonstrated originality.
In addition to the clinical parameters measured in this study, accumulating evidence indicates that genetic factors play a pivotal role in the personalized application of platinum-based chemotherapy. For instance, deficiency in the DNA damage repair pathway resulting from mutations in BRCA1/2 constitute a fundamental mechanism underlying the heightened sensitivity of tumor cells to platinum-based chemotherapy, particularly cisplatin. Consequently, patients harboring such mutations exhibit significantly higher objective response rates and experience meaningful survival benefits.34,35 Beyond its role in sensitivity, BRCA1/2 genotype also serves as a critical biomarker for predicting the efficacy of platinum-based chemotherapy in metastatic breast cancer.36 Beyond this, single nucleotide polymorphisms in the DNA damage repair pathway genes (eg, XRCC1, ERCC1/2) and drug-metabolizing enzyme genes (eg, GSTP1, GSTM1) are also significantly correlated with platinum-based chemotherapy sensitivity and resistance.37,38 At the cellular level, platinum-sensitive cells (eg, the testicular cancer 833K cell line) accumulate substantially higher levels of platinum-DNA adducts (eg, Pt-1,2-d(GpG)) compared to resistant cells (eg, the breast cancer MDA-MB-231 cell line).39 Therefore, to refine precision treatment strategies for platinum-based chemotherapy, future predictive models should integrate genomic factors in addition to the clinical indicators identified herein.
Our current predictive model has certain limitations that warrant acknowledgment. First, the findings are derived from a single-center study, and their generalizability requires further validation through multi-center prospective cohorts. Second, constrained by the sample size, we were unable to perform stratified analyses to reinforce our conclusions. For instance, metabolic-related cancers may lead to elevated platinum accumulation, thereby increasing the risk of dose-dependent toxicity; dedicated stratified analyses could elucidate the correlation between platinum accumulation and metabolism-related adverse reactions. However, filtering by specific cancer types would inevitably reduce the training set size, which in turn would compromise the robustness and credibility of the model. Therefore, expanding sample sizes via multi-center studies and integrating pharmacogenomic monitoring data represent key priorities for our future research. Building on the present study, constructing a multi-omics prediction model that integrates clinical indicators with genetic biomarkers using machine learning algorithms would be of significant scientific value. We hypothesize that such a multidimensional prediction system could enhance both the accuracy and safety of platinum-based chemotherapy administration, ultimately facilitating the development of a more refined, personalized precision medicine decision-making system for clinical practice.
Conclusion
Platinum accumulation may prolong the length of hospital stay through mechanisms involving reduced red blood cell count. Monitoring and managing platinum accumulation, along with implementing timely interventions, are key steps in optimizing treatment strategies. This preventive, personalized risk management approach helps reduce unplanned treatment interruptions due to toxicity, and is essential for improving patients’ long‑term quality of life and treatment outcomes. The present study established a preliminary framework for early identification of high‑risk patients, offering a strategy to enhance the clinical efficacy and safety of platinum‑based drugs at an individualized level, and providing a foundation for subsequent multi‑center research.
Author Contributions
Ling Fang: Funding acquisition, Project administration, Writing-review & editing; Yuling Zhang: Methodology; Xiaoting Huang and Chen Chen: Data curation, Formal Analysis; Xiaoting Huang: Writing-original draft; Jieting Zheng: Investigation; Yier Lai and Yi Yang: Resource, Software. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Fund of Guangdong Basic and Applied Basic Research Foundation (2022A1515220076), Wu Jieping Medical Foundation Clinical Research Special Fund (320.6750.2024-6-45) and Chinese Youth Medical Innovation Research Project.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sharma R, Singh VJ, Chawla PA. Advancements in the use of platinum complexes as anticancer agents. Anticancer Agents Med Chem. 2022;22(5):821–13. doi:10.2174/1871520621666210805150705
2. Zhang C, Xu C, Gao X, Yao Q. Platinum-based drugs for cancer therapy and anti-tumor strategies. Theranostics. 2022;12(5):2115–2132. doi:10.7150/thno.69424
3. Ivanova S. Comparative assessment of clinical trials, indications, pharmacokinetic parameters and side effects of approved platinum drugs. Pharmacia. 2022;69(1):1–7. doi:10.3897/pharmacia.69.e78813
4. Kweekel DM, Gelderblom H, Guchelaar HJ. Pharmacology of oxaliplatin and the use of pharmacogenomics to individualize therapy. Cancer Treat Rev. 2005;31(2):90–105. doi:10.1016/j.ctrv.2004.12.006
5. Zhang Y, Zheng J, Jiang Y, Huang X, Fang L. Neglected, drug-induced platinum accumulation causes immune toxicity. Front Pharmacol. 2020;11:1166. doi:10.3389/fphar.2020.01166
6. Zhang Y, Huang X, Feng S, Chen C, Guo D, Fang L. Platinum accumulation and cancer-related fatigue, correlation with IL-8, TNF-α and hemocytes. Front Pharmacol. 2021;12:658792. doi:10.3389/fphar.2021.658792
7. Boskabady MH, Karimi GR, Samarghandian S, Farkhondeh T. Tracheal responsiveness to methacholine and ovalbumin; and lung inflammation in Guinea pigs exposed to inhaled lead after sensitization. Ecotoxicol Environ Saf. 2012;86:233–238. doi:10.1016/j.ecoenv.2012.09.025
8. Samarghandian S, Borji A, Afshari R, Delkhosh MB, Gholami A. The effect of lead acetate on oxidative stress and antioxidant status in rat bronchoalveolar lavage fluid and lung tissue. Toxicol Mech Methods. 2013;23(6):432–436. doi:10.3109/15376516.2013.777136
9. Santa Maria MP, Hill BD, Kline J. Lead (Pb) neurotoxicology and cognition. Appl Neuropsychol Child. 2019;8(3):272–293. doi:10.1080/21622965.2018.1428803
10. Satarug S, Gobe GC, Vesey DA, Phelps KR. Cadmium and lead exposure, nephrotoxicity, and mortality. Toxics. 2020;8(4):86. doi:10.3390/toxics8040086
11. Wiseman CLS, Zereini F. Airborne particulate matter, platinum group elements and human health: a review of recent evidence. Sci Total Environ. 2009;407(8):2493–2500. doi:10.1016/j.scitotenv.2008.12.057
12. Yang L, Zhang Y, Wang F, Luo Z, Guo S, Strähle U. Toxicity of mercury: molecular evidence. Chemosphere. 2020;245:125586. doi:10.1016/j.chemosphere.2019.125586
13. Brouwers EEM, Huitema ADR, Beijnen JH, Schellens JHM. Long-term platinum retention after treatment with cisplatin and oxaliplatin. BMC Clin Pharmacol. 2008;8:7. doi:10.1186/1472-6904-8-7
14. Wei G, Gu Z, Gu J, et al. Platinum accumulation in oxaliplatin-induced peripheral neuropathy. J Peripher Nerv Syst. 2021;26(1):35–42. doi:10.1111/jns.12432
15. Agrawal NY, Thawani R, Edmondson CP, Chen EY. Estimating the time toxicity of contemporary systemic treatment regimens for advanced esophageal and gastric cancers. Cancers. 2023;15(23):5677. doi:10.3390/cancers15235677
16. Rocque GB, Williams CP, Ingram SA, et al. Health care‐related time costs in patients with metastatic breast cancer. Cancer Med. 2020;9(22):8423–8431. doi:10.1002/cam4.3461
17. Zhang YL. A study on the determination of total platinum in serum of cancer patients after medication by digestion-GFAAS. Wangfang Data. 2020. Available from: https://d.wanfangdata.com.cn/Periodical/sdyygc202004002.
18. Qin Z, Ren G, Yuan J, et al. Systemic evaluation on the pharmacokinetics of platinum-based anticancer drugs from animal to cell level: based on total platinum and intact drugs. Front Pharmacol. 2020;10:1485. doi:10.3389/fphar.2019.01485
19. Wu SW, Pan Q, Wei LY, et al. Research on 2041 cases of high inpatient expenditure and influence factors during 3 years in a single center. Chin Med J. 2016;129(19):2325–2330. doi:10.4103/0366-6999.190681
20. Lin RJ, Evans AT, Chused AE, Unterbrink ME. Anemia in general medical inpatients prolongs length of stay and increases 30-day unplanned readmission rate. South Med J. 2013;106(5):316–320. doi:10.1097/SMJ.0b013e318290f930
21. Freitas A, Silva-Costa T, Lopes F, et al. Factors influencing hospital high length of stay outliers. BMC Health Serv Res. 2012;12:265. doi:10.1186/1472-6963-12-265
22. Smith CG, Davenport DL, Gorski J, et al. Clinical factors associated with longer hospital stay following ovarian cancer surgery. Healthcare. 2019;7(3):85. doi:10.3390/healthcare7030085
23. Cook S, Samuel V, Meyers DE, et al. Immune-related adverse events and survival among patients with metastatic NSCLC treated with immune checkpoint inhibitors. JAMA Network Open. 2024;7(1):e2352302. doi:10.1001/jamanetworkopen.2023.52302
24. Burz C, Berindan-Neagoe IBN, Balacescu O, et al. Clinical and pharmacokinetics study of oxaliplatin in colon cancer patients. J Gastrointestin Liver Dis. 2009;18(1):39–43.
25. Pabla N, Dong Z. Cisplatin nephrotoxicity: mechanisms and renoprotective strategies. Kidney Int. 2008;73(9):994–1007. doi:10.1038/sj.ki.5002786
26. Lyrio RMDC, Rocha BRA, Corrêa ALRM, et al. Chemotherapy-induced acute kidney injury: epidemiology, pathophysiology, and therapeutic approaches. Front Nephrol. 2024;4:1436896. doi:10.3389/fneph.2024.1436896
27. Forgie BN, Prakash R, Telleria CM. Revisiting the anti-cancer toxicity of clinically approved platinating derivatives. Int J Mol Sci. 2022;23(23):15410. doi:10.3390/ijms232315410
28. Mühlberg W, Platt D. Age-dependent changes of the kidneys: pharmacological implications. Gerontology. 1999;45(5):243–253. doi:10.1159/000022097
29. Meixner E, Hoeltgen L, Hoegen P, et al. Age-dependent hematologic toxicity profiles and prognostic serologic markers in postoperative radiochemotherapy treatment for uterine cervical cancer. Technol Cancer Res Treat. 2022;21:15330338221118188. doi:10.1177/15330338221118188
30. Latcha S, Jaimes EA, Patil S, Glezerman IG, Mehta S, Flombaum CD. Long–term renal outcomes after cisplatin treatment. Clin J Am Soc Nephrol. 2016;11(7):1173–1179. doi:10.2215/CJN.08070715
31. Zhang Y, Guo P, Huang X, Xu YW, Zheng Z, Fang L. Risk assessment of heavy metal toxicity induced by platinum accumulation in tumor patients. PeerJ. 2025;13:e19375. doi:10.7717/peerj.19375
32. Zhang J, Luo X, Fan Y, et al. Development and validation of a LASSO prediction model for cisplatin induced nephrotoxicity: a case-control study in China. BMC Nephrol. 2024;25:194. doi:10.1186/s12882-024-03623-w
33. Li X, Li L, Zhang L. Development and validation of a prediction model for myelosuppression in lung cancer patients after platinum-based doublet chemotherapy: a multifactorial analysis approach. Am J Cancer Res. 2025;15(2):470–486. doi:10.62347/TFUC2568
34. Byrski T, Dent R, Blecharz P, et al. Results of a Phase II open-label, non-randomized trial of cisplatin chemotherapy in patients with BRCA1-positive metastatic breast cancer. Breast Cancer Res. 2012;14(4):R110. doi:10.1186/bcr3231
35. Isakoff SJ, Mayer EL, He L, et al. TBCRC009: a multicenter phase II clinical trial of platinum monotherapy with biomarker assessment in metastatic triple-negative breast cancer. J Clin Oncol. 2015;33(17):1902–1909. doi:10.1200/JCO.2014.57.6660
36. Matuszczak M, Kiljańczyk A, Marciniak W, et al. Blood molybdenum level as a marker of cancer risk on BRCA1 carriers. Hered Cancer Clin Pract. 2024;22(1):19. doi:10.1186/s13053-024-00291-7
37. Sawers L, Ferguson MJ, Ihrig BR, et al. Glutathione S-transferase P1 (GSTP1) directly influences platinum drug chemosensitivity in ovarian tumour cell lines. Br J Cancer. 2014;111(6):1150–1158. doi:10.1038/bjc.2014.386
38. Gu AQ, Wang WM, Chen WY, Shi CL, Lu JH, Han JQ. XRCC1 genetic polymorphisms and sensitivity to platinum-based drugs in non-small cell lung cancer: an update meta-analysis based on 4708 subjects. Int J Clin Exp Med. 2015;8(1):145–154.
39. Hah SS, Henderson PT, Turteltaub KW. Towards biomarker-dependent individualized chemotherapy: exploring cell-specific differences in oxaliplatin-DNA adduct distribution using accelerator mass spectrometry. Bioorg Med Chem Lett. 2010;20(8):2448–2451. doi:10.1016/j.bmcl.2010.03.020
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Computational Study of Bis-(1-(Benzoyl)-3-Methyl Thiourea) Platinum (II) Complex Derivatives as Anticancer Candidates

Ruswanto R, Mardianingrum R, Nofianti T, Fizriani R, Siswandono S
Advances and Applications in Bioinformatics and Chemistry 2023, 16:15-36
Published Date: 10 February 2023
The Associations and Causal Relationships of Ovarian Cancer - Construction of a Prediction Model
Liu J, Hu T, Guan Y, Zhai J
International Journal of Women's Health 2024, 16:1127-1135
Published Date: 18 June 2024
Characteristics Associated with Length of Stay in Intensive Care Unit for Cancer Patients in China: A Nationwide Retrospective Cohort Study
Zhang G, Liu H, Xia R, Zhang L, Liu K, Zhou D, Xing X, Liu H
Journal of Multidisciplinary Healthcare 2025, 18:6025-6035
Published Date: 22 September 2025