")
Back to Journals » International Journal of General Medicine » Volume 13
Torsion of Wandering Spleen Attached to the Omentum: A Rare Case Report from Iran
Authors Abaszadeh F, Taebi M, Nikzad Jamnani H
Received 3 February 2020
Accepted for publication 9 June 2020
Published 24 June 2020 Volume 2020:13 Pages 333—336
DOI https://doi.org/10.2147/IJGM.S248259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Farzad Abaszadeh,1 Mozhgan Taebi,2 Habiballah Nikzad Jamnani3
1Department of Operation Room Nurse, Faculty of Allied Medicine, Kerman University of Medical Sciences, Kerman, Iran; 2Department of Anesthesiology, Faculty of Allied Medicine, Kerman University of Medical Sciences, Kerman, Iran; 3Imam Khomeini Educational & Remedial Center, Jiroft University of Medical Sciences, Jiroft, Iran
Correspondence: Farzad Abaszadeh
Department of Operation Room Nurse, Faculty of Allied Medicine, Kerman University of Medical Sciences, Kerman, Iran
Tel +989383697388
Email [email protected]
Background: Wandering spleen is a rare condition with less than 0.2% prevalence, and it is the cause of 0.25% of total splenectomies. This condition happens as a result of the lack or looseness of the spleen suspensory ligaments, and it may manifest as an acute abdomen due to the spleen becoming twisted around its vascular base.
Case Presentation: This study reports the case of a wandering spleen attached to the omentum (with blood supply from the omentum) in the pelvic area, with ectopic appendix (located in the right upper quadrant), ectopic liver (located in the abdominal midline), and ectopic stomach (located in the right upper abdominal region), in a 15-year-old male complaining about abdominal pain, nausea, vomiting, and lack of appetite, who was referred to the hospital. The patient underwent laparotomy with the diagnosis of acute abdomen; the twisted ectopic spleen in the pelvis was removed and appendectomy was also performed. The clinical manifestations of wandering spleen vary extensively, and its presurgical diagnosis is difficult in the absence of radiological studies. Therefore, spleen torsion has to be considered as a diagnosis for acute abdomen in order to prevent necrosis of the spleen and other related complications.
Conclusion: Wandering spleen should be borne in mind for patients presenting with a palpable intra-abdominal mass causing acute or intermittent abdominal symptoms.
Keywords: ectopic spleen, spleen torsion, splenectomy, case report
Background
The spleen is an intraperitoneal organ which is held in place by several ligaments including phrenicosplenic, splenorenal, colicosplenic, and gastrosplenic.1 Wandering spleen is a rare condition with less than 0.2% prevalence, and it is the cause of 0.25% of total splenectomies.2
The prevalence of wandering spleen is 13 times higher in women than in men.3 Its etiology is not known, but the looseness or lack of spleen ligaments is claimed to be a factor.4 The mobility of the wandering spleen leads to various complications such as torsion, gangrene, abscess, spleen hemorrhage, and necrosis of the spleen tail.5
The standard treatment option in patients with ectopic spleen is splenopexy, which is specifically recommended for children to preserve the function of the spleen and prevent severe infections. However, in cases of twisted and necrotic spleen, splenectomy is necessary.6
In the present study, the case of a 15-year-old male with ectopic spleen attached to the omentum is introduced to draw physicians’ attention to this rare condition when facing a mass or pelvic and abdominal pain.
Case Presentation
A 15-year-old male patient complaining about permanent abdominal pain was referred to Imam Khomeini hospital in Jiroft, Iran. He had experienced abdominal pain, right lower quadrant (RLQ) pain, pain under his bladder, pelvic pain, rebound tenderness, fever, nausea, vomiting, and lack of appetite over the few past days. His vital signs were: temperature = 38°C, blood pressure = 115/70 mmHg, pulse = 73 bpm, and respiratory rate = 17 bpm. The laboratory findings are shown in Table 1. The physician performed an examination, and ordered specific tests of the pelvic, liver, and abdominal regions. The CT scans (Figure 1) show that the liver was abnormally located in the abdominal midline (under normal circumstances, a large volume of the liver is located on the right side), and the biliary ducts and gallbladder were in their normal location without the presence of any stones. The aorta, pancreas, and kidneys were of normal size and in the normal locations, whereas the location of the appendix was not visible on the CT scan. A 90×90×85 mm cystic lesion was seen posterior to the bladder.
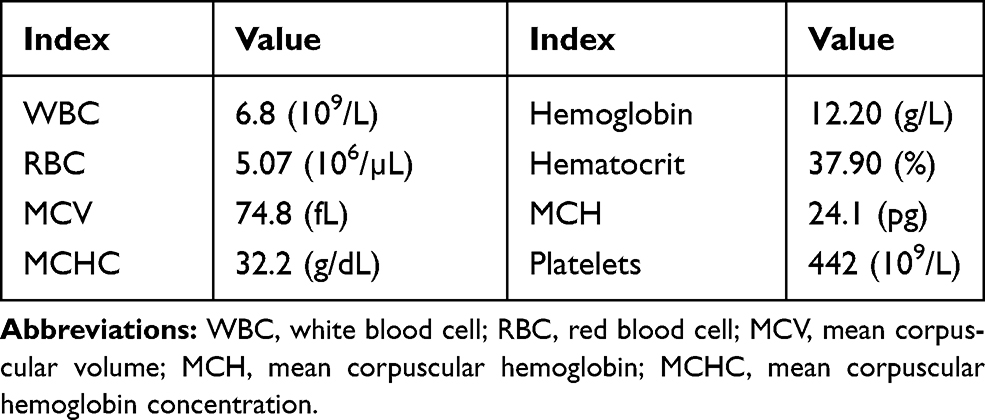 |
Table 1 Laboratory Findings of the Patient |
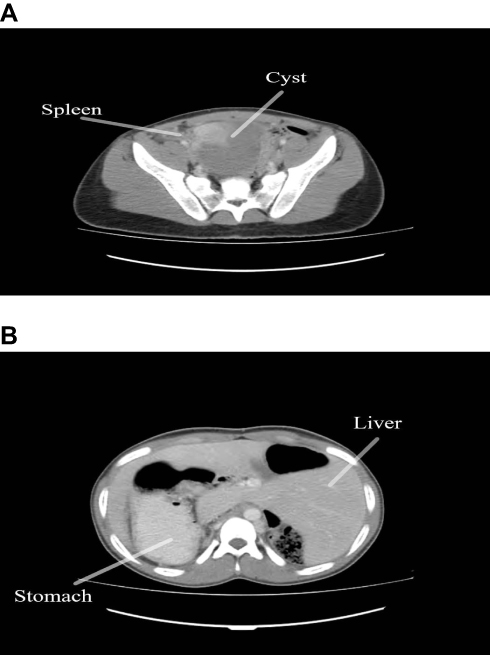 |
Figure 1 Abdominal CT scan. (A) Location of the cyst and the spleen in the pelvic area. (B) Location of the liver and stomach in the abdominal space. |
The spleen was not in its anatomical location; however, a cystic lesion with thin walls and size of 85×88×105 mm (similar to the size of the spleen) and solid content (30×30×47 mL), which was probably an ectopic spleen, was detected in the lower abdomen, attached to the omentum. Evidence of echogenic inflammation and edema in the RLQ and left lower quadrant was also seen. According to the findings, the patient underwent emergency laparotomy with the diagnosis of acute abdomen. The abdomen was incised in the midline. The kidneys were in their proper location and the intestine was in the center of the body. The stomach was oriented to the right upper abdominal region (under normal circumstances, the bulk of the stomach tends slightly to the left) and the liver was oriented to the abdominal midline (normally, the bulk of the liver is located in the right upper quadrant [RUQ]). The appendix was seen in the RUQ (normally, the appendix is located in the RLQ), and a large, thrombosed cystic mass attached to the omentum (with a blood supply from the omentum; normally, the splenic artery is responsible for the blood supply to the spleen), twisted around its axis (clockwise), was seen (Figure 2). The mass and the appendix were resected, and the pelvis and abdomen were washed. After achieving hemostasis, the abdomen was sutured and dressed. The lesion was sent to the pathology laboratory. The pathological findings reported both the spleen and cyst. After surgery, the patient was vaccinated and there were no infectious complications after splenectomy. The patient was discharged in good condition after two days.
 |
Figure 2 Photo taken during surgery, showing the position of the wandering spleen in the pelvic area. |
Discussion
Wandering spleen is a rare condition. It is also known as ectopic spleen, misplaced spleen, or accessory spleen, and can be located anywhere in the abdominal cavity.2 An ectopic spleen hangs by its vascular base owing to the lack or looseness of its suspensory ligaments.4 The clinical symptoms of wandering spleen are diverse. Many patients are asymptomatic, and their ectopic spleen is diagnosed incidentally as an uncomplicated abdominal mass during a physical examination or imaging for other reasons.7 The patient may experience mild intermittent abdominal pain due to congestion of the spleen as it twists and untwists intermittently, or show the symptoms of acute abdomen due to the torsion and infraction of the spleen vascular base.3 Other clinical manifestations include nausea, vomiting, fever, leukocytosis, peritoneal stimulation signs, and a palpable pelvic or abdominal mass. The patient in the present study had a wandering spleen in the pelvic area attached to the omentum (with a blood supply from the omentum) with symptoms of severe pain in the abdomen, fever, nausea, vomiting, and lack of appetite.
Various imaging techniques can be used to diagnose ectopic spleen, including plain abdominal radiography, barium studies, scintigraphy, sonography, and CT scan.7 Sonography and CT scan can diagnose the comma-shaped spleen in an ectopic location in the absence of the spleen tissue in the left upper quadrant (LUQ). Sonography can show adjacent visceral involvement, such as the tail of the pancreas with variable echo, and this was the diagnostic technique used in the present study. However, intestinal gas limits the accuracy of sonography.8
Similarly to the treatment performed for the case reported in this study, the standard treatment of wandering spleen with torsion is splenectomy. Splenopexy is a less invasive surgical procedure.9 In 2008, a case of familial wandering spleen was reported in two sisters. It manifested in the first sister when she was 13 years old. Three years later, it manifested in the second sister when she was 12 years old. This is the only report of familial wandering spleen.10 The first sister underwent splenectomy due to the spleen infraction. However, this condition was diagnosed early in the second sister, and she underwent splenopexy.
Ectopic liver has been reported in less than 0.5% in various studies and can be reported as a rare case.11,12 For example, in a study by Pandit et al, a case of ectopic liver attached to the gallbladder (with separate bleeding from the liver) was reported.13 In the study by Doshi et al, a case of ectopic liver was reported in the intrathoracic space.14 All studies have shown that the ectopic liver is located in the abdomen or chest. In our study, the ectopic liver is such that a large volume of the liver is visible in the LUQ and the liver is seen in the midline of the abdomen, as shown in the CT scan of the patient.
In the absence of trauma, most cases of ectopic liver are rooted in congenital causes.15 Ectopic stomach, which is congenital, is seen in only 0.4–2% of the population, and its most common location is the jejunum and ileum.16,17 Numerous cases of ectopic stomach have been reported. For example, in Hazan’s study, ectopic stomach was seen in the intestine.18 In our study, according to the patient’s CT scan, the ectopic stomach is located in the RUQ of the abdomen. The presence of three ectopic organs, namely the stomach, spleen, and liver, makes our report different from most studies.
Conclusion
Wandering spleen should be borne in mind for patients presenting with a palpable intra-abdominal mass causing acute or intermittent abdominal symptoms. Emergency intervention is mandatory in cases with torsion. Treatment is almost always surgical, with either conventional or minimally invasive approaches.
Data Sharing Statement
The authors declare that they had full access to all of the data in this study, and the authors take complete responsibility for the integrity of the data. All original data are available in the Imam Khomeini Educational, Remedial Center, Jiroft University of Medical Sciences, Jiroft, Iran. Data used to support the findings of this study are available from the corresponding author upon request.
Ethics and Consent Statement
Based on the regulations of the department of research of the Jiroft University of Medical Science, institutional review board approval is not required for case reports.
Consent for Publication
Written informed consent has been provided by the patient and his father to have the case details and any accompanying images published.
Author Contributions
All authors made substantial contributions to acquisition of data, or analysis, conception and design, and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Hemmati H. Acute torsion of wandering spleen: report of one case. Koomesh. 2009;11(1):71–74.
2. Misawa T, Yoshida K, Shiba H, Kobayashi S, Yanaga K. Wandering spleen with chronic torsion. Am J Surg. 2008;195(4):504–505. doi:10.1016/j.amjsurg.2006.08.083
3. Tan H, Ooi L, Tan D, Tan C. Recurrent abdominal pain in a woman with a wandering spleen. Singapore Med J. 2007;48(4):e122–e124.
4. Alawi MH, Khalifa A, Bana SH. Wandering spleen: a challenging diagnosis. Pak J Med Sci. 2005;21(4):482.
5. Alimoglu O, Sahin M, Akdag M. Torsion of a wandering spleen presenting with acute abdomen: a case report. Acta Chir Belg. 2004;104(2):221–223. doi:10.1080/00015458.2004.11679541
6. Fonseca AZ, Ribeiro M
7. Ely AB, Zissin R, Copel L, et al. The wandering spleen: CT findings and possible pitfalls in diagnosis. Clin Radiol. 2006;61(11):954–958. doi:10.1016/j.crad.2006.06.007
8. Arda K, Kizilkanat K, Celik M, Turkalp E. Intermittent torsion of a wandering spleen in a child: the role of MRI in diagnosis. JBR-BTR. 2004;87(2):70–72.
9. Palanivelu C, Rangarajan M, Senthilkumar R, Parthasarathi R, Kavalakat AJ. Laparoscopic mesh splenopexy (sandwich technique) for wandering spleen. JSLS. 2007;11(2):246.
10. Ely AB, Seguier E, Lotan G, Strauss S, Gayer G. Familial wandering spleen: a first instance. J Pediatr Surg. 2008;43(5):e23–e25. doi:10.1016/j.jpedsurg.2007.12.077
11. Watanabe M, Matsura T, Takatori Y, et al. Five cases of ectopic liver and a case of accessory lobe of the liver. Endoscopy. 1989;21(01):39–42.
12. Asada K, Onji M, Yamashita Y, et al. Ectopic liver observed by peritoneoscopy: report of a case. Gastroenterol Endosc. 1982;24(2):309–315.
13. Pandit N, Sah R, Lacoul R. Ectopic liver tissue on the gallbladder: a rare incidental finding. Indian J Surg. 2019;81(1):94–95.
14. Doshi A, Shah D, Gupta S, et al. A rare case of an ectopic liver presenting as right atrial mass. Case Rep Cardiol. 2019;2019.
15. Trocciola SM, Balsam LB, Yee H, Gianos E, Srichai MB, DeAnda A
16. Nawaz K, Graham DY, Fechner RE, Eiband JM. Gastric heterotopia in the ileum with ulceration and chronic bleeding. Gastroenterology. 1974;66(1):113–117.
17. Fang Y, Chen L, Chen D-F, et al. Prevalence, histologic and clinical characteristics of heterotopic gastric mucosa in Chinese patients. World J Gastroenterol. 2014;20(46):17588.
18. Hazan S. Thinking outside the box: visualization of an ectopic stomach via surgically advanced endoscopy at site of intussusception. ACG Case Rep J. 2019;6(10).
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.