Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Tooth-Bone-Borne vs Bone-Borne Rapid Maxillary Expanders on Dentoskeletal Changes
Authors Echarri-Nicolás J, González-Olmo MJ ![]() , Echarri-Lobiondo P, Lagravère M, Romero M
, Echarri-Lobiondo P, Lagravère M, Romero M
Received 21 January 2024
Accepted for publication 22 April 2024
Published 29 April 2024 Volume 2024:17 Pages 1877—1886
DOI https://doi.org/10.2147/JMDH.S433693
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Javier Echarri-Nicolás,1 María José González-Olmo,2 Pablo Echarri-Lobiondo,3 Manuel Lagravère,4 Martin Romero2
1Doctoral Program in Health Sciences, International PhD School, Rey Juan Carlos University (URJC), Móstoles, Madrid, Spain; 2Department of Orthodontics, University Rey Juan Carlos, Alcorcón, Madrid, Spain; 3Athenea Dental Institute, San Jorge University, Zaragoza, Spain; 4Division of Orthodontics, Faculty of Dentistry, University of Alberta, Edmonton, Alberta, Canada
Correspondence: María José González-Olmo, Department of Orthodontics, University Rey Juan Carlos, Avda de Atenas s/n 28922, Alcorcón, Madrid, Spain, Email [email protected]
Purpose: This study compared the insertion and thickness of the cortical bone, the parallelism of the midpalatal suture, and the skeletal transverse dimension using a microimplant-assisted rapid palatal expansion (MARPE) with those produced by bone-anchored maxillary expander (BAME) in adults.
Patients and Methods: The sample comprised 18 patients (mean age, 29.9± 9.4 years) selected for the MARPE group and 18 (mean age 24.8± 6.8 years) selected for the BAME group. Cone-Beam computed tomography scans taken just before and after the expansion.
Results: After treatment, there was a significant palatal depth decrease. In addition, maxillary and mandibular width were increased in both groups. Regarding the cortical bone insertion and cortical bone width, it is shown an increase in both groups but those changes are not significant. However, the anterior suture opening effect occurs more frequently in the BAME than in the MARPE device. There are no differences in the frequency of opening of the midpalatal suture in the cases treated with MARPE and BAME, in both cases the most frequent opening morphology is parallel, independently of midpalatal suture maturation.
Conclusion: There are no differences in the use of MARPE or BAME in the parallelism of the middle palatal suture, the cortical bone insertion, and thickness according to the maturation stages of the midpalatal suture but significantly increases the transverse dimensions of the maxillary skeleton.
Keywords: 3D-scanner, CT, microimplant, expansion
Introduction
The microimplant-assisted rapid palatal expansion (MARPE) technique was described by Dr Won Moon in 2013 and consists of a tooth-bone-borne appliance with a retention using four bicortical microscrews from the palatal cortical bone to the nasal floor.1 The microscrews are inserted into the posterior area of the palate, regardless of the age or sex of the patient. Its advantage is that it reduces the load applied by the appliance to the vestibular periodontal ligament of the anchoring teeth. In 2013, the bone-anchored maxillary expansion (BAME) concept described by Winsauer et al2 was introduced. It is an expansion screw attached to four or six microimplants in the palatal area without tooth support.
Complications with microscrew-assisted separators tend to arise when orthopedic forces are applied in the vicinity of the maxillary, frontal maxillary, and frontal zygomatic-maxillary buttresses in patients who have already completed midpalatal suture ossification.
Various investigations have been carried out to compare the results in the airway,3 periodontal, dentoalveolar, and skeletal changes.4–7 Other authors have also been compared to tooth-supported and BAME expanders; three-dimensional dental and skeletal changes,8–11 and periodontal effects.12 The effects of MARPE and BAME devices on patients previously treated with Surgical Assisted Rapid Palatal Expansion (SARPE) have also been compared.7,13 Only Canan and Senisik,14 Moon et al15 and Bazzani et al16 have compared MARPE and BAME therapies.
Although these investigations have compared the therapeutic effects of MARPE and BAME on tooth expansion, labiolingual angulation changes,14,15 and skeletal expansion,15,16 there are still no articles that link the maxillary and mandibular skeletal expansion, palatal depth, and the morphology of the midpalatal suture after expansion in adults treated with MARPE and BAME, taking into account the ossification stage17 of the midpalatal suture and measured with cone beam computed tomography (CBCT) techniques.
In this context, this article has two main objectives: The primary objective is to compare the insertion (described as the distance between the buccal cortical bone and the cementoenamel junction) and thickness (described as the distance from the furca of the upper first molar to the most external point of the labial cortical bone) of the cortical bone of the upper first molar, the parallelism of the midpalatal suture, and the skeletal transverse dimension using a MARPE and BAME expansion therapy. The secondary objective is to compare the differences in palatal suture opening morphology using MARPE and BAME. The third objective is to evaluate if the maturation stage of the midpalatal suture conditions the morphology of the suture opening with microimplant-assisted expansion therapy.
This article has a significant clinical implication for orthodontists, because it provides information on which expansion therapy is most beneficial at the skeletal and periodontal level, as well as what type of morphology of midpalatal suture opening is obtained with each type of appliance.
Materials and Methods
Design and Participants
Patients' data were involved retrospectively. Those patients were under treatment with MARPE (Figure 1) or BAME (Figure 2) in private dental office (xxxx) from September 2021 to March 2023 were involved.
 |
Figure 1 MARPE (microimplant assisted rapid palatal expansion). |
 |
Figure 2 BAME (bone-anchored maxillary expansion). |
The study’s inclusion criteria comprised adult patients with maxillary compression who were suitable for surgery and intended to undergo maxillary expansion treatment with the assistance of microimplants. Exclusion criteria encompassed patients with craniofacial malformations, fissured palates, those unwilling to accept orthodontic treatment, or those who declined participation or refused to provide informed consent.
Demographic data and sample images were utilized, with all information anonymized.
The sample size was determined using Jamovi 2.3.18, as there were no previous studies comparing skeletal changes between BAME and MARPE techniques. Sample size calculations were based on findings from a pilot study involving ten patients. The calculated mean ± standard deviation (SD) for maxillary width change was 1.96 mm ± 0.22 for BAME and 2.31 mm ± 0.35 for MARPE. By employing a two-tailed test with an alpha risk of 0.05 and a beta risk of 0.2 for bilateral contrast, it was estimated that 16 subjects per group would be required to detect a difference of 0.35 mm or greater. Consequently, 36 subjects were selected and divided evenly between the MARPE and BAME therapy groups, each containing 18 subjects.
Procedure and Measurements
Palalign Round Head Type microimplants (manufactured by Osteonic Co. Ltd., Seoul, Republic of Korea), made from Ti6Al4V alloy, were employed with a diameter of 1.8 mm and lengths of 10, 12, 14, or 16 mm, depending on the specific case. The use of bicortical placement has been emphasized as it is essential for enhancing stability and minimizing the risk of microimplant deformation and fractures.18 An expansion screw of Power MARPE Type 1 (also from Osteonic Co Ltd., Seoul, Republic of Korea) was utilized, and it was activated at a rate of four turns per day until the interincisal diastema became apparent. Subsequently, the activation rate was adjusted to two turns per day until a 1.5 mm overcorrection per side was achieved. Both in MARPE and BAME devices appliances have been used a Power MARPE Type 1 expansion screw. In MARPE design, it was used a molar bands in both upper first molars and anterior bonded arms to palatal surfaces of first and second bicuspids. In BAME design, it was used just the expansion screw so a transfer surgical tray is needed during microimplants placement. All orthodontic treatments were consistently administered by the same orthodontist. All patients were informed about the specifics of the orthodontic procedure and signed the informed to be part of this study. The study protocol was reviewed and approved by the Rey Juan Carlos University Ethics Committee with internal number (1504202110721).
A CT-type radiographic scan was conducted on the patient using a NewTom Giano HR scanner (QR, Verona, Italy) with a voxel size of 300 μm and a field of view (FOV) measuring 16×18 cm. This imaging procedure was performed both prior to and following the application of either MARPE or BAME treatment, allowing for the subsequent calculation of various indicators based on the 3D X-ray images acquired at the two time points, denoted as T0 (before treatment) and T1 (after treatment) (see Table 1, Figures 3 and 4). The morphology of the midpalatal suture opening was studied by measuring the aperture at the level of incisive foramen and at the level of posterior nasal spine. A parallel opening of the midpalatal suture is considered when the openings at the level of the incisive foramen and at the level of the posterior nasal spine were equal; an anterior opening is considered when the measurement at the level of the incisive foramen was greater, and a posterior opening is considered when the opening at the level of the posterior nasal spine was greater. The time elapsed between these two measurements averaged 1.5 months.
 |
Table 1 Indicators |
 |
Figure 3 Indicator measurements. |
 |
Figure 4 Axial CBCT-slice of the midpalatal suture opening. |
Statistical Analysis
All statistical analyses were performed using SPSS version 28.0 for Windows (IBM, Armonk, NY). The data analysis included Kolmogorov–Smirnov test to evaluate the assumption of normality, which was confirmed. A descriptive analysis was conducted to present sample characteristics, including age, gender, appliance type, suture maturation stage, and the type of suture opening achieved post-treatment. The intraclass correlation coefficient (ICC) was calculated considering ICC < 0.4 as low, between 0.4 and 0.75 as acceptable and >0.75 as high. Each indicator was measured three times at each investigation time, and measurement errors were determined. A paired sample t-test was subsequently utilized to assess changes in bone measurements from T0 to T1 for both MARPE and BAME treatments. Furthermore, a Student’s t-test was employed to compare bone measurement changes between MARPE and BAME. The effect of the sample on the mean differences in the t-test was analyzed using Cohen’s d, with effects classified as low at d ≈ 0.2, medium at d ≈ 0.5, and high at d ≈ 0.8.19
Results
General Descriptive Analysis
The sample comprised 36 subjects, with 41.7% being male and 58.3% female. The subjects’ mean age was 27.42±8.53, ranging from 18 to 49 years. Both the MARPE and BAME techniques were each used in 50% of the cases. In terms of device type and gender, MARPE was applied to 60% of male subjects, while BAME was employed for the remaining 40%. For female subjects, MARPE was used in 42.9% of cases, and BAME was chosen for the remaining 57.1%. There were no significant differences in gender distribution (χ² (1)=1.029; p=0.310). All patients presented suture opening confirmed through the CBCT taken after expansion on every patient.
The distribution of subjects according to the maturation stage of midpalatal suture according to Angelieri et al17 was: in stage B, BAME was placed in 1 subject and MARPE was placed in 2 subjects; in stage C, MARPE was placed in 3 subjects and BAME in 6 subjects, in stage D, MARPE was placed in 7 subjects and BAME in 4 subjects and in stage E, MARPE was placed in 7 subjects and BAME in 6 subjects. No differences were found in the distribution by stage of suture maturation in T0 (X (3)=2.228; p=0.526)
Regarding the type of expansion, a parallel expansion was obtained in 72.2% of the treated cases, a greater anterior expansion was obtained in 7 cases (19.4%), and more posterior expansion was observed in 3 cases (8.3%).
This study presents an ICC > 0.9 in the evaluations carried out (see Table 2).
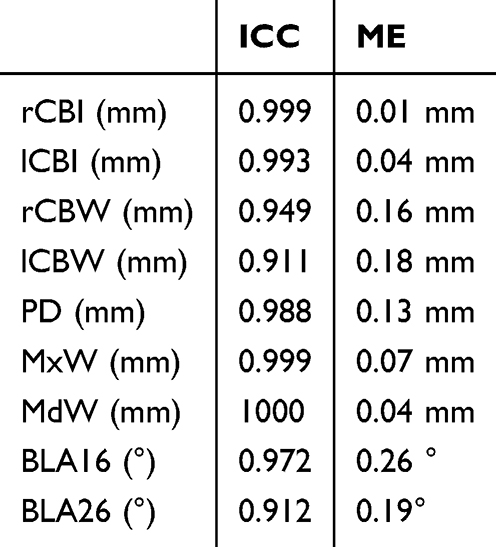 |
Table 2 Intraclass Correlation Coefficiency and Measurement Error |
To evaluate the similarity between groups at T0, age was compared (MARPE: 29.9±9.4 and BAME: 24.8±6.8; t=1.83, p=0.076) finding no significant differences. As can be seen in Table 3, an analysis of the clinical variables was performed at T0, in terms of cortical bone insertion, cortical bone width, maxillary width, mandibular width, palatal depth and buccolingual angulation in upper molars, no differences were found between MARPE and BAME at T0.
 |
Table 3 Descriptive and Comparative Analysis of Cortical Bone Insertion, Cortical Bone Thickness, Maxillary Transverse Dimension, Mandibular Transverse Dimension and Palatal Depth in T0 for MARPE and BAME Appliance |
Comparison of Bone Measurements at T0–T1 in Patients Treated with MARPE and BAME
After treatment, there was a significant palatal depth decrease in both group (P < 0.05). In addition, maxillary and mandibular width were increased (P < 0.01) in both groups. In both groups, similar data were obtained for all variables except for maxillary width, which was slightly higher in the BAME group (MARPE = 2.84±1.91; BAME = 2.2±2.08). Regarding the cortical bone insertion and cortical bone width, it is shown an increase in both groups but those changes are not significant. (Tables 4 and 5)
 |
Table 4 Descriptive and Comparative Analysis of Cortical Bone Insertion, Cortical Bone Thickness, Maxillary Transverse Dimension, Mandibular Transverse Dimension and Palatal Depth in T0, T1 and T1-T0 for MARPE Appliance |
 |
Table 5 Descriptive and Comparative Analysis of Cortical Bone Insertion, Cortical Bone Thickness, Maxillary Transverse Dimension, Mandibular Transverse Dimension and Palatal Depth in T0, T1 and T1-T0 for BAME Appliance |
When comparing the results obtained in the treatment with these two therapies, no significant differences were found (Table 6).
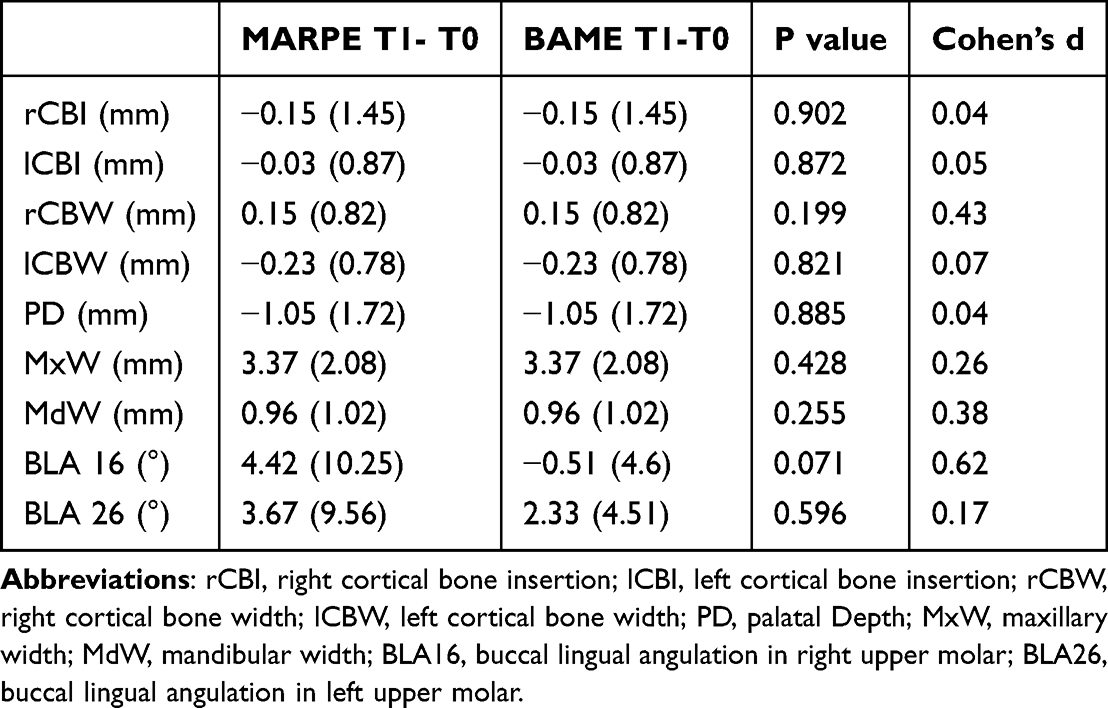 |
Table 6 Comparative Analysis of Changes in Cortical Bone Insertion, Cortical Bone Thickness, Maxillary Transverse Dimension, Mandibular Transverse Dimension and Palatal Depth for the MARPE and BAME Appliances |
Midpalatal Suture Expansion Type and Maturation According Device Therapy (MARPE VS BAME)
There are no differences in the frequency of opening of the midpalatal suture in the patients treated using the MARPE and BAME methods (see Table 7). In both cases, the most frequent opening morphology is parallel, for MARPE 15 cases (83.3%) and in BAME 11 cases (61.1%) showed a parallel opening of the suture (see Table 7). Midpalatal suture expansion type and maturation stage of the suture.
 |
Table 7 MARPE Vs BAME Expansion Type |
The midpalatal suture expansion type was studied according to the maturation stage described by Angelieri et al.17 Parallel expansion of the midpalatal suture was observed in most cases at all maturation stages (see Table 8).
 |
Table 8 Type of Expansion According to the Maturation Stage (Angelieri)17 |
Discussion
The objectives of this research were to study the skeletal and periodontal changes of adult patients with maxillary compression treated with MARPE and BAME. For this study, the different measurements were made in the CBCT taken before (T0) and after (T1) the maxillary expansion therapy.
In the literature,12,20 bone insertion in the first molars has also been measured, although in a different way. In the study carried out by Jia et al,20 a −0.41±0.95 mm decrease in bone height was obtained at the level of the upper right first molar, and −0.79±0.98 mm at the level of the left one, although it was only significant in the left molars. Instead, Garib et al12 concluded that therapy with conventional expanders reduces the buccal bone width of posterior teeth. In this study, a slight increase[A1] in buccal bone width was observed in both groups. These changes in the results can be attributed to the age difference in the sample group.
Regarding the cortical bone width, Toklu et al4 conducted a prospective study on 25 patients with maxillary compression, of which 13 underwent tooth-supported expansion, and 12 underwent a MARPE expansion. Three-dimensional radiographic records were taken before the expansion and 3 months after the expansion, concluding that the patients showed a decrease of buccal cortical bone width at the level of molars in both groups. In the MARPE-treated patient group in this study, a decrease was observed at the level of the upper right first molar and an increase in the first left molar. In the BAME-treated patient group in this study, a decrease of cortical bone width was observed at the level of the upper right and left first molar. These changes in the outcomes may be attributable to the age difference in the sample group, the different location and number of microimplants in the MARPE group used in each study, and the different methods used to measure the periodontal changes.
Although the importance of achieving a bicortical placement of the microimplants from the palatal vault to the nasal floor has been described as essential,18,21 few articles have described the morphological changes undergone by the palatal complex in the microimplant-assisted expansion. Kurt et al22 compared 18 young patients treated with RME, 18 non-growing patients treated with RME, and 18 patients treated with surgically assisted RME (SARME). Regarding the morphology of the palatal vault, the angle between the tangent lines to the right and left palatal surfaces was calculated. In the three groups, an increase of this angle was found to be less in growing patients. This research follows the line of these results, because the palatal height decreased, and this decrease was −1.12±1.65 mm in MARPE-treated patients and −1.04±1.72 mm in BAME-treated patients.18,21,22
The increase of skeletal transverse dimension was to be expected in microimplant-assisted rapid maxillary expansion therapy, something that has already been confirmed by previous literature.4,7,9,20,23,24 This study shows that patients treated with RPE assisted with microimplants obtained a statistically significant increase in maxillary transverse dimension. The results of this study show a similar increase in patients treated with MARPE and BAME, coinciding with the conclusions drawn from the systematic review of Khosravi et al.9 An increase in maxillary and mandibular transverse dimension was observed in both MARPE- and BAME-treated patients, but being slightly higher in the second group.
This article also studied the anteroposterior parallelism of the midpalatal suture opening, whether it was parallel, more anterior, or more posterior. The symmetrical separation of the midpalatal suture was shown in most MARPE-treated cases (83.3%), and it was lower in the BAME-treated cases (61.1%). There were no differences in the maturation stage of Angelieri et al.17 Parallel expansion was always present in the majority of cases. There is no consensus in the literature about the morphology in the midpalatal suture expansion in MARPE-treated patients. There is scientific evidence for obtaining parallel anterior-posterior and superior-inferior expansion;4,22,23 there is also scientific evidence for V-shaped expansion,7,25 but measured in the horizontal plane.
The significance of this study’s findings should be considered in light of its limitations. The data provided in this research should be approached with care because of the relatively small sample size, wide age range, and significant variability in suture maturation. The observational period of the results was also short, and a measurement after removal of the device may prove useful to corroborate the stability of the results. With respect to periodontal measurements, an investigation performed using a periodontal probe may be more beneficial than measurements obtained from CBCT.
Both techniques are effective for the treatment of maxillary transverse discrepancy, because it is possible to increase the maxillary skeletal width maintaining both the cortical width and the cortical insertion at the level of the upper first molar, using both techniques. Although all patients had suture opening, most patients had suture opening in parallel morphology. Therapeutic decision-making should be at the discretion of each specialist, and the particularities of each patient must be considered.
Conclusions
Both MARPE and BAME, regardless of the type of suture maturation, significantly increase the maxillary skeletal transverse dimension. In most cases, the midpalatal suture opens in parallel, increasing the maxillary transverse dimension, minimally increasing bone insertion and minimally decreasing bone width.
Acknowledgments
The authors acknowledge patients who have participated in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Moon W. An interview with Won Moon. Dental Press J Orthod. 2013;18(3):12–28.
2. Winsauer H, Vlachojannis J, Winsauer C, et al. A bone-borne appliance for rapid maxillary expansion. J Clin Orthod. 2013;47(6):375–388.
3. Kabalan O, Gordon J, Heo G, et al. Nasal airway changes in bone-borne and tooth-borne rapid maxillary expansion treatments. Int Orthod. 2015;13(1):1–15. doi:10.1016/j.ortho.2014.12.011
4. Toklu MG, Germec-Cakan D, Tozlu M. Periodontal, dentoalveolar, and skeletal effects of tooth-borne and tooth-bone-borne expansion appliances. Am J Orthod Dentofacial Orthop. 2015;148(1):97–109. doi:10.1016/j.ajodo.2015.02.022
5. Bazargani F, Lund H, Magnuson A, et al. Skeletal and dentoalveolar effects using tooth-borne and tooth-bone-borne RME appliances: a randomized controlled trial with 1-year follow-up. Eur J Orthod. 2021;43(3):245–253. doi:10.1093/ejo/cjaa040
6. Kayalar E, Schauseil M, Kuvat SV, et al. Comparison of tooth-borne and hybrid devices in surgically assisted rapid maxillary expansion: a randomized clinical cone-beam computed tomography study. J Craniomaxillofac Surg. 2016;44(3):285–293. doi:10.1016/j.jcms.2015.12.001
7. Zandi M, Miresmaeili A, Heidari A. Short-term skeletal and dental changes following bone-borne versus tooth-borne surgically assisted rapid maxillary expansion: a randomized clinical trial study. J Craniomaxillofac Surg. 2014;42(7):1190–1195. doi:10.1016/j.jcms.2014.02.007
8. Lagravère MO, Carey JP, Heo G, et al. Transverse, vertical, and anteroposterior changes from bone-anchored maxillary expansion vs traditional rapid maxillary expansion: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 2010;137(3):304–305. doi:10.1016/j.ajodo.2009.10.004
9. Khosravi M, Ugolini A, Miresmaeili A, et al. Tooth-borne versus bone-borne rapid maxillary expansion for transverse maxillary deficiency: a systematic review. Int Orthod. 2019;17(3):425–436. doi:10.1016/j.ortho.2019.06.003
10. Lin L, Ahn HW, Kim SJ, et al. Tooth-borne vs bone-borne rapid maxillary expanders in late adolescence. Angle Orthod. 2015;85(2):253–262. doi:10.2319/030514-156.1
11. Lagravère MO, Gamble J, Major PW, et al. Transverse dental changes after tooth-borne and bone-borne maxillary expansion. Int Orthod. 2013;11(1):21–34. doi:10.1016/j.ortho.2012.12.003
12. Garib DG, Henriques JFC, Janson G, et al. Periodontal effects of rapid maxillary expansion with tooth-tissue-borne and tooth-borne expanders: a computed tomography evaluation. Am J Orthod Dentofacial Orthop. 2006;129(6):749–758. doi:10.1016/j.ajodo.2006.02.021
13. Koudstaal MJ, Smeets JBJ, Kleinrensink GJ, et al. Relapse and stability of surgically assisted rapid maxillary expansion: an anatomic biomechanical study. J Oral Maxillofac Surg. 2009;67(1):10–14. doi:10.1016/j.joms.2007.11.026
14. Canan S, Şenışık NE. Comparison of the treatment effects of different rapid maxillary expansion devices on the maxilla and the mandible. Part 1: evaluation of dentoalveolar changes. Am J Orthod Dentofacial Orthop. 2017;151(6):1125–1138. doi:10.1016/j.ajodo.2016.11.022
15. Moon HW, Kim MJ, Ahn H-W, et al. Molar Inclination and surrounding alveolar bone change relative to the design of bone-borne maxillary expanders: a CBCT study. Angle Orthod. 2020;90(1):13–22. doi:10.2319/050619-316.1
16. Bazzani M, Cevidanes LHS, Al Turkestani NN, et al. Three-dimensional comparison of bone-borne and tooth-bone-borne maxillary expansion in young adults with maxillary skeletal deficiency. Orthod Craniofac Res. 2022;26(2):1–12.
17. Angelieri F, Cevidanes LHS, Franchi L, et al. Midpalatal suture maturation: classification method for individual assessment before rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2013;144(5):759–769. doi:10.1016/j.ajodo.2013.04.022
18. Lee RJ, Moon W, Hong C. Effects of monocortical and bicortical mini-implant Anchorage on bone-borne palatal expansion using finite element analysis. Am J Orthod Dentofacial Orthop. 2017;151(5):887–897. doi:10.1016/j.ajodo.2016.10.025
19. Cohen JM. Statistical Power Analysis for the Behavioral Sciences. Lawrence Eribaum Associates Publishers; 1988.
20. Jia H, Zhuang L, Zhang N, et al. Comparison of skeletal maxillary transverse deficiency treated by microimplant-assisted rapid palatal expansion and tooth-borne expansion during the post-pubertal growth spurt stage: a prospective cone beam computed tomography study. Angle Orthod. 2021;91(1):36–45. doi:10.2319/041920-332.1
21. Cantarella D, Savio G, Grigolato L, et al. A new methodology for the digital planning of micro-implant-supported maxillary skeletal expansion. Med Devices. 2020;13:93–106. doi:10.2147/MDER.S247751
22. Kurt G, Altuǧ AT, Türker G, et al. Effects of surgical and nonsurgical rapid maxillary expansion on palatal structures. J Craniofac Surg. 2017;28(3):775–780. doi:10.1097/SCS.0000000000003468
23. de Oliveira CB, Ayub P, Ledra IM, et al. Microimplant assisted rapid palatal expansion vs surgically assisted rapid palatal expansion for maxillary transverse discrepancy treatment. Am J Orthod Dentofacial Orthop. 2021;159(6):733–742. doi:10.1016/j.ajodo.2020.03.024
24. Carlson C, Sung J, McComb RW, et al. Microimplant-assisted rapid palatal expansion appliance to orthopedically correct transverse maxillary deficiency in an adult. Am J Orthod Dentofacial Orthop. 2016;149(5):716–728. doi:10.1016/j.ajodo.2015.04.043
25. Deeb W, Hansen L, Hotan T, Hietschold V, Harzer W, Tausche E. Changes in nasal volume after surgically assisted bone-borne rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2010;137(6):782–789. doi:10.1016/j.ajodo.2009.03.042
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.