Back to Journals » Journal of Inflammation Research » Volume 15
TNF-α is a Novel Biomarker for Predicting Plaque Rupture in Patients with ST-Segment Elevation Myocardial Infarction
Authors Luo X ![]() , Zhao C
, Zhao C ![]() , Wang S, Jia H, Yu B
, Wang S, Jia H, Yu B
Received 4 December 2021
Accepted for publication 14 February 2022
Published 14 March 2022 Volume 2022:15 Pages 1889—1898
DOI https://doi.org/10.2147/JIR.S352509
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monika Sharma
Xing Luo,1,2 Chen Zhao,1,2 Shengfang Wang,1,2 Haibo Jia,1,2 Bo Yu1,2
1Department of Cardiology, 2nd Affiliated Hospital of Harbin Medical University, Harbin, 150001, People’s Republic of China; 2Key Laboratory of Myocardial Ischemia, Ministry of Education, Harbin Medical University, Harbin, 150001, People’s Republic of China
Correspondence: Haibo Jia; Bo Yu, Tel/Fax +86 0451 86297221 ; +86 0451 86297220, Email [email protected]; [email protected]
Background and Aims: Patients with plaque rupture (PR) present with different cardiovascular risks, clinical strategies, and outcomes from those with plaque erosion (PE). However, there are lack of noninvasive biomarkers to distinguish PE from PR.
Methods: A prospective analysis of 382 patients with ST-segment elevation myocardial infarction (STEMI) was conducted. Of these patients, 262 and 120 presented with PR and PE, respectively. An additional 83 patients diagnosed with stable angina pectoris were enrolled as control group. Peripheral blood monocytes were collected pre-percutaneous coronary intervention and used to evaluate the mRNA expression of IL-4, IL-10, IL-1β, and TNF-α in all patients.
Results: STEMI patients had higher IL-4, IL-10, IL-1β, and TNF-α expression than the control patients. The mRNA levels of IL-4, IL-1β, and TNF-α were significantly higher in PR patients than PE; however, no significant difference was observed in IL-10 between PE and PR. The areas under the receiver-operating characteristic curves for IL-4, IL-1β, and TNF-α for PR versus PE were 0.685, 0.747, and 0.895, respectively. At the cut-off value of 2.52, TNF-α demonstrated a sensitivity of 70.61% and specificity of 93.33% for discriminating PR from PE patients. When added to the model of established clinical risk factors, TNF-α significantly improved the predictive accuracy of PR. Multivariable logistic regression analysis indicated that TNF-α mRNA level was independently associated with PR (odds ratio, 3.09; 95% confidence interval, 2.29– 4.16; p < 0.001).
Conclusion: The inflammatory response of peripheral blood mononuclear cells in patients with PR was higher than that in patients with PE. TNF-α may be a potential biomarker for predicting PR that could facilitate risk stratification and management in STEMI patients.
Keywords: acute coronary syndrome, plaque rupture, plaque erosion, inflammation, TNF-α
Graphical Abstract:

Introduction
Acute coronary syndrome (ACS) results from the sudden thrombotic occlusion of the coronary artery and is one of the most important cardiovascular diseases in humans. ACS can be divided into three common subtypes based on the pathological mechanism: plaque rupture (PR), plaque erosion (PE), and calcified nodules (CN).1 Our previous studies indicated that PR is the most common subtype of ACS, and accounts for approximately two-thirds of ACS cases, whereas PE has been found in approximately one-third of ACS cases.2 Current guidelines for the management of ACS generally recommend early percutaneous coronary intervention (PCI) and stent implantation to achieve reperfusion and revascularization.1 However, evidence from our group and Sugiyama’s group demonstrate that antithrombotic therapy, instead of stent implantation, may be safe and effective for some patients with PE. Furthermore, it was reported that the risk of major adverse cardiac events and complications was higher in patients with PR than in patients with PE.3–6 Thus, it is important to differentiate between PE and PR to establish a personalized treatment strategy and improve the prognosis of patients with ACS.
Serum biomarkers for predicting PE and PR have received considerable attention. Several studies have reported that serum levels of trimethylamine N-oxide (TMAO), myeloperoxidase (MPO), and microRNA-3667-3p are associated with plaque morphology and could be used as biomarkers for predicting PE or PR in patients with ACS.7–10 However, either the patient population in each study was too small to be conclusive or the results were unsatisfactory. Therefore, large sample size population trials and more accurate markers are needed to identify biomarkers for PR.
Autopsy and OCT studies demonstrate that culprit lesions from PR express a higher inflammatory response than those from PE.11,12 Nonetheless, the association between inflammatory factors and culprit lesion morphology in patients with ACS has not yet been investigated. Interleukin-4 (IL-4) and IL-10, and IL-1β and tumor necrosis factor-α (TNF-α) constitute two classic pairs of anti- and pro-inflammatory factors, respectively. Here, we first explored the IL-4, IL-10, IL-1β, and TNF-α mRNA expression in the monocytes from peripheral blood samples using quantitative RT-PCR and then analyzed the relationship between mRNA expression and plaque morphology as determined using OCT in patients with ST-segment elevation myocardial infarction (STEMI).
Materials and Methods
Study Population and Design
The study flow chart was shown in Supplemental Figure 1. Between August 2014 and April 2016, 466 STEMI patients underwent OCT examination were included in the study, 84 patients were excluded, and 382 patients were included in the final analysis. In addition, according to ESC guidelines (13), 83 patients diagnosed with stable angina pectoris served as controls group at same time. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki. The study was approved by the Harbin Medical University ethics committee, all the patients provided written informed consent. We prospectively enrolled 466 STEMI patients (EROSION study, ClinicalTrials.gov ID: NCT02041650) who underwent OCT examination in the Second Hospital of Harbin Medical University. The definition of STEMI and identification of the culprit lesion were described previously.5 STEMI was defined as typical chest pain, ST-segment–elevation >0.1 mV in at least 2 contiguous leads or new left bundle-branch block on the 18-lead ECG, and cardiac troponin values with at least one value above the upper reference. The patients with cardiac shock, congestive heart failure, end-stage renal disease, and coronary artery bypass graft were excluded.7 According to OCT image of culprit lesion, the patients were divided into PE and PR.
Optical Coherence Tomography Image Acquisition and Analysis
C7-XR OCT intravascular imaging system (OCT C7 Dragonfly, St. Jude Medical, St Paul, MN, USA) was used in this study. According to our previous study, OCT-erosion was identified by the presence of attached thrombus overlying an intact and visualized plaque, while OCT-rupture was identified by disruption of fibrous cap and cavity formation in the plaque.2 The typical image of PE and PR were shown in Supplemental Figure 2. All OCT images were analysis by 3 independent investigators blinded to the other data.
PCR Analysis
The blood samples were collected pre-PCI, and monocytes were separated by monocyte separation medium kit according to manufacturer’s instructions (Solarbio, China). And add 500ul trizol (Thermo Scientific, USA) into the monocytes for RNA extraction, the RNA concentration was evaluated by BioSpec-nano (SHIMADZU, Japan). The RNA quality which out of the range (OD260/280,1.6–2.2; OD260/230, 1.6–2.2) was excluded, and Reverse transcription kit (Roche, Switzerland) was used to reverse RNA to cDNA. The PCRs were amplified for 40 cycles (95°C for 10 seconds, 61°C for 30 seconds) on a 96-well CFX96 Real-Time System (BIO-RAD, Canada). mRNA analyzed for proinflammatory factor (IL-1β and TNF-α), and anti-inflammatory factor (IL-4, and IL-10). The sequences were designed in Universal Probe Library Assay Design Center and were shown in Supplemental Table 1. According to previous studies for the calculation of expression fold change, through the calculation of threshold cycle value (CT) value of each sample, the quantitative results are obtained according to 2−ΔΔCT methods. β-actin was regarded as the internal parameter.13,14
Statistical Analysis
Continuous data are presented as mean ± SD or median (interquartile range). The student t test or the Mann–Whitney U-test were used for statistical comparisons in two groups. Categorical variables are presented as count (percent), comparisons between groups were made with the χ2 or Fisher exact test. Hemoglobin and platelet count were transformed to binary variables based on above-median or below-median cut off values. A logistic regression model was used to evaluate the association between plaque classification and mRNA of TNF-α and was adjusted for all other baseline characteristics with p<0.10 on univariable analysis. Receiver-operating characteristic curve (ROC) was performed to evaluate the diagnostic accuracy in the detection of plaque characteristics for candidate mRNAs.
Results
Patient Characteristics and OCT Findings
Of the 466 STEMI patients who underwent OCT examination and were thus included in this study, 63 were excluded because of in-stent thrombosis (n = 13), neoatherosclerosis (n = 10), massive thrombus (n = 24), and poor imaging quality (n = 16). The remaining 403 patients were suitable for plaque morphology evaluation. Plaque morphology evaluation revealed that 262 of these patients had PR, and 120 had PE. The baseline data for the 382 STEMI patients and 89 control patients are summarized in Table 1 and Supplemental Table 2. The mean age in the PE cohort was 51.7 years; 75.8% of participants were males, 73.3% were current smokers, 9.2% had diabetes mellitus, and 16.7% had hypertension. Patients with PR were more likely to be older. Diabetes mellitus (p < 0.001) and hypertension (p < 0.001) were more frequent in patients with PR. The percentage of current smokers in the PR group was significantly lower than that in the PE group (42.4% versus 73.3%, p < 0.001). Additionally, there were no significant differences in the history of previous myocardial infarction, previous stroke, or sex between the two groups. Clinical laboratory examinations revealed that the PE group had a higher white blood cell count (p < 0.001), hemoglobin concentration (p < 0.001), and platelet count (p < 0.001), as well as higher blood lipid levels than the PR group. However, there was no significant difference in high-sensitivity C-reactive protein (hs-CRP) (p = 0.083) and creatinine (p = 0.088) levels between these two groups. In addition, preoperative medication was recorded. There was no significant difference in preoperative use of statins, angiotensin converting enzyme inhibitor (ACEI), double antiplatelet therapy (DAPT), angiotensin receptor blocker (ARB), calcium channel blocker (CCB) in PE and PR patients. The OCT findings are summarized in Supplemental Table 3. The results revealed that the length of the eroded plaques was significantly shorter than that of ruptured plaques (19.3 ± 6.5 mm versus 21.4 ± 6.8 mm, p = 0.003). Furthermore, the prevalence of lipid-rich plaques was higher in patients with plaque rupture (p < 0.001). In addition, thin cap fibroatheroma (TCFA), calcification, macrophages, and microchannels were all significantly less prevalent in the PE group when compared to the PR group. The minimal lumen area (MLA) was significantly larger in the eroded plaques than in the ruptured plaques (p < 0.001).
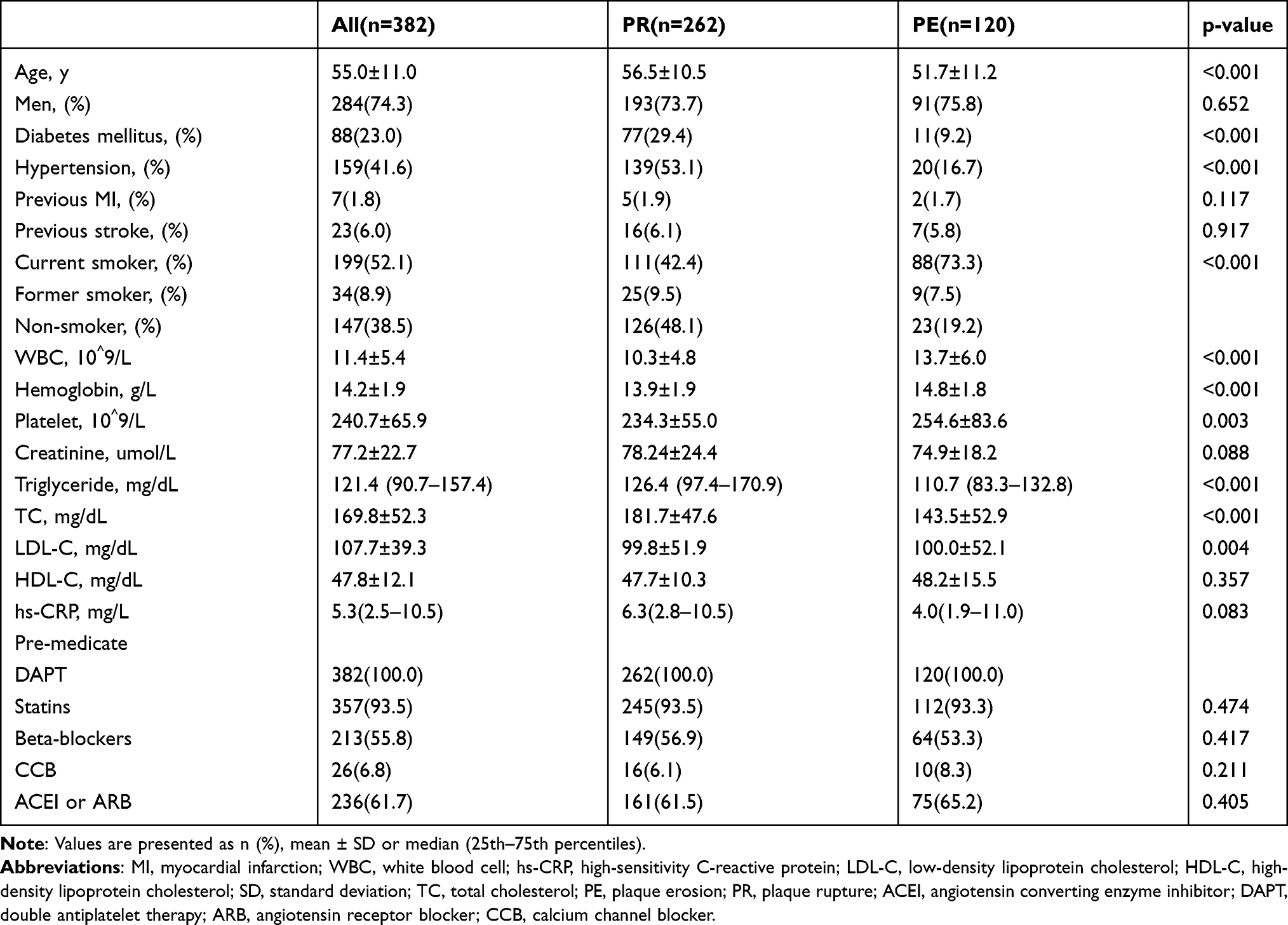 |
Table 1 Baseline Characteristics of PR and PE |
The Inflammatory Response in PR and PE Patients
We compared the mRNA expression profile for both anti-inflammatory factors (IL-4 and IL-10) and pro-inflammatory factors (IL-1β and TNF-α) in the monocytes from both PE and PR patients. Patients with STEMI exhibited increased expression for IL-4 (4.17-fold change, p < 0.001), IL-10 (2.59-fold change, p = 0.036), IL-1β (3.43-fold change, p < 0.001), and TNF-α (4.49-fold change, p < 0.001) compared to the controls (Supplemental Figure 3). In addition, patients with PR showed higher expression of IL-4 (3.35-fold change, p < 0.001), IL-1β (1.61-fold change, p = 0.012), and TNF-α (4.51-fold change, p < 0.001) than patients with PE (Figure 1). However, no significant difference was observed in IL-10 mRNA levels between these groups (P = 0.625). Additionally, a heat map of the inflammatory factors is shown in Supplemental Figure 4.
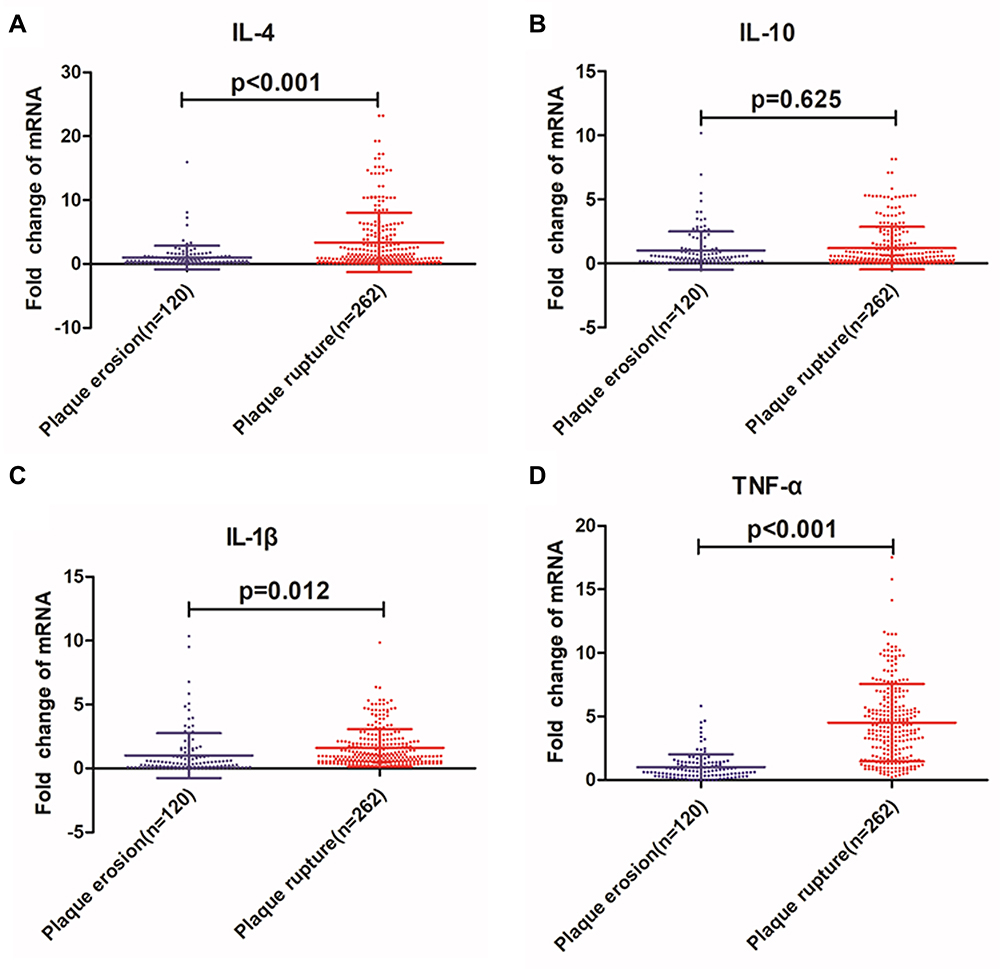 |
Figure 1 Comparison of IL-4, IL-10, IL-1β and TNF-α mRNA levels between patients with PR and those with PE. (A) IL-4 mRNA level in PE and PR (fold change). (B) IL-10 mRNA level in PE and PR (fold change). (C) IL-1β mRNA level in PE and PR (fold change). (D) TNF-α mRNA level in PE and PR (fold change). The data shown as mean ± SD. |
Diagnostic and Predictive Value of IL-4, IL-10, and TNF-α in Distinguishing PR from PE
Given the significant differences in the mRNA expression of IL-4, IL-10 and TNF-α between the PE and PR groups, we performed ROC curve analysis to evaluate the diagnostic value of IL-4, IL-10 and TNF-α in differentiating between PE and PR. The area under the ROC curve (AUC) for IL-4, IL-10 and TNF-α for PR versus PE was 0.685 (95% Cl, 0.631–0.739, p < 0.001), 0.747 (95% Cl, 0.686–0.809, p < 0.001), and 0.895 (95% Cl, 0.864–0.927, p < 0.001), respectively (Supplemental Figure 5). Furthermore, we found that TNF-α achieved a maximum sensitivity of 70.61% and specificity of 93.33% for PR when using a cutoff value of 2.52 (mRNA fold change) (Supplemental Table 4). Furthermore, we determined the extra predictive value of TNF-α as a risk factor for PR by completing several evaluations using the previously established risk factor model (all variables with p <0.10 in the univariate logistic regression). It was revealed that the AUC was significantly increased when TNF-α was added to the classical clinical risks for PR (0.85 versus 0.95) (Figure 2). Multivariable logistic regression demonstrated that the mRNA levels of TNF-α were independently correlated with PR (Table 2). Subgroup analysis (Figure 3) showed that the associations between TNF-α and PR were generally consistent across common clinical risk factors (age, sex, smoking status, diabetes, and dyslipidemia). In addition, IL-4 also showed a correlation with PR (Supplemental Table 5). To better understand the predictive power of TNF-α for PR, we divided our 382 STEMI patients into two groups based on their median TNF-α level, the incidence of PR risk factors (hypertension, diabetes mellitus, and dyslipidemia), and unique OCT features (TCFA and lipid-rich plaque) were compared between the two groups. The results (Supplemental Table 6) revealed that there was a higher proportion of patients with hypertension and diabetes in the high-TNF-α group than in the low-TNF-α group, and that patients with high TNF-α levels had worse lipid levels. As for OCT features, we found that, comparing to the low-TNF-α group, the high-TNF-α group had a higher proportion of TCFA, calcification and lipid-rich plaques, smaller MLA, and thinner fiber cap thickness, which is more similar to PR.
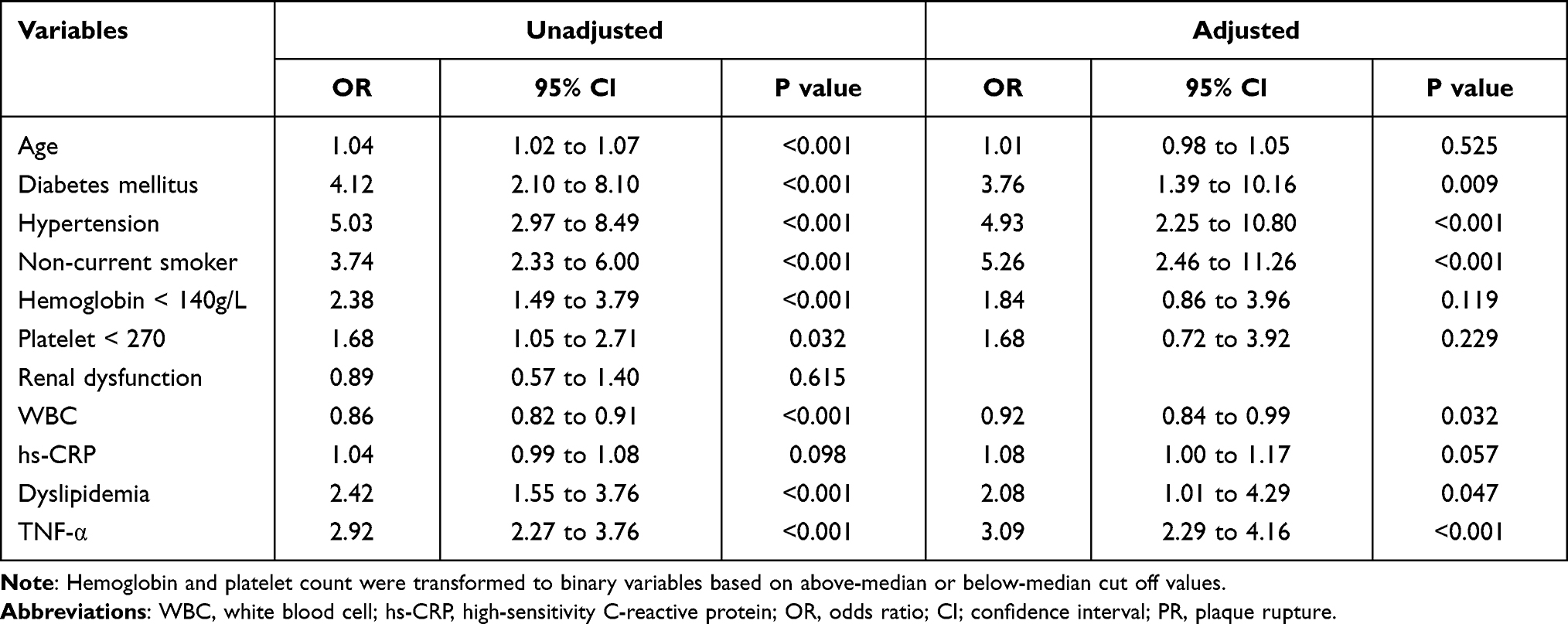 |
Table 2 Logistic Regression Analysis of PR |
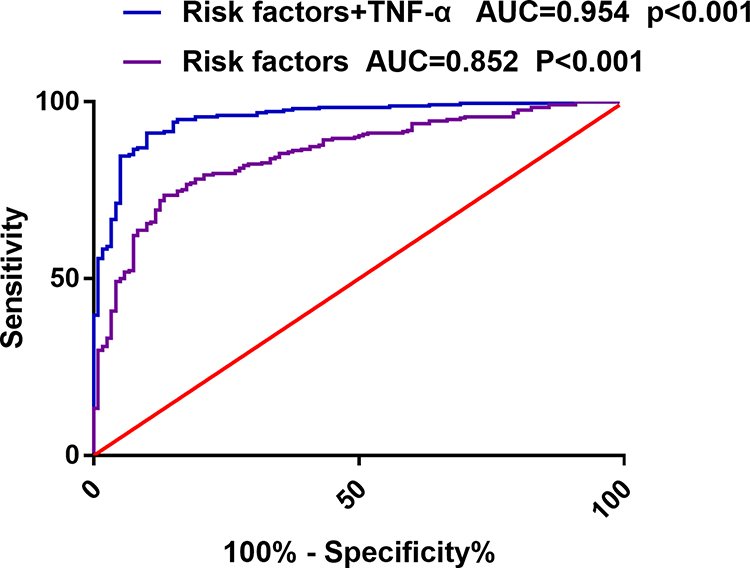 |
Figure 2 ROC curve for models of established cardiovascular risk factors with or without the incorporation of TNF-α level. |
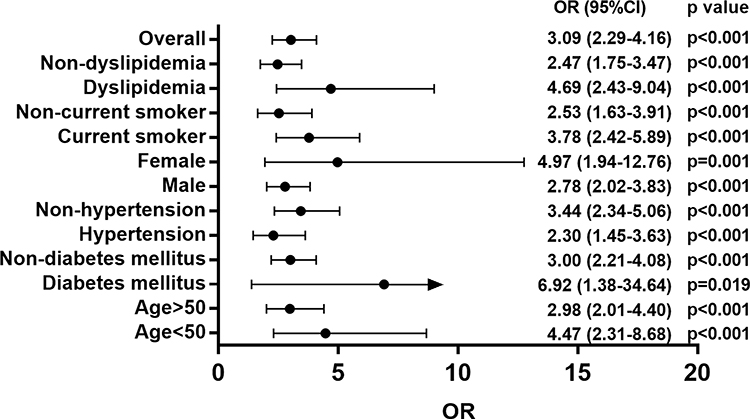 |
Figure 3 Subgroup analysis of TNF-α for predicting PR across common clinical risk factors. |
Discussion
The major findings of this study are as follows: (1) STEMI patients presented with increased IL-4, IL-10, IL-1β, and TNF-α mRNA levels in their blood monocytes than stable angina pectoris patients. Furthermore, PR patients expressed higher levels of IL-4, IL-1β, and TNF-α mRNA than PE patients, while there were no significant differences in IL-10 expression between these two groups. (2) STEMI patients with higher TNF-α expression (fold change >2.55) presented with more vulnerable plaque characteristics (larger mean lipid arc, thinner fibrous cap thickness, and more frequent TCFA and calcification), smaller MLA, and longer lipid length compared to those with lower TNF-α expression. (3) Elevated blood monocyte TNF-α mRNA levels independently correlated with PR and increased the diagnostic accuracy for PR when added to models of established clinical risk factors. (4) The AUC for IL-4, IL-1β, and TNF-α for PR versus PE was 0.685, 0.747, and 0.895, respectively, indicating that TNF-α mRNA in blood monocytes could be a potential biomarker for the discrimination of PR versus PE.
TNF-α as a Biomarker for PR
PR and PE are considered to be the two most important pathologic mechanisms of ACS, accounting for two-thirds and one-third of ACS cases, respectively.2 There is growing evidence suggesting that the risk of cardiovascular events is significantly higher in patients with PR than in those with PE.15 In addition, the optimal clinical management strategy for patients with PE may differ from that for patients with PR.1 To date, OCT is the only imaging method that can differentiate between PE and PR in vivo. Therefore, noninvasive differentiation between PE and PR is of great clinical significance for optimizing the treatment strategy and risk management of ACS.
Several recent studies have reported that clinical characteristics and laboratory tests can be used to discriminate between PR and PE. Jang and colleagues found that age <68 years, absence of diabetes mellitus, hemoglobin level >15.0 g/dL, and normal renal function are all independent parameters associated with PE.16 Furthermore, Dai et al reported that active smoking was significantly associated with PE.17 In this study, we found that patients with PE were younger than patients with PR and that diabetes mellitus, dyslipidemia, and hypertension were more frequent in the PR group than in the PE group. Subsequent multivariable logistic regression analysis demonstrated that diabetes mellitus, dyslipidemia, and hypertension were all independently correlated with PR, consistent with previous studies. However, clinical features and laboratory tests in previous studies had limited predictive power for plaque morphology. Therefore, there is an urgent need for effective and accurate serum biomarkers to distinguish PR from PE.
A previous study found that serum MPO level was associated with PE, and ROC analysis indicated that the AUC was 0.75 for MPO when discriminating between PE and PR.8 Another study enrolled 77 patients with PR and 69 patients with PE and collected their sera to evaluate TMAO levels,7 the results showed that the TMAO level was higher in PR, and had a good ability to predict PR, with an AUC of 0.89. However, many of these studies had minor shortcomings, including small sample sizes and low prediction ability. Based on previous studies, it was found that there were significant differences in inflammatory responses between PR and PE, especially monocytes and macrophages.11 Recently, an increasing number of studies have shown that the RNA level in monocytes can serve as a potential biomarker to diagnose diseases and predict clinical outcomes.13,18 In this study, we analyzed the mRNA expression of IL-10, IL-4, IL-1β, and TNF-α in blood monocytes from 382 STEMI patients (262 patients with PR and 120 patients with PE) and found that the PR group exhibited higher expression of IL-10, IL-4, IL-1β, and TNF-α mRNA than the PE group. It is noteworthy that there is no significant difference in preoperative medication status between PE and PR patients, which to some extent avoids the impact of statins and DAPT on inflammatory response. Our results also suggest that TNF-α mRNA may exhibit superior diagnostic capacity for PR, with an AUC of 0.895. Moreover, multivariate logistic regression analysis indicated that TNF-α mRNA levels in monocytes were independently associated with PR (odds ratio [OR], 2.99; 95% confidence interval, 2.25–3.97; p < 0.0001). In addition, subgroup analysis demonstrated that the associations between TNF-α mRNA and PR were generally consistent across common clinical risk factors. These data suggest that TNF-α mRNA is a good predictor of PR, even in specific populations.
Possible Role of TNF-α in Ruptured Plaque Progression
Inflammation plays a vital role in the progression of atherosclerotic plaques.19 Among the many inflammatory factors, IL-4 and IL-10, and IL-1β and TNF-α comprise the two pairs of classic anti- and pro-inflammatory factors, respectively. We found that the mRNA expression of the pro-inflammatory factors IL-1β and TNF-α was significantly increased in the PR group when compared to the PE group. Furthermore, in our study, the high-TNF-α group showed a higher percentage of TCFA and lipid-rich plaque and larger lipid core than the low-TNF-α group in STEMI patients. Lipid-rich plaques, including abundant inflammatory cells, a large necrotic core, and thin fibrous cap plaque, are the main pathological characteristics of ruptured plaques. Previous studies have provided some insights into the involvement of IL-1β and TNF-α in the progression of atherosclerosis. Sustained TNF-α activation has been reported in patients with stable angina and ACS when compared to healthy patients.20 Furthermore, IL-1β and TNF-α have been reported to contribute to the adhesion between monocytes and endothelial cells in atherosclerotic plaques.21–23 Subsequently, the CANTOS Trials suggested that anti-inflammatory therapy targeting IL-1β, using canakinumab, led to a significantly lower rate of recurrent cardiovascular events.24 Several additional studies have also shown that TNF-α damages endothelial and smooth muscle cells, thereby leading to the formation of necrotic cores in these plaques.25 TNF-α inhibitors have also been shown to reduce atherosclerotic plaque progression and improve vascular inflammation.26 These studies indicate that IL-1β and TNF-α are essential for the progression of lipid-rich plaques. Interestingly, we observed that levels of the anti-inflammatory factors IL-4 and IL-10 were increased in patients with STEMI; additionally, the level of IL-4 was increased in PR patients compared to PE patients. This phenomenon has also been observed by other research groups and may be associated with the negative feedback regulation of the body’s anti-inflammatory response.27,28
Clinical Significance of TNF-α in PR
The current standard of care mandates immediate stenting for STEMI, regardless of the morphologic characteristics of the plaque responsible for it, often described as a “one-size-fits-all” clinical strategy.29 However, it was reported that patients with PE experience delayed vascular healing after drug-eluting stent implantation.30 In addition, anti-thrombotic therapy, instead of stent implantation, is largely safe and effective for many patients with PE.3–5 Moreover, criminal plaque morphology is important for the prognosis of ACS patients, as previous studies indicate that patients with PR have a higher risk of major adverse cardiac events and complications than those with PE.15 Taken together, these data suggest that non-invasive prediction of plaque morphology using serum biomarkers may be an important improvement for the clinical management of these diseases, allowing for personalized treatment strategies and improved prognosis for patients with ACS. Herein, we compared the mRNA levels of IL-4, IL-10, IL-1β, and TNF-α in monocytes from both PE and PR STEMI patients and found that TNF-α is independently correlated with PR and has a good diagnostic capacity for this pathobiology. Our results suggest that TNF-α in monocytes could not only serve as a biomarker for PR but also provide clinical value for risk stratification and aid in the determination of the optimal treatment strategy for patients with ACS.
Conclusion
The inflammatory response of peripheral blood mononuclear cells in patients with PR was higher than that in patients with PE. TNF-α may be a potential biomarker for predicting PR that could facilitate risk stratification and management in STEMI patients.
Data Sharing Statement
All original data are available from the corresponding author.
Acknowledgments
We sincerely thank Editage for assistance in language editing and manuscript writing. We thank Tianhao Li and Zhaojin Li for professional suggestions in statistical analyses.
Author Contributions
Conception & study design: Bo Yu, and Haibo Jia.Execution & acquisition of data: Xing Luo. Analysis and interpretation: Chen Zhao. Took part in drafting & critically reviewing the article: Shenfang Wang and Xing Luo. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research is supported by the National Natural Science Foundation of China (No. 82061130223 and No. 82072031), HMU Marshal Initiative Funding (HMUMIF-21016) and Fund of Key Laboratory of Myocardial Ischemia, Ministry of Education (KF202020/LX).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Partida RA, Libby P, Crea F, Jang I-K. Plaque erosion: a new in vivo diagnosis and a potential major shift in the management of patients with acute coronary syndromes. Eur Heart J. 2018;39(22):2070–2076. doi:10.1093/eurheartj/ehx786
2. Jia H, Abtahian F, Aguirre AD, et al. In vivo diagnosis of plaque erosion and calcified nodule in patients with acute coronary syndrome by intravascular optical coherence tomography. J Am Coll Cardiol. 2013;62(19):1748–1758.
3. He L, Qin Y, Xu Y, et al. Predictors of Non-Stenting Strategy for Acute Coronary Syndrome Caused by Plaque Erosion: 4-Year Outcomes of the EROSION Study. EuroIntervention. 2020;1:543.
4. Xing L, Yamamoto E, Sugiyama T, et al. EROSION Study (Effective Anti-Thrombotic Therapy Without Stenting: intravascular Optical Coherence Tomography-Based Management in Plaque Erosion): a 1-Year Follow-Up Report. Circ Cardiovasc Interv. 2017;10(12):986.
5. Jia H, Dai J, Hou J, et al. Effective anti-thrombotic therapy without stenting: intravascular optical coherence tomography-based management in plaque erosion (the EROSION study). Eur Heart J. 2017;38(11):792–800.
6. Sugiyama T, Xing L, Yamamoto E, et al. Thrombus resolution with tirofiban in the conservative management of patients presenting with plaque erosion. Coron Artery Dis. 2018;29(4):301–308.
7. Tan Y, Sheng Z, Zhou P, et al. Plasma Trimethylamine N-Oxide as a Novel Biomarker for Plaque Rupture in Patients With ST-Segment-Elevation Myocardial Infarction. Circ Cardiovasc Interv. 2019;12(1):e007281.
8. Tan Y, Yang S, Chen R, et al. High Plasma Myeloperoxidase Is Associated with Plaque Erosion in Patients with ST-Segment Elevation Myocardial Infarction. J Cardiovasc Transl Res. 2020;13(6):908–915.
9. Ferrante G, Nakano M, Prati F, et al. High levels of systemic myeloperoxidase are associated with coronary plaque erosion in patients with acute coronary syndromes: a clinicopathological study. Circulation. 2010;122(24):2505–2513.
10. Dong H, Hu S, Sun R, et al. High Levels of Circulating MicroRNA-3667-3p Are Associated with Coronary Plaque Erosion in Patients with ST-Segment Elevation Myocardial Infarction. Int Heart J. 2019;60(5):1061–1069.
11. Libby P. Inflammation during the life cycle of the atherosclerotic plaque. Cardiovasc Res. 2021.
12. Oikonomou EK, West HW, Antoniades C. Cardiac Computed Tomography: assessment of Coronary Inflammation and Other Plaque Features. Arterioscler Thromb Vasc Biol. 2019;39(11):2207–2219.
13. Wang XM, Li XM, Song N, Zhai H, Gao XM, Yang YN. Long non-coding RNAs H19, MALAT1 and MIAT as potential novel biomarkers for diagnosis of acute myocardial infarction. Biomed Pharmacother. 2019;118:109208.
14. Xuan L, Sun L, Zhang Y, et al. Circulating long non-coding RNAs NRON and MHRT as novel predictive biomarkers of heart failure. J Cell Mol Med. 2017;21(9):1803–1814.
15. Niccoli G, Montone RA, Di Vito L, et al. Plaque rupture and intact fibrous cap assessed by optical coherence tomography portend different outcomes in patients with acute coronary syndrome. Eur Heart J. 2015;36(22):1377–1384.
16. Yamamoto E, Yonetsu T, Kakuta T, et al. Clinical and Laboratory Predictors for Plaque Erosion in Patients With Acute Coronary Syndromes. J Am Heart Assoc. 2019;8(21):e012322.
17. Dai J, Xing L, Jia H, et al. In vivo predictors of plaque erosion in patients with ST-segment elevation myocardial infarction: a clinical, angiographical, and intravascular optical coherence tomography study. Eur Heart J. 2018;39(22):2077–2085.
18. Hwang S, Kwon AY, Jeong JY, et al. Immune gene signatures for predicting durable clinical benefit of anti-PD-1 immunotherapy in patients with non-small cell lung cancer. Sci Rep. 2020;10(1):643.
19. Soehnlein O, Libby P. Targeting inflammation in atherosclerosis - from experimental insights to the clinic. Nat Rev Drug Discov. 2021;20(8):589–610.
20. Mizia-Stec K, Gasior Z, Zahorska-Markiewicz B, et al. Serum tumour necrosis factor-alpha, interleukin-2 and interleukin-10 activation in stable angina and acute coronary syndromes. Coron Artery Dis. 2003;14(6):431–438.
21. Wang X, Wu Z, He Y, et al. Humanin prevents high glucose-induced monocyte adhesion to endothelial cells by targeting KLF2. Mol Immunol. 2018;101:245–250.
22. Fu H, Spieler F, Großmann J, et al. Interleukin-1 potently contributes to 25-hydroxycholesterol-induced synergistic cytokine production in smooth muscle cell-monocyte interactions. Atherosclerosis. 2014;237(2):443–452.
23. Nallasamy P, Si H, Babu PV, et al. Sulforaphane reduces vascular inflammation in mice and prevents TNF-α-induced monocyte adhesion to primary endothelial cells through interfering with the NF-κB pathway. J Nutr Biochem. 2014;25(8):824–833.
24. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N Engl J Med. 2017;377(12):1119–1131.
25. Ma Y, Huang D, Yang F, et al. Long Noncoding RNA Highly Upregulated in Liver Cancer Regulates the Tumor Necrosis Factor-α-Induced Apoptosis in Human Vascular Endothelial Cells. DNA Cell Biol. 2016;35(6):296–300.
26. Eder L, Joshi AA, Dey AK, et al. Association of Tumor Necrosis Factor Inhibitor Treatment With Reduced Indices of Subclinical Atherosclerosis in Patients With Psoriatic Disease. Arthritis Rheumatol. 2018;70(3):408–416.
27. Li C, Zong W, Zhang M, et al. Increased Ratio of Circulating T-Helper 1 to T-Helper 2 Cells and Severity of Coronary Artery Disease in Patients with Acute Myocardial Infarction: a Prospective Observational Study. Med scie monitor. 2019;25:6034–6042.
28. Fourman LT, Saylor CF, Cheru L, et al. Anti-Inflammatory Interleukin 10 Inversely Relates to Coronary Atherosclerosis in Persons With Human Immunodeficiency Virus. J Infect Dis. 2020;221(4):510–515.
29. Libby P. Superficial erosion and the precision management of acute coronary syndromes: not one-size-fits-all. Eur Heart J. 2017;38(11):801–803.
30. Hu S, Wang C, Zhe C, et al. Plaque erosion delays vascular healing after drug eluting stent implantation in patients with acute coronary syndrome: an In Vivo Optical Coherence Tomography Study. Catheterization Cardiovascular Interventions. 2017;89(S1):592–600.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.