")
Back to Journals » Journal of Asthma and Allergy » Volume 15
Tiotropium Add-On and Treatable Traits in Asthma-COPD Overlap: A Real-World Pilot Study
Authors Ishiura Y , Fujimura M, Ohkura N , Hara J , Nakahama K, Sawai Y, Tamaki T , Murai R, Shimizu T, Miyashita N, Nomura S
Received 28 January 2022
Accepted for publication 6 May 2022
Published 23 May 2022 Volume 2022:15 Pages 703—712
DOI https://doi.org/10.2147/JAA.S360260
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Amrita Dosanjh
Yoshihisa Ishiura,1 Masaki Fujimura,2 Noriyuki Ohkura,3 Johsuke Hara,3 Kahori Nakahama,1 Yusuke Sawai,1 Takeshi Tamaki,1 Ryuta Murai,1 Toshiki Shimizu,1 Naoyuki Miyashita,1 Shosaku Nomura1
1First Department of Internal Medicine, Kansai Medical University, Osaka, Japan; 2Respiratory Medicine, National Hospital Organization Nanao Hospital, Nanao, Japan; 3Respiratory Medicine, Kanazawa University Hospital, Kanazawa, Japan
Correspondence: Yoshihisa Ishiura, First Department of Internal Medicine, Kansai Medical University, 10-15 Fumizono-cho, Moriguchi, Osaka, 570-8507, Japan, Tel +81-6-6992-1001, Fax +81-6-6993-9837, Email [email protected]; [email protected]
Purpose: The ‘treatable traits’ strategy for patients with chronic inflammatory airway diseases, especially asthma and chronic obstructive pulmonary disease (COPD), is a focus of interest, because it implements precision and personalized medicine. Asthma-COPD overlap (ACO), a phenotype involving both asthma and COPD, is an important disease entity because patients with ACO have significantly worse outcomes, conferring greater economical and social burdens. Some guidelines for ACO recommend add-on therapy of long-acting muscarinic antagonists to inhaled corticosteroids and long-acting β2 agonists. However, this approach is based on extrapolation from patients with asthma or COPD alone. Consequently, a ‘treatable traits’ approach suitable for ACO remains obscure.
Methods: A 12-week open-label cross-over pilot study was conducted in patients with ACO to investigate the effect of tiotropium bromide (TIO) 5 μg/day add-on therapy to fluticasone propionate/formoterol fumarate (FP/FM) 500/20 μg/day compared with FP/FM 500/20 μg/day alone. A 4-week run-in period and two 4-week treatment periods were included.
Results: A total of 18 male patients with stable ACO participated in this pilot study. All patients were ex-smokers. Mean values ± standard deviation (SD) for forced expiratory volume in 1 second (FEV1) were 1.21 ± 0.49 L after the run-in period, 1.20 ± 0.51 L after the FP/FM combination therapy period, and 1.30 ± 0.48 L after the TIO add-on therapy to FP/FM period. FEV1 values after the TIO add-on therapy FP/FM period were significantly higher than those after the run-in period (p < 0.01).
Conclusion: TIO add-on therapy to FP/FM in patients with ACO, considered difficult to treat because of the presence of both asthma and COPD, resulted in improvements in lung function parameters in this real-world pilot study, indicating the potential value of TIO add-on therapy as a “treatable traits” option for standard treatment for ACO.
Keywords: treatable trait, asthma-COPD overlap, tiotropium, fluticasone, formoterol, triple therapy
Introduction
Asthma is a common disorder with variable severity characterized by reversible airway obstruction, airway hyperresponsiveness (AHR), and chronic airway inflammation.1,2 According to worldwide surveys, approximately 350 million individuals currently suffer from asthma, and the number is expected to increase to 400 million by 2025.1,2 Asthma is generally regarded as a controllable condition. However, in approximately 5–10% of cases, it can be difficult to control, with individual risk for exacerbation, hospitalization, and death leading to a social burden, and these cases are considered to have severe asthma.3 Severe asthma can present many clinical phenotypes, and thus personalized medicine is required for these cases.4,5 Meanwhile, the Severe Asthma Program at the National Heart, Lung and Blood Institute has reported several severe asthma clusters and indicated the importance of clinical severe asthma phenotypes involving adult-onset asthma with less reversible and/or chronic airway obstruction.6 Recently, the “treatable traits” approach for chronic airway obstruction, mainly asthma and chronic obstructive pulmonary disease (COPD), has been a focus of interest, because personalized and precision medicine is important for these disease entities.7 Asthma-COPD overlap (ACO) has also been a focus of interest, because this disease entity has an important phenotype involving both asthma and COPD and patients with ACO have worse health-related quality of life, more rapid disease progression, increased comorbidities, and greater healthcare utilization, conferring a greater socioeconomic burden than patients with asthma or COPD alone.8–11 Therefore, it is important to determine a suitable treatment approach for ACO.
Tiotropium bromide (TIO; Spiriva™; Boehringer Ingelheim Pharma GmbH & Co. KG, Ingelheim am Rhein, Germany), a long-acting muscarinic antagonist (LAMA), exerts a bronchodilator effect via a different mechanism to both inhaled corticosteroids (ICSs) and long-acting β2 agonists (LABAs).12 TIO also ameliorates airflow limitation in patients with asthma and/or COPD, reduces air trapping and exertional dyspnea, and improves exercise tolerance and health-related quality of life.13,14 However, little is known about the TIO add-on effect as a “treatable traits” approach for patients with ACO, as a difficult-to-treat phenotype involving both asthma and COPD, because only a few therapeutic studies have been conducted on ACO.9–11 We therefore conducted this pilot study to elucidate the add-on effect of TIO as a “treatable traits” option for patients with ACO.
Patients and Methods
This was a 12-week open-label cross-over pilot study to elucidate the real-world effect of TIO 5 µg/day (2.5 µg two inhalations once daily) via a Soft Mist™ inhaler (SMI) as add-on therapy to fluticasone propionate/formoterol fumarate (FP/FM; Flutiform™; Kyorin Pharmaceutical Co., Tokyo, Japan) 500/20 µg/day (125/5 µg two inhalations twice daily) via a pressurized metered-dose inhaler (pMDI). For the study, a sealed-envelope method was used to randomly allocate patients with ACO into two groups, as shown in Figure 1. The study was registered in the University Hospital Medical Information Network (UMIN) under 000039091 and was conducted between March 2019 and August 2020.
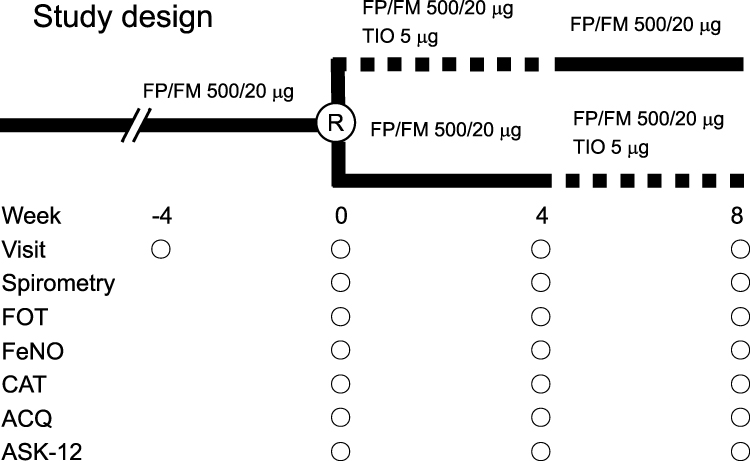 |
Figure 1 Design of the open-label cross-over study. Solid line, dual therapy with fluticasone propionate/formoterol fumarate (FP/FM); dotted line, tiotropium bromide (TIO) add-on therapy to FP/FM. ACQ, asthma control questionnaire; ASK-12, adherence status with knowledge-12; CAT, chronic obstructive pulmonary disease assessment test; FeNO, fractional exhaled nitric oxide; R, randomization. |
Study Subjects
Outpatients with ACO were enrolled in this real-world pilot study when they fulfilled the following criteria based on its originally proposed by Gibson et al known to be related to worse health-related quality of life, more rapid disease progression, increased comorbidities: episodic respiratory symptoms and increased airflow variability (asthma: AHR or bronchodilator response [BDR]) and incompletely reversible airway obstruction (COPD: post-bronchodilator forced expiratory volume in 1 s [FEV1]/forced vital capacity [FVC] <70%, and post-bronchodilator FEV1 <80% of predicted value). AHR was defined as a 20% decrease in FEV1 from baseline after inhalation of <8 mg/mL methacholine. BDR was defined as an increase in post-bronchodilator FEV1 of 200 mL and 12% compared with pre-bronchodilator FEV1.8–11,15,16 All patients were permitted to take mucolytic agents and bronchodilator agents such as oral theophylline and/or leukotriene receptor antagonist, as shown in Table 1. Table 1 does not compare the treated and untreated groups, since all patients were administered TIO in this real-world pilot study. Patients were excluded if they received oral steroid therapy for at least 8 weeks prior to participation. Patients were also excluded if their symptoms were moderate to severe and unstable A total of 18 patients with stable ACO (18 men, 0 women) with a mean age ± standard deviation (SD) of 75.0 ± 5.1 years (range, 59–82 years) participated in this real-world pilot study. In Japanese elderly, there are more men than women with smoking habit, so this pilot study only contains men. All patients were outpatients of Medical Center of Kansai Medical University and ex-smokers with a smoking history ± SD of 53.0 ± 42.1 pack-years.
 |
Table 1 Patient Characteristics |
Study Protocol
The medication was discontinued at 9.00 pm 2 days before starting the examinations to allow a washout period of at least 24 h before measurement of respiratory functions at 10.00 am on each test day. Each patient completed four visits, separated by 4 weeks, at the same time each day. All patients with ACO received FP/FM 500/20 µg/day for at least 4 weeks before randomization, as shown in Figure 1. Subsequently, patients were randomly allocated into two groups and underwent treatment with TIO 5 µg/day add-on to FP/FM 500/20 µg/day or FP/FM 500/20 µg/day alone. Respiratory function was measured at 0, 4, and 8 weeks after randomization and included vital capacity (VC), FVC, FEV1, FEV1/FVC, forced expiratory flow at 25–75% (FEF25–75), maximum expiratory flow (MEF), maximum expiratory flow rate at 50% forced vital capacity (MEF50), and maximum expiratory flow rate at 25% forced vital capacity (MEF25). Measurements of other parameters were also conducted at each visit, including respiratory impedance by the forced oscillation technique (FOT), fractional exhaled nitric oxide (FeNO), asthma control questionnaire (ACQ) score, COPD assessment test (CAT) score, adherence status with knowledge-12 (ASK-12) score, and blood examinations such as peripheral blood eosinophils and immunoglobulin E (IgE) as described in our previous studies.9–11
Measurements
Respiratory functions assessed in the study were measured using a dry wedge spirometer (Chestac 8900™; Chest Co. Ltd., Tokyo, Japan) to evaluate the bronchodilator effect of the treatment regimens on small airway obstruction as previously reported.17–19 For respiratory impedance, FOT was evaluated using another device (MostGraph-01™; Chest Co. Ltd.) in accordance with the recommended techniques.20,21 FeNO was measured using a commercially available device (NIOX MINO™; Aerocrine, Stockholm, Sweden) prior to any forced expiratory maneuvers to assess eosinophilic airway inflammation.22
To evaluate asthma control status during the previous 4 weeks, patients were asked to complete the ACQ5, an easy five-question questionnaire that assesses asthma symptoms.23 Each question was scored from 0 to 6, giving a total score of 0–30, with high scores corresponding to high levels of symptoms and poor asthma control. To assess and measure the effects of COPD symptoms on their health status, patients were requested to complete the CAT, a simple questionnaire that acts as a reliable and valid tool to examine the impact of COPD symptoms over time.24 The CAT comprised eight items scored from 0 to 5, giving a maximum total score of 40. CAT scores of 1–10, 11–20, 21–30, and 31–40 were considered to indicate mild, moderate, severe, and very severe health status impairment, respectively.24 To detect patient-specific barriers to medication adherence, all patients were requested to complete the ASK-12, a 12-item questionnaire consisting of three domains related to medication adherence: inconvenience and/or forgetfulness, treatment beliefs, and behavior.25 The response for each item was scored from 1 to 5, giving a final score range of 12–60, with higher values representing greater barriers to adherence.25 All adverse events such as palpitations were recorded during the study period.
Data Analysis
Data obtained in the study are shown as mean ± SD. One-way analysis of variance (ANOVA) was used to analyze differences between the run-in period, the FP/FM combination therapy period and the TIO add-on therapy to FP/FM period for respiratory functions, FOT parameters, FeNO levels, CAT scores, ACQ scores, heart rates, and blood examinations including IgE. Values of p < 0.05 were considered statistically significant. All analyses were performed using StatView 4.5J software (Abacus Concepts, Berkeley, CA, USA).
Results
The results for the respiratory function measurements obtained by spirometry are shown in Table 2. Several parameters were significantly higher after the TIO add-on therapy to FP/FM period compared with their values after the run-in period or FP/FM combination therapy period. The changes in FVC after the run-in period and each treatment period are shown in Figure 2. The mean FVC values were 2.61 ± 0.70 L after the run-in period, 2.52 ± 0.75 L after the FP/FM combination therapy period, and 2.76 ± 0.74 L after the TIO add-on therapy to FP/FM period. The FVC values after the TIO add-on therapy to FP/FM period were significantly higher than those after the run-in period (p < 0.05). The changes in FEV1 after the run-in period and each treatment period are shown in Figure 3. The mean FEV1 values were 1.21 ± 0.49 L after the run-in period, 1.20 ± 0.51 L after the FP/FM combination therapy period, and 1.30 ± 0.48 L after the TIO add-on therapy to FP/FM period. The FEV1 values after the TIO add-on therapy to FP/FM period were significantly higher than those after the run-in period (p < 0.01).
 |
Table 2 Spirometry Parameters After Each Treatment |
 |
Figure 2 Individual data for forced vital capacity (FVC) before each treatment with fluticasone propionate/formoterol fumarate (FP/FM) combination therapy and after tiotropium bromide (TIO) add-on therapy to FP/FM in patients with asthma-chronic obstructive pulmonary disease overlap (ACO). Each panel shows the parameter changes for all patients and the mean ± standard deviation (SD). P < 0.05, determined by one-way analysis of variance (ANOVA). |
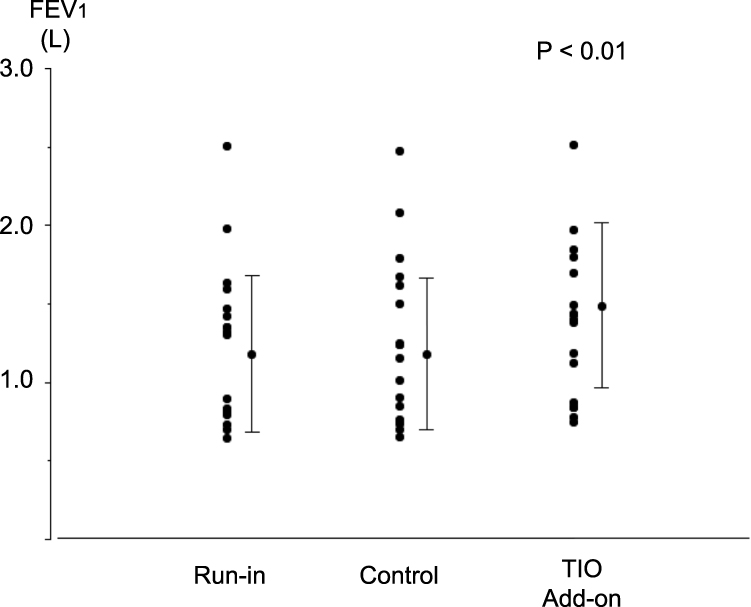 |
Figure 3 Individual data for forced expiratory volume in 1 s (FEV1) before each treatment and after fluticasone propionate/formoterol fumarate (FP/FM) combination therapy and tiotropium bromide (TIO) add-on therapy to FP/FM in patients with asthma-chronic obstructive pulmonary disease overlap (ACO). Each panel shows the parameter changes for all patients and the mean ± standard deviation (SD). P< 0.01, determined by one-way ANOVA. |
The respiratory impedances during inspiration measured by FOT are shown in Table 3. Each parameter was significantly improved after the TIO add-on therapy to FP/FM period compared with those after the run-in period and FP/FM treatment period. The R5 values during inspiration after the run-in period and each treatment period are shown in Figure 4. The mean R5 values were 3.8 ± 1.1 cmH2O/L/s after the run-in period, 3.6 ± 1.2 cmH2O/L/s after the FP/FM treatment period, and 3.2 (± 1.1) cmH2O/L/s after the TIO add-on therapy to FP/FM period. The R5 values after the TIO add-on therapy period to FP/FM were significantly lower than those after the run-in period (p < 0.05). The FeNO levels, CAT scores, ACQ scores, ASK-12 scores, and blood examination findings (eosinophils and IgE) did not differ significantly among the run-in period, FP/FM combination therapy period, and TIO add-on therapy to FP/FM period, as shown in Table 3. None of the patients enrolled in the study complained of cardiovascular or gastroenterological symptoms after administration of FP/FM or TIO add-on to FP/FM. Furthermore, no exacerbations or adverse events were observed in the two groups during the study period.
 |
Table 3 FOT Parameters, FeNO, CAT, ACT and Blood Examination Parameters After Each Treatment |
 |
Figure 4 Individual data for resistance at 5 Hz (R5) before each treatment and after fluticasone propionate/formoterol fumarate (FP/FM) combination therapy and tiotropium bromide (TIO) add-on therapy to FP/FM in patients with asthma-chronic obstructive pulmonary disease overlap (ACO). Each panel shows the parameter changes for all patients and the mean ± standard deviation (SD). P < 0.05, determined by one-way ANOVA. |
Discussion
The present results obtained by this real-world pilot study clearly showed that TIO add-on therapy to FP/FM improved lung functions and respiratory impedances in patients with ACO. These findings indicate the potential of TIO add-on therapy via SMI, to be known to generate a high fine-particle fraction, to FP/FM as a “treatable traits” option in patients with ACO, a difficult-to-treat phenotype involving both asthma and COPD.
Asthma and COPD are two common and prevalent chronic airway diseases with many risks for exacerbation, hospitalization, and death, leading to considerable social burdens. Asthma is estimated to affect 350 million people worldwide,26 and approximately 5–10% of patients remains hard to control. Meanwhile, COPD is estimated to affect 251 million people worldwide and represents the third leading cause of mortality worldwide.27 Acute exacerbations occur in approximately half of COPD patients and about 20% of patients require hospitalization.27
Recently, the “treatable traits” strategy for patients with chronic inflammatory airway diseases, especially asthma and COPD, has been a focus of attention, because this clinically important approach implements precision and personalized medicine on the basis of genetic, biomarker, phenotypic, or psychosocial characteristics that distinguish a given patient from other patients with similar clinical presentations.5,7,27,28 In the last decade, ACO has also been a focus of interest, because patients with ACO exhibit more rapid disease progression, worse health-related quality of life, more frequent respiratory exacerbation, decreased lung functions, increased comorbidities, and higher healthcare utilization than patients with asthma or COPD alone.9–11,16 Therefore, ACO is an important phenotype involving both asthma and COPD. However, current treatment approaches for patients with ACO are based on extrapolation of data derived from studies on patients with asthma or COPD alone, because only a few therapeutic studies have been conducted on ACO.9–11 The present findings indicate the importance of the “treatable traits” strategy in patients with ACO. We previously examined the effect of LAMA via dry powder inhalation (DPI) added to ICS/LABA via DPI in patients with ACO, but did not examine other devices.9–11 DPI devices are convenient for drug delivery, but their efficacy depends on the speed of inhalation, the inhalation volume, and the inspiratory effect.29 Since ACO is characterized by low lung function, more suitable methods are required for different inhalers with distinct drug administration effects as a “treatable traits” option for patients with ACO.7–11 Therefore, we conducted the present pilot study and clearly showed a beneficial effect of TIO add-on therapy via SMI to FP/FM via pMDI in patients with ACO, indicating the clinical efficacy of TIO add-on therapy to FP/FM as a “treatable traits” option for this phenotype.
TIO, one of the LAMAs, exerts a bronchodilator effect via a different mechanism both ICSs and LABAs.12 The primary pharmacologic target for bronchoconstriction is muscarinic receptor type 3 (M3). TIO is the most potent M3 antagonist that selectively binds to this muscarinic receptor with the slowest dissociation suitable for a once-daily administration schedule in clinical practice.29,30 Although the pharmacological mechanisms remain unclear, LAMAs reduce airway allergic inflammation and inhibit airway remodeling induced by allergens, resulting in improvement of airway obstruction in patients with bronchial asthma.13,31,32 Therefore, TIO is considered to improve lung function, quality of life, and exercise endurance and to reduce exacerbation in patients with asthma and COPD.14,33 Recently, Iwanaga et al reported that an aerosol of TIO generated by SMI had a high fine-particle fraction delivered at a slow velocity, compared with that generated by DPI.29 They also clarified that TIO via SMI had maximized lung deposition in the whole lung and peripheral airways with minimized oropharyngeal deposition, even at low inhalation flows.29 We therefore consider that TIO via SMI is a suitable potent bronchodilator agent in patients with ACO characterized by low lung functions.7–11
FP, administered in this study, is a potent ICS with anti-inflammatory activity under conditions of oxidative stress, implying its efficacy in patients with COPD who tend to exhibit high levels of oxidative stress.9,10,19 FM is a LABA with a rapid onset of action and a sustained dose-dependent bronchodilator effect.11 FP/FM combination therapy via pMDI was reported to be an efficacious treatment option compared with other ICS/LABA combination therapies via DPI even in patients with moderate to severe asthma.34,35 Iwanaga et al also investigated and reported higher drug deposition in the lungs and peripheral airways after FP/FM via pMDI compared with other ICS/LABA combination therapies via DPI.29 Since most DPI devices require a high inspiratory flow to overcome the device resistance and achieve more effective drug deposition, FP/FM via pMDI is considered suitable for patients with low lung functions.7–11
In this study, we clearly showed that TIO add-on therapy via SMI to FP/FM combination therapy via pMDI can ameliorate airflow limitations in patients with ACO. Therefore, we consider that TIO add-on therapy via SMI to FP/FM combination therapy via pMDI is a suitable “treatable traits” strategy for patients with ACO, a difficult-to-treat phenotype involving both asthma and COPD.7–11
The present study had several limitations. First, although we demonstrated statistically significant improvements in respiratory functions, these results alone cannot elucidate the etiology of the clinically beneficial effects. A potent bronchodilator effect may be the main factor for the results in this clinical study because the FeNO levels did not change after the TIO add-on therapy to FP/FM period. We therefore consider that an examination of airway mediators may help to clarify the underlying mechanism, because several studies showed anti-inflammatory effects of LAMAs.13,31,32,36 Further studies are required to investigate the airway mediators and clarify the mechanisms of the bronchodilator effects of TIO add-on therapy to FP/FM. Second, a specific and formal definition of ACO remains to be established.7–11 Although several definitions have been proposed based on specific inflammatory patterns,37,38 these definitions are not specific for asthma and/or COPD alone. For example, eosinophilic airway inflammation has been identified in only 48% of patients with asthma and 34% of those with COPD.8 We conducted the present study based on physiological lung function criteria described in previous reports.8–11 Several different studies in patients with ACO indicates the validity of the physiological lung function criteria.8,39,40 Further studies are required to reach a consensus on better diagnostic criteria for ACO. Third, this study was conducted as a pilot study. Therefore, the sample size is too small to make comparisons within each group and not between groups as would be expected in a clinical trial and only contains men because smoking habit is for men in Japanese elderly. Succeeding larger randomized study is required. Furthermore, this study used ACQ-5, not ACQ-6, to evaluate patient symptoms. We are afraid that this is the one reason could not indicate the difference among each group despite the improvement of respiratory functions. We also think that succeeding study have to conduct ACQ-6 to evaluate patient symptoms. Measurement of the frequency of the usage of SABA may be the help for indicating the improvement of symptoms after TIO administration. Finally, the pulmonary physiology outcome measures confirmed the bronchodilator effects of TIO add-on therapy to FP/FM, but the CAT scores and ACQ scores did not show benefits with respect to healthcare outcomes despite the improvement in each respiratory function. The number of enrolled patients in the present study may have been insufficient to detect differences in symptom scores. A larger study may therefore be required to clarify the benefits of TIO add-on therapy to FP/FM in patients with ACO with respect to healthcare outcomes.
Conclusions
In conclusion, 4-week treatment of TIO add-on therapy via SMI to FP/FM in patients with ACO as a real-world pilot study resulted in a significant improvement from baseline in lung function, including FOT, compared with FP/FM combination therapy alone, and with a comparable safety profile. The present findings support the potential for TIO add-on therapy via SMI, to be known to generate a high fine-particle fraction, to FP/FM to FP/FM as a therapeutic option for ACO. Further, larger studies are required to define the precise etiology of the clinical efficacy of this combination therapy.
Abbreviations
ACO, asthma-COPD overlap; ACQ, asthma control questionnaire; AHR, airway hyperresponsiveness; ANOVA, analysis of variance; ASK-12, adherence status with knowledge-12; BDR, bronchodilator response; CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; DPI, dry powder inhalation; FEF25–75, forced expiratory flow at 25%–75%; FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in 1 s; FOT, forced oscillation technique; FP, fluticasone propionate; FM, formoterol fumarate; FVC, forced vital capacity; ICS, inhaled corticosteroid; IgE, immunoglobulin E; LABA, long-acting β2 agonist; LAMA, long-acting muscarinic antagonist; MEF, maximum expiratory flow rate; MEF25, maximum expiratory flow rate at 25% forced vital capacity; MEF50, maximum expiratory flow rate at 50% forced vital capacity; pMDI, pressurized metered-dose inhaler; M3, muscarinic receptor type 3; SD, standard deviation; SMI, Soft Mist™ inhaler; TIO, tiotropium bromide; UMIN, University Hospital Medical Information Network; VC, vital capacity.
Data Sharing Statement
The clinical study data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Kansai Medical University (approval no. 2017315). Written informed consent was obtained from all patients prior to participation.
Acknowledgment
The authors thank Alison Sherwin, PhD, from Edanz for editing a draft of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. To T, Stanojevic S, Moores G, et al. Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Publ Health. 2012;12:204. doi:10.1186/1471-2458-12-204
2. Adachi M, Kozawa M, Yoshisue H, et al. Real-world safety and efficacy of omalizumab in patients with severe allergic asthma: a long-term post-marketing study in Japan. Respir Med. 2018;141:56–63. PMID: 30053973. doi:10.1016/j.rmed.2018.06.021
3. Hekking PP, Wener RR, Amelink M, Zwinderman AH, Bouvy ML, Bel EH. The prevalence of severe refractory asthma. J Allergy Clin Immunol. 2015;135:896–902. doi:10.1016/j.jaci.2014.08.042
4. McDonald VM, Clark VL, Cordova-Rivera L, Wark PAB, Baines KJ, Gibson PG. Targeting treatable traits in severe asthma: a randomised controlled trial. Eur Respir J. 2020;55(3):1901509. doi:10.1183/13993003.01509-2019
5. McDonald VM, Osadnik CR, Gibson PG. Treatable traits in acute exacerbations of chronic airway diseases. Chron Respir Dis. 2019;16:1479973119867954. doi:10.1177/1479973119867954
6. Jarjour NN, Erzurum SC, Bleecker ER, et al.; NHLBI Severe Asthma Research Program (SARP). Severe asthma: lessons learned from the National heart, lung, and blood institute severe asthma research program. Am J Respir Crit Care Med. 2012;185(4):356–362. doi:10.1164/rccm.201107-1317PP
7. Gaspar Marques J, Lobato M, Leiria Pinto P, Neuparth N, Carreiro Martins P. Asthma and COPD “overlap”: a treatable trait or common several treatable-traits? Eur Ann Allergy Clin Immunol. 2020;52(4):148–159. doi:10.23822/EurAnnACI.1764-1489.138
8. Fu JJ, Gibson PG, Simpson JL, McDonald VM. Longitudinal changes in clinical outcomes in older patients with asthma, COPD and asthma-COPD overlap syndrome. Respiration. 2014;87:63–74. doi:10.1159/000352053
9. Ishiura Y, Fujimura M, Shiba Y, Ohkura N, Hara J, Kasahara K. A comparison of the efficacy of once-daily fluticasone furoate/vilanterole with twice-daily fluticasone propionate/salmeterol in Asthma-COPD overlap syndrome. Pulm Pharmacol Ther. 2015;35:28–33. doi:10.1016/j.pupt.2015.10.005
10. Ishiura Y, Fujimura M, Ohkura N, et al. Effect of triple therapy in patients with asthma-COPD overlap. Int J Clin Pharmacol Ther. 2019;57(8):384–392. doi:10.5414/CP203382
11. Ishiura Y, Fujimura M, Ohkura N, et al. Therapy with budesonide/glycopyrrolate/formoterol fumarate improves inspiratory capacity in patients with asthma-chronic obstructive pulmonary disease overlap. Int J Chron Obstruct Pulmon Dis. 2020;15:269–277. doi:10.2147/COPD.S231004
12. Buhl R, FitzGerald JM, Busse WW. Tiotropium add-on to inhaled corticosteroids versus addition of long-acting β 2-agonists for adults with asthma. Respir Med. 2018;143:82–90. doi:10.1016/j.rmed.2018.08.014
13. Doherty DE, Bleecker ER, Moroni-Zentgraf P, Zaremba-Pechmann L, Kerstjens HAM. Tiotropium respimat efficacy and safety in asthma: relationship to age. J Allergy Clin Immunol Pract. 2020;8(8):2653–2660.e4. doi:10.1016/j.jaip.2020.04.013
14. Incorvaia C, Riario-Sforza GG, Pravettoni C, Yacoub MR, Frati F. Impairment of small airways in COPD patients with frequent exacerbations and effects of treatment with tiotropium. Int J Chron Obstruct Pulmon Dis. 2008;3(1):123–126. doi:10.2147/copd.s2386
15. Marsh SE, Travers J, Weatherall M, et al. Proportional classification of COPD phenotypes. Thorax. 2008;63(9):761–767. doi:10.1136/thx.2007.089193
16. Gibson PG, Simpson JL. The overlap syndrome of asthma and COPD: what are its features and how important is it? Thorax. 2009;64(8):728–735. doi:10.1136/thx.2008.108027
17. Ishiura Y, Fujimura M, Yamamoto H, Ishiguro T, Ohkura N, Myou S. COX-2 inhibition attenuates cough reflex sensitivity to inhaled capsaicin in patients with asthma. J Investig Allergol Clin Immunol. 2009;19:370–374.
18. Ishiura Y, Fujimura M, Yamamoto H, Ohkura N, Myou S. Role of COX-2 in cough reflex sensitivity to inhaled capsaicin in patients with sinobronchial syndrome. Cough. 2010;6(1):7. doi:10.1186/1745-9974-6-7
19. Ishiura Y, Fujimura M, Shiba Y, et al. A comparison of the efficacy of once-daily fluticasone furoate/vilanterole with twice-daily fluticasone propionate/salmeterol in elderly asthmatics. Drug Res. 2018;68(1):38–44. doi:10.1055/s-0043-118536
20. Oostveen E, MacLeod D, Lorino H, et al.; Force on Respiratory Impedance Measurements. The forced oscillation technique in clinical practice: methodology, recommendations and future developments. Eur Respir J. 2003;22:1026–1041. doi:10.1183/09031936.03.00089403
21. Mori K, Shirai T, Mikamo M, et al. Colored 3-dimensional analyses of respiratory resistance and reactance in COPD and asthma. COPD. 2011;8(6):456–463. doi:10.3109/15412555.2011.626818
22. Alving K, Janson C, Nordvall L. Performance of a new hand-held device for exhaled nitric oxide measurement in adults and children. Respir Res. 2006;7(1):67. doi:10.1186/1465-9921-7-67
23. Werner CU, Linde K, Schäffner J, Storr C, Schneider A. Weekly self-measurement of FEV1 and PEF and its impact on ACQ (asthma control questionnaire)-scores: 12-week observational study with 76 patients. NPJ Prim Care Respir Med. 2017;27(1):64. doi:10.1038/s41533-017-0064-4
24. Mackay AJ, Donaldson GC, Patel AR, Jones PW, Hurst JR, Wedzicha JA. Usefulness of the chronic obstructive pulmonary disease assessment test to evaluate severity of COPD exacerbations. Am J Respir Crit Care Med. 2012;185:1218–1224. doi:10.1164/rccm.201110-1843OC
25. Matza LS, Park J, Coyne KS, Skinner EP, Malley KG, Wolever RQ. Derivation and validation of the ASK-12 adherence barrier survey. Ann Pharmacother. 2009;43(10):1621–1630. doi:10.1345/aph.1M174
26. Chari VM, McIvor RA. Tiotropium for the treatment of asthma: patient selection and perspectives. Can Respir J. 2018;2018:3464960. doi:10.1155/2018/3464960
27. Park HK, Song WJ. Sex and treatable traits in severe asthma. Allergy Asthma Immunol Res. 2021;13(2):167–170. doi:10.4168/aair.2021.13.2.167
28. Agusti A, Bel E, Thomas M, et al. Treatable traits: toward precision medicine of chronic airway diseases. Eur Respir J. 2016;47(2):410–419. doi:10.1183/13993003.01359-2015
29. Iwanaga T, Tohda Y, Nakamura S, Suga Y. The respimat ® soft mist inhaler: implications of drug delivery characteristics for patients. Clin Drug Investig. 2019;39(11):1021–1030. doi:10.1007/s40261-019-00835-z
30. Casarosa P, Bouyssou T, Germeyer S, Schnapp A, Gantner F, Pieper M. Preclinical evaluation of long-acting muscarinic antagonists: comparison of tiotropium and investigational drugs. J Pharmacol Exp Ther. 2009;330(2):660–668. PMID: 19478135. doi:10.1124/jpet.109.152470
31. Cazzola M, Ora J, Rogliani P, Matera MG. Role of muscarinic antagonists in asthma therapy Expert. Rev Respir Med. 2017;11(3):239–253. doi:10.1080/17476348.2017.1289844
32. Hoshino M, Ohtawa J, Akitsu K. Effects of the addition of tiotropium on airway dimensions in symptomatic asthma. Allergy Asthma Proc. 2016;37(6):147–153. doi:10.2500/aap.2016.37.3991
33. Wise RA, Anzueto A, Cotton D, et al.; TIOSPIR Investigators. Tiotropium respimat inhaler and the risk of death in COPD. N Engl J Med. 2013;369(16):1491–1501. PMID: 23992515. doi:10.1056/NEJMoa1303342
34. Corren J, Mansfield LE, Pertseva T, Blahzko V, Kaiser K. Efficacy and safety of fluticasone/formoterol combination therapy in patients with moderate-to-severe asthma. Respir Med. 2013;107(2):180–195. doi:10.1016/j.rmed.2012.10.025
35. Papi A, Mansur AH, Pertseva T, et al. Long-term fluticasone propionate/formoterol fumarate combination therapy is associated with a low incidence of severe asthma exacerbations. J Aerosol Med Pulm Drug Deliv. 2016;29(4):346–361. doi:10.1089/jamp.2015.1255
36. Benfante A, Braido F, Scichilone N. The anti-inflammatory properties of tiotropium. Lancet Respir Med. 2018;6(8):e37. doi:10.1016/S2213-2600(18)30190-5
37. Miravitlles M, Soler-Cataluña JJ, Calle M, et al. Spanish guideline for COPD (GesEPOC). Arch Bronconeumol. 2014;50(Suppl 1):1–16. doi:10.1016/S0300-2896(14)70070-5
38. The Japanese Respiratory Society. The JRS guidelines for the management of ACO 2018. Tokyo: Medical Review; 2017. Japanese
39. Soriano JB, Visick GT, Muellerova H, Payvandi N, Hansell AL. Patterns of comorbidities in newly diagnosed COPD and asthma in primary care. Chest. 2005;128(4):2099–2107. doi:10.1378/chest.128.4.2099
40. McDonald VM, Higgins I, Gibson PG. Managing older peoples with coexistent asthma and chronic obstructive lung disease; diagnostic and therapeutic challenge. Drugs Aging. 2013;30:1–17. doi:10.1007/s40266-012-0042-z
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.