Back to Journals » Journal of Inflammation Research » Volume 18
Time-Weighted Cumulative High-Sensitivity C-Reactive Protein and Risk of Cardiac Conduction Block: Findings from a Prospective Cohort
Authors Zhang M, Shi D, Chen Y, Liao Y, Liu Z, Fu R, Bian Y, Chen S, Zhao H, He H ![]() , Zu C, Liu C, Huo H, Wu S
, Zu C, Liu C, Huo H, Wu S ![]() , Wu Y
, Wu Y
Received 18 June 2025
Accepted for publication 6 December 2025
Published 14 December 2025 Volume 2025:18 Pages 17477—17493
DOI https://doi.org/10.2147/JIR.S547484
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Durga Misra
Mo Zhang,1,2,* Dou Shi,1,* Yixiu Chen,2,3 Yicheng Liao,2,3 Zhihui Liu,2,3 Renjie Fu,2,3 Yufeng Bian,2,3 Shuohua Chen,2 Haiyan Zhao,2 Honghong He,2 Changhao Zu,2 Chunlu Liu,2 Hongqiu Huo,2 Shouling Wu,2 Yuntao Wu2
1Graduate School, Hebei North University, Zhangjiakou City, Hebei Province, 075000, People’s Republic of China; 2Department of Cardiology, Kailuan General Hospital, Tangshan City, Hebei Province, 063000, People’s Republic of China; 3Graduate School, North China University of Science and Technology, Tangshan City, Hebei Province, 063210, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuntao Wu, Department of Cardiology, Kailuan General Hospital, No. 57 Xinhua East Road, Tangshan City, Hebei Province, 063000, People’s Republic of China, Tel +8613933305222, Email [email protected]
Purpose: Chronic low-grade inflammation is increasingly recognized as a contributing factor in the development of cardiovascular events. This study aimed to evaluate the association between time-weighted cumulative exposure to high-sensitivity C-reactive protein (cumhsCRP) and the risk of new-onset cardiac conduction block (CCB).
Patients and Methods: A total of 48,703 participants from a prospective community-based cohort were included. The average exposure time for cumhsCRP was 6.36 years. Participants were stratified into two groups: cumhsCRP < 2 mg/L and cumhsCRP ≥ 2 mg/L. The incidence of new-onset cardiac conduction block and its subtypes was identified through standard 12-lead electrocardiograms. Cox proportional hazards models were used to assess the relationship between cumhsCRP levels and incident CCB risk, adjusting for potential confounders. A restricted cubic spline curve further explored the dose-response pattern.
Results: During a mean follow-up period of 9.24 years, 803 cases of new-onset CCB were documented (incidence rate: 1.65%). After full multivariable adjustment, individuals in the cumhsCRP ≥ 2 mg/L group exhibited a significantly higher risk of CCB compared to those with cumhsCRP < 2 mg/L (HR: 1.24, 95% CI: 1.07– 1.44). The RCS analysis suggested a linear association between log-transformed cumhsCRP and CCB risk (p for non-linearity = 0.294).
Conclusion: Elevated cumulative exposure to high-sensitivity C-reactive protein is independently associated with an increased risk of developing CCB, especially left bundle branch block and left anterior fascicular block. This study will provide new insights into the prevention of CCB.
Keywords: inflammation, high-sensitivity C-reactive protein, cumulative exposure, cardiac conduction block
Introduction
Cardiac conduction block (CCB) refers to a temporary or permanent electrical impulse conduction disorder caused by structural or functional abnormalities of the heart, which can occur in any part of the cardiac conduction system. A US multicenter cohort study involving over 180,000 participants found that after a median follow-up of 10 years, the prevalence of conduction disorders reached 27% in men and 15% in women, with incidence rates of 8.78 per 1,000 person-years and 4.34 per 1,000 person-years respectively.1 According to statistics, the prevalence of atrioventricular block (AVB) among Chinese adults reached 7.06‰ in 2018.2 Among whites in the United States, the incidence rate of high-degree AVB reaches 2.79 per 1,000 person-years.3 Even first-degree AVB has been associated with an increased risk of adverse events such as atrial fibrillation, heart failure, and all-cause mortality.4,5 Additionally, similar phenomena have been observed in individuals with bundle branch block (BBB).6,7
CCB is associated with increased risk of bradyarrhythmia, sudden cardiac death, and adverse cardiovascular events, making it particularly important to identify high-risk populations early and implement interventions. Previous studies have identified risk factors for CCB, such as male sex, older age, obesity, hypertension, and diabetes.7–12 However, analyses of its risks and prognosis remain limited. Myocardial fibrosis is one of the early pathophysiological changes in CCB, which contributes to arrhythmogenesis by disrupting basic electrophysiological pathways.13 Fibrosis is typically driven by chronic inflammation,14 and inflammatory signaling within the body can directly promote cardiac structural remodeling (myocardial fibrosis formation) and electrical remodeling (dysregulation of ion channels and calcium homeostasis), leading to an increased tendency for arrhythmia.15 In experimental animal models, it was discovered that macrophage GMCSF/CCL2/CCR2 signal transduction, mediated through the NLRP3 inflammasome cascade and phenotypic switching, promotes chronic fibrotic remodeling of myocardial tissue in mice with acute myocardial ischemia.16 High-sensitivity C-reactive protein (hsCRP) is a commonly used clinical marker of inflammation. Multiple studies have indicated that high levels of hsCRP is one of the risk factors for cardiovascular diseases and heart failure.17–19 And recent studies have highlighted a positive association between elevated baseline hsCRP levels and the incidence of CCB.20,21 However, previous analyses of the association between hsCRP and CCB were based on single measurements of hsCRP, which can be influenced by factors such as metabolic disturbances, dietary changes, environmental pollution, and certain pathological conditions, potentially causing short-term elevations in hsCRP levels.17 This limitation prevents these measurements from adequately reflecting chronic inflammation status. As a result, using single time point hsCRP measurements as a risk predictor may affect the accuracy of risk assessments for CCB events. In contrast, cumulative hsCRP exposure (cumhsCRP), which accounts for both intensity and duration, may offer better predictive value.
To explore the relationship between cumhsCRP and CCB, this study utilized data from the Kailuan Study (Registration Number: ChiCTR-TNRC-11001489). A prospective cohort study design was adopted to investigate the effect of time-weighted cumulative hsCRP exposure on the risk of new-onset CCB.
Materials and Methods
Study Population
The study population was derived from the Kailuan Study, a prospective cohort study initiated in 2006. Active and retired employees of the Kailuan Group underwent comprehensive assessments at the Kailuan General Hospital and its 11 affiliated hospitals in 2006. These assessments included anthropometric measurements (eg, height and weight), questionnaire surveys, electrocardiogram evaluations, and laboratory biochemical tests, followed by biennial follow-up examinations. Follow-up assessments included high-sensitivity C-reactive protein (hsCRP) measurements and routine electrocardiogram evaluations. Participants were included in the study if they met the following criteria: (1) completed at least the 2006 and 2012 health examinations among the 2006, 2008, 2010, and 2012 examination cycles; (2) had complete electrocardiogram data; and (3) provided written informed consent for participation. Exclusion criteria included: (1) a history of cardiac conduction block at the 2012 examination; (2) missing hsCRP data in the health examination records; and (3) hsCRP measurement >10 mg/L in any examination, indicative of acute inflammation or related infectious diseases. The study protocol was carried out following the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of Kailuan General Hospital ([2006] Med Ethics No. 5).
Data Collection
General Clinical Characteristics
Information on participants’ age, sex, height, weight, disease history, and medication use was collected via questionnaires. The methods and standards used were consistent with those described in previously published studies by this research group.22
High-Sensitivity C-Reactive Protein and Related Biochemical Marker Testing
Participants were required to fast for at least 8 hours before undergoing venous blood collection from the elbow in the morning of the health examination. The serum was then separated by centrifugation and analyzed for high-sensitivity C-reactive protein (hsCRP). Serum hsCRP was measured using an immunoturbidimetric method on a Hitachi-7600 automatic biochemical analyzer, with reagents from Kanto Chemical Co., Inc. (Tokyo, Japan). The same methodology and platform were maintained throughout the study period. The laboratory adhered to a strict quality control protocol, including regular calibration and the use of internal quality control samples to monitor precision.Between 2006 and 2009, the laboratory’s proficiency testing (PT) for hsCRP, evaluated by the former Ministry of Health, consistently achieved a score of 100%. Additionally, two specimens were analyzed twice daily with a minimum interval of two hours between measurements, repeated over a period of 20 days to evaluate measurement precision. The intra-assay coefficient of variation (CV) was 6.53%, inter-assay CV was 4.78%, daily variation CV was 6.61%, and the total CV was 9.37%. The reference range for serum hsCRP was 0–5 mg/L, with a minimum detectable concentration of 0.1 mg/L. For participants whose hsCRP levels were below the detection limit, the value was substituted with half of the minimum detectable concentration (0.05 mg/L).
The enzymatic colorimetric method (Mind Bioengineering Co Ltd., Shanghai, China) was used to measure low-density lipoprotein cholesterol (LDL-C). For each measurement, the inter-assay coefficient of variation was < 10% with the use of an autoanalyzer (Hitachi 747, Hitachi,Tokyo, Japan).
Electrocardiogram Measurements
Routine electrocardiogram (ECG) measurements were conducted during the 2012 health examinations and at subsequent biennial follow-ups. Participants rested in a supine position in a quiet room between 7:00 and 9:00 a.m. for 5 minutes before undergoing a standard 12-lead ECG (Nihon Kohden Electrocardiograph, Model ECG-9130P) for 10 seconds. The ECG recordings and diagnoses were independently reviewed by two cardiology experts.
Definition and Tracking of Endpoint Events
Based on the ACC/AHA/HRS guidelines,23,24 cardiac conduction block (CCB) was defined as the presence of any type of conduction block, including atrioventricular block (AVB), bundle branch block (BBB), and nonspecific intraventricular conduction delay (NS-IVCD). AVB included first- to third-degree AVB, while BBB encompassed left bundle branch block (LBBB) and right bundle branch block (RBBB). LBBB was further classified into complete left bundle branch block (CLBBB), incomplete left bundle branch block (ILBBB), left anterior fascicular block (LAFB), and left posterior fascicular block (LPFB). Similarly, RBBB was categorized into complete right bundle branch block (CRBBB) and incomplete right bundle branch block (IRBBB). Detailed definitions of endpoint events are provided in Supplementary Table 1.
The follow-up period began at the time of the 2012 health examination and ended at the occurrence of any type of CCB. For participants with multiple CCB events, the first occurrence and corresponding time were considered the endpoint. For participants without any events, the follow-up ended on December 31, 2022. If a participant died before experiencing a CCB event, the follow-up period was defined as the time of death. In subtype analyses of CCB, each CCB occurrence was treated as an independent event with its corresponding time recorded.
Definition of Potential Covariates
Smoking was defined as smoking at least 1 cigarette per day during the preceding year. Alcohol consumption was defined as drinking an average of 100 mL of liquor (with an alcohol content ≥50%) daily over the past year. Physical activity was defined as exercising at least three times per week, with each session lasting a minimum of 30 minutes. High salt intake was defined as consuming more than 6 grams of sodium daily. Participants who developed myocardial infarction or heart failure during follow-up were identified and recorded this using the International Classification of Diseases codes (ICD-10) by trained personnel.
Calculation and Grouping of Time-Weighted Cumulative hsCRP
Based on the formula for calculating the time-weighted cumulative plasma atherogenic index,25 the time-weighted cumulative hsCRP was calculated as the time-weighted sum of the average hsCRP levels measured at two consecutive health examinations, then standardized by the total exposure time (2006 to 2012).
- Participants who consistently attended the 2006, 2008, 2010, and 2012 health examinations:cumhsCRP=[(hsCRP1+hsCRP2)/2*time1+(hsCRP2+hsCRP3)/2*time2+(hsCRP3+hsCRP4)/2*time3]/time4;
- Personnel who have participated in the physical examination in 2006, 2008 and 2012:cumhsCRP=[(hsCRP1+hsCRP2)/2*time1+(hsCRP2+hsCRP4)/2*time5]/time4;
- Personnel who have participated in the physical examination in 2006, 2010 and 2010:cumhsCRP=[(hsCRP1+hsCRP3)/2*time6+(hsCRP3+hsCRP4)/2*time3]/time4;
- Personnel who have participated in the physical examination in 2006 and 2012:cumhsCRP=[(hsCRP1+hsCRP4)/2*time4]/time4.
The variables hsCRP1, hsCRP2, hsCRP3, and hsCRP4 represent the hsCRP levels measured during physical examinations in 2006, 2008, 2010, and 2012, respectively. The variables time1, time2, time3, time4, time5, and time6 indicate the time intervals (in years) between consecutive physical examinations for the periods 2006–2008, 2008–2010, 2010–2012, 2006–2012, 2008–2012, and 2006–2010, respectively. The average durations for time1, time2, time3, time4, time5, and time6 are 2.13, 1.95, 2.27, 6.36, 4.22, and 4.06 years, respectively.
High time-weighted cumulative hsCRP level was defined as cumhsCRP ≥ 2 mg/L. Therefore, participants were divided into two groups: cumhsCRP < 2 mg/L (N=34,136) and cumhsCRP ≥ 2 mg/L (N=14,567).The selection of the 2 mg/L cutoff for hsCRP in this study was based on well-established clinical practice guideline, some large-scale cohort studies and randomized controlled trials,26–29 which categorize individuals with hsCRP levels below 2 mg/L as having lower cardiovascular risk and those above 2 mg/L as having higher risk. This dichotomy reflects the underlying inflammatory activity relevant to atherosclerosis and its complications. Therefore, employing this validated and clinically relevant cutoff allows for a more direct comparison of our findings with the broader field of cardiovascular epidemiology.
Statistical Analysis
Data analysis was performed using SAS 9.4 (SAS Institute, Cary, North Carolina). Normally distributed continuous variables were expressed as means ± standard deviations () and compared between groups using independent sample t-tests. Non-normally distributed continuous variables were expressed as medians (p25, p75) and compared using nonparametric rank-sum tests (Kruskal–Wallis). Categorical variables were expressed as frequencies and percentages, with group comparisons conducted using chi-square tests.
The Kaplan-Meier method was used to calculate cumulative incidence rates of CCB in different groups, with group comparisons performed using Log rank tests. To examine the effect of cumhsCRP on the incidence of new-onset CCB, a proportional hazards Cox regression model was used, with the occurrence of CCB as the dependent variable and different levels of cumhsCRP as the independent variable. The cumhsCRP < 2 mg/L group was used as the reference. Adjustments were made for age, sex, smoking (yes/no), alcohol consumption (yes/no), physical activity (yes/no), high salt intake (yes/no), body mass index (BMI), LDL-C, baseline use of antihypertensive, hypoglycemic, or lipid-lowering medications (yes/no), and new-onset myocardial infarction and heart failure during follow-up (yes/no), as well as hsCRP levels in 2006 and 2012. Log-transformed cumhsCRP was treated as a continuous variable, and restricted cubic spline curves were drawn with nodes at the 10th, 50th, and 90th percentiles of log(cumhsCRP) to explore the dose-response relationship between log(cumhsCRP) and new-onset CCB.
To compare the relative impacts of cumhsCRP and baseline hsCRP on the risk of new-onset cardiac conduction block, we performed additional Cox regression analyses, treating hsCRP levels measured in 2006 and 2012 separately as independent variables. After adjusting for the same covariates, we additionally adjusted for the time-weighted cumulative hsCRP level (from 2006 to 2012) in the final model.
To assess the robustness of the findings, sensitivity analyses were conducted by regrouping participants based on cumhsCRP concentrations according to different cardiovascular disease risk,30 excluding participants who experienced endpoint events within the first 2 years of follow-up, as well as those with a history of malignancy, heart failure, atrial fibrillation, myocardial infarction, or who has a history of coronary revascularization, or who used beta-blockers or non-dihydropyridine calcium channel blockers. To account for the potential influence of all-cause mortality on endpoint events, a competing risk model (Fine-Gray model) for death was constructed for the entire population. Stratified analyses were performed by stratifying participants by age (<45, 45 to 65, 65 to 80, ≥80 years), sex (male or female), and BMI (<24 kg/m² or ≥24 kg/m²), and the potential multiplicative interaction between these factors and cumhsCRP was explored using the proportional hazards Cox regression model. A two-sided p-value of <0.05 was considered statistically significant.
Results
Of the 70,156 participants who completed at least the 2006 and 2012 health examinations and had complete electrocardiogram data, 12,957 were excluded due to missing hsCRP data, 2,611 due to a diagnosis of CCB prior to or in 2012, and 5,885 due to hsCRP > 10 mg/L during any examination within the exposure period, leaving 48,703 participants for statistical analysis (Figure 1).
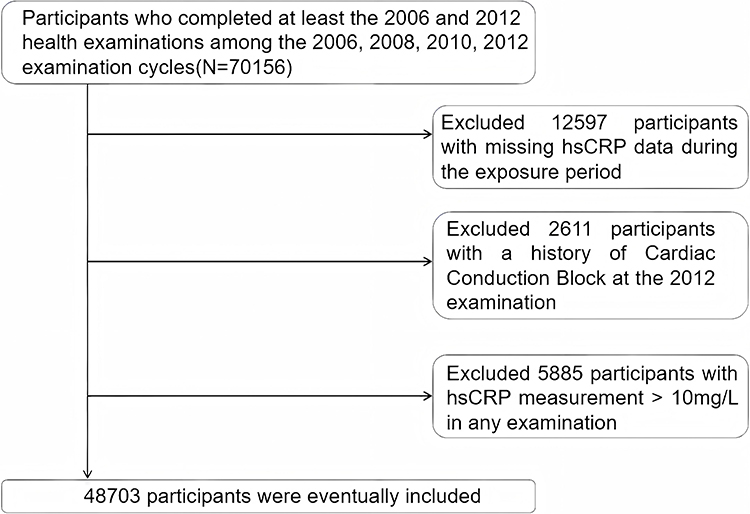 |
Figure 1 Inclusion and exclusion flow chart. |
Baseline Characteristics
Baseline characteristics of the participants in 2012 are shown in Table 1. The average age was 55.38 ± 11.66 years, with males accounting for 76.61% of the population. Results indicated that age, BMI, hsCRP levels in 2006 and 2012, fasting blood glucose (FBG), and LDL-C levels increased with increasing cumhsCRP levels. The proportion of current smokers, users of antihypertensive, hypoglycemic, or lipid-lowering medications at baseline, and individuals with new-onset myocardial infarction and heart failure during follow-up were significantly higher in groups with higher cumhsCRP levels (p < 0.001).
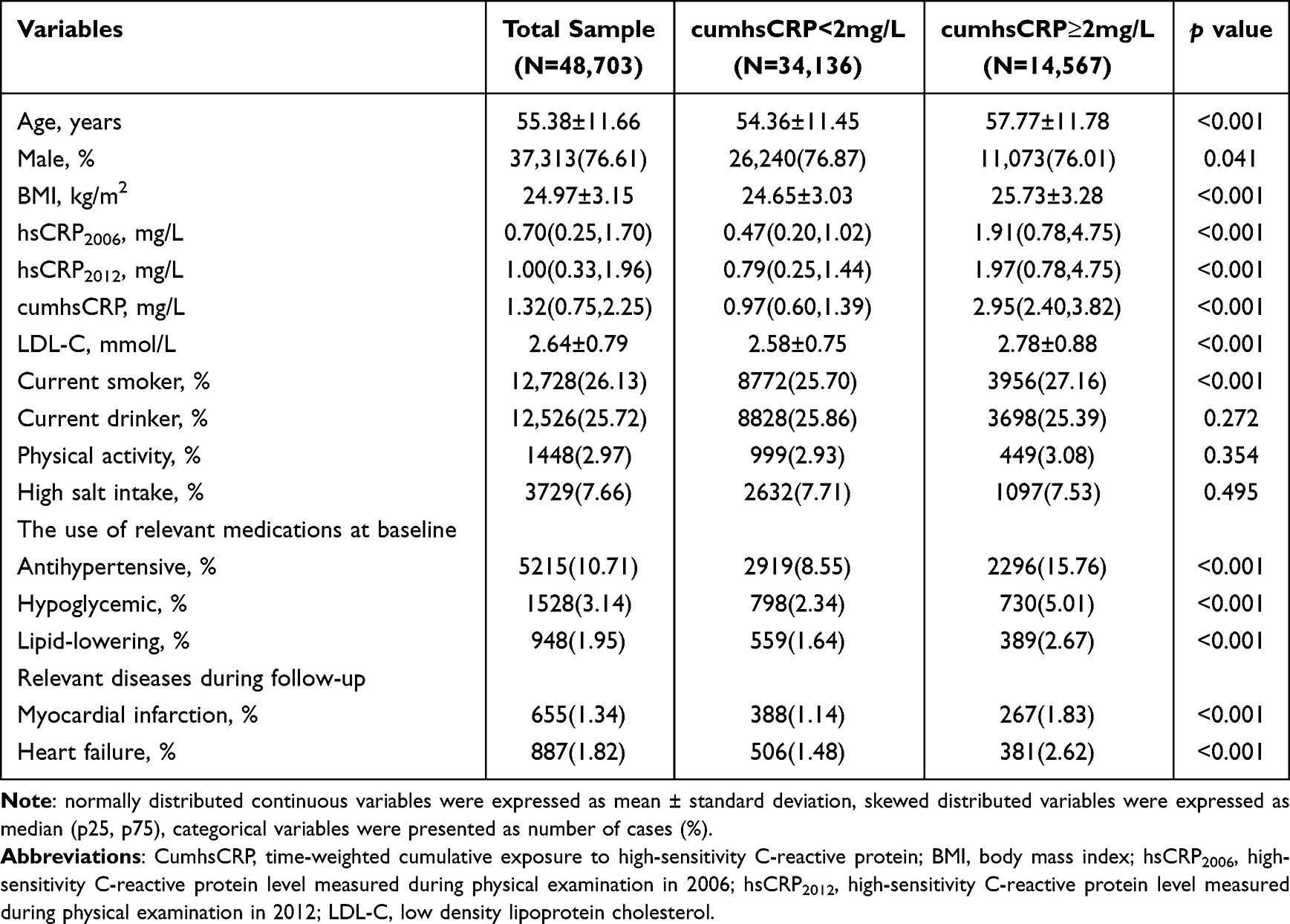 |
Table 1 Baseline Characteristics of the Individuals Selected for Study |
Incidence of New-Onset Cardiac Conduction Block by Group
The mean follow-up duration was 9.24 ± 1.60 years, during which 803 cases of new-onset CCB were recorded (1.65%). The incidence densities of CCB in the cumhsCRP < 2 mg/L and cumhsCRP ≥ 2 mg/L groups were 1.66 and 2.09 per 1,000 person-years, respectively. The cumulative incidence of CCB increased with higher time-weighted cumulative hsCRP exposure, and the Log rank test showed significant differences between groups (p = 0.002; Figure 2).
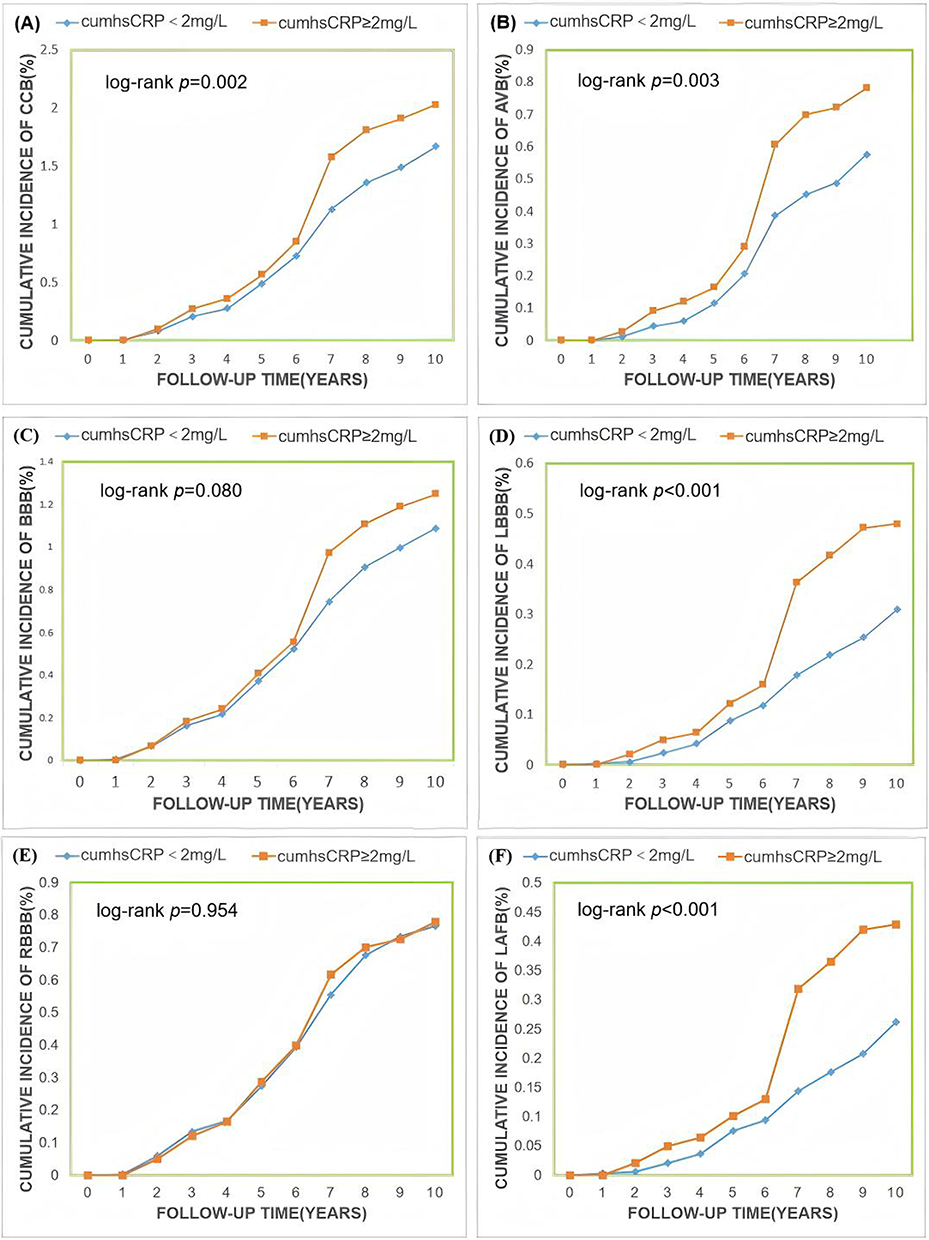 |
Figure 2 Cumulative incidence of Cardiac Conduction Block. Notes: (A) cardiac conduction block. (B) atrioventricular block. (C) bundle branch block. (D) left bundle branch block. (E) right bundle branch block. (F) left anterior fascicular block. |
Multivariable Cox analysis showed that participants in the cumhsCRP ≥ 2 mg/L group had a 24% higher risk of developing CCB compared to the cumhsCRP < 2 mg/L group (HR:1.24, 95% CI: 1.07,1.44). For each interquartile range (IQR) increase in cumhsCRP, the hazard ratio (HR) for new-onset CCB was 1.10 (95% CI: 1.04,1.16; Table 2). In the analysis of baseline hsCRP and the risk of new-onset cardiac conduction block, using 2006 and 2012 as baseline years, the risk ratios (95% CI) for the hsCRP ≥ 2 mg/L group compared with the hsCRP < 2 mg/L group were 1.20 (1.08,1.34) and 1.05 (0.86,1.30), respectively (Supplementary Table 2).After adjusting for the variables mentioned above, a restricted cubic spline curve was plotted to illustrate the relationship between log(cumhsCRP) and CCB risk. The results indicated a linear relationship between log(cumhsCRP) and CCB risk (p for overall association < 0.001; p for non-linearity = 0.294; Figure 3).
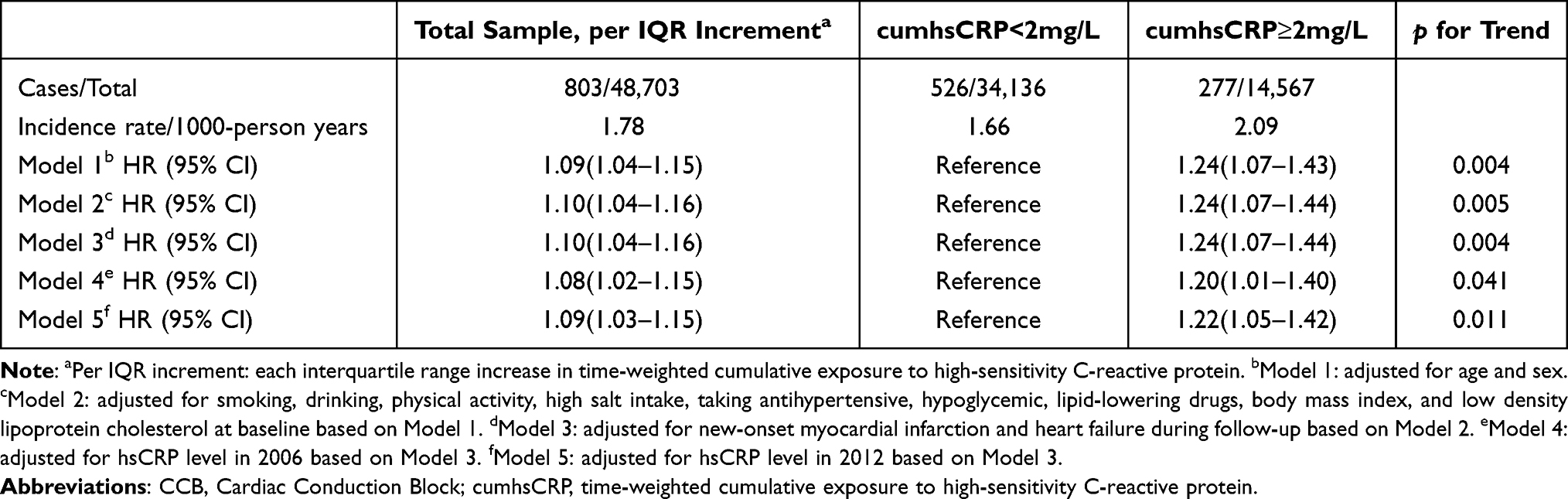 |
Table 2 Multivariate Cox Proportional Hazards Regression Model for the Incidence of CCB |
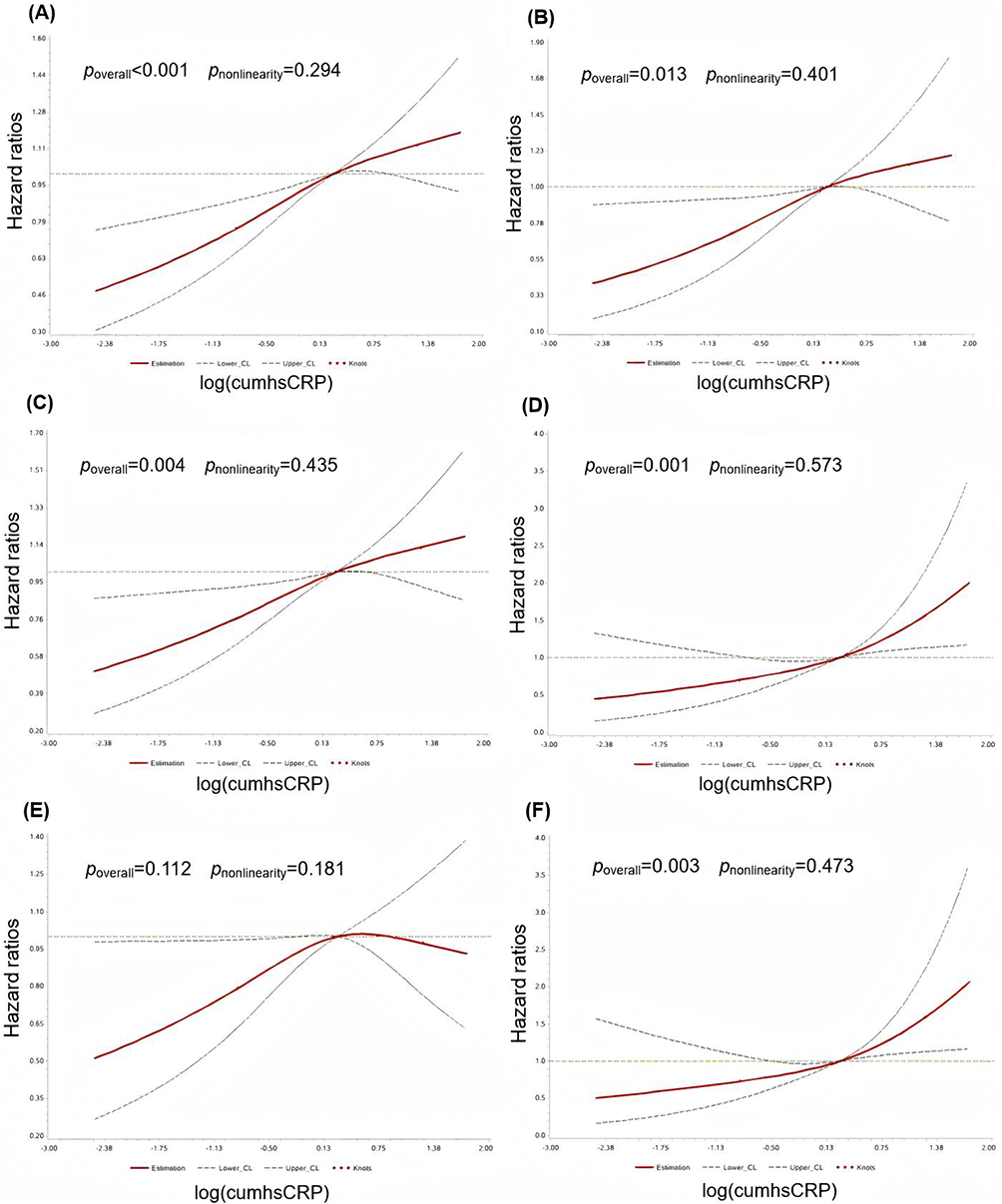 |
Figure 3 Restricted cubic spline curves of the effect of log(cumhsCRP) on the incidence of Cardiac Conduction Block. Abbreviations: HR, hazard ratio; CI, confidence interval; Log(cumhsCRP), log-transformed time-weighted cumulative exposure to high-sensitivity C-reactive protein. Notes: (A) cardiac conduction block. (B) atrioventricular block. (C) bundle branch block. (D) left bundle branch block. (E) right bundle branch block. (F) left anterior fascicular block. |
Incidence of Subtypes of New-Onset Cardiac Conduction Block
Among the 803 cases of new-onset CCB, 283 were atrioventricular block (AVB), 513 were bundle branch block (BBB), 152 were left bundle branch block (LBBB), 355 were right bundle branch block (RBBB), 6 cases of indeterminate/non-specific intraventricular conduction delay.,130 were left anterior fascicular block (LAFB), and 5 were left posterior fascicular block (LPFB). Proportional hazards Cox regression analysis showed that compared to the cumhsCRP < 2 mg/L group, the hazard ratios (95% CI) for new-onset AVB, BBB, LBBB, RBBB, and LAFB in the cumhsCRP ≥ 2 mg/L group were 1.38 (1.08,1.76), 1.18 (0.98,1.42), 1.71 (1.23,2.38), 1.01 (0.80,1.27), and 1.82 (1.28,2.60), respectively (Table 3). The cumulative incidence of each CCB subtype increased with higher time-weighted cumulative hsCRP exposure (Figure 2). After adjusting for confounding factors, a restricted cubic spline curve was plotted using log(cumhsCRP) as a continuous variable, showing a linear relationship between log(cumhsCRP) and the risk of AVB, BBB, LBBB, and LAFB (Figure 3).
 |
Table 3 Multivariate Cox Proportional Hazards Regression Model for the Incidence of Subtypes of CCB |
Sensitivity Analysis
To further validate the robustness of the results, sensitivity analyses were performed by regrouping participants based on cumhsCRP concentrations according to different cardiovascular disease risk, excluding participants who experienced endpoint events within the first two years of follow-up, as well as those with a history of malignancy, heart failure, atrial fibrillation, myocardial infarction, coronary revascularization, or use of beta-blockers or non-dihydropyridine calcium channel blockers. The results showed that the risk of new-onset CCB continued to increase with higher cumhsCRP exposure, consistent with the primary findings. A total of 4,374 all-cause deaths were reported in this study. To account for the potential influence of all-cause mortality on follow-up outcomes, a competing risk model was applied. Cox regression analysis, adjusted for the same confounding factors, showed results consistent with the primary findings (Table 4).
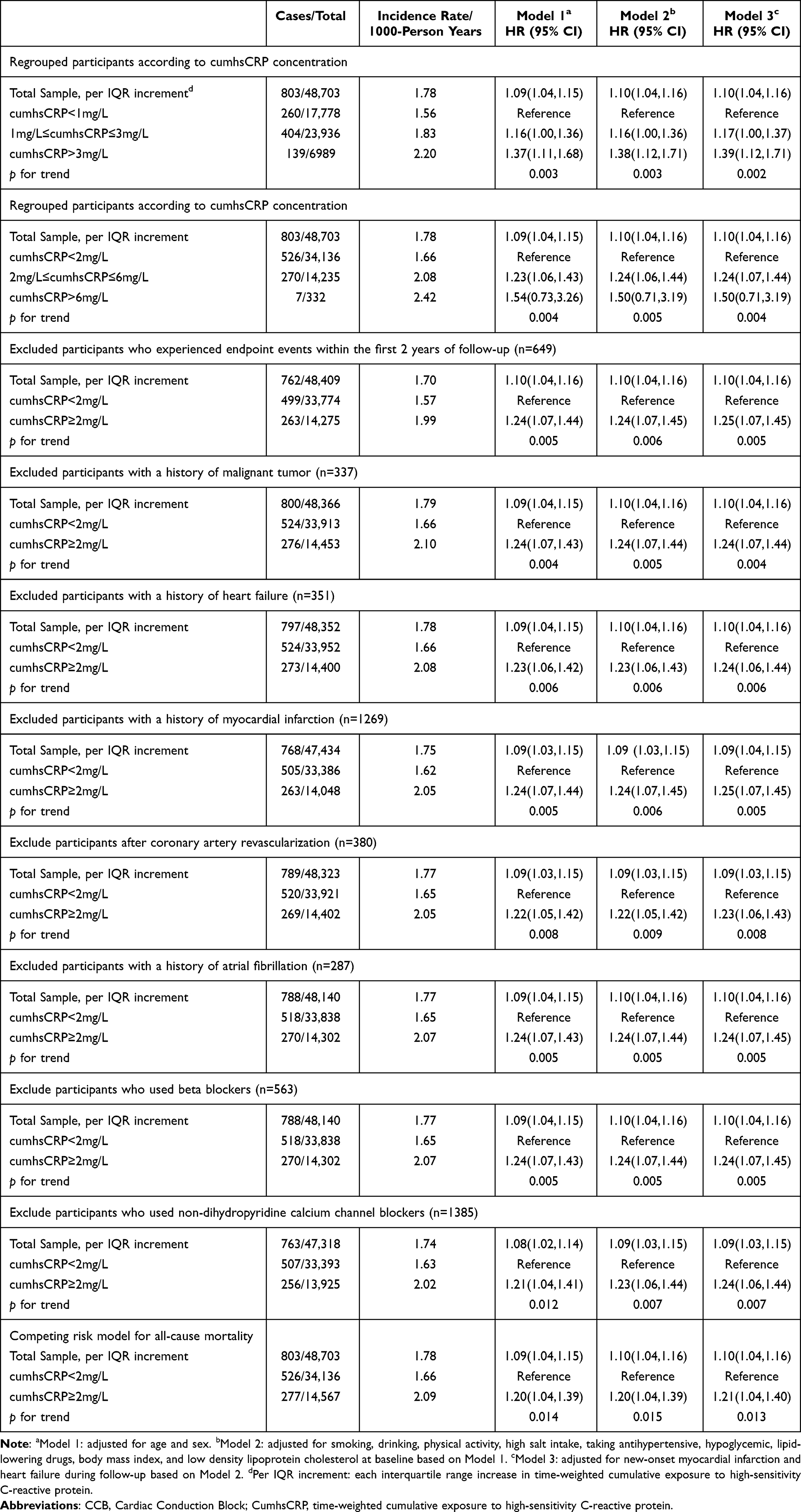 |
Table 4 Sensitivity Analyses of the Association Between cumhsCRP and Incidence of CCB |
Stratified Analysis
To explore potential multiplicative interactions between age, sex, BMI, and CCB, stratified analyses were conducted. Proportional hazards Cox regression analysis showed that in the cumhsCRP ≥ 2 mg/L group, males, middle-aged and older adults, and overweight individuals (BMI ≥ 24 kg/m²) had higher risks of CCB compared to the cumhsCRP < 2 mg/L group. The HRs (95% CI) were 1.24 (1.06,1.46), 1.28 (1.10,1.50), and 1.28 (1.07,1.53), respectively (Table 5).
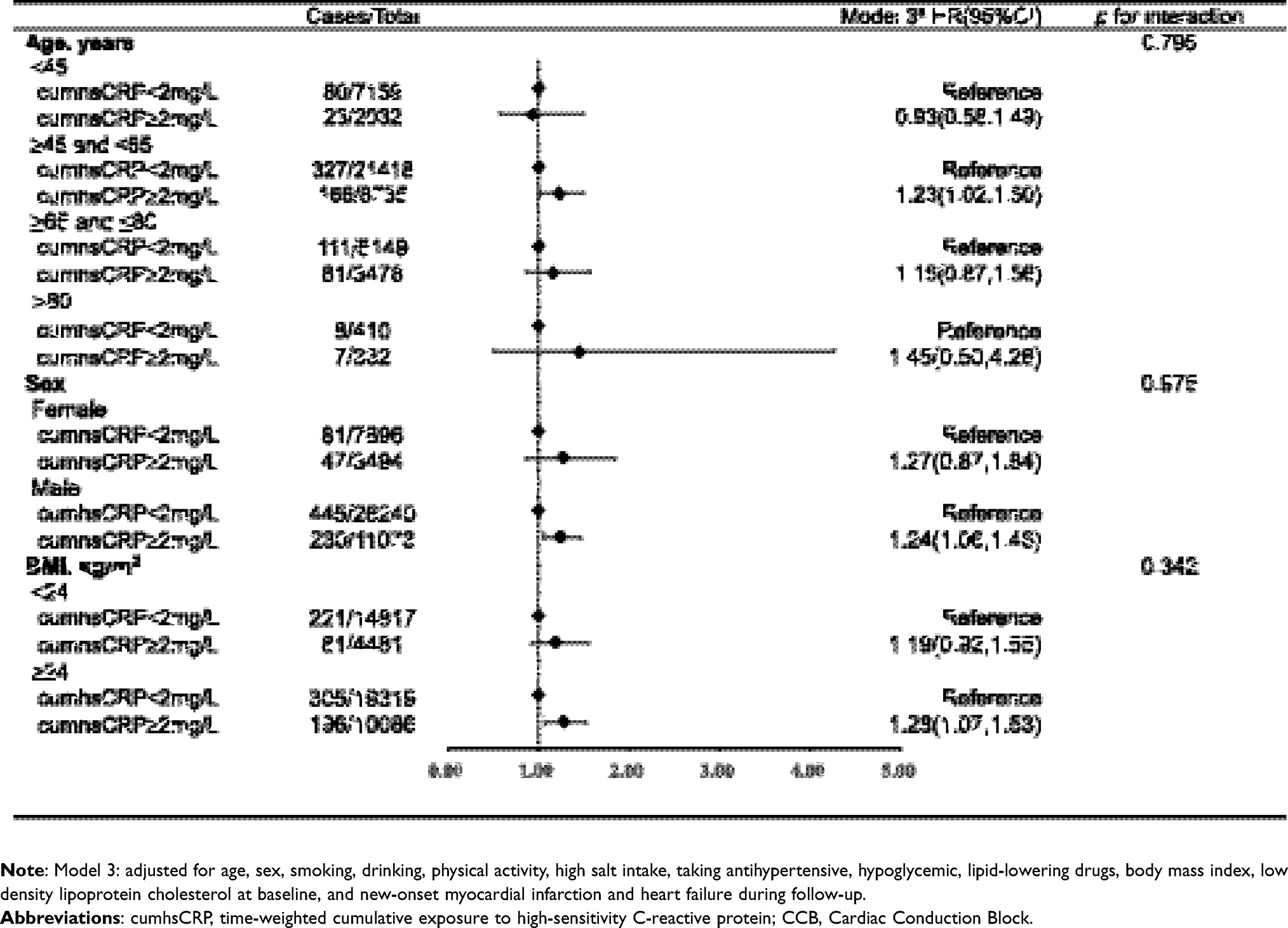 |
Table 5 Stratified Analyses of the Impact of cumCRP Exposure Levels on the Risk of Incident CCB |
Discussion
This study revealed that time-weighted cumulative high hsCRP exposure is positively associated with the risk of new-onset CCB, demonstrating a dose-response relationship. The association between cumulative hsCRP levels and conduction block risk was stronger than that observed with single hsCRP measurements. This relationship is more pronounced in LBBB and LAFB, but it is not significant in the RBBB.
We identified cumulative high hsCRP exposure as a risk factor for CCB, with the cumhsCRP ≥ 2 mg/L group showing a 24% increased risk of CCB compared to the cumhsCRP < 2 mg/L group. Additionally, for each interquartile range (IQR) increase in cumhsCRP, the risk of CCB increased by 10%. These findings suggest that high cumulative hsCRP exposure is a risk factor for new-onset CCB, with a dose-response relationship between cumhsCRP and CCB risk. This was further confirmed by the restricted cubic spline analysis.
Previous studies have demonstrated a positive association between high hsCRP levels and the risk of CCB, but these were based on single hsCRP measurements. For example, Frimodt-Møller et al investigated 4,314 individuals aged 65 and above, reporting that elevated baseline hsCRP levels predicted cardiac conduction block events, with a 10 mg/L increase in hsCRP associated with a hazard ratio of 1.10 (95% CI: 1.03,1.17).21 Another cohort study based on the UK Biobank found a significant positive correlation between CRP levels and bradycardia events. Compared to the group with lower CRP levels (<0.5 mg/L), the risk of bradycardia increased by 15%, 18%, and 30% in the CRP 3.0–4.0 mg/L, 4.0–10.0 mg/L, and ≥10.0 mg/L groups, respectively.31 Compared to these previous studies, our study used a time-weighted cumulative exposure method to evaluate the relationship between hsCRP and CCB, resulting in more reliable findings.
The impact of risk factor exposure on adverse outcomes depends not only on the dose but also on the duration of exposure. Previous studies on the relationship between hsCRP and CCB primarily focused on single-point exposure levels without considering exposure duration. Our study not only confirmed that cumulative high hsCRP levels are a risk factor for CCB but also demonstrated that cumulative hsCRP is more strongly associated with CCB than single-timepoint measurements. In the primary model, the risk of CCB increased by 24% in the cumhsCRP ≥ 2 mg/L group compared to the cumhsCRP < 2 mg/L group. After adjusting for hsCRP levels in 2006 and 2012, the risk ratio slightly decreased. When using single hsCRP measurements from 2006 and 2012, the risk of new-onset CCB in the hsCRP ≥ 2 mg/L group increased by 29% and 12%, respectively, compared to the hsCRP < 2 mg/L group. After adjusting for cumulative hsCRP, the risk ratios decreased to 20% and 5%, respectively. Moreover, early hsCRP levels were found to have a stronger influence on the future development of CCB. Taking the groups with hsCRP < 2 mg/L in 2006 and 2012 as reference groups, the hazard ratios (95% CI) for incident CCB among individuals with hsCRP ≥ 2 mg/L were 1.20 (1.08,1.34) and 1.05 (0.86,1.30), respectively. These further indicate that the impact of inflammation on conduction block is a prolonged and chronic process. They underscore the importance of closely monitoring the body’s long-term inflammatory status. These findings are significant, suggesting that cumulative hsCRP levels should be considered, in addition to single-timepoint values, when identifying high-risk populations for CCB. With increasing digitization, cumulative hsCRP data will become more accessible.
We found that time-weighted cumulative hsCRP exposure is associated with CCB risk and exhibits site-specific dependency. Compared to the cumhsCRP < 2 mg/L group, individuals in the cumhsCRP ≥ 2 mg/L group had significantly higher risks of LAFB and LBBB, with adjusted risk ratios of 1.82 and 1.71, respectively. The association between cumulative hsCRP and AVB was weaker, and no significant association was observed with RBBB. Although this observational study cannot elucidate the underlying mechanisms, several potential explanations are considered: First of all, the left bundle branch has a complex structure and distribution, appearing as a thick band with three branches responsible for activating the left ventricle.32 Its subendocardial location and distance from the main supplying artery (the left anterior descending artery) make it more susceptible to inflammation and ischemia, leading to delayed signal conduction. Secondly, chronic high hsCRP levels often indicate systemic diseases such as diabetes33 and hypertension,34 which can cause endothelial dysfunction and left ventricular hypertrophy,35 further impairing left bundle branch conduction. Lastly, The left ventricle bears greater mechanical load under normal physiological conditions, especially under increased hemodynamic pressure, resulting in higher stress on the left bundle branch conduction system. This mechanical pressure disparity increases the risk of left bundle branch block, particularly under conditions of elevated cardiac load or structural changes.
In stratified analyses, we found that the risk of new-onset CCB increased more prominently with cumulative hsCRP exposure in middle-aged and older adults (≥45 years). In this group, the risk of CCB was 28% higher in the cumhsCRP ≥ 2 mg/L group compared to the cumhsCRP < 2 mg/L group, consistent with previous studies.21 This may be attributed to the declining cardiac function with age and the higher prevalence of hypertension, diabetes, and coronary artery disease in middle-aged and older populations. These factors, combined with elevated inflammation, increase the likelihood of conduction block. Additionally, the association between cumulative hsCRP exposure and new-onset CCB differed across BMI groups, with overweight and obese individuals (BMI ≥ 24 kg/m²) experiencing a significantly increased risk of CCB when cumhsCRP ≥ 2 mg/L. Previous studies have confirmed a positive association between high BMI and new-onset CCB,10,36 potentially due to the higher risk of coronary artery disease in obese individuals.37 Coronary artery disease can lead to ischemic events that disrupt the normal blood supply to the cardiac conduction system, causing delayed or interrupted electrical conduction.
Potential Mechanisms for the Increased Risk of CCB with Cumulative hsCRP Exposure: hsCRP is not only a marker of chronic inflammation but also an important mediator, promoting inflammation through the TLR4/NF-κB/TGF-β pathway in HL-1 cells, which contributes to myocardial fibrosis.38 Fibrosis is a key factor in the development of CCB,13 and anti-inflammatory and anti-fibrotic interventions may theoretically slow or reverse CCB progression. Additionally, local and systemic inflammation can remodel the electrophysiological processes of cardiomyocytes by disrupting the function and expression of ion channel proteins, causing membrane potential fluctuations and intracellular calcium dysregulation, thereby promoting arrhythmias.39,40 This has also been indicated in previous study:41 in sudden death young obese patients, all patients exhibited focal mononuclear cell infiltration around the sinoatrial node, along with varying degrees of fibrosis in the cardiac conduction system, which may be associated with the pro-inflammatory mechanisms of obesity.42 Our study provides evidence that elevated cumulative hsCRP levels increase the risk of CCB, independent of traditional risk factors. We hypothesize that inflammatory responses may directly drive the development and progression of conduction block.
This study has significant implications for preventing CCB. First, we extended the observation of single hsCRP measurements to longitudinal changes over time, the median (p25,p75) exposure period was 6.36 (6.04,6.62) years, highlighting the role of time-weighted cumulative hsCRP exposure in identifying high-risk populations during long-term cohort follow-up. Since hsCRP levels are modifiable, individuals at risk should adopt healthy lifestyles, including anti-inflammation diets, regular physical activity, and proper rest, to reduce inflammation43 and lower the risk of CCB. Second, while previous studies commonly used 3 mg/L as the high-risk threshold for hsCRP,30 our findings suggest that CCB risk begins to rise at hsCRP levels of 2 mg/L, emphasizing the clinical importance of lowering the risk threshold for early identification of high-risk individuals. Additionally, cumulative hsCRP exposure has a stronger association with LBBB than other subtypes. The left bundle branch plays a critical role in activating and transmitting electrical signals throughout the left ventricle, and LBBB is closely linked to adverse cardiovascular events. Early intervention to reduce high hsCRP levels may lower the incidence of these events. Finally, the study included a large sample size, long-term follow-up, and repeated measurements of hsCRP and other laboratory indicators, ensuring reliable findings. Based on the findings of this study, incorporating hsCRP testing into routine health check-ups for the general population may help identify individuals at high risk of cardiac conduction block. Such individuals could potentially benefit from more frequent ECG monitoring. For individuals with persistently elevated hsCRP, intensive lifestyle interventions—such as adopting an anti-inflammatory diet, engaging in regular physical activity, and quitting smoking—to reduce systemic inflammation may serve as a strategy to prevent future degenerative changes in the cardiac conduction system.
Despite these strengths, the study has some limitations. As our cohort was predominantly composed of middle-aged active workers (mean age 55.38 years), individuals over 65 were a minority (20%). This demographic profile, while valuable for investigating the target population of working adults, limits the extrapolation of our results to the general elderly population. Second, although we adjusted for potential confounders, the single-center nature of the study may leave residual confounding factors. Finally, this is an observational study, although we made every effort to control the confounding factors through multivariate adjustments and sensitivity analyses, residual confounding cannot be entirely ruled out, such as systematic echocardiographic evaluation, we cannot definitively rule out that undiagnosed structural heart disease (eg, aortic stenosis) may have contributed to both elevated cumhsCRP levels and the presence of conduction defects in some participants. Therefore, our findings should be interpreted as indicative of a strong association rather than a definitive causal relationship. These findings alone are insufficient to serve as direct evidence for immediate changes in clinical practice (such as initiating targeted drug therapies), but they provide an important hypothesis-generating basis for subsequent mechanistic studies and randomized controlled trials.
Conclusion
Our findings demonstrate that long-term cumulative exposure to elevated hsCRP levels is independently associated with an increased risk of incident cardiac conduction block in the general population. This supports the hypothesis that chronic low-grade inflammation may contribute not only to atherosclerotic progression but also to subclinical electrophysiological disturbances. Given the ease of hsCRP monitoring in clinical settings, cumulative inflammatory burden may serve as a valuable early marker for identifying individuals at heightened risk of cardiovascular electrical remodeling. These results highlight the importance of integrating inflammatory profiling into preventive cardiovascular diseases strategies, particularly in aging populations.
Data Sharing Statement
The datasets generated and analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study protocol was carried out following the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of Kailuan General Hospital ([2006] Med Ethics No. 5). All participants provided written informed consent for participation.
Acknowledgments
We thank the participants of the Kailuan Study and the laboratory staff of the Department of Cardiology of Kailuan General Hospital for their contributions to this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Medical Science Research Project of Hebei Province (Grant No. 20242230).
Disclosure
The authors declare that they have no competing interests.
References
1. Haimovich JS, Di Achille P, Nauffal V, et al. Frequency of electrocardiogram-defined cardiac conduction disorders in a multi-institutional primary care cohort. JACC Advances. 2024;3(7):101004. doi:10.1016/j.jacadv.2024.101004
2. Shan R, Ning Y, Ma Y, et al. Prevalence and risk factors of atrioventricular block among 15 million Chinese health examination participants in 2018: a nation-wide cross-sectional study. BMC Cardiovascu Disord. 2021;21(1):289. doi:10.1186/s12872-021-02105-3
3. Zhang J, Liu J, Ye M, Zhang M, Yao F, Cheng Y. Incidence and risk factors associated with atrioventricular block in the general population: the atherosclerosis risk in communities study and cardiovascular health study. BMC Cardiovascu Disord. 2024;24(1):509. doi:10.1186/s12872-024-04163-9
4. Cheng S, Keyes MJ, Larson MG, et al. Long-term outcomes in individuals with prolonged PR interval or first-degree atrioventricular block. JAMA. 2009;301(24):2571–2577. doi:10.1001/jama.2009.888
5. Crisel RK, Farzaneh-Far R, Na B, Whooley MA. First-degree atrioventricular block is associated with heart failure and death in persons with stable coronary artery disease: data from the heart and soul study. Eur Heart J. 2011;32(15):1875–1880. doi:10.1093/eurheartj/ehr139
6. Mandyam MC, Soliman EZ, Heckbert SR, Vittinghoff E, Marcus GM. Long-term outcomes of left anterior fascicular block in the absence of overt cardiovascular disease. JAMA. 2013;309(15):1587–1588. doi:10.1001/jama.2013.2729
7. Bussink BE, Holst AG, Jespersen L, Deckers JW, Jensen GB, Prescott E. Right bundle branch block: prevalence, risk factors, and outcome in the general population: results from the copenhagen city heart study. Eur Heart J. 2013;34(2):138–146. doi:10.1093/eurheartj/ehs291
8. Jeong JH, Kim JH, Park YH, et al. Incidence of and risk factors for bundle branch block in adults older than 40 years. Korean J Internal Med. 2004;19(3):171–178. doi:10.3904/kjim.2004.19.3.171
9. Frimodt-Møller EK, Soliman EZ, Kizer JR, et al. Lifestyle habits associated with cardiac conduction disease. Eur Heart J. 2023;44(12):1058–1066. doi:10.1093/eurheartj/ehac799
10. Liu P, Wang Y, Zhang X, et al. Obesity and cardiac conduction block disease in China. JAMA Network Open. 2023;6(11):e2342831. doi:10.1001/jamanetworkopen.2023.42831
11. Haxha S, Halili A, Malmborg M, et al. Type 2 diabetes mellitus and higher rate of complete atrioventricular block: a Danish nationwide registry. Eur Heart J. 2023;44(9):752–761. doi:10.1093/eurheartj/ehac662
12. Kerola T, Eranti A, Aro AL, et al. Risk factors associated with atrioventricular block. JAMA Network Open. 2019;2(5):e194176. doi:10.1001/jamanetworkopen.2019.4176
13. Kléber AG, Rudy Y. Basic mechanisms of cardiac impulse propagation and associated arrhythmias. Physiol Rev. 2004;84(2):431–488. doi:10.1152/physrev.00025.2003
14. Wynn TA. Cellular and molecular mechanisms of fibrosis. J Pathol. 2008;214(2):199–210. doi:10.1002/path.2277
15. Nguyen MN, Kiriazis H, Gao XM, Du XJ. Cardiac fibrosis and arrhythmogenesis. Compr Physiol. 2017;7(3):1009–1049. doi:10.1002/j.2040-4603.2017.tb00771.x
16. Shen SC, Xu J, Cheng C, et al. Macrophages promote the transition from myocardial ischemia reperfusion injury to cardiac fibrosis in mice through GMCSF/CCL2/CCR2 and phenotype switching. Acta Pharmacol Sin. 2024;45(5):959–974. doi:10.1038/s41401-023-01222-3
17. Wang A, Liu J, Li C, et al. Cumulative exposure to high-sensitivity C-reactive protein predicts the risk of cardiovascular disease. J Ame Heart Assoc. 2017;6(10). doi:10.1161/JAHA.117.005610
18. Cui C, Liu L, Qi Y, et al. Joint association of TyG index and high sensitivity C-reactive protein with cardiovascular disease: a national cohort study. Cardiovascu Diabetol. 2024;23(1):156. doi:10.1186/s12933-024-02244-9
19. Burger PM, Koudstaal S, Mosterd A, et al. C-reactive protein and risk of incident heart failure in patients with cardiovascular disease. J Amer College of Cardiol. 2023;82(5):414–426. doi:10.1016/j.jacc.2023.05.035
20. Wu L, Wu M, Zhao D, et al. Elevated high-sensitivity C-reactive protein levels increase the risk of new-onset cardiac conduction disorders. Cardiovascu Diabetol. 2023;22(1):268. doi:10.1186/s12933-023-01987-1
21. Frimodt-Møller EK, Gottdiener JS, Soliman EZ, et al. Inflammation and incident conduction disease. J Ame Heart Assoc. 2023;12(1):e027247. doi:10.1161/JAHA.122.027247
22. Wu S, Huang Z, Yang X, et al. Prevalence of ideal cardiovascular health and its relationship with the 4-year cardiovascular events in a northern Chinese industrial city. Circ Cardiovasc Qual Outcomes. 2012;5(4):487–493. doi:10.1161/CIRCOUTCOMES.111.963694
23. Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American college of cardiology/American heart association task force on practice guidelines (writing committee to revise the ACC/AHA/NASPE 2002 guideline update for implantation of cardiac pacemakers and antiarrhythmia devices) developed in collaboration with the American association for thoracic surgery and society of thoracic surgeons. J Amer College of Cardiol. 2008;51(21):e1–62. doi:10.1016/j.jacc.2008.02.032
24. Surawicz B, Childers R, Deal BJ, et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American heart association electrocardiography and arrhythmias committee, council on clinical cardiology; the American College of cardiology foundation; and the heart rhythm society. endorsed by the international society for computerized electrocardiology. J Amer College of Cardiol. 2009;53(11):976–981. doi:10.1016/j.jacc.2008.12.013
25. Zhang Y, Chen S, Tian X, et al. Association between cumulative atherogenic index of plasma exposure and risk of myocardial infarction in the general population. Cardiovascu diabetol. 2023;22(1):210. doi:10.1186/s12933-023-01936-y
26. Grundy SM, Stone NJ, Bailey AL, et al. AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Circulation. 2019;139(25):e1082–e1143. doi:10.1161/CIR.0000000000000625
27. Ridker PM, Danielson E, Fonseca FAH, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. New Engl J Med. 2008;359(21):2195–2207. doi:10.1056/NEJMoa0807646
28. Zhang W, Speiser JL, Ye F, et al. High-sensitivity C-reactive protein modifies the cardiovascular risk of lipoprotein(a): multi-ethnic study of atherosclerosis. J Amer College Cardiol. 2021;78(11):1083–1094. doi:10.1016/j.jacc.2021.07.016
29. Arnold N, Blaum C, Goßling A, et al. C-reactive protein modifies lipoprotein(a)-related risk for coronary heart disease: the BiomarCaRE project. Eur Heart J. 2024;45(12):1043–1054. doi:10.1093/eurheartj/ehad867
30. Pearson TA, Mensah GA, Alexander RW, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the centers for disease control and prevention and the American heart association. Circulation. 2003;107(3):499–511. doi:10.1161/01.CIR.0000052939.59093.45
31. Yang X, Zhao S, Wang S, et al. Systemic inflammation indicators and risk of incident arrhythmias in 478,524 individuals: evidence from the UK biobank cohort. BMC Med. 2023;21(1):76. doi:10.1186/s12916-023-02770-5
32. Padala SK, Cabrera J-A, Ellenbogen KA. Anatomy of the cardiac conduction system. Pacing Clin Electrophysiol. 2021;44(1):15–25. doi:10.1111/pace.14107
33. DeFronzo RA, Ferrannini E, Groop L, et al. Type 2 diabetes mellitus. Nature Rev Dis Primers. 2015;1:15019. doi:10.1038/nrdp.2015.19
34. Oparil S, Acelajado MC, Bakris GL, et al. Hypertension. Nat Rev Dis Prim. 2018;4(1):18014. doi:10.1038/nrdp.2018.14
35. Yildiz M, Oktay AA, Stewart MH, Milani RV, Ventura HO, Lavie CJ. Left ventricular hypertrophy and hypertension. Prog Cardiovasc Dise. 2020;63(1):10–21. doi:10.1016/j.pcad.2019.11.009
36. Frank S, Colliver JA, Frank A. The electrocardiogram in obesity: statistical analysis of 1,029 patients. J Amer College of Cardiol. 1986;7(2):295–299. doi:10.1016/S0735-1097(86)80494-6
37. Park J-S, Ahn S-G, Hwang J-W, et al. Impact of body mass index on the relationship of epicardial adipose tissue to metabolic syndrome and coronary artery disease in an Asian population. Cardiovascu diabetol. 2010;9(1):29. doi:10.1186/1475-2840-9-29
38. Sun W, Wu Y, Gao M, et al. C-reactive protein promotes inflammation through TLR4/NF-κB/TGF-β pathway in HL-1 cells. Biosci Rep. 2019;39(8). doi:10.1042/BSR20190888
39. Hagiwara Y, Miyoshi S, Fukuda K, et al. SHP2-mediated signaling cascade through gp130 is essential for LIF-dependent ICaL, [Ca2+]i transient, and APD increase in cardiomyocytes. J Mol Cell Cardiol. 2007;43(6):710–716. doi:10.1016/j.yjmcc.2007.09.004
40. Kawada H, Niwano S, Niwano H, et al. Tumor necrosis Factor-.ALPHA. Downregulates the voltage gated outward k+ current in cultured neonatal rat cardiomyocytes a possible cause of electrical remodeling in diseased hearts. Circulation J. 2006;70(5):605–609. doi:10.1253/circj.70.605
41. Bharati S, Lev M. Cardiac conduction system involvement in sudden death of obese young people. Am Heart J. 1995;129(2):273–281. doi:10.1016/0002-8703(95)90008-X
42. Lu X, Kong X, Wu H, et al. UBE2M-mediated neddylation of TRIM21 regulates obesity-induced inflammation and metabolic disorders. Cell Metab. 2023;35(8):1390–1405.e1398. doi:10.1016/j.cmet.2023.05.011
43. Kasapis C, Thompson PD. The effects of physical activity on serum C-reactive protein and inflammatory markers: a systematic review. J Amer College Cardiol. 2005;45(10):1563–1569. doi:10.1016/j.jacc.2004.12.077
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
U-Shaped Association Between Monocyte-Lymphocyte Ratio and Risk of Cardiac Conduction Block

Li M, Li X, Gao H, Li P, Zhang L, Zhang X, Liu P, Yang X, Wu L, Zeng J, Wu S, Sun L
Journal of Inflammation Research 2023, 16:5393-5402
Published Date: 18 November 2023
The Combination of Hyperuricemia and Elevated High-Sensitivity C-Reactive Protein Increased the Risk of Cardiac Conduction Block

Li N, Cui L, Tse G, Korantzopoulos P, Letsas KP, Bazoukis G, Chen S, Zhang N, Yang X, Liu P, Wu L, Yan GX, Lip GYH, Wu S, Liu T
Journal of Inflammation Research 2024, 17:3725-3736
Published Date: 11 June 2024