Back to Journals » Infection and Drug Resistance » Volume 19
Tigecycline-Associated Hypofibrinogenemia and Major Bleeding: Incidence, Predictors, and Clinical Outcomes in a Retrospective Cohort
Authors Huang YT, Yang JS, Huang YM ![]() , Tseng YJ, Lin FJ
, Tseng YJ, Lin FJ ![]()
Received 8 March 2026
Accepted for publication 27 May 2026
Published 9 June 2026 Volume 2026:19 607775
DOI https://doi.org/10.2147/IDR.S607775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Yu-Ting Huang,1,2 Jhih Syuan Yang,2 Yen-Ming Huang,1– 3 Yu-Ju Tseng,1,2 Fang-Ju Lin2– 4
1Department of Pharmacy, National Taiwan University Hospital, Taipei City, 100229, Taiwan; 2School of Pharmacy, College of Medicine, National Taiwan University, Taipei City, 100025, Taiwan; 3Graduate Institute of Clinical Pharmacy, College of Medicine, National Taiwan University, Taipei City, 100025, Taiwan; 4Department of Pharmacy, National Taiwan University Cancer Center, Taipei City, 106037, Taiwan
Correspondence: Yu-Ju Tseng, Department of Pharmacy, National Taiwan University Hospital, Taipei City, 100229, Taiwan, Email [email protected]
Background: Tigecycline-associated hypofibrinogenemia has been increasingly reported, but its clinical significance and predictors of bleeding remain unclear. We assessed incidence, predictors, and bleeding outcomes in routine care.
Methods: We conducted a retrospective cohort study of adults receiving tigecycline at a tertiary medical center in 2022. Hypofibrinogenemia was defined as fibrinogen less than 200 mg/dL during treatment. Major bleeding was defined using International Society on Thrombosis and Haemostasis criteria. Patients were followed from treatment initiation until 7 days after discontinuation. Multivariable logistic regression identified independent predictors of hypofibrinogenemia and major bleeding. Receiver operating characteristic analyses determined optimal cut-offs using the Youden index.
Results: Among 231 included patients, 98 (42.4%) developed hypofibrinogenemia. Major bleeding occurred in 52 (22.5%) patients and was more frequent in patients with hypofibrinogenemia (30.6% vs 16.5%, p = 0.01). Independent predictors of hypofibrinogenemia included baseline fibrinogen less than 350 mg/dL (aOR: 3.27, 95% CI: 1.73– 6.19), hemodialysis (aOR: 2.34, 95% CI: 1.02– 5.38), peptic ulcer disease (aOR: 7.10, 95% CI: 1.38– 38.53), and cumulative tigecycline dose greater than 1125 mg (aOR: 2.60, 95% CI: 1.40– 4.84). Hypofibrinogenemia was the only independent predictor of major bleeding (aOR: 2.25, 95% CI: 1.14– 4.44).
Conclusion: Hypofibrinogenemia was common during tigecycline therapy and independently associated with major bleeding. Baseline fibrinogen and cumulative exposure may help identify high-risk patients. Routine fibrinogen monitoring should be considered during tigecycline treatment.
Plain Language Summary: Tigecycline is often used when infections are difficult to treat, especially when bacteria are resistant to many standard antibiotics. However, this drug can sometimes lower fibrinogen, a clotting protein that helps prevent bleeding. This change may not be noticed right away, but it can become clinically important during treatment.
We studied hospitalized adults who received tigecycline at a tertiary medical center. Our goal was to find out how often low fibrinogen developed, which patients were at higher risk, and whether this complication was associated with bleeding. We found that hypofibrinogenemia was common and was linked to major bleeding. Higher-risk groups included people with lower fibrinogen levels before treatment, those undergoing hemodialysis, those with peptic ulcer disease, and those who received a greater total amount of tigecycline.
Our results support the use of fibrinogen monitoring before and during tigecycline treatment. This may be particularly helpful when longer treatment courses are expected or when patients already have factors that increase bleeding risk.
Keywords: tigecycline, hypofibrinogenemia, bleeding
Introduction
Tigecycline is a glycylcycline antimicrobial derived from minocycline that exhibits broad-spectrum activity against multidrug-resistant (MDR) gram-positive, gram-negative, and anaerobic pathogens. Owing to its stability against common tetracycline resistance mechanisms, including efflux pumps and ribosomal protection proteins, tigecycline is frequently used for severe infections caused by carbapenem-resistant Acinetobacter baumannii, extended-spectrum β-lactamase–producing Enterobacterales (ESBL), and vancomycin-resistant Enterococci (VRE).1,2 Its large volume of distribution and prolonged half-life support use in deep-seated infections; however, systemic exposure may also contribute to off-target effects.2,3
Beyond gastrointestinal intolerance and liver enzyme elevations, increasing post-marketing evidence has identified coagulation abnormalities during tigecycline therapy.4 Among these, hypofibrinogenemia has emerged as a clinically relevant laboratory abnormality. A systematic review reported that tigecycline may be associated with decreased fibrinogen levels and prolongation of prothrombin time and activated partial thromboplastin time, suggesting impaired synthesis or altered regulation of coagulation factors. Recent observational and real-world studies have consistently reported a high incidence of tigecycline-associated hypofibrinogenemia, generally ranging from approximately 38% to more than 60% in treated patients.5–11 In response, the tigecycline prescribing information was updated in 2021 to recommend monitoring coagulation parameters, particularly fibrinogen, before and during therapy.3
Despite growing recognition of tigecycline-associated hypofibrinogenemia, its clinical implications remain incompletely understood. Some studies have identified hypofibrinogenemia as an independent predictor of bleeding,6 whereas others have observed marked declines in fibrinogen levels without a corresponding increase in clinically overt hemorrhage.8 These inconsistent findings may be attributable to variations in patient populations, illness severity, baseline coagulation status, cumulative tigecycline exposure, concomitant medications, fibrinogen monitoring practices, and definitions of bleeding outcomes across studies.10 Furthermore, the underlying mechanisms of tigecycline-associated fibrinogen decline have not been fully illustrated. Proposed mechanisms include impaired hepatic protein synthesis, inflammation-related fibrinogen consumption, and dose-dependent pharmacodynamic effects.11
From both clinical and antimicrobial stewardship perspective, identifying patients at increased risk is important when prolonged or high-dose tigecycline therapy is considered. Recent multicenter and retrospective studies have reported several potential risk factors for tigecycline-associated hypofibrinogenemia, including older age, longer treatment duration, greater tigecycline exposure, and impaired baseline hepatic or coagulation function.5,9,11,12 However, most prior studies have primarily focused on hypofibrinogenemia itself, while the relationship between these factors and clinically important bleeding remains less well characterized. To our knowledge, data specifically evaluating tigecycline-associated bleeding outcomes in Taiwanese populations are limited, and regional differences in comorbidity profiles and antimicrobial utilization patterns may influence risk estimates. Therefore, we conducted a retrospective cohort study of adults receiving tigecycline to determine the incidence and timing of hypofibrinogenemia and major bleeding using prespecified criteria,13 and to identify independent clinical factors associated with these outcomes.
Materials and Methods
Study Design and Data Source
We conducted a retrospective cohort study at National Taiwan University Hospital (NTUH), a tertiary academic medical center in Taipei, Taiwan. Electronic health record data were extracted from the NTUH Integrated Medical Database (NTUH iMD) for patients treated between January 1 and December 31, 2022. The year 2022 was selected because the tigecycline prescribing information was updated in 2021 to recommend routine monitoring of coagulation parameters, including fibrinogen, before and during therapy, which increased the likelihood of systematic laboratory assessment during clinical use.
The study protocol was approved by the NTUH Research Ethics Committee (approval number: 202302047RINC) and conducted in accordance with the principles of the Declaration of Helsinki. Because this study used a retrospective design with de-identified data, the requirement for informed consent was waived.
Study Population
Adult patients of 18 years or older who received at least one dose of intravenous tigecycline during the study period were screened. Patients were excluded if tigecycline therapy lasted less than 72 hours, if baseline fibrinogen measurement within 48 hours prior to tigecycline initiation was unavailable, if no follow-up fibrinogen measurement was obtained during therapy, or if baseline fibrinogen was less than 200 mg/dL. Figure 1 depicts the process of patient selection. The index date was defined as the first day of tigecycline administration. Patients were followed from the index date until 7 days after tigecycline discontinuation, hospital discharge, or death, whichever occurred first.
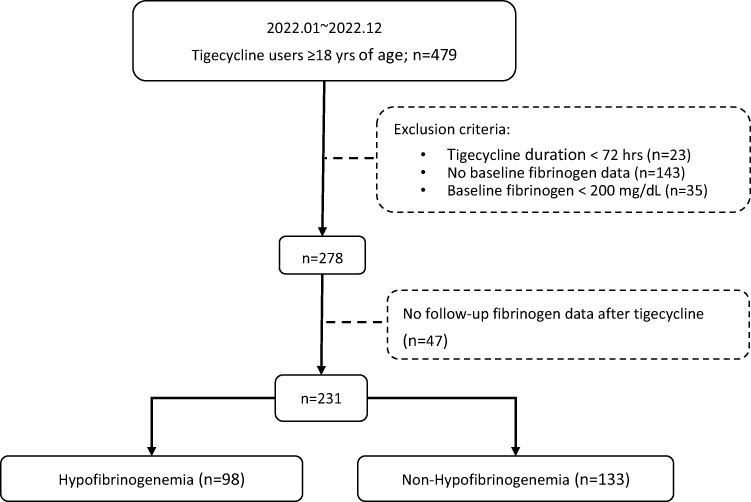 |
Figure 1 Flowchart of patient selection. |
Data Collection and Exposure Assessment
Baseline demographic characteristics, comorbidities, intensive care unit admission, and concomitant antithrombotic therapy (ie., anticoagulants and/or antiplatelet agents) were recorded. Laboratory data collected within 48 hours before tigecycline initiation included alanine aminotransferase (ALT), total bilirubin, serum creatinine (SCr), blood urea nitrogen (BUN), hemoglobin, platelet count, albumin, and international normalized ratio, and fibrinogen.
Tigecycline exposure variables included loading dose, daily maintenance dose, treatment duration, and cumulative dose, defined as the total administered dose during therapy, including the loading dose when applicable. Standard-dose therapy consisted of a 100 mg loading dose followed by 50 mg every 12 hours, whereas high-dose therapy consisted of a 200 mg loading dose followed by 100 mg every 12 hours, according to prescribing recommendations. High-dose therapy was defined as a maintenance dose greater than 100 mg per day. For exposure-response analyses, cumulative dose was further evaluated using receiver operating characteristic analysis to determine optimal discrimination thresholds. When available, microbiological data, including pathogen identification and infection sites, were recorded to characterize clinical indications for tigecycline therapy.
Outcomes
The primary outcome was development of hypofibrinogenemia, defined as fibrinogen less than 200 mg/dL at any time during tigecycline therapy or within 7 days after discontinuation. The second outcome was major bleeding, defined according to the International Society on Thrombosis and Haemostasis (ISTH) criteria as a hemoglobin decrease greater than 2 g/dL accompanied by red blood cell transfusion or documented clinically significant bleeding occurring after tigecycline initiation.13 Minor bleeding was operationally defined as the initiation of new hemostatic therapy, including proton pump inhibitors, tranexamic acid, or somatostatin, following tigecycline initiation. The timing of hypofibrinogenemia and bleeding events was recorded relative to tigecycline initiation to assess temporal sequence.
Secondary and Subgroup Analyses
Among patients who developed hypofibrinogenemia, severity was categorized according to the nadir fibrinogen level during therapy as mild (100–200 mg/dL) or moderate-to-severe (less than 100 mg/dL). Subgroup analyses evaluated the associations between hypofibrinogenemia severity and major bleeding, as well as transfusion of fresh frozen plasma or cryoprecipitate.
Statistical Methods
Continuous variables were summarized as mean and standard deviation or median with interquartile range, as appropriate. Categorical variables were summarized as frequencies and percentages. Between-group comparisons were performed using Student’s t test or Mann–Whitney U-test for continuous variables and χ2-test or Fisher’s exact test for categorical variables. Multivariable logistic regression was performed to identify independent predictors of hypofibrinogenemia and major bleeding. Candidate variables were selected primarily based on univariate analyses (p < 0.10), with additional clinically relevant covariates included regardless of statistical significance. Multicollinearity was assessed using variance inflation factors. Because treatment duration varied across patients, cumulative exposure and intensive care unit admission were considered in adjusted models to mitigate potential time-at-risk bias. Sensitivity analyses for the major bleeding model included a parsimonious model with clinically essential covariates and a clinically informed model that additionally forced antithrombotic therapy and intensive care unit admission into the model irrespective of univariate significance. Adjusted odds ratios with 95% confidence intervals were reported. Receiver operating characteristic (ROC) curve analysis was conducted to assess discriminatory performance of continuous predictors. Optimal cut-off values were determined using the Youden index. The area under the curve was calculated to evaluate model discrimination. All statistical tests were two-sided, and p < 0.05 was considered statistically significant. Analyses were performed using Microsoft Excel 2016 (Microsoft Corp., Redmond, WA, USA) and SPSS Statistics version 31.0 (IBM Corp., Armonk, NY, USA).
Results
Study Population
During the study period, 479 adult patients received tigecycline and were screened for eligibility. A total of 231 patients met inclusion criteria and were included in the analytic cohort (Figure 1). The mean age was 64.1 ± 17.2 years, 38.5% were male, and 64.9% required intensive care unit admission at the time of tigecycline initiation. The mean tigecycline treatment duration was 13.7 ± 13.7 days, and the mean cumulative dose was 1,566.5 ± 1,536.7 mg.
Incidence and Timing of Hypofibrinogenemia
Overall, 98 patients (42.4%) developed hypofibrinogenemia (fibrinogen less than 200 mg/dL) during tigecycline therapy (Figure 1). The mean duration of therapy did not differ significantly between patients who developed hypofibrinogenemia and those who did not (14.3±15.0 vs. 13.3±12.7 days, p = 0.61). Among patients who developed hypofibrinogenemia, the mean time from tigecycline initiation to first documented fibrinogen less than 200 mg/dL was 7.5 ± 3.9 days, indicating that fibrinogen decline typically occurred during the first week of therapy.
Baseline Characteristics and Tigecycline Exposure
Baseline characteristics were generally comparable between the groups (Table 1). Patients who developed hypofibrinogenemia had significantly lower baseline fibrinogen levels (379.6 ± 136.0 vs. 465.9 ± 164.8 mg/dL, p < 0.001), were more frequently admitted to the intensive care unit (77.6% vs. 55.6%, p < 0.001), and more commonly required hemodialysis (32.7% vs. 12.8%, p < 0.001). Concomitant use of antithrombotic agents was also more frequent in the hypofibrinogenemia group (50.0% vs. 36.8%, p = 0.046). With respect to antimicrobial exposure, patients who developed hypofibrinogenemia were more likely to receive high-dose tigecycline (greater than100 mg/day, p < 0.001) and had a higher proportion of cumulative dose exceeding 1125 mg (59.2% vs 42.9%, p = 0.014).
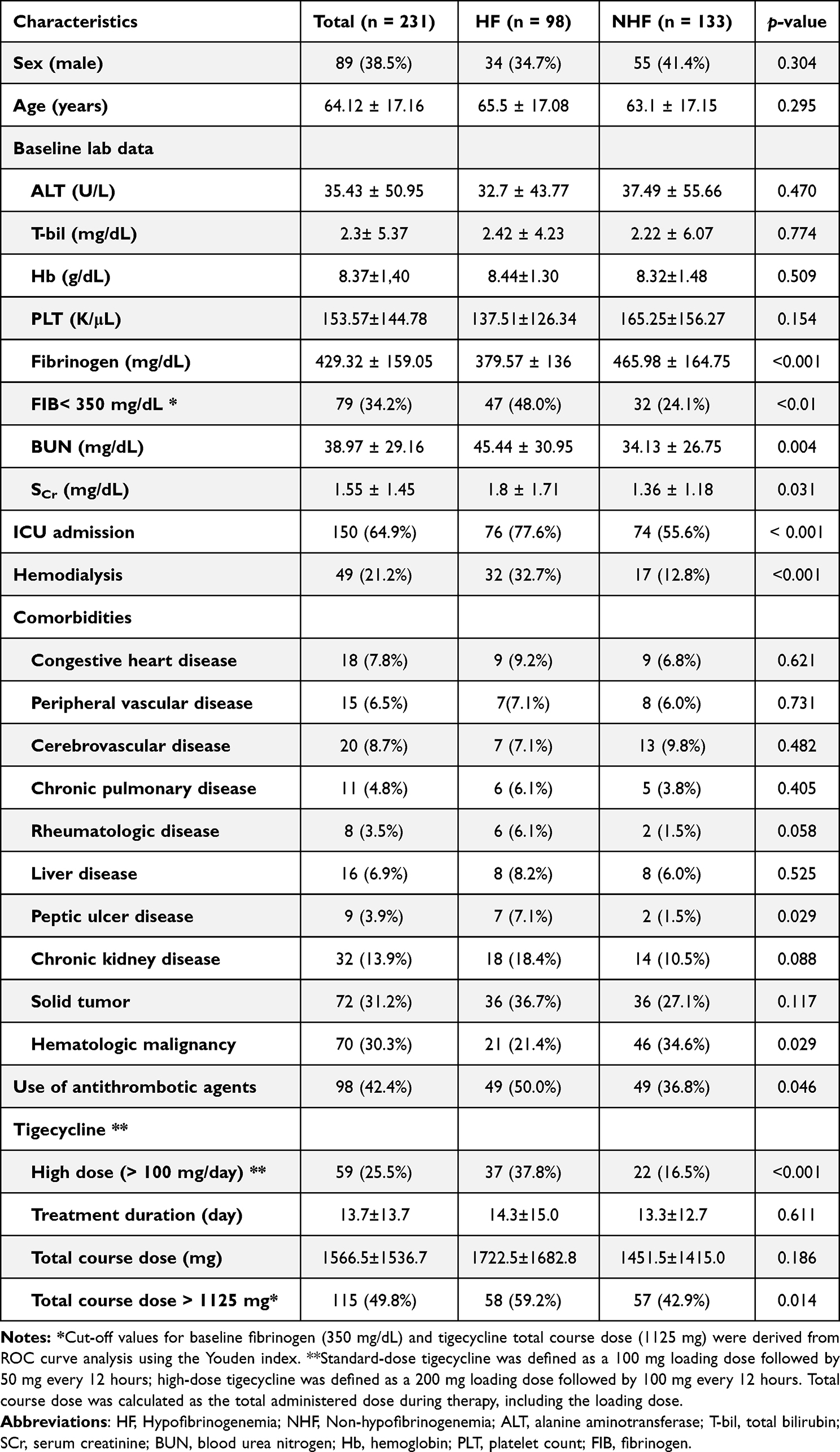 |
Table 1 Patient Characteristics Between Hypo- and Non-Hypofibrinogenemia Group |
Bleeding Events
Major bleeding occurred in 52 patients (22.5%), and minor bleeding occurred in 112 patients (48.5%) (Table 2). Both major and minor bleeding events were significantly more frequent among patients who developed hypofibrinogenemia. Major bleeding occurred in 30.6% of patients with hypofibrinogenemia compared with 16.5% those without (p = 0.01). Minor bleeding occurred in 57.1% versus 42.1%, respectively (p = 0.02). Among patients who experienced major bleeding, the events occurred a mean of 3.0 ± 3.4 days after documentation of hypofibrinogenemia, supporting a temporal association between fibrinogen decline and subsequent bleeding.
 |
Table 2 Bleeding Events in Tigecycline Users |
Risk Factors for Hypofibrinogenemia
In univariate analyses, baseline fibrinogen less than 350 mg/dL, renal dysfunction (elevated BUN or serum creatinine), hemodialysis, peptic ulcer disease, and cumulative dose greater than 1125 mg were associated with hypofibrinogenemia (Table 3). In multivariate logistic analysis independent predictors of hypofibrinogenemia were: baseline fibrinogen less than 350 mg/dL (aOR: 3.27, 95% CI: 1.73–6.19, p < 0.01), hemodialysis (aOR: 2.34, 95% CI: 1.02–5.38, p = 0.05), peptic ulcer disease (aOR: 7.10, 95% CI: 1.38–38.53, p = 0.02), and cumulative tigecycline dose greater than 1125 mg (aOR: 2.60, 95% CI: 1.40–4.84, p < 0.01) were independent predictors of hypofibrinogenemia. After adjustment, high daily dose and ICU admission were not independently associated with hypofibrinogenemia.
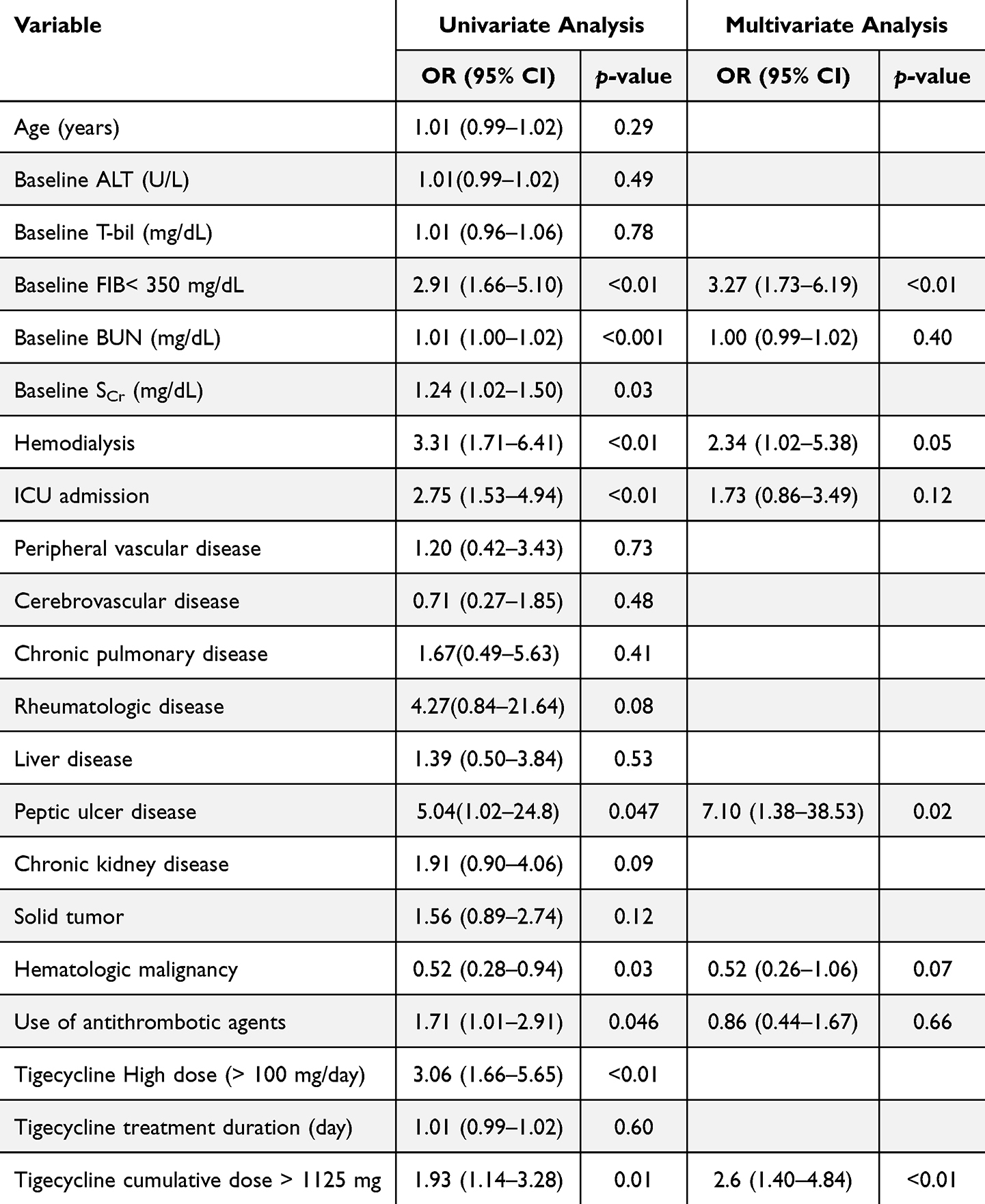 |
Table 3 Risk Factors Related to Hypofibrinogenemia in Tigecycline Users |
Risk Factor Analysis for Bleeding
Major bleeding occurred more frequently among patients with hypofibrinogenemia than those without (30.6% vs. 16.5%, p = 0.01). In multivariate analysis (Table 4), hypofibrinogenemia remained the only independent predictor of major bleeding (aOR: 2.25, 95% CI: 1.14–4.44, p = 0.02). Renal dysfunction, hemodialysis, ICU admission, and antithrombotic therapy showed numerical associations with bleeding risk but did not reach statistical significance after adjustment. Tigecycline dosing parameters, including daily dose, treatment duration, and cumulative dose, were not independently associated with major bleeding, with effect estimates similar to those of the primary analysis. Sensitivity analyses demonstrated consistent findings (Supplementary Table S1). Hypofibrinogenemia remained independently associated with major bleeding in both the parsimonious model (aOR 2.04, 95% CI 1.06–3.93, p = 0.034) and the clinically informed model that included antithrombotic therapy and ICU admission regardless of univariate significance (aOR 2.01, 95% CI 1.03–3.92, p = 0.040). Inclusion of antithrombotic therapy did not materially alter the effect estimate for hypofibrinogenemia.
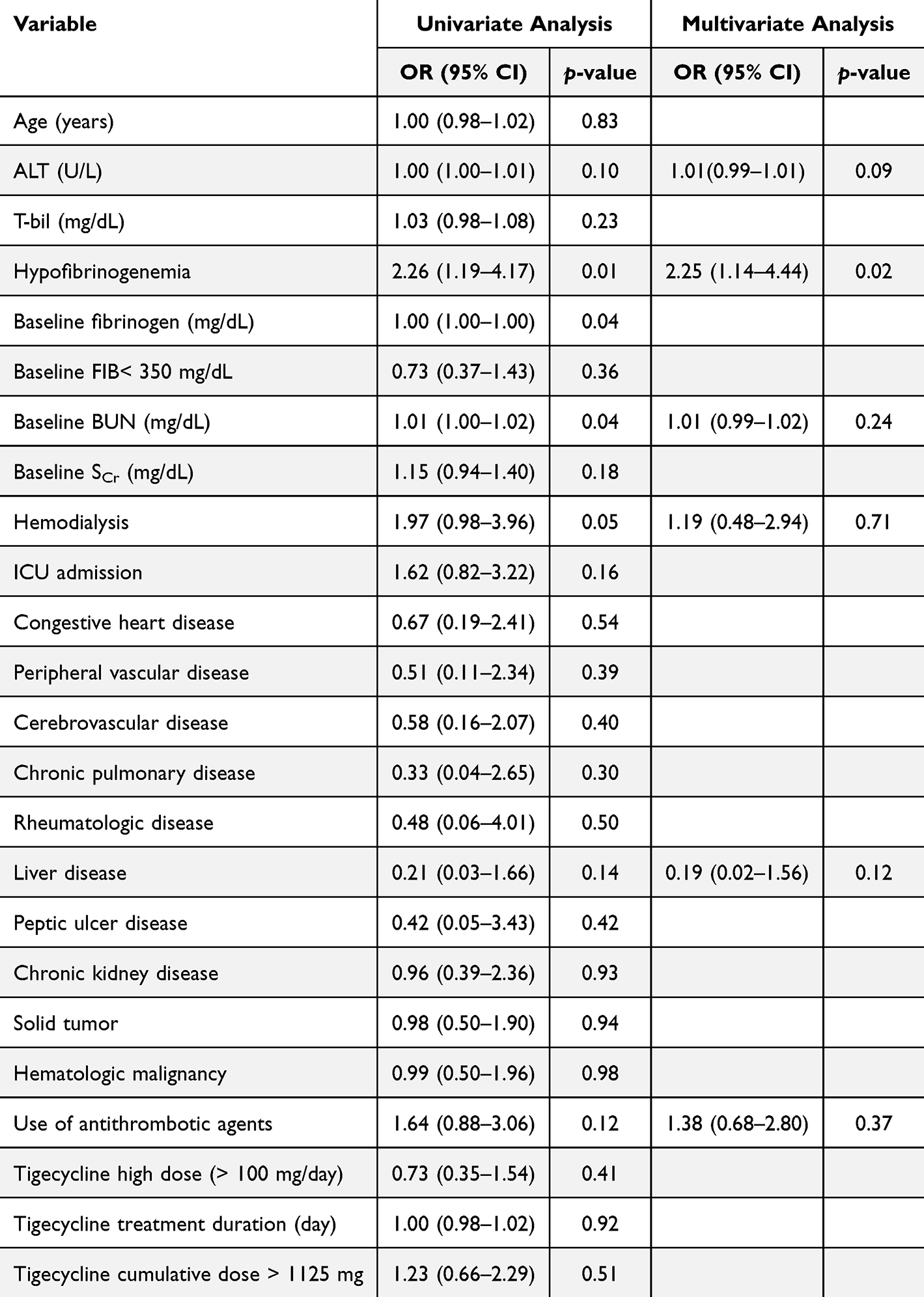 |
Table 4 Risk Factors Related to Major Bleeding in Tigecycline Users |
Hypofibrinogenemia Severity and Transfusion
Among the 98 patients who developed hypofibrinogenemia, 90 had mild (100–200 mg/dL) and 8 had moderate-to-severe (less than 100 mg/dL) fibrinogen decline (Table 5). The incidence of major bleeding was numerically higher in patients with fibrinogen levels less than 100 mg/dL compared with those with levels 100–200 mg/dL (37.5% vs. 30.0%, p = 0.70). Fresh frozen plasma transfusion (75.0% vs. 40.0%, p = 0.07) and cryoprecipitate use (87.5% vs. 57.8%, p = 0.14) also trended in the same direction. However, given the small number of patients with fibrinogen nadir below 100 mg/dL, these subgroup comparisons should be considered exploratory and descriptive only and interpreted with caution.
 |
Table 5 Major Bleeding and Transfusion Patterns Across Hypofibrinogenemia Severity |
Discussion
In this retrospective cohort of hospitalized adults, hypofibrinogenemia occurred in 42% of patients receiving tigecycline and was independently associated with subsequent major bleeding. Baseline fibrinogen less than 350 mg/dL, hemodialysis, peptic ulcer disease, and higher cumulative tigecycline exposure were independent predictors of hypofibrinogenemia. Of note, hypofibrinogenemia was the only independent predictor of major bleeding in adjusted analysis, supporting its role as a clinical meaningful intermediate event rather than an isolated laboratory abnormality.
The incidence of hypofibrinogenemia observed in our study is consistent with prior reports describing rates approaching 40–60% in critically ill populations.8,11
However, the reported clinical consequences of tigecycline-associated hypofibrinogenemia have varied across studies. Some studies have found hypofibrinogenemia to be independently associated with bleeding events,9,11 whereas others have reported substantial fibrinogen decline without a corresponding increase in clinically overt hemorrhage.10,14 Our findings support the clinical relevance of hypofibrinogenemia to major bleeding. Differences across studies may reflect variation in patient populations, baseline severity of illness, fibrinogen monitoring practices, concomitant medications,15,16 and definitions of bleeding outcomes. Our study applied prespecified criteria for major bleeding and also captured treatment-related minor bleeding, which may account for higher event detection compared with studies relying solely on diagnostic codes or spontaneous reporting. Notably, a recent self-controlled analysis demonstrated increased hypofibrinogenemia during tigecycline exposure but did not detect a difference in bleeding risk, underscoring ongoing uncertainty regarding clinical consequences. Our findings provide additional evidence that fibrinogen decline is temporally associated with bleeding events.10
The temporal sequence observed in our cohort strengthens this association. Hypofibrinogenemia typically developed within the first week of therapy and preceded major bleeding by several days. This pattern suggests that declining fibrinogen may serve as an early warning signal rather than a coincidental finding in critically ill patients. Although bleeding events were numerically more frequent in patients with more severe fibrinogen depletion, statistical power was limited in subgroup analyses.
The mechanisms underlying tigecycline-associated hypofibrinogenemia remain incompletely understood. Proposed explanations include impaired hepatic synthesis of coagulation factors, inflammation-mediated consumption, and pharmacodynamic effects related to prolonged systemic exposure.17 Tigecycline has a large volume of distribution and prolonged elimination half-life,2 which may contribute to cumulative exposure, particularly in patients with organ dysfunction. Potential biological mechanisms include suppression of interleukin-6 leading to reduced hepatic fibrinogen synthesis and mitochondrial toxicity associated with high tigecycline exposure, resulting in impaired hepatic synthetic function.9,17,18 Vitamin K deficiency due to disruption of intestinal flora has also been proposed; however, the limited response to vitamin K supplementation makes this explanation less convincing.9,18 The independent association between cumulative dose and hypofibrinogenemia observed in our study supports a potential exposure–response relationship. However, cumulative exposure was not independently associated with major bleeding after adjustment, suggesting that bleeding risk is mediated primarily through development of hypofibrinogenemia rather than direct dose effects.
Hemodialysis was independently associated with hypofibrinogenemia.19 A previous retrospective study also identified renal failure, regardless of dialysis requirement, as a risk factor for tigecycline-induced hypofibrinogenemia. Although tigecycline is not primarily eliminated renally, patients undergoing hemodialysis often have altered albumin binding, chronic inflammation, and multiple comorbid conditions that may predispose them to coagulation abnormalities.20 These findings support careful fibrinogen monitoring in patients with advanced renal impairment, especially those receiving hemodialysis.
From a clinical and antimicrobial stewardship perspective, our findings suggest that measuring baseline fibrinogen before tigecycline initiation and monitoring fibrinogen during therapy may help identify patients at increased risk of bleeding. This may be particularly relevant in patients with lower baseline fibrinogen levels or greater cumulative tigecycline exposure. As tigecycline is increasingly used for multidrug-resistant infections, such risk stratification may be especially useful when prolonged treatment is anticipated.
Several limitations should be considered. First, this was a single-center retrospective study, which may limit the generalizability. Inclusion required available fibrinogen measurements, potentially introducing selection bias because testing was performed based on clinical judgment rather than a standardized protocol. Second, minor bleeding was defined using an operational, treatment-based definition derived from the available database and may not fully capture clinically adjudicated minor bleeding events. Therefore, these findings should be interpreted with caution. Third, the subgroup with fibrinogen nadir below 100 mg/dL was small, limiting the reliability of severity-based subgroup analyses. Residual confounding related to illness severity may persist despite multivariable adjustment. In addition, baseline nutritional status, subclinical vitamin K deficiency, and sepsis-related consumption coagulopathy were not systematically evaluated and may have influenced fibrinogen levels and bleeding risk. The high proportion of patients required intensive care (64%) may also have contributed to the observed bleeding incidence. Furthermore, dynamic fibrinolytic markers and other coagulation factors were not evaluated, and that might limit mechanistic interpretation. Finally, the observational design precludes causal inference.
Despite these limitations, this study provides clinically relevant evidence that hypofibrinogenemia is common during tigecycline therapy and independently associated with major bleeding. Baseline fibrinogen level, hemodialysis, peptic ulcer disease, and cumulative tigecycline exposure help identify patients at increased risk. Routine monitoring of fibrinogen, particularly during the first week of therapy and in high-risk individuals, may support earlier intervention and mitigation of bleeding complications.
Conclusion
In conclusion, hypofibrinogenemia frequently occurred in patients receiving tigecycline and was independently associated with major bleeding. These findings highlight the importance of awareness and fibrinogen monitoring during tigecycline therapy, particularly in higher-risk patients. Nevertheless, given the retrospective single-center design, the findings should be interpreted cautiously and require confirmation in larger prospective studies.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the National Taiwan University Hospital Research Ethics Committee (approval number: 202302047RINC) and was conducted in accordance with the principles of the Declaration of Helsinki. Given the retrospective study design, the requirement for informed consent was waived by the ethics committee.
Acknowledgments
The authors acknowledge the staff of the Department of Medical Research at NTUH for facilitating the use of NTUH-iMD. AI tools, specifically OpenAI’s ChatGPT 5.4, were used to improve the clarity and grammar of human-generated text; all authors reviewed and take responsibility for the final content. All authors have approved the manuscript for submission. No external funding was received for this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a research grant from National Taiwan University Hospital (grant number: 115-S0035). The funder had no role in the study design, data collection, data analysis, data interpretation, manuscript preparation, or the decision to submit the article for publication.
Disclosure
The authors declare that they have no financial or non-financial competing interests related to this work.
References
1. Cui N, Cai H, Li Z, Lu Y, Wang G, Lu A. Tigecycline-induced coagulopathy: a literature review. Int J Clin Pharm. 2019;41(6):1408–11. doi:10.1007/s11096-019-00912-5
2. Wyeth Pharmaceuticals Inc. Tygacil (tigecycline) for injection, powder, lyophilized, for solution. Package Insert. 2005.
3. Wyeth Pharmaceuticals LLC. Tygacil (tigecycline) injection. Prescribing Informat. 2021.
4. Wu PC, Wu CC. Tigecycline-associated hypofibrinogenemia: a case report and review of the literature. IDCases. 2018;11:56–57. doi:10.1016/j.idcr.2018.01.003
5. Campany-Herrero D, Larrosa-Garcia M, Lalueza-Broto P, et al. Tigecycline-associated hypofibrinogenemia in a real-world setting. Int J Clin Pharm. 2020;42(4):1184–1189. doi:10.1007/s11096-020-01072-7
6. Zhang Q, Zhou S, Zhou J. Tigecycline treatment causes a decrease in fibrinogen levels. Antimicrob Agents Chemother. 2015;59(3):1650–1655. doi:10.1128/aac.04305-14
7. Leng B, Xue YC, Zhang W, Gao TT, Yan GQ, Tang H. A retrospective analysis of the effect of tigecycline on coagulation function. Chem Pharm Bull. 2019;67(3):258–264. doi:10.1248/cpb.c18-00844
8. Hu J, Xiao YH, Zheng Y, Lai YX, Fang XL, Fang Q. Clinical characteristics and risk factors of tigecycline-associated hypofibrinogenaemia in critically ill patients. Eur J Clin Pharmacol. 2020;76(7):913–922. doi:10.1007/s00228-020-02860-w
9. Liu J, Yan Y, Zhang F. Risk factors for tigecycline-associated hypofibrinogenemia. Ther Clin Risk Manag. 2021;17:325–332. doi:10.2147/tcrm.S302850
10. Firat O, Kara E, Malkan ÜY, Demirkan K, Inkaya A. Tigecycline-associated hypofibrinogenemia: a single center, retrospective, controlled study. Thromb Res. 2024;236:155–160. doi:10.1016/j.thromres.2024.03.003
11. Leng B, Shen C, Gao T, et al. Incidence, characteristics and risk factors of hypofibrinogenemia associated with tigecycline: a multicenter retrospective study in China. Front Pharmacol. 2022;13:943674. doi:10.3389/fphar.2022.943674
12. Brandtner A, Bachler M, Fries D, et al. Tigecycline interferes with fibrinogen polymerization independent of peripheral interactions with the coagulation system. Antibiotics. 2020;9(2). doi:10.3390/antibiotics9020084
13. Schulman S, Angerås U, Bergqvist D, Eriksson B, Lassen MR, Fisher W. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in surgical patients. J Thromb Haemost. 2010;8(1):202–204. doi:10.1111/j.1538-7836.2009.03678.x
14. Hakeam HA, Al Duhailib Z, Salahuddin N, Amin T. Impact of tigecycline versus imipenem-cilastatin on fibrinogen levels following cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC): a randomized-controlled study. J Chemother. 2018;30(4):224–232. doi:10.1080/1120009x.2018.1452333
15. Zhang L, Cai X, Peng F, et al. Comparison of bleeding risk and hypofibrinogenemia-associated risk factors between tigecycline with cefoperazone/sulbactam therapy and other tigecycline-based combination therapies. Front Pharmacol. 2023;14:1182644. doi:10.3389/fphar.2023.1182644
16. Huang YT, Yu CI, Chen PY, Wang CC, Wu CC. Comparison of bleeding risk between colistin-tigecycline and colistin-carbapenem treatment regimens: a retrospective cohort study. Infect Drug Resist. 2021;14:4949–4955. doi:10.2147/idr.S339188
17. Liu X, Yuan X, Wen L, Tan X, Sui Q, Liu J. Identification of risk factors and predictive indicators for tigecycline-associated hypofibrinogenemia. Clin Transl Sci. 2025;18(4):e70213. doi:10.1111/cts.70213
18. Fan Q, Huang W, Weng Y, Xie X, Shi Z. Hypofibrinogenemia induced by high-dose tigecycline-case report and review of literature. Medicine. 2020;99(43):e22638. doi:10.1097/md.0000000000022638
19. Meijers BK, Bammens B, Verbeke K, Evenepoel P. A review of albumin binding in CKD. Am J Kidney Dis. 2008;51(5):839–850. doi:10.1053/j.ajkd.2007.12.035
20. Zhang Q, Wang J, Liu H, Ma W, Zhou S, Zhou J. Risk factors for tigecycline-induced hypofibrinogenaemia. J Clin Pharm Ther. 2020;45(6):1434–1441. doi:10.1111/jcpt.13250
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.