Back to Journals » Journal of Pain Research » Volume 16
Thermal Grill Illusion in Chronic Lower Back Pain: A Case-Control Study
Authors Kim HC, Chang MC ![]() , Oh SH, Lee SB, Yang SY
, Oh SH, Lee SB, Yang SY ![]() , Shin DA
, Shin DA
Received 24 January 2023
Accepted for publication 8 May 2023
Published 17 May 2023 Volume 2023:16 Pages 1573—1579
DOI https://doi.org/10.2147/JPR.S403387
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Hyung Cheol Kim,1,* Min Cheol Chang,2,* Sung Han Oh,1 Su Bin Lee,3 Soo Young Yang,3 Dong Ah Shin3
1Department of Neurosurgery, Bundang Jesaeng General Hospital, Seongnam-si, Gyeonggi-do, Republic of Korea; 2Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Namku, Taegu, Republic of Korea; 3Department of Neurosurgery, Spine and Spinal Cord Institute, Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea
*These authors contributed equally to this work
Correspondence: Dong Ah Shin, Department of Neurosurgery, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemungu, Seoul, 03722, Republic of Korea, Tel +82 02-2-2228-1004, Email [email protected]
Purpose: This study aimed to use thermal grill illusion (TGI), an experimental model of pain processing and central mechanisms, to evaluate the perception of TGI-related sensations or pain in patients with chronic lower back pain (CLBP).
Patients and Methods: The perception of TGI (warmth/heat, cold, unpleasantness, pain, burning, stinging, and prickling) was examined in 66 patients with CLBP and compared with that in 22 healthy participants. The visual analog scale (VAS) scores for CLBP, Oswestry Disability Index (ODI), and 12-Item Short Form Survey (SF-12) scores were obtained from the included patients with CLBP.
Results: The CLBP group showed a less intense perception of TGI for sensations of warmth/heat, unpleasantness, and pain than the control group. The CLBP group felt burning sensations lesser than the control (2.77 vs 4.55, P=0.016). In the CLBP group, there were significant correlations between the ODI and the degree of unpleasantness (r=0.381, P=0.002) and prickling sensation (r=0.263, P=0.033). There were also significant correlations between the mental component score of the SF-12 and the degree of warmth/heat (r=− 0.246, P=0.046), unpleasantness (r=− 0.292, P=0.017), pain (r=− 0.292, P=0.017), and burning sensations (r=− 0.280, P=0.023).
Conclusion: Our results may be useful for clinicians to evaluate the effectiveness of drugs or interventions to manage centralized LBP.
Keywords: thermal grill illusion, chronic pain, back pain
Introduction
Thermal grill illusion (TGI) is a paradoxical pain sensation induced by the simultaneous application of interlaced warm (38–42 °C) and cool (18–22 °C) stimuli to the skin.1–3 Isolated cold and warm stimulations to the skin are felt as cold and warmth, respectively; however, the exposure to cold and warm stimulation in combination can create a thermo-nociceptive prickling sensation. The device (interlaced grill) used to generate TGI consists of warm and cold aluminum bars arranged in parallel with an alternative pattern. When a hand is placed on an interlaced grill, burning heat and pain can be generated. As the temperatures of the interlaced bar are innocuous, the peripheral nociceptive system is not activated when a hand is placed on an interlaced grill. Accordingly, TGI-associated pain is considered as a pure central phenomenon.1–6 Over the last decade, this phenomenon has evoked considerable interest among researchers. Several studies were conducted in the fields of psychiatric diseases or elucidate sex-based differences to evaluate the application of TGI responses and further unravel this phenomenon.7–10 Recent studies have used TGI to investigate the mechanisms underlying chronic pain, wherein TGI was used to apply nociceptive stimuli, without inflicting harm to human participants.2,11,12
Chronic pain is closely associated with the abnormal central processing of pain, which increases the facilitation of nociceptive signals.13–15 Because TGI-associated pain is an integrative central nervous phenomenon, several studies have been conducted to understand chronic pain using the TGI phenomenon.1,3,15,16 Previous TGI studies have reported that some perceived pain-related sensations were reduced in patients with chronic pain.2,3,15 In contrast, Heavner et al reported an increased perception of pain-related sensations in the presence of chronic pain.17 This altered perception of pain-related sensations has been suggested to be correlated with an altered central integration of ascending pain signals.18–20 For the application of TGI to chronic pain in research and clinical practice, TGI-related responses should be clearly elucidated through further studies. Recently, the number of patients with chronic lower back pain (CLBP) has increased due to changes in lifestyle and increase in spine surgeries. However, CLBP is difficult to diagnose, which affects its effective treatment. To the best of our knowledge, none of the studies have assessed CLBP and TGI so far. In the current study, we investigated the perception of TGI-related sensations and pain in patients with CLBP.
Materials and Methods
Ethics Statements
The study was approved by the Institutional Review Board (IRB) of Severance Hospital (date of approval: November 21, 2021; IRB number:4–2021-1424). Written informed consent was obtained from the patients for the publication of this paper. This study complied with the Declaration of Helsinki’s ethical standards.
Study Design
A total of 66 patients with CLBP and 22 healthy controls (without pain or psychological disorders) were included in this study. The patients and healthy controls were recruited by a spine neurosurgeon (H.C.K.) from among patients with CLBP and their guardians who visited the spine center of a university hospital. CLBP was defined as pain that persisted for more than 3 months despite administration of various conservative treatments, such as oral medication, physical modality, and injection. The inclusion criteria for patients with CLBP were as follows: 1) adult men and women between 19 and 90 years of age; 2) those who provided voluntary consent to participate in this clinical study; and 3) those willing to abide by the experimental protocol. We excluded patients with pain other than CLBP. Patients with psychiatric disorders and central nervous system disorders, such as multiple sclerosis and spondylotic myelopathy, were also excluded.
Device Construction
The thermal grill was designed and manufactured by Anatz (Seoul, Republic of Korea) according to previous validated studies (Figure 1).21–23 The device used for generating the TGI consists of two parts: a control unit and thermal bars. The temperatures of the cold and hot bars were controlled and recorded using a digital thermometer. The temperature of each bar was generated by Peltier elements and finely controlled by the settings of the control unit. The temperature of the cold bar was set to 20±2 °C and that of the hot bar was set to 40±2 °C. A grill consisting of six 12-mm wide and 120-mm long aluminum bars separated by 2-mm spacing was present at the top center of the machine. The hot and cold aluminum bars were arranged in parallel with an alternating pattern.
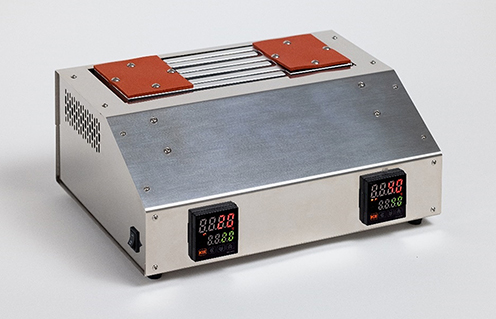 |
Figure 1 Image of the thermal grill device. |
The center of the box is the stimulation surface, where the participants were required to place their palms orthogonally to the long axis of the bars (Figure 2). The stimulation surface consists of six 12-mm wide and 120-mm long aluminum bars separated by approximately 2 mm. The control unit set the temperature of the individual bars to alternating cold and hot temperatures.
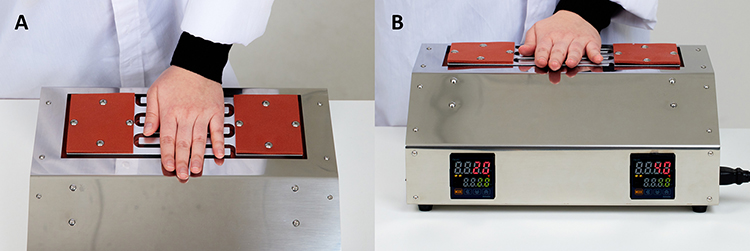 |
Figure 2 Experimental setup of the thermal grill device (views from above (A) and front on the device (B)). |
Experiment
None of the participants knew the temperature settings of the bars or about the TGI phenomenon. Before obtaining informed consent, participants were informed that this experiment was aimed to investigate somatosensory functions, and that their hand would not be harmed even though they might feel painful sensation. Patients were instructed to remember their hand perceptions during the study, and asked to rate the sensations (warmth/heat, cold, unpleasant, painful, burning, stinging, and prickling) generated from the thermal grill using a visual analog scale (VAS; ranging from 0 to 10; 0 = no sensation, 10 = worst imaginable sensation), immediately after the procedure. The participants were required to place their non-dominant palm on the thermal grill bars, orthogonally to the long axis of the bars for approximately 30 seconds. Following the experiment, the ratings were recorded from the VAS pain scores.
Parameters
Before the TGI test, each participant quantified their current lower back pain (LBP) and functional disability using the VAS and Oswestry Disability Index (ODI) (range, 0–100; 0=no disability, 100=maximum disability). In addition, all the participants completed the 12-Item Short Form Health Survey (SF-12) to evaluate their quality of life.
Statistical Analysis
To test for differences between the data of patients with CLBP and those of healthy controls, the independent t-test with Cohen’s d and chi-square tests were used. Additionally, a Pearson linear correlation analysis was performed to analyze the correlation between the data related to the degree of current LBP (VAS, ODI, and PCS and MCS of SF-12) and perceived TGI-related sensations. All the statistical analyses were performed using SPSS, version 25 for Windows (IBM Corp., Armonk, NY, USA). The statistical significance was set at P<0.05.
Results
Demographic Data
Overall, 66 patients with CLBP and 22 healthy controls participated in the study. The demographic and clinical characteristics of the participants are presented in Table 1. The duration of LBP in CLBP was 4.7±3.1 years. The average VAS score for LBP was 5.45±2.61, and the average ODI score was 28.86±21.84. The CLBP group consisted of 36 patients with discogenic back pain (diagnosed using discography) and 30 patients with non-specific LBP. The sex distribution was not significantly different between the CLBP and control groups. However, the CLBP group was significantly older than the control group (P<0.001). In addition, the PCS and MCS scores of the SF-12 were significantly higher in the control group than in the CLBP group (P<0.001).
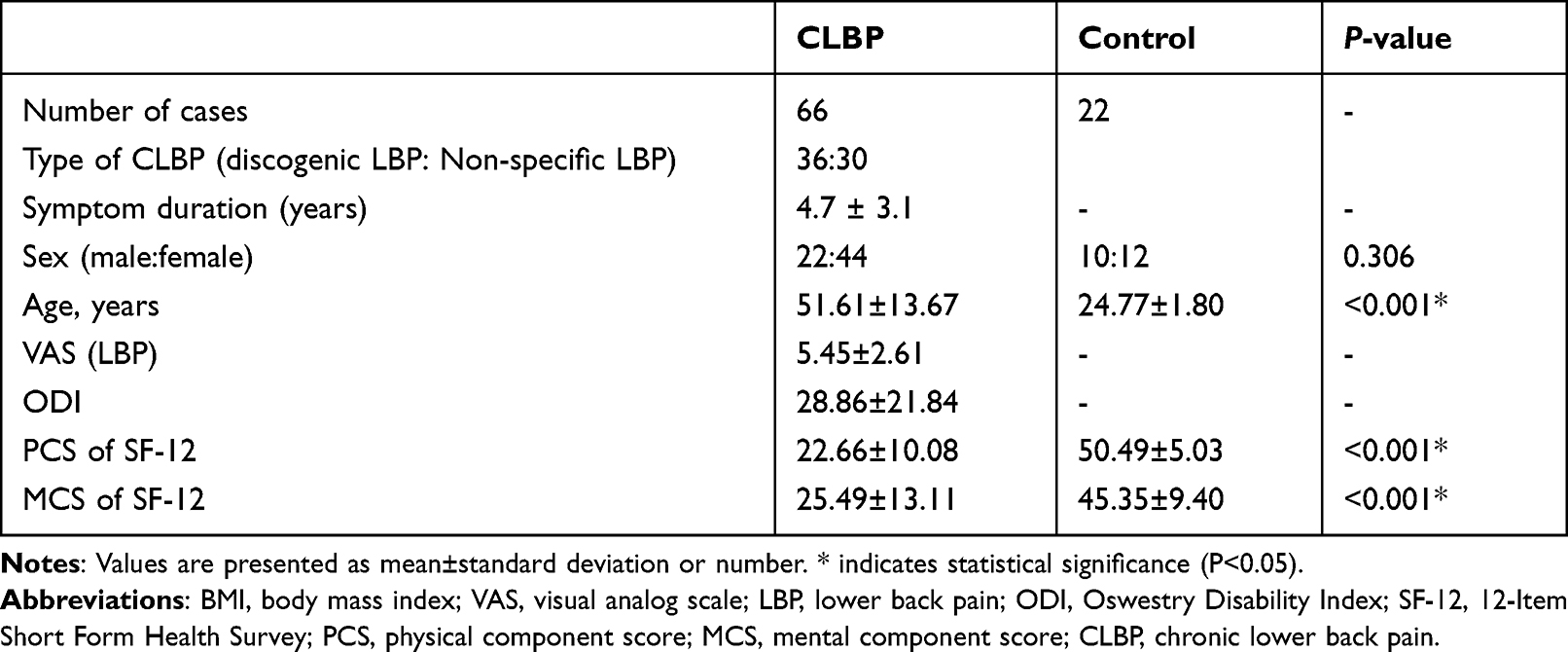 |
Table 1 Demographic and Clinical Data of Participants |
Response to the Thermal Grill Illusion
In the CLBP group, the patients reported significantly lesser warm/hot sensations (5.80± 2.37 vs 7.36±2.21, P=0.008), unpleasantness (2.76±2.82 vs 4.96±2.50, d=−0.801, P=0.002), pain (1.91±2.76 vs 4.00±2.35, d=−0.784, P=0.002), and burning sensation (2.77±3.04 vs 4.55±2.58, d=−0.607, P=0.016). In contrast, there were no significant differences with respect to cold (P=0.194), stinging (P=0.591), or prickling sensations (P=0.178) between the groups (Table 2). In the CLBP group, the ODI scores were observed to significantly correlate with the degree of unpleasantness (r=0.381, P=0.002) and prickling sensations (r=0.263, P=0.033) (Table 3). Additionally, there were significant correlations between the MCS of the SF-12 and the degree of warmth/heat (r=−0.246, P=0.046), unpleasantness (r=−0.292, P=0.017), pain (r=−0.292, P=0.017), and burning sensations (r=−0.280, P=0.023). However, the VAS and PCS scores of the SF-12 showed no significant correlation with the degree of sensations from the TGI in the CLBP group.
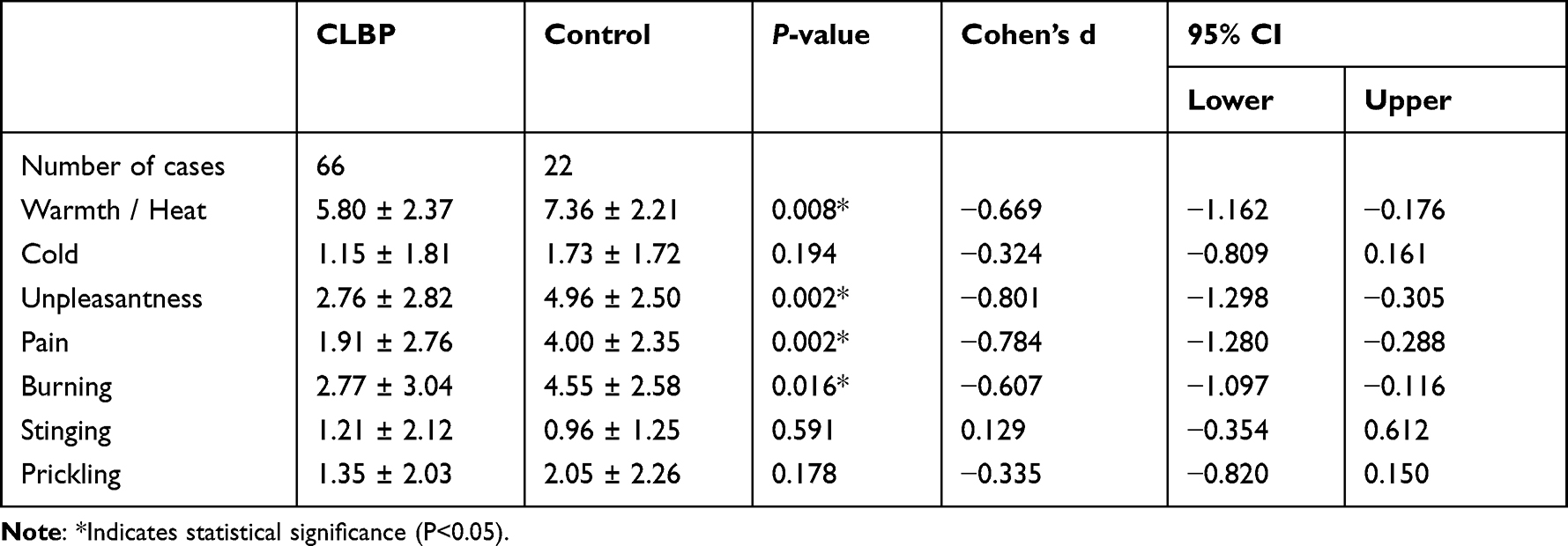 |
Table 2 Descriptive Statistics for the Visual Analog Scale Score of Each Sensation Elicited by the Thermal Grill Illusion in the Chronic Lumbar Back Pain (CLBP) and Control Groups |
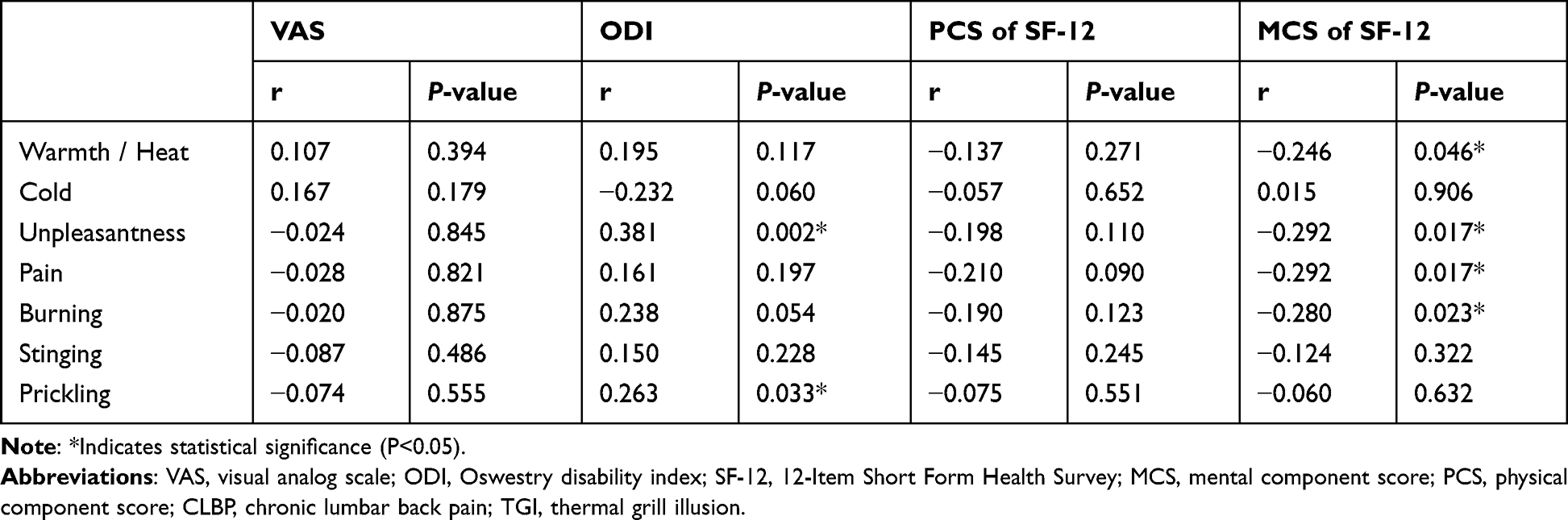 |
Table 3 Correlation Between the Clinical Scale (VAS, ODI, SF-12) Scores and Degree of Sensations from the TGI According to the Pearson Correlation Coefficient in the CLBP Group |
Discussion
In this study, we found that patients with CLBP perceived significantly lesser sensations of warmth/heat, unpleasantness, pain, and burning during the test using TGI than the healthy controls. Additionally, there was a significant correlation between the ODI scores in patients with CLBP and the degree of unpleasantness and prickling sensations. A significant correlation was also found between the MCS of the SF-12 in patients with CLBP and the degree of warmth/heat, unpleasantness, pain, and burning sensations.
The fact that some types of perceptions during the TGI test were lower in patients with CLBP is in agreement with previous studies.24 Sumracki et al reported that 18 patients with chronic pain from various disorders, such as osteoarthritis, nerve injury, fibromyalgia, and complex regional pain syndrome, had a lower TGI response (pain, heat, and unpleasantness) than 16 pain-free participants.2,3 Defrin et al found that 47 patients with central neuropathic pain due to multiple sclerosis had higher cold and warm sensation thresholds than 32 healthy controls during the TGI test.15 The lower sensory perception related to TGI in patients with chronic pain may be attributed to the altered central integration of ascending pain signals, which is associated with long-term functional or microstructural changes in the central nervous system (CNS).7,25,26 Furthermore, in the current study, by confirming the significant correlation between the ODI and MCS of SF-12 in patients with CLBP and some types of TGI-related sensations, the close association between CLBP and changes in the CNS became more established.
Unlike in this study, there are reports of increased TGI responses in patients with chronic pain. Heavner et al reported that a patient with type 1 complex regional pain syndrome (CRPS) experienced severe burning pain when putting their hand on a thermal grill.17 Boettger et al reported that the temperature differentials for the perception of TGI were higher in patients with major depressive disorder than in controls.10 The results of Heavner et al and Boettger et al’s studies were opposite to those of our study; therefore, further research on the reasons and mechanisms is needed.
In our opinion, the results in the current study can be used to determine the presence or extent of LBP centralization. In addition, we believe that the results of this study can be used to evaluate the effectiveness of drugs or interventions to manage CLBP. In addition, our results may be helpful in differentiating between malingering and the presence of real chronic pain.
There have been no previous studies on the TGI response characteristics in patients with CLBP. Accordingly, this study is the first to show TGI response in patients with CLBP by comparing it to healthy controls with no pain. However, our study had a few limitations. First, there was a significant age difference between the two groups. However, it has been reported that the response to thermal stimuli varies with age despite there being no difference in the response to TGI by age.3 To date, no studies have reported whether age is a significant factor for TGI. Second, the medications used for pain control were not considered in the analysis of the results. Finally, we did not evaluate the psychological state of the included patients, such as depression or anxiety. Previous studies have reported that psychological disorders can affect the threshold of TGI-related sensations.8,10,21 Further studies are required to compensate for these limitations.
Conclusion
Patients with CLBP reported significantly less intense responses to TGI for sensations of warmth/heat, unpleasantness, pain, and burning sensations. In the CLBP group in this study, various TGI-induced sensations or pain were associated with the ODI and MCS of the SF-12 scores. We believe that our results will help clarify TGI-related responses in the presence of chronic pain. Furthermore, the findings in this study may be helpful for clinicians to determine the therapeutic effect of drugs or interventions to control centralized LBP and for researchers to develop new drugs and widen the knowledge of chronic centralized pain.
Acknowledgments
Hyung Cheol Kim and Min Cheol Chang contributed equally to this work as co-first authors.
Funding
This study was supported by the 2022 Joint Research Project of the Institutes of Science and Technology.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Osumi M, Sumitani M, Nobusako S, et al. Pain quality of thermal grill illusion is similar to that of central neuropathic pain rather than peripheral neuropathic pain. Scand J Pain. 2022;22:40–47. doi:10.1515/sjpain-2021-0020
2. Shin DA, Chang MC. A review on various topics on the thermal grill illusion. J Clin Med. 2021;11:10. doi:10.3390/jcm11010010
3. Sumracki NM, Buisman-Pijlman FT, Hutchinson MR, et al. Reduced response to the thermal grill illusion in chronic pain patients. Pain Med. 2014;15:647–660. doi:10.1111/pme.12379
4. Bach P, Becker S, Kleinböhl D, et al. The thermal grill illusion and what is painful about it. Neurosci Lett. 2011;505:31–35. doi:10.1016/j.neulet.2011.09.061
5. Leung AY, Wallace MS, Schulteis G, et al. Qualitative and quantitative characterization of the thermal grill. Pain. 2005;116:26–32. doi:10.1016/j.pain.2005.03.026
6. Green BG, Pope JV. Innocuous cooling can produce nociceptive sensations that are inhibited during dynamic mechanical contact. Exp Brain Res. 2003;148:290–299. doi:10.1007/s00221-002-1280-9
7. Averbeck B, Seitz L, Kolb FP, et al. Sex differences in thermal detection and thermal pain threshold and the thermal grill illusion: a psychophysical study in young volunteers. Biol Sex Differ. 2017;8:29. doi:10.1186/s13293-017-0147-5
8. Bekrater-Bodmann R, Chung BY, Richter I, et al. Deficits in pain perception in borderline personality disorder: results from the thermal grill illusion. Pain. 2015;156:2084–2092. doi:10.1097/j.pain.0000000000000275
9. Boettger MK, Grossmann D, Bär KJ. Increased cold and heat pain thresholds influence the thermal grill illusion in schizophrenia. Eur J Pain. 2013;17:200–209. doi:10.1002/j.1532-2149.2012.00188.x
10. Boettger MK, Grossmann D, Bär KJ. Thresholds and perception of cold pain, heat pain, and the thermal grill illusion in patients with major depressive disorder. Psychosom Med. 2013;75:281–287. doi:10.1097/PSY.0b013e3182881a9c
11. Kern D, Plantevin F, Bouhassira D. Effects of morphine on the experimental illusion of pain produced by a thermal grill. Pain. 2008;139:653–659. doi:10.1016/j.pain.2008.07.001
12. Kong Y, Posada-Quintero HF, Chon KH. Pain detection using a smartphone in real time. Annu Int Conf IEEE Eng Med Biol Soc. 2020;2020:4526–4529. doi:10.1109/EMBC44109.2020.9176077
13. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397:2082–2097. doi:10.1016/S0140-6736(21)00393-7
14. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the iasp classification of chronic pain for the international classification of diseases (icd-11). Pain. 2019;160:19–27. doi:10.1097/j.pain.0000000000001384
15. Rivel M, Achiron A, Dolev M, et al. Central neuropathic pain in multiple sclerosis is associated with impaired innocuous thermal pathways and neuronal hyperexcitability. Pain Med. 2021;22:2311–2323. doi:10.1093/pm/pnab103
16. Leung A, Shukla S, Li E, et al. Supraspinal characterization of the thermal grill illusion with fmri. Mol Pain. 2014;10:18. doi:10.1186/1744-8069-10-18
17. Heavner JE, Calvillo O, Racz GB. Thermal grill illusion and complex regional pain syndrome type i (reflex sympathetic dystrophy). Reg Anesth. 1997;22:257–259. doi:10.1016/S1098-7339(06)80011-8
18. Fitzcharles MA, Cohen SP, Clauw DJ, et al. Nociplastic pain: towards an understanding of prevalent pain conditions. The Lancet. 2021;397:2098–2110. doi:10.1016/S0140-6736(21)00392-5
19. Kosek E, Cohen M, Baron R, et al. Do we need a third mechanistic descriptor for chronic pain states? Pain. 2016;157:1382–1386. doi:10.1097/j.pain.0000000000000507
20. Meacham K, Shepherd A, Mohapatra DP, et al. Neuropathic pain: central vs. peripheral mechanisms. Curr Pain Headache Rep. 2017;21:28. doi:10.1007/s11916-017-0629-5
21. Boettger MK,Schwier C, Bär KJ. Sad mood increases pain sensitivity upon thermal grill illusion stimulation: implications for central pain processing. Pain. 2011;152:123–130. doi:10.1016/j.pain.2010.10.003
22. Bouhassira D, Attal N, Alchaar H, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. 2005;114:29–36. doi:10.1016/j.pain.2004.12.010
23. Craig AD, Bushnell MC. The thermal grill illusion: unmasking the burn of cold pain. Science. 1994;265:252–255. doi:10.1126/science.8023144
24. Harper DE, Hollins M. Conditioned pain modulation dampens the thermal grill illusion. Eur J Pain. 2017;21:1591–1601. doi:10.1002/ejp.1060
25. Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by central neural plasticity. J Pain. 2009;10:895–926. doi:10.1016/j.jpain.2009.06.012
26. Pelletier R, Higgins J, Bourbonnais D. Is neuroplasticity in the central nervous system the missing link to our understanding of chronic musculoskeletal disorders? BMC Musculoskelet Disord. 2015;16:25. doi:10.1186/s12891-015-0480-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pain Experience and Sensory Changes in Astronauts During and After Short-Lasting Commercial Spaceflight: A Proof-of-Concept Study
Sauer AK, Vigouroux M, Dougherty PM, Cata JP, Ingelmo PM
Journal of Pain Research 2023, 16:4253-4266
Published Date: 11 December 2023