Back to Journals » Journal of Pain Research » Volume 19
Therapeutic Exercise for Forward Head Posture in Neck Pain Patients: A Systematic Review and Meta-Analysis
Authors Xing Y ![]() , Wang R, Zhao X, Xu A
, Wang R, Zhao X, Xu A
Received 7 April 2026
Accepted for publication 26 June 2026
Published 9 July 2026 Volume 2026:19 614524
DOI https://doi.org/10.2147/JPR.S614524
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Alaa Abd-Elsayed
Yachen Xing,1 Ronghui Wang,1 Xingrui Zhao,2 Anjie Xu1
1School of Sport Science, Beijing Sport University, Beijing, People’s Republic of China; 2School of Sport Science, José Rizal University, Mandaluyong, National Capital Region, Philippines
Correspondence: Yachen Xing, Email [email protected]
Background: Forward Head Posture (FHP) is a prevalent musculoskeletal disorder strongly associated with neck pain and functional disability. Although therapeutic exercise is commonly recommended in clinical practice, there remains a lack of consensus regarding the most effective exercise modalities and optimal intervention duration. This systematic review evaluated the efficacy of therapeutic exercise on posture, pain, and functional outcomes in individuals with FHP, and to identify key factors that may influence treatment effectiveness.
Methods: Literature searches were conducted following the PRISMA guidelines to identify randomized controlled trials (RCTs) on therapeutic exercises for FHP. Dates were extracted and pooled using a random-effects model. Prespecified subgroup analyses were performed to examine the influence of exercise modality (single vs combined) and intervention duration (< 8 weeks vs ≥ 8 weeks).
Results: Ten RCTs, involving 550 participants were included in the analysis. Compared with control groups, therapeutic exercise significantly improved the craniovertebral angle (MD = 3.38°, 95% CI: 2.10° to 4.65°, p < 0.001; SMD = 0.95, 95% CI: 0.61 to 1.28), reduced pain intensity (MD = − 1.42, 95% CI: − 2.11 to − 0.73, p < 0.001; SMD = − 1.72, 95% CI: − 2.69 to − 0.71), and enhanced neck functional capacity (MD = − 5.44, 95% CI: − 8.56 to − 2.32, p < 0.001; SMD = − 1.08, 95% CI: − 1.66 to − 0.50). Exploratory subgroup analyses suggested potential trends: interventions employing combined exercise modalities and those lasting ≥ 8 weeks appeared to be associated with greater clinical benefits, although these findings should be interpreted with caution due to limited statistical power and high between-study heterogeneity.
Conclusion: Therapeutic exercise may be associated with improved craniovertebral angle, reduced pain intensity, and better neck function in individuals with FHP and neck pain. Exploratory analyses suggested that combined exercise approaches and interventions lasting at least 8 weeks may yield larger improvements, although the overall certainty of evidence remains low to moderate.
Keywords: forward head posture, therapeutic exercise, neck pain, meta-analysis, cervical stabilization, postural correction
Introduction
Neck pain caused by excessive use of electronic devices has become a worldwide public health issue in the digital age. One of the factors that contributes to it is Forward Head Posture (FHP) which is a common postural presentation closely associated with neck pain and related symptoms. FHP is among the most prevalent postural disorders in contemporary society, with an anterior shift of the head towards the vertical line of the shoulders, reduced craniovertebral angle (CVA), elongated scapulae, and enhanced thoracic kyphosis.1,2 According to epidemiological research, FHP occurs in more than 70% of office workers, students, and high screen time people. Prolonged exposure to FHP adds mechanical stress to the cervical spine, posterior neck musculature, and zygapophyseal joints, hence resulting in muscle fatigue, trigger points, neural irritation, and chronic neck pain.3
From a biopsychosocial perspective, the relationship between FHP and neck pain is not merely biomechanical but involves complex interactions among peripheral tissue damage, central nervous system sensitization, and psychosocial factors.4,5 Pioneering work by Farina et al has demonstrated that cervical motor control impairment and deep neck flexor dysfunction play critical roles in the transition from acute to chronic neck pain, independent of structural abnormalities.6 Falla et al further identified that altered muscle activation patterns―notably the overactivity of superficial neck muscles and inhibition of deep stabilizers―contribute to both postural distortion and pain persistence.7 Importantly, the posture-pain relationship is nonlinear: while FHP increases mechanical loading, central sensitization can amplify pain perception disproportionately, creating a self-sustaining pain-spasm-posture cycle that requires multimodal intervention.8
Neck pain is one of the most common musculoskeletal conditions with an average prevalence rate of 23% globally, and it is the fourth leading cause of disability globally.9,10 It causes massive pain, disability and economic loss.11 The weight is not only on the individual but also affects families, healthcare systems, and national economic systems significantly.12,13 A number of cross-sectional studies have established that there is a strong correlation between the severity of forward head posture and the degree of neck pain, neck disability, and frequency of headaches.3,14–16 Cross-sectional evidence indicates consistent associations between greater severity of FHP and higher levels of neck pain, neck disability, and headache frequency. Correcting abnormal posture may help reduce symptom burden and improve function.
Exercise therapy is identified as a non-invasive first-line intervention in treating neck pain and postural dysfunction. Its main goals are to restore balance of muscles, increase stability, regain range of motion and neuromuscular control. Examples of exercise modalities are cervical flexor strengthening, scapular stabilization training, pectoralis/upper trapezius stretching, and cervical proprioception training.17–20 Although it has been widely used in clinical practice, discrepancies exist concerning the overall magnitude of exercise effect on FHP, optimal intensity, duration, intervention periods and combinations.21–26 Though there have been some narrative reviews summarizing exercise techniques to treat FHP,27,28 most meta-analyses available are limited to changes in pain and FHP, optimal exercise dosage remains unclear, and conflicting efficacy across exercise modalities awaits resolution.29–31 Thus, this systematic review and meta-analysis were conducted to systematically assess the impact of therapeutic exercise on the craniovertebral angle, pain, and disability of patients with neck pain and FHP. Moreover, exploratory subgroup analyses were performed to identify the best types of exercises and durations of interventions and offer evidence-based guidelines to clinical practice. The research was carried out strictly based on PRISMA 2020,32 The study protocol was registered in PROSPERO (Registration No.: CRD420241331709).
Methods
Study Design
The research was a systematic review and meta-analysis, which followed the PRISMA (Preferred Reporting Items to Systematic Reviews and Meta-Analyses) guidelines strictly. A protocol was set up beforehand, with clear definition of search strategy, eligibility criteria, data extraction procedures, and methods for assessing risk of bias. The literature search included publications till December 2025. Search strategies were customized according to the language and syntax rules of each database.
Grading of Recommendations Assessment, Development and Evaluation (GRADE) Approach
The certainty of evidence for each primary outcome was assessed using the GRADE framework.33 Evidence quality was rated as high, moderate, low, or very low based on five domains: (1) risk of bias (study limitations), (2) inconsistency (heterogeneity), (3) indirectness, (4) imprecision, and (5) publication bias. Randomized trials initially start as high-quality evidence but may be downgraded based on identified limitations. A Summary of Findings (SoF) table was constructed to present the absolute and relative effects, the number of participants and studies, and the overall certainty of evidence for each primary outcome.
Inclusion and Exclusion Criteria
According to the Population, Intervention, Comparison, Outcome and Study design (PICOS) framework, the inclusion and exclusion criteria were as follows:
Population
The population of the study was made up of adults (aged 18 years and above) who had been diagnosed with a confirmed case of neck pain, which included subtypes like non-specific neck pain and chronic neck pain. The research that was not included in the studies was one where patients suffering cervical fractures, dislocations, tumors, infections, inflammatory arthritis or had undergone previous cervical surgery.
Intervention
Eligible interventions included therapeutic exercise programs comprising muscle strengthening, stretching, stabilization, proprioceptive training, postural correction, and telerehabilitation.
Definition of Exercise Modalities for Subgroup Analysis:
Single-mode exercise: Intervention involving only one type of exercise approach (eg, cervical stabilization exercises alone, stretching alone, or proprioception training alone).
Combined exercise: Intervention integrating two or more distinct exercise modalities from the following categories:
- Cervical deep flexor stabilization training (craniometrical flexion test-based exercises).
- Scapular stabilization and muscle balance training.
- Postural correction and ergonomic education.
- Stretching of tight muscles (pectoralis major/minor, upper trapezius, suboccipital muscles).
- Cervical proprioception and neuromuscular control training.
- Thoracic spine mobility exercises.
Studies were excluded if the exercise intervention was combined with manual therapy, acupuncture, or electrotherapy. Furthermore, studies that did not include a dedicated exercise-only group were also excluded to ensure the isolation of the exercise effect.
Comparison
Eligible comparators included placebo, no exercise, or non-exercise interventions such as physical modalities (eg, heat therapy, electrotherapy) and pharmacological treatments. Additionally, studies were included if the control group received a different type of exercise regimen, minimal intervention, or was placed on a waitlist.
Outcomes
To be eligible for inclusion, studies were required to report at least one of the following core outcome measures:
- CVA: An objective biomechanical metric used to quantify FPH by assessing the anterior displacement of the head relative to the shoulder girdle.24,34
- Pain Intensity: Assessed using the Visual Analog Scale (VAS).
- Neck Disability: Measured by the Neck Disability Index (NDI).
Studies reporting only non-core outcomes were excluded.
Study Design
Only randomized controlled trials (RCTs) were eligible for inclusion. We excluded non-randomized controlled trials, observational studies, case series, case reports, and review articles. Furthermore, eligibility was restricted to studies published in the English language.
Search Strategy
A comprehensive literature search was conducted across six international core databases covering biomedicine, clinical research, and multidisciplinary fields: PubMed, Web of Science, Medline, Embase, Scopus and Cochrane Central Register of Controlled Trials. The search strategy was built around three core concepts: (1) For-ward Head Posture, (2) Neck Pain, and (3) Therapeutic Exercise. Synonyms and related terms were identified using the PubMed Medical Subject Headings (Mesh) database and preliminary scoping searches. The search strategy is presented in Supplementary Table S1.
Data Extraction
Data extraction was performed independently by the same two reviewers (YX and XZ) using a standardized data extraction form created in Microsoft Word. For each included study, the following information was extracted:
Study Characteristics: First author, year of publication, mean age of participants, and sample size. Intervention Details: Specific type of exercise, frequency, duration per session, and total intervention period.
Outcome Data: Baseline and post-intervention values for the primary outcomes: CVA, VAS for pain, and NDI. All included studies measured forward head posture using the CVA. No alternative FHP metrics were pooled. CVA is the standard and most widely accepted objective measure for quantifying FHP, and all studies used consistent measurement protocols. Therefore, results were directly comparable and pooled without additional transformation.
For studies featuring a multi-arm design (ie, comprising two experimental groups and one shared control group), we extracted baseline and post-intervention data—including sample size, mean, and standard deviation—for each experimental group as well as for the shared control group individually. Data splitting and sample size adjustment for such studies were subsequently implemented during the statistical analysis phase.
Regarding statistical data, the mean difference (MD) and corresponding standard deviation (SD) were extracted for continuous outcomes. If a study reported the standard error (SE) instead of the SD, the SD was calculated and converted using the formula (where n is the sample size) to ensure consistency in the analysis. Like the selection process, any disagreements during data extraction were resolved through discussion or consultation with the third reviewer (RW).
Risk of Bias Assessment
The methodological quality and risk of bias of all included randomized controlled trials (RCTs) were assessed using a dual-framework approach. The primary assessment was conducted using the Cochrane Risk of Bias tool (RoB 2.0),35 supplemented by the Physiotherapy Evidence Database (PEDro) scale to evaluate the overall design quality of rehabilitation interventions.36 Detailed bias assessment can be found in Supplementary Table S2.
The risk of bias and quality assessments were performed independently by two reviewers (YX and XZ). Any discrepancies in judgments between the two reviewers were resolved through discussion and consensus. If an agreement could not be reached, a third senior reviewer (RW) was consulted to make the final decision. The final assessment results are presented in a Risk of Bias Summary Table and a Risk of Bias Graph to ensure transparency in reporting.
Statistical Analysis
Stata version 18.0 (Stata Corp LLC, College Station, TX, USA) was used to conduct all statistical analysis and meta-analysis. The significance level of the statistical tests was two-tailed at a=0.05. The MD with the respective 95% CI was applied as the measure of effect size because all outcome measures in this study were continuous variables. MD direction interpretation: CVA: A positive value of MD means that the intervention group had a greater CVA than the control group, which is an improvement in forward head posture (ie, less severe FHP). VAS and NDI: Lower scores are better when it comes to these outcomes. Hence, a negative MD will be considered as a good treatment effect. In its turn, should the analysis be organized so that positive value denotes improvement, the interpretation will be modified. Standard convention: Normally, VAS and NDI, when comparing raw post-intervention scores, an MD < 0 favors the intervention. The statistics and Chi-square test were used to determine statistical heterogeneity among the included studies. Low Heterogeneity: When, ie, low to moderate heterogeneity, a fixed-effects model was used to pool the data. High Heterogeneity: When >50%, meaning that there is high heterogeneity, a random-effects model based on Der Simonian-Laird approach was adopted. Where there was significant heterogeneity (>50%), subgroup analyses and sensitivity analyses were done to investigate possible sources of variation. Funnel plots were used to visually evaluate publication bias. Egger linear regression test was also conducted to quantitatively determine the asymmetry of the funnel plot. The result of the test by Egger was taken as significant in case of a P -value below 0.05.
To examine the strength and consistency of the pooled findings, a sensitivity analysis was carried out by omitting each of the studies including one after another (leave-one-out analysis) and re-estimating the combined effect estimates. Any substantial alteration in the direction or extent of the pooled MD once a particular study has been omitted would indicate that the overall finding is strongly dependent on that specific study. For multi-arm studies that include two experimental groups and one shared control group, we decomposed each study into two independents pairwise comparisons (Experimental Group 1 vs Control, Experimental Group 2 vs Control) to align with the meta-analytic framework. To prevent unit-of-analysis error arising from the repeated use of the shared control group, we followed the guidance of the Cochrane Handbook for Systematic Reviews of Interventions and evenly divided the control group’s sample size by the number of experimental groups in the study. This adjustment avoids over-weighting multi-arm studies in the pooled effect-size estimation while maintaining the original total sample size and statistical power. In contrast, for head-to-head studies comprising only two experimental groups without an independent control group, no sample-size splitting was performed, as the pairwise comparisons do not involve reuse of a control group.
In addition to the leave-one-out sensitivity analysis, we conducted a pre-specified sensitivity analysis by excluding studies with low methodological quality, defined as those with a Physiotherapy Evidence Database (PEDro) score <6—a widely accepted threshold for low-quality randomized controlled trials in physical therapy research. The pooled effect size, heterogeneity, and statistical significance following this exclusion were compared with the primary analysis to assess the robustness of our core findings. All analyses were performed after applying sample size correction for multi-arm studies to avoid unit-of-analysis error.
Meta-Regression Analysis
To investigate the sources of heterogeneity across studies, meta-regression analyses were performed using the restricted maximum likelihood (REML) method with Knapp-Hartung adjustments. Two pre-defined covariates were incorporated into the model: (1) intervention duration, categorized as <8 weeks versus ≥8 weeks; and (2) exercise modality, classified as single-mode exercise versus combined exercise. The proportion of between-study heterogeneity explained by these covariates was quantified using the adjusted R-squared, with statistical significance set at p < 0.05.
Results
Study Selection
The study selection process was conducted independently by two reviewers (YX and XZ) based on the predefined inclusion and exclusion criteria. YX and XZ at either stage was resolved through discussion and consensus. If an agreement could not be reached, a third senior reviewer (RW) was consulted to arbitrate and make the final decision. The initial database search yielded a total of 6718 records. After importing the records into EndNote X9, 1495 duplicates were identified and removed through a combination of automated software deduplication and manual verification. The remaining 5223 unique records underwent title and abstract screening. Based on the predefined inclusion and exclusion criteria, 5088 records were excluded at this stage as they were clearly irrelevant (eg, wrong study design, inappropriate population, or non-eligible interventions). Subsequently, the full texts of the remaining 135 potentially eligible studies were retrieved for detailed assessment. Following a rigorous review of the full texts,125 studies were excluded. Finally, 10 studies met all eligibility criteria and were included in the systematic review and meta-analysis. The complete study selection process, including the number of records identified, screened, assessed for eligibility, and included, along with the specific reasons for exclusions at each stage, is illustrated in the PRISMA 2020 flow diagram (Figure 1).
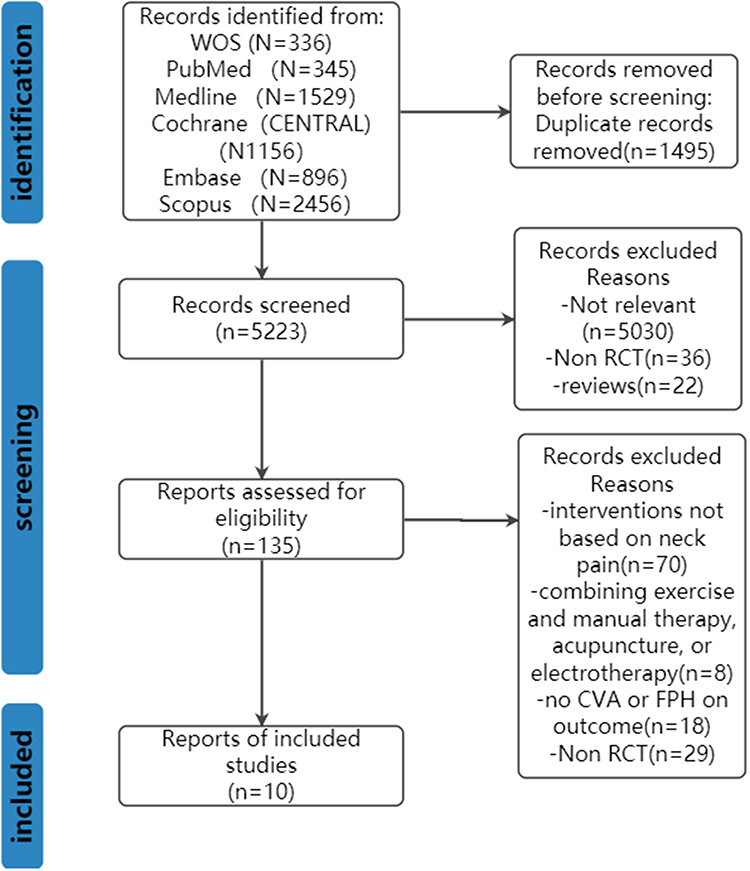 |
Figure 1 Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram. |
Characteristics of Included Studies
A total of 10 studies met the inclusion criteria and were included in this systematic review and meta-analysis. The detailed characteristics of these studies are summarized in Table 1.
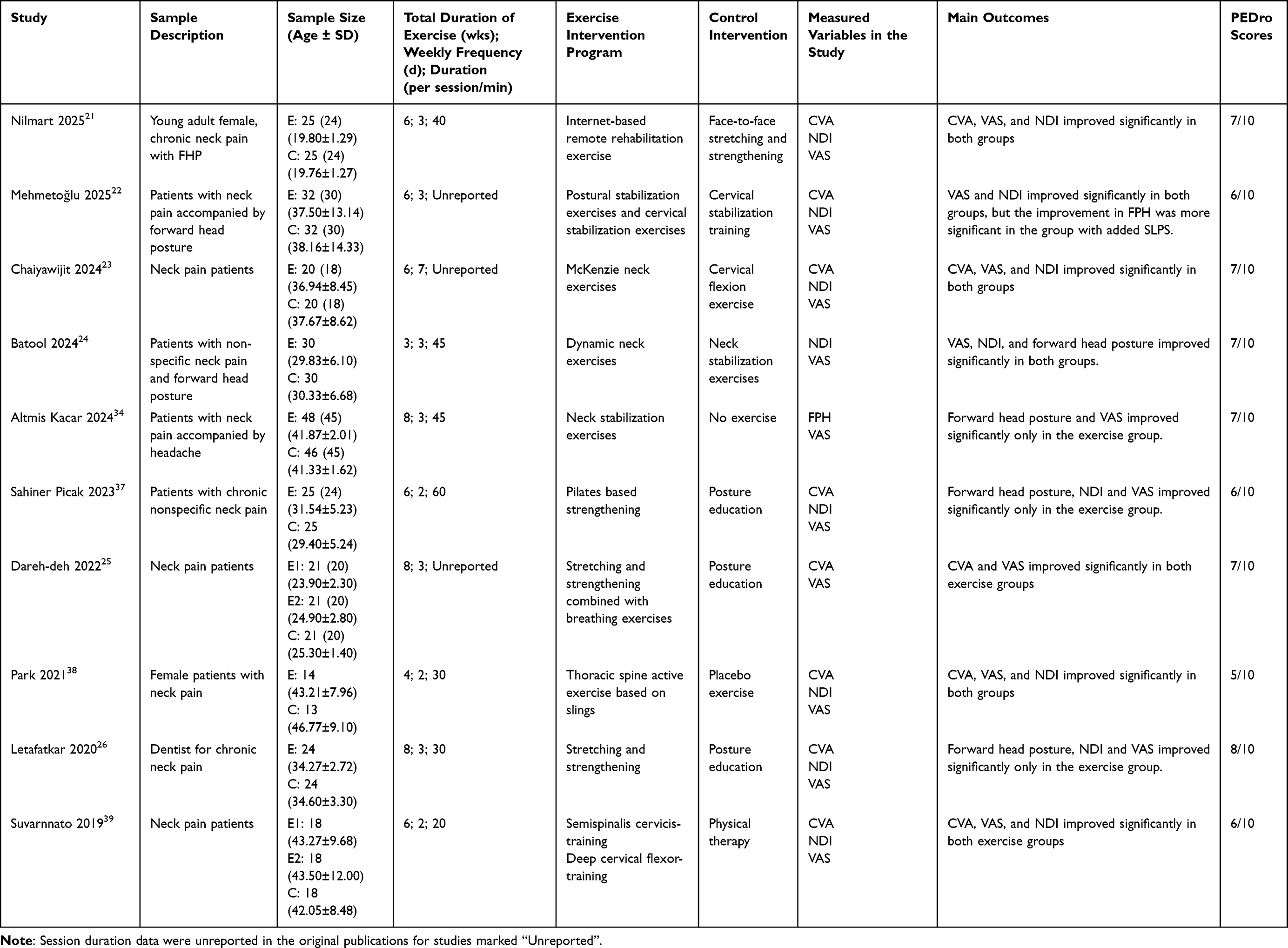 |
Table 1 A Description of Eligible Studies (n = 10) |
The included studies were published between 2019 and 2025. The distribution by year was as follows: one study in 2019,39 one in 2020,26 one in 2021,38 one in 2022,25 one in 2023,37 three in 2024,23,24,34 and two in 2025.21,22 The total sample size across all studies was 550 participants. Individual study sample sizes ranged from 40 to 120, with the experimental group sizes varying between 20 and 60 participants and the control group sizes similarly ranging from 20 to 60 participants. Nine of the included ten RCTs delivered entirely clinic-supervised exercise programmers, and one trial adopted a hybrid intervention model of online guidance plus supervised home.
All included studies investigated active exercise interventions for the management of forward head posture. The specific types of exercises employed included (Neck stabilization exercises, Postural correction exercises, Dynamic exercises, Pilates-based exercises, McKenzie neck exercises). The duration of the intervention programs ranged from 3 to 8 weeks. The prescribed frequency was predominantly 3 to 5 sessions per week, with each session lasting between 20 and 60 minutes. The control groups received various comparators, including routine nursing care, no intervention (wait-list control), general exercise programs, or standard physical therapy. All included studies reported at least one of the core outcome measures defined in our protocol. CVA was reported in 8 studies. FPH metrics (alternative to CVA) were reported in 2 studies. Pain intensity, measured by the VAS, was reported in 9 studies. Neck disability, measured by the NDI, was reported in 9 studies.
Risk of Bias Assessment
The methodological quality and risk of bias of the 10 included RCTs were assessed using the Cochrane RoB 2.0 tool. The detailed assessment results for each domain are summarized below and illustrated in Figure 2.
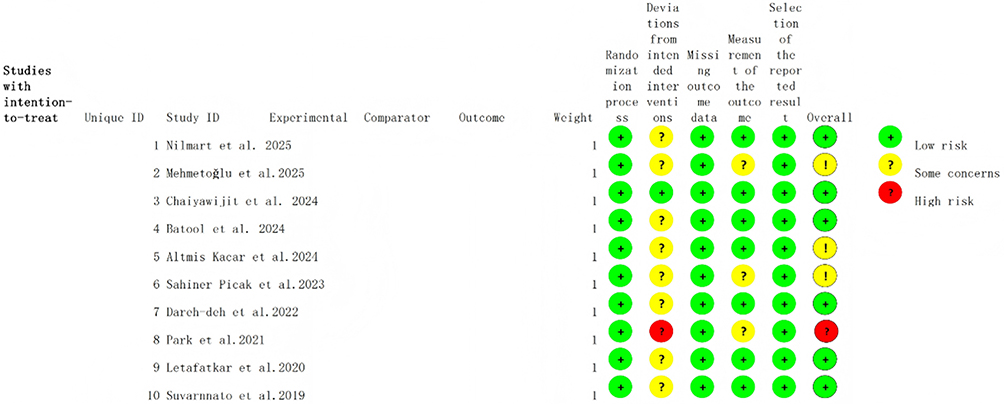 |
Figure 2 Cochrane risk of bias 2 assessment of bias within randomized studies. Symbol definitions: Green circle (+): Low risk of bias; Yellow circle (?): Some concerns of bias; Red circle (! /?): High risk of bias. |
Bias arising from the randomization process: All 10 studies explicitly described appropriate methods for random sequence generation. Consequently, all studies were judged as having a Low risk of bias in this domain.
Bias due to deviations from intended interventions: All studies employed adequate methods such as sealed opaque envelopes or central randomization, resulting in a Low risk rating. Due to the nature of therapeutic exercise interventions, it was impossible to blind the therapists delivering the intervention or fully blind the participants to their group allocation in any of the studies. Therefore, all studies were rated as having High risk or Some concern in this domain. This represents the primary source of potential bias across the included literature.
Bias in measurement of the outcome: 5 studies implemented blinded outcome assessment and were rated as Low risk. 4 studies did not clearly specify whether outcome assessors were blinded, leading to a judgment of Some concern.1 study likely did not employ blinding for outcome assessment and was rated as High risk.
Bias due to missing outcome data: All studies reported follow-up rates of ≥80% (attrition rates ≤20%) and provided clear descriptions of reasons for dropout and handling methods. Thus, all studies were judged as Low risk.
Bias in selection of the reported result: All studies reported all pre-specified outcome measures without evidence of selective reporting. This domain was rated as Low risk for all included studies.
Other bias: The baseline characteristics were well balanced across groups in all studies and no significant baseline imbalances were found. This area was rated as being Low risk.
Results
Effect of Forward Head Posture (CVA)
There were 8 studies with a total of 420 participants that reported the CVA to determine the effects of therapeutic exercise on FHP. These studies had different structures. 3 studies involved one experimental group and one control group. 2 studies comprised two separate experimental groups; both compared independently with a shared control group. 3 articles were based on the comparison between two experimental groups.
Heterogeneity testing revealed moderate to high between study inconsistency in the primary analysis of raw angle changes (I2 = 74.6%, p < 0.001) (Figure 3). Consequently, a Der Simonian Laird random effects model was applied to pool the effect estimates. The pooled MD in the CVA was 3.38° (95% CI: 2.10° to 4.65°, p < 0.001), indicating that therapeutic exercise led to a statistically significant increase in CVA compared to control conditions. A positive MD reflects improved FHP, as a larger CVA corresponds to a more neutral, physiologically normal head and neck alignment. Notably, this improvement of 3.38° exceeds the minimal clinically important difference (MCID) of 1.4° for CVA, representing a meaningful postural correction that is perceptible to clinicians and associated with reduced mechanical loading on cervical structures.40
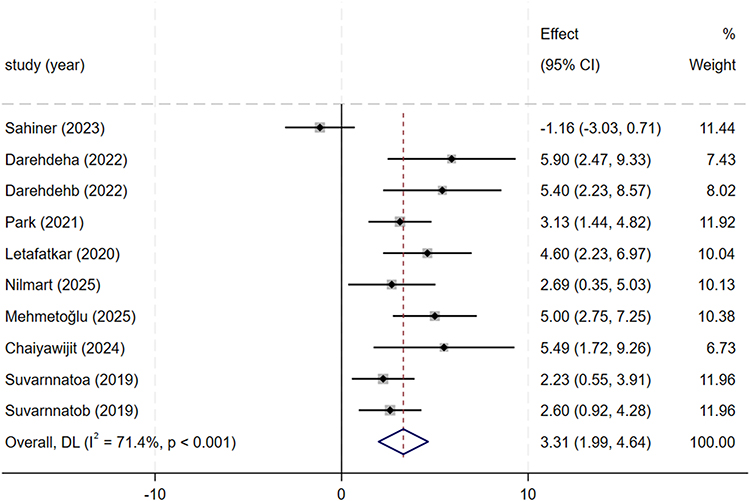 |
Figure 3 Forest plot of the effect of therapeutic exercise on CVA. Note: Weights are from random effects model. |
To verify the robustness of these findings, a sensitivity analysis was performed using the standardized mean difference (SMD, Hedges’ g). The pooled effect size was 0.95 (95% CI: 0.61 to 1.28), with between-study heterogeneity of I2 = 64.21% (p < 0.05). The overall effect test yielded a Z-value of 5.49 (p < 0.001), and the 95% confidence interval did not cross the null line of 0, fully aligning with the direction and statistical significance of the primary MD analysis.
These results confirm that therapeutic exercise is significantly more effective than control conditions in increasing CVA, thereby effectively correcting FHP in patients with neck pain.
Effect of Pain Intensity (VAS)
There were 9 studies (480 participants) that reported Visual Analog Scale (VAS) scores to determine the effects of therapeutic exercise on pain intensity in patients with neck pain.
Extreme Heterogeneity Analysis (VAS): Extremely high between study heterogeneity was observed (I2 = 95.49%, p < 0.001) (Figure 4), representing substantial variability across studies that warrants detailed investigation. Multiple sources likely contributed to this extreme inconsistency:
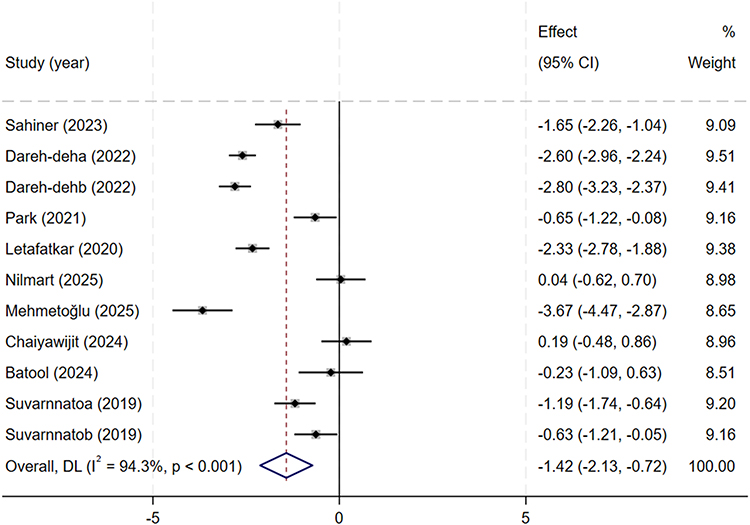 |
Figure 4 Forest plot of the effect of therapeutic exercise on VAS. Note: Weights are from random effects model. |
Clinical heterogeneity: Variations in baseline pain severity (acute vs chronic neck pain), pain duration, and comorbid conditions (headache, dizziness) across study populations.
Methodological heterogeneity: Differences in VAS administration (100mm vs 10cm scale), timing of outcome assessment (immediate post-treatment vs follow-up), and exercise dosage parameters.
Conceptual heterogeneity: Diverse theoretical frameworks underpinning exercise interventions (biomechanical vs neurophysiological approaches) Despite this high heterogeneity, the direction of effect consistently favored therapeutic exercise across all included studies, supporting the robustness of the core finding.
Leading to the use of a priori specified random effects model for pooling. Therapeutic exercise significantly reduced VAS scores compared with control conditions, with a pooled MD of –1.42 points (95% CI: –2.11 to –0.73, p < 0.001). This reduction exceeds the established minimal clinically important difference (MCID) of 1.0–1.5 points on the 10-point VAS scale for neck pain, confirming a meaningful clinical benefit that patients can perceive.41 A negative MD value reflects decreased pain intensity and improved outcomes.
Sensitivity analysis using the standardized mean difference (Hedges’ g = –1.72, 95% CI: –2.69 to –0.71, p = 0.001) confirmed the robustness of the primary findings.
Meta-regression identified exercise modality as a key source of heterogeneity. Despite the substantial between-study inconsistency, these results consistently demonstrate that therapeutic exercise effectively alleviates pain intensity in patients with neck pain.
Effect of Neck Disability (NDI)
The effect of therapeutic exercise on neck disability was studied in 8 studies, which included 400 subjects and the NDI used.
High Heterogeneity Analysis (NDI): High between study heterogeneity was observed (I2 = 86.65%, p < 0.001) (Figure 5), This substantial inconsistency can be attributed to:
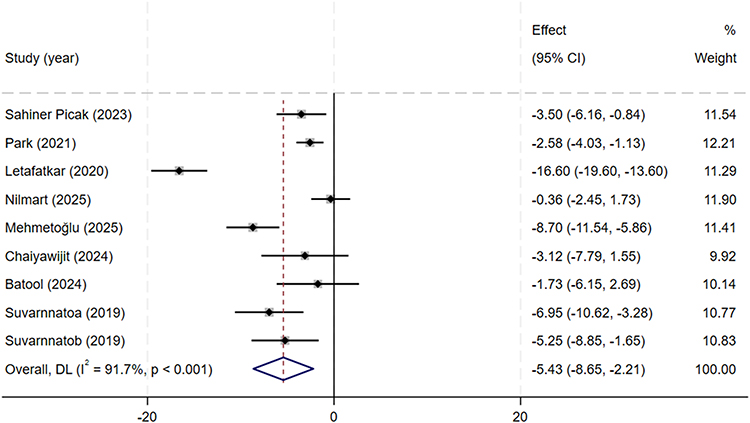 |
Figure 5 Forest plot of the effect of therapeutic exercise on NDI. Note: Weights are from random effects model. |
Clinical heterogeneity: Variations in baseline disability levels, chronicity of symptoms, and participant age ranges.
Methodological heterogeneity: Differences in NDI version usage, language translations, and cultural adaptations across studies.
Conceptual heterogeneity: Variable operationalization of “disability” across different healthcare contexts and study populations.
Notably, meta-regression revealed that intervention duration and exercise modality collectively explained 85.56% of this heterogeneity, indicating these are the primary modifiable factors driving outcome variability.
Prompting the use of a priori specified random effects model for pooling. Therapeutic exercise significantly reduced NDI scores compared with control conditions, with a pooled MD of –5.44 points (95% CI: –8.56 to –2.32, p < 0.001). This reduction exceeds the established minimal clinically important difference (MCID) of 3.5–5 points on the NDI, confirming a meaningful improvement in patients’ daily functional capacity that translates to real-world benefits in activities of daily living.42 A negative MD value indicates reduced disability and improved functional outcomes.
Sensitivity analysis using the standardized mean difference (Hedges’ g = –1.08, 95% CI: –1.66 to –0.50, p < 0.001) confirmed the robustness of the primary findings.
Meta-regression identified intervention duration and exercise modality as the primary sources of heterogeneity, with these two covariates explaining 85.56% of the between study variation. Collectively, these results consistently demonstrate that therapeutic exercise effectively reduces neck disability and enhances functional status in patients with neck pain.
Subgroup Analysis
To explore the sources of the substantial heterogeneity observed in the primary meta-analyses (I2 >50% for all outcomes), exploratory subgroup analyses were conducted for the core outcome measures: Craniovertebral Angle (CVA), Visual Analog Scale (VAS), and Neck Disability Index (NDI). The studies were stratified based on two key clinical variables: type of exercise and duration of intervention. Studies were categorized into single-mode exercise (eg, neck stabilization exercises alone) and combined exercise (eg, neck stabilization combined with postural correction or other modalities). The exploratory analysis suggested a trend that combined exercise interventions were associated with greater improvements across all three outcome measures (CVA, VAS, and NDI) compared to single-mode exercises. The differences between subgroups were statistically significant for all outcomes (P<0.05 for each comparison). This exploratory finding suggests that a multimodal approach addressing both muscle stability and postural alignment may be more effective than isolated training, but requires confirmation in larger, adequately powered studies specifically designed to compare these modalities. Studies were divided into two groups based on the intervention period: short-term (< 8 weeks) and long-term (≥ 8 weeks). Exploratory analysis indicated that interventions lasting ≥ 8 weeks appeared to show superior efficacy in improving CVA, reducing pain (VAS), and alleviating disability (NDI) compared to those lasting < 8 weeks. The subgroup differences were statistically significant for all indicators (P<0.05), suggesting that a longer duration of therapeutic exercise may be critical for achieving optimal clinical outcomes. Given the limited number of studies in each duration subgroup, this finding should be considered hypothesis-generating rather than definitive. These exploratory subgroup analyses indicate that both exercise modality and intervention duration are potential moderators of treatment efficacy. Specifically, combined exercise protocols implemented over a period of at least 8 weeks appear to be associated with the most effective strategy for managing forward head posture, pain, and disability in patients with neck pain. These factors likely account for a substantial portion of the heterogeneity observed in the overall pooled estimates. All subgroup findings should be interpreted cautiously as exploratory analyses, not as definitive clinical recommendations. Detailed subgroup analyses can be found in Supplementary Figures S1–S6.
Summary of Findings Table (GRADE)
The certainty of evidence was graded as moderate for craniovertebral angle and low for both pain intensity and neck disability (Table 2). Evidence was downgraded primarily due to substantial statistical heterogeneity, moderate risk of bias across included studies, and imprecision due to small sample sizes. No outcome was rated as high certainty. The low to moderate certainty of evidence indicates that future research may substantially change these effect estimates.
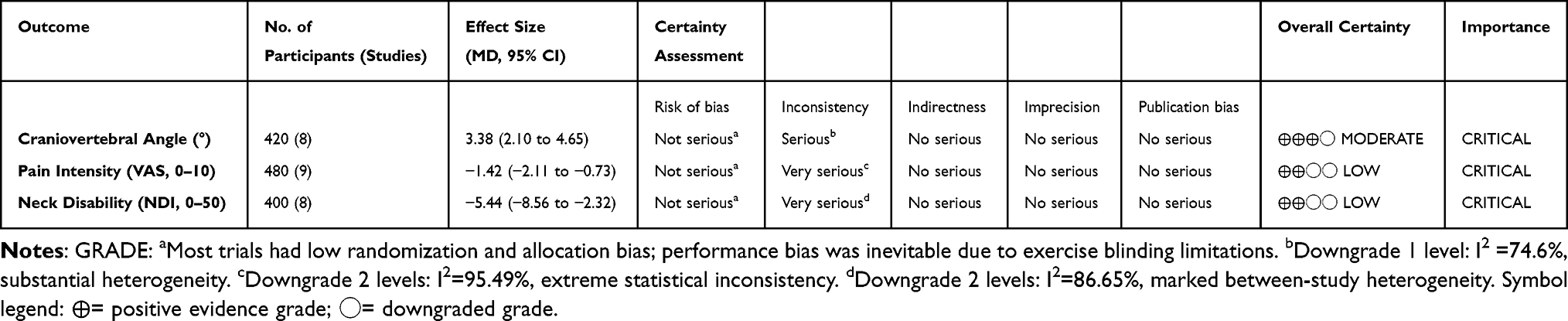 |
Table 2 Summary of Findings (GRADE) |
Meta-Regression Analysis
We conducted meta-regression analyses to examine the influence of intervention duration and exercise modality on treatment outcomes, with results presented in Supplementary Table S3.
Regarding the CVA, the joint model incorporating both covariates was not statistically significant (F = 2.27, p = 0.174), although the covariates collectively accounted for 34.28% of the between-study heterogeneity. Neither intervention duration (β = 1.686, p = 0.341) nor exercise modality (β= 1.64, p = 0.335) showed a statistically significant association with CVA improvement, despite a positive trend suggesting potential benefits of longer interventions and combined exercise modalities.
For the NDI, the joint model reached statistical significance (F = 18.10, p = 0.003), explaining 89.08% of the between-study heterogeneity explained by the two covariates (residual I2=51.95%). Longer intervention duration (≥ 8 weeks) was associated with a greater reduction in NDI scores (β= -7.900, p = 0.041), and combined exercise demonstrated a superior effect on functional improvement compared to single-mode exercise (β= -5.607, p = 0.070), with both relationships approaching marginal significance.
In the analysis of the VAS, the joint model was also statistically significant (F = 5.29, p = 0.034), accounting for 49.26% of the between-study heterogeneity explained by the two covariates (residual I2=88.43%). Combined exercise was associated with a greater reduction in pain intensity (β = -1.489, p = 0.086), showing a trend toward significance, whereas intervention duration did not exhibit a significant association (β= -0.796, p = 0.319).
Sensitivity Analysis and Publication Bias
Sensitivity Analysis
To evaluate the strength and consistency of the pooled effect estimates, a sensitivity analysis was performed by applying the leave-one-out method to all three key outcomes CVA, VAS, and NDI. The process involved removing one study at a time in this procedure and repeating the meta-analysis to see how the pooled effect size changed. It was found that when any individual study was omitted, there was no significant change in the direction or magnitude of the pooled effect sizes of CVA, VAS, or NDI (all P>0.05 on the difference in estimates). These results show that the overall findings of the meta-analysis are consistent and reliable and are not influenced by any single outlier or extreme value.
To validate the robustness of our findings, a sensitivity analysis was performed by excluding studies with a PEDro score <6—indicating low methodological quality, which in this analysis included only Park et al The results are summarized in Supplementary Figures S7–S9 and Supplementary Table S4.
After removing the low-quality study, the direction and statistical significance of the pooled effect sizes remained fully consistent with the primary analysis across all three core outcomes:
CVA: The pooled MD was 3.38° (95% CI: 1.84° to 4.91°, p < 0.001), there was no substantial change in the direction, magnitude, or statistical significance of the pooled effect size, while the between-study heterogeneity remained stable (I2 = 74.5%, p < 0.001).
VAS: The pooled MD was −1.50 (95% CI: −2.24 to −0.76, p < 0.001), with I2 = 94.5% (primary analysis I2 = 94.3%).
NDI: The pooled MD was −5.82 (95% CI: −9.75 to −1.89, p < 0.001), with I2 = 92.0% (primary analysis I2 = 91.7%).
No substantial change was observed in the magnitude of the pooled effect sizes. Moreover, the superiority of combined exercise modalities and interventions lasting ≥8 weeks remained consistent in subgroup and meta-regression analyses. These results confirm that our core conclusions are not influenced by low-quality studies and demonstrate good robustness and reliability.
Publication Bias
Publication bias was determined visually with the help of funnel plots and statistically with the help of linear regression test by Egger. The CVA, VAS, and NDI funnel plots showed a relatively symmetric distribution of studies around the pooled effect estimate and there was no apparent asymmetry that could be attributed to missing studies (Figure 6). The results of the test conducted by Egger confirmed the visual inspection indicating that none of the outcomes had any statistically significant evidence of publication bias CVA (p=0.066), VAS (P=0.059), NDI (P=0.327). As all P -values were more than 0.05, we can state that this meta-analysis has no significant publication bias. The fact that the sensitivity analysis findings are consistent and that there is no major publication bias enhances the validity of the results, which justifies the conclusion that therapeutic exercise is an effective treatment of neck pain even though heterogeneity was observed.
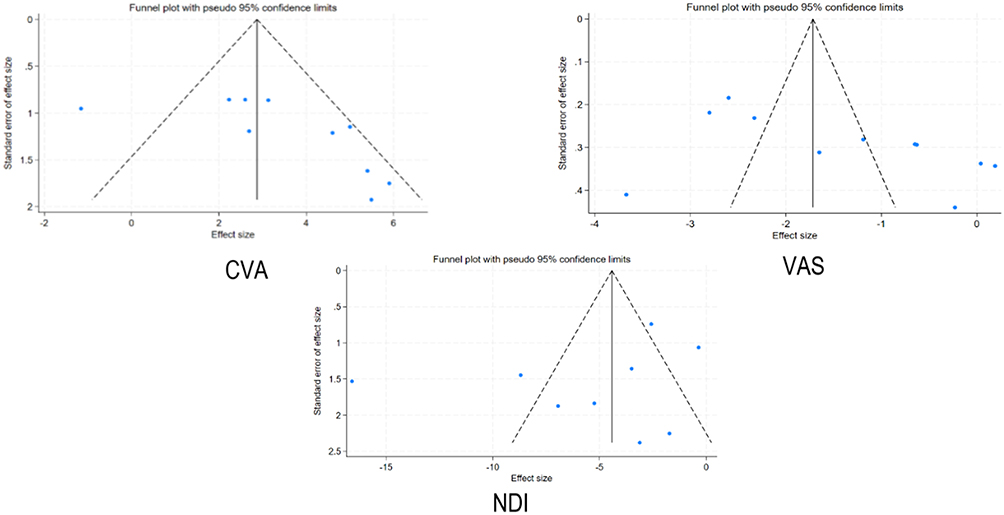 |
Figure 6 Funnel plots of CVA, VAS, and NDI in various studies. |
Discussion
Main Findings
This systematic review and meta-analysis provide a comprehensive assessment of the efficacy of therapeutic exercise on FPH and related clinical outcomes in patients with neck pain. Through a systematic search of six core databases, we included 10 RCTs with a total of 550 participants. Our quantitative synthesis yielded several key findings: therapeutic exercise significantly corrected FHP, as evidenced by a notable improvement in the CVA. Meanwhile, patients experienced significant reductions in pain intensity (VAS) and functional disability (NDI). Exploratory subgroup analyses provided preliminary evidence for optimizing treatment strategies: specifically, combined exercise modalities appeared to be associated with superior therapeutic effects compared to single-mode exercises. Furthermore, interventions with a duration of at least 8 weeks showed trends toward better outcomes across all measured indicators, compared to shorter-term interventions (<8 weeks). These findings are broadly consistent with existing literature, which supports structured therapeutic exercise as a first-line intervention for the management of FHP and neck pain. Importantly, our study adds to the existing evidence by quantitatively validating the precise benefits of multimodal interventions and longer intervention durations, and provides preliminary evidence-based recommendations for clinical practice.
Supervision pattern was consistent across most trials (full in-clinic supervision in nine studies), with merely one hybrid protocol identified; hence differences in exercise supervision could not explain the prominent between-study heterogeneity of VAS and NDI. The extreme heterogeneity observed for VAS (I2 = 95.49%) and NDI (I2 = 86.65%) merits careful interpretation from multiple perspectives. From a clinical standpoint, this variability reflects the heterogeneous nature of neck pain itself a condition encompassing diverse pathophysiological mechanisms from mechanical strain to central sensitization. Methodologically, the variability stems from differences in exercise dosage, treatment fidelity, outcome measurement timing, and participant characteristics across studies. Conceptually, this heterogeneity underscores that “therapeutic exercise” is not a uniform intervention but encompasses diverse approaches targeting different mechanisms (biomechanical, neurophysiological, sensorimotor). Importantly, despite this statistical heterogeneity, the direction of effect consistently favored exercise across all studies, suggesting a robust treatment effect that transcends methodological variations. The meta-regression finding that exercise modality and duration explain 85.56% of NDI heterogeneity provides critical insight: much of the apparent “inconsistency” in the literature reflects systematic differences in intervention quality, not true treatment efficacy variability.
Significant between-study heterogeneity was observed across all three primary outcomes, which was further investigated through meta-regression analyses. Our findings indicate that intervention duration and exercise modality serve as important sources of heterogeneity, particularly for functional outcomes (NDI), where these two covariates accounted for more than 85% of the between-study variation. Consistent with the results from exploratory subgroup analyses, combined exercise modalities and intervention durations of at least 8 weeks were associated with greater improvements in posture, pain, and function, although some associations showed only marginally significant trends, likely due to the limited number of included studies and insufficient statistical power. The residual heterogeneity observed in CVA and VAS outcomes may be explained by other unmeasured factors, such as baseline symptom severity, participant age, and CVA measurement methods, which warrant further investigation in future large-scale studies.
Potential Mechanisms for Postural and Pain Improvements
Building on the seminal work of Farina et al6 and Falla et al,7 the effectiveness of therapeutic exercise can be understood through an integrated biopsychosocial model encompassing three interrelated mechanisms:
Three physiological and biomechanical mechanisms, which are interrelated, can be used to explain the effectiveness of therapeutic exercise in improving FPH and related symptoms in patients with neck pain: Restoration of Cervical Stability through Deep Muscle Strengthening The weakness and inhibition of deep cervical flexors (DCF), especially longus colli and longus capitis, and overactivity of superficial extensors is the main biomechanical cause of FHP.43,44 These stabilizers are particularly targeted by therapeutic exercises, specifically stabilization protocols, aimed at reactivating and strengthening them. Through increasing the strength-generating capacity and endurance of the DCF, these exercises restore the natural lordotic curvature of the cervical spine and overcome the anterior gravitational moment of the head.45,46 This results in a quantifiable rise in the Craniovertebral Angle (CVA) and enhanced segmental stability, decreasing mechanical stress on cervical joints and ligaments that lead to pain.
Breaking the Vicious Cycle: Pain-Spasm-Posture and Central Sensitization. Chronic neck pain involves not only peripheral tissue damage but also central nervous system sensitization, as demonstrated by. Prolonged FHP creates a self-perpetuating cycle: mechanical stress triggers nociceptive input, which leads to muscle guarding and spasm, further exacerbating postural distortion. Therapeutic exercise interrupts this cycle through two pathways: (1) reducing peripheral nociceptive input by improving mechanical alignment, and (2) modulating central pain processing through descending inhibitory pathways. Proprioception and Motor Control Improvement. In addition to muscular strength and flexibility, FHP is often tainted by sensorimotor control changes and lack of postural awareness.47,48 From a neurophysiological perspective, FHP is associated with distorted proprioceptive input from cervical mechanoreceptors, which impair joint position sense and motor control. Therapeutic exercise―particularly proprioceptive and neuromuscular training―retrains the central nervous system to recognize and maintain neutral head posture. Improved postural control does not only maintain the improvements made during therapy but is also an important preventive tool against recurrence of FHP once the intervention has ended. Importantly, the posture-pain relationship is nonlinear: small postural improvements can trigger disproportionate pain reduction through central sensitization reversal, which explains why the observed CVA improvement of 3.38° is associated with clinically meaningful pain reduction.
Comparison with Previous Studies
Our results are consistent with yet greatly expanding the findings of current systematic reviews and meta-analyses. Although previous meta-analyses were mostly based on single outcomes, ie, assessing either pain intensity or functional disability alone,29,30 our research used a three-dimensional evaluation model that included CVA, VAS, and NDI. We simultaneously assessed posture, pain, and function and gave strong evidence that therapeutic exercise has a synergistic effect in all three areas. This creates an unbroken chain of evidence between postural correction (FHP reduction) and symptom relief and subsequent functional recovery which provides a holistic view which was lacking in much of the earlier literature. One of the significant contributions of this paper is the resolution of discrepancies observed in other reviews. Previous research has frequently provided conflicting findings concerning the effectiveness of particular forms of exercise probably because of the pooling of various intervention procedures without sufficient stratification.49,50 Conversely, we have shown through exploratory subgroup analyses that combined exercise modalities (combination of stabilization and postural correction) may produce significantly better results than single-mode interventions using prespecified subgroup analyses. This observation explains the fact that the low efficacy of some studies conducted previously might have been due to the use of less comprehensive exercise programs instead of the lack of efficacy of exercise itself. Moreover, our analysis fills one of the gaps that most previous reviews did not cover thoroughly, namely, the time aspect of treatment. The previous works tended to consider short-term and long-term interventions as the same, but our exploratory findings established a specific time point of at least 8 weeks. We noted that the interventions with durations of less than 8 weeks had transient effects and increased rates of recurrence, whereas longer periods enabled long-lasting improvements in functioning. Such dose-response relationships not only explain the differences in past conclusions, but also highlight the fact that chronic Forward Head Posture needs long-term neuromuscular adaptation-physiological processes which cannot be effectively addressed by short term interventions. Together, through multidimensional outcomes, separating exercise modalities and establishing optimal treatment duration, our study provides a refined evidence base that eliminates the contradictions of previous research and offers more practical recommendations to clinical practice.
Minimal Clinically Important Difference (MCID) Interpretation
The observed treatment effects demonstrate meaningful clinical significance when compared to established MCID thresholds:
CVA (3.38° improvement): Exceeds the MCID of 1.4° for postural correction.40 This magnitude of change is visible on clinical assessment and associated with reduced compressive forces on cervical facet joints and decreased muscle activation requirements for postural maintenance.
VAS (1.42-point reduction): Falls within the MCID range of 1.0–1.5 points for chronic neck pain.41 This represents a change that patients perceive as “much improved” and correlates with reduced analgesic medication use. NDI (5.44-point reduction): Exceeds the MCID of 3.5–5 points for functional improvement.42
This degree of change translates to meaningful improvements in activities of daily living, including work productivity, sleep quality, and social participation. Collectively, these findings confirm that therapeutic exercise produces not only statistically significant but also clinically meaningful improvements across all three core domains.
Limitations
The comparatively low number of studies that were included (n=10) and the relatively small sample sizes in certain trials (less than 60 participants) can restrict the statistical power and stability of our meta-analytic estimates. Even though we used stringent procedures to reduce bias, a bigger set of high-quality RCTs would be required to validate the strength of these findings. Subgroup Analysis Limitations: The exploratory nature of subgroup analyses represents an important limitation. These analyses were not powered to detect definitive differences between modalities or durations, and multiple testing increases the risk of Type I error. The findings regarding combined exercise and ≥8-week duration should be considered hypothesis generating, requiring confirmation in prospective RCTs specifically designed to test these comparisons. Although we had prespecified subgroup analyses to investigate sources of heterogeneity, there was still a lot of clinical and methodological diversity among the included studies. The differences in the modalities of exercise, the length of interventions, and follow-up plans create some inherent variability that could not be entirely explained. This means that the confounding variables that are unmeasured might still affect the pooled effect sizes, which is why it is necessary to interpret the aggregated data with caution. Most of the available evidence is largely found on short-term follow-ups (12 weeks). The lack of long-term data does not allow making a definite conclusion about the effectiveness of therapeutic exercises over a long period after the immediate post-intervention phase. We cannot draw strong conclusions concerning the long-term maintenance of postural corrections or recurrence rates of FPH following the discontinuation of structured training. Lastly, partial reporting of exercise parameters in various primary studies limited our capacity to undertake an exhaustive dose-response analysis. Important information like the exact movement routines, intensity and progression criteria were frequently not provided. This granularity makes us unable to determine the ideal amount of exercise needed to achieve the highest level of therapeutic benefit, which is a major reason why standardized reporting should be done in future research. Overall, although our results offer useful information about the effectiveness of therapeutic exercise in treating FHP, such limitations highlight the importance of conducting future large-scale, long-term RCTs using standardized protocols and extensive reporting to confirm and improve clinical recommendations.
Conclusions
Therapeutic exercise may be associated with improved craniovertebral angle, reduced neck pain, and better neck function in individuals with FHP and neck pain. Exploratory analyses suggest that combined exercise protocols that include cervical stabilization and postural correction may offer greater benefits than single-mode exercises. In addition, interventions lasting at least 8 weeks may be associated with more evident functional improvements. However, the overall certainty of evidence remains limited due to heterogeneity, methodological variations, and the relatively small number of studies included. Future largescale, high-quality RCTs with long-term follow-up and standardized exercise protocols are needed to strengthen the evidence base, particularly to definitively compare exercise modalities and optimal intervention durations.
Data Sharing Statement
All data relevant to the study are included in the article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lotfian S, Fesharaki MJ, Shahabbaspour Z, Akbarzadeh H, Moezy A. The impact of forward head posture on neck muscle endurance and thickness in women with chronic neck pain: a cross-sectional study. BMC Musculoskelet Disord. 2025;26(1):468. doi:10.1186/s12891-025-08705-w
2. Yang S, Boudier-Revéret M, Yi YG, Hong KY, Chang MC. Treatment of chronic neck pain in patients with forward head posture: a systematic narrative review. Healthcare. 2023;11(19):2604. doi:10.3390/healthcare11192604
3. Lin CC, Hua SH, Lin CL, Cheng CH, Liao JC, Lin CF. Impact of prolonged tablet computer usage with head forward and neck flexion posture on pain intensity, cervical joint position sense and balance control in mechanical neck pain subjects. J Med Biol Eng. 2020;40(3):372–18. doi:10.1007/s40846-020-00525-8
4. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
5. Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–332. doi:10.1016/S0304-3959(99)00242-0
6. Falla D, Farina D. Neural and muscular factors associated with motor impairment in neck pain. Curr Rheumatol Rep. 2007;9(6):497–502. doi:10.1007/s11926-007-0080-4
7. Falla DL, Jull GA, Hodges PW. Patients with neck pain demonstrate reduced electromyographic activity of the deep cervical flexor muscles during performance of the craniocervical flexion test. Spine. 2004;29(19):2108–2114. doi:10.1097/01.brs.0000141170.89317.0e
8. O’Sullivan P. It’s time for change with the management of non-specific chronic low back pain. Br J Sports Med. 2012;46(4):224–227. doi:10.1136/bjsm.2010.081638
9. Hoy DG, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24(6):783–792. doi:10.1016/j.berh.2011.01.019
10. Guzman J, Hurwitz EL, Carroll LJ, et al. A new conceptual model of neck pain. J Manipulative Physiol Ther. 2009;32(2):S17–S28. doi:10.1016/j.jmpt.2008.11.007
11. Henschke N, Kamper SJ, Maher CG. The epidemiology and economic consequences of pain. Mayo Clin Proc. 2015;90(1):139–147. doi:10.1016/j.mayocp.2014.09.010
12. Manchikanti L, Singh V, Datta S, Cohen SP, Hirsch JA; American Society of Interventional Pain Physicians. Comprehensive review of epidemiology, scope, and impact of spinal pain. Pain Physician. 2009;12(4):E35–70.
13. Haldeman S, Carroll L, Cassidy JD. Findings from the bone and joint decade 2000 to 2010 task force on neck pain and its associated disorders. J Occup Environ Med. 2010;52(4):424–427. doi:10.1097/JOM.0b013e3181d44f3b
14. Gustafsson E, Thomée S, Grimby-Ekman A, Hagberg M. Texting on mobile phones and musculoskeletal disorders in young adults: a five-year cohort study. Appl Ergon. 2017;58:208–214. doi:10.1016/j.apergo.2016.06.012
15. Cagnie B, Danneels L, Van Tiggelen D, De Loose V, Cambier D. Individual and work related risk factors for neck pain among office workers: a cross sectional study. Eur Spine J. 2007;16(5):679–686. doi:10.1007/s00586-006-0269-7
16. Nunes A, Espanha M, Teles J, Petersen K, Arendt-Nielsen L, Carnide F. Neck pain prevalence and associated occupational factors in Portuguese office workers. Int J Ind Ergon. 2021;85:103172. doi:10.1016/j.ergon.2021.103172
17. Saleh MS, Mohamed WM, Elsayed WH, Abdelatief EEM. Proprioceptive neuromuscular facilitation stretching exercises for treatment of temporomandibular dysfunction in patients with forward head posture: a double-blinded, randomized, controlled trial. J Back Musculoskelet Rehabil. 2024;37(5):1259–1268. doi:10.3233/BMR-230358
18. Anwar S, Zahid J, Alexe CI, et al. Effects of myofascial release technique along with cognitive behavior therapy in university students with chronic neck pain and forward head posture: a randomized clinical trial. Behav Sci. 2024;14(3):205. doi:10.3390/bs14030205
19. Abd El-Azeim AS, Mahmoud AG, Mohamed MT, El-Khateeb YS. Impact of adding scapular stabilization to postural correctional exercises on symptomatic forward head posture: a randomized controlled trial. Eur J Phys Rehabil Med. 2022;58(5):757. doi:10.23736/S1973-9087.22.07361-0
20. Hyeon DA, Kim JS, Lim HW. Effects of capital flexion exercise on craniovertebral angle, trunk control, balance, and gait in stroke patients with forward head posture: a randomized controlled trial. Medicina. 2025;61(5):797. doi:10.3390/medicina61050797
21. Nilmart P, Sichuai A, Chedang A, Goontharo C, Janjamsai N. Internet-based telerehabilitation versus in-person therapeutic exercises in young adult females with chronic neck pain and forward head posture: randomized controlled trial. JMIR Rehabil Assist Technol. 2025;12:e74979. doi:10.2196/74979
22. Mehmetoğlu G, Yüksel İ. Effect of postural stabilization exercises in combination with cervical stabilization exercises on craniovertebral angle, pain, disability, and quality of life in patients with chronic neck pain: a randomized controlled trial. Healthcare. 2025;13(12):1388. doi:10.3390/healthcare13121388
23. Chaiyawijit S, Kanlayanaphotporn R. McKenzie neck exercise versus cranio-cervical flexion exercise on strength and endurance of deep neck flexor muscles, pain, disability, and craniovertebral angle in individuals with chronic neck pain: a randomized clinical trial. J Man Manip Ther. 2024;32(6):573–583. doi:10.1080/10669817.2024.2337979
24. Batool A, Soomro RR, Baig AAM. Comparing the effects of neck stabilization exercises versus dynamic exercises among patients having nonspecific neck pain with forward head posture: a randomized clinical trial. BMC Musculoskelet Disord. 2024;25(1):707. doi:10.1186/s12891-024-07749-8
25. Dareh-deh HR, Hadadnezhad M, Letafatkar A, Peolsson A. Therapeutic routine with respiratory exercises improves posture, muscle activity, and respiratory pattern of patients with neck pain: a randomized controlled trial. Sci Rep. 2022;12(1):4149. doi:10.1038/s41598-022-08128-w
26. Letafatkar A, Rabiei P, Alamooti G, Bertozzi L, Farivar N, Afshari M. Effect of therapeutic exercise routine on pain, disability, posture, and health status in dentists with chronic neck pain: a randomized controlled trial. Int Arch Occup Environ Health. 2020;93(3):281–290. doi:10.1007/s00420-019-01480-x
27. Sepehri S, Sheikhhoseini R, Piri H, Sayyadi P. The effect of various therapeutic exercises on forward head posture, rounded shoulder, and hyperkyphosis among people with upper crossed syndrome: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2024;25(1):105. doi:10.1186/s12891-024-07224-4
28. Sheikhhoseini R, Shahrbanian S, Sayyadi P, O’Sullivan K. Effectiveness of therapeutic exercise on forward head posture: a systematic review and meta-analysis. J Manipulative Physiol Ther. 2018;41(6):530–539. doi:10.1016/j.jmpt.2018.02.002
29. Pensri C, Liang Z, Treleaven J, Jull G, Thomas L. Cervical musculoskeletal impairments in migraine and tension-type headache and relationship to pain related factors: an updated systematic review and meta-analysis. Musculoskelet Sci Pract. 2025;76:103251. doi:10.1016/j.msksp.2024.103251
30. Andias R, Silva AG. A systematic review with meta-analysis on functional changes associated with neck pain in adolescents. Musculoskeletal Care. 2019;17(1):23–36. doi:10.1002/msc.1377
31. Mahmoud NF, Hassan KA, Abdelmajeed SF, Moustafa IM, Silva AG. The relationship between forward head posture and neck pain: a systematic review and meta-analysis. Curr Rev Musculoskelet Med. 2019;12(4):562–577. doi:10.1007/s12178-019-09594-y
32. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
33. Alonso-Coello P, Oxman AD, Moberg J, et al. GRADE evidence to decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: clinical practice guidelines. BMJ. 2016;353:i2089. doi:10.1136/bmj.i2089
34. Altmis Kacar H, Ozkul C, Baran A, Guclu-Gunduz A. Effects of cervical stabilization training in patients with headache: a single-blinded randomized controlled trial. Eur J Pain. 2024;28(4):633–648. doi:10.1002/ejp.2208
35. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
36. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–721. doi:10.1093/ptj/83.8.713
37. Sahiner Picak G, Yesilyaprak SS. Effects of clinical pilates exercises in patients with chronic nonspecific neck pain: a randomized clinical trial. Ir J Med Sci. 2023;192(3):1205–1214. doi:10.1007/s11845-022-03101-y
38. Park GW, An J, Kim SW, Lee BH. Effects of sling-based thoracic active exercise on pain and function and quality of life in female patients with neck pain: a randomized controlled trial. Healthcare. 2021;9(11):1514. doi:10.3390/healthcare9111514
39. Suvarnnato T, Puntumetakul R, Uthaikhup S, Boucaut R. Effect of specific deep cervical muscle exercises on functional disability, pain intensity, craniovertebral angle, and neck-muscle strength in chronic mechanical neck pain: a randomized controlled trial. J Pain Res. 2019;12:915–925. doi:10.2147/JPR.S190125
40. Heydari Z, Sheikhhoseini R, Shahrbanian S, Piri H. Establishing minimal clinically important difference for effectiveness of corrective exercises on craniovertebral and shoulder angles among students with forward head posture: a clinical trial study. BMC Pediatr. 2022;22(1):230. doi:10.1186/s12887-022-03300-7
41. Kovacs FM, Abraira V, Royuela A, et al; The Spanish Back Pain Research Network. Minimum detectable and minimal clinically important changes for pain in patients with nonspecific neck pain. BMC Musculoskelet Disord. 2008;9(1):43. doi:10.1186/1471-2474-9-43
42. Hung M, Saltzman CL, Kendall R, et al. What are the MCIDs for PROMIS, NDI, and ODI instruments among patients with spinal conditions? Clin Orthop. 2018;476(10):2027–2036. doi:10.1097/CORR.0000000000000419
43. Norasteh AA, Karimi K, Faraji S, et al. Exercise therapy to improve cervical proprioception in individuals with asymptomatic forward head posture: a systematic review of randomized controlled trials. PLoS One. 2025;20(9):e0330665. doi:10.1371/journal.pone.0330665
44. Lee JH, Hwang UJ, Kwon OY. Relationship between cervical lordotic angle and cervical segmental motion during craniocervical flexion test: a cross-sectional study. Medicine. 2024;103(15):e37830. doi:10.1097/MD.0000000000037830
45. Suwaidi ASA, Moustafa IM, Kim M, Oakley PA, Harrison DE. A comparison of two forward head posture corrective approaches in elderly with chronic non-specific neck pain: a randomized controlled study. J Clin Med. 2023;12(2):542. doi:10.3390/jcm12020542
46. Zhang Y, Lin W, Yi M, Song J, Ding L. Effect of long-term cervical extensor exercise program on functional disability, pain intensity, range of motion, cervical muscle mass, and cervical curvature in young adult population with chronic non-specific neck pain: a randomized controlled trial. J Orthop Surg. 2024;19(1):9. doi:10.1186/s13018-023-04487-w
47. Moustafa IM, Diab AAM, Harrison DE. Does forward head posture influence somatosensory evoked potentials and somatosensory processing in asymptomatic young adults? J Clin Med. 2023;12(9):3217. doi:10.3390/jcm12093217
48. Lee H, Oh B, Kim SC. Recognition of forward head posture through 3D human pose estimation with a graph convolutional network: development and feasibility study. JMIR Form Res. 2024;8:e55476. doi:10.2196/55476
49. Park S, Kim K, Kang M. The effects of rehabilitation programs incorporating breathing interventions on chronic neck pain among patients with forward head posture: a systematic review and meta-analysis. Bioengineering. 2025;12(9):947. doi:10.3390/bioengineering12090947
50. Saini N, Tiwari S, Singh L. Evaluating the impact of cervical stabilisation exercises on chronic neck pain: a systematic review. Musculoskeletal Care. 2025;23(2):e70091. doi:10.1002/msc.70091
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.