Back to Journals » Journal of Pain Research » Volume 16
The Value of Pain Sensitivity Questionnaire in Predicting Postoperative Pain in Living Kidney Donors: A Prospective Observational Study
Authors Wu Q ![]() , Luo Y
, Luo Y ![]() , Han M
, Han M ![]() , Li J
, Li J ![]() , Kang F
, Kang F ![]()
Received 16 May 2023
Accepted for publication 11 August 2023
Published 23 August 2023 Volume 2023:16 Pages 2899—2907
DOI https://doi.org/10.2147/JPR.S419719
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Qixing Wu,* Yiyuan Luo,* Mingming Han, Juan Li, Fang Kang
Department of Anesthesiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fang Kang, Department of Anesthesiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei City, Anhui Province, 230036, People’s Republic of China, Tel +86 18155127799, Email [email protected]
Purpose: This study aimed to investigate the value of the Pain Sensitivity Questionnaire (PSQ) for the prediction of postoperative pain and the relationship between pain sensitivity and postoperative pain in kidney donors undergoing living-related kidney transplantation.
Patients and Methods: A total of 148 kidney donors were selected and the preoperative pain sensitivity questionnaire was administered the day before surgery. Kidney donors were assigned to low PSQ group (PSQ < 6.5, n = 76) or high PSQ group (PSQ ≥ 6.5, n = 72). The primary endpoint was the number of patient-controlled analgesia (PCA). Other outcomes included: the incidence of acute pain, flurbiprofen axetil remediation rate, the incidence of chronic pain, neuropathic pain assessment scale (Douleur Neuropathique 4 Questions, DN4), visual analog scale (VAS) at rest after surgery as well as the correlation between PSQ and QST (Quantitative Sensory Testing).
Results: The low PSQ group had a significantly lower number of PCA than high PSQ group (P < 0.0001). The incidence of acute pain was 75% in low PSQ group and 100% in high PSQ group (P < 0.0001). Furthermore, flurbiprofen axetil remediation rate was lower in low PSQ group than that in high PSQ group (P = 0.042). The incidence of chronic pain was significantly lower in low PSQ group than in high PSQ group (6.6% vs 61.1%, P < 0.001). Moreover, DN4 was significantly lower in low PSQ group than that in high PSQ group (P < 0.001). The PSQ-mean was significantly negatively correlated with QST in kidney donors. VAS at rest for the low PSQ group were lower than those of the high PSQ group.
Conclusion: The PSQ was found to be associated with the intensity or postoperative pain and might be used to screen patients prior to living-kidney transplantation.
Keywords: pain, pain sensitivity, pain sensitivity questionnaire, kidney donor
Introduction
Pain is a subjective feeling, and it is related to situations of trauma or disease.1 It is difficult to measure accurately because of its complex symptoms, duration, difficulty in treatment, and the possible pain pathway associated with it.2 Living kidney donor surgery is generally an open surgery, with significant trauma and slow postoperative recovery, often requiring more opioid drugs.3 The pain sensitivity questionnaire (PSQ) is a self-assessment scale of pain sensitivity that was designed by Ruth Ruscheweyh et al.4 It aids in the assessment of the pain sensitivity of the participant, prediction of acute postoperative pain, and screening of individuals who are at a high risk of postoperative chronic pain.4,5 The evaluation effect of PSQ on pain sensitivity has been fully confirmed in various studies globally.6–9 Some studies have also found that PSQ applies to patients with chronic pain and that its correlation with pain sensitivity in healthy patients is significant.10,11
Living kidney donor surgery usually requires a long operation time, which causes excessive trauma to both the kidney donors as well as the recipients.4 In addition, kidney donation may be associated with long-term disease and pain.12,13 Inadequate treatment of postoperative pain can reduce the patient’s ability to participate in rehabilitation plans, leading to poor postoperative outcomes, and delaying patient recovery and discharge time, reducing quality of life and satisfaction, increasing resource consumption and medical costs. PSQ is a non-invasive method for measuring pain sensitivity. Measuring the pain sensitivity of kidney donors can help anesthesiologists enhance postoperative pain management.
It has not been reported whether PSQ can reflect the pain sensitivity of living kidney transplant donors who are healthy patients that undergo nephrectomy. Further, it has not been reported whether PSQ is consistent with the quantitative sensory testing (QST) of pain sensitivity and whether it can help predict postoperative pain levels. Therefore, this study aimed to evaluate the value of PSQ in predicting pain sensitivity and postoperative pain in living-related kidney transplant donors.
Methods
Participants
We performed a prospective observational clinical study. The study received ethical approval from the Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (Anhui Provincial Hospital). An informed consent was given by every patient and the study was registered on the China Clinical Trials Registry (Registration number: ChiCTR2200058704). We confirm that this study complies with the Declaration of Helsinki. Initially, 168 kidney donors who underwent elective living-related kidney transplantation between April 2022 and December 2022 in our hospital were included. We confirmed that all kidney donors signed and provided informed consent to donate their kidneys, along with confirmation that this consent was given voluntarily and under free will.
Inclusion criteria were as follows: (1) age, 40‒80 years; (2) ASA class I‒II; (3) no speech or communication impairment; (4) no history of chronic pain or long-term use of analgesic drugs.
Exclusion criteria: (1) postoperative delirium or other serious complications; (2) reoperation within 3 months; (3) postoperative admission to an intensive care unit (ICU); (4) loss of visit.
Outcomes
The primary endpoint was the number of patient-controlled analgesia (PCA). It is defined as the number of effective patient-controlled analgesia by kidney donors after surgery. Other outcomes included the incidence of acute pain, flurbiprofen axetil remediation rate, the incidence of chronic pain, neuropathic pain assessment scale (Douleur Neuropathique 4 Questions, DN4), VAS at rest after surgery and correlation between PSQ and QST (Quantitative Sensory Testing). Acute pain was defined as the pain after surgery that requires PCA for kidney donors. Chronic pain was defined as the presence of pain in the donor three months after surgery.
Anesthesia and Analgesia Protocol
Preoperative fasting for 8 h and water fasting for 6 h was routine and was ensured without preoperative medication. After admission, ECG, SpO2, ABP, PETCO2, and BIS were monitored. Further, 1‒2mg/kg of intravenous propofol, 0.5ug/kg of sufentanil, and 0.2mg/kg of cis-atracurium bromide were administered to induce anesthesia. The I-gel mask was placed for mechanical ventilation to maintain PETCO2 at 35‒45 mmHg. 2.5mg/L, remifentanil TCI (Ce2.5‒4ng/L), inhalation of 1‒1.5% sevoflurane, BIS of 40‒60. Moreover, continuous pumping of phenylephrine to maintain systolic blood pressure >140 mmHg, supplementation of crystalloids according to ABP, bleeding, and urine output was ensured. Ondansetron (8 mg) was used to prevent postoperative nausea and vomiting. After surgery, the analgesic pump was connected to perform patient-controlled analgesia (PCA). Sufentanil 2ug/kg was diluted to 100 mL with saline, and the first dose was 4 mL. The background infusion rate was 1 mL/h, the PCA dose was 4 mL, and the lock time was 20 min. If the patient complains of inadequate PCA analgesia and the VAS score is >4, accordingly, the nurse can press the PCA once (4mL) and record. In case of the pain was still not relieved, flurbiprofen axetil (50 mg) is administered intravenously for pain rescue. The anesthesiologist, surgeon, recovery room nurse or follow-up coordinator were blinded to the PSQ results.
Pain Sensitivity Questionnaire
Before measuring PSQ scores, choose an examination room with an area of 8 square meters, a quiet and enclosed environment, and maintain a room temperature of 20–25 °C (68–77 °F). This procedure was completed by a specific research coordinator. First, explain to the kidney donors the purpose of this experiment and the non-invasive nature of the test, in order to relieve their anxiety. The measurement time of PSQ lasts 10 minutes.
The preoperative PSQ scores were recorded. The Chinese version of PSQ5 was completed by the patient independently or with the assistance of a researcher in a quiet, separate room the day before the operation.
An individual’s pain sensitivity is assessed by imagining specific scenarios in life and scoring the pain. The scale consists of 17 entries; of these, 3 are pain-free items and 14 items are related to pain that includes different types of pain and pain intensity levels14 (Figure 1). Higher scores indicate greater sensitivity to painful stimuli. The mean PSQ-mean of the 14 pain items calculated from the PSQ score was divided into two groups, a low PSQ group with PSQ < 6.5 and a high PSQ group with a PSQ ≥ 6.5, according to the overall median PSQ-mean of the study. All patients were recorded as overall.
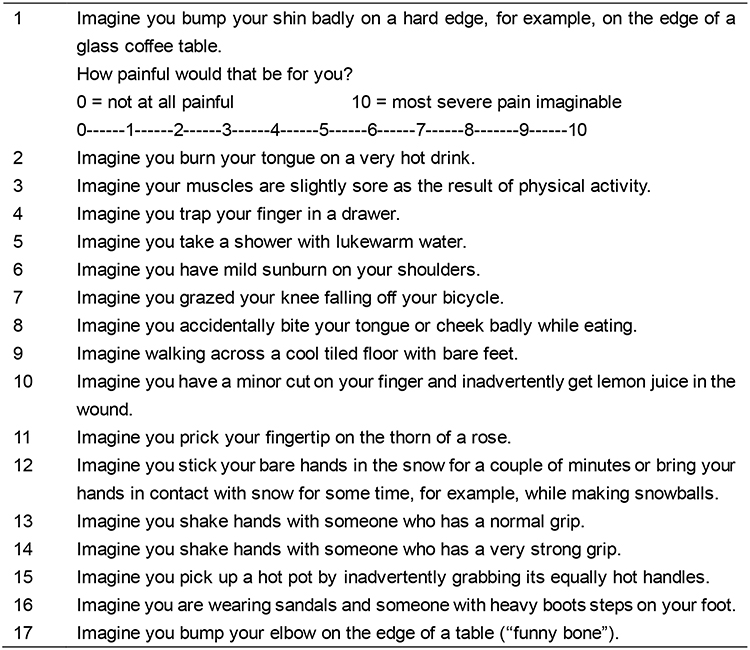 |
Figure 1 Pain sensitivity questionnaire. Patients are asked to rate how painful each situation would be from 0 (not painful at all) to 10 (most severe pain imaginable). The scale consists of 17 entries. 3 items (5, 9, 13) describe situations that are normally not rated as painful by healthy individuals and do not form part of the final score. Of these, 14 items are related to pain that includes different types of pain and pain intensity levels. The final PSQ score is calculated as the average rating of items from the questionnaire. |
Quantitative Sensory Testing
Measure QST value in the same environment as measuring PSQ scores. A Pinprick pain detector (MRC SYSTEM pain meter, Germany) was used by the research coordinator to measure the QST value. The Pinprick pain detector has a total of 7 weights, namely 8, 16, 32, 64, 128, 256, and 512N. Select the patient’s forearms and measure them 10cm below the palmar elbow on both sides, in descending order of severity. If the patient has already felt pain at the lightest 8N, it is considered that the patient’s pain threshold value is 4N. If the patient still does not feel pain at the heaviest 512N, it is considered that the patient’s pain threshold value is 1024N. Record the QST value at five painful and non-painful times. The measurement time lasts 10 minutes. The arithmetic mean was determined as the patient’s mechanical pain threshold.15,16
The number of effective PCA and flurbiprofen axetil remedial analgesia rates in the kidney donors for 48 h after surgery were recorded, and VAS scores at rest on the first postoperative day (POD 1), third postoperative day (POD 3), and seventh postoperative day (POD 7) were determined. Three months after discharged, Neuropathic Pain Assessment Scale (Douleur Neuropathique 4 Questions, DN4) was recorded by telephone follow-up. The DN4 is composed of nine questions, total score 0‒9, with > 4 scores as positive. The occurrence of chronic pain was recorded, and a score greater than 0 indicated the presence of chronic pain.
Statistical Analysis
SPSS 27.0 was used for analysis. Normal distribution data were expressed as mean ± standard deviation (SD). Non-normally distributed data were expressed as the median and interquartile range (IQR). The χ2 test was used to compare the count data. Pearson correlation analysis was used for normally distributed data, and Spearman correlation analysis was used for non-normally distributed data. P < 0.05 was considered statistically significant.
Results
Cohort Characteristics
A total of 148 relative living-related kidney transplant donors were included in this study and their clinical characteristics are shown in Table 1. Six cases did not meet the inclusion criteria, and two patients were re-operated within 3 months. Further, one patient was transferred to the ICU after surgery, five patients were excluded due to incomplete follow-up data, and six patients refused to be enrolled in the trial. Finally, 148 patients were enrolled, including 76 cases in PSQ < 6.5 group and 72 cases in the PSQ ≥ 6.5 group (Figure 2).
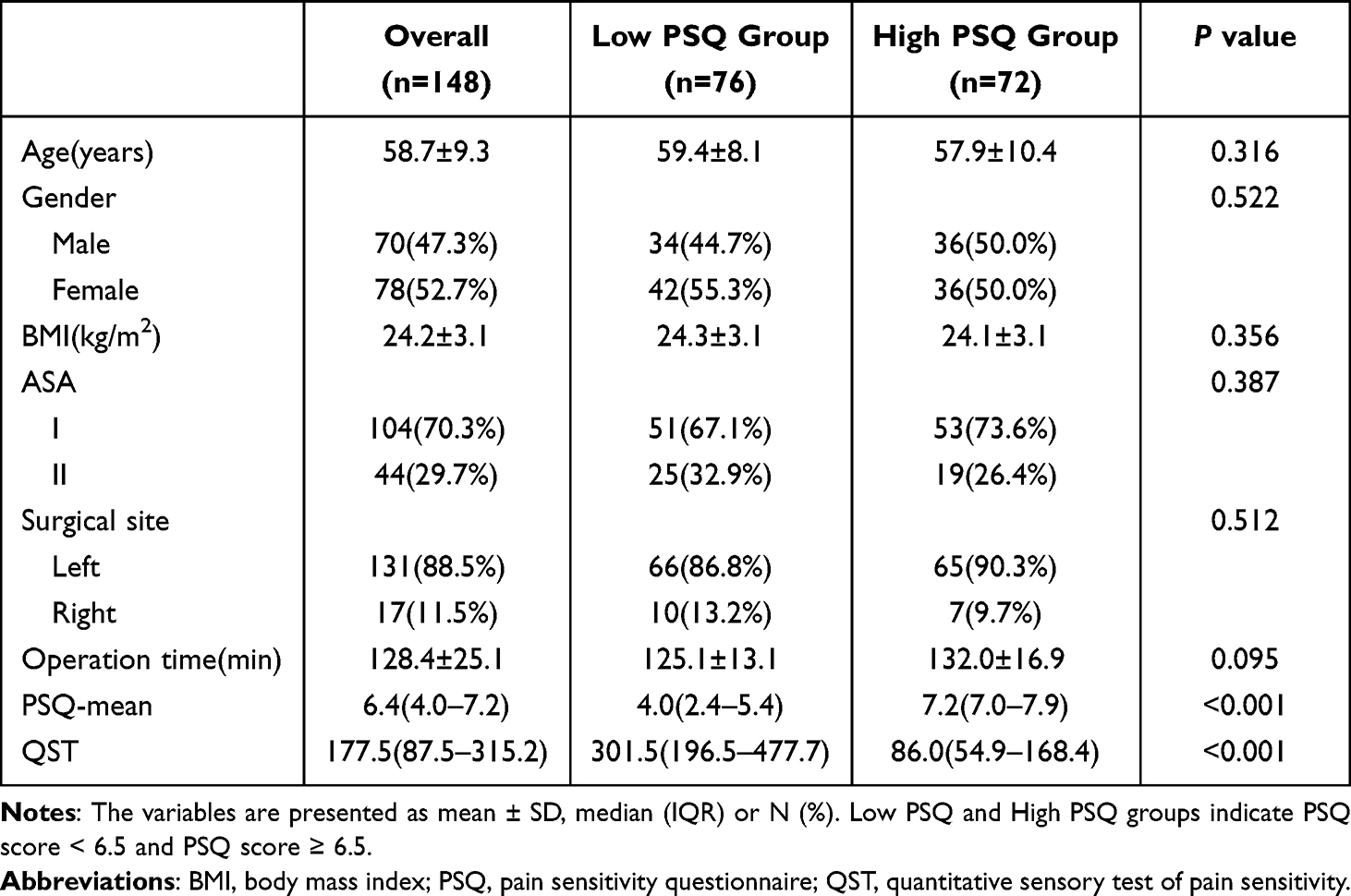 |
Table 1 Patient Demographic and Operative Characteristics |
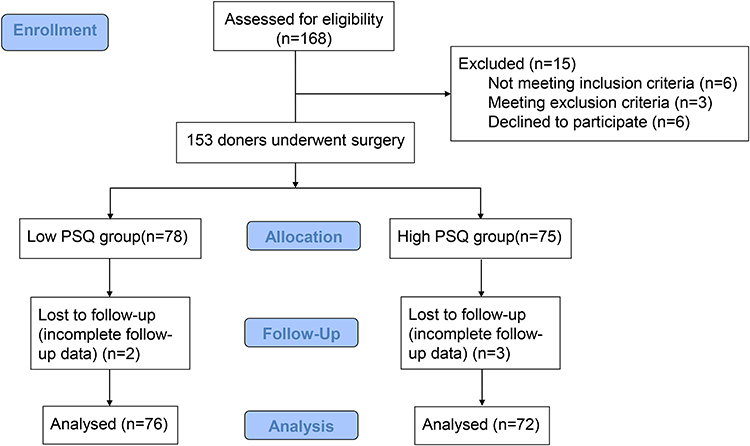 |
Figure 2 Flowchart of clinical procedures for the study. |
Patient Features
The general data of the patients are shown in Table 1. Overall, the mean (SD) age was 58.7±9.3 years old, the mean (SD) BMI was 24.2±3.1 kg/cm2, the average operation time was 128.4±25.1 minutes, the median (IQR) PSQ-mean was 6.4 (4.0–7.2) and the median (IQR) QST was 177.5 (87.5–315.2). The number of male subject was 70 (47.3%), 131 (88.5%) patients underwent left nephrectomy, and 104 (70.3%) patients was ASA grade I (Table 1). Age, gender, BMI, surgical location, and time of surgery were not statistically significant in both groups (P > 0.05). The preoperative PSQ-mean was 4.0 (2.4‒5.4) in the low PSQ group and 7.2 (7.0‒7.9) in the high PSQ group, and the difference was statistically significant (P < 0.0001). The preoperative QST was 301.5 (196.5‒477.7) in the low PSQ group and 86.0 (54.9‒168.4) in the high PSQ group, and the difference was statistically significant (P < 0.0001).
Differences Between PSQ Groups
The number of PCA was significantly lower in the low PSQ group than that in the high PSQ group, and the difference was statistically significant (P < 0.0001). The incidence of acute pain was 75% in the low PSQ and 100% in the high PSQ group (P < 0.0001). The flurbiprofen axetil remediation rate was lower in the low PSQ group (21.1%) than that in the high PSQ group (36.1%) (P = 0.042). The incidence of chronic pain was significantly lower in the low PSQ group (6.6%) than that in the high PSQ group (61.1%) (P < 0.001) (Table 2).
 |
Table 2 Postoperative Pain and Remediation Indicators |
As well as DN4, the low PSQ group was significantly lower than the high PSQ group, with a statistically significant difference (P < 0.001) (Table 2). VAS scores at rest on the first, third, and seventh day after donor surgery were statistically lower in the low PSQ group than that in the high PSQ group (P<0.001; P = 0.031 and P = 0.027, respectively) (Table 3).
 |
Table 3 VAS on Postoperative Days 1, 3, and 7 |
Correlation Between PSQ and QST
The PSQ-mean in the overall group of kidney donors was significantly negatively correlated with QST (r = −0.88, P < 0.0001) (Figure 3A). Similarly, the PSQ-mean in the low PSQ group of kidney donors was significantly negatively correlated with QST (r = −0.74, P < 0.0001) (Figure 3B). The PSQ-mean in the high PSQ group of kidney donors was also significantly negatively correlated with QST (r = −0.72, P < 0.0001) (Figure 3C).
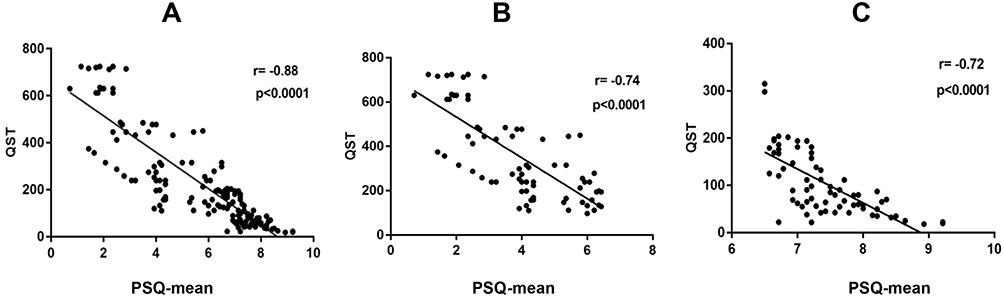 |
Figure 3 Illustration of the correlations between PSQ scores and QST. Linear regression lines are displayed. (A) The PSQ-mean in the overall group of kidney donors was significantly negatively correlated with QST (r = −0.88, P < 0.0001). (B) The PSQ-mean in the low PSQ group of kidney donors was significantly negatively correlated with QST (r = −0.74, P < 0.0001). (C) The PSQ-mean in the high PSQ group of kidney donors was also significantly negatively correlated with QST (r = −0.72, P < 0.0001). |
Discussion
In this prospective cohort study, the high PSQ group had more times of PCA compressions as compared to the low PSQ group. Moreover, the high PSQ group had higher postoperative rest pain on POD 1, 3, and 7. Further, it was noted that PSQ had a significant negative correlation with QST in living-related kidney transplant donors, indicating that PSQ could predict postoperative pain in living-related kidney transplant donors.
In our study, we found that PSQ could predict acute postoperative pain in living kidney donors, which corroborated with a previous clinical study.17 The difference between the two studies is that we adopted the median PSQ (6.5) for the grouping criteria while calculating their study’s cutoff value of PSQ (5.0).
While considering kidney donation, candidates should be aware of personal long-term risks based on the demographics and any other risks that may be attributed to kidney donation, such as hypertension and other health outcomes as well as short-term and long-term pain.18 In this study, we aimed to find a simple, economical, and robust pain sensitivity measurement method for kidney donation operation. Notably, PSQ is not related to kidney donors’ characteristics, such as age, gender, BMI, ASA, surgical site, or operation time.
In this study, we proved the effectiveness of PSQ in evaluating postoperative pain of kidney donors using various indicators of pain measurement, including the number of PCA, acute pain incidence, flurbiprofen remediation incidence, chronic pain incidence, and DN4. The values of all these indicators increased as the PSQ score increased. The number of PCA may increase as kidney donors experience pain. When PCA is not effective enough to relieve the pain, a second analgesic such as flurbiprofen could alleviate the effect of formalin-induced inflammatory pain.19 Flurbiprofen axetil enhances the analgesic effect of sufentanil, reduce inflammatory reactions, and alleviate visceral pain.20 Therefore, flurbiprofen axetil was used as an analgesic remedy in this study. DN4, which measured neuropathic pain using an assessment scale with nine questions,21 was used to assess the degree of long-term pain 3 months after surgery. These results indicated that PSQ is not only applicable for the evaluation of acute pain after the kidney donor operation but also for the evaluation of chronic pain after the operation.
Visual analog scale (VAS) is widely used for pain assessment in China.22 A higher VAS score corresponds to more intense pain. The VAS score on postoperative day 1, 3 and 7 supported our findings that PSQ was a good tool for assessing the pain of living kidney donors. The difference in VAS scores between the low and high PSQ groups on postoperative days 3 and 7 was significant. This is consistent with previous study23 that donors with high PSQ may have higher VAS after surgery.
Compared with the aforementioned pain sensitivity accessing tools, QST is a relatively objective indicator of the pain sensitivity accessing method. QST is not the routinely used in the management of living kidney donors. However, QST provides an objective numerical value. The results of this study show that PSQ and QST scores are highly correlated, both in the low and high PSQ groups. Similar findings have been observed in women with persistent pelvic pain.4 We further confirmed this relationship in kidney donors.
Notably, psychosomatic factors have a complex effect on pain. They may alter pain responses at the molecular and behavioral levels,24 with anxiety and depression having the most significant impact on pain sensitivity. Some studies have shown that living kidney donors are more prone to anxiety and depression.25,26 Hermesdorf et al27 compared the differences in sensitivity to stress pain and PSQ between depressed patients and healthy volunteers. They found that the pain thresholds for stress pain in depressed patients were reduced and were associated with related subjective factors. Anxiety is defined as the apprehensive anticipation of a potential threat. It is characterized by negative emotions, which result in increased attention to the environment and somatic concerns and divert attention from pain processing. Thus the pain threshold is lowered, leading to increased pain sensitivity.28 Elevated pain sensitivity is a risk factor for the development of chronic pain,29 leading to a high prevalence of pain in depressed patients. Furthermore, pain leads to depression30 with pain and depression exacerbating each other. In this study, kidney donors with high PSQ are more likely to have higher pain sensitivity, indicating that kidney donors may be more prone to anxiety and depression. Based on the results of this study, PSQ questionnaire might be used in the future identify patients who were sensitive to postoperative pain in an early stage, so as to give timely intervention, including psychological counseling and preparation of analgesic drugs, to reduce the occurrence of anxiety and depression.
Kidney donors experienced postoperative acute pain from surgery that hindered recovery and created anxiety and fear in some.31,32 Furthermore, the incidence of chronic pain after donor nephrectomy was underestimated.33 Given the voluntary and benefits of living-kidney transplantation, and complications caused by postoperative pain, anesthesiologists should be more aware of perioperative pain management strategies. Those involved with the preparation and post-operative management could use PSQ in predicting postoperative pain and guiding pain management strategies for living kidney donors in the future.
The advantage of this study is that it was designed as a prospective controlled study. There was no significant difference in the demographic and surgical site in kidney donors between the low and high PSQ groups. Another advantage is that the follow-up was completed by independent observers. Finally, the study used multiple pain assessment indicators to evaluate the effect of PSQ scores on accessing the pain sensitivity of kidney donors after surgery.
There are several limitations to our study. Firstly, the enrolled patients were categorized according to a total PSQ score of 6.5 which was determined based on the median total PSQ score, since there are no reference criteria for total PSQ scores for the low and high PSQ groups. Therefore, this value does not represent a cutoff for favorable outcomes after surgery for nephrectomy. Secondly, considering that too many questionnaires may affect the survey results of kidney donors, we did not collect anxiety and depression related data from kidney donors. Anxiety and depression may affect the pain sensitivity of kidney donors. Thirdly, this observational study cannot establish a causal relationship between PSQ and postoperative pain. Fourthly, the results of PSQ may be influenced by some potential confounding factors, such as educational level, this study did not perform such corrections although no significant relationship was found between PSQ and kidney donors’ characteristics in this study. Finally, PSQ is a self-assessment questionnaire with strong subjectivity. The effect of PSQ in evaluating long-term postoperative pain in kidney donors or any surgical patients suffering from severe trauma requires further prospective cohort studies in large samples. Furthermore, future directions require evaluating the long-term impact of PSQ on pain management outcomes and exploring its utility in different surgical populations.
Conclusions
The PSQ was found to be associated with the intensity or postoperative pain and might be used to screen patients prior to living-kidney transplantation.
Data Sharing Statement
The data presented in this study are available on reasonable request from the corresponding author.
Acknowledgments
The authors thank all the participants of the study, including patients and our colleagues.
Funding
This study was funded by the Natural Science Foundation of Anhui Province (grant no. 2108085MH323).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kim HJ, Lee JI, Kang KT, et al. Influence of pain sensitivity on surgical outcomes after lumbar spine surgery in patients with lumbar spinal stenosis. Spine. 2015;40(3):193–200. doi:10.1097/brs.0000000000000699
2. Bushnell MC, Ceko M, Low LA. Cognitive and emotional control of pain and its disruption in chronic pain. Nat Rev Neurosci. 2013;14(7):502–511. doi:10.1038/nrn3516
3. Andersen MH, Mathisen L, Oyen O, et al. Postoperative pain and convalescence in living kidney donors-laparoscopic versus open donor nephrectomy: a randomized study. Am J Transplant. 2006;6(6):1438–1443. doi:10.1111/j.1600-6143.2006.01301.x
4. Grundström H, Larsson B, Arendt-Nielsen L, et al. Associations between pain thresholds for heat, cold and pressure, and Pain Sensitivity Questionnaire scores in healthy women and in women with persistent pelvic pain. Eur J Pain. 2019;23(9):1631–1639. doi:10.1002/ejp.1439
5. Quan X, Fong DYT, Leung AYM, et al. Validation of the Mandarin Chinese version of the pain sensitivity questionnaire. Pain Pract. 2018;18(2):180–193. doi:10.1111/papr.12587
6. Ibancos-Losada MDR, Osuna-Pérez MC, Cortés-Pérez I, et al. Validation and cross-cultural adaptation of the Spanish version of the pain sensitivity questionnaire (PSQ-S). J Clin Med. 2021;11(1):151. doi:10.3390/jcm11010151
7. Granot M, Srulovici E, Granovsky Y, et al. Dispositional and situational personal features and acute post-collision head and neck pain: double mediation of pain catastrophizing and pain sensitivity. PLoS One. 2022;17(1):e0262076. doi:10.1371/journal.pone.0262076
8. Inal FY, Gul K, Yilmaz Camgoz Y, et al. Validation of the Turkish version of the pain sensitivity questionnaire in patients with chronic pain. J Int Med Res. 2021;49(12):3000605211060158. doi:10.1177/03000605211060158
9. Yilmaz Inal F, Yilmaz Camgoz Y, Daskaya H, et al. The effect of preoperative anxiety and pain sensitivity on preoperative hemodynamics, propofol consumption, and postoperative recovery and pain in endoscopic ultrasonography. Pain Ther. 2021;10(2):1283–1293. doi:10.1007/s40122-021-00292-7
10. Tuna T, Van Obbergh L, Van Cutsem N, et al. Usefulness of the pain sensitivity questionnaire to discriminate the pain behaviour of chronic pain patients. Br J Anaesth. 2018;121(3):616–622. doi:10.1016/j.bja.2018.04.042
11. Van Boekel RLM, Timmerman H, Bronkhorst EM, et al. Translation, cross-cultural adaptation, and validation of the pain sensitivity questionnaire in Dutch healthy volunteers. Pain Res Manag. 2020;2020:1050935. doi:10.1155/2020/1050935
12. Palzer EF, Helgeson ES, Evans MD, et al. Long-term outcomes associated with post-kidney donation pregnancy complications. Transplantation. 2023;107:1615–1623. doi:10.1097/tp.0000000000004540
13. Chen Y, Ahn JB, Bae S, et al. Gabapentin, concomitant prescription of opioids, and benzodiazepines among kidney transplant recipients. Clin J Am Soc Nephrol. 2023;18(1):91–98. doi:10.2215/cjn.0000000000000019
14. Ruscheweyh R, Marziniak M, Stumpenhorst F, et al. Pain sensitivity can be assessed by self-rating: development and validation of the pain sensitivity questionnaire. Pain. 2009;146(1–2):65–74. doi:10.1016/j.pain.2009.06.020
15. Vadivelu N, Kai AM, Kodumudi G, et al. Pain and psychology-A reciprocal relationship. Ochsner J. 2017;17(2):173–180. doi:10.1016/j.jad.2010.10.022
16. van den Broeke EN, Lambert J, Huang G, et al. Central sensitization of mechanical nociceptive pathways is associated with a long-lasting increase of pinprick-evoked brain potentials. Front Hum Neurosci. 2016;10:531. doi:10.3389/fnhum.2016.00531
17. Yaari L, Dolev A, Kittani M, et al. Preoperative pain sensitivity questionnaire helps customize pain management after arthroscopic partial meniscectomy. Knee Surg Sports Traumatol Arthrosc. 2021;29(12):4198–4204. doi:10.1007/s00167-021-06438-6
18. Garg AX, Arnold JB, Cuerden M, et al. The living kidney donor safety study: protocol of a prospective cohort study. Can J Kidney Health Dis. 2022;9:20543581221129442. doi:10.1177/20543581221129442
19. Huang L, Zheng X, Zhang Y, et al. Flurbiprofen axetil alleviates the effect of formalin-induced inflammatory pain on the cognitive function of rats with mild cognitive impairment through the AMPKα/NF-κB signaling pathway. Ann Transl Med. 2022;10(22):1210. doi:10.21037/atm-22-4997
20. Geng W, Hong W, Wang J, et al. Flurbiprofen axetil enhances analgesic effects of sufentanil and attenuates postoperative emergence agitation and systemic proinflammation in patients undergoing tangential excision surgery. Mediators Inflamm. 2015;2015:601083. doi:10.1155/2015/601083
21. Galiero R, Salvatore T, Ferrara R, et al. The role of neuropathy screening tools in patients affected by fibromyalgia. J Clin Med. 2022;11(6):1533. doi:10.3390/jcm11061533
22. Gonai S, Yoneoka D, Miyoshi T, et al. A systematic review with pairwise and network meta-analysis of closed reduction methods for anterior shoulder dislocation. Ann Emerg Med. 2023;81(4):453–465. doi:10.1016/j.annemergmed.2022.10.020
23. Kadum B, Inngul C, Ihrman R, et al. Higher preoperative sensitivity to pain and pain at rest are associated with worse functional outcome after stemless total shoulder arthroplasty: a prospective cohort study. Bone Joint J. 2018;100(4):480–484. doi:10.1302/0301-620x.100b4.Bjj-2017-1000.R1
24. Salberg S, Noel M, Burke NN, et al. Utilization of a rodent model to examine the neurological effects of early life adversity on adolescent pain sensitivity. Dev Psychobiol. 2020;62(3):386–399. doi:10.1002/dev.21922
25. Pawłowski M, Fila-Witecka K, Rymaszewska JE, et al. Quality of life, depression and anxiety in living donor kidney transplantation. Transplant Rev. 2020;34(4):100572. doi:10.1016/j.trre.2020.100572
26. Holscher CM, Leanza J, Thomas AG, et al. Anxiety, depression, and regret of donation in living kidney donors. BMC Nephrol. 2018;19(1):218. doi:10.1186/s12882-018-1024-0
27. Hermesdorf M, Berger K, Baune BT, et al. Pain sensitivity in patients with major depression: differential effect of pain sensitivity measures, somatic cofactors, and disease characteristics. J Pain. 2016;17(5):606–616. doi:10.1016/j.jpain.2016.01.474
28. Rhudy JL, Meagher MW. Fear and anxiety: divergent effects on human pain thresholds. Pain. 2000;84(1):65–75. doi:10.1016/s0304-3959(99)00183-9
29. Staud R. Abnormal endogenous pain modulation is a shared characteristic of many chronic pain conditions. Expert Rev Neurother. 2012;12(5):577–585. doi:10.1586/ern.12.41
30. Walker AK, Kavelaars A, Heijnen CJ, et al. Neuroinflammation and comorbidity of pain and depression. Pharmacol Rev. 2014;66(1):80–101. doi:10.1124/pr.113.008144
31. Dreesmann NJ, Jung W, Shebaili M, et al. Kidney donor perspectives on acute postoperative pain management. Clin Nurs Res. 2023:10547738231156151. doi:10.1177/10547738231156151
32. Fleishman A, Khwaja K, Schold JD, et al. Pain expectancy, prevalence, severity, and patterns following donor nephrectomy: findings from the KDOC Study. Am J Transplant. 2020;20(9):2522–2529. doi:10.1111/ajt.15861
33. Owen M, Lorgelly P, Serpell M. Chronic pain following donor nephrectomy--A study of the incidence, nature and impact of chronic post-nephrectomy pain. Eur J Pain. 2010;14(7):732–734. doi:10.1016/j.ejpain.2009.11.013
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.