")
Back to Journals » International Journal of General Medicine » Volume 16
The Value of Immunocytochemical Staining for the HPV E7 Protein in the Diagnosis of Cervical Lesions
Authors Fei M, Yu Y, Hu X, Xu H, Liu F
Received 26 December 2022
Accepted for publication 10 March 2023
Published 24 March 2023 Volume 2023:16 Pages 1081—1089
DOI https://doi.org/10.2147/IJGM.S402759
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mingjian Fei,1 Yawei Yu,1 Xiaolan Hu,1 Haimiao Xu,2 Fang Liu3
1Department of Pathology, The Second Affiliated Hospital of Jiaxing University, Jiaxing, Zhejiang, People’s Republic of China; 2Department of Pathology, Zhejiang Provincial People’s Hospital, Hangzhou, Zhejiang, People’s Republic of China; 3Department of Gynecology, The Second Affiliated Hospital of Jiaxing University, Jiaxing, Zhejiang, People’s Republic of China
Correspondence: Mingjian Fei, Department of Pathology, The Second Hospital of Jiaxing, 1518 Huanchen North Road, Jiaxing, Zhejiang, 314000, People’s Republic of China, Email [email protected]
Purpose: To investigate the value of immunocytochemical (ICC) staining for human papillomavirus (HPV) E7 protein (E7-ICC staining) as a new-generation immunological method in the cytological diagnosis of cervical lesions.
Methods: The exfoliated cervical cell samples of 690 women were subjected to a liquid-based cytology test (LCT), high-risk HPV (HR-HPV) test, E7-ICC staining, and cervical biopsy for pathological diagnosis.
Results: E7-ICC staining as a preliminary screening scheme for cervical precancerous lesions was comparable to the HR-HPV test in sensitivity and to the LCT in specificity. E7-ICC staining was advantageous in facilitating the secondary triage of HR-HPV-positive patients; therefore, this method can be used as an auxiliary scheme to routine LCT for diagnostic grading to improve the accuracy of cervical cytology.
Conclusion: E7-ICC staining as a primary or auxiliary cytological screening scheme can effectively reduce the colposcopy referral rate.
Keywords: cervical cancer, early screening for cervical cancer, cervical intraepithelial neoplasia, immunohistochemistry, HPV, E7 oncoprotein
Cervical cancer is a major threat to women’s health worldwide, with more than 500,000 new cases every year.1 The commonly used cervical cancer screening methods mainly include the liquid-based cytology test (LCT), the human papillomavirus (HPV) test, and the combined use of the two.2 LCT is less sensitive and is affected by the subjective judgement of the physician, while the HPV test lacks specificity, which may lead to unnecessary colposcopy referral and excessive intervention, increase the cost of public health and cause anxiety in high-risk HPV (HR-HPV) positive women.3 The HPV E6 and E7 viral oncoproteins play a key role in driving cell carcinogenesis. In the process of viral genome replication, they can induce all the characteristics of cancer cells, including uncontrolled proliferation, angiogenesis, invasion, metastasis, unrestricted telomerase activity, and evasion of apoptosis and growth suppressors.4
E7 was the first oncogene to be discovered in HPV. E7 is a relatively small phosphoprotein with approximately 100 amino acids and three conserved regions, CR1, CR2, and CR3. A small portion of CR1 at the amino-terminus and almost all of CR2 have sequence similarity with the adenovirus (Ad) E1A protein and the large T antigen of SV40.5 CR2 is composed of poorly conserved sequences. CR3, at the carboxyl-terminus, is a conserved region that encodes a zinc finger domain, which contains two CXXC motifs separated by 29 amino acid residues.6 This region is responsible for zinc-dependent dimerization and mediates the interaction between E7 and cellular proteins responsible for cell cycle regulation and apoptosis (p21 and retinoblastoma protein (pRb)).7 E7-mediated inhibition of pRb is an important step to achieve unrestricted cell proliferation. Cells pass through the mandatory checkpoints from G1 to S phase to allow the pRb–E2F interaction. Before the cells enter S phase, pRb still binds to the E2F transcription factors to prevent them from transcribing the genes required for transition to S phase. In HPV-infected cells, E7 targets pRb for ubiquitination, resulting in the release of E2F transcription factors, which are transcribed to form cyclin E, cyclin A, and p16INK4A (cyclin-dependent kinase (CDK)4/6 inhibitor), causing premature transition of cells to S phase.8
The CDK inhibitor p16INK4A (tumour suppressor protein) is an important target of HPV E7 in cell cycle regulation. The HPV E7 protein not only allows the expression of p16INK4A through pRb disintegration but also epigenetic changes in KDM6B.9 Therefore, the protein encoded by the HR-HPV E7 gene is an important factor leading to the carcinogenesis of cervical epithelial tissue.10 Overexpression of E7 protein is a marker of HR-HPV integration, oncogene expression, and precancerous lesion status.11 Therefore, immunocytochemical (ICC) staining for the E7 oncoprotein with the monoclonal antibody developed for E7 can become a new-generation cervical cytology method that can help optimize the strategy of cervical cancer screening.
This study used a large sample of a natural population to evaluate the value of ICC staining for the E7 protein (referred to as E7-ICC staining) as a preliminary screening method for cervical precancerous lesions and as an auxiliary method for preliminary screening for cervical lesions with LCT or HR-HPV test.
Materials and Methods
Data Sources
Research Sample
The data were collected from 4088 20- to 70-year-old non-pregnant women treated in the gynaecological clinic of the Second Hospital of Jiaxing from November 2020 to October 2021. They had a history of sexual intercourse, no history of cervical cancer or precancerous lesions, and no history of cervical surgery. E7-ICC staining, LCT, and the HR-HPV test were used for screening for cervical cancer. The screening results were collected, and pathological examinations of cervix tissue were performed using the three-step criteria. This study was approved by the Ethics Committee of the Second Hospital of Jiaxing (JXEY-ZFYJ047), which accorded with the ethical standards formulated in the Helsinki Declaration. All subjects signed informed consent forms. A written consent from the patient was obtained prior to collecting the case material and accompanying images, operating histopathological biopsy, writing the final manuscript and publishing the case report.
Main Reagents
Cell preservation solution for LCT, Papanicolaou staining solution, cell preservation solution for cytological staining of E7, and an E7-ICC staining kit were purchased from Attobio (Suzhou) (monoclonal antibody, DAB staining solution, immune chromogenic reagent, etc.). The cervista HR-HPV test kit (Hologic, USA) was a type 2+ type 14 separate detection kit.
Collection and Detection of Exfoliated Cervical Cells
Collection of Cervical Exfoliated Cells
All subjects were recruited by physicians in our hospital. The physicians used a speculum to expose the cervix, removed the cervical surface secretions, placed a cytobrush into the cervical canal, turned the cytobrush for several rounds, took the cytobrush out, and placed the brush head and the cells attached on it in the cell preservation solution. The collected cell samples were used for LCT and HR-HPV test. The cells collected for LCT and E7-ICC staining were stored in the same preservation solution and randomized for LCT or E7-ICC staining.
LCT
The thin smear for LCT was prepared using the automatic liquid-based cell preparation system. According to the criteria of the Bethesda classification system for cervical cytology, the results were interpreted as negative for intraepithelial lesion or malignancy (NILM), atypical squamous cells of undetermined significance (ASCUS), atypical squamous cells when high-grade squamous intraepithelial lesions could not be ruled out (ASC-H), low-grade squamous intraepithelial lesions (LSILs), or high-grade squamous intraepithelial lesions (HSILs).
HR-HPV Test
An HPV nucleic acid detection kit was used to determine the HPV types, including HPV16, HPV18, and other 12 subtypes of HR-HPV (31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68).
E7-ICC Staining
Among the 4088 women screened in this study, 419 received both an HR-HPV test and E7-ICC staining, which were done on one of the two samples of exfoliated cervical cells that were collected in the clinic and stored separately in the cell preservation solution. The sampling for LCT and the E7-ICC staining were performed alternately with the same sampling method and by the same sampler whenever possible (to minimize the influence of sampling error on the results). The women with positive HR-HPV or LCT screening results out of the other 3669 women were called for colposcopy to collect exfoliated cervical cells for E7-ICC staining.
E7-ICC staining procedure: (1) The specimens stored in the E7-stained cell preservation solution were prepared using an automatic liquid-based cell preparation machine to prepare thin-cell slices (unstained cell slices). No Pap smear was performed. (2) E7-ICC staining was performed using an automatic immunohistochemical staining machine. The procedures included antigen retrieval, incubation with primary and secondary antibodies, and 3,3′-diaminobenzidine (DAB) and haematoxylin chromogenesis. The E7-ICC staining results were interpreted by two senior cytological pathologists (one from the Second Hospital of Jiaxing and the other one from Suzhou Municipal Hospital) in a blinded manner. Cells with positive E7-ICC staining results were brown or tan, stained in the cytoplasm, and not stained in the nucleus. Under the microscope, if the cytoplasm of one or more cells was stained brown, the E7-ICC staining result was defined as E7-positive in Figure 1A, an E7-negative is defined in Figure 1B.
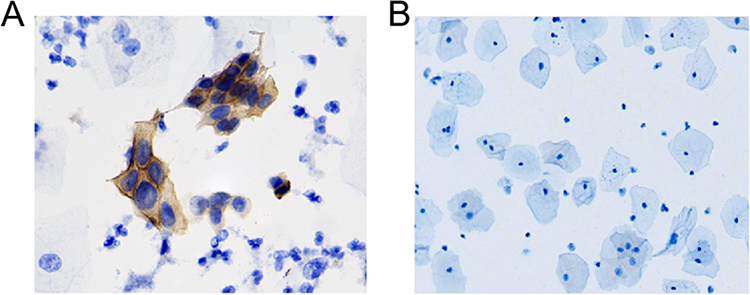 |
Figure 1 Immunocytochemical staining of E7 in exfoliated cervical cells (E7-ICC staining). (A) In an E7-positive result, the cytoplasm was stained brown; (B) In an E7-negative result, the nucleus and cytoplasm were bluish-purple without brown. E7-ICC staining ×20. |
The criteria for interpretation of positive E7-ICC staining results were as follows: brown staining in the cytoplasm of exfoliated cervical cells, significantly enlarged nuclei, and at least one of the following abnormal conditions: (1) nucleocytoplasmic ratio >1; (2) coarse and dark chromatin; and (3) irregularly shaped nuclei with small concave and convex grooves. The criteria for interpretation of negative E7-ICC staining results (non-specific stain) were as follows: blue and purple nuclei and cytoplasm without brown staining, or cells with brown E7 stains but without evident morphological change.
Colposcopy and Cervical Biopsy
Among the 4088 women undergoing preliminary screening for cervical cancer, 271 were called for colposcopy and tissue biopsy due to positive HR-HPV results, LCT results of LSIL or worse, or positive E7-ICC staining results in the preliminary screening. In the other 3817 cases, the patients positive for HPV16 and/or HPV18 or the other 12 HR-HPV subtypes and with an LCT result of ASCUS or worse or LCT results of LSIL or worse were called for colposcopy with cervical biopsy, which was performed by the following protocol: biopsy of visible lesions in the lower four quadrants + random biopsy of invisible lesions + endocervical curettage (Preventive Oncology International self-sampler).12 The histopathological results were classified into chronic cervical inflammation, LSIL, and HSIL. Cervical intraepithelial neoplasia (CIN) 1 was classified as LSIL, and CIN2 and 3 were classified as HSIL.
Cervical Cancer Screening Schemes
Preliminary screening: E7-ICC staining, HR-HPV nucleic acid test, or LCT alone was used as the preliminary screening scheme. Auxiliary screening: 1. LCT and E7-ICC staining were done together for screening, with E7-ICC staining to assist in the interpretation of the screening results. 2. HR-HPV test and E7-ICC staining were done together for screening, with E7-ICC staining to assist in the interpretation of the screening results.
Calculation Methods
Sensitivity (true-positive rate): Pathological diagnosis was used as the gold standard, and the pathological and screening results were both positive. Sensitivity is calculated as follows: sensitivity = number of true positives/(number of true positives + number of false negatives)×100%. Specificity (true-negative rate) refers to the proportion of disease-free cases diagnosed as disease-free according to the screening results. Specificity is calculated as: specificity = number of true negatives/(number of true negatives + number of false positives)×100%. Positive predictive value (PPV) = number of true positives/(number of true positives + number of false positives)×100%. Negative predictive value (NPV) = number of true negatives/(number of true negatives + number of false negatives)×100%. Accuracy = [(number of true positives + number of true negatives)/total number of cases]×100%. False-positive rate = number of false positives/(number of true negatives + number of false positives)×100%. Youden index = (sensitivity + specificity) − 1.
Statistics
The data collected in this study were analysed with SPSS 24.0 software. Patients with complete data of E7-ICC staining, the Bethesda System report of LCT, HR-HPV test, and pathological diagnosis via cervical biopsy were included in the statistical analysis. The diagnostic results from pathological sections prepared from biopsy samples were used as the gold standard to compare with the screening results based on E7-ICC staining, LCT, or HR-HPV alone. In addition, the efficiencies of E7-ICC staining plus LCT and of E7-ICC staining plus HR-HPV for detecting HSIL (CIN2+ and CIN3+) were assessed. The McNemar test was used to compare the screening efficiencies of different screening schemes. Count data are expressed as percentages and were compared by the χ2 test. P<0.05 was considered statistically significant.
Results
Overview of the data included in this screening study: Among the 4088 women who received preliminary screening, 690 patients with complete data from LCT, HR-HPV test, E7-ICC staining, and pathological diagnosis via cervical biopsy were included in this study. The age range of the 690 women was 43.1±6.8 years (20–73 years). Among them, 419 underwent E7-ICC staining during the preliminary screening through the HR-HPV test and LCT, and 271 with positive preliminary screening results were called for colposcopy to collect samples for E7-ICC staining. According to the pathological diagnostic results, there were 637 cases of normal cervix, 25 cases of LSIL (CIN1), 26 cases of HSIL (CIN2 and CIN3), and 2 cases of cervical cancer. There were 28 cases of HSIL (CIN2+, namely CIN2 and above), and 16 cases of HSIL (CIN3+, namely CIN3 and above). The screening schemes are shown in Figure 2, and the screening results are shown in Table 1.
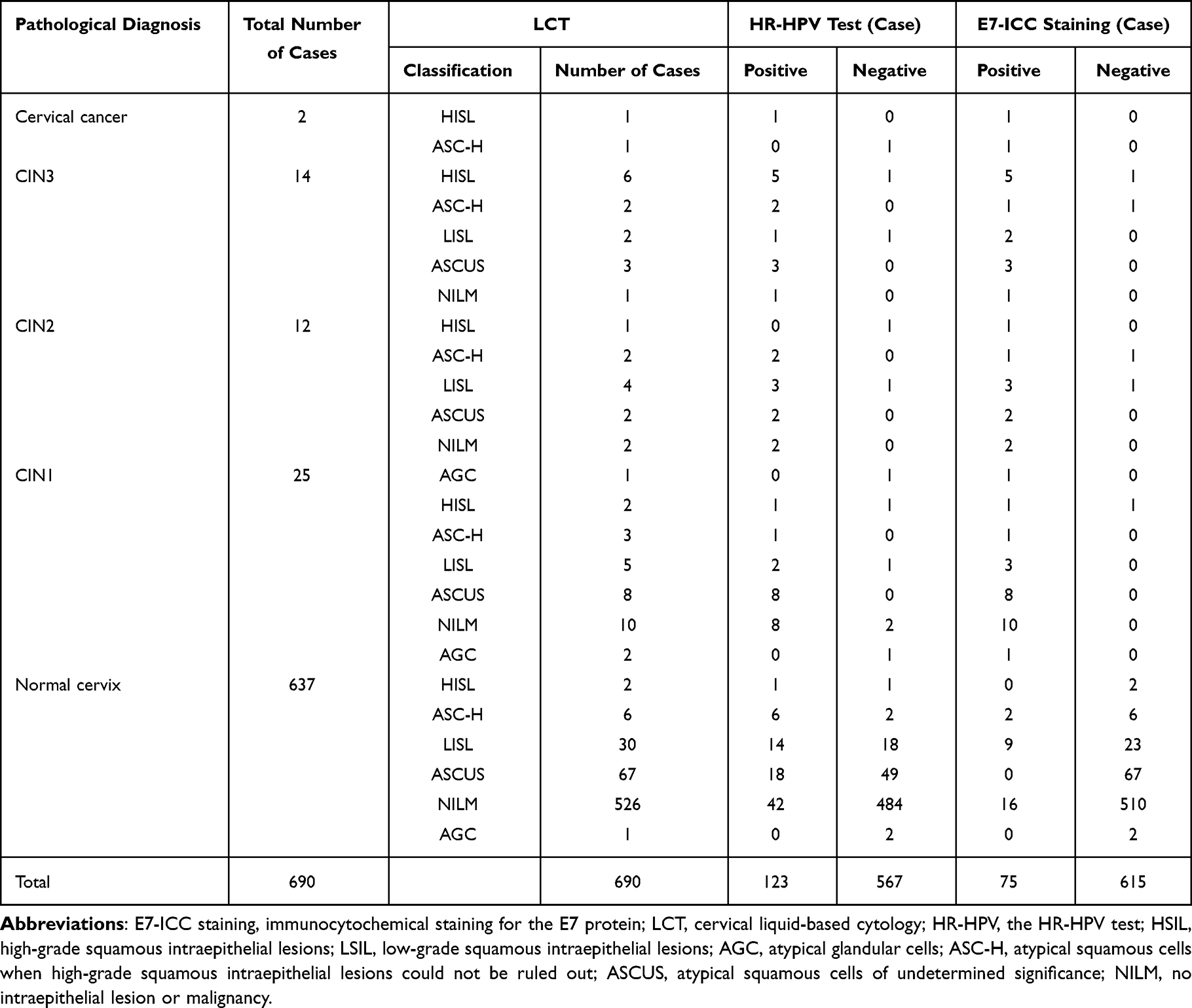 |
Table 1 Results of LCT, HR-HPV Test, and E7-ICC Staining of Women with Different Grades of Precancerous Lesions |
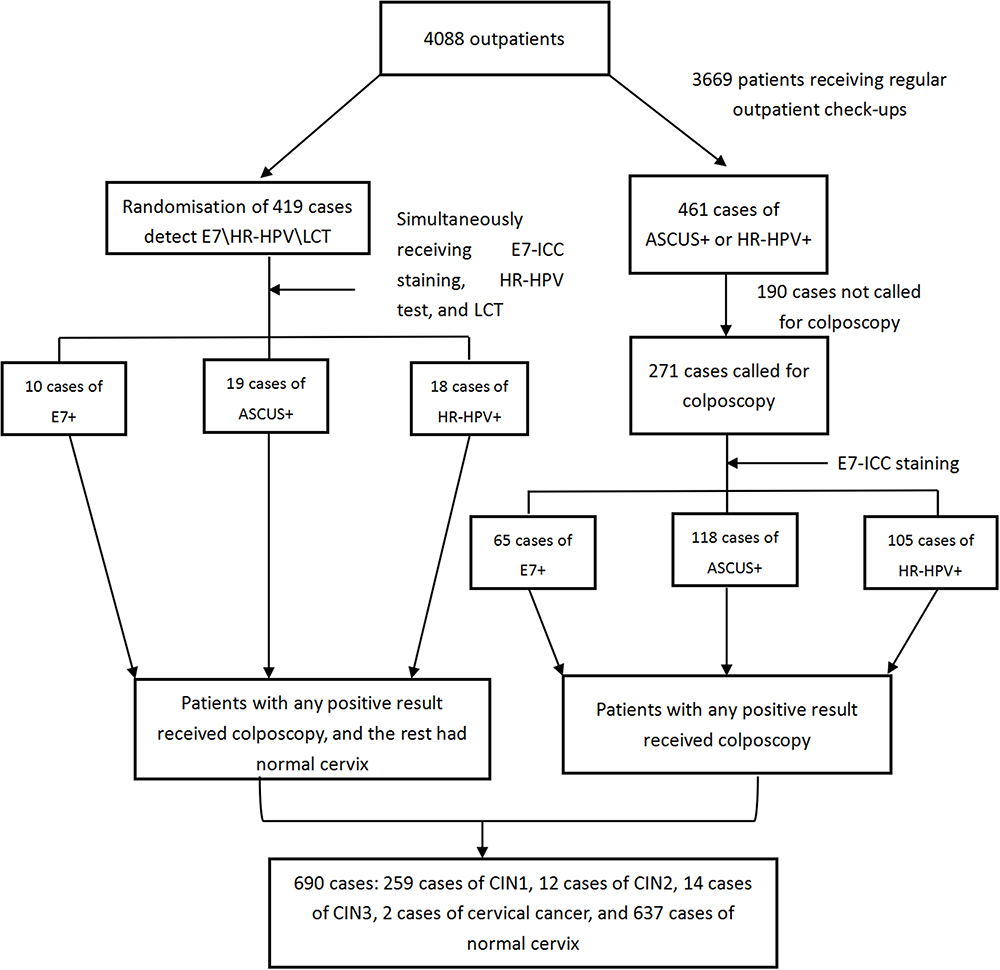 |
Figure 2 Flowchart of the screening protocol. |
Among the 14 women with a pathological diagnosis of CIN3, 6 (42.9%, 6/14) were diagnosed with HSIL by LCT, 12 (85.7%, 12/14) were HR-HPV-positive, and 12 (85.7%) were E7-positive. Three women diagnosed with ASCUS by LCT and two women diagnosed with LSIL by LCT were E7-positive. Among the 637 women with normal cervix diagnosed by pathological biopsy, 67 women diagnosed with ASCUS by LCT were E7-negative, and 23 out of 30 women diagnosed with LSIL by LCT were E7-negative. The E7-positive rate of the 16 patients with a pathological diagnosis of HSIL (CIN3+) was 87.5% (14/16), which was significantly higher than that (8.8%, 59/674) of the women pathologically diagnosed with CIN1 or normal cervix (χ2 = 304.5, P < 0.01), which is shown in Table 1.
Evaluation of the clinical screening performance of the HR-HPV test, LCT, or E7-ICC staining alone and their paired combinations for screening: Among 4088 women screened, 180 with positive screening results but no colposcopy were excluded. Eventually, 690 patients were included in the cervical cancer screen to compare the efficacy of different screening schemes. The sensitivities of E7-ICC staining, LCT, and the HR-HPV test in the diagnosis of CIN2 and CIN3 were 85.7%, 85.7%, and 78.6%, respectively, and the corresponding specificities were 92.3%, 81.4%, and 84.7%. The sensitivities of E7+LCT, HPV+LCT, and E7+HR-HPV were 71.4%, 67.9%, and 76.9%, respectively, with corresponding specificities of 96.4%, 92.3%, and 92.9% (Table 2).
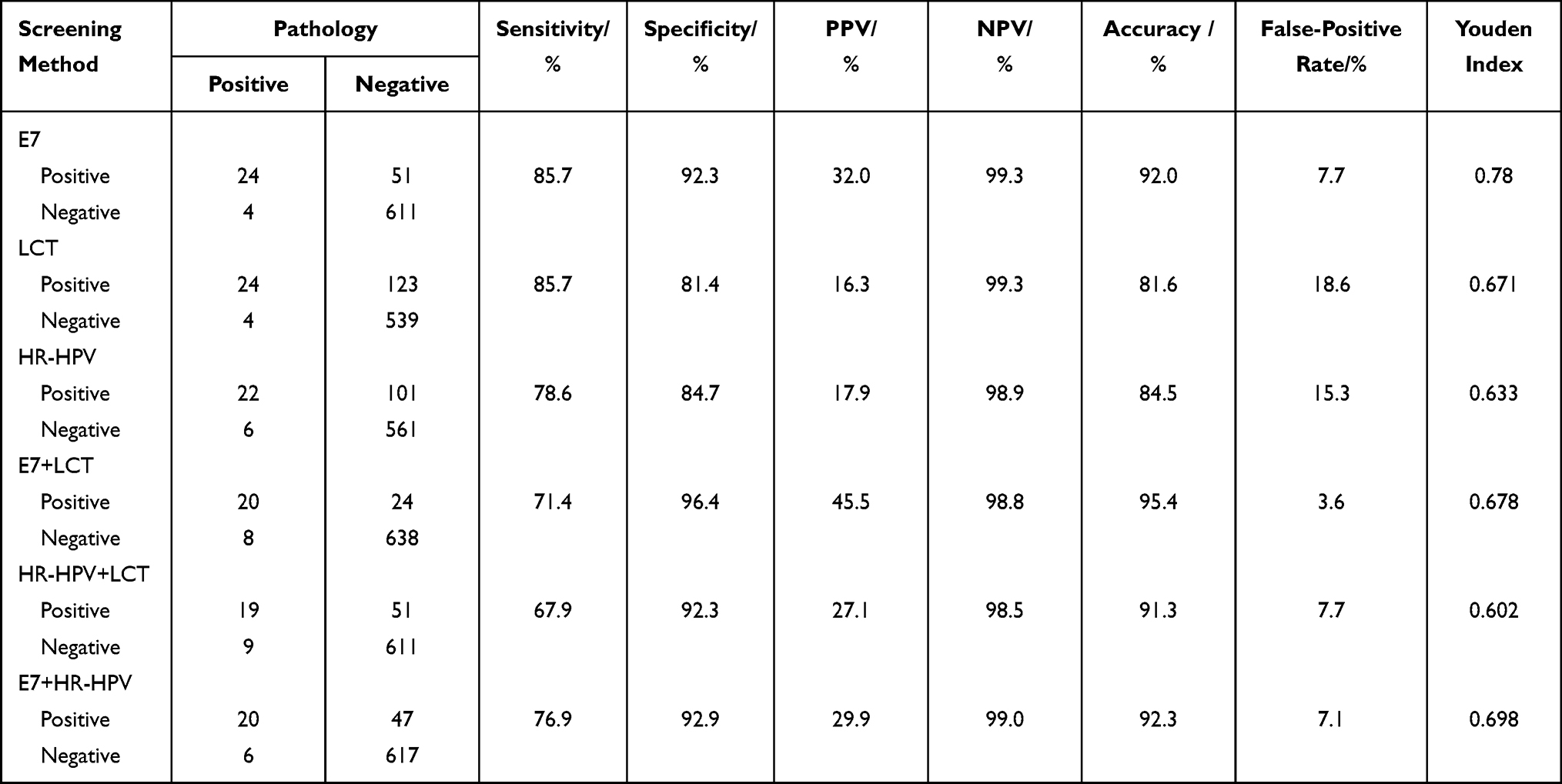 |
Table 2 Evaluation of the Clinical Performances of E7-ICC Staining, LCT, or HR-HPV Test Alone for Cervical Precancerous Lesion Screening and Their Paired Combinations for Screening for Cervical Precancerous Lesions with CIN2+ (HISL) as the Endpoint |
Regarding the preliminary screening schemes for cervical precancerous lesions, the colposcopy referral rate was 10.9% in patients with positive E7 test results, 18% in patients with positive HR-HPV test results, 21.3% in patients with LCT results of ASCUS or worse, and 7.7% in HR-HPV-positive patients with LCT results of LISL or worse (Table 3).
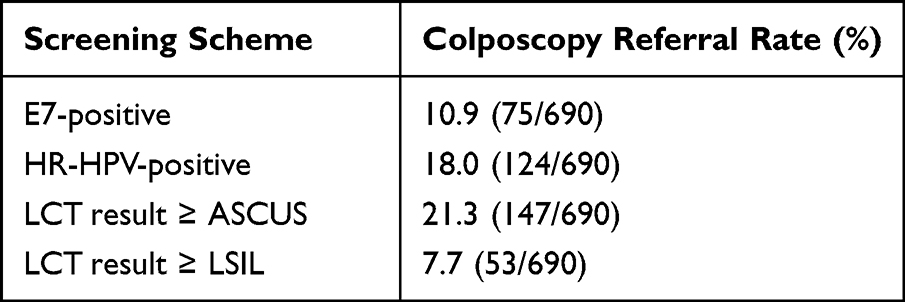 |
Table 3 Colposcopy Referral Rates for Cervical Precancerous Lesions Diagnosed Using Different Preliminary Screening Regimens |
Discussion
The complete elimination of cervical cancer has entered the national and WHO strategic plans, which are expected to effectively control the incidence of cervical cancer by 2030. Although the HPV vaccines are gradually becoming popular in China, HPV vaccination has not yet reached the requirements to reach the goal of complete elimination of cervical cancer by 2030. For example, the effectiveness of the vaccines needs to be improved, and the vaccination rate is low in high-risk age-appropriate women. Regular screening for cervical cancer is still an important measure to reduce the incidence and mortality of cervical cancer.12 As a routine screening method used in hospitals, LCT of exfoliated cervical cells has high specificity, but low sensitivity. Moreover, this screening method depends highly on the experience of the pathologist. Due to the large regional differences in economic development in China, the levels of medical care vary greatly between regions. Efficient cytology cannot be performed in some impoverished areas with limited resources, poor infrastructure, and a lack of cytological pathologists. In addition, high missed diagnosis rates and low efficiency are common due to the subjective interpretation of this test.
As a preliminary screening method for cervical cancer, HR-HPV nucleic acid detection has its own advantages, such as high sensitivity. Due to the characteristics of HPV itself and the active clearance of human autoimmunity, there will be a large number of transient infections. However, this does not directly indicate whether HPV has been integrated into the original human genome, nor can it directly indicate that HR-HPV positive patients are patients with cervical intraepithelial neoplasia. Therefore, the reason for HR-HPV false positive is that the specificity of this test is low.2 Therefore, although HPV vaccines with different prices are becoming more popular, universal cervical cancer screening is facing severe challenges. Developing screening methods that can precisely predict cervical lesions and clarifying the scope of triage screening are the future directions of cervical cancer screening. It will be particularly important to find new molecular markers and develop new detection techniques for fast and efficient triage screening.
Overexpression of E7 protein indicates persistent HPV infection and HR-HPV integration into the human genome, and it can reflect the cellular variation caused by HR-HPV infection. Zhao and Qiao13 showed that the high expression of E6 and E7 proteins indicates that the patient’s risk of high-grade lesions will increase in the next 10 years.13 E7-ICC staining can fill the gap in current cervical cancer screens and warn of the integration status after HPV infection, so it could be promoted as a standard for triage screening. In persistent infection with HR-HPV, the DNA of HPV integrates into the genome of normal cells. Once the virus destroys the E1 and E2 regions in the cell’s genome through integration, the expression of E6 and E7 is no longer inhibited. After DNA integration, the E6 and E7 oncoproteins will be expressed at persistently high levels. The E7 protein binds to pRb to dissociate the pRb–E2F complex, causing the loss of control of the Rb pathway, which stimulates the expression of cell proliferation–related genes, such as the p16INK4A, Ki67, and cyclin E genes, through feedback, resulting in disordered cell cycles and uncontrollable proliferation of cervical epithelial cells. In summary, E7 protein is a key biomarker leading to the malignant progression of cervical epithelial cells.
This study showed that E7-ICC staining had a sensitivity of 85.7%, a specificity of 92.3%, a PPV of 32%, an NPV of 99.3%, an accuracy of 92%, and a false-positive rate of 7.7% for the preliminary screening of cervical cancer with the presence of HSILs (or worse lesions) in the cervix (pathological results: CIN2+) as the endpoint. E7-ICC staining alone had significantly higher specificity and accuracy and a significantly lower false-positive rate than HR-HPV nucleic acid detection alone, which indicates the higher diagnostic accuracy of E7-ICC staining for HSILs and worse. Zhao14 performed cytology, E6/E7 protein detection, and HPV genotyping on 1461 patients who were HPV-positive in initial screening and found that E6/E7 protein detection in women had a sensitivity of 67.74% and a specificity of 89.47% for diagnosing CIN2+ and a sensitivity of 100% and a specificity of 85.94% for diagnosing CIN3+. In this study, the specificity and accuracy of E7-ICC staining alone for the diagnosis of HSILs and worse were higher than those of HPV or LCT alone. We found that the combined use of E7-ICC staining and LCT or the HR-HPV test had higher specificity and accuracy than E7-ICC staining alone, so this combination effectively avoided the limitations of single methods for preliminary screening.
The HR-HPV test is often used as a preliminary screening method for cervical cancer. This test is very sensitive to HR-HPV but has low specificity for cervical cancer. It fails to indicate the actual presence of cervical cancer due to its high false-positive rate. The main reason for the high false-positive rate is the presence of transient infection due to the characteristics of HPV. Therefore, the HR-HPV test must be combined with other screening methods to improve the specificity while maintaining the high sensitivity for triage purposes. Another preliminary screening method is LCT, which has high specificity and high accuracy, but its low sensitivity results in missed diagnosis and misdiagnosis. Furthermore, ASCUS is one of its interpretation criteria. Therefore, LCT depends highly on the experience of the pathologist. There are few registered pathologists in China, so it is difficult to apply LCT in large-scale screens. A growing number of studies have shown that E7-ICC plays an important role in distinguishing ASCUS, LSIL, and HSIL results by LCT; it can distinguish between transient and persistent HR-HPV infections; and it enables finer screening.15 Our results also showed that the combined use of E7-ICC staining and LCT morphology for the triage of HPV-positive women could significantly reduce the colposcopy referral rate while maintaining high sensitivity, could greatly reduce the number of patients who cannot be diagnosed or who need repeat LCT in a short time due to ASCUS, and could reduce the cost and time of manual interpretation. The results of combined screening in this study showed that the sensitivity of the E7+HR-HPV test for screening of CIN2+ was 76.9%, which was higher than that of HR-HPV+LCT (67.9%) or that of E7+LCT (71.4%). The specificity of E7+LCT was 96.4%, which was significantly higher than that of HR-HPV+LCT (92.3%) or that of E7+HR-HPV (92.9%). These results suggest that E7+HR-HPV may be used as a preliminary screening method for cervical cancer. E7-ICC staining can be used to triage ASCUS in the LCT results. Ghittoni et al16 found that E7-ICC staining could be used to interpret LSILs and HSILs in cervical precancerous lesions. The data in this study also showed that E7-ICC staining alone could be used as a preliminary screening scheme for cervical cancer to determine the status of cervical lesions. The sensitivity of E7-ICC staining for HSIL (CIN2+) and HSIL (CIN3+) was comparable to that of the HR-HPV test, and the specificity of E7-ICC staining was close to that of traditional morphological interpretation–based LCT. Therefore, E7-ICC staining fully integrates the advantages of the HR-HPV test and LCT. Screening with E7-ICC staining alone resulted a lower colposcopy referral rate (10.9%) than the 18% by the HR-HPV test or the 21.3% by LCT (results of ASCUS or worse). Therefore, E7-ICC staining can be used for the triage screening of cervical precancerous lesions and the preliminary screening of cervical precancerous lesions in large populations.
E7-ICC staining with the monoclonal antibody targeting the cervical cancer oncoprotein E7 can be used as a preliminary screening scheme for cervical precancerous lesions. Its sensitivity is comparable to that of HR-HPV nucleic acid detection for cervical precancerous lesions, and its specificity is comparable to that of LCT. In addition, E7-ICC staining can facilitate the further detection of E7 protein in HR-HPV-positive patients to indicate whether HR-HPV is integrated and to indicate the occurrence of precancerous lesions, thus avoiding over-diagnosis of HR-HPV infection. Moreover, E7-ICC staining can facilitate graded diagnosis in LCT, thereby avoiding situations of uncertainty based on morphology, such as ASCUS, and effectively improving the accuracy and sensitivity of LCT for cervical cancer screening.
In summary, E7-ICC staining, a new-generation cervical cytology technique, integrates immunology with morphology, giving it high sensitivity and specificity and good preliminary screening performance. E7-ICC staining can be used as an auxiliary scheme for conventional screening along with LCT and HR-HPV, and the interpretation of E7-ICC staining results is simple and objective. Therefore, it can become the preferred technique for the triage screening of cervical precancerous lesions in large populations. E7-ICC staining can also be used for large-sample, low-cost screening through integrated automated test equipment.17 However, prospective multicentre studies with large sample sizes and long-term follow-ups will be needed to evaluate the effect of E7-ICC staining in the prediction, treatment, and prognosis of cervical lesions through clinical practice from multiple perspectives.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arbyn M, Weiderpass E, Bruni L, et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health. 2020;8:e191–e203. doi:10.1016/S2214-109X(19)30482-6
2. Ronco G, Dillner J, Elfström KM, et al. Efficacy of HPV‑based screening for prevention of invasive cervical cancer: follow‑up of four European randomized controlled trials. Lancet. 2014;383(9916):
3. Huh WK, Ault KA, Chelmow D, et al. Use of primary high‑risk human papillomavirus testing for cervical cancer screening: interimclinical guidance. Gynecol Oncol. 2015;136(2):
4. Yamato K, Yamada T, Kizaki M, et al. New highly potent and specific E6 and E7 siRNAs for treatment of HPV 16 positive cervical cancer. Cancer Gene Ther. 2008;15:140–153. doi:10.1038/sj.cgt.7701118
5. Phelps WC, Yee CL, Münger K, Howley PM. The human papillomavirus type 16 E7 gene encodes transactivation and transformation functions similar to those of adenovirus E1A. Cell. 1988;53:539–547. doi:10.1016/0092-8674(88)90570-3
6. Barbosa MS, Edmonds C, Fisher C, Schiller JT, Lowy DR, Vousden KH. The region of the HPV E7 oncoprotein homologous to adenovirus E1a and SV40 large T antigen contains separate domains for Rb binding and casein kinase II phosphorylation. EMBO J. 1990;9:153–160. doi:10.1002/j.1460-2075.1990.tb08091.x
7. Ohlenschlager O, Seiboth T, Zengerling H, et al. Solution structure of the partially folded high-risk human papilloma virus 45 oncoprotein E7. Oncogene. 2006;25:5953–5959. doi:10.1038/sj.onc.1209584
8. Boyer SN, Wazer DE, Band V. E7 protein of human Papillomavirus16 induces degradation of retinoblastoma protein through the ubiquitin-proteasome pathway. Cancer Res. 1996;56:4620–4624.
9. McLaughlin-Drubin ME, Park D, Munger K. Tumour suppressor p16 INK4A is necessary for survival of cervical carcinoma cell lines. Proc Natl Acad Sci USA. 2013;110:16175–16180. doi:10.1073/pnas.1310432110
10. Egawa N, Egawa K, Griffin H, et al. Human Papillomaviruses, epithelial tropisms, and the Development of Neoplasia Viruses. Viruses. 2015;7(7):3863–3890. doi:10.3390/v7072802
11. Shi WJ, Liu H, Wu D, et al. E6/E7 proteins are potential markers for the screening and diagnosis of cervical pre‑cancerous lesions and cervical cancer in a Chinese population. Oncol Lett. 2017;14:6251–6258. doi:10.3892/ol.2017.6932
12. Belinson JL, Pretorius RG. A standard protocol for the colposcopy exam. J Low Genit Tract Dis. 2016;20(4):
13. Jansen E, Zielonke N, Gini A, et al. Effect of organised cervical cancer screening on cervical cancer mortality in Europe: a systematic review. Eur J Cancer. 2020;127:
14. Rezhake R, Qiao YL, Zhao FH. Eight-type human papillomavirus E6/E7 oncoprotein detection as a novel and promising triage strategy for managing HPV-positive women. Int J Cancer. 2019;144:34–42. doi:10.1002/ijc.31633
15. Shi L, Han F, Shi C, Huang Y, Liu Y, Chang X. Immunohistochemical detection of E7 human papillomavirus protein in pre-malignant and malignant lesions of uterine cervix. Mol Med Rep. 2018;18:3949–3956. doi:10.3892/mmr.2018.9416
16. Ghittoni R, Accardi R, Hasan U, et al. The biological properties of E6 and E7 oncoproteins from human papillomaviruses. Virus Genes. 2010;40(1):1–13. doi:10.1007/s11262-009-0412-8
17. Qiao YL, Jeronimo J, Zhao FH, et al. Lower cost strategies for triage of human papillomavirus DNA-positive women. Int J Cancer. 2014;134(12):2891–2901. doi:10.1002/ijc.28616
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.