")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Utilization of Pediatric Hip Spica Tables Among Orthopedic Surgeons: Locally Customized versus Company-Manufactured (Cross-Sectional Study)
Authors Alomran AK , Almulhim H, Alabdulqader S, Almutairi DS, Alrusayyis DF, Althwaiqb SA, Alumran A
Received 28 February 2023
Accepted for publication 17 July 2023
Published 28 July 2023 Volume 2023:16 Pages 2145—2153
DOI https://doi.org/10.2147/JMDH.S398953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ammar K Alomran,1 Hadeel Almulhim,2 Shahad Alabdulqader,2 Danah S Almutairi,2 Danah F Alrusayyis,2 Sarah A Althwaiqb,2 Arwa Alumran3
1Orthopedics Department, Imam Abdulrahman bin Faisal University, College of Medicine, Dammam, Saudi Arabia; 2College of Medicine, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 3Health Information Management and Technology Department, Imam Abdulrahman bin Faisal University, College of Public Health, Dammam, Saudi Arabia
Correspondence: Hadeel Almulhim, Tel +966501407070, Email [email protected]
Background: Hip spica tables are widely used among pediatric orthopedic surgeons to maintain the hip position during cast application and drying processes for a better outcome. Locally customized spica tables can be a significant concern if their limitations significantly interfere with the quality of care.
Objective: This study aims to explore the current practice of pediatric hip spica table application among hospitals in the GCC countries and report comprehensive data that help surgeons enhance their practice.
Methods: This is a cross-sectional study on pediatric orthopedic surgeons using a self-administered Online Questionnaire. The respondents were grouped as those using locally customized tables, where further information about the material and characteristics were collected, and those using company manufactured tables. Both groups answered analytical questions related to their current practice of hip spica tables.
Results: Sixty-three surgeons completed the survey. More than half the physicians in this study are using locally customized spica tables (n= 41, 65%). Compared to company-manufactured tables, locally customized tables were associated with a higher rate of difficulties when taking an X-ray, when the patient weighs more than 50.0 kg, and with anesthesia, although not statistically significant.
Conclusion: Obtaining a good quality spica table at a suitable price is a primary obstacle pediatric orthopedic surgeons face. This study shows no statistically significant difference between locally customized and company-manufactured tables regarding the outcomes and that spica tables have room for development to optimize their utilization.
Keywords: spica tables, pediatric orthopedics, spica cast, developmental dysplasia of the Hip, DDH, fractures
Introduction
For thousands of years, the immobilization of a fractured/injured limb has been a cornerstone for proper healing and achieving a favorable outcome concerning orthopedic-related injuries and procedures. Therefore, the principe of cast application was born and it developed over the years through individuals attempting broken bones immobilization by using various materials, leading up to the modern day cast application as we know it. As earlier as 350 BC, Hippocrates described casting material when he wrote about using bandages soaked in wax and resins to wrap injured limbs.1 However, with the advancement in medicine, cast application was not limited to peripheral fractures; it proved its effectiveness in treating pediatric-related orthopedic conditions involving the hip joint, pelvis, and femur through a particular type of cast called hip spica cast.2
There are numerous traumatic and non-traumatic pediatric orthopedic conditions that necessitate the application of a spica cast in different setting such as emergency rooms, operating rooms, and clinics. Regardless of the setting, the common denominator among these scenarios is the need for prolonged immobilization during the process of cast application, which is achieved by using certain unique tables known as spica tables that ensure the best outcome, according to Swain.3
The main principle of the hip spica table is to maintain the hip position during cast application for a better outcome.4 The patient’s torso must be supported while the limbs are appropriately angled and immobilized. Although spica table designs widely vary, most of them consist of head support, torso support, buttock support, arm support, and foot support, and they can be adjustable or non-adjustable.3
Spica tables can be purchased from a manufacturing company or be locally built and customized as per the surgeon’s preference and financial capacity, which majorly contributes to the heterogeneous characteristics of spica tables in literature. For example, some locally customized spica tables are basic as they spare arm support, which however may require compensating by adding one or more cast-application assistants, as can be observed in a picture provided by one of our study participants (Figure 1). One the other hand, Gill et al5 described the “box-and-bar” technique that needs only one assistant for holding the child’s leg with the hip flexed and abducted, suggesting an approach that is considered friendly to smaller staffed hospitals. It consists of a sliding bar that supports the spine and sacrum which is positioned in the center of a square wooden box. The latter is designed to hold the patient’s head and chest. The physician then can apply the cast comfortably without limitations. This technique has been adopted by the authors’ institution for over 15 years in the operative room setting, with a high success rate. The table’s design is claimed to be simple, safe, cost-effective, and reproducible. Popkin et al reported a similar hip spica box configuration for managing femoral fractures.6 However, the presence of three assistants is imperative to reposition the injured leg with adequate stabilization of the head and the other non-fractured leg.
 |
Figure 1 Locally- customized spica table, courtesy of one of our research participants. |
Alsidiky et al described one of the recent sophisticated advancements in the spica table structure that was granted a patent in 2019.7 Along with an adjustable vertical post and extendable arms with a “U” shaped leg holder, this device contains a platform that extends from the top of the vertical post for engagement with a table similar to the surgical table as illustrated (Figure 2).4 Additionally, the device holds the patient’s lower extremities to facilitate sterilization and draping.7
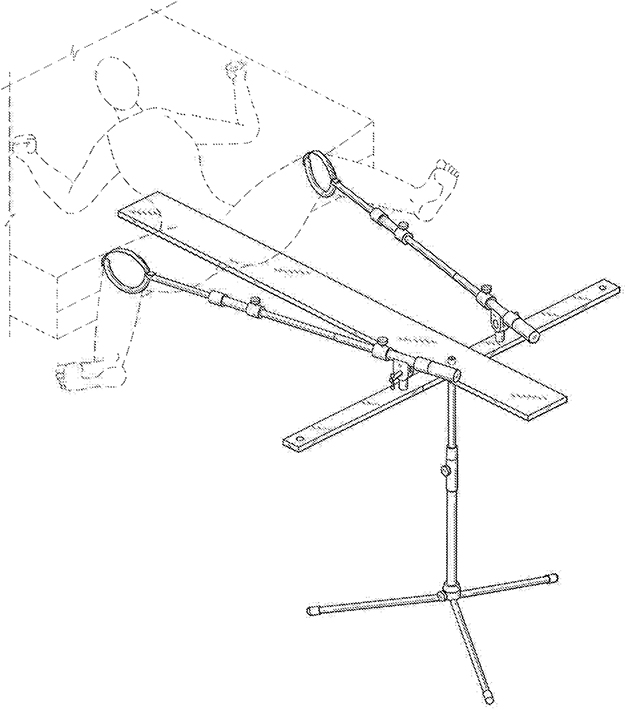 |
Figure 2 Company -manufactured spica table.4 |
The examples discussed above highlight the discrepancies among spica tables which cannot be overlooked and necessitate the conduction of comparative studies in an attempt to conclude whether locally customized tables, which are significantly cheaper, are an adequate replacement of company-manufactured spica tables.
This study aims to explore the current use of hip spica tables in cast-application and in the management of pediatric patients among hospitals in the GCC countries, as well as compare company-manufactured and locally-customized tables, setting a cornerstone in pediatric orthopedic research by discussing different spica tables, aiding surgeons to find practical, cost-effective solutions to enhance their practice and encourage exploring new horizons of spica table invention.
Methods
This cross-sectional, questionnaire-based study has targeted pediatric orthopedic surgeons in Saudi Arabia and Gulf Cooperation Council (GCC) countries (United Arab Emirates, Kuwait, Bahrain, Qatar, and Oman) between December 8th, 2021, and March 1st, 2022, to study their current practice.
Surgeons of both genders and with all levels of training were considered, including specialists, fellows, and consultants. Surgeons from any other specialty or currently practicing outside the aforementioned countries were excluded from the study.
The approximate number of pediatric orthopedic surgeons in Saudi Arabia and the GCC is 100. The sample size was then calculated using the formula denoted by Daniel,8 where the confidence interval is set to 95% and the margin of error is 5%. The formula shows the appropriate sample size for the study population to be 79 participants. The study population was selected based on the accessibility of their contact information, ie, convenient sampling.
This study was carried out following the relevant guidelines after approval from the Institutional Review Board (IRB) of Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia [IRB-UGS-2021-01-210]. The participation was voluntary with maintaining confidentiality and anonymity. Informed consent was obtained from each participant prior to filling out the questionnaire.
A self-administered Online Questionnaire was structured in the English language by the authors after reviewing recent literature and consulting expert surgeons in pediatric orthopedics. It consists of two parts. The first part includes respondent and institution information, it is composed of 5 items and all of them represent independent variables; these are: Current medical practice position, Years of experience in pediatric orthopedics, Country of training in pediatric orthopedic fellowship, Current institution, and Country of current institution.
The second part includes hip spica table and related practice, this part includes 16 items related to the characteristics of the currently used hip spica table, usual utilization of the table, the advantages and encountered difficulties related to the adopted table design, and number of assistants needed to apply hip spica. While the outcome variable is the Origin of the currently used hip spica table (locally customized or company manufactured).
All collected data was transferred into an excel spreadsheet for data cleaning and management, then was exported to the Statistical Package for Social Sciences (SPSS) software version 249 software for formal analyses. Descriptive analysis was used to show summaries and percentages of the variables in the study, while chi-square test was used to conduct bivariate analysis. Odds ratio was calculated to find the odds of difficulties that physicians might face using locally customized tables compared to company manufactured.
Results
Out of the 79 pediatric orthopedic surgeons in the study sample, 63 completed the survey about the spica table with a response rate of 80%. More than half of the physicians in the study indicated that they use a locally customized spica table (n= 41, 65%), while the rest used a company-manufactured one (n= 22, 35%).
Most of the study participants were consultants (n=48, 75%). At the same time, more than half of the respondents indicated that they received their training in pediatric orthopedic fellowship in a local program (n= 30, 47%), followed by North America (n=18, 28%). The majority of physicians in the study indicated that they have 0 to 10 years of experience (n=35, 55%), while only nine physicians denoted that they have more than 20 years of experience (14%).
Most of the physicians in the study worked in a public institute (n= 52, 81%), while only 19% worked in private ones. More than half of the physician in the study work in hospitals affiliated to the Saudi Ministry of Health (n= 29, 45%), followed by 23% (n=15) in institutes affiliated to the ministry of education, ie, teaching hospitals (Table 1).
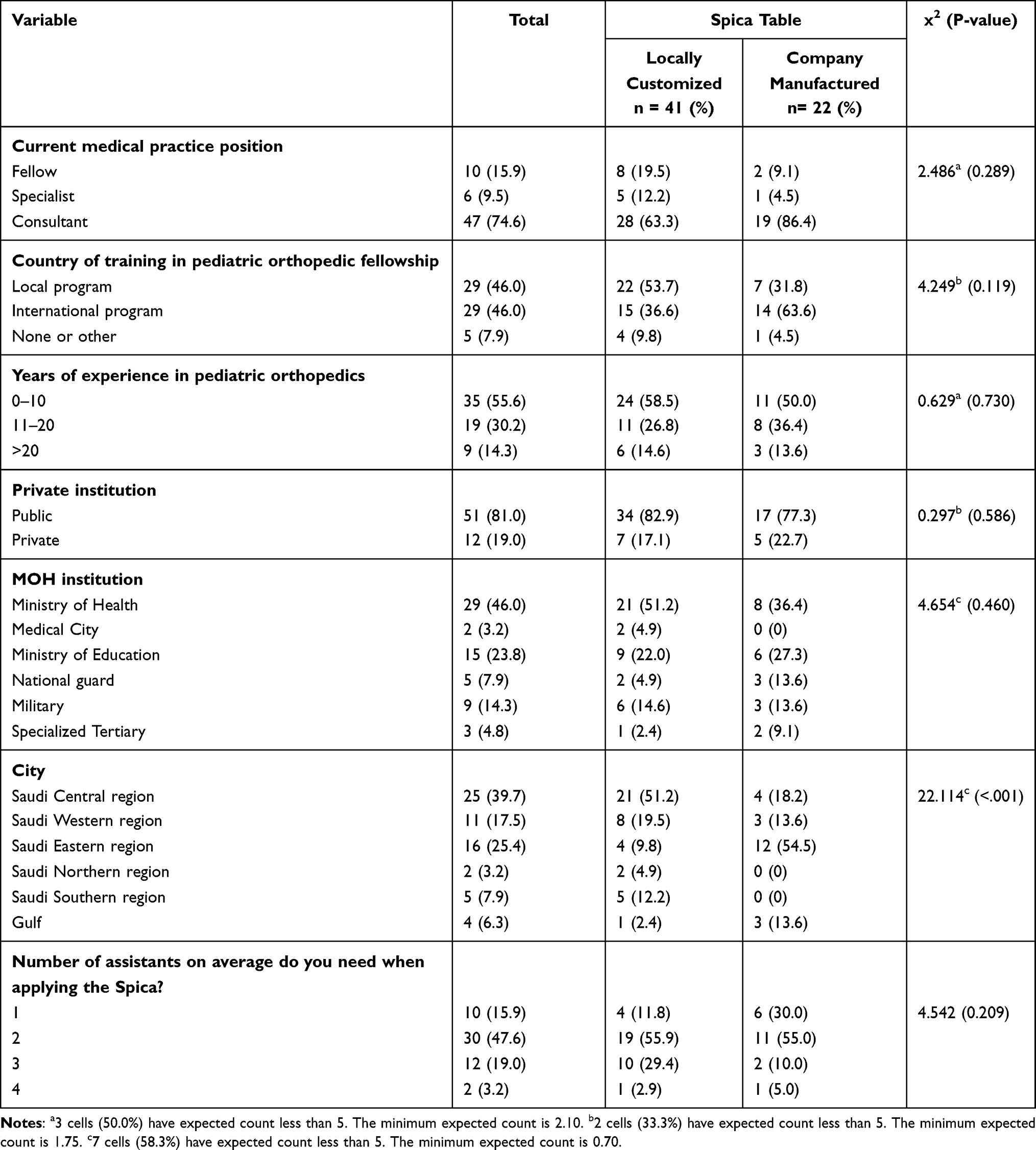 |
Table 1 Factors Associated with the Utilization of Different Types of Spica Table |
Further, when the physicians were asked about the number of assistants they need to apply the spica cast, half of them indicated that they need two assistants (n= 30, 48%). None of the abovementioned variables are statistically significantly different in utilizing the type of spica table (locally customized or company manufactured).
Given the higher population density in the Central region of Saudi Arabia, most physicians in the study are from the Central region (n= 26, 41%), followed by the Eastern region where the study was conducted (n= 16, 25%). In addition, four respondents were not from Saudi Arabia and were from the Arabian Gulf region (6%). The difference in the selection of the type of the spica table is statistically significantly different in different regions in the study (x2= 22.114, P<0.001). Most of the physicians in the Central and Western regions of Saudi Arabia use a locally customized table (84% and 73%, respectively), while the majority of physicians from the Eastern region use a company manufactured one (75% of physicians in the study from the Eastern region).
When the physicians were asked about the materials and design of their locally customized table, half of them indicated that the spica tables they use were made of wood, while the rest were made of metal, and most of them have back support (n=31, 91%), almost all of them have sacral support (n= 32, 94%), and all of them are portable (Table 2).
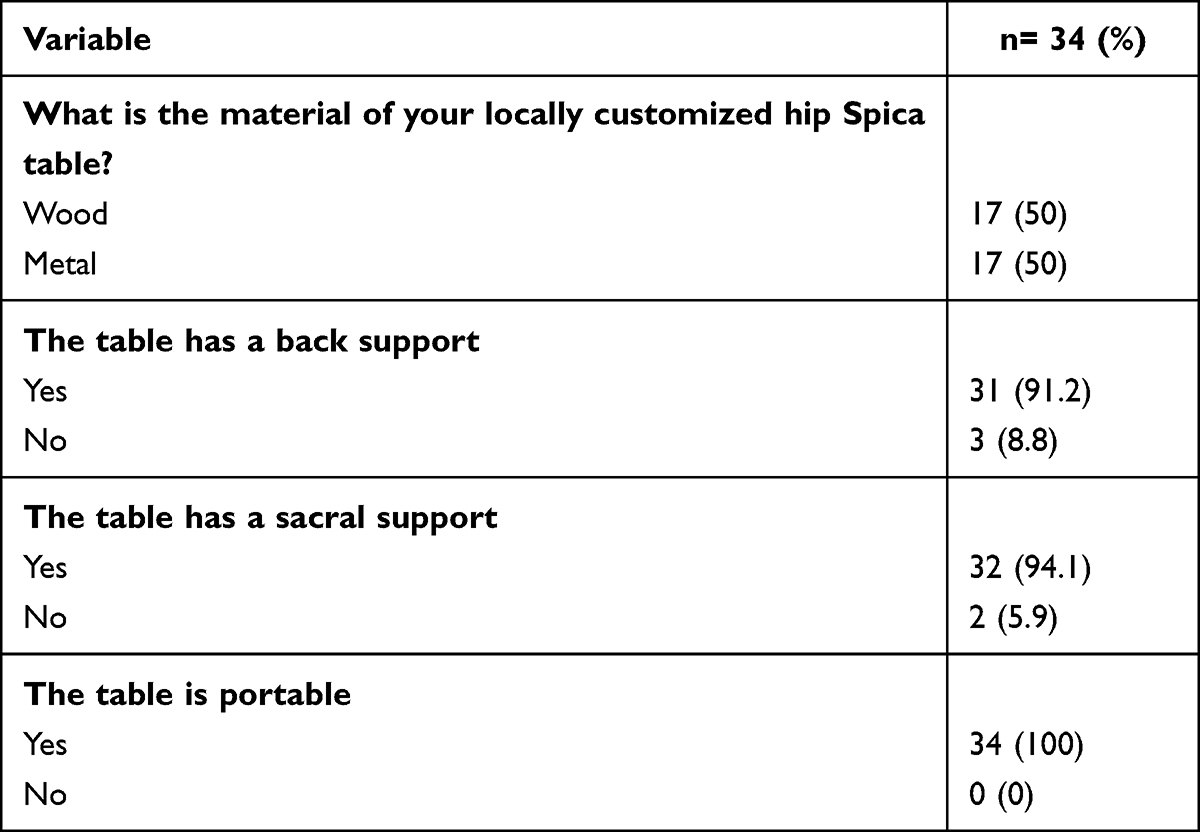 |
Table 2 Characteristics of the Locally Customized Spica Table |
A third of the participants believe that the company manufactured spica table is expensive (n=19), while only 16% indicated that they do not know the companies that provide spica tables. Other reasons for not using a company-manufactured spica table include they have a better option, it is complicated, requested but was not provided by the hospital, it is not practical, and very few cases are treated. Two physicians believed that the locally customized table is faster, easier, cheaper, and easy to build.
Almost half of the physicians in the study perceived a price range that their institutes are willing to pay for a company manufactured spica table between 1000 to 10,000 (n=25, 46%). While 30% (n= 16) did not know how much their institutes were willing to pay for a company-manufactured spica table (Figure 3).
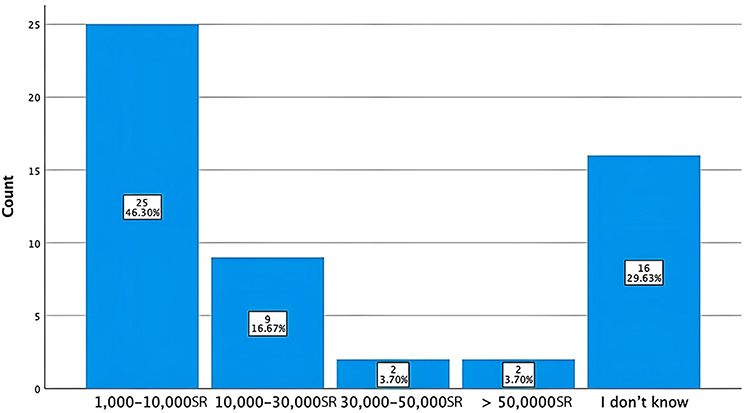 |
Figure 3 Perceived suitable price range of company-manufactured table. The currency that is used in this figure is Saudi Riyal (SR). One United States Dollar (USD) equals 3.75 SR. |
Most physicians in the study indicated that they use the spica table in the Operating room (n= 34, 83%), while less than half use it in the Emergency room (n= 17, 42%), and only 12% use it in the inpatients’ ward (n=5), and 20% use it in the out-patients clinic (n= 8) (Table 3). The utilization of the spica table is not statistically significant according to the type of the table, in other words, both locally customized and company manufactured tables are utilized similarly.
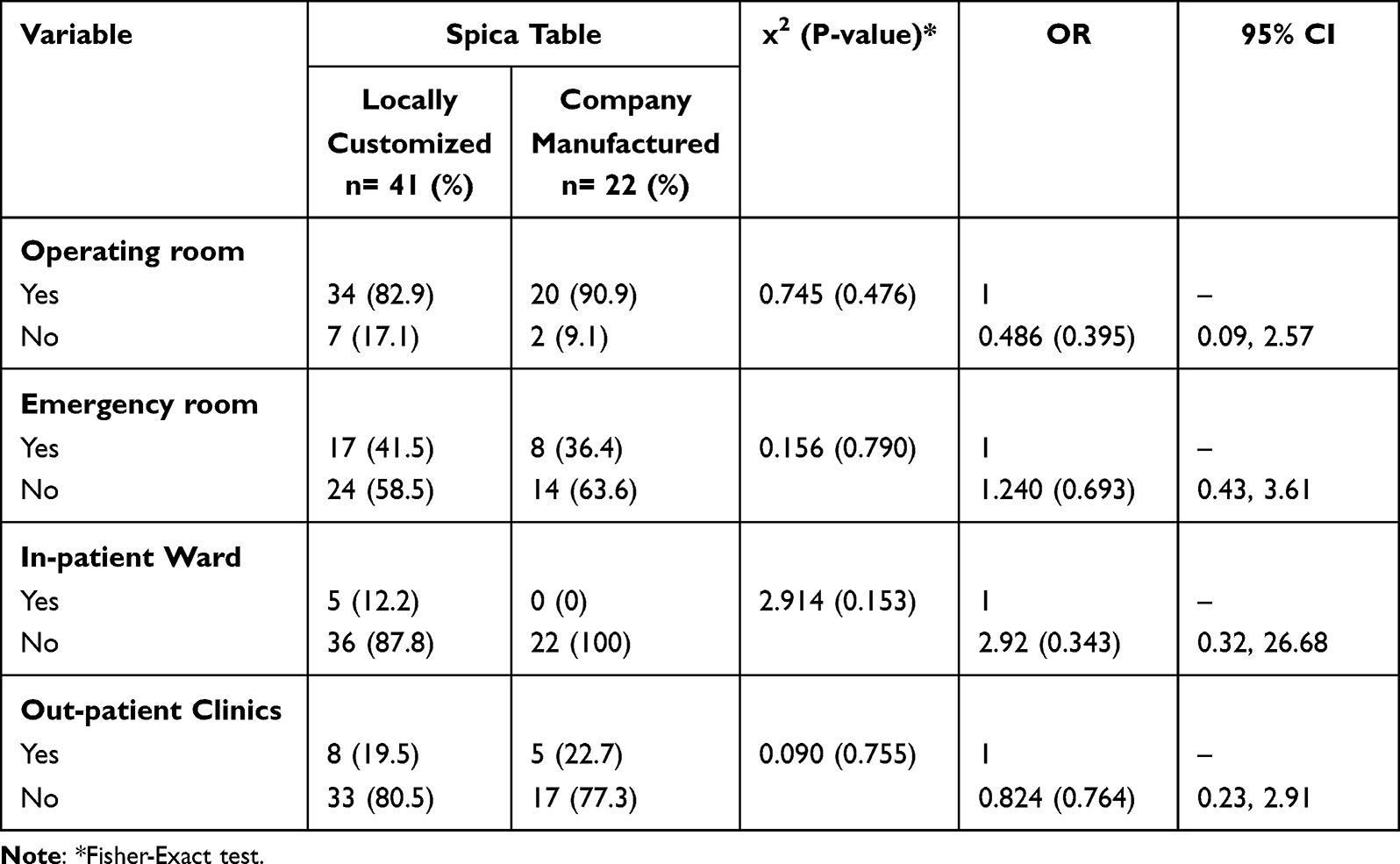 |
Table 3 Utilization of the Spica Table |
Physicians in the study were asked about the difficulties they face with their spica table; 41% indicated that they face difficulty when taking an x-ray (n= 22). While the majority mentioned that they have difficulty when the patient weighs more than 50 kg (n=41), and only 24% have difficulty with the anesthesia (n= 12). There is no statistically significant difference in the difficulties between the two types of spica tables (Table 4).
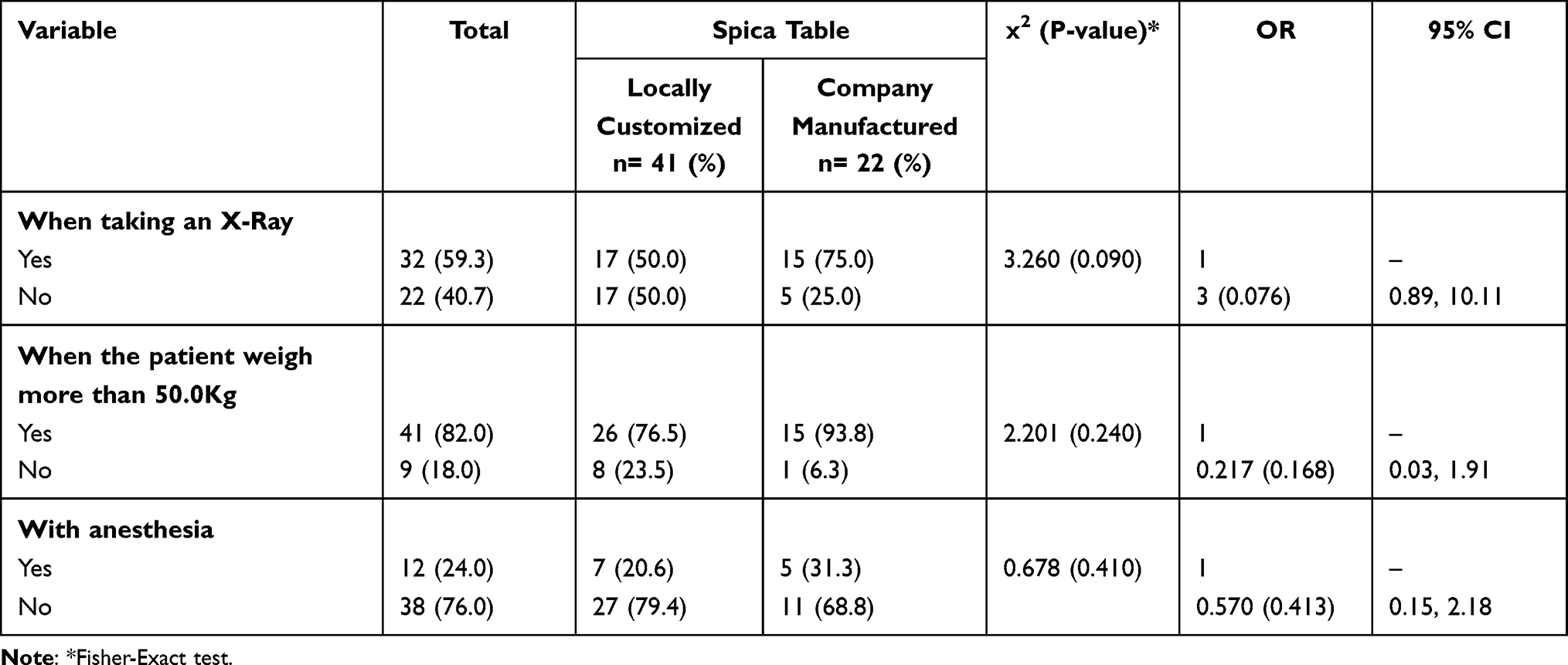 |
Table 4 Difficulties with Your Current Spica Table Application |
Discussion
The study assessed the differences in the utilization and difficulties physicians face using two different kinds of spica tables, the locally customized ones and the company manufactured ones.
There are no significant differences in utilization nor the difficulties between the locally customized spica tables and the company manufactured ones. This result is consistent with the study hypothesis where it has hypothesized that the affordable locally customized spica tables are no different from the expensive company manufactured ones.
This study has shown no statistically significant difference in terms of utilization when comparing the two types of spica tables. Both were found to be just as effective in achieving the desired outcome, which is applying a spica cast onto the pediatric patient successfully. This finding is supported by a couple of other studies, stating that manufactured tables’ outcomes could be achieved at a much lower price point with the help of locally customized tables, which could be used to treat the same range of cases that are managed on a manufactured one.5,10 This similarity in clinical outcome is a relief to most pediatric orthopedic surgeons, as manufactured table’s pricy nature prevents many medical establishments from owning one, forcing surgeons to improvise a design for their tables.
Regarding possible difficulties faced in the spica cast application process, our study found that the same issues were faced by both tables’ users. The issues ranged from lack of back support to the inability of the tables to bear some pediatric patients’ weights.
The issue of durability and the inability of most spica tables to accommodate different-sized patients is not new. As an article by Hashemi-Nejad and Cole11 considered this an obstacle that was commonly faced ever since, even with company-manufactured tables. Therefore, accommodating and supporting the bodies of pediatric patients of bigger sizes was and still is an obstacle spica tables have to overcome to be considered somewhat ideal.7 However, the current study showed that there is no statistical difference in the support provided to pediatric patients over 50 kg between the two tables. This indicates that the locally customized tables are just as competent as the company-manufactured ones when it comes to stability and support, and none of them exceeds the other when it comes to difficulty accommodating larger pediatric patients, whether in terms of height or weight.
Another particular challenge often faced with spica tables is radiolucency, which is an important characteristic that spica tables should have, as it is crucial to obtain multiple radiographs of the patient’s pelvic region throughout the process of spica cast application.6 The current study highlights the concern regarding the radiolucency of both types of spica tables. The results show no significant differences in this difficulty between the two types of tables in terms of radiolucency. Users of both tables reported facing about the same difficulties as each other in this department.
Searching further for possible discrepancies between company-manufactured tables and locally customized ones, the authors inquired about the number of assistants needed during the process of spica cast application. The study found that predominantly the number of assistants needed for such procedure was two assistants, according to our participants, despite the type of table used.
Our study is the first of its kind, to the knowledge of the authors, in terms of discussing Spica-table practice in the Kingdom of Saudi Arabia and the Gulf region, as well as the financial burden associated with acquiring manufactured Spica-tables as opposed to locally customized ones which could be obtained at a much lower price point.
Limitations
A difficulty that was faced while reviewing relevant literature was in finding locally-conducted studies to scope out the local practice, as not many studies were published on the use of spica tables in Gulf countries or even worldwide, limiting what we know about some potential challenges that may have arisen for some locally-customized spica tables’ users such as certain materials obstructing the view when taking radiographs of the patient over the table or certain procedures being more difficult due to unexpected impractical aspects of locally-customized tables, and how they attempted to overcome those obstacles. However, we have attempted to mitigate this gap in literature by designing a comprehensive qualitative Online Questionnaire in the initial data collecting stages. The questionnaire was built and distributed in a way that provides a sufficient scope of the current practice in Gulf countries, setting our data and findings as a foundation for similar future studies to rely on. Needless to say, the questionnaire was distributed to be filled by a statistically and clinically representative sample, as priorly mentioned in the Methodology section of this research.
Our particular population choice of pediatric orthopedic surgeons brought on some obstacles, such as reaching this specific population in the Kingdom of Saudi Arabia and the Gulf region, and getting them to fill out the survey, providing sufficient data in each section for the authors to analyze, which posed a significant challenge given the surgeons’ hectic schedules due to their relative rarity. Another obstacle was the shortage of time over which this study was conducted, as the authors were allocated a specific tight timeline and had to expedite the research process in all its stages while maintaining a high level of accuracy and precision. The authors, therefore, were also presented with a challenge regarding obtaining the appropriate response rate in such a timely manner.
Furthermore, it is worthy of mentioning that our study, due to time constraints, was not an observational field study, where we visited the field and documented our observations on the use of spica tables ourselves, but rather a questionnaire-based study, where information was sought out from the participants, not only about their practice and current tables’ designs but also on the characteristics they wish for the most in their current spica tables, whether manufactured or customized, and inquired about the difficulties based by those who chose to build locally-customized tables compared to their peers who are manufactured-tables’ users.
Conclusion
Spica tables have an undeniably crucial role in helping to manage various pediatric orthopedic cases, and therefore should be made more accessible to hospitals by proposing cost-effective company-manufactured spica table alternatives to low-budget or rural hospitals that are just as efficient and more affordable. The financial burden of company-manufactured spica tables was illustrated in our study, as we found that one of the main obstacles faced by pediatric orthopedic surgeons in regards to spica tables was obtaining a good quality table at a suitable price. The hefty price tag that often comes with purchasing a manufactured table has driven many of those surgeons towards the option of building their customized spica tables locally.
At last, spica tables have room for development in terms of materials used to build them, as well as the flexibility to accommodate different pediatric patients of different physical measurements in different clinical settings, to make the tables’ utilization easier. These things, however, should not be at the expense of the stability, durability, and radiolucency of the tables. Therefore, we recommend that our study gets recreated on a larger global scale to possibly reach the ideal and most cost-effective spica table design that could significantly improve future pediatric orthopedic practices worldwide.
We believe that study could open a new horizon for the creation of an advanced spica table that is practical yet feasible to develop, as conducting a larger study would allow the particular population of pediatric orthopedic surgeons all around the world to benefit from each other’s expertise with spica tables, which will hopefully eventually lead to the evolution of spica table practice in the future.
Abbreviations
GCC, Arabia and Gulf Cooperation Council; IRB, Institutional Review Board; SPSS, Statistical Package for Social Sciences.
Ethical Approval
Institutional review board approval was obtained from Imam Abdul Rahman bin Faisal University (IRB-UGS-2021-01-410), dated 8/11/2021.
Consent to Participate
Informed consent was obtained from all the participants in the study.
Funding
This research received no external funding.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Szostakowski B, Smitham P, Khan WS. Plaster of Paris–short history of casting and injured limb immobilization. Open Orthop J. 2017;11:291.
2. Bitar KM, Ferdhany ME, Ashraf EI, Saw A. Physical and clinical evaluation of Hip spica cast applied with three-slab technique using fibreglass material. Malays Orthop J. 2016;10(3):17. doi:10.5704/MOJ.1611.008
3. Swain SM; SPICA TABLE. United States patent US 8001633 B2. JENSEN + PUNTIGAM, P.S., Assignee. 2011.
4. Alsiddiky A, Alatassi RM; King Saud University. Hip spica cast application device. United States patent US 10729577. 2020.
5. Gill IP, Kolimarala V, Montgomery RJ. Application of Hip spica cast using a box-and-bar technique. Ann R Coll Surg Engl. 2008;90(8):700. doi:10.1308/rcsann.2008.90.8.700
6. Popkin CA, Dold AP, Vitale MG. Treatment of pediatric diaphyseal femur fractures: spica casting and traction. In: Popkin CA, Dold AP, Vitale MG, editors. Pediatric Femur Fractures. Boston: Springer; 2016:117–132.
7. Alsiddiky A, Alatassi RM, Dous AB; King Saud University. Hip spica cast application stand. United States patent US 10265236. 2019.
8. Daniel WW. Biostatistics: A Foundation for Analysis in the Health Sciences.
9. IBM Corp. IBM SPSS Statistics for Macintosh. Armonk, NY: IBM Corp; 2017.
10. Pasque CB, Harbach GP. Hip spica application using an operating table armboard. J Pediatr Orthop. 2000;20(6):757–758. doi:10.1097/01241398-200011000-00011
11. Hashemi-Nejad A, Cole WG. A universal hip spica pedestal. Injury. 1997;28(8):567–569. doi:10.1016/S0020-1383(97)00081-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.