")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
The Usefulness of Present-on-Admission Data as an Indicator of Healthcare Quality Evaluation Using the Korean National Hospital Discharge in-Depth Injury Survey Data from 2006 to 2019
Authors Lee K, Hwang J , Lee CM
Received 3 July 2023
Accepted for publication 19 October 2023
Published 6 November 2023 Volume 2023:16 Pages 2309—2320
DOI https://doi.org/10.2147/RMHP.S423555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kubra Kaya
Kyunghee Lee,1 Jieun Hwang,2 Chang Min Lee3
1Department of Healthcare Management, Eulji University of Korea, Seongnam, Republic of Korea; 2College of Health and Welfare, Department of Health Administration, Dankook University, Cheonan, Republic of Korea; 3Department of Gastroenterology, Changwon Hanmaeum Hospital, Changwon, Republic of Korea
Correspondence: Jieun Hwang, College of Health and Welfare, Department of Health Administration, Dankook University, Cheonan, Republic of Korea, Email [email protected]
Purpose: Comorbidities of a principal diagnosis have varying impacts on disease and require different management depending on the onset timing. This study investigated the usefulness of present-on-admission (POA), specifically focusing on decubitus ulcers, delirium, and hypokalemia, as an indicator of healthcare quality.
Patients and Methods: We analyzed patient discharge data for 14 years from 2006 to 2019 using Korean National Hospital Discharge In-Depth Injury Survey (KNHDIS).
Results: Out of 3,231,731 discharged patients, 19,871 had secondary diagnosis codes for decubitus ulcers (n=10,390, 52.3%), delirium (n=6103, 30.7%), or hypokalemia (n=3378, 17.0%). Analysis of patients with secondary diagnoses of decubitus ulcers, delirium, or hypokalemia revealed notable differences in demographics, including gender distribution, mean age, admission route, insurance type, surgical intervention rates, mortality rates, and length of stay (LOS). Among patients with one of the top 20 principal diagnoses, those with secondary diagnoses of decubitus ulcers, delirium, or hypokalemia exhibited higher odds of surgery, increased mortality risks, and longer LOS compared to those without these secondary diagnoses.
Conclusion: All three of these diseases commonly occur postoperatively or during treatment and thus should be designated as potentially preventable complications that require special attention, and should also be considered as quality-of-care indicators.
Keywords: healthcare quality evaluation indicators, present on admission, POA, decubitus ulcers, delirium, hypokalemia
Introduction
Comorbidities affect the treatment and outcomes of an illness.1–3 Comorbidities can be divided into underlying diseases that existed before the onset of the principal diagnosis and before complications that occur during treatment at the hospital.
Comorbidities of the principal diagnosis may have varying effects on the disease and require different management depending on the onset timing. Cardiovascular comorbidities of the coronavirus disease 2019 (COVID-19), which has emerged as an important issue, manifest and are treated differently depending on whether they were an underlying disease before the COVID-19 infection or whether they were a complication of COVID-19.4,5 In particular, complications that occur during the process of treating the principal diagnosis are subject to healthcare quality evaluation and cause analysis. Thus, present-on-admission (POA) indicators and Patient Safety Indicators (PSI) have been implemented to manage the onset timing of comorbidities and patient safety.
PSI were developed by the Agency for Healthcare Research and Quality (AHRQ); they are used to identify and manage diseases that are likely to occur during the process of treating patients at a healthcare facility and threaten patient safety.6 There are 20 AHRQ PSI,7 and the indicators are continually reviewed by the Organisation for Economic Co-operation and Development (OECD).8,9 The POA indicator is a system for distinguishing between a new diagnosis that was made during a hospital stay (POA) and one that was present before admission (POA Y flag) when healthcare facilities bill for reimbursement. The US Centers for Medicare & Medicaid Services (CMS) requires all Medicare and Medicaid claims to include the POA indicator in the principal and secondary diagnoses since 2007. From 2008, the CMS makes reimbursement decisions for diseases defined as a hospital-acquired condition (HAC) based on the POA indicator on the patient’s discharge data and declines reimbursement of 10 types of HAC based on the POA indicator.10,11
Studies that examined the effects of implementing the POA indicator in Medicare and Medicaid reimbursement denials for HACs and pressure ulcers12,13 showed that reimbursement was reduced, further highlighting the importance of preventing and managing HACs.
In 2012, the diagnosis-related group (DRG) reimbursement model was implemented in South Korea. Healthcare facilities are now required to specify the POA indicator in the DRG and new DRG reimbursement claims.14 The new DRG reimbursement system, which is an expansion of the previous seven systems, currently runs as a pilot program.15 In addition, the Health Insurance Review and Assessment Service (HIRA) provides subsidies for participating healthcare facilities to facilitate the establishment of the new DRG system and periodically performs qualitative evaluations of medical records, diagnostic coding, and POA data.16
POA data in Korea contribute to the thoroughness of medical record documentation and the enhanced accuracy of diagnostic coding.17 However, data utility remains low due to poor accuracy resulting from the short time elapsed since implementation and relevant staff and healthcare professionals’ inadequate awareness and training.10,14,16,18–20
In other countries, studies examining the conditions that markedly impact severity or treatment process and outcomes, such as hemorrhage, thrombosis, anemia, and coronary artery disease, have utilized the POA indicator to analyze the cause of HACs and promote quality of care.21–25 For instance, in the United States, POA data flagged in Medicare and Medicaid claims are utilized to monitor the quality of care provided to low-income individuals and older adults.26,27
POA data—along with PSI—may be an important source of information for detecting HACs, and it serves as a useful indicator to identify and ameliorate the risk factors and causes of complications. Hence, it is strongly associated with the quality of diagnostic coding28–31 and ultimately is a crucial means to promote the quality of healthcare.
However, a study that investigated the accuracy of POA data collected since 2012 in Korea based on PSI reported that the data has low reliability and accuracy and thus cannot be used as an indicator of healthcare quality. The study also suggested that diagnoses flagged with an N POA indicator, as opposed to the admitting diagnosis, should be monitored.16
Thus, this study aims to investigate whether decubitus ulcers, delirium, and hypokalemia—three conditions ranked in the top 20 diagnoses flagged with an N POA indicator in the new DRG claims data10 are useful as indicators of healthcare quality. In particular, POA codes for decubitus ulcers and delirium have been reported to have significant benefits in patient treatment and statistics data.32,33 Further, because the ICD-10 codes for these conditions do not indicate whether the condition was hospital-acquired or is a complication of treatment (T code), the POA flag is particularly useful in distinguishing this. Hence, if they are useful indicators of healthcare quality, our findings will provide evidence supporting their use as target diseases for POA management.
Materials and Methods
This study analyzed patient discharge data for a 14-year period from 2006–2019 using the Korean National Hospital Discharge In-Depth Injury Survey (KNHDIS). The KNHDIS aims to produce statistics based on the scale and epidemiological characteristics of injuries in Korea and to provide basic data for the development of healthcare policies to promote public health. To achieve this goal, the survey recruits all patients who have been discharged from a 100-bed or larger hospital nationwide each year as its study population and uses a two-step stratified cluster sampling to select about 9% of patients who were discharged from approximately 200 sampled hospitals. The survey is composed of 20 general items, such as disease and treatment information, and 10 in-depth injury items, including intentionality of injury, mechanism, place of occurrence, and activity, based on medical records. In this study, we focused on only the general items.
After examining the characteristics of all discharge patients within a 14-year period, those with a secondary diagnosis code (ICD) of L89 (decubitus ulcer), F058 or F059 (delirium), or E876 (hypokalemia) were identified and classified. Discharge patients who had more than one of the three secondary codes were excluded from the analysis. The three secondary code groups were compared for patient’s sex (men, women), age (<65, ≥65), route of admission (emergency department, outpatient department, others), type of insurance (National Health Insurance, medicaid, others), hospital bed size (100–299, 300–499, 500–999, ≥1000), treatment outcomes (alive, death), surgery (no, yes), and length of stay (LOS) using chi-square tests and one-way ANOVA.
The frequency of principal diagnoses of the three secondary diagnosis code groups (decubitus ulcers, delirium, hypokalemia) was examined based on the third digit of the ICD-10 code. Subsequently, the 20 most frequent principal diagnoses were identified. For patients with one of the top 20 principal diagnoses, the associations between their secondary diagnosis (decubitus ulcers, delirium, hypokalemia) and surgery, death, and LOS were analyzed using logistic regression and linear regression. The results were adjusted for sex, age, route of admission, type of insurance and hospital bed size. An adjusted odds ratio (aOR) with a 95% confidence interval (CI) was presented for the logistic regression, and an unstandardized coefficient and standardized coefficient were presented for the linear regression.
Statistical analyses were performed using the SAS version 9.4 software, and p<0.05 was deemed statistically significant.
Results
Sociodemographic Characteristics of the Study Population
From 2006 to 2019, 49.3% of all discharge patients were male, and 50.7% were female. The mean age was 46.2 years old (SD 25.2). Of all the discharged patients, 1.8% died and 29.8% had surgery. The mean LOS was 8.5 days (SD 24.0) (Table 1).
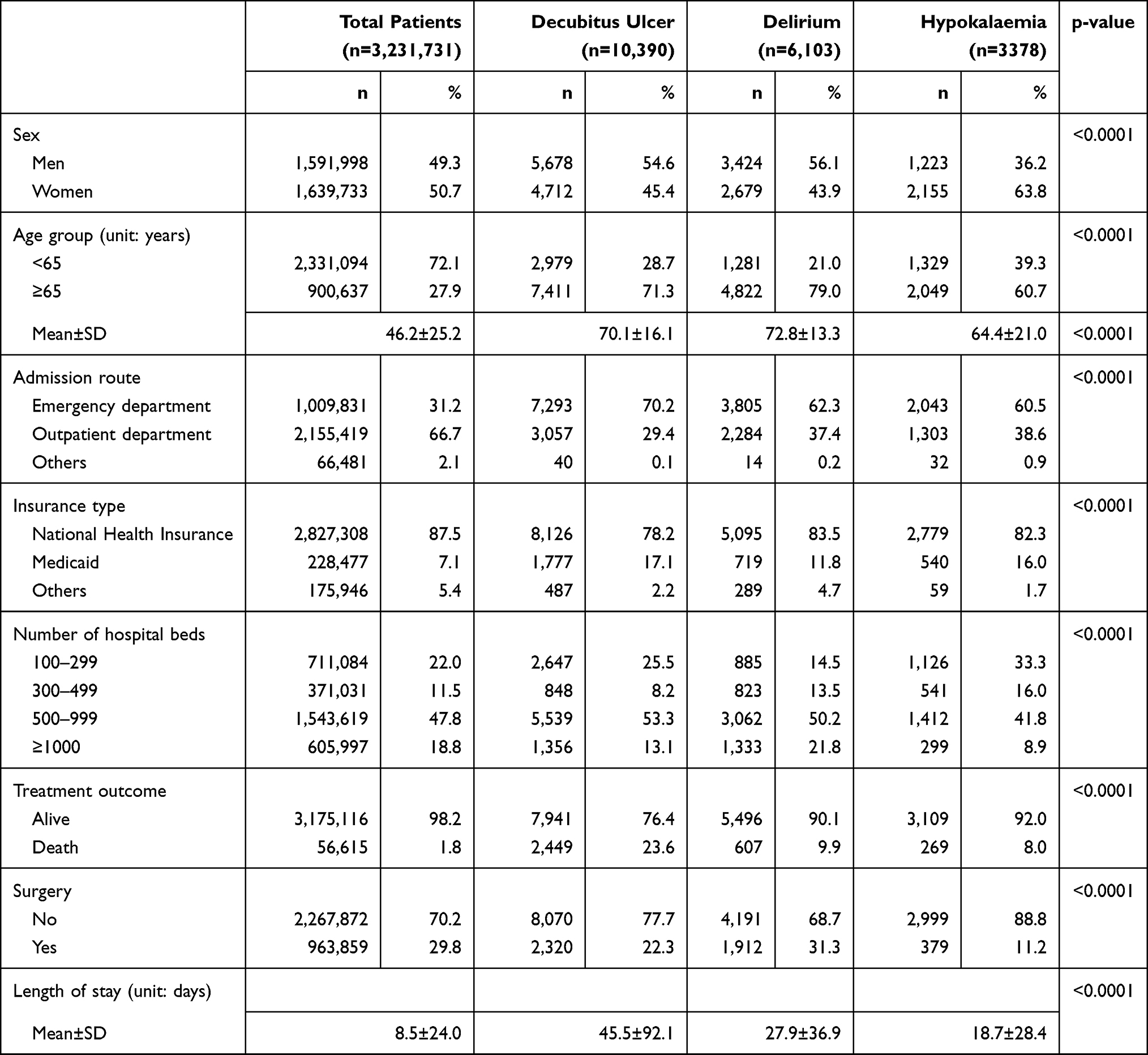 |
Table 1 Sociodemographic Characteristics of the Total Study Population and Patients with a Secondary Diagnosis of Decubitus Ulcers, Delirium, or Hypokalemia |
Sociodemographic Characteristics of Patients with a Secondary Diagnosis of Decubitus Ulcers, Delirium, or Hypokalemia
Of 19,871 discharge patients, 10,390 (52.3%) patients had a secondary diagnosis of decubitus ulcers, 6103 (30.7%) had delirium, and 3378 (17.0%) had hypokalemia (Table 1).
Regarding gender, there was a higher percentage of males in the decubitus ulcer group (male 54.6%, female 45.4%) and the delirium group (male 56.1%, female 43.9%), but there was a higher percentage of females in the hypokalemia group (female 63.8%, male 36.2%) (p<0.0001).
The mean age was 70.1 years (±16.1) in the decubitus ulcer group, 73.8 years (±13.3) in the delirium group, and 64.4 years (±21.0) in the hypokalemia group. In all three groups, there were more older adults aged 65 years and over than those under 65 years, but the percentage of individuals under 65 years was higher in the hypokalaemia group compared to the other groups (p<0.0001).
In contrast to the general population, there were more patients admitted through the emergency department than through outpatient services in all three groups (p<0.0001), and national health insurance was the more common type of health insurance over medical aid (p<0.0001).
Regarding treatment outcomes, more people survived than those who died, but the percentage of deaths was higher in the decubitus ulcer group compared to the other two groups (p<0.0001).
The rate of surgery was the highest in the delirium group (p<0.0001), and LOS was the highest in the decubitus ulcer group (45.5±92.1 days), followed by the delirium group (27.9±36.9 days) and the hypokalemia group (18.7±28.4 days) (p<0.0001).
Distribution of Principal Diagnosis and Associations in the Decubitus Ulcer Group
The most frequently occurring principal diagnoses in the group of patients with a secondary diagnosis of decubitus ulcer was J18 (pneumonia, organism unspecified) (n=922, 8.87%), followed by J69 (pneumonitis due to solids and liquids) (n=437, 4.21%), I63 (cerebral infarction) (n=378, 3.64%), N39 (other disorders of the urinary system) (n=332, 3.20%), and A41 (other sepsis) (n=305, 2.94%). Approximately 47.93% of the patients in this group had one of the top 20 principal diagnoses (Table 2).
 |
Table 2 Top 20 Principal Diagnoses in the Group with a Secondary Diagnosis of Decubitus Ulcer and the Association Between a Decubitus Ulcer and Treatment Outcomes |
Regarding the association between a secondary diagnosis of decubitus ulcers and surgery among patients with one of the top 20 principal diagnoses, those who had a secondary diagnosis of decubitus ulcers had 1.566 to 7.876 times higher odds of surgery than those without a secondary diagnosis of decubitus ulcers (p<0.0001).
Regarding mortality risk, patients with one of the top 20 principal diagnoses (excluding G82 and I61) and a secondary diagnosis of decubitus ulcers had 1.523 to 39.085 times higher mortality risk than those without a secondary diagnosis of decubitus ulcers (p<0.0001).
Regarding LOS, patients with one of the top 20 principal diagnoses and a secondary diagnosis of decubitus ulcers had significantly longer LOS than those without a secondary diagnosis of decubitus ulcers (p<0.0001).
Distribution of Principal Diagnosis and Associations in the Delirium Group
The most frequently occurring principal diagnoses in the group of patients with a secondary diagnosis of delirium was S72 (fracture of femur) (n=425, 6.96%), followed by J18 (pneumonia, organism unspecified) (n=282, 4.62%), C34 (malignant neoplasm of bronchus and lung) (n=220, 3.60%), S06 (intracranial injury) (n=212, 3.47%), and I63 (cerebral infarction) (n=175, 2.87%). Approximately 44.78% of the patients in this group had one of the top 20 principal diagnoses (Table 3).
 |
Table 3 Top 20 Principal Diagnoses in the Group with a Secondary Diagnosis of Delirium and the Association Between Delirium and Treatment Outcomes |
Regarding the association between a secondary diagnosis of delirium and surgery among patients with one of the top 20 principal diagnoses, those with a secondary diagnosis of delirium had 1.633 to 3.679 times higher odds of surgery than those without a secondary diagnosis of delirium (p<0.0001).
Regarding mortality risk, patients with a principal diagnosis of C34, Z51, C22, or C16 and a secondary diagnosis of delirium had 2.935 to 16.991 times higher mortality risk than those without a secondary diagnosis of delirium. However, patients with a principal diagnosis of S06 or I61 had a lower mortality risk when they had a secondary diagnosis of delirium (p<0.0001).
Regarding LOS, patients with one of the top 20 principal diagnoses (excluding J69) and a secondary diagnosis of delirium had a significantly longer LOS than those without a secondary diagnosis of delirium (p<0.0001).
Distribution of Principal Diagnosis and Associations in the Hypokalemia Group
The most frequently occurring principal diagnoses in the group of patients with a secondary diagnosis of hypokalemia was J18 (n=244, 7.22%), followed by E87 (n=167, 4.94%), A09 (n=154, 4.56%), K70 (n=88, 2.61%), N39 (n=88, 2.61%), and N10 (n=84, 2.49%). Approximately 44.94% of the patients in this group had one of the top 20 principal diagnoses (Table 4).
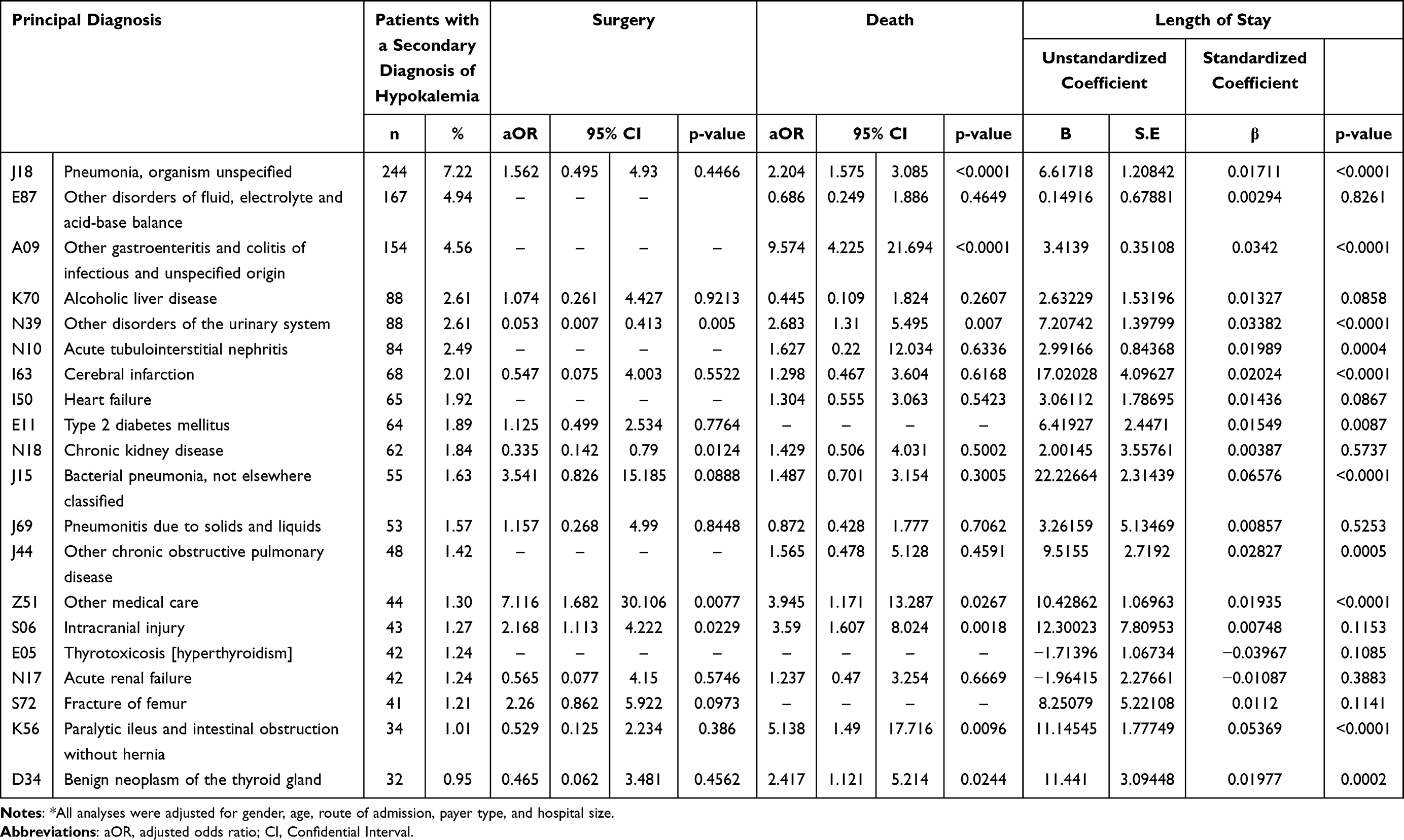 |
Table 4 Top 20 Principal Diagnoses in the Group with a Secondary Diagnosis of Hypokalemia and the Association Between Hypokalemia and Treatment Outcomes |
Regarding the association between a secondary diagnosis of hypokalemia and surgery, patients with a principal diagnosis of Z51 and S06 with a secondary diagnosis of hypokalemia had 7.116 times higher odds and 2.168 times higher odds of surgery, respectively, compared to those without a secondary diagnosis of hypokalemia. However, patients with a principal diagnosis of N39 or N18 had lower odds of surgery when they had a secondary diagnosis of hypokalemia (p<0.0001).
Regarding mortality risk, patients with a principal diagnosis of J18, A09, N39, Z51, S06, K56 or D34 and a secondary diagnosis of hypokalemia had 2.204–9.574 times higher mortality risk than those without a secondary diagnosis of hypokalemia (p<0.0001).
Among patients with a principal diagnosis of J18, A09, N39, N10, I63, E11, J15, J44, Z51, K56 and D34, those with a secondary diagnosis of hypokalemia had a significantly longer LOS than those without a secondary diagnosis of hypokalemia (p<0.0001).
Discussion
In this study, we chose delirium (F058, F059), decubitus ulcer (L89), and hypokalemia (E876) as diseases of interest, as they are three of the most common conditions with an N POA indicator in the new DRG, according to a previous study.10 We used the KNHDIS data for a 14-year period between 2006 and 2019 to identify the top 20 principal diagnoses with a secondary diagnosis code for one of the three conditions and compared death, surgery, and LOS according to the presence of these secondary diagnosis codes to explore the usefulness of these conditions as the targets of POA management. Comorbidities impact the severity and treatment outcomes of the principal diagnosis1 and the treatment process and required resources vary depending on the timing of their onset.34 Thus, diseases that influence treatment outcomes but are not present on admission must be managed as healthcare quality indicators.
The sociodemographic characteristics of patients who had additional diagnoses of decubitus ulcers, delirium, and hypokalemia were examined, and all three groups had a high proportion of patients aged 65 or older. This is attributable to the fact that these conditions are caused by chronic diseases prevalent among older adults,35 and delirium is a common postoperative complication in older patients.36,37 Therefore, intensive care with varying management timing is needed for older adults depending on their POA indicator. Furthermore, the rate of death was higher among patients with decubitus ulcers than those with delirium or hypokalemia. Decubitus ulcers tend to occur more in socially and economically vulnerable patients38,39 and they prolong the duration of treatment and increase the risk for sepsis, thereby elevating overall risk.40,41 Thus, decubitus ulcers require thorough management from the time of admission (if present on admission), and, if not present on admission, intensive nursing care and intervention protocol should be followed with patient monitoring to prevent this complication during hospital stays.42,43
Decubitus ulcers are defined as local injuries caused by disrupted blood flow to the skin or subcutaneous tissue as a result of continuous pressure on bony prominences.44 In particular, the prevalence of decubitus ulcers is rising owing to the increasing older adult population and prevalence of chronic diseases, consequently increasing relevant treatment cost.45 Accordingly, the need for a differentiated management system for decubitus ulcers according to onset timing before and after hospitalization has been emphasized.46,47 In this study, the differences comparison in the distribution of principal diagnoses between groups with and without decubitus ulcers as a secondary diagnosis showed that the group with decubitus ulcers as a secondary diagnosis had a higher prevalence of chronic diseases such as cerebral infarction, brain injury, and chronic renal disease. They also had 1.566 to 7.876 times higher odds of surgery and 1.523 to 39.085 times greater mortality risk compared to the group without decubitus ulcers. Additionally, LOS increased significantly in all of the patients with one of the top 20 principal diagnoses. This suggests that decubitus ulcers are a meaningful indicator of patient safety and healthcare quality and are a viable target disease for POA management.48–50
The most common principal diagnosis for patients with delirium as a secondary diagnosis was surgery due to femoral fracture (6.96%). This is similar to previous results, which show that delirium is more common in postoperative older adult patients and that femoral fracture is a common type of fracture among older adults.37,51,52 Prompt treatment is crucial to prevent or minimize the adverse consequences of postoperative delirium, which is a form of cerebral dysfunction that occurs postoperatively.53 Therefore, delirium is an important target disease for POA management and is a useful patient safety and healthcare quality indicator, especially for older adult surgical patients. Additionally, we compared the mortality rates between the groups with and without delirium as a secondary diagnosis among those with one of the top 20 principal diagnoses and observed that patients with lung cancer had a 2.935 to 16.991 times higher mortality risk and longer LOS when they had delirium as a secondary diagnosis. This supports previous findings that delirium is an indicator requiring management.54,55
Potassium is the most abundant electrolyte inside cells, and hypokalemia refers to a state in which the serum potassium level drops below normal. Potassium must be consumed through food, and since it is abundant in the gastrointestinal tract, hypokalemia can occur from malnutrition, osmotic diuresis, insulin excess, and gastrointestinal fluid loss caused by vomiting and diarrhea. It is often asymptomatic but can affect cardiac function, making its diagnosis and treatment important.56 Further, hypokalemia is common postoperatively, particularly as a common complication following total thyroidectomy.53 In this study, the top 20 principal diagnoses among patients with a secondary diagnosis of hypokalemia included gastrointestinal disorders and thyroid cancer. In this group, the odds of surgery, LOS, and mortality risk differed according to the presence of hypokalemia as a secondary diagnosis, with the hypokalemia group having 2.204 to 9.574 times higher mortality risk than those without hypokalemia. Given that hypokalemia impacts the severity of the patient’s condition and frequently occurs postoperatively, that is, during the treatment process, hypokalemia should be managed as a target for POA management and as a healthcare quality indicator.57
The results of this study demonstrated that treatment outcomes, odds of surgery, and LOS differed according to the presence of decubitus ulcers, delirium, or hypokalemia as a secondary diagnosis flagged with an N POA indicator among patients with one of the top 20 principal diagnoses. The results highlighted that decubitus ulcers, delirium, and hypokalemia are significant target diseases for POA management. However, we could not monitor the accuracy of disease coding for discharged patients reported in the KNHDIS data owing to the extensive dataset spanning 16 years. Additionally, we could not comparatively analyze the diseases of interest according to the N POA indicator, that is, the timing of onset, owing to the limited availability of study data. Therefore, we investigated the usefulness of these diseases as targets of POA management and healthcare quality indicators by comparing the differences according to the presence of these diseases as a secondary diagnosis.
Conclusion
Our findings showed that decubitus ulcers, delirium, and hypokalemia are common conditions that arise postoperatively or during hospital stays. As such, patients with one of the top 20 principal diagnoses have increased mortality risk, surgery risk, and LOS when one of these three conditions is a secondary diagnosis. As decubitus ulcers, delirium, and hypokalemia are linked to the severity of the principal diagnosis, these conditions should be designated as target diseases for POA management for monitoring. Ultimately, they will be useful as healthcare quality indicators. Our findings provide useful foundational data for selecting target diseases for POA monitoring and healthcare quality indicators.
Ethics Statement
This study was conducted in compliance with Declaration of Helsinki, and performed in accordance with national ethics regulation. It was also approved by the Institutional Review Board of Eulji University of South Korea (IRB no. EUIRB2023-002).
Informed Consent Statement
The Korean National Hospital Discharge In-depth Injury Survey data provided by the Korea Disease Control and Prevention Agency did not include patient personal information, identification information, or institutional information, hence, patient consent was not required. All data accessed complied with relevant data protection and privacy regulations.
Acknowledgments
The authors would like to thank the Korean Disease Control and Prevention Agency and Eulji University.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. RS-2022-00165715).※ MSIT: Ministry of Science and ICT.
Disclosure
The authors have no conflicts of interest to declare for this study.
References
1. Lee K, Hong K, Kang S, Hwang J. Characteristics and epidemiology of discharged pneumonia patients in South Korea using the Korean National Hospital Discharge In-Depth Injury Survey Data from 2006 to 2017. Infect Dis Rep. 2021;13(3):730–741. doi:10.3390/idr13030068
2. Lee K, Kang S, Hwang J. Lung cancer patients’ characteristics and comorbidities using the Korean National Hospital Discharge In-depth Injury Survey Data. J Epidemio Glob Health. 2022;12(3):258–266. doi:10.1007/s44197-022-00044-6
3. Sanyaolu A, Okorie C, Marinkovic A, et al. Comorbidity and its impact on patients with COVID-19. SN Compr Clin Med. 2020;2:1069–1076. doi:10.1007/s42399-020-00363-4
4. Bohn MK, Hall A, Sepiashvili L, Jung B, Steele S, Adeli K. Pathophysiology of COVID-19: mechanisms underlying disease severity and progression. Physiology. 2020;35(5):288–301. doi:10.1152/physiol.00019.2020
5. Long B, Brady WJ, Koyfman A, Gottlieb M. Cardiovascular complications in COVID-19. AM J Emerg Med. 2020;38(7):1504–1507. doi:10.1016/j.ajem.2020.04.048
6. McLoughlin V, Millar J, Mattke S, et al. Selecting indicators for patient safety at the health system level in OECD countries. Int J Qual Health Care. 2006;18(Suppl 1):14–20. doi:10.1093/intqhc/mzl030
7. Bahl V, Thompson MA, Kau T-Y, Hu HM, Campbell DA Jr. Do the AHRQ patient safety indicators flag conditions that are present at the time of hospital admission? Med Care. 2008;46(5):516–522. doi:10.1097/MLR.0b013e31815f537f
8. Barbara L, Vanda R, Quinto T, Giovanni C, Sieds KN, Fabrizio C. Patient safety monitoring in acute care in a decentralized national health care system: conceptual framework and initial set of actionable indicators. J Patient Saf. 2022;18(2):e480–e488. doi:10.1097/PTS.0000000000000851
9. Drösler SE, Romano PS, Tancredi DJ, Klazinga NS. International comparability of patient safety indicators in 15 OECD member countries: a methodological approach of adjustment by secondary diagnoses. Health Serv Res. 2012;47(1pt1):275–292. doi:10.1111/j.1475-6773.2011.01290.x
10. Lee S, Kim S, Ok M, et al. Present on admission (POA) collection and utilization. Seoul: Health Insurance Review and Assessment Service;. 2019.
11. Cafardi S, Healy D, Cromwell J. Hospital-Acquired Conditions–Present on Admission: Examination of Spillover Effects and Unintended Consequences. Washington D.C: U.S. Department of Health & Human Services; 2012.
12. McNair PD, Luft HS, Bindman AB. Medicare’s policy not to pay for treating hospital-acquired conditions: the impact. Health Aff. 2009;28(5):1485–1493. doi:10.1377/hlthaff.28.5.1485
13. Nero DC, Lipp MJ, Callahan MA. The financial impact of hospital-acquired conditions. J Health Care Finance. 2012;38(3):40–49. PMID: 22515043
14. Hwang S, Kim M, Oh D, Park C. Development and management of system to collect data for evaluation of appropriateness of reimbursement. Seoul: Health Insurance Review and Assessment Service; 2017.
15. Shon C, You M. Evaluation of health policy governance in the introduction of the new DRG-based hospital payment system from interviews with policy elites in South Korea. Int J Environ Res Public Health. 2020;17(11):3757. doi:10.3390/ijerph17113757
16. Kim J, Choi EY, Lee W, et al. Feasibility of capturing adverse events from insurance claims data using international classification of diseases, tenth revision, codes coupled to present on admission indicators. J Patient Saf. 2022;18(5):404–409. doi:10.1097/PTS.0000000000000932
17. Chung S. The Analysis of Changes in Coding Practices Before and After the Introduction of the Reporting System for Present on Admission [Dissertation]. Graduate School of Public Health, Yonsei University; 2020.
18. Kim N, Hwang J, Park S, Chae S, Choi Y. Feasibility of using administrative data to compare healthcare-associated infection performance. Seoul. Health Society Welfare Rev. 2017;37(3):495–518. doi:10.15709/hswr.2017.37.3.495
19. Park C. Production and development of 2011 OECD healthcare quality indicators. Seoul: Health Insurance Review and Assessment Service; 2013.
20. Pyo J, Choi E, Oh H, et al. Perceptions of hospital health information managers regarding present on admission indicators in Korea: a qualitative study. Qual Improv Health Care. 2020;26(1):23–34. doi:10.14371/QIH.2020.26.1.23
21. Ghazvinian R, White RH, Gage BF, Fang MC, Saeed R, Khanna RR. Predictive value of the present-on-admission indicator for hospital-associated hemorrhage. Thromb Res. 2019;180:20–24. doi:10.1016/j.thromres.2019.05.014
22. Khanna RR, Kim SB, Jenkins I, et al. Predictive value of the present-on-admission indicator for hospital-acquired venous thromboembolism. Med Care. 2015;53(4):e31–e6. doi:10.1097/MLR.0b013e318286e34f
23. Fokkema M, Hurks R, Curran T, et al. The impact of the present on admission indicator on the accuracy of administrative data for carotid endarterectomy and stenting. J Vasc Surg. 2014;59(1):32–38. e1. doi:10.1016/j.jvs.2013.07.006
24. Koch CG, Li L, Sun Z, et al. Hospital‐acquired anemia: prevalence, outcomes, and healthcare implications. J Hosp Med. 2013;8(9):506–512. doi:10.1002/jhm.2061
25. Koch CG, Li L, Sun Z, et al. From bad to worse: anemia on admission and hospital-acquired anemia. J Patient Saf. 2017;13(4):211–216. doi:10.1097/PTS.0000000000000142
26. Triche EW, Xin X, Stackland S, et al. Incorporating present-on-admission indicators in Medicare claims to inform hospital quality measure risk adjustment models. JAMA Netw Open. 2021;4(5):e218512–e. doi:10.1001/jamanetworkopen.2021.8512
27. Maurici M, Rosati E. Development of classification and payment system of in patient hospital admissions in the United States: introduction of Medicare Severity Diagnosis-Related Groups (MS-DRGs) and the present on admission (POA) indicator. Ig Sanita Pubbl. 2007;63(6):691–701. PMID: 18216884
28. Hughes JS, Averill RF, Goldfield NI, et al. Identifying potentially preventable complications using a present on admission indicator. Health Care Financ Rev. 2006;27(3):63. PMID: 17290649
29. Fuller RL, McCullough EC, Bao MZ, Averill RF. Estimating the costs of potentially preventable hospital acquired complications. Health Care Financ Rev. 2009;30(4):17. PMID: 19719030
30. Goldman LE, Chu PW, Osmond D, Bindman A. The accuracy of present‐on‐admission reporting in administrative data. Health Serv Res. 2011;46(6pt1):1946–1962. doi:10.1111/j.1475-6773.2011.01300.x
31. Bharmal A, Wilson R, Winters BD. Erratum: validity of the agency for healthcare research and quality patient safety indicators and the centers for medicare and medicaid hospital-acquired conditions: a systematic review and meta-analysis. Med Care. 2016;54(12):1105–1111. doi:10.1097/MLR.0000000000000550
32. Triep K, Beck T, Donzé J, Endrich O. Diagnostic value and reliability of the present-on-admission indicator in different diagnosis groups: pilot study at a Swiss tertiary care center. BMC Health Serv Res. 2019;19(1):1–10. doi:10.1186/s12913-018-3858-3
33. Jarrett N, Callaham M, Jarrett N. Evidence-based guidelines for selected hospital-acquired conditions. CMS Contract GS-10F-0097L, RTI International. International Nursing Review. 2016;63(1):78–83. doi:10.1111/inr.12203
34. Dadson P, Tetteh CD, Rebelos E, Badeau RM, Moczulski D. Underlying kidney diseases and complications for COVID-19: a review. Front Med. 2020;7:600144. doi:10.3389/fmed.2020.600144
35. Alderden J, Rondinelli J, Pepper G, Cummins M, Whitney J. Risk factors for pressure injuries among critical care patients: a systematic review. Int J Nurs Stud. 2017;71:97–114. doi:10.1016/j.ijnurstu.2017.03.012
36. Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. The Lancet. 2014;383(9920):911–922. doi:10.1016/S0140-6736(13)60688-1
37. Park E, Kim M. Postoperative delirium in elderly patients with osteoarthritis surgery: incidence and risk factors. J Muscle Jt Health. 2015;22(2):57–66. doi:10.5953/JMJH.2015.22.2.57
38. Kim GH, Lee JY, Kim J, Kim HJ, Park J-U. Prevalence of pressure injuries nationwide from 2009 to 2015: results from the National Inpatient Sample Database in Korea. Int J Environ Res Public Health. 2019;16(5):704. doi:10.3390/ijerph16050704
39. Lee J-H. Socioeconomic effects of pressure ulcer. J Korean Med Assoc. 2021;64(1):11–15. doi:10.5124/jkma.2021.64.1.11
40. Jeong HS, Lee BH, Lee HK, Kim HS, Moon MS, Suh IS. Negative pressure wound therapy of chronically infected wounds using 1% acetic acid irrigation. Arch Plast Surg. 2015;42(01):59–67. doi:10.5999/aps.2015.42.1.59
41. Shin JH, Hong IP, Park CG, Chung CM. A modified total thigh flap in the reconstruction of decubitus ulcer. Arch Plast Surg. 2014;41(04):440–442. doi:10.5999/aps.2014.41.4.440
42. Taylor VE. Decubitus Prevention Through Early Assessment. NJ: SLACK Incorporated Thorofare; 1980:389–391.
43. Sriwulaningdyah M, Wahyunu ED. The development of a six sigma-based ulcus decubitus prevention model to respond to adverse events. Journal Ners. 2017;12:219–224. doi:10.20473/jn.v12i2.5241
44. Seoul National University Hospital. Homepage on the Internet 2023. Available from: http://www.snuh.org/health/nMedInfo/nView.do?category=DIS&medid=AA000555.
45. Healthcare Bigdata Hub. Homepage on the Internet 2023; Availabel from: http://opendata.hira.or.kr.
46. Pachá HHP, Faria JIL, KAd O, Beccaria LM. Pressure ulcer in intensive care units: a case-control study. Rev Bras Enferm. 2018;71:3027–3034. doi:10.1590/0034-7167-2017-0950
47. Lee M, Seo E, Kim M, et al. Differences in associated factors according to the time of occurrence of pressure ulcers in intensive care unit. J Korean Crit Care Nurs Vol. 2021;14(3):26–36. doi:10.34250/jkccn.2021.14.3.26
48. Cho BK, Ko Y, Kwak C. Risk factors of severity of pressure injuries in acute university hospital inpatients. J Converg Inf Technol. 2020;10(11):98–106. doi:10.22156/CS4SMB.2020.10.11.098
49. Galpin JE, Chow AW, Bayer AS, Guze LB. Sepsis associated with decubitus ulcers. Am J Med. 1976;61(3):346–350. doi:10.1016/0002-9343(76)90371-5
50. Eachempati SR, Hydo LJ, Barie PS. Factors influencing the development of decubitus ulcers in critically ill surgical patients. Crit Care Med. 2001;29(9):1678–1682. doi:10.1097/00003246-200109000-00004
51. Leung JM, Tsai TL, Sands LP. Preoperative frailty in older surgical patients is associated with early postoperative delirium. Anesth Analg. 2011;112(5):1199. doi:10.1213/ANE.0b013e31820c7c06
52. Lee K, Hwang J. The association between comorbidities and comorbid injuries on treatment outcome in pediatric and elderly patients with injuries in Korea: an observational study. Int J Environ Res Public Health. 2022;19(10):6277. doi:10.3390/ijerph19106277
53. Reddy SV, Irkal JN, Srinivasamurthy A. Postoperative delirium in elderly citizens and current practice. J Anaesthesiol Clin Pharmacol. 2017;33(3):291. doi:10.4103/joacp.JOACP_180_16
54. Elie M, Cole MG, Primeau FJ, Bellavance F. Delirium risk factors in elderly hospitalized patients. J Gen Intern Med. 1998;13(3):204–212. doi:10.1046/j.1525-1497.1998.00047.x
55. Pandharipande P, Cotton BA, Shintani A, et al. Prevalence and risk factors for development of delirium in surgical and trauma ICU patients. J Trauma. 2008;65(1):34. doi:10.1097/TA.0b013e31814b2c4d
56. Asan Medical Center. Homepage on the Internet 2023. Available from https://www.amc.seoul.kr/asan/healthinfo/disease/diseaseDetail.do?contentId=32306.
57. Liu J, Han P, Wu J, Gong J, Tian D. Prevalence and predictive value of hypocalcemia in severe COVID-19 patients. J Infect Public Health. 2020;13(9):1224–1228. doi:10.1016/j.jiph.2020.05.029
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.