Back to Journals » Local and Regional Anesthesia » Volume 15
The Use of a New Device-Assisted Needle Guidance versus Conventional Approach to Perform Ultrasound Guided Brachial Plexus Blockade: A Randomized Controlled Study
Authors Vydyanathan A ![]() , Agrawal P
, Agrawal P ![]() , Shetty N, Nair S, Shilian N, Shaparin N
, Shetty N, Nair S, Shilian N, Shaparin N ![]()
Received 4 March 2022
Accepted for publication 6 July 2022
Published 25 July 2022 Volume 2022:15 Pages 61—69
DOI https://doi.org/10.2147/LRA.S363563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Stefan Wirz
Amaresh Vydyanathan,1 Priya Agrawal,2 Naveen Shetty,3 Singh Nair,1 Nancy Shilian,4 Naum Shaparin1
1Department of Anesthesiology and Pain Management, Montefiore Medical Center, Bronx, NY, USA; 2Sutter Health System, Oakland, CA, USA; 3Department of Anesthesiology, New York University, New York, NY, USA; 4Department of Family Medicine, Mount Sinai South Nassau Hospital, Oceanside, NY, USA
Correspondence: Amaresh Vydyanathan, 1250 Waters Place, Tower II, 8th Floor, Bronx, NY, USA, Tel +216-702-5965, Fax +929-263-3950, Email [email protected]
Purpose: Ultrasound guidance during nerve blockade poses the challenge of maintaining in-plane alignment of the needle tip. The needle guidance device maintains needle alignment and assists with in-plane needle visualization. The purpose of this study is to evaluate the utility of this device by comparing procedure performance during brachial plexus blockade with the conventional approach.
Methods: After the Institutional Review Board approval and obtaining informed consent, 70 patients receiving either interscalene or supraclavicular nerve blocks were randomly assigned into 2 groups, a conventional approach versus utilizing the needle guidance device. An independent observer recorded: total procedure time; needle insertion time; number of unplanned redirections; and number of reinsertions. Additionally, physician satisfaction and ease of needle visualization were assessed.
Results: Data from seventy patients were analyzed. The median [25th percentile-75th percentile] time to complete the block by the device assisted needle guidance group was 3 (2– 3.75) minutes and 4 (3– 6) minutes in the conventional approach group (p < 0.001). Additionally, subgroup analyses were performed in the supraclavicular block and interscalene block. Supraclavicular blockade, needle insertion time (median [25th percentile-75th percentile] in seconds) (106 [92– 162] vs 197 [140– 278]), total procedure time (3 [2– 3] vs 4.5 [4– 6] in minutes) and unplanned needle redirections (2 [1– 5] vs 5.5 [3– 9]) were significantly lower in needle guidance group (p < 0.001). With interscalene blockade, needle insertion time (86 [76– 146] vs 126 [94– 295]) and unplanned needle redirections (2 [1– 3] vs 4 [2– 8.5]) were significantly lower with needle guidance (p < 0.001), but total procedure time was similar. All the physicians reported that they would use the needle guidance again, and 90% would prefer it for in-plane blocks.
Conclusion: Performing regional blocks using the needle guidance device reduces needle insertion time and unplanned needle redirections in brachial plexus blockade. Moreover, physician satisfaction also improved compared to the use of the conventional technique.
Keywords: brachial plexus blockade, ultrasound guidance, peripheral nerve blockade, needle guidance, needle visualization
Introduction
Regional anesthetic techniques utilized in perioperative blockade of peripheral nerves are invasive and, while exceedingly rare, carry the risk of complications, including hematoma formation, infection, pneumothorax, and neural injury. Peripheral nerve blocks in particular, have the highest incidence of local anesthetic systemic toxicity (7.5 per 10,000).1 Moreover, these interventions can also be uncomfortable for patients. Nowadays, most of these interventions are being performed using ultrasound guided approaches, which have been associated with excellent patient outcomes and improved patient satisfaction.2,3
Primarily, two techniques of needle insertion are used to perform ultrasound guided peripheral nerve blockade, the in-plane technique, and the out-of-plane technique. The in-plane technique is often preferred due to its ease of needle visualization, and perceived improvement in safety, in comparison to the out-of plane technique. Simulated models have demonstrated improved visibility of the needle tip using the in-plane approach.4 An essential requirement in ultrasound guided needle placement is the complete visualization of the needle, especially the needle tip. While the in-plane technique eases needle tip visualization, this can nevertheless be challenging for many practitioners of regional anesthesia and could increase the duration of the procedure. Moreover, in our experience, many practitioners utilize multiple passes and needle reinsertions to maintain this alignment, thereby increasing patient discomfort.
Recently, a new device that assists in-plane needle visualization has become available. The new needle guidance device (InfinitiPlusTM, CIVCO Medical Solutions, Kalona, IA, USA) attaches to the ultrasound probe and maintains needle alignment in the in-plane technique, thus potentially increasing the ease of intervention, and possibly allowing for greater patient comfort and safety (Figure 1). A central venous catheter study reported superior placement of the needle and better satisfaction rate among the providers.5 Another study evaluating femoral nerve catheter placement showed reduced procedure time to perform ultrasound-guided femoral nerve catheter placement when using the needle guidance device.6 A prospective randomized trial compared the use of this device vs freehand technique in performing ultrasound guided transversus abdominis plane blocks and reported improved needle tip visibility, procedure time and proceduralist satisfaction when using the device7 However, no study has yet evaluated the benefits of using the needle guide device in performing upper extremity regional anesthetic interventions.
 |
Figure 1 Needle guidance device attached to the sterile probe cover. |
In this study, we evaluated the use of needle guidance as it pertains to needle visualization and duration of the procedure. We hypothesized that using the device would allow for faster procedure time, with less needle redirections, compared to the conventional method. The study’s primary endpoint was the needle insertion time (in seconds) taken to complete upper extremity blocks, with and without a needle guidance device. A post-procedure survey was provided to all clinicians to assess overall satisfaction with the device.
Materials and Methods
This randomized controlled parallel-group study was conducted at Montefiore Medical Center of the Albert Einstein College of Medicine in Bronx, New York. This study evaluated the effectiveness of using a guided approach versus the conventional approach in performing brachial plexus blockade. Subjects of this study were patients scheduled for upper extremity surgeries requiring supraclavicular and interscalene brachial plexus blocks at Montefiore Medical Center sites. After obtaining institutional review board approval (Albert Einstein College of Medicine of Yeshiva University/Montefiore Medical Center IRB# 2014–3414) and obtaining informed consent, 70 patients (enrolled between January 2015 and June 2015) scheduled to receive either block were randomly assigned into 2 groups, one using the conventional approach and the other utilizing the needle guidance device (Figure 2).
 |
Figure 2 Methodology of study showing distribution of subjects in each group. |
Clinician Volunteers
Residents (CA-2 and CA-3), attendees, and fellows involved in performing regional anesthesia were study participants if they were assented (Table 1). All participants were given ample time to familiarize themselves with the device before performing the blocks. The company manufacturing this device conducted periodic in-service training on the device. Additionally, the PI of the study was a certified trainer for additional support. Residents who declined to participate in the study continued to perform the blocks as per the standard of care at our institution.
 |
Table 1 Breakdown of Clinician Experience of Participants |
Study participants were randomly assigned to either perform the block under device guidance or use a conventional technique. Each participant performed one interscalene block with the device, one without the device, and/or one supraclavicular block with the device and one without.
Study Protocol
The guidance device (Infiniti TM, CIVCO Medical Solutions, Kalona, IA, USA) consists of a custom reusable bracket attached to an ultrasound transducer. A disposable snap-on needle guide is then attached to the sterile transducer cover.
Attending regional anesthesia physicians called the patients in advance. Participation was voluntary; an alternative option for the patient was to receive the brachial plexus block with no guidance device, which was the standard of care. Subsequently, a written informed consent was also obtained on the day of surgery. All the brachial plexus blocks were single-injection blocks utilizing the in-plane technique for needle insertion, which is the usual protocol at our institution.
Randomization
This was an openly randomized controlled study. We used randomization.com, a freely available online software to generate the randomization list. Randomization was maintained by a member of the research team who was not involved with any study-related activities. After each patient was evaluated prior to the block, individual, sealed envelopes containing patient randomization were given to the person performing the block. A stratified randomization approach was used to assign the participants to the two types of blocks. Stratification was based on their year of residency (as this denotes their familiarity with these blocks) and the brachial plexus block to be performed. For attending anesthesiologists, stratification was based only on the brachial plexus block performed.
Measurements
An independent observer was present during all cases and was responsible for recording: needle insertion time, total procedure time, number of needle redirections (planned and unplanned), and number of needle reinsertions. Needle insertion time was defined as the time from when the needle is inserted to when it is removed. Total procedure time was defined as the time from the start of prep through the end of the dressing, including the time to set up the needle guidance system. The number of needle reinsertions was defined as the number of times when the needle was removed above the skin and then reinserted. The observer also administered a satisfaction questionnaire to the participants after they completed the block. Efficacy of the block was assessed by the standard of care practiced at our center. Finally, clinicians were given questionnaires to fill out immediately after performing the block (Supplementary Material).
Inclusion and Exclusion Criteria
Our study’s inclusion criteria included patients who were as follows: ≥18 years old, receiving upper extremity surgery that required interscalene or supraclavicular blockade, ASA 1–3, and the ability to understand and complete the informed consent.
Our exclusion criteria included patients who: refused regional anesthesia, had contraindications to regional anesthesia, had anatomical or neurological disorders, or had any other conditions that the anesthesiologist felt could complicate performing the block.
Calculation of Sample Size
The study’s primary endpoint was the needle insertion time taken to complete upper extremity blocks, with and without a needle guidance device. This was calculated in seconds and was considered a continuous variable. In our institution, the needle insertion time taken to conduct supraclavicular blocks is about 120 seconds, with a standard deviation of 40 seconds. We assumed that using the device guidance would decrease this time by 30%.8 As such, we needed 24 subjects in the experimental (needle guidance group) and 24 in the control group (no needle guidance group) to reject the null hypothesis with a power of 0.80. Interscalene blocks take a longer time to perform when compared to supraclavicular blocks. In our institution, the time taken to conduct interscalene blocks is about 180 seconds, with a standard deviation of 40 seconds. In order to reject the null hypothesis with a power of 0.80, we needed 11 subjects in the experimental group and 11 subjects in the control group. The type I error associated with the test of this null hypothesis is 0.05. The total sample size for this study was 70 subjects (35 guided and 35 freehand). Considering the immediate outcome endpoints of the study, we did not anticipate any withdrawal of subjects from the study.
Statistical Analysis
All the analysis was performed as an intention-to-treat analysis. Standard descriptive statistics, such as mean± standard deviation, median (25th–75th percentile), and proportions, were used to explain demographic and clinical characteristics. After assessing the normality of the data, quantitative variables were compared using Mann Whitney U-test. A Chi-square test or Fisher’s exact tests was used for the comparison of categorical outcomes. All significance tests were two-tailed, and values of p < 0.05 were considered to be statistically significant.
Results
A total of fifteen residents participated in the study; 4 of whom were CA-2ʹs and 11 of whom were CA-3ʹs. Regional fellows and attending anesthesiologists also participated in the study. The breakdown of the clinician experience is demonstrated in Table 1.
Among the seventy patients enrolled, 35 patients were randomized to the needle guidance group and 35 patients to the conventional approach group. Baseline patient characteristics were similar in the two groups (Table 2). The breakdown of patients in each group is shown in Figure 2.
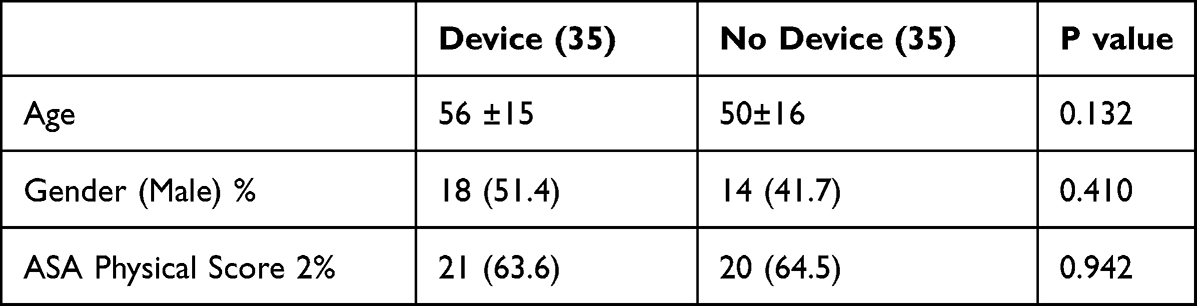 |
Table 2 Baseline Patient Characteristics Undergoing Brachial Plexus Blockade |
The study’s primary objective, the time taken to complete the block, was significantly different between the needle guidance group vs the conventional approach group. The median [25th percentile-75th percentile] time to complete the block by the needle guidance group was 3 (2–3.75) minutes and 4 (3–6) minutes in the conventional approach group (p < 0.001). Similarly, the number of unplanned re-directions were lower in the needle guidance group: 5 (3–9) in the guidance group and 2 (1–3) in the conventional approach group (p < 0.001).
In the supraclavicular group, the needle insertion time (median [25th percentile–75th percentile] in seconds) (106 [92–162], vs 197 [140–278]), total procedure time (3 [2–3] vs 4.5 [4–6] in minutes), and unplanned redirections (2 [1–5] vs 5.5 [3–9]) were all significantly less in the needle guidance group vs the conventional approach group (p < 0.001 Table 3).
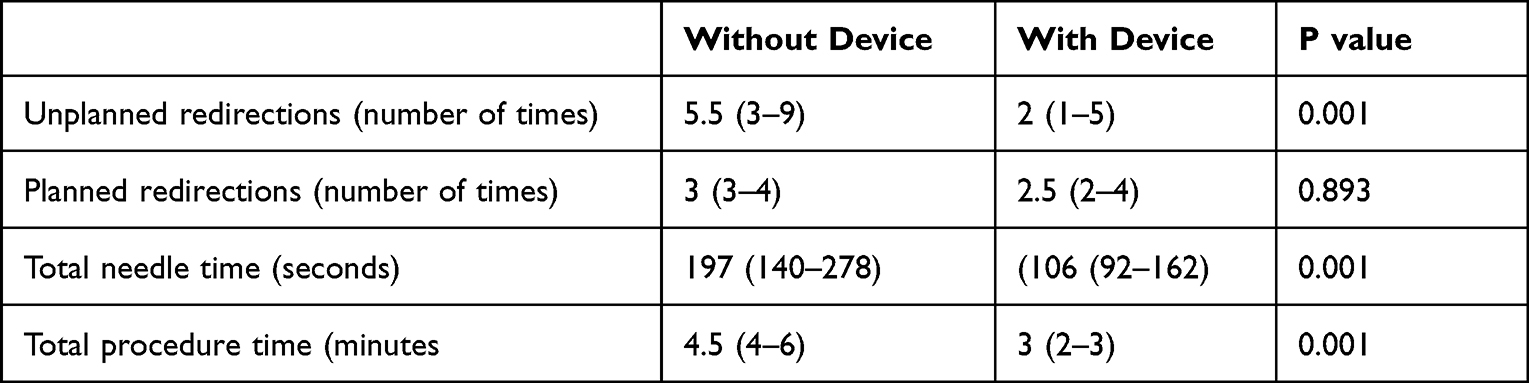 |
Table 3 Block Performance Data for Supraclavicular Brachial Plexus Block in Study (Data Presented as Median (25th and 75th Percentile) Analyzed Mann Whitney U-Test) |
In the interscalene group, the needle insertion time (86 [76–146] vs 126 [94–295]) and the unplanned needle redirections (2 [1–3] vs 4 [2–8.5]) was significantly less in the needle guidance group compared to the standard group (p < 0.001), but there was no difference in the total procedure time (p-0.33 (Table 4)).
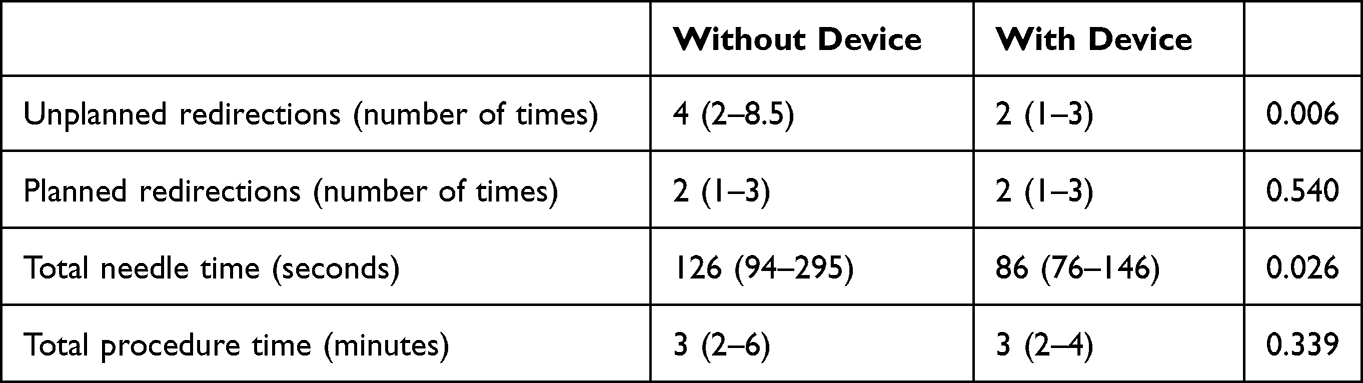 |
Table 4 Block Performance Data for Interscalene Brachial Plexus Block in Study (Data Presented as Median (25th and 75th Percentile) Analyzed Mann Whitney U-Test) |
The incidence of needle reinsertion did not differ significantly between the groups, however in the supraclavicular group, reinsertion percentages were 27.8% and 5.3% in the no device and device group, respectively (p-0.063). 100% of the physicians reported that they would use the needle guidance again, and 90% reported that they would prefer it in all in-plane blocks.
Among the physicians who responded to the survey question regarding the ease of the set-up of the device, 96–97% of correspondents reported that the device was “easy to set up”, and “easy to use.” This was defined as a score of 3/5 or greater on the survey. The response given for “how much did it reduce image quality” was (4.22 [0.82]) (mean [SD]). The lowest response was given for “how much did it reduce the amount of needle manipulations” (2.47 [1.12]) (Figure 3).
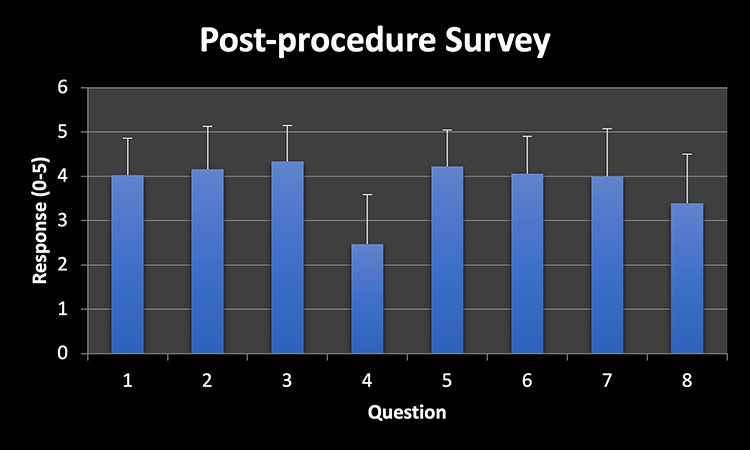 |
Figure 3 Post-procedure survey responses shown in a bar chart. (Post-procedure survey included in Supplementary Material). |
Of note, in the supraclavicular group, one instance of local anesthetic toxicity occurred in the conventional approach group. The patient had seizures that resolved with lipid infusion, and the patient was able to have surgery and recovered uneventfully.
Discussion
In this single-center randomized controlled study, we have demonstrated the utilization of a needle guidance device in performing regional blocks. The results are particularly favorable for the supraclavicular block performance.
The use of ultrasound guided peripheral nerve blocks has become ubiquitous. Two approaches have been used when performing these procedures: the in-plane and the out-of-plane approaches. Visualization of the needle tip is an important aspect of patient safety, as to avoid inadvertent injury of nearby structures.
Several studies have investigated methods for improving needle tip visualization during ultrasound guidance. An in-vitro study showed that echogenic needle tips have a limited role in enhancing needle visualization, and optimization of conditions prior to performing the procedure provides more benefit.9 Other studies have shown that using large bore needles with medium-sized guide wires improved visibility, while water priming the needle, insulation, and insertion of a stylet do not.10
Although the in-plane approach requires skill from the operator, it may improve visualization of the needle tip. A study of emergency medicine residents obtaining vascular access showed that they were more likely to identify the needle tip during vessel puncture in the long axis approach.11 Nonetheless, the need to maintain proper alignment of the needle and ultrasound probe remains a challenge during these procedures. A study of novice emergency medicine residents showed increased procedure time when using the long axis method while obtaining vascular access.12 However, there remains a paucity of literature pertaining specifically to peripheral nerve blocks and improving needle visualization during the long axis approach.
A new needle guidance device (InfinitiTM, CIVCO Medical Solutions, Kalona, IA, USA) has recently been introduced, and provides a way to maintain needle alignment with the ultrasound probe. The use of this device was previously studied for obtaining central venous access,13 where it improved visualization of the needle compared to the free hand technique. This study is the first randomized controlled trial assessing improvement in upper extremity nerve block performance using this device.
Our study demonstrated that the device group had improved needle insertion times, total procedure times, and less unplanned redirections for the supraclavicular block. For the interscalene block, the device group showed an improvement in needle insertion time and less unplanned redirections. Given these data, we found that the device improves the practitioner’s performance of the regional block, particularly in terms of needle insertion times and reduced unplanned redirections. We surmise that this is likely to improve patient comfort during the procedure.
Nerve injury, while exceedingly rare, remains a devastating complication of peripheral nerve blockade. Pascarella et al noted the potential value of a triple monitoring technique in reducing nerve needle contact.14 One of the components is ultrasound guided needle visualization, which the needle guide could embellish. In our study, we noted no difference in block success or incidence of complications, but this is expected given the high success rate of these blocks and very low complication rate. Of note, one major complication did occur in the conventional approach group, though it was successfully managed.
The device seems to provide more of a benefit when using the supraclavicular approach to brachial plexus blockade as compared to the interscalene approach. This may be due to the fact that the supraclavicular approach requires a relatively steeper angle of needle insertion and relatively longer distance for needle to travel, allowing for greater opportunity to lose sight of the needle tip. Moreover, the construction of the needle guidance device allows better needle manipulation when the needle insertion angle is not too superficial. Thus, device-assisted needle guidance may be especially beneficial targeting nerves that are not too superficial.
Through the post-procedure questionnaire, clinicians expressed overall satisfaction with the device. Of note, respondents did not seem to think that the device reduced the number of needle manipulations. This is surprising, given our quantitative data, which show a significant decrease in redirections. This could be due to the fact that the clinician was so focused on using the device properly that they did not notice their manual manipulations. Furthermore, respondents reported that the device reduced the image quality “very much.” However, we feel that the incongruency in the recorded responses to this question may be due to a misunderstanding of the grading system, as the grading system for this question alone is reversed relative to all the other questions.
A limitation of this study was that most of the clinicians using the device were either senior residents (CA-3ʹs), or fellows. It is possible that this device could provide more benefit to newer trainees; as such, further studies should stratify resident experience while using the device. We were also under-powered to study any significant difference in block success or complication rate, including potential nerve injury, between the groups. Further, given that all patients received sedation for the block and subsequently general anesthesia or deep sedation, there was no direct measurement of patient satisfaction. Thus, the advantages of using the needle guidance device are mainly perceived as improvements in block times and patient comfort given the reduction in unplanned redirections. Finally, instead of 24 patients, we only recruited 18 patients in the supraclavicular group. However, based on the observed time difference between the groups in the supraclavicular block, the study’s conclusions are unlikely to change even with enrolling the calculated sample size.
A common concern when new technology is introduced to improve the ease of a procedure is the cost and the thought that physicians may become reliant on these new devices. The cost of the device is twofold; the cost of the reusable bracket that fits on the probe (For the Sonosite probe used in the study, this cost was $450) and the cost of the kits with the disposable needle guides (This cost is $400–450 for a pack of 24 kits). It is also important for residents to gain an appreciation for and expertise in the hand eye coordination needed for the free hand technique. Nonetheless, this device provides a method for novice and experienced practitioners to further advance their skillset, and possibly provide a safer, more comfortable block to their patients.
Conclusion
Performing regional blocks using the needle guidance device reduces the total needle insertion time and unplanned needle redirections in supraclavicular and interscalene blocks, but total procedure time is only reduced in the supraclavicular blocks. Moreover, all physicians were satisfied with the performance of the needle guidance system. Additional studies should be performed to assess the device’s utility in other types of peripheral nerve blocks.
Implication Statement
This is a randomized controlled trial comparing brachial plexus blockade performed using a needle guidance device versus a conventional approach. The study identifies the utility of using a needle guidance device for brachial plexus blockade. This study conforms to the Helsinki Declaration.
Data Sharing Information
De-identified raw data used for supporting the findings of this study are available from the corresponding author, Dr. Amaresh Vydyanathan, on request.
Acknowledgment
The findings in this paper were presented at the American Society of Regional Anesthesia, New Orleans LA in 2016.
Funding
This study was financially supported by CIVCO Medical Solutions. They provided partial funding as an investigator-initiated study grant (Grant #OCT14-0474I). The Principal Investigator was Dr. Amaresh Vydyanathan. The sponsor was not involved in study design, data analysis or manuscript preparation.
Disclosure
Dr Amaresh Vydyanathan reports grants from CIVCO, during the conduct of the study. Dr Naum Shaparin reports grants from CIVCO, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Faccenda KK, Finucane BT. Complications of regional anaesthesia incidence and prevention. Drug Saf. 2001;24:413–442. doi:10.2165/00002018-200124060-00002
2. Bendtsen TF, Nielsen TD, Rohde CV, Kibak K, Linde F. Ultrasound guidance improves a continuous popliteal sciatic nerve block when compared with nerve stimulation. Reg Anesth Pain Med. 2011;36(2):181–184. doi:10.1097/AAP.0b013e31820d421f
3. Bloc S, Mercadal L, Garnier T, et al. Comfort of the patient during axillary blocks placement: a randomized comparison of the neurostimulation and the ultrasound guidance techniques. Eur J Anaesthesiol. 2010;27(7):628–633. doi:10.1097/EJA.0b013e328333fc0a
4. Stone MB, Moon C, Sutijono D, Blaivas M. Michael Blaivas: needle tip visualization during ultrasound-guided vascular access: short-axis vs long-axis approach. Am J Emerg Med. 2010;28(3):343–347. doi:10.1016/j.ajem.2008.11.022
5. Ball RD, Scouras NE, Orebaugh S, Wilde J, Sakai T. Randomized, prospective, observational simulation study comparing residents’ needle-guided vs freehand ultrasound techniques for central venous catheter access. Br J Anaesth. 2012;108(1):72–79. doi:10.1093/bja/aer329
6. Turan A, Babazade R, Elsharkawy H, et al. Novel needle guide reduces time to perform ultrasound-guided femoral nerve catheter placement: a randomized controlled trial. Eur J Anaesthesiol. 2017;34(3):135–140. doi:10.1097/EJA.0000000000000584
7. Kim C, Ratnayake M, Lethbridge G, Ng I. Comparing the use of a needle guidance device vs. freehand technique in performing ultrasound- guided TAP blocks: a prospective randomised trial. J Anesth Clin Res. 2014;5:429.
8. Bluvol N, Kornecki A, Shaikh A, Fernandez D, Taves D, Fenster A. Freehand versus guided breast biopsy: comparison of accuracy, needle motion, and biopsy time in a tissue model. Am J Roentgenol. 2009;192:1720–1725. doi:10.2214/AJR.08.1434
9. Hopkins RE, Bradley M. In-vitro visualization of biopsy needles with ultrasound: a comparative study of standard and echogenic needles using an ultrasound phantom. Clin Radiol. 2001;56:499–502. doi:10.1053/crad.2000.0707
10. Schafhalter-Zoppoth I, McCulloch CE, Gray AT. Ultrasound visibility of needles used for regional nerve block: an in vitro study. Reg Anesth Pain Med. 2004;29:480–488. doi:10.1097/00115550-200409000-00014
11. Sierzenski P, Polan D, Baty G, et al. Junior emergency medicine residents demonstrate improved accuracy for the identification of a central venous needle tip with a long-axis ultrasound transducer orientation. Ann Emerg Med. 2008;52(4):S501.
12. Blaivas M, Brannam L, Fernandez E. Short-axis versus long-axis approaches for teaching ultrasound-guided vascular access on a new inanimate model. Acad Emerg Med. 2003;10:1307–1311. doi:10.1197/S1069-6563(03)00534-7
13. Maecken T, Heite L, Wolf B, Zahn P, Litz R. Ultrasound-guided catheterisation of the subclavian vein: freehand vs needle-guided technique. Anesthesia. 2015;70(11):1242–1249. doi:10.1111/anae.13187
14. Pascarella G, Strumia A, Costa F, et al. Triple monitoring may avoid intraneural injection during interscalene brachial plexus block for arthroscopic shoulder surgery: a prospective preliminary study. J Clin Med. 2021;10(4):781. doi:10.3390/jcm10040781
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Costotransverse Foramen Block with Thoracic Paravertebral Block and Erector Spinae Plane Block for Patients Undergoing Video-Assisted Thoracoscopic Surgery: A Randomized Controlled Non-Inferiority Trial
Li J, Shao P, Wen H, Ma D, Yang L, He J, Jiang J
Journal of Pain Research 2025, 18:2427-2438
Published Date: 13 May 2025
Retrospective Comparison of Extrafascial versus Intrafascial Interscalene Brachial Plexus Block with Reduced Volume: Impact on Hemidiaphragmatic Paralysis and Hemodynamic Effects in Shoulder Surgery Patients
Coviello A, Ranieri G, Coppola F, Damonte R, Cirillo D, De Siena AU, Fattorini F, Scimia P, Castellano G, Rucci F, Servillo G
Local and Regional Anesthesia 2025, 18:87-102
Published Date: 17 September 2025