")
Back to Journals » Infection and Drug Resistance » Volume 16
The Update of HIV-1 Prevalence and Incidence and Spatio-Temporal Analyses of HIV Recent Infection Among Four Sub-Groups in Sichuan, China During Surveillance Period Between 2016 and 2022
Authors Yang H , Li Y , Xu M, Hu Y, Yuan F, Liu L, Li L, Yuan D , Ye L, Zhou C, Zhang Y, Su L, Liang S
Received 1 August 2023
Accepted for publication 27 September 2023
Published 4 October 2023 Volume 2023:16 Pages 6535—6548
DOI https://doi.org/10.2147/IDR.S428744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Hong Yang, Yiping Li, Mengjiao Xu, Ying Hu, Fengshun Yuan, Lunhao Liu, Ling Li, Dan Yuan, Li Ye, Chang Zhou, Yan Zhang, Ling Su, Shu Liang
Center for AIDS/STD Control and Prevention, Sichuan Center for Disease Control and Prevention, Chengdu, People’s Republic of China
Correspondence: Shu Liang; Ling Su, Email [email protected]; [email protected]
Background: Sichuan Province has gradually become a hot-spot for HIV/AIDS. Little is known about the HIV-1 incidence and prevalence among four sub-groups since 2015. Meanwhile, the distributions of hot-spot areas related to recent infection cases that indicate current transmission among the four subgroups are also rare.
Objective: The main purpose of this study was to assess the HIV-1 prevalence and incidence and to visualize the distributions of hot-spot areas of current transmission among four subgroups (people who inject drugs, male STD clinic attendees, female sex workers and men who had sex with men) during the surveillance period in Sichuan province between 2016 and 2022.
Results: Of the 267,617 individuals, 2158 HIV-positive samples were tested with Lag-Avidity EIA, among which 493 samples were identified as recent infections. Among people who inject drugs (PWID), both HIV-1 prevalence (from 1.41% to 0.34%) and incidence (from 0.03% to 0.140%) showed a significant decreasing trend. Among men who had sex with men (MSM), female sex workers (FSWs), and male STD clinic attendees, HIV-1 prevalence indicated significant decreasing trends, whereas HIV-1 incidence showed no significant changes. Spatial analysis demonstrated the formation of hot-spots and clusters of current transmissions sharing regional differences, mainly concentrated in the southeast, and most of these were consecutive hot-spots.
Conclusion: The prevention and control were efficacious and persistent. However, among the other three subgroups, there is a need for a regional cooperative in prevention and control approaches and collaborative research in many aspects.
Keywords: human immunodeficiency virus, recent infection, hot spots, people who inject drugs, PWID, male STD clinic attendees, mSTD, female sex workers, FSWs
Background
Sichuan Province is located in Southwest China and has gradually become a new HIV/AIDS “hot-spot” in recent years.1 In Sichuan, the number of people living with HIV reached to 0.17 million at 2020, ranked first in China and the prevalence increased from 0.16% at 2018 and 0.20% at 2020.2 The development of the HIV infection in Sichuan province was too remarkable to be ignored.
The Key Population is an important driver of the HIV/AIDS epidemic in groups with high-risk behaviors in the general population in China.3 Therefore, surveillance of Key population is important. A national HIV/AIDS surveillance system was established in 1985.4 Now it is mainly consisted of three parts: the national HIV sentinel surveillance system started in 1995,4 covering STD clinic attendees, female sexual workers (FSWs), people who inject drugs(PWID), long-distance truck drivers, pregnant women, paid blood donors, men who have sex with men (MSM), clients of female sex workers and tuberculosis (TB) patients;3 a web-based HIV/AIDS case reporting system established in 2005;4 special epidemiological surveys have been launched among various groups to augment surveillance data,4 and those data have been entered into annual joint assessment reports.5,6 HIV sentinel surveillance is a series of annual cross-sectional surveys on risk behaviors and sero-testing in representative areas and populations,7 including national sentinel surveillance sites and provincial sentinel surveillance sites, which is a necessary complement to the former.4
Traditionally, the focus of analysis of data from sentinel surveillance was a trend of HIV prevalence7,8 and risk factors associated9,10 with HIV infection in a given region and population; however, there is a dearth of information regarding the hot-spot distribution of recent infection cases among the four sub-populations at the city level in Sichuan province. Moreover, the HIV prevalence and incidence after 2015 have remained unclear.
Thus, to address the paucity of relevant information regarding the hot-spot distribution and an update of HIV prevalence, incidence, we conducted a spatial analysis of HIV-1 recent infection cases among four sub-populations (people who inject drugs, male STD clinic attendees, female sex workers and men who had sex with men) and updated the HIV prevalence and incidence between 2016 and 2022.
Methods
Sample Collection and Laboratory Testing
Sentinel surveillance is a cross-sectional survey and conducted annually between 2016 and 2022, according to the National AIDS sentinel surveillance implementation program,11,12 the surveillance period is from April to June. If the sample size is still insufficient at the end of the surveillance period, it can be extended by up to one month. Between 2016 and 2021, 119 sentinel sites were set up for regular surveillance among PWID (39 sites), male STD clinic attendees (30 sites), FSWs (40 sites), and MSM (10 sites) in Sichuan Province (Table 1). By 2022,4 PWID sites and three FSWs sites were closed. Generally, the sample size is 400 per site; when the infection rate of a local high-risk population is higher than 10%, the sample size can be reduced to 250. If the sample size cannot meet the requirements until the end of the surveillance period, then the actual sample size should be reported. Anonymous interviews were dispensed to every participant to collect information on demographic features and HIV-1 transmission-related risk behaviors, and each participant provided 2–3 mL of whole blood at the local CDC. Plasma was separated from the whole blood and used for HIV-1 serological testing. Plasma samples were first screened twice by an enzyme immunoassay and confirmed by a Western blot assay (HIV-1 BLOT 2.2, MP Diagnostics, Singapore) or Recombinant Strip Immunoblot assay (recomLine HIV-1 and HIV-2 IgG, MIKROGEN DIAGNOSTIK, Germany). All HIV-1 tests were voluntary and informed of the study. Written consent was obtained from all the participants. The study was approved by the Ethics Committee of the Sichuan Center for Disease Control and Prevention and conducted in accordance with the Helsinki Declaration of 1964.
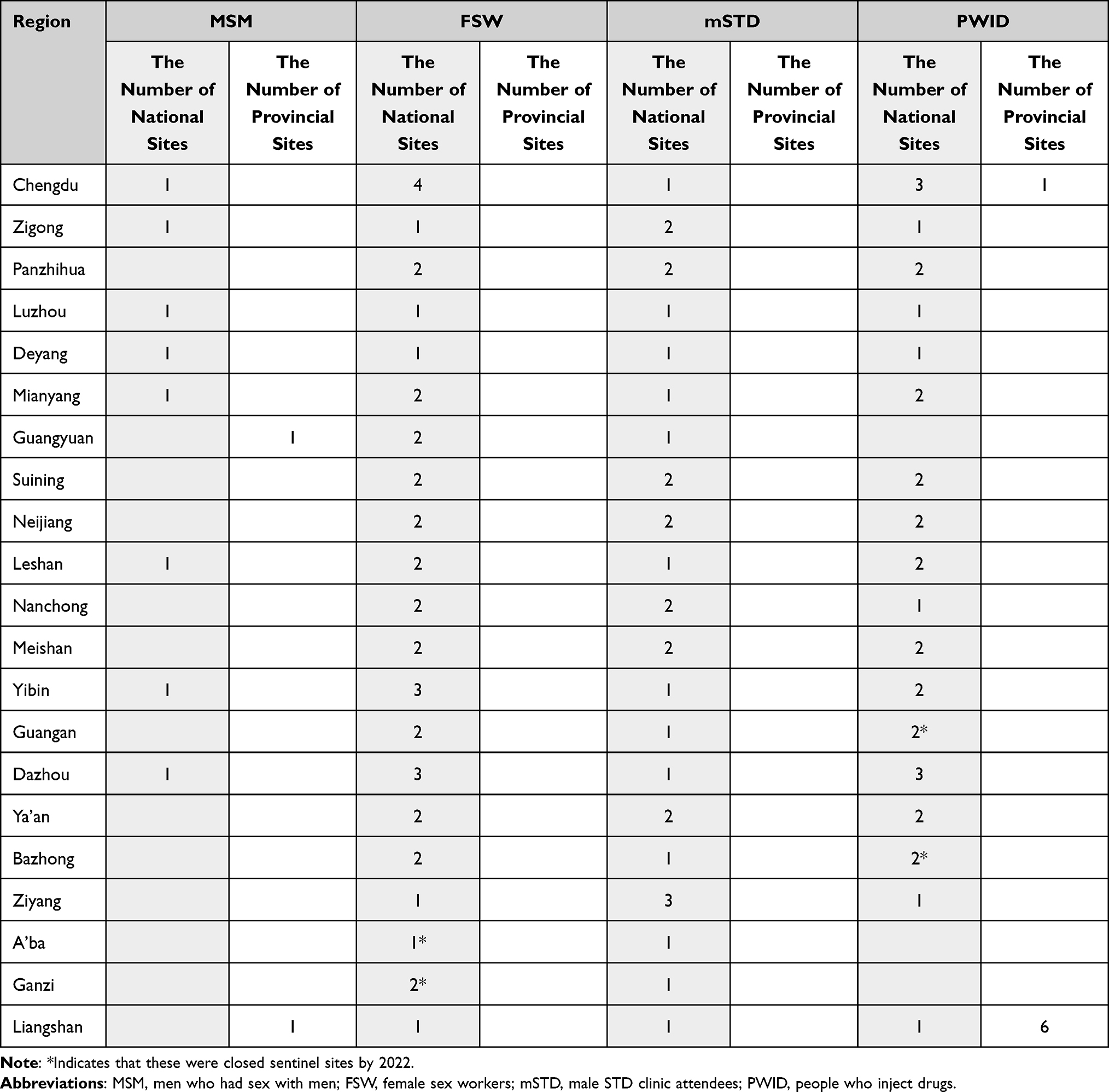 |
Table 1 Distribution of Sentinel Sites (n=119) in Sichuan, 2016–2022 |
Limiting Antigen Avidity Assay
The LAg-Avidity EIA Test13–20 is an in vitro 96-well format enzyme immunoassay that measures the increasing avidity of HIV antibodies from liquid serum/plasma or dried blood spot-eluted specimens after seroconversion. Antibody avidity reflects the relative binding strength, a functional property, of developing antibodies and is likely to be more robust in detecting recent HIV-1 infections than assays that detect antibody levels, which is a passive parameter.21 Specimens that are initially < 2.0 normalized optical density(ODn) in the assay are repeat tested in triplicate (confirmatory testing), and specimens that are confirmed < 1.5 normalized optical density(ODn) in the assay are considered to represent recent infection.
Calculation of Prevalence and Incidence
HIV-1 prevalence is defined as the proportion of individuals currently living with HIV-1 infection.22,23 The prevalence can be estimated by p=yi/n, where yi is the total number of all cases testing positive for HIV-1 and n is the total number of people who were tested.23
The HIV-1 incidence is the rate at which HIV-1 infection occurs in a population.22 It is a quantitative index that measures the extent of ongoing HIV-1 transmission within a population.22 In this study, we calculated the prevalence and incidence as rates because sentinel surveillance is a cross-sectional survey conducted annually between 2018 and 2022 (the surveillance period was from April to June). For a reliable comparison of the incidence between this work and previous works, we continued to use the McDougal formula8,24 to calculate the incidence. A difference existed in the window period (the mean length of time individuals remained classified as “recently infected”). Previous studies have used BED-CEIA to test for evidence of recent infection, and in China, the window period was 168 days.8,24 Our study used the Limiting Antigen Avidity assay, and in China, the window period was 130 days.11
According to the Operations Manual,24 when the number of recent infections identified by the LAg-avidity EIA is more than 10, the estimated incidence is reliable. In most cities, the recent infections for each year is less than 10, and a solution is to combine data from several years to calculate the incidence.
Spatial Analysis for HIV Recent Infections
The spatial analysis was conducted with ArcGIS 10.7 (ESRI, Redlands, CA, USA) to visualize the hot-spot areas of four sub-populations in sentinel surveillance. Local spatial auto-correlation was used to analyze the correlation between the distribution of recent HIV cases in a specific city and that in adjacent cities. The Getis-Ord Gi* statistic was used to calculate the z-scores and p-values; local clusters with a z-value >1.76 were defined as hot-spots, indicating that the distribution in those counties was highly clustered.
Statistical Analysis
Data analysis was conducted using SPSS (version 23.0; IBM, Armonk, New York, USA). Trend tests were performed using χ2 tests with linear-by-linear association. All tests were two-tailed, and statistical significance was set at p <0.05.
Results
Summarization
In total, there were 119 sentinel surveillance sites covering the four sub-group between 2016 and 2021. As 3 STD sites and 4 DUS sites were closed, there were 112 sentinel surveillance sites by 2022 [Table 1]. A total of 267,617 individuals participated in a sentinel surveillance program for HIV between 2016 and 2022, including 22,991 MSM, 62,725 male STD clinic attendees, 85,572 FSWs, and 96,329 PWID. HIV-1 antibodies were distinguished in 7876 samples by serum screening twice, of which 4426 samples were reported previously. All newly reported HIV-1 infected cases were immediately confirmed by Western blotting or Recombinant Strip Immunoblot assays. Excluding 168 samples whose volumes were not sufficient for LAg-avidity EIA, a total of 2158 samples (92.78%) were tested with Lag-Avidity EIA, among which 493 samples were identified as HIV-1 recent infection. Based on these results, the prevalence and estimated incidence were obtained for each of the four sub-populations (Table 2).
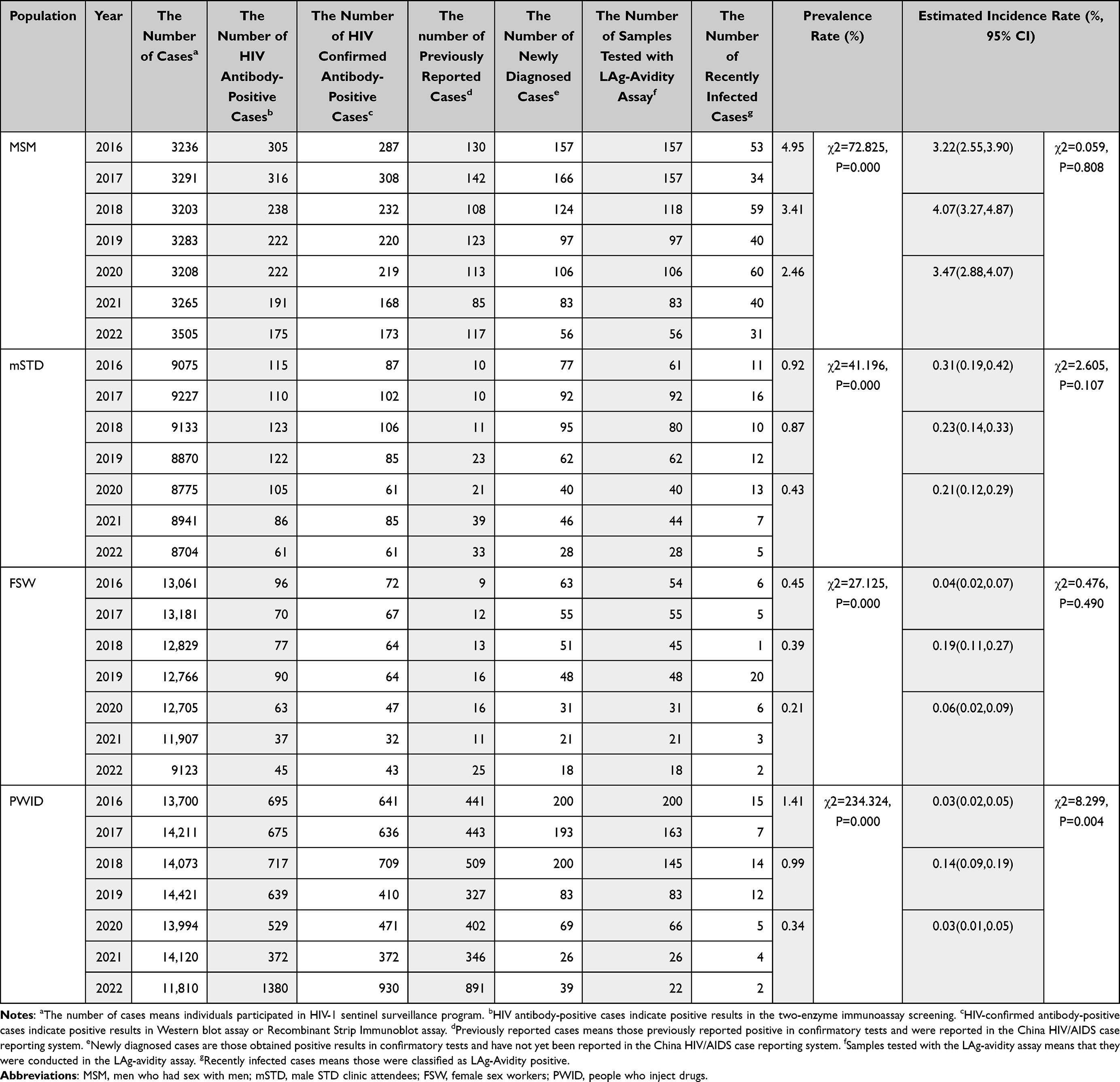 |
Table 2 HIV-1 Prevalence Rate and Incidence Rate from Four-Groups Sentinel Surveillance |
PWID
HIV prevalence and estimated incidence between 2016 and 2022 among STD are shown in Table 2. The estimated incidence showed a significant trend (χ2=8.299, P=0.004) and the prevalence showed a significant decreasing trend between 2016–2022 (χ2=234.324, P=0.000). Spatial analysis revealed a significant cluster in Liangshan (2016–2022, Figure 1A-C), while Panzhihua (2016–2017 and 2020–2022, Figure 1A and C) showed a secondary cluster.
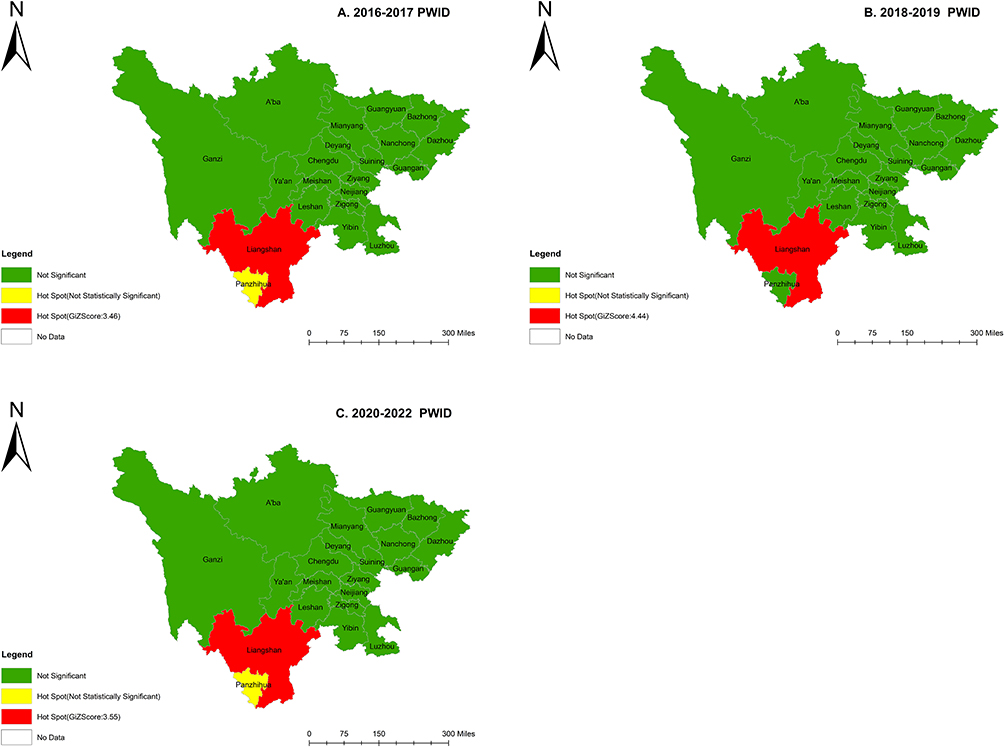 |
Figure 1 2016–2022 Hot spots of HIV recent cases among PWID at city level by year. (A) Sichuan province, 2016–2017. (B) Sichuan province, 2018–2019. (C) Sichuan province, 2020–2022. |
Male STD Clinic Attendees
HIV prevalence and estimated incidence between 2016 and 2022 among STD are shown in Table 2. The estimated incidence did not show a significant trend (χ2=2.605, P=0.107); however, the prevalence showed a significant decreasing trend between 2016–2022 (χ2=41.196, P=0.000). Spatial analysis revealed a significant cluster in Deyang (2016–2017, Figure 2A), Yibin (2018–2019, Figure 2B) and Luzhou (2020–2022, Figure 2C), respectively, and Liangshan and Yibin (2020–2022, Figure 2C) showed a secondary cluster.
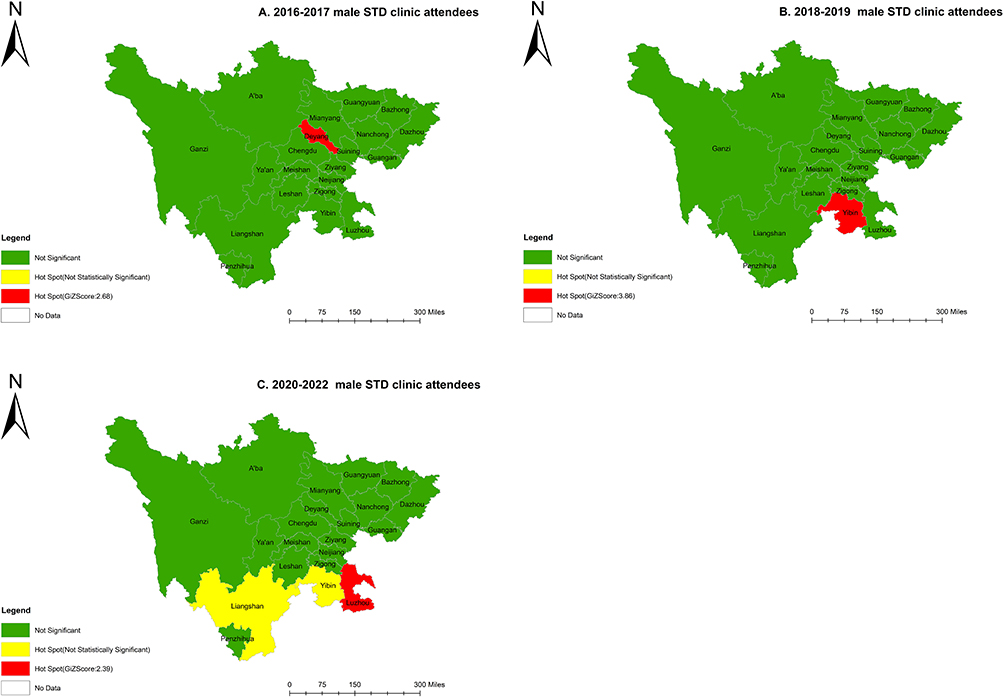 |
Figure 2 2016–2022 Hot spots of HIV recent cases among mSTD at city level by year. (A) Sichuan province, 2016–2017. (B) Sichuan province, 2018–2019. (C) Sichuan province, 2020–2022. |
FSW
HIV prevalence and estimated incidence between 2016 and 2022 among STD are shown in Table 2. The estimated incidence did not show a significant trend (χ2=0.476, P=0.490); however, the prevalence showed a significant decreasing trend between 2016–2022 (χ2=27.125, P=0.000). Spatial analysis revealed a significant cluster in Mianyang (2018–2019, Figure 3B), Yibin (2016–2022, Figure 3A-C), and Luzhou (2020–2022, Figure 3C), respectively, and Luzhou (2018–2019, Figure 3B) and Deyang (2016–2017, Figure 3A) showed a secondary cluster.
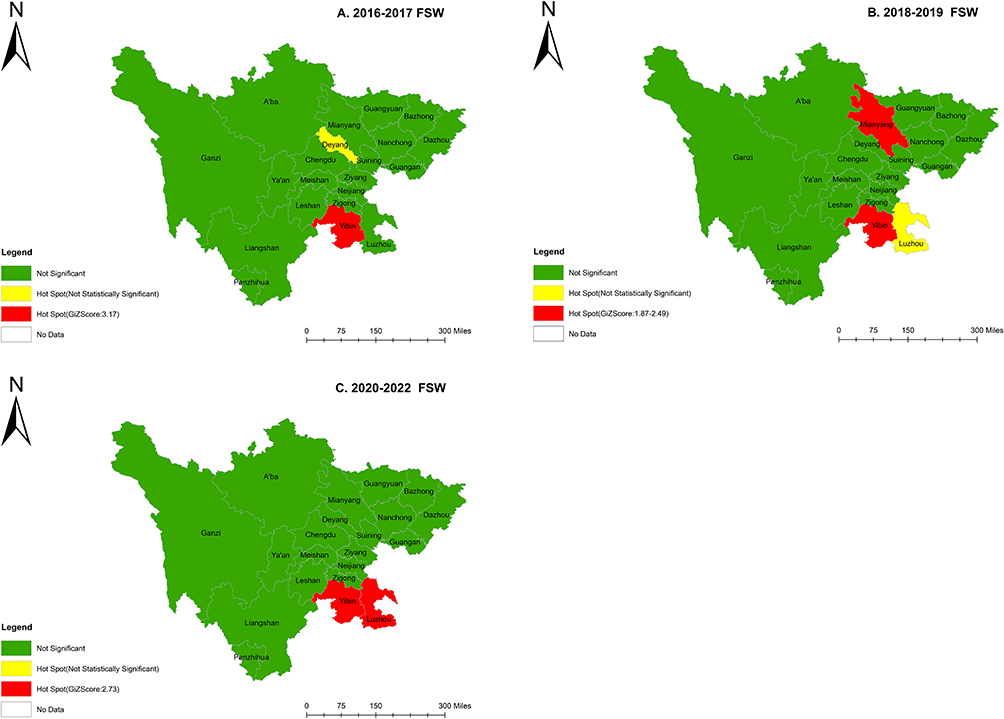 |
Figure 3 2016–2022 Hot spots of HIV recent cases among FSW at city level by year. (A) Sichuan province, 2016–2017. (B) Sichuan province, 2018–2019. (C) Sichuan province, 2020–2022. |
MSM
The HIV prevalence and estimated incidence between 2016 and 2022 among MSM are shown in Table 2. The estimated incidence did not show a significant trend (χ2=0.059, P=0.808); however, the prevalence showed a significant decreasing trend between 2016–2022 (χ2=72.825, P=0.000). Spatial analysis revealed a significant cluster in Yibin (2016–2017, Figure 4A) and Luzhou (2016–2022, Figure 4A-C).
 |
Figure 4 2016–2022 Hot spots of HIV recent cases among MSM at city level by year. (A) Sichuan province, 2016–2017. (B) Sichuan province, 2018–2019. (C) Sichuan province, 2020–2022. |
Discussion
To our knowledge, this study is the first to report a combined application of spatial analysis and LAg-avidity EIA to illustrate hot-spot areas of recent HIV-1 cases at the city level among four sub-groups in China for seven years in a row, which will incentivize the focus of intervention efforts on relevant areas and populations. Furthermore, we first updated the HIV-1 prevalence and incidence among the four subgroups until 2022, continuing previous works.8
Overall, among the four subgroups, a relatively high level emerged in 2018–2019 and a relatively low level emerged in 2020–2022. We believe that the emergence of this phenomenon during 2018–1019 was related to China’s scale-up testing policies. In January 2017, <China’s 13th Five-Year Plan for HIV/AIDS prevention>25 was issued by General Office of the State Council of the People’s Republic of China issued China. This plan was first required to identify infected individuals and patients to a large extent. Accordingly, the plan required that medical institutions, maternity and child healthcare institutions, and disease prevention and control institutions at or above the county level should all have the capacity for HIV testing. Moreover, HIV testing and consultation should be included in voluntary premarital medical and physical examinations of the target population. In September 2019, the Chinese CDC issued an implementation plan for HIV/AIDS prevention (2019–2022)>26 was issued by Chinese CDC. In the plan, it was required that community health service centers and township health centers should all be capable of rapid HIV testing and counseling. This suggests that HIV testing should be included in the health examinations of the elderly in basic public health services. Despite these scale-up testing policies, more HIV infection cases were found, resulting in a relatively higher incidence among the four subgroups. Between 2020 and 2022, the outbreak of SARS-CoV-2 led to an unprecedented disruption in life.27 To mitigate viral transmission, many governments have introduced prevention measures based on social and behavioral restrictions (eg, physical distancing, stay-at-home policies, or quarantine).28,29 Sexual behavioral changes,30,31 pathological disorders,32,33 and income reduction34,35 may result in a temporarily lower incidence among the four subgroups.
PWID was the only group in which the HIV incidence significantly decreased. In 1989, the first HIV epidemic in Yunnan was identified among PWID in Ruili County bordering Myanmar, and then further spread along major drug-trafficking roads to Guangxi, Sichuan, Xinjiang, Guangdong, and other provinces.7,36–38 Historically, HIV-1 infection has been largely confined to certain high-risk populations such as intravenous drug users.37,39,40 The relative importance of IDU in contributing to the total number of reported HIV/AIDS cases has been declining over the years as sexual transmission increases.41 In this study, both HIV-1 incidence and prevalence of PWID among the four sub-populations were lower than those reported in previous studies.7,8,37 A relatively higher HIV-1 incidence among PWID was observed between 2018 and 2019, for the reasons mentioned above. Among PWID, the significant decreasing trend in HIV-1 incidence could mainly result from the persistent implementation of needle exchange programs and methadone maintenance treatment.42–44 The decrease between 2020–2022, it was possibly due to the pandemic of SARS-Cov-2, with a reduction in drug supplies,45 different lockdown measures,23 and alteration of drug use patterns.46 Spatial analysis illustrated that Liangshan Prefecture and Panzhihua City were hot-spot areas. Liangshan is an autonomous prefecture of Sichuan Province and consists of 17 counties, with 5 counties having a high HIV prevalence (>1%).47 In particular, long-term poverty and a long history of drug production and trade are the primary reasons for high HIV prevalence.47–49 In September 2017, the National Health Commission and Sichuan Provincial Government jointly issued the “First Phase Action Plan for HIV Prevention and Health Poverty Alleviation in Liangshan Prefecture, Sichuan Province, China (2017–2020)”, which led to positive challenges in HIV prevention and control.50
With the implementation of the National Methadone Maintenance Treatment Program and the Needle Exchange Program in 2004,51 sexual contact has gradually become the primary transmission route for HIV/AIDS, particularly heterosexual transmission.41,52 Through commercial sex work, male STD clinic attendees and female sex workers represent a crucial “bridge population” driving HIV infection in the general population.53,54 In this study, STD and FSW had an observably lower HIV-1 prevalence than previous reports in Sichuan and Yunnan provinces;7,8 however, there were no significant trends in HIV-1 incidence. As previous works reported,53–55 consistent condom use was still low both in heterosexual STD clinic patients and FSW. Without condom protection, the risk of HIV transmission among sexual behaviors would be greatly increase.56 Spatial analysis illustrated that the southeastern cities were consecutive hot-spot areas, such as Yibin and Luzhou. This result can be interpreted as follows. The southeast region of Sichuan has a high population density and accounts for a large migrant labor force in large cities across the country.57 Migrant workers showed a significant increase in engagement with commercial sex workers and a low percentage of consistent condom use during commercial sex.58–60 In addition, HIV infection is widely prevalent among older men (aged≥50 years) in this region.57 Among older men, the primary mode of heterosexual transmission is commercial heterosexual contact due to sex needs, single, widowhood, and a stable financial situation.61–63 Besides, works64 on HIV-1 molecular epidemiology showed that commercial heterosexuality caused an aggregated HIV epidemic in this region, and HIV-1 genetic transmission networks65,66 suggested that there was more likely regional transmission in these areas. In summary, HIV prevention approaches in these areas may require joint interventions, both inside and outside (eg, information exchange for better launching joint interventions and collaborating with each other).
MSM had the highest HIV prevalence and incidence among the four subgroups in this study, and HIV incidence was estimated to be lower than the national level calculated by a meta-analysis67 and previous data reported in Sichuan.68 The low level is partly due to progress in diagnosing infections among people living with HIV-1 and ensuring that they have access to early, ongoing treatment69–71 and, in part, to the pandemic of SARS-CoV-2. Some studies30,31 have suggested a reduction in sexual activity among MSM during this period. Thus, future studies should monitor the HIV epidemic in this high-risk population. Spatial analysis demonstrated a significant and consecutive hot spot in Luzhou City, which confirmed a supposition about an HIV-1 epidemic spreading from the core city (like Chengdu) to the peripheral region among MSM, as reported in our previous work.68 This spread may be derived from its geographical position neighboring other provinces with a high HIV-1 burden67,72,73 and Luzhou’s policies,74,75 which increased screening for HIV and AIDS, and more cases are being detected.76 According to Yuan,65 Luzhou does not have a strong HIV-1 transmission link with other cities within Sichuan. In these contexts, more intensive work should be conducted, concentrating on the identification of transmission networks of new infections, demographic characteristics, and spatial distribution, as well as the exploration of the relationship between molecular transmitted clusters and social covariates.
This study had some limitations. First, most sentinel surveillance systems have limited geographical coverage, with under-representation of rural and smaller areas; therefore, the results of this study were not entirely representative of the whole province. Second, the implementation of sentinel surveillance varies considerably between cities, and the quality of surveys might differ over time depending on available resources; therefore, the results of this study were undoubtedly affected by these factors. Third, given the nature of a cross-sectional survey, temporality between surveillance periods cannot be inferred. For example, we cannot claim the findings of this study, which represent the entire year. Fourth, considering the mis-classification of the LAg-avidity EIA, there is a possibility of overestimation of the incidence. Fifth, owing to stringent SARS-CoV-2 prevention measures, it is not yet clear whether the declining trends were actual.
Conclusion
In this work, we updated the data on HIV-1 prevalence and incidence among four subgroups until 2022, continuing and confirming the supposition of previous studies. HIV-1 prevalence and incidence among PWID showed a declining trend, and spatial analysis indicated that Liangshan Prefecture was still a consecutive hot-spot area among PWID, which suggests that the prevention and control of this population in this region were efficacious and should be persistent. However, among the three sub-groups belonging to heterosexual transmission routes, HIV-1 prevalence and incidence showed no significant changes, and spatial analysis indicated that the southeastern region in Sichuan province was a hot-spot area in the study period, which is referred to as a regional cooperative in prevention and control approaches and collaborative research in many aspects.
Abbreviations
PWID, people who inject drugs; STD, sexually transmitted diseases; FSWs, female sex workers; MSM, men who have sex with men; LAg-Avidity EIA, Limiting Antigen Avidity enzyme immunoassay; HIV, Human immunodeficiency virus; CDC, Centers for Disease Control and Prevention; ODn, normalized optical density.
Acknowledgments
We are grateful to the staff of local Centers for Disease Control and Prevention for their support for sample collection and data acquisition.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Natural Science Foundation of Sichuan Province (2022NSFSC1547) and Sichuan Science and Technology Program (2019YFS0369).
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Liu Z, Shi O, Yan Q, et al. Changing epidemiological patterns of HIV and AIDS in China in the post-SARS era identified by the nationwide surveillance system. BMC Infect Dis. 2018;18(1):700. doi:10.1186/s12879-018-3551-5
2. Yang H, Yiping L, Fang H, et al. Demographic Characteristics and Hot-Spot Areas of Recent Infections Among New HIV Diagnoses in Sichuan, China, Between 2018 and 2020. Infect Drug Resist. 2023;16:779–789. doi:10.2147/IDR.S394828
3. Wang L, Wang N. HIV/AIDS epidemic and the development of comprehensive surveillance system in China with challenges. Chin Med J. 2010;123(23):3495–3500.
4. Sun X, Wang N, Li D, et al. The development of HIV/AIDS surveillance in China. AIDS. 2007;21(Suppl 8):S33–S38. doi:10.1097/01.aids.0000304694.54884.06
5. Ministry of Health of China, UNAIDS, WHO. 2005 Update on the HIV/AIDS Epidemic and Response in China. Beijing: Ministry of Health; 2006.
6. State Council AIDS Working Committee Office, UN Theme Group on HIV/AIDS in China. A Joint Assessment of HIV/AIDS Prevention, Treatment and Care in China. Beijing: China Ministry of Health; 2004.
7. Yang L, Chen M, Yanling M, et al. The changing trends of HIV-1 prevalence and incidence from sentinel surveillance of five sub-populations in Yunnan, China, 2001–2010. BMC Public Health. 2015;15(1):376. doi:10.1186/s12889-015-1722-5
8. Yang H, Su L, Ye L, et al. Incidence rates of HIV-1 epidemics among 4 high risk groups in Sichuan province during 2011-2015. Zhonghua Liu Xing Bing Xue Za Zhi. 2017;38(12):1649–1654. doi:10.3760/cma.j.issn.0254-6450.2017.12.014
9. Zhang F, Nie CL, Yuan FC, et al. HIV infection status and related factors in men who have sex with men in sentinel surveillance in Shanxi province, 2010, 2015 and 2020. Zhonghua Liu Xing Bing Xue Za Zhi. 2022;3(4):554–559. doi:10.3760/cma.j.cn112338-20210611-00469
10. Bai JY, Ning TL, Zhou N, et al. HIV infection status and related factors in men who have sex with men in sentinel surveillance in Tianjin, 2016-2018. Zhonghua Liu Xing Bing Xue Za Zhi. 2019;40(9):1106–1110. doi:10.3760/cma.j.issn.0254-6450.2019.09.016
11. Chinese center for disease control and prevention. The National AIDS Sentinel Surveillance Implementation Program Issued by Chinese Center for Disease Control and Prevention. Chinese center for disease control and prevention; 2022.
12. Chinese center for disease control and prevention. The National AIDS Sentinel Surveillance Implementation Program Issued by Chinese Center for Disease Control and Prevention. Chinese center for disease control and prevention; 2017.
13. Wei X, Liu X, Dobbs T, et al. Development of two avidity-based assays to detect recent HIV type 1 seroconversion using a multisubtype gp41 recombinant protein. AIDS Res Hum Retroviruses. 2010;26(1):1–11. doi:10.1089/aid.2009.0133
14. Duong YT, Qiu M, De AK, et al. Detection of recent HIV-1 infection using a new limiting-antigen avidity assay: potential for HIV-1 incidence estimates and avidity maturation studies. PLoS One. 2012;7(3):e33328. doi:10.1371/journal.pone.0033328
15. Suligoi B, Massi M, Galli C, et al. Identifying recent HIV infections using the avidity index and an automated enzyme immunoassay. J Acquir Immune Defic Syndr. 2003;32(4):424–428. doi:10.1097/00126334-200304010-00012
16. Chawla A, Murphy G, Donnelly C, et al. Human immunodeficiency virus (HIV) antibody avidity testing to identify recent infection in newly diagnosed HIV type 1 (HIV-1)-seropositive persons infected with diverse HIV-1 subtypes. J Clin Microbiol. 2007;45(2):415–420. doi:10.1128/JCM.01879-06
17. Suligoi B, Galli C, Massi M, et al. Precision and accuracy of a procedure for detecting recent human immunodeficiency virus infections by calculating the antibody avidity index by an automated immunoassay-based method. J Clin Microbiol. 2002;40(11):4015–4020. doi:10.1128/JCM.40.11.4015-4020.2002
18. Martró E, Suligoi B, González V, et al. Comparison of the avidity index method and the serologic testing algorithm for recent human immunodeficiency virus (HIV) seroconversion, two methods using a single serum sample for identification of recent HIV infections. J Clin Microbiol. 2005;43(12):6197–6199. doi:10.1128/JCM.43.12.6197-6199.2005
19. Schwarcz S, Kellogg T, McFarland W, et al. Differences in the temporal trends of HIV seroincidence and seroprevalence among sexually transmitted disease clinic patients, 1989-1998: application of the serological testing algorithm for recent HIV seroconversion. Am J Epidemiol. 2001;153(10):925–934. doi:10.1093/aje/153.10.925
20. Machado DM, Delwart EL, Diza RS, et al. Use of the sensitive/less-sensitive (detuned) EIA strategy for targeting genetic analysis of HIV-1 recently infected blood donors. AIDS. 2002;16(1):113–119. doi:10.1097/00002030-200201040-00014
21. Biomedical M. Maxim HIV-1 Limiting Antigen Avidity EIA, Single Well Avidity Enzyme Immunoassay for Detection of Recent HIV-1 Infection. Rockville, Maryland USA: Maxim Biomedical, Inc; 2013.
22. UNAIDS/WHO Working Group on Global HIV/AIDS and STI Surveillance. When and How to Use Assays for Recent Infection to Estimate HIV Incidence at a Population Level. ISBN 978 92 4 150167 5 (NLM Classififi Cation: WC 503.41). Avenue Appia 20 1211 Geneva 27 Switzerland: World Health Organization Department of HIV/AIDS; 2011.
23. UNAIDS/WHO Working Group on Global HIV/AIDS/STI Surveillance. Guidelines for Measuring National HIV Prevalence in Population-Based Surveys. Geneva: UNAIDS/WHO; 2005. Available from: http://data.unaids.org/pub/manual/2005/20050101_gs_guidemeasuringpopulation_en.pdf.
24. Chinese center for disease control and prevention. The Operations Manual for Estimating HIV-1 Incidence Using a Laboratory Assay Issued by Chinese Center for Disease Control and Prevention. Chinese center for disease control and prevention; 2011.
25. General Office of the State Council of the People’s Republic of China.Notice on the Issuance of the Thirteenth Five-Year Plan of Action for Curbing and Preventing AIDS in China. Government of China; 2017. Available from: http://www.gov.cn/zhengce/content/2017-02/05/content_5165514.htm.
26. National Health Commission of the People’s Republic of China. Notice on the issuance of the Implementation plan for HIV/AIDS prevention (2019-2022); 2019. Available from: www.gov.cn/zhengce/zhengceku/2019-11/13/content_5451669.htm.
27. Kanwugu ON, Adadi P. HIV/SARS-CoV-2 coinfection: a global perspective. J Med Virol. 2021;93(2):726–732. doi:10.1002/jmv.26321
28. National Health Commission of the People’s Republic of China. Guidance for Corona Virus Disease 2019(first edition); 2020. Available from: www.gov.cn/zhengce/zhengceku/2020-01/23/content_5471857.htm.
29. European Centre for Disease Prevention and Control. Questions and answers on COVID-19: prevention; 2019. Available from: https://www.ecdc.europa.eu/en/covid-19/questions-answers/questions-answers-prevention.
30. Winter BL, Hovaguimian F, Kouyos RD, et al. Changes in mental and sexual health among MSM using HIV pre-exposure prophylaxis during the SARS-CoV-2 pandemic: longitudinal analysis of the SwissPrEPared cohort study. Swiss Med Wkly. 2022;152:w30192. doi:10.4414/SMW.2022.w30192
31. Pampati S, Emrick K, Siegler AJ. Changes in Sexual Behavior, PrEP adherence, and Access to Sexual Health Services Because of the COVID-19 Pandemic Among a Cohort of PrEP-Using MSM in the South. J Acquir Immune Defic Syndr. 2021;87(1):639–643. doi:10.1097/QAI.0000000000002640
32. Holtmann N, Edimiris P, Andree M, et al. Assessment of SARS-CoV-2 in human semen-a cohort study. Fertil Steril. 2020;114(2):233–238. doi:10.1016/j.fertnstert.2020.05.028
33. Yang M, Chen S, Huang B, et al. Pathological findings in the testes of COVID-19 patients: clinical implications. Eur Urol Focus. 2020;6(5):1124–1129. doi:10.1016/j.euf.2020.05.009
34. Sanchez TH, Zlotorzynska M, Rai M, Baral SD. Characterizing the Impact of COVID-19 on Men Who Have Sex with Men Across the United States in April, 2020. AIDS Behav. 2020;24(7):2024–2032. doi:10.1007/s10461-020-02894-2
35. Vasylyeva TI, Smyrnov P, Strathdee S, Friedman SR. Challenges posed by COVID-19 to people who inject drugs and lessons from other outbreaks. J Int AIDS Soc. 2020;23(7):e25583. doi:10.1002/jia2.25583
36. Ma Y, Li ZZ, Zhang KX, et al. Identification of HIV infection among drug users in China. Zhonghua Liu Xing Bing Xue Za Zhi. 1990;11:184–185.
37. Ruan Y, Qin G, Liu S, et al. HIV Incidence and Factors Contributed to Retention in a 12-Month Follow-up Study of Injection Drug Users in Sichuan Province, China. J Acquir Immune Defic Syndr. 2005;39(4):459–463. doi:10.1097/01.qai.0000152398.47025.0f
38. Beyrer C, Razak MH, Lisam K, et al. Overland heroin trafficking routes and HIV-1 spread in south and South-East Asia. AIDS. 2000;14(1):75–83. doi:10.1097/00002030-200001070-00009
39. Lin L, Jia M, Yanling M, et al. The changing face of HIV in China. Nature. 2008;455(7213):609–611. doi:10.1038/455609a
40. Yifei H, Liang S, Zhu J, et al. Factors Associated with Recent Risky Drug Use and Sexual Behaviors among Drug Users in Southwestern China. J AIDS Clin Res. 2011;2(120):2155–6113-2–120. doi:10.4172/2155-6113.1000120
41. Yin L, Qin G, Qian H-Z, et al. Continued spread of HIV among injecting drug users in southern Sichuan Province, China. Harm Reduct J. 2007;4(1):6. doi:10.1186/1477-7517-4-6
42. Li J, Ha TH, Zhang C, Liu H. The Chinese government’s response to drug use and HIV/AIDS: a review of policies and programs. Harm Reduct J. 2010;7(1):4. doi:10.1186/1477-7517-7-4
43. Pang L, Hao Y, Mi G, et al. Effectiveness of first eight methadone maintenance treatment clinics in China. Aids AIDS. 2007;21(Suppl 8):S103–7. doi:10.1097/01.aids.0000304704.71917.64
44. Yin W, Hao Y, Sun X, et al. Scaling up the national methadone maintenance treatment program in China: achievements and challenges. Int J Epidemiol. 2010;2(Suppl 2):ii29–37. doi:10.1093/ije/dyq210
45. Farhoudian A, Radfar SR, Mohaddes Ardabili H, et al. A Global Survey on Changes in the Supply, Price, and Use of Illicit Drugs and Alcohol, and Related Complications During the 2020 COVID-19 Pandemic. Front Psychiatry. 2021;12:646206. doi:10.3389/fpsyt.2021.646206
46. Zolopa C, Hoj S, Bruneau J, et al. A rapid review of the impacts of “Big Events” on risks, harms, and service delivery among people who use drugs: implications for responding to COVID-19. Int J Drug Policy. 2021;92:103127. doi:10.1016/j.drugpo.2021.103127
47. Joint United Nations Programme on HIV/AIDS. Delivering as one UN:The UN Joint Programme on AIDS in China 2018–2019. Available from: http://www.unaids.org.cn/pics/20181128171427.pdf.
48. Li L, Wei D, Hsu W-L, et al. CRF07_BC strain dominates the HIV-1 epidemic in injection drug users in Liangshan Prefecture of Sichuan, China. AIDS Res Hum Retroviruses. 2015;31(5):479–487. doi:10.1089/AID.2014.0120
49. Zhu C, Zhou Y, Song X, et al. Review on the influence factors of AIDS epidemic and control in Liangshan Prefecture Sichuan Province of China. Fudan Uni J Med Sci. 2015;42:675–679.
50. Liu Z, Tang X, Liu Y, et al. HIV Prevention and Health Poverty Alleviation – liangshan Prefecture, Sichuan Province, China, 2017-2020. China CDC Wkly. 2021;3(48):1031–1035. doi:10.46234/ccdcw2021.250
51. Smith K, Bartlett N, Wang N. A harm reduction paradox: comparing China’s policies on needle and syringe exchange and methadone maintenance. Int J Drug Policy. 2012;23(4):327–332. doi:10.1016/j.drugpo.2011.09.010
52. Gill B, Okie S. China and HIV – a window of opportunity. N Engl J Med. 2007;356(18):1801–1805. doi:10.1056/NEJMp078010
53. Wang QQ, Chen XS, Yin YP, et al. HIV/STD pattern and its associated risk factors among male STD clinic attendees in China: a foci for HIV intervention. BMC Public Health. 2011;11:955. doi:10.1186/1471-2458-11-955
54. Zhang H, Hsieh E, Wang L, et al. HIV/AIDS Among Female Sex Workers in China: epidemiology and Recent Prevention Strategies. Curr HIV/AIDS Rep. 2020;17(2):151–160. doi:10.1007/s11904-019-00477-y
55. Zhao P, Tang W, Cheng H, et al. Uptake of provider-initiated HIV and syphilis testing among heterosexual STD clinic patients in Guangdong, China: results from a cross-sectional study. BMJ Open. 2020;10(12):e041503. doi:10.1136/bmjopen-2020-041503
56. Xiao Z, Noar SM, Zeng L. Systematic review of HIV prevention interventions in China: a health communication perspective. Int J Public Health. 2014;59(1):123–142. doi:10.1007/s00038-013-0467-0
57. Yuan FS, Liu L, Liu LH, et al. Epidemiological and spatiotemporal analyses of HIV/AIDS prevalence among older adults in Sichuan, China between 2008 and 2019: a population-based study. Int J Infect Dis. 2021;105:769–775. doi:10.1016/j.ijid.2021.02.077
58. Li W, Jiang J, Su J, et al. Commercial sexual behaviors among male rural-to-urban migrants in Western China: implications for HIV prevention. Asia Pac J Public Health. 2017;29(5):388–400. doi:10.1177/1010539517709029
59. Wang Y, Lu R, Wu G, et al. Changing trends of HIV, syphilis, and hepatitis c among male migrant workers in Chongqing, China: nine consecutive cross-sectional surveys, 2010–2018. Int J Environ Res Public Health. 2020;17(3):875. doi:10.3390/ijerph17030875
60. Ling S, Liang S, Hou X, et al. Impact of worker emigration on HIV epidemics in labour export areas: a molecular epidemiology investigation in Guangyuan, China. Sci Rep. 2018;8(1):16046. doi:10.1038/s41598-018-33996-6
61. Yuan F-S, Liu L, Su L, Zeng Y-L, Liang S. The related factors of new HIV infection among older men in Sichuan, China: a case-control study. Epidemiol Infect. 2022;150:e156. doi:10.1017/S0950268822001352
62. Wang X, Lan G, Shen Z, et al. HIV and syphilis prevalence trends among men who have sex with men in Guangxi, China: yearly cross-sectional surveys, 2008–2012. BMC Infect Dis. 2014;14(1):367. doi:10.1186/1471-2334-14-367
63. Zhou Y, Ding Y, Gu K, et al. Motivations for sexual risk behaviors among older men in Shanghai, China: a qualitative study. BMC Public Health. 2014;14(1):802. doi:10.1186/1471-2458-14-802
64. Zhou C, Liang S, Yiping L, et al. Characterization of HIV-1 molecular epidemiology and transmitted drug-resistance in newly diagnosed HIV-infected patients in Sichuan, China. BMC Infect Dis. 2022;22:602. doi:10.1186/s12879-022-07576-z
65. Yuan D, Bin Y, Liang S, et al. HIV-1 genetic transmission networks among people living with HIV/AIDS in Sichuan, China: a genomic and spatial epidemiological analysis. Lancet Reg Health West Pac. 2021;18:100318. doi:10.1016/j.lanwpc.2021.100318
66. Zhou C, Kang R, Liang S, et al. Risk Factors of Drug Resistance and the Potential Risk of HIV-1 Transmission of Patients with ART Virological Failure: a Population-Based Study in Sichuan, China. Infect Drug Resist. 2021;14:5219–5233. doi:10.2147/IDR.S334598.eCollection2021
67. Zhang W, Xu -J-J, Zou H, Zhang J, Wang N, Shang H. HIV incidence and associated risk factors in men who have sex with men in Mainland China: an updated systematic review and meta-analysis. Sex Health. 2016;13(4):373. doi:10.1071/SH16001
68. Yang H, Ye L, Su L. An analysis on incidence of HIV-1 epidemics among men who have sex with men in Sichuan Province during 2011-2015. Zhonghua Yu Fang Yi Xue Za Zhi. 2019;53(3):327–329. doi:10.3760/cma.j.issn.0253-9624.2019.03.018
69. Nkambule RN-BH, Mnisi Z, Ao TT, et al. Substantial progress in confronting the HIV epidemic in Swaziland: first evidence of national impact.
70. Nsanzimana S, Nshogoza Rwibasira G, Sewava Malamba S, et al. HIV incidence and prevalence among adults aged 15-64 years in Rwanda: results from the Rwanda Population-based HIV Impact Assessment (RPHIA) and District-level Modeling, 2019. Int J Infect Dis. 2022;116:245–254. doi:10.1016/j.ijid.2022.01.032
71. Nkambule R, PhilipID NM, Reid G, et al. HIV incidence, viremia, and the national response in Eswatini: two sequential population-based surveys. PLoS One. 2021;16(12):e0260892. doi:10.1371/journal.pone.0260892
72. Yang S, Alice PYC, Lin Q. HIV epidemics in Shenzhen and Chongqing, China. PLoS One. 2018;13(2):e0192849. doi:10.1371/journal.pone.0192849
73. Dong M-J, Peng B, Liu Z-F. The prevalence of HIV among MSM in China: a large-scale systematic analysis. BMC Infect Dis. 2019;19(1):1000. doi:10.1186/s12879-019-4559-1
74. Notice of the Office of the Luzhou Municipal People’s Government on the issuance of the thirteenth five-year plan of action for curbing and preventing AIDS in Luzhou. Government of Luzhou; 2018. Available from: http://wjw.luzhou.gov.cn/zwgk/lzyj/bmwj/zcwj/content_552514.
75. Implementation opinions of the Office of the Committee on Prevention and Treatment of Major Infectious Diseases in Luzhou on further strengthening the management of HIV antiretroviral treatment and follow-up. Government of Luzhou. Available from: http://wjw.luzhou.gov.cn/zwgk/lzyj/bmwj/zcwj/content_537126.
76. RenN, YuanshengL, WangR, et al.The Distribution of HIV and AIDS Cases in Luzhou, China, From 2011 to 2020. JMIR Public Health Surveill. 2022;8(6):e37491. doi:10.2196/37491
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.