")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
The Translation, Culture-Adaptation and Psychometric Evaluation of the Cardiac Rehabilitation Barriers Scale Among Chinese Older Population
Authors Zhang S, Yu M, Zhang Y, Liang C, Hu D, Wang DW, Meng X
Received 16 November 2023
Accepted for publication 5 February 2024
Published 17 February 2024 Volume 2024:17 Pages 723—734
DOI https://doi.org/10.2147/JMDH.S450135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sisi Zhang,1 Miao Yu,2 Yu Zhang,2 Conying Liang,2 Dayi Hu,1 Dao Wen Wang,1 Xiaoping Meng2
1Division of Cardiology, Department of Internal Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China; 2Department of Cardiology and Cardiac Rehabilitation, Affiliated Hospital of Changchun University of Chinese Medicine, Changchun, 130000, People’s Republic of China
Correspondence: Xiaoping Meng, Department of Cardiology and Cardiac Rehabilitation, Affiliated Hospital of Changchun University of Chinese Medicine, #1473 Gongnong Road, Chaoyang District, Changchun, 130000, People’s Republic of China, Email [email protected]
Purpose: This study aimed to translate and cross-culturally adapt the cardiac rehabilitation barriers scale to the Chinese, and examine its reliability and validity among the older population.
Methods: An approach comprising translation, cultural adaptation, reliability, and validity examination in the Chinese version was conducted in two hospitals in Jilin, China. The t-tests were used to compare the sex differences between each item. Participants included Chinese individuals > 60 who were eligible for the cardiac rehabilitation program.
Results: In total, 325 participants completed the questionnaire with an average age of 61.23 ± 9.68 years. The item-total correlations were 0.432 to 0.678. Factor analysis of CRBS-C (Kaiser Meyer Olkin = 0.867, Bartlett’s test p = 0.000) revealed four factors: logistical factors, comorbidities/functional status, perceived need/healthcare factors, and work/time conflict. The confirmatory factor analysis (CFA) indicated a good model fit (χ 2/df = 1.84, RMSEA = 0.051, CFI = 0.953, TLI = 0.945, SRMR=0.046). Cronbach’s alpha was 0.88 for the scale, ranging from 0.801 to 0.88 for each item, which indicates the internal reliability was acceptable.
Conclusion: The Chinese version of the CRRS has acceptable reliability and validity in the Chinese elderly population.
Keywords: cardiac rehabilitation, internal reliability, cross-cultural adaptation, exploratory factor analysis, confirmatory factor analysis
Introduction
Cardiovascular disease is the leading cause of premature death and disability worldwide, especially in China.1 With the economic and social development and population aging acceleration, the prevalence of CVD in China is increasing. In 2019, there were more than 330 million cases of CVD in China, and 2 out of every 5 deaths from it.2 Meanwhile, as one of the world’s fastest-aging countries, 254 million people in China are more than 60 years old, and this number is projected to reach 402 million by 2040.3 Accounting for older adults (> 60 years) is expected to lead to higher rates of cardiovascular disease, mortality rate, and readmission rate.4
Cardiac rehabilitation (CR) as a multidisciplinary and comprehensive approach that could effectively reduce mortality of cardiac events, has been regarded as a Class Ia recommendation by the American Heart Association (AHA), the American College of Cardiology (ACC), and the European Society of Cardiology (ESC).5,6 Despite the well-known benefits, CR utilization across the world is still low, ranging from 10% to 50%, especially for the older population.7,8
Reasons for CR underuse are identified and involve factors at the patient, provider, and health system levels.9 In an attempt to improve CR attendance and accessibility, a valid scale was necessary to address potential barriers to be mitigated among Chinese, especially for the older population. The Cardiac Rehabilitation Barriers Scale (CRBS) was developed by Grace et al in Canada which assesses barriers to CR participation and enrolment from patient to health system level.10 The final version consists of 21 items and was regarded as the most widely administered and comprehensive tool to assess CR barriers.11,12 It was developed following a review of the literature, and revised with input from cardiologists, and CR staff. The original version of the CRBS consists of 21 items, which are composed of four subscales: logistical factors, comorbidities/functional status, perceived need/healthcare factors, and work/time conflict.10 Each item is scored on a 5-point Likert-type scale(1 -strongly disagree to 5 -strongly agree), with higher scores indicating greater barriers to the CR program. To date, it has been translated into 14 languages, including Colombian-Spanish, French, Persian, Brazilian Portuguese, and Korean. Only one simplified Chinese version of CRBS has been published. In that study, most of the samples (95%) were those who did not participate in the CR program.13
Therefore, the study aimed to translate and cross-culturally adapt the CBRS into Chinese, and to psychometrically validate the Chinese version in the elderly population.
Methods
Translation and Cross-Cultural Adaptation
Based on the best practices, two bilingual native Chinese speakers, that were fluent in the English language performed the translation process.14–16
One of the translators was a cardiologist who had over 10 years of experience in the CR field and who had translated English books. The other translator was an English language PhD proficient in English and Chinese.
The translations were performed independently, and then the two translation versions were reviewed for discrepancies until a consensus was reached. Then, the first translated version underwent backward translation to English by another translator, who did not know about the original version of the scale. The expert panel which was comprised of cardiologists, experts in the CR field, physiatrists, linguists, and CR nurses reviewed the differences between the first version and the back-translated version and developed a preliminary version of the Chinese version of CRBS.
Next, 30 randomly selected volunteers were asked to perform the pretest of the preliminary version. Each subject answered the Chinese version of CRBS, and each item could be selected either “clear” or “not clear”. Some modifications could be made to ensure comprehension.17 Interviewees were patients diagnosed with coronary heart disease, stable angina, and no severe cognitive impairment.
Participants
Patients were recruited from outpatient CR clinics and cardiology wards in 2 hospitals in Jilin Province, China. From October 2022 to March 2023. Patients ≥60 years old who were eligible for the CR program were included. Exclusion criteria include communication and comprehension deficits; serious visual or cognitive illness, and other conditions that would preclude them from completing the questionnaire.
Procedure
One of the CR nurses familiar with the Chinese version of CRBS administrated the questionnaire in person and collected the data via self-report. Before participation, patients were informed of the significance, objective, and anonymous characteristics of the study. As recommended a sample size of 10 subjects per item for the factor analysis, and the 20% drop-up rate, at least 252 participants were recruited.18 Sociodemographic information and clinical data were obtained from the electronic medical record.
The Psychometric Properties Test and Statistical Analysis
SPSS V.26 (IBM) and Analysis of Moment Structures (AMOS) 18.0 were used for the statistical analysis. A descriptive statistic was performed of participant characteristics. Categorical variables were described as absolute and relative frequency, and continuous variables were performed using means ± standard deviation. The independent samples t-test was used for sex differences in each CRBS item. P value <0.05 was considered significant. We also use Pearson’s correlation coefficient to compare each item score and the total score of the scale, and the r-value less than 0.4 will be deleted.19
The content validity of the scale on a 4-point Likert-type scale, ranging from 1 (not at all) to 4 (highly relevant) was evaluated by the expert panel who were involved in the cultural adaptation process, and assessed by the item-level content validity index (I-CVI) and the scale-level content validity index(S-CVI).20 I-CVI was the ratio of the experts ranking the item for 3 or 4 scores, and the S-CVI was the average value of all the I-CVI scores. As recommended, an I-CVI of more than 0.78 and an S-CVI score of 0.9 or higher were considered satisfactory.21,22
Exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were performed to assess the construct validity of the CRBS. As prerequisites, the Kaiser-Meyer-Olkin (KMO) value>0.6, and p < 0.05 for Bartlett’s test of sphericity, then the CFA was performed to verify the factorial structure.23 Factor analysis was performed with the principal components method, with varimax as the rotation method. A scree plot helps identify the number of retained factors.24
Consistent with the original scale, the CRBS scale was specified as a 4-factor, 21-item model to assess model fit. The structural equation modeling with a maximum likelihood parameter estimation method was used to generate parameter estimates. Based on previous reports, 1 ≤ chi-square/df index(χ2/df)≤ 3, goodness-of-fit index (GFI), comparative fit index (CFI), Tucker–Lewis Index (TLI), and the incremental index of fit(IFI) >0.9, root mean square error of approximation (RMSEA) and standardized root mean square residual (SRMR)<0.08 were considered a good model.25,26
Cronbach’s alpha was used to test the internal consistency, while the value more than 0.6 was considered satisfactory.27 To evaluate the test–retest reliability, 50 participants were required to readminister the questionnaire again after the first completion with an interval of one week.28 The Intraclass Correlation Coefficient (ICC) was calculated based on absolute agreement type and two-way mixed effects model, for which more than 0.7 was regarded as good reliability.27,29
Internal consistency analysis and test-retest reliability analysis were performed to test the scale’s reliability. The EFA was conducted to determine the factor structure within the 21 items, and the item could be loaded if the matrix coefficient was greater than 0.4. The CFA was used to confirm the fitness of the exploratory model.
Results
Translation and Cultural Adaptation
Most of the items were retained with subtle adjustments in several domains consistent with the Chinese cultural background. According to the experts’ opinions, the modifications are as follows: Item 20 “it took too long to get referred and into the program” was deleted, and the item “COVID-19”.
Sample Characteristics
Among the 325 participants, the ages ranged from 60 to 81 years old (with an average of 61.23±9.68). Of these, 86% of the respondents participated in Urban Employees Basic Medical Insurance (UEBMI), 12% in Urban Resident Basic Medical Insurance (URBMI), and 2% out-of-pocket. Two-thirds of the participants were male (63.5%, n = 206). The proportion of CHD populations was 43.4%. 279(86%) participated in Phase 2 CR, only 5.8% participated in Phase 1 CR, and 8.2% in Phase 3. Other characteristics of the participants are shown in Table 1.
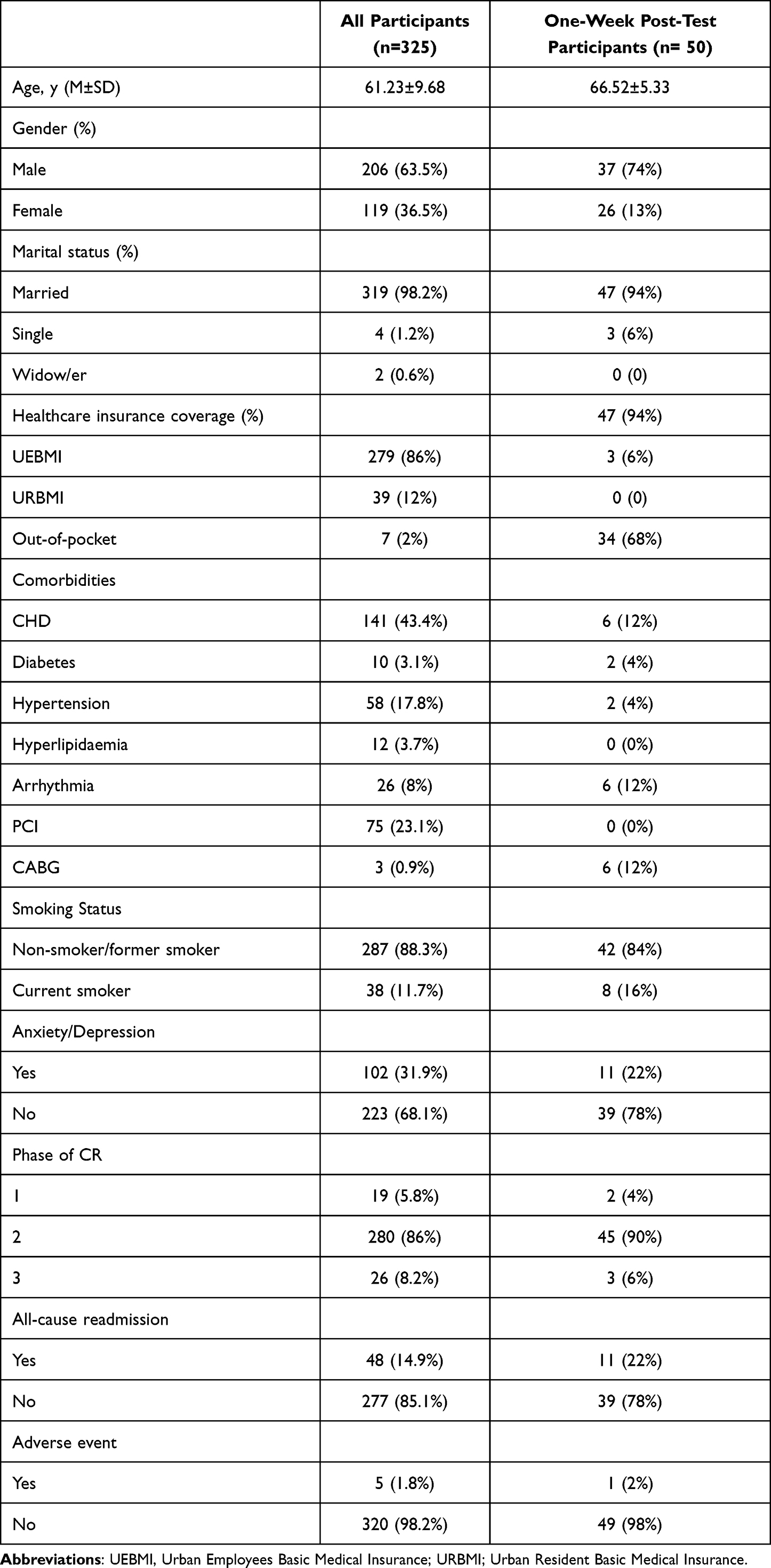 |
Table 1 Basic Characteristics of the Participants |
Content Validity
The I-CVIs ranged from 0.83 to 1.0, and the S-CVI was 0.94, which represents acceptable content validity(Supplementary Table 1).
Construct Validity
Construct validity was analyzed using EFA. The KMO value was 0.867, and Bartlett’s sphericity was χ2=3327.59 (P=0.000), indicating the appropriateness of factor analysis. Four factors with eigenvalues ≥ 1.0 were extracted, which accounted for 62.937% of the total variance. The four factors are named logistical factors, comorbidities/functional status, perceived need/healthcare factors, and work/time conflict. Table 2 shows the eigenvalues and the each variance explained by the four factors. The scree plot is shown in Figure 1. Further, CFA confirmed the four-factor model. The initial analysis revealed fit indices approaching acceptable levels (GFI = 0.881, CFI = 0.915, TLI = 0.902, RMSEA=0.068, IFI = 0.915). Based on the modification indices (MI) recommendations, the model fit could be improved if the error covariance between items 8 and 11, items 14 and 15, and items 1 and 3 were free to covary. After the modifications, all the fit metrics have reached the recommended level (χ2/df =1.84, RMSEA = 0.051, CFI = 0.953, TLI = 0.945, SRMR=0.046), demonstrating that the four-model of the CRBS was acceptable. (Figure 2) (Table 3)
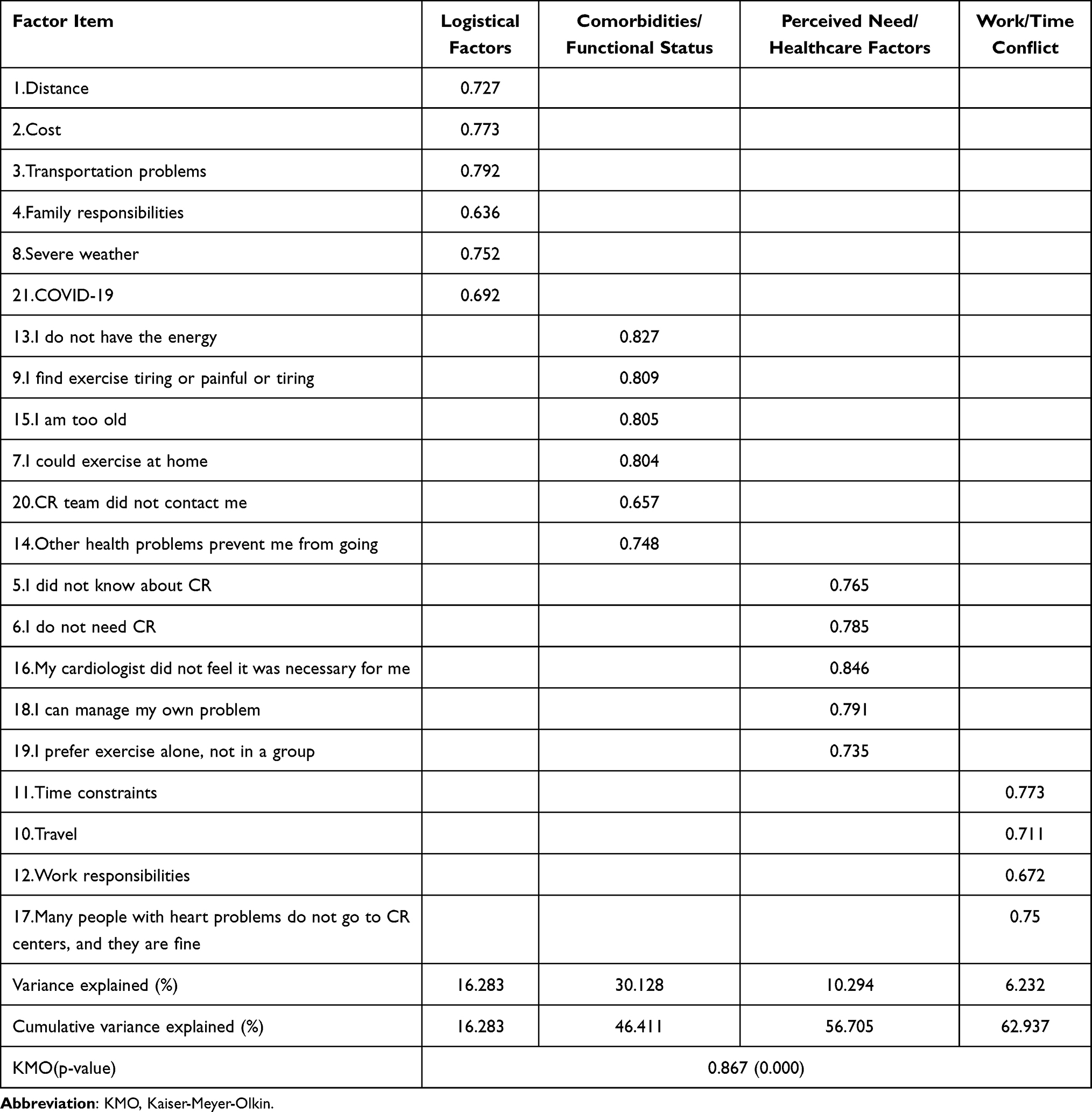 |
Table 2 Exploratory Factor Analysis of CRBS, n=325 |
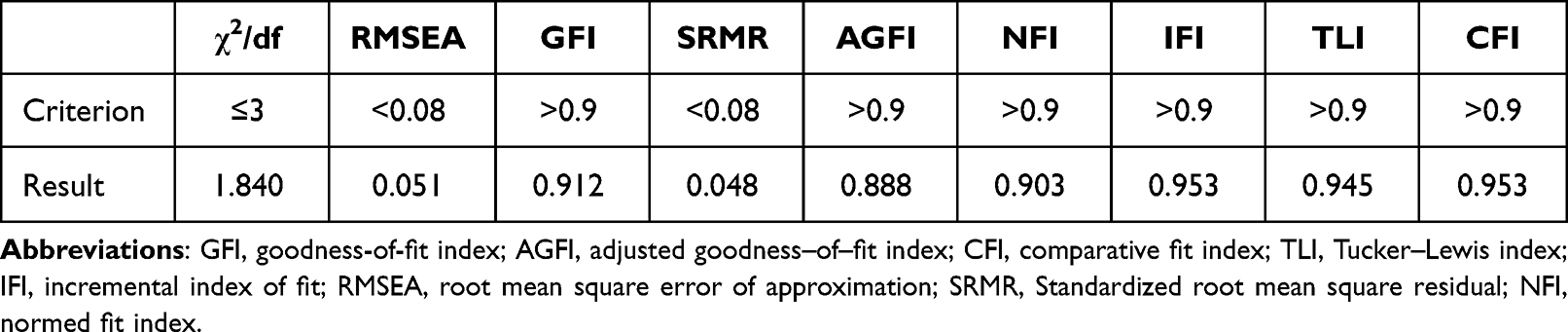 |
Table 3 Goodness of Fit Indices for the Four‐factor Model in the Confirmatory Factor Analysis |
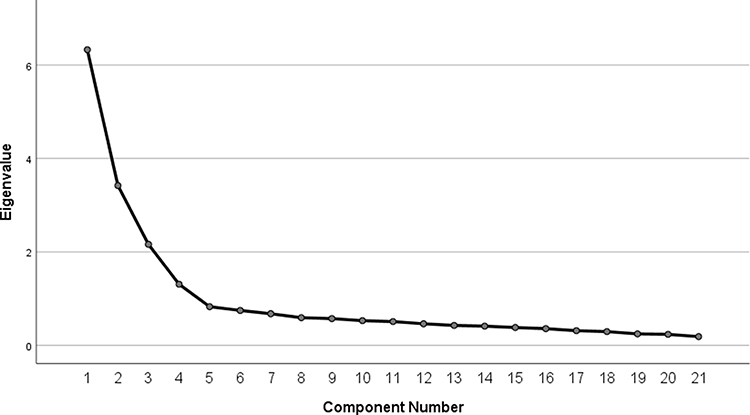 |
Figure 1 Scree plot. |
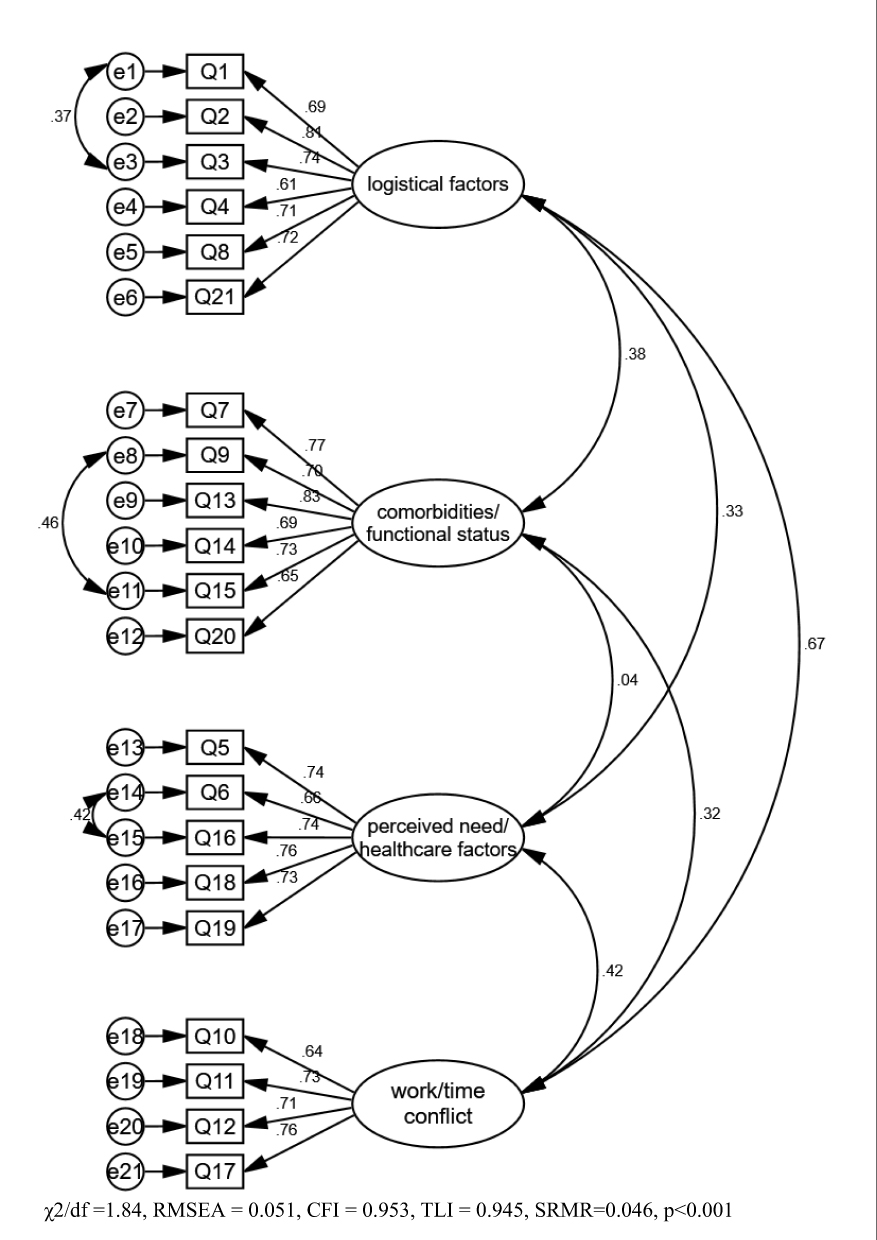 |
Figure 2 Confirmatory factor analysis model with modifications. |
Reliability
Cronbach’s alpha value was accepted for each extracted factor (0.801–0.88). Test–retest reliability was also excellent. The ICC value was 0.99 for logistical factors, 0.942 for comorbidities/functional status, 0.894 for perceived need/healthcare factors, and 0.91 for work/time conflict, respectively. (Table 4). The correlations between each item and the total scores ranged from 0.432 to 0.678 (p<0.01). (Table 5).
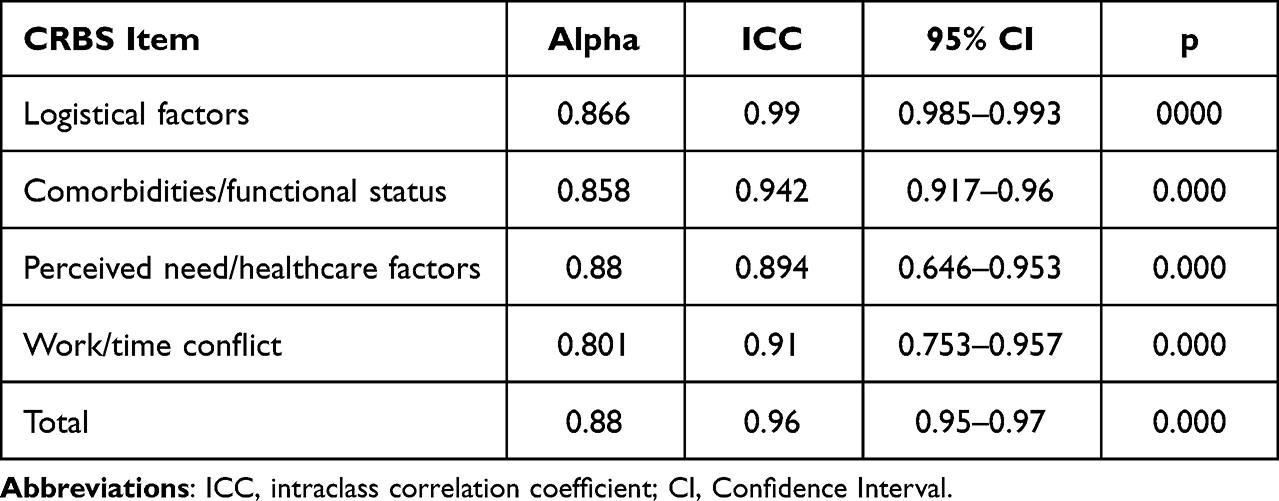 |
Table 4 Internal Consistency and Reliability of the Cardiac Rehabilitation Barriers Scale |
 |
Table 5 The Item-to-Total Correlation results of the Chinese Version of CRBS |
4.5 In this study, the mean CRBS score was 62.92±12.53. There were no differences in scores on each item based on gender (Table 6).
 |
Table 6 Sex Difference by CRBS Item |
Discussion
The Chinese versions of the CRBS were translated, culture-adapted, and validated in elderly patients who participated in the CR program in mainland China. Through the Delphi process, the original scale was made some adjustments for the cultural adaption. The translated version of CRBS consists of four factors and 21 items and shows accepted internal consistency, reliability, and validity among older populations.
In China, there is no corresponding referral system in the CR center, consider this, the item “it took too long to get referred and into the program” was deleted. Meanwhile, in 2019, the coronavirus disease-2019 (COVID-19) outbreak and pandemic had a significant influence on the CR program. Patients with chronic diseases were encouraged to live and work at home to avoid the potential exposure to COVID-19. The center-based CR programs were closed or suspended, and the expert consensus suggested keeping the safety distance between rehabilitation therapists and patients. As per the previous survey, 49.1% of programs completely stopped CR delivery, while 27.1% stopped for a period due to the coronavirus pandemic.30 Hence, “COVID-19” as a barrier of CR was added to this version.
The number of items and the factor structure are consistent with the original English version, as well as the Malay, Greek, and Persian versions (logistical factors, comorbidities/functional status, perceived need/healthcare factors, and work/time conflict), and the overall psychometric properties were favorable.10,31–33 Contrarily, the Brazilian, Turkish, and Mandarin versions identified five factors, and the Korean version revealed six factors, namely: comorbidities/functional limitations, perceived need, external factors (similar to work/time conflicts), logistical factors, healthcare system factors and already exercising.13,34–36 However, the items loading on each factor were different when compared with the original version. For example, item 17 “many people with heart problems don’t go to CR centers, and they are fine” loaded onto the “Work/time conflict” factor, but on the “perceived need/healthcare factors” in the English version, and item 7 “I could exercise at home” and item 20 “CR team did not contact me” loaded onto the “Comorbidities/functional status” factor, but on the “perceived need/healthcare factors” in the English version. These differences are due to cultural background diversity and population specificity. Overall, the factor structure of the scale is viable.
In this study, one week was applied to establish the test–retest reliability, which was satisfactory for all four subscales. Internal consistency of the scale was established with a Cronbach’s alpha value of 0.88. Good internal aggregation was proved by the correlation between each item with the total score (0.432–0.678, P<0.001). Despite the established psychometric properties, the utility of the CRBS in the older population is unknown. To our best known, this is the first reliable and valid study of CRBS among the older population participating in the CR program in China.
The top barriers identified in this study included “I didn’t know about CR”, “Distance”, “Transportation problems”, and “My cardiologist didn’t feel it was necessary for me”, which had also been as main barriers in other studies.13,32 Certainly, lack of physician endorsement and lack of awareness are well-known barriers to CR. Female and older populations, who could gain the most benefit from CR, usually tend to perceive lower physician endorsement.37,38 Travel conditions and distances from home to the CR center are also important for patients with chronic diseases, especially for older people. CR in China is still in the process of developing and maturing, and the referral of CR has also been limited by a lack of enough CR centers nationwide in China. Hence, new CR delivery models are urgently needed. One potential approach is home-based cardiac rehabilitation (HBCR), which can be carried out in various methods, including telemedicine and wearable sensors.
Limitation
First, the participants were recruited from Jilin Province, which was located in the northeast of China, the generalizability to people of other regions remained to be established. Secondly, most of the included participants were male, and patients with Urban Employees Basic Medical Insurance, which may have a selection bias. Finally, 86% of the respondents participated in the Phase II CR program, and barriers may be different during different periods. Further research should be conducted to assess barriers between CR attendees and non-attendees.
Conclusion
The translated Chinese version of CRBS consists of 21 items, and four subscales, with good psychometric properties. It showed good reliability (internally consistent, test–retest), content (including face), and construct (including cross-cultural and structural) validity. In the Chinese older population, the key barriers to participation CR program include“I didn’t know about CR”, “Distance”, “Transportation problems”, and “My cardiologist didn’t feel it was necessary for me”. Mitigation strategies could be further applied to increase CR program utilization in China.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the Affiliated Hospital of Changchun University of Chinese Medicine (protocol code CCZYFYKYLL2023-164).
Data Sharing Statement
The data presented in this study are available on request from the corresponding author.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Yang G, Wang Y, Zeng Y, et al. Rapid health transition in China, 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet. 2013;381(9882):1987–2015. doi:10.1016/S0140-6736(13)61097-1
2. Hu S-S; The Writing Committee. Report on cardiovascular health and diseases in China 2021: an updated summary. J Geriatr Cardiol. 2023;20(6):399–430. doi:10.26599/1671-5411.2023.06.001
3. The L. Population ageing in China: crisis or opportunity? Lancet. 2022;400(10366):1821. doi:10.1016/S0140-6736(22)02410-2
4. Kulmala J, Nykänen I, Hartikainen S. Frailty as a predictor of all-cause mortality in older men and women. Geriatr Gerontol Int. 2014;14(4):899–905. doi:10.1111/ggi.12190
5. Naidu SS, Baran DA, Jentzer JC, et al. SCAI SHOCK stage classification expert consensus update: a review and incorporation of validation studies: this statement was endorsed by the American College of Cardiology (ACC), American College of Emergency Physicians (ACEP), American Heart Association (AHA), European Society of Cardiology (ESC) Association for Acute Cardiovascular Care (ACVC), International Society for Heart and Lung Transplantation (ISHLT), Society of Critical Care Medicine (SCCM), and Society of Thoracic Surgeons (STS) in December 2021. J Am Coll of Cardiol. 2022;79(9):933–946. doi:10.1016/j.jacc.2022.01.018
6. Ambrosetti M, Abreu A, Corrà U, et al. Secondary prevention through comprehensive cardiovascular rehabilitation: from knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur J Prev Cardiol. 2021;28(5):460–495. doi:10.1177/2047487320913379
7. Clark RA, Conway A, Poulsen V, Keech W, Tirimacco R, Tideman P. Alternative models of cardiac rehabilitation: a systematic review. Eur J Prev Cardiol. 2015;22(1):35–74. doi:10.1177/2047487313501093
8. Chong MS, Sit JWH, Choi KC, Suhaimi A, Chair SY. Barriers to cardiac rehabilitation and patient perceptions on the usage of technologies in cardiac rehabilitation: a cross-sectional study. J Clin Nurs. 2023. doi:10.1111/jocn.16919
9. Neubeck L, Freedman SB, Clark AM, Briffa T, Bauman A, Redfern J. Participating in cardiac rehabilitation: a systematic review and meta-synthesis of qualitative data. Eur J Prev Cardiol. 2012;19(3):494–503. doi:10.1177/1741826711409326
10. Shanmugasegaram S, Gagliese L, Oh P, et al. Psychometric validation of the cardiac rehabilitation barriers scale. Clin rehabilitat. 2012;26(2):152–164. doi:10.1177/0269215511410579
11. Ghisi GL, dos Santos RZ, Aranha EE, et al. Perceptions of barriers to cardiac rehabilitation use in Brazil. Vasc Health Risk Manag. 2013;9:485–491. doi:10.2147/VHRM.S48213
12. Grace SL, Gravely-Witte S, Kayaniyil S, Brual J, Suskin N, Stewart DE. A multisite examination of sex differences in cardiac rehabilitation barriers by participation status. J Women’s Health. 2009;18(2):209–216. doi:10.1089/jwh.2007.0753
13. Liu X, Fowokan A, Grace SL, et al. Translation, cross-cultural adaptation, and psychometric validation of the Chinese/Mandarin Cardiac Rehabilitation Barriers Scale (CRBS-C/M). Rehabil Res Pract. 2021;2021:5511426. doi:10.1155/2021/5511426
14. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
15. Bullinger M, Alonso J, Apolone G, et al. Translating health status questionnaires and evaluating their quality: the IQOLA Project approach. International Quality of Life Assessment. J Clin Epidemiol. 1998;51(11):913–923. doi:10.1016/S0895-4356(98)00082-1
16. Van Deyk K, Pelgrims E, Troost E, et al. Adolescents’ understanding of their congenital heart disease on transfer to adult-focused care. Am j Cardiol. 2010;106(12):1803–1807. doi:10.1016/j.amjcard.2010.08.020
17. Reichenheim ME, Moraes CL. Michael Eduardo ReichenheimClaudia Leite Moraes [Operationalizing the cross-cultural adaptation of epidemiological measurement instruments]. Revista de saude publica. 2007;41(4):665–673. Portuguese. doi:10.1590/S0034-89102006005000035
18. Sousa VD, Rojjanasrirat W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. J Eval Clin Pract. 2011;17(2):268–274. doi:10.1111/j.1365-2753.2010.01434.x
19. Kang H. 구성타당도 평가에 있어서 요인분석의 활용 [A guide on the use of factor analysis in the assessment of construct validity]. J Korean Acad Nurs. 2013;43(5):587–594. Korean. doi:10.4040/jkan.2013.43.5.587
20. Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–497. doi:10.1002/nur.20147
21. Almanasreh E, Moles R, Chen TF. Evaluation of methods used for estimating content validity. Res Social Administrative Pharm. 2019;15(2):214–221. doi:10.1016/j.sapharm.2018.03.066
22. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res Nurs Health. 2007;30(4):459–467. doi:10.1002/nur.20199
23. Yang Z, Sun L, Sun Y, Dong Y, Wang A. A conceptual model of home-based cardiac rehabilitation exercise adherence in patients with chronic heart failure: a constructivist grounded theory study. Patient Preference Adherence. 2023;17:851–860. doi:10.2147/PPA.S404287
24. Cattell RB. The scree test for the number of factors. Multivar Behav Res. 1966;1(2):245–276. doi:10.1207/s15327906mbr0102_10
25. Steiger JH. Structural model evaluation and modification: an interval estimation approach. Multivar Behav Res. 1990;25(2):173–180. doi:10.1207/s15327906mbr2502_4
26. Li J, Ding H, Wang Z, et al. Translation, cultural adaptation, reliability, and validity testing of a Chinese version of the self-administered Mediterranean diet scale. Front Nutr. 2022;9:831109. doi:10.3389/fnut.2022.831109
27. Terwee CB, Bot SDM, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42. doi:10.1016/j.jclinepi.2006.03.012
28. Hopkins WG. Measures of reliability in sports medicine and science. Sports Med. 2000;30(1):1–15. doi:10.2165/00007256-200030010-00001
29. Nunnally JC, Bernstein IH. Psychometric Theory. New York: McGraw-Hil; 1994.
30. Ghisi GLM, Xu Z, Liu X, et al. Impacts of the COVID-19 pandemic on cardiac rehabilitation delivery around the world. Global Heart. 2021;16(1):43. doi:10.5334/gh.939
31. Chai LS, Siop S, Putit Z, Lim L, Gunggu A, Tie SF. Translation, adaptation, and validation of the Malay version of the cardiac rehabilitation barriers scale. J Res Nurs. 2020;28(1):e64. doi:10.1097/jnr.0000000000000328
32. Ghanbari-Firoozabadi M, Mirzaei M, Vafaii Nasab M, et al. Cross-cultural adaptation and psychometric validation of the Persian version of the Cardiac Rehabilitation Barriers Scale (CRBS-P). BMJ Open. 2020;10(6):e034552. doi:10.1136/bmjopen-2019-034552
33. Antoniou V, Pasias K, Loukidis N, et al. Translation, cross-cultural adaptation and psychometric validation of the Greek Version of the Cardiac Rehabilitation Barriers Scale (CRBS-GR): what are the barriers in South-East Europe? Int J Environ Res Public Health. 2023;20(5):5. doi:10.3390/ijerph20054064
34. Kenis-Coskun O, Göçmen S, Sağdıç B. Validity and reliability of the Turkish version of “cardiac rehabilitation barriers scale”. Gul Med J. 2019;61(2):59. doi:10.26657/gulhane.00055
35. Ghisi GL, Santos RZ, Schveitzer V, et al. Development and validation of the Brazilian Portuguese version of the Cardiac Rehabilitation Barriers Scale. Arquivos brasileiros de cardiologia. 2012;98(4):344–351. doi:10.1590/S0066-782X2012005000025
36. Baek S, Park HW, Lee Y, Grace SL, Kim WS. Translation, cross-cultural adaptation and psychometric validation of the Korean-Language Cardiac Rehabilitation Barriers Scale (CRBS-K). Ann Rehabil Med. 2017;41(5):858–867. doi:10.5535/arm.2017.41.5.858
37. Tsui CK, Shanmugasegaram S, Jamnik V, Wu G, Grace SL. Variation in patient perceptions of healthcare provider endorsement of cardiac rehabilitation. J Cardiopulm Rehabil Prev. 2012;32(4):192–197. doi:10.1097/HCR.0b013e318255a39d
38. Ades PA, Waldmann ML, McCann WJ, Weaver SO. Predictors of cardiac rehabilitation participation in older coronary patients. Arch Intern Med. 1992;152(5):1033–1035. doi:10.1001/archinte.1992.00400170113021
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.