Back to Journals » Journal of Inflammation Research » Volume 16
The Systemic Inflammation Index Predicts Poor Clinical Prognosis in Patients with Initially Diagnosed Acute Coronary Syndrome Undergoing Primary Coronary Angiography
Authors Gao Y, Li Y ![]() , Chen X, Wu C, Guo Z, Bai G, Liu T, Li G
, Chen X, Wu C, Guo Z, Bai G, Liu T, Li G
Received 14 August 2023
Accepted for publication 7 November 2023
Published 13 November 2023 Volume 2023:16 Pages 5205—5219
DOI https://doi.org/10.2147/JIR.S435398
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Yi Gao,1,* Yuqing Li,1,* Xiaolin Chen,1,* Chen Wu,2 Ziqiang Guo,1 Geng Bai,1 Tong Liu,1 Guangping Li1
1Tianjin Key Laboratory of Logic-Molecular Function of Cardiovascular Disease, Department of Cardiology, Tianjin Institute of Cardiology, the Second Hospital of Tianjin Medical University, Tianjin, 300211, People’s Republic of China; 2Department of Emergency Medicine, The Second Hospital of Tianjin Medical University, Tianjin, 300211, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guangping Li; Tong Liu, Tel +86-022-88328648, Fax +86-022-28261158, Email [email protected]; [email protected]
Background: Systemic inflammation index (SII: neutrophil count * platelet count/lymphocyte count) is a new inflammatory marker that can reflect the degree of systemic inflammatory response after coronary artery disease (CAD). However, the predictive value of the SII for clinical prognosis in patients with initially diagnosed acute coronary syndrome (ACS) has yet to be thoroughly studied.
Patients and Methods: Patients with initially diagnosed ACS who underwent primary coronary angiography in our hospital from January 2019 to April 2021 were included in this study. 757 patients with ACS who underwent primary coronary angiography were enrolled. According to the baseline SII level, the patients were divided into a high SII group and a low SII group. The primary endpoint was major cardiovascular events (MACEs), defined as cardiac death, non-fatal myocardial infarction (MI), and non-fatal stroke.
Results: At a median follow-up of 33.9 months, 140 (18.5%) MACEs were recorded. Receiver operating characteristic (ROC) curve analysis showed that SII’s best cut-off value for predicting MACEs was 713.9*109/L. Kaplan-Meier survival curve analysis showed that the survival rate of the low SII group was higher than the high SII group (P< 0.001). Compared with the low SII group, the risk of MACEs was significantly increased in the high SII group (89 cases (33.3%) vs.51 patients (10.4%), P< 0.001). Univariate and multivariate Cox regression analysis manifested that high SII level was independently associated with the occurrence of MACEs in patients with ACS undergoing primary coronary angiography (adjusted hazard ratio [HR]: 2.915, 95% confidence interval (CI%): 1.830– 4.641, P< 0.001). Adding SII to the conventional risk factor model improved the predictive value of MACEs.
Conclusion: This study showed that elevated SII was associated with adverse cardiovascular prognosis in patients with ACS undergoing primary coronary angiography, making SII a valuable predictor of poor prognosis in patients with ACS undergoing primary coronary angiography.
Keywords: systemic inflammation index, immune response, coronary angiography, acute coronary syndrome, clinical prognosis
Introduction
Results from the World Health Organization show that CAD is a significant health problem worldwide and is a primary cause of morbidity and mortality.1 In 2015 alone, ischemia heart disease caused 8.9 million deaths and 164 million disability-adjusted life years (DALYs) lost.2 In 2019, ischemic heart disease will remain the leading cause of death in the over-fifth age group. However, the age-standardized DALYs lost due to ischemic heart disease decreased significantly.3 Although the mortality from CAD has declined over the past 40 years, it still accounts for nearly one-third of deaths in people over 35 years of age.4 Approximately 50% of this reduction was attributable to enhanced management of the acute phase of the ACS and related complications, effective primary and secondary prevention strategies, and revascularization of CAD.5 Percutaneous coronary intervention (PCI) has been developed with the continuous expansion of its indications. With the improvement of imaging and the improvement of the ability to identify the best location of diseased vessels, more complex CAD have been treated. Finally, the criminals’ blood vessels can get better revascularization, and the clinical prognosis of patients can be improved.6 Identifying high-risk ACS patients and strengthening clinical prognosis management helps reduce the social burden of cardiovascular disease.
Despite significant advances in the diagnosis and treatment of ACS in recent years, significant racial and gender disparities remain.7 Globally, there are substantial differences in rates of vascular remodeling and long-term mortality after ACS.8 With the decline in smoking rates in Western Europe and North America and the use of high-sensitivity troponin in diagnostic analysis in non-ST-segment elevation myocardial infarction (NSTEMI) patients, the proportion of ST-segment elevation myocardial infarction (STEMI) patients is decreasing in high-income countries. However, the in-hospital mortality rate for patients with STEMI and shock remains high, especially in the context of cardiac arrest.9 Therefore, identifying the high-risk ACS population has become an urgent problem to be solved.
Recently, clinical biomarkers based on the results of laboratory tests have helped to objectively assess the severity of the disease and predict the clinical prognosis of patients.10–12 Blood routine and biochemistry have attracted wide attention due to their availability as routine test indicators. These measures are based on blood cell counts (neutrophils, lymphocytes, monocytes, and platelets) and biochemical indicators and include a neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), mononuclear-to-lymphocyte ratio (MLR), SII, and fibrinogen to albumin ratio (FAR).13 When values from two or more different cell lines that interact are considered together, the predictive effect on CAD and mortality increases synergistically.14,15 Considering the complex pathophysiological relationship between CAD and atherosclerosis, the predictive role of inflammatory markers for CAD deserves further study. PLR and MLR have recently been shown to correlate well with CAD and patient mortality.16,17 NLR has also been shown to be an independent predictor of all-cause mortality in ACS patients.18 High FAR is associated with increased left ventricular systolic dysfunction in ACS patients.19
For patients with CAD, SII is significantly associated with the degree of atherosclerosis in patients with stable angina pectoris.20 At the same time, SII is an independent predictor of functional coronary artery stenosis detected by FFR in patients with chronic coronary syndrome. Its predictive efficiency is more vital than that of PLR.21 SII has also been described as an independent predictor of severity in patients with acute pulmonary embolism22 and a predictor of poor clinical prognosis in patients with chronic kidney disease (CKD) who develop ACS.11
Patients with ACS should be routinely treated with dual antiplatelet and statins after PCI, which is helpful for the prognosis of the disease.7 The anti-inflammatory effects of statins have been demonstrated in experimental and clinical settings, and the inhibition of the inflammatory response helps to play a positive role in the progression of atherosclerosis.23 Platelets play an essential role in thrombosis, MI, and stroke. The application of antiplatelet drugs limits the progress of atherosclerosis.24 Therefore, the new inflammatory markers may have a more robust predictive effect on patients with ACS undergoing primary coronary angiography who have not taken antiplatelet and statin drugs.
This research aimed to investigate the value of SII in predicting poor clinical prognosis in patients with ACS undergoing primary coronary angiography.
Materials and Methods
Study Population
We retrospectively collected patients with initially diagnosed ACS undergoing primary coronary angiography and confirmed ACS in our hospital from January 2019 to April 2021. ACS is caused by acute occlusion of the coronary artery. Patients with ACS included unstable angina pectoris, NSTEMI, and STEMI. All STEMI patients received PCI. All non-STEMI patients underwent diagnostic coronary angiography, and PCI was determined according to the degree of coronary artery stenosis. The selection of the study population is represented by a flow chart (Figure 1). The primary endpoint was MACEs, including cardiac death, non-fatal MI, and non-fatal stroke. The secondary endpoints included cardiac death, non-fatal MI, non-fatal stroke, rehospitalization for congestive heart failure (HF), and repeat revascularization.
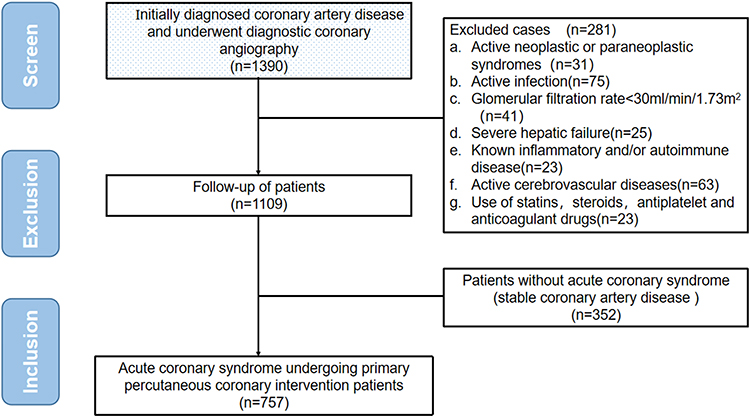 |
Figure 1 Flowchart of the study cohort. |
Exclusion criteria were as follows: (1) active tumor or paraneoplastic syndrome, (2) acute infection, (3) severe renal insufficiency (eGFR<30mL/min/1.73m2), (4) severe liver failure, (5) known inflammatory/autoimmune disease, (6) active cerebrovascular disease, (7) use of statins, steroids, antiplatelet and anticoagulant drugs.
Clinical and Laboratory Data
Electronic medical record systems collected data on demographic characteristics and laboratory test results. Gaps in medical records were obtained by asking the patient about hospitalization. Results of the first venous blood sample and complete blood count were obtained from all hospitalized patients before diagnostic coronary angiography. Regarding biomarkers, NLR is the ratio of neutrophil to lymphocyte count, PLR is the ratio of platelet to lymphocyte calculation, and MLR is the ratio of monocyte matter to lymphocyte. SII is defined as platelet count * neutrophil count/lymphocyte count. FAR is defined as the fibrinogen-to-albumin ratio.
The Youden index determines the best cut-off value of SII. The ROC curve is drawn to calculate the sensitivity and specificity of each SII value, and the sum of the two can get the Youden index. The SII value corresponding to the maximum value of the Youden index is the best cut-off value. According to the optimal cut-off value of SII, we divided the included population into two groups: the high SII group and the low SII group.
These patients were followed by telephone, outpatient review, or inpatient observation and administered by competent medical professionals or nurses. In the course of our actual statistics, patients with cardiac death, non-fatal MI, or non-fatal stroke, any one of these, we will immediately stop follow-up to record an endpoint event. Subsequent end-point events in patients were recorded and not included in the final statistical analysis. The final statistical analysis was based on the patient’s first endpoint event.
Statistical and Analysis
Continuous variables were demonstrated in mean ± standard deviation (SDs) or median (25th to 75th percentile) form and compared using t-tests or Wilcoxon rank-sum tests when appropriate. Categorical variables are shown as numbers with percentages, using Fisher’s exact or chi-square test, as suitable to determine the significance of categorical variables between the two groups. The ROC curve was drawn to calculate the Youden index. The best cut-off value of the biomarker was the value with the highest sum of sensitivity and specificity. Kaplan-Meier curve was used for survival analysis to analyze the prognosis differences and event-free survival rates of patients in different SII groups. Primary and secondary clinical outcomes were presented as percentages and proportions with 95% CIs. After adjusting for individual risk factors, univariate and multivariate Cox regression analyses were used to assess the HRs for combined and individual endpoints with 95% CIs. The multivariate analysis included baseline clinical factors that differed significantly between the two groups (P<0.005). The basic model consisted of known risk factors, including sex, age, hypertension, diabetes, newly diagnosed dyslipidemia, and smoking. To evaluate whether SII added to the base model could improve the ability of the model to predict the endpoint events. Evaluation indicators included C-index, net reclassification improvement (NRI), and integrated discrimination improvement (IDI). Two-tailed P values of within 0.05 were thought statistically necessary. All statistical analyses were performed employing SPSS 27.0, R 4.2.2, and GraphPad Prism 8.0.
Results
Characteristics of Patients
A flow chart shows enrolled and excluded patients (Figure 1). A total of 1390 patients were recruited, and finally, 757 patients with ACS undergoing primary coronary angiography were included in this retrospective study. The ROC curve was drawn to calculate the Youden index. The Youden index determined the optimal cut-off value of SII. We separated the study population into two groups based on the cut-off value of SII, and Table 1 shows the baseline characteristics of the patients after grouping by SII. The proportion of male patients and the proportion of smoking patients were higher in the high SII group. The white blood cell (WBC) count, neutrophil count, monocyte count, and platelet count were higher, and the lymphocyte count was lower. The values were higher for fibrinogen and lower for albumin. The high SII group patients were less likely to receive angiotensin receptor blockers (ARB) and calcium channel blockers (CCB) antihypertensive drugs. The SII, NLR, PLR, MLR, and FAR values of the high SII group were higher than those of the low SII group (P<0.001). The two groups had no statistically significant diversities in other baseline characteristics.
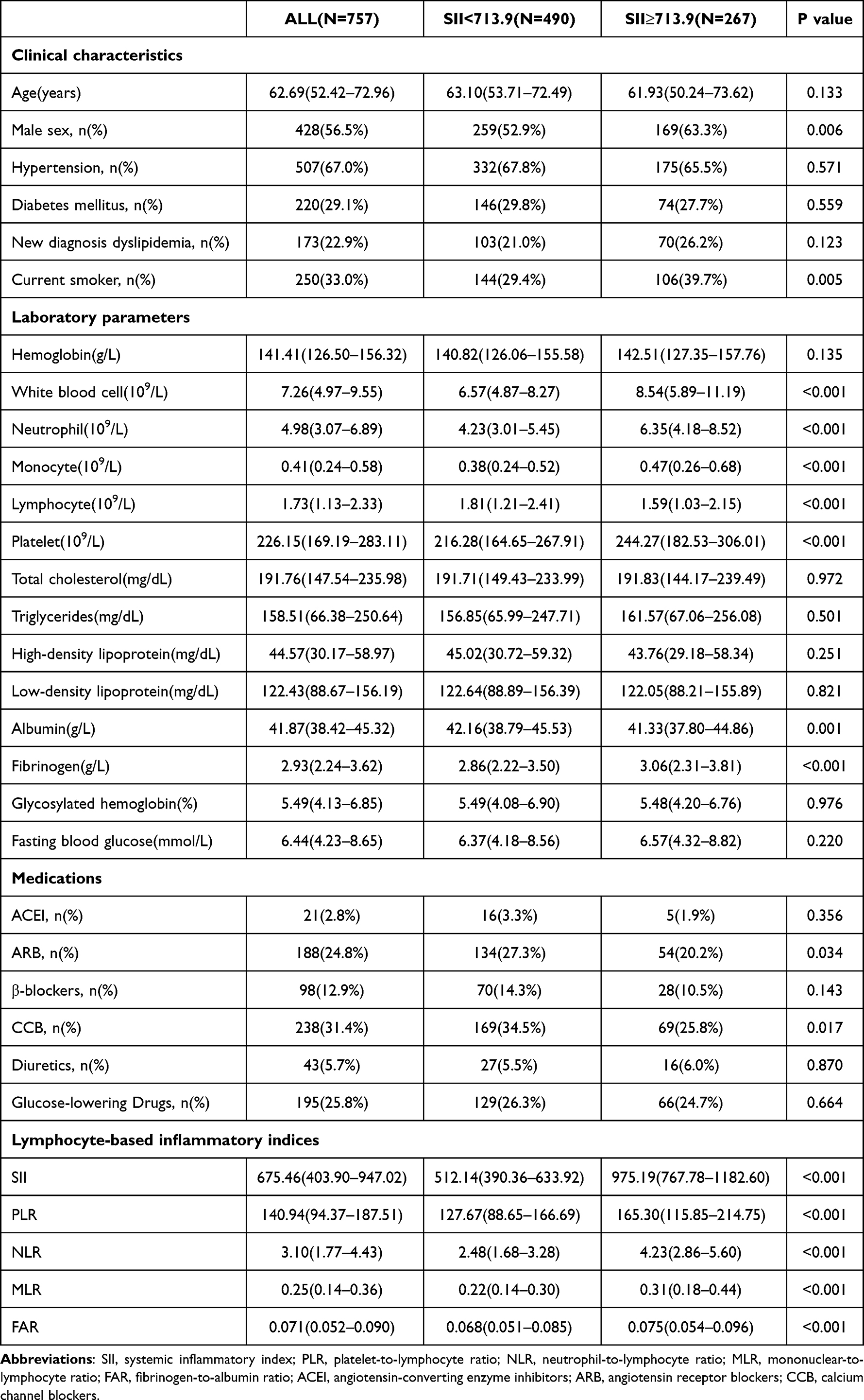 |
Table 1 Baseline Characteristics of 757 Patients with Initially Diagnosed Acute Coronary Syndrome |
ROC Curve and Optimal Cut-off Value
During a median follow-up of 33.9 months, MACEs occurred in 140 (18.49%) patients, including 1 cardiac death, 120 non-fatal MI, and 19 non-fatal strokes. At the same time, 51 patients developed congestive HF for rehospitalization, and 207 underwent revascularization. The optimal cut-off values for SII, NLR, PLR, MLR, and FAR were shown by ROC curves (Figure 2) and determined by calculating the Youden index. Among them, SII had a better predictive performance than the other four (AUC: 0.709, 95% CI (0.660–0.757), P<0.001). ROC curve analysis evaluated the optimal SII cut-off value of 713.9*109/L for predicting MACEs. The optimal cut-off values, 95% CI, sensitivity, and specificity of each biomarker are shown in Table 2.
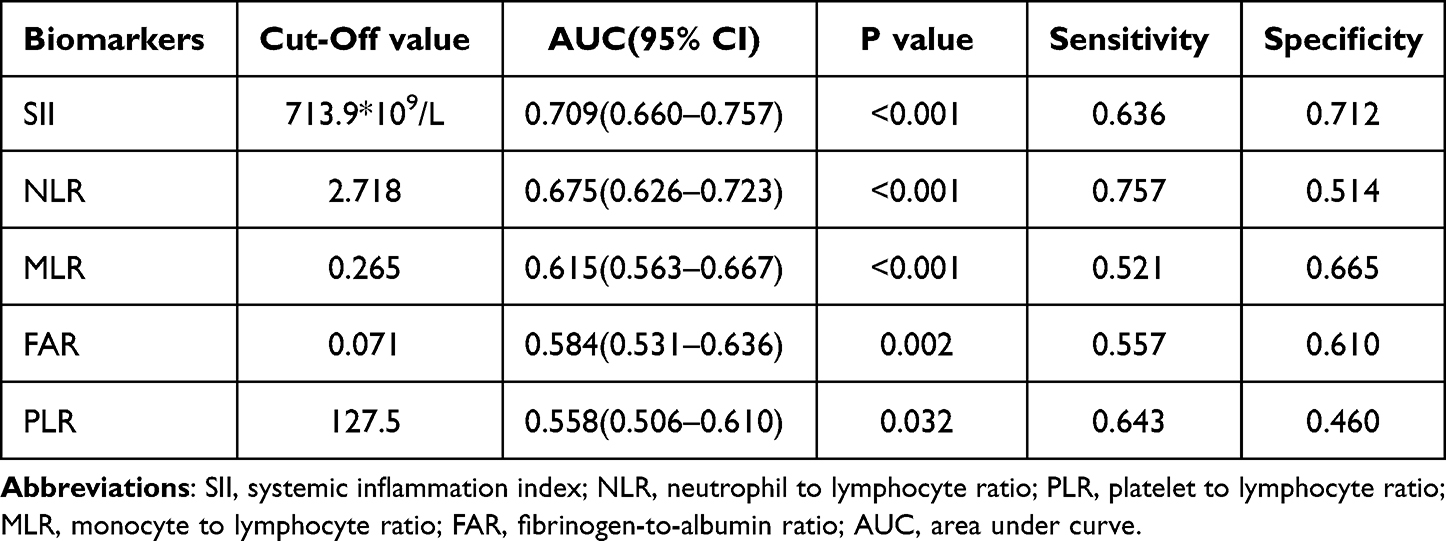 |
Table 2 Receiver Operating Characteristic Curve Analysis |
 |
Figure 2 Receiver operating characteristic (ROC) curve analysis with the area under the curve of SII, NLR, PLR. MLR and FAR in predicting. |
Clinical Endpoint Events After SII Grouping
The clinical outcomes of patients in the low SII group and the high SII group are shown in Table 3. The prevalence of MACEs in the high SII group was higher than that in the low SII group [89 (33.3%) vs 51 (10.4%), P<0.001]. The prevalence of non-fatal MI, congestive HF, and revascularization was higher in the high SII group than in the low SII group. However, there was no statistically significant diversity between the two groups in the rates of cardiac death (P=0.999) and non-fatal stroke (P=0.143). K-M survival curves and Log rank test also showed that the high SII group was associated with an increased risk of MAECs (Figure 3A), non-fatal MI (Figure 3C), non-fatal stroke (Figure 3D), congestive HF for rehospitalization (Figure 3E), and undergoing revascularization (Figure 3F). The risk of cardiac death (Figure 3B) was not increased in the high SII group, and this finding may be related to the small number of patients and the short follow-up period.
 |
Table 3 Clinical Outcomes in Initially Diagnosed Acute Coronary Syndrome Patients According to SII Score |
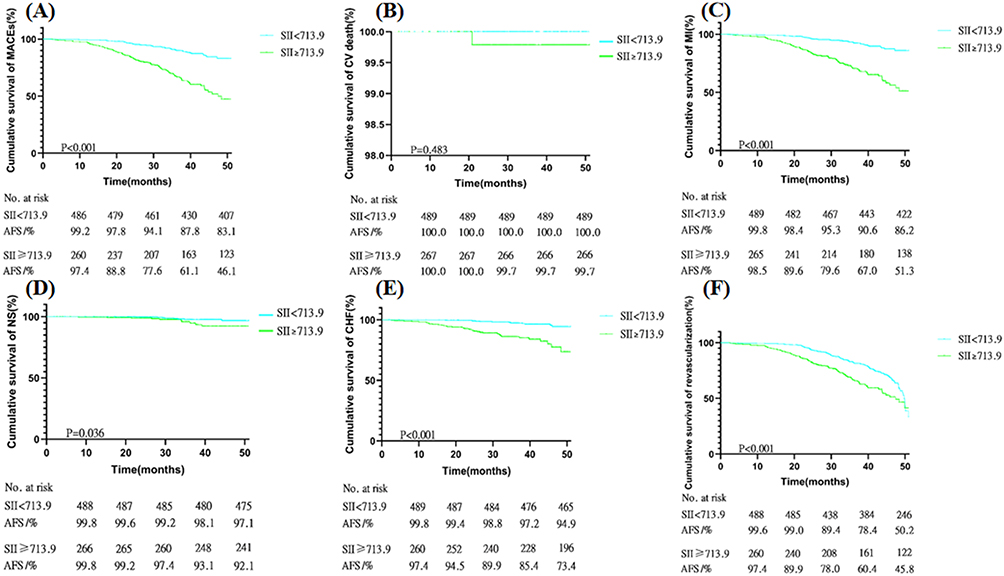 |
Figure 3 Kaplan-Meier survival curve analysis showing: (A) MACEs, (B) cardiac death, (C) non-fatal myocardial infarction, (D) non-fatal stroke, (E) rehospitalization for congestive heart failure, (F) Revascularization. |
Univariate and Multivariate Analysis of SII in Patients with Initially Diagnosed ACS
Univariate and multivariate Cox regression analyses were completed to identify independent indicators of MACEs in patients with initially diagnosed ACS (Table 4). According to Cox regression analysis, SII≥713.9*109/L (HR:2.808, 95% CI (1.776–4.439), P<0.001) was an independent predictor of MACEs. Cox proportional hazards regression model analyses competed in four separate models to test for independent predictors of clinical prognosis (Table 5). The study found that after adjusting for sex, age, hypertension, diabetes, newly diagnosed hyperlipidemia, smoking history, ACEI/ARB, β-blockers, CCB, diuretics, and hypoglycemic drugs, SII≥713.9*109/L was associated with MACEs (HR:3.946, 95% CI (2.764–5.633), P<0.001), non-fatal MI (HR:4.320, 95% CI (2.921–6.390), P<0.001), non-fatal stroke (HR:2.691, 95% CI (1.071–6.761), P =0.035), rehospitalization for congestive HF (HR:5.407, 95% CI (2.855–10.238), P<0.001) and revascularization (HR:1.766, 95% CI (1.331–2.342), P<0.001) was independently associated with increased risk. Cardiac deaths could not be assessed because of the small number of cases.
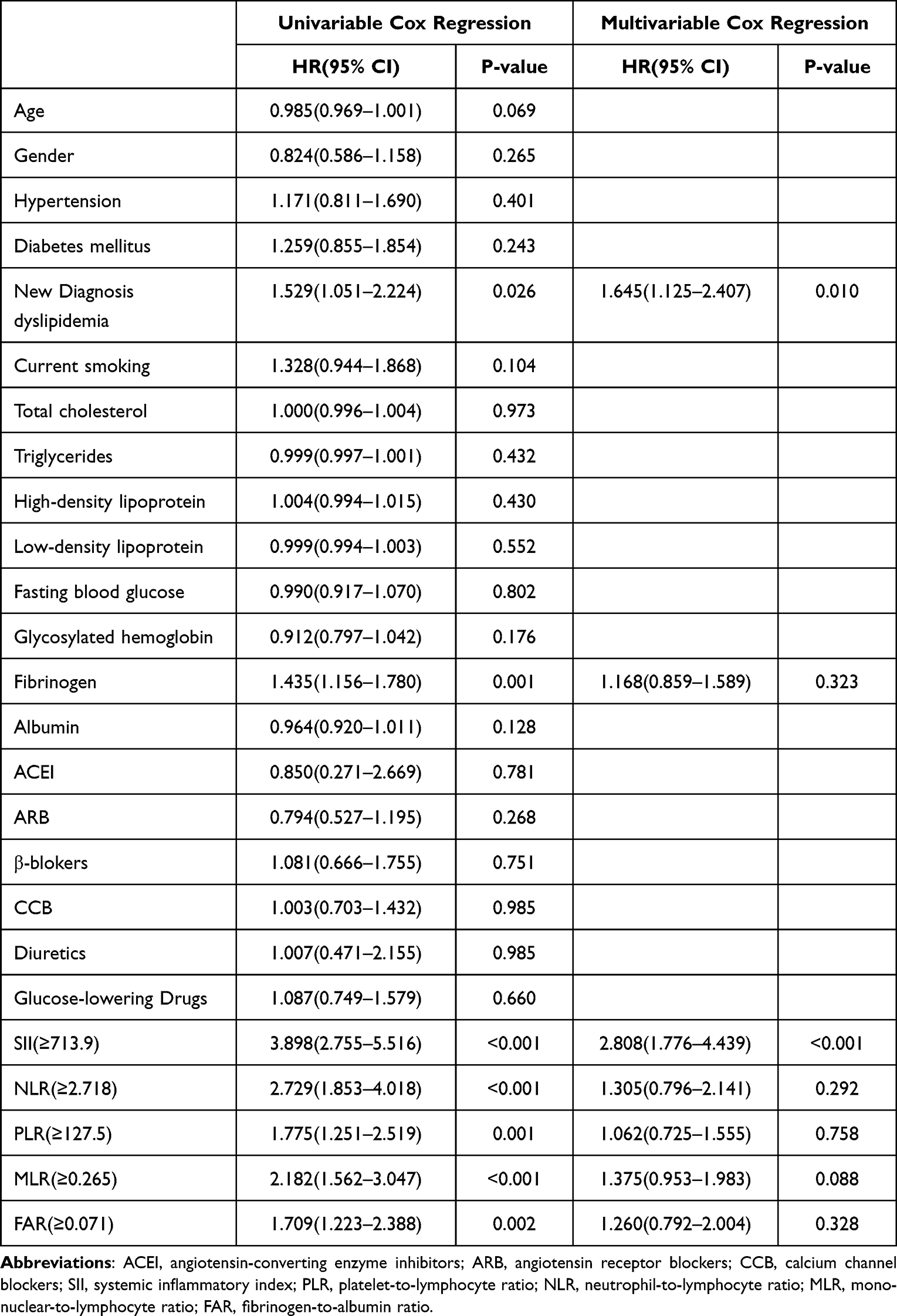 |
Table 4 Cox Regression Analysis |
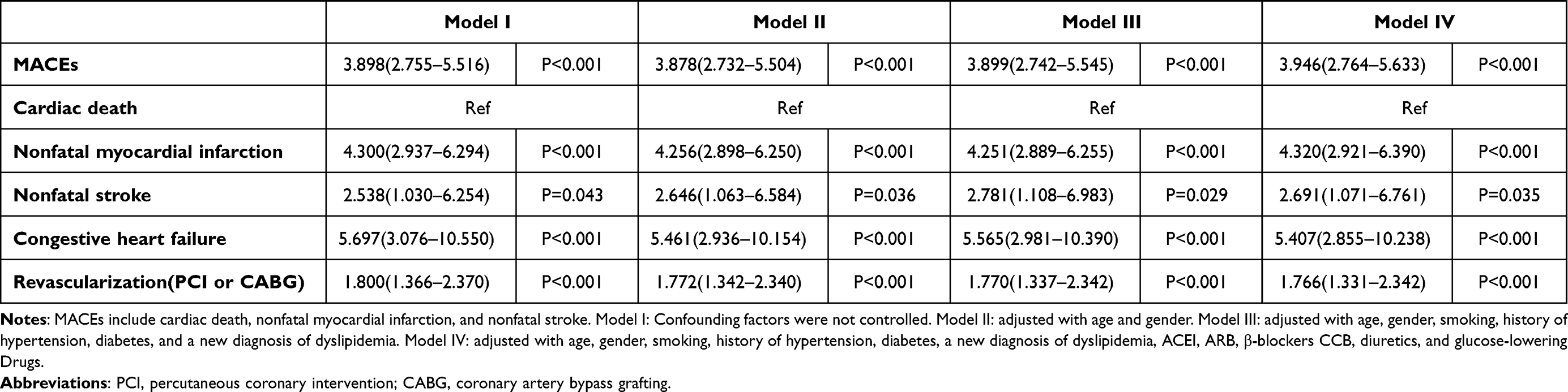 |
Table 5 The Association of High SII (≥713.9*109/L) and Future Adverse Events in Initially Diagnosed Acute Coronary Syndrome Patients |
Subgroup Analysis of SII in Patients with Initially Diagnosed ACS
Subsequent subgroup analysis showed that MACEs with SII≥713.9*109/L remained consistent across different subgroups. Subgroup analysis further confirmed the robustness of the association between SII≥713.9*109/L and major adverse cardiovascular events. See Figure 4 for details.
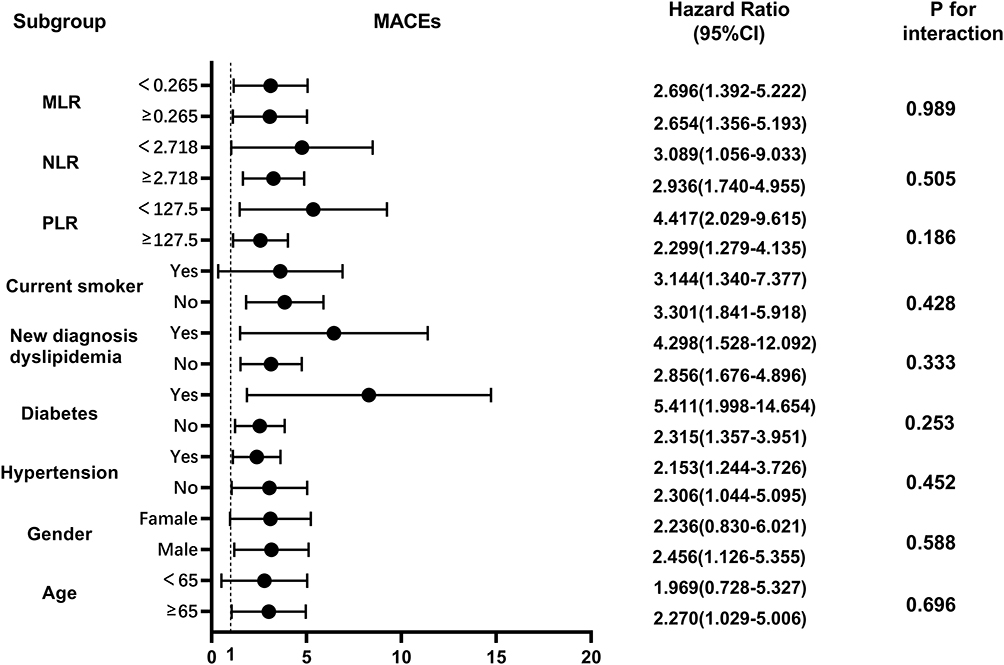 |
Figure 4 Subgroup analysis of the predictive value of high SII vs low SII for MACEs in initially diagnosed acute coronary syndrome patients. |
Additional Effects on MACEs After Adding SII to Baseline Models
Adding SII≥713.9*109/L to the base model with conventional risk factors improved the predictive value of MACEs (P<0.001). As shown in Table 6. In addition, adding SII≥713.9*109/L also improved the predictive value of NRI and IDI for MACEs, with IDI improved by 0.106 (P<0.001) and NRI increased by 8.4% (P=0.011). Adding SII≥713.9*109/L is suggested to increase the predictive value of traditional risk factors for MAECs in patients with initially diagnosed ACS.
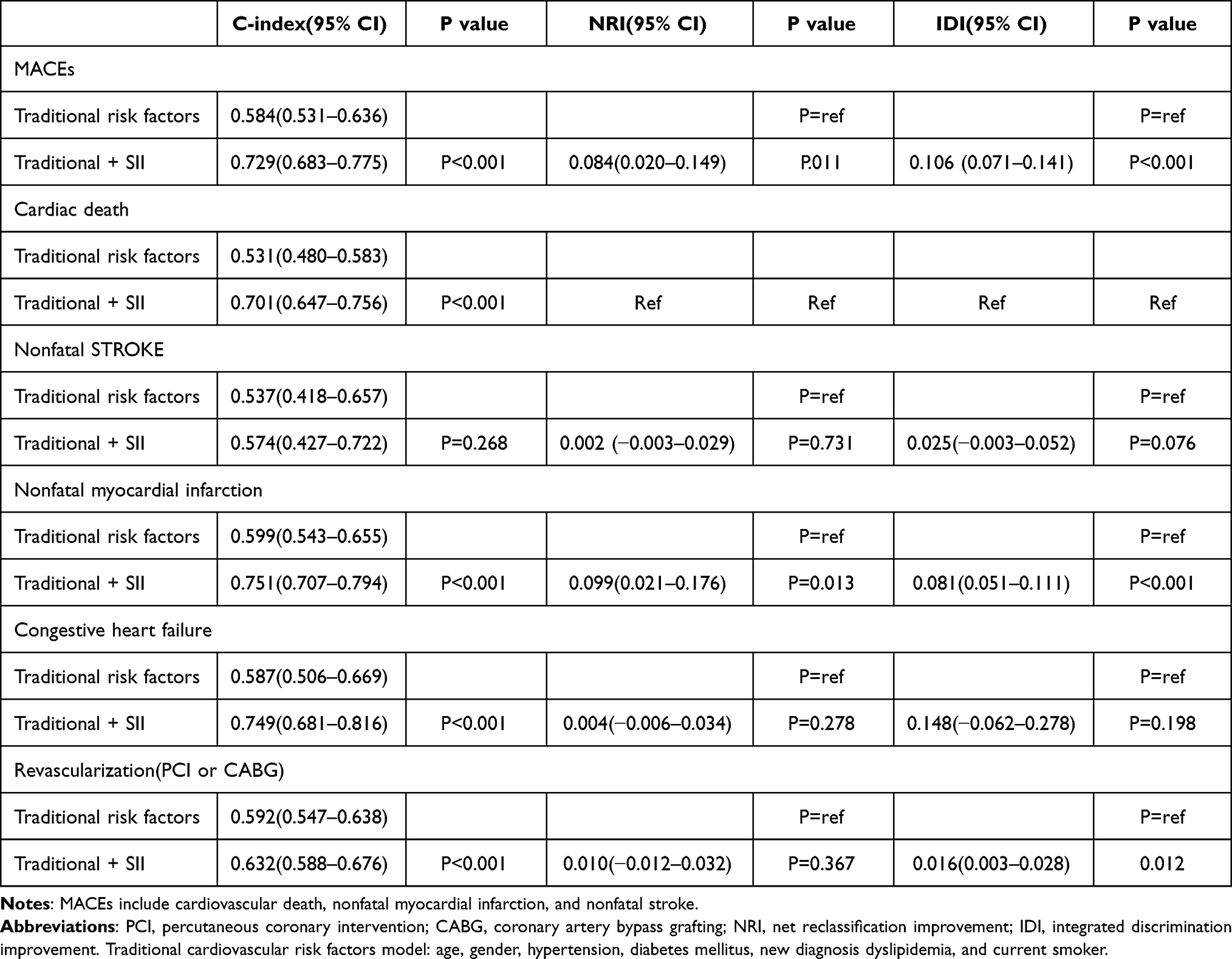 |
Table 6 Evaluation of Predictive Models for Cardiovascular Events |
Discussion
Here, we demonstrate that the novel inflammatory marker SII can be used as an independent indicator of poor clinical prognosis in patients with initially diagnosed ACS. Interestingly, high SII remained independently associated with MACEs, non-fatal MI, rehospitalization for congestive HF, and revascularization, even after controlling for age and other cardiovascular risk factors. At the same time, we demonstrate that adding SII to existing conventional risk factor models can significantly improve the predictive value of predicting MACEs in patients with initially diagnosed ACS. Therefore, SII can be a convenient and reliable indicator to identify high-risk patients with initially diagnosed ACS.
ACS patients have a large population and a high risk of recurrence. In addition, the epidemiology and prognostic characteristics of ACS are still unclear, posing a significant challenge to preventing disease recurrence and managing the clinical prognosis of patients.25 Elevated levels of standard inflammatory markers, such as neutrophils and C-reactive protein, are associated with higher cardiovascular risk in patients with ACS. At the same time, inflammation and its resolution may act as a decisive factor in the occurrence of ACS.26,27 Chronic, low-grade inflammation may contribute to the progression of cardiovascular disease.28 In addition, after recanalization of vascular occlusion in patients with ACS, inflammation can cause myocardial ischemia-reperfusion injury.29 Therefore, research is ongoing to mitigate the risk of inflammatory responses through various therapeutic approaches, and blood cell-based and biochemical biomarkers have recently been extensively investigated due to their easy availability.
Dziedzic et al studied the relationship between SII and the severity of patients with CAD and found that patients with CASSC scores had higher SII values. However, there was no significant difference in SII between patients with different diagnoses, which may be related to the use of statins.10 Plaque types may reflect different levels of inflammation during ACS. The study found significant differences in SII value between mixed plaque and non-calcified plaque rupture.30 Inflammatory markers may also be good screening tools for patients with high-risk CAD. In a prospective follow-up study of 42,875 patients in the United States, SII was associated with cardiovascular and all-cause mortality.31 Data from NHANES also suggest that higher SII dealt with a higher risk of death from cardiovascular disease in individuals with hypertension.32 Interestingly, higher SII was associated with increased total and cardiovascular mortality in middle-aged and older adults, but physical activity benefits these associations.33
The immune system and inflammatory response play an indispensable role in the happening and development of atherosclerosis.34 Various inflammatory cells play a crucial role in the development of atherosclerosis. The rupture and thrombosis of atherosclerotic plaques cause blood stasis in the relevant feeding arteries, and inflammation promotes the initiation of this process.35 Leukocytosis, primarily neutropenia, is an independent risk factor for the development of CAD. Leukocytosis is predictive of adverse cardiovascular events.36
Basic studies have found that CXCR4 and its ligand CXCL12 regulate neutrophil recruitment to atherosclerotic lesions. Chronic blockade of CXCR4 can increase neutrophil recruitment and apoptosis in atherosclerotic lesions, suggesting a proinflammatory role of neutrophils.37 During myocardial ischemia, neutrophils phagocytose dead tissue and release inflammatory mediators: a failed immune response to surviving cardiomyocytes after ischemic injury. Neutrophils are believed to be detrimental during MI but eventually undergo apoptosis and are cleared by macrophages.38 Platelets can regulate the recruitment of white blood cells to atherosclerotic lesions and control inflammation and immune response.39
On the other hand, the expression of matrix metalloproteinase-2 on the surface of living platelets can trigger endothelial PAR-1 pathway expression to initiate atherosclerosis.40 Macrophages are the main components of atherosclerotic plaques. They produce proinflammatory cytokines, participate in lipid retention and vascular remodeling, and express pattern recognition receptors to regulate immune responses.41 Studies have found that lymphopenia positively correlates with MACEs, HF, and poor prognosis in patients with ACS.42
ACS is triggered by thrombosis following the rupture of an atherosclerotic plaque. Fibrinogen levels are elevated after the onset of ACS, and thrombin converts fibrinogen to fibrin, promoting thrombosis.43 Fibrinogen can be used as a simple biomarker to evaluate the level of inflammation in ACS.44 Similarly, albumin levels are decreased at the onset of ACS. The combination of the two markers, FAR, is associated with the increased risk of ACS.45
In addition, some studies have investigated the relationship between inflammatory markers and clinical prognosis in patients with ACS. Fan et al showed that high NLR was independently associated with MACEs in patients with ACS.46 High NLR increased the risk of major cardiovascular ischemic events in patients with ACS receiving ticagrelor dual antiplatelet therapy.47 The study by Yang et al also confirmed that SII was superior to traditional risk factors in predicting major cardiovascular events in patients undergoing CAD after PCI.48
This study also correlated SII with clinical prognosis in patients with initially diagnosed ACS. Our results were compliant with the results of Karadeniz et al; SII had better predictive power than NLR, PLR, MLR, and FAR.49 However, we controlled for factors such as C-reactive protein level and patients taking statins and antiplatelet drugs during the screening process, so the predictive power of SII may be general (AUC: 0.709, 95% CI (0.660–0.757), P<0.001).
In addition, recent studies have shown that the systemic immune inflammatory response index (SIIRI) can be an independent predictor of disease severity in patients with ACS.50 Similarly, our previous studies have also confirmed that SIIRI is associated with adverse cardiovascular prognosis in patients with initially diagnosed CAD, suggesting that SIIRI may be a valuable predictor of adverse prognosis in patients with initially diagnosed CAD.51 In future studies, SIIRI may also become a valuable predictor of inflammation, and the predictive ability of SIIRI with SII in different patient populations needs to be investigated.
In our cohort, the higher proportion of male patients with high SII may be related to the different pathophysiology of underlying coronary microvascular dysfunction between men and women. Men are more likely to meet the “traditional” atherosclerotic profile than women.52 The ROC curve and K-M survival curve were used to evaluate the effect of SII on the poor clinical prognosis of patients with ACS undergoing primary coronary angiography. Higher SII was an independent predictor of poor clinical prognosis in patients with initially diagnosed ACS. Meanwhile, newly diagnosed dyslipidemia remained statistically significant in the adjusted multivariate analysis. Further study should be on whether dyslipidemia before primary coronary angiography is associated with poor clinical prognosis in initially diagnosed ACS patients.
Limitations
Our study has several limitations. First, this study is a single-center, retrospective, observational study with a small sample size that may have selection bias. Secondly, the follow-up of patients in this study was not all completed by patients visiting the hospital, and the telephone follow-up may have a subjective bias of patients and understanding bias of follow-up personnel. Third, we did not include the coronary angiography results or address the effect of differential plaque properties. Fourth, our patient recruitment period is long, and given possible seasonal fluctuations in blood cell ratios, it may limit our ability to draw broad conclusions. Finally, laboratory test results were obtained from the first venous blood collection before diagnostic coronary angiography in all patients after hospitalization, and we did not evaluate the impact of the dynamic evolution of SII on outcome events at the postoperative follow-up of patients. Based on this trial’s observational and retrospective nature, we can only conclude the association and cannot establish any causal link. The results still need to be further verified in multi-center prospective studies.
Conclusion
Elevated SII is associated with adverse cardiovascular prognosis in patients with initially diagnosed ACS, suggesting that SII may be a valuable predictor of poor clinical prognosis in patients with initially diagnosed ACS. The predictive role of SII needs to be validated in more extensive clinical trials.
Ethics Statement
The study complied with the Declaration of Helsinki and was permitted by the Second Affiliated Hospital of Tianjin Medical University (IRB number 2023-05-B023). Patients/participants all signed informed consent before enrollment. Permission was obtained from the patient/participant at each follow-up visit.
Acknowledgments
We gratefully acknowledge the assistance of the Second Hospital of Tianjin Medical University investigators and the participant’s support.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82100342) and the Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-029A).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–25. doi:10.1016/j.jacc.2017.04.052
2. Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1459–1544.
3. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222.
4. Ferreira-González I. The epidemiology of coronary heart disease. Rev Espan De Cardiol. 2014;67(2):139–144. doi:10.1016/j.rec.2013.10.002
5. Ralapanawa U, Sivakanesan R. Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review. J Epidemiol Glob Health. 2021;11(2):169–177. doi:10.2991/jegh.k.201217.001
6. Hoole SP, Bambrough P. Recent advances in percutaneous coronary intervention. Heart. 2020;106(18):1380–1386. doi:10.1136/heartjnl-2019-315707
7. Bergmark BA, Mathenge N, Merlini PA, Lawrence-Wright MB, Giugliano RP. Acute coronary syndromes. Lancet. 2022;399(10332):1347–1358. doi:10.1016/S0140-6736(21)02391-6
8. Dagenais GR, Leong DP, Rangarajan S, et al. Variations in common diseases, hospital admissions, and deaths in middle-aged adults in 21 countries from five continents (PURE): a prospective cohort study. Lancet. 2020;395(10226):785–794. doi:10.1016/S0140-6736(19)32007-0
9. Omer MA, Tyler JM, Henry TD, et al. Clinical characteristics and outcomes of STEMI patients with cardiogenic shock and cardiac arrest. JACC Cardiovasc Interv. 2020;13(10):1211–1219. doi:10.1016/j.jcin.2020.04.004
10. Dziedzic EA, Gąsior JS, Tuzimek A, et al. Investigation of the associations of novel inflammatory biomarkers-systemic inflammatory index (SII) and systemic inflammatory response index (SIRI)-with the severity of coronary artery disease and acute coronary syndrome occurrence. Int J Mol Sci. 2022;23(17):9553. doi:10.3390/ijms23179553
11. Shi S, Kong S, Ni W, et al. Association of the systemic immune-inflammation index with outcomes in acute coronary syndrome patients with chronic kidney disease. J Inflamm Res. 2023;16:1343–1356. doi:10.2147/JIR.S397615
12. Arbel Y, Finkelstein A, Halkin A, et al. Neutrophil/lymphocyte ratio is related to the severity of coronary artery disease and clinical outcome in patients undergoing angiography. Atherosclerosis. 2012;225(2):456–460. doi:10.1016/j.atherosclerosis.2012.09.009
13. Wheeler JG, Mussolino ME, Gillum RF, Danesh J. Associations between differential leucocyte count and incident coronary heart disease: 1764 incident cases from seven prospective studies of 30,374 individuals. Eur Heart J. 2004;25(15):1287–1292. doi:10.1016/j.ehj.2004.05.002
14. Balta S, Ozturk C. The platelet-lymphocyte ratio: a simple, inexpensive and rapid prognostic marker for cardiovascular events. Platelets. 2015;26(7):680–681. doi:10.3109/09537104.2014.979340
15. Han K, Shi D, Yang L, et al. Prognostic value of systemic inflammatory response index in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Ann Med. 2022;54(1):1667–1677. doi:10.1080/07853890.2022.2083671
16. Fan Z, Ji H, Li Y, Jian X, Li L, Liu T. Relationship between monocyte-to-lymphocyte ratio and coronary plaque vulnerability in patients with stable angina. Biomark Med. 2017;11(11):979–990. doi:10.2217/bmm-2017-0235
17. Ayça B, Akin F, Çelik Ö, et al. Platelet to lymphocyte ratio as a prognostic marker in primary percutaneous coronary intervention. Platelets. 2015;26(7):638–644. doi:10.3109/09537104.2014.968117
18. Muhmmed Suliman MA, Bahnacy Juma AA, Ali Almadhani AA, Pathare AV, Alkindi SS, Uwe Werner F. Predictive value of neutrophil to lymphocyte ratio in outcomes of patients with acute coronary syndrome. Arch Med Res. 2010;41(8):618–622. doi:10.1016/j.arcmed.2010.11.006
19. Wang X, Hu Y, Luan H, et al. Predictive impact of fibrinogen-to-albumin ratio (FAR) for left ventricular dysfunction in acute coronary syndrome: a cross-sectional study. Eur J Med Res. 2023;28(1):68. doi:10.1186/s40001-023-01029-2
20. Candemir M, Kiziltunç E, Nurkoç S, Şahinarslan A. Relationship between systemic immune-inflammation index (SII) and the severity of stable coronary artery disease. Angiology. 2021;72(6):575–581. doi:10.1177/0003319720987743
21. Erdoğan M, Erdöl MA, Öztürk S, Durmaz T. Systemic immune-inflammation index is a novel marker to predict functionally significant coronary artery stenosis. Biomark Med. 2020;14(16):1553–1561. doi:10.2217/bmm-2020-0274
22. Gok M, Kurtul A. A novel marker for predicting severity of acute pulmonary embolism: systemic immune-inflammation index. Scand Cardiovasc J. 2021;55(2):91–96. doi:10.1080/14017431.2020.1846774
23. Satny M, Hubacek JA, Vrablik M. Statins and Inflammation. Curr Atheroscler Rep. 2021;23(12):80. doi:10.1007/s11883-021-00977-6
24. Koupenova M, Clancy L, Corkrey HA, Freedman JE. Circulating platelets as mediators of immunity, inflammation, and thrombosis. Circ Res. 2018;122(2):337–351. doi:10.1161/CIRCRESAHA.117.310795
25. Pezel T, Unterseeh T, Hovasse T, et al. Phenotypic clustering of patients with newly diagnosed coronary artery disease using cardiovascular magnetic resonance and coronary computed tomography angiography. Front Cardiov Med. 2021;8:760120. doi:10.3389/fcvm.2021.760120
26. Libby P, Tabas I, Fredman G, Fisher EA. Inflammation and its resolution as determinants of acute coronary syndromes. Circ Res. 2014;114(12):1867–1879. doi:10.1161/CIRCRESAHA.114.302699
27. Libby P, Ridker PM, Hansson GK. Inflammation in atherosclerosis: from pathophysiology to practice. J Am Coll Cardiol. 2009;54(23):2129–2138. doi:10.1016/j.jacc.2009.09.009
28. Kaptoge S, Di Angelantonio E, Pennells L, et al. C-reactive protein, fibrinogen, and cardiovascular disease prediction. N Engl J Med. 2012;367(14):1310–1320.
29. Eisen A, Giugliano RP, Braunwald E. Updates on acute coronary syndrome: a review. JAMA Cardiol. 2016;1(6):718–730. doi:10.1001/jamacardio.2016.2049
30. Yildiz C, Yuksel Y, Rakici IT, Katkat F, Ayça B, Turhan Çağlar FN. Assessment of systemic immune-inflammation index and systemic inflammation-response index in different coronary artery plaque types. Angiology. 2023;74(6):536–544. doi:10.1177/00033197231158937
31. Xia Y, Xia C, Wu L, Li Z, Li H, Zhang J. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and risk of all-cause mortality and cardiovascular mortality: a 20-year follow-up cohort study of 42,875 US adults. J Clin Med. 2023;12(3):1128. doi:10.3390/jcm12031128
32. Cao Y, Li P, Zhang Y, et al. Association of systemic immune inflammatory index with all-cause and cause-specific mortality in hypertensive individuals: results from NHANES. Front Immunol. 2023;14:1087345. doi:10.3389/fimmu.2023.1087345
33. Li H, Wu X, Bai Y, et al. Physical activity attenuates the associations of systemic immune-inflammation index with total and cause-specific mortality among middle-aged and older populations. Sci Rep. 2021;11(1):12532. doi:10.1038/s41598-021-91324-x
34. Galkina E, Ley K. Immune and inflammatory mechanisms of atherosclerosis (*). Annu Rev Immunol. 2009;27:165–197. doi:10.1146/annurev.immunol.021908.132620
35. Medina-Leyte DJ, Zepeda-García O, Domínguez-Pérez M, González-Garrido A, Villarreal-Molina T, Jacobo-Albavera L. Endothelial dysfunction, inflammation and coronary artery disease: potential biomarkers and promising therapeutical approaches. Int J Mol Sci. 2021;22(8):3850. doi:10.3390/ijms22083850
36. Swirski FK, Nahrendorf M. Leukocyte behavior in atherosclerosis, myocardial infarction, and heart failure. Science. 2013;339(6116):161–166. doi:10.1126/science.1230719
37. Zernecke A, Bot I, Djalali-Talab Y, et al. Protective role of CXC receptor 4/CXC ligand 12 unveils the importance of neutrophils in atherosclerosis. Circ Res. 2008;102(2):209–217. doi:10.1161/CIRCRESAHA.107.160697
38. Lowenthal J, Hull SC, Pearson SD. The ethics of early evidence--preparing for a possible breakthrough in Alzheimer’s disease. N Engl J Med. 2012;367(6):488–490. doi:10.1056/NEJMp1203104
39. von Hundelshausen P, Weber C. Platelets as immune cells: bridging inflammation and cardiovascular disease. Circ Res. 2007;100(1):27–40. doi:10.1161/01.RES.0000252802.25497.b7
40. Momi S, Falcinelli E, Petito E, Ciarrocca Taranta G, Ossoli A, Gresele P. Matrix metalloproteinase-2 on activated platelets triggers endothelial PAR-1 initiating atherosclerosis. Eur Heart J. 2022;43(6):504–514. doi:10.1093/eurheartj/ehab631
41. Gerrity RG, Naito HK, Richardson M, Schwartz CJ. Dietary induced atherogenesis in swine. Morphology of the intima in prelesion stages. Am J Pathol. 1979;95(3):775–792.
42. Levy WC, Mozaffarian D, Linker DT, et al. The Seattle heart failure model: prediction of survival in heart failure. Circulation. 2006;113(11):1424–1433. doi:10.1161/CIRCULATIONAHA.105.584102
43. Weitz JI. Insights into the role of thrombin in the pathogenesis of recurrent ischaemia after acute coronary syndrome. Thromb Haemost. 2014;112(5):924–931. doi:10.1160/th14-03-0265
44. Athyros VG, Kakafika AI, Karagiannis A, Mikhailidis DP. Do we need to consider inflammatory markers when we treat atherosclerotic disease? Atherosclerosis. 2008;200(1):1–12. doi:10.1016/j.atherosclerosis.2008.02.026
45. Binti NN, Ferdausi N, Anik MEK, Islam LN. Association of albumin, fibrinogen, and modified proteins with acute coronary syndrome. PLoS One. 2022;17(7):e0271882. doi:10.1371/journal.pone.0271882
46. Fan W, Zhang Y, Gao X, et al. the prognostic value of a derived neutrophil-lymphocyte ratio in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Clin Appl Thromb Hemost. 2021;27:10760296211034579. doi:10.1177/10760296211034579
47. Verdoia M, Nardin M, Gioscia R, et al. Higher neutrophil-to-lymphocyte ratio (NLR) increases the risk of suboptimal platelet inhibition and major cardiovascular ischemic events among ACS patients receiving dual antiplatelet therapy with ticagrelor. Vascul Pharmacol. 2020;132:106765. doi:10.1016/j.vph.2020.106765
48. Yang YL, Wu CH, Hsu PF, et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Invest. 2020;50(5):e13230. doi:10.1111/eci.13230
49. Karadeniz F, Karadeniz Y, Altuntaş E. Systemic immune-inflammation index, and neutrophil to-lymphocyte and platelet-to-lymphocyte ratios can predict clinical outcomes in patients with acute coronary syndrome. Cardiovasc J Afr. 2023;34:1–7. doi:10.5830/CVJA-2023-011
50. Mangalesh S, Dudani S, Mahesh NK. Development of a novel inflammatory index to predict coronary artery disease severity in patients with acute coronary syndrome. Angiology. 2023;33197231151564. doi:10.1177/00033197231151564
51. Li YQ, Bai G, Gao Y, et al. The systemic immune inflammatory response index can predict the clinical prognosis of patients with initially diagnosed coronary artery disease. J Inflamm Res. 2023;16:5069–5082. doi:10.2147/JIR.S432506
52. Kwan AC, Wei J, Ouyang D, et al. Sex differences in contributors to coronary microvascular dysfunction. Front Cardiov Med. 2023;10:1085914. doi:10.3389/fcvm.2023.1085914
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.