")
Back to Journals » Orthopedic Research and Reviews » Volume 14
The Surgical Procedure in Managing Peroneal Tendon Injury: A Case Series
Authors Pitarini A , Anastasia M , Kennedy D, Sumargono E, Kholinne E
Received 15 March 2022
Accepted for publication 8 July 2022
Published 27 July 2022 Volume 2022:14 Pages 255—262
DOI https://doi.org/10.2147/ORR.S351356
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Clark Hung
Astuti Pitarini,1 Maria Anastasia,2 Dave Kennedy,2 Endrotomo Sumargono,1,2 Erica Kholinne1,3
1St. Carolus Bone & Joint Center, St. Carolus Hospital, Jakarta, Indonesia; 2Faculty of Medicine, Universitas Katolik Indonesia Atma Jaya, Jakarta, Indonesia; 3Faculty of Medicine, Universitas Trisakti, Jakarta, Indonesia
Correspondence: Erica Kholinne, Email [email protected]
Introduction: Peroneal tendon injury is one of the pathological ankle conditions which causes pain and is frequently misdiagnosed as ankle sprain. There is a variety of peroneal tendon injuries, depending on the mechanism of injury. We report a series of three peroneal injuries in our institution.
Case Presentation: All three of the patients presented with ankle pain and instability following injuries. There was a presence of peroneus quartus in one of the patients. Retromalleolar pain was revealed in all of the patients, in addition to instability. All of the three patients received open peroneal tendon repair with groove tubular deepening for the 1st patient. Following the surgery, the patients could partially weight-bear after 3– 4 weeks. Full range of motion was restored 6 weeks after surgery.
Discussion: The peroneal muscle functions as a dynamic stabilizer of the ankle, which is vital to control the dynamic stability of the lateral ankle. There is a variety of peroneal injuries ranging from split tear to chronic dislocation. The treatment for peroneal tendon subluxation can be conservative or surgical. There are several surgical techniques for peroneal tendon subluxation repair, such as: 1) direct repair of retinaculum; 2) retromalleolar groove deepening; 3) tendon graft reconstruction; 4) bone block procedure; 5) tendon rerouting procedure.
Conclusion: Peroneal tendon injury should always be considered following inversion ankle trauma, especially in case of chronic lateral retromalleolar pain. Surgeries are often required after failure of conservative treatment which can cause impaired walking, decreased sports performance, or chronic pain and muscle strain.
Keywords: peroneal tendon injury, peroneal tendon surgery, ankle injury
Introduction
Peroneal tendon injury is a common source of ankle pain which is sometimes an under-recognized contributor to lateral ankle pain and dysfunction. It often happens as the result of excessive tension or strain, particularly strain on tendons weakened by degenerative (tendinosis) or inflammatory (tenosynovitis) diseases. There are some types of peroneal injury, such as peroneal tendinosis, which is thickening and swelling of the peroneal tendon and peroneal tendinitis, which is inflammation of the peroneal tendon sheath. Both of these pathological conditions are the result of overuse and repetitive ankle activity that irritates the tendon. Then there is peroneal tendon tear which occurs following subluxation of peroneal tendon or in isolation caused by inversion injuries. Another form of peroneal tendon injury is dislocation due to tear of the peroneal retinaculum.1,2 In this case series, we will report 3 different types of peroneal tendon injuries.
In the United States, it is estimated that peroneal tendon dislocation occurs in 0.3–0.5% of ankle injuries. Mulcahey5 reported that out of 85 professional football players who had tendon injury, 55 of them were diagnosed with peroneal tendon injury. Van Dijk6 found peroneal tendon pathology in 23% to 77% of patients with lateral ankle instability. Another study by Squires7 found that the estimated incidence of peroneal tendon tear ranged between 11–37% in cadaveric samples and up to 30% in patients who underwent surgery for ankle instability.
Peroneal dislocation is a form of ankle injury which is often misdiagnosed as ankle sprain. Although frequently found, peroneal injury is an under-recognized contributor to lateral ankle pain and dysfunction. It is a traumatic injury of the ankle which is caused by dorsiflexion and inversion of the foot with a strong force.1,3 The peroneal longus muscle arises from the proximal third of the fibula and becomes tendinous 3–4 cm proximally from the ankle joint. The tendon lies posteriorly from the lateral malleolus in the retrofibular groove. Any high impact injury with the afore-mentioned mechanism may produce a disruption of the superior peroneal retinaculum (SPR) and allow the tendon to displace anteriorly out from the retrofibular groove. Since the mechanism of injury is similar to that of a lateral ankle sprain, it can lead to a potential misdiagnosis. Therefore, the peroneal tendon injury should be considered as a differential diagnosis of lateral ankle pain following a traumatic ankle injury or a concomitant injury to lateral ligament complex injury.4
Case Presentation
All three patients provided written informed consent for their case details and any accompanying images to be published. Institutional approval is not required to publish case details.
The first patient, a 42 year-old female presented with left ankle pain for 6 months following a twisting injury. Pain was felt with discomfort (giving-away) while doing a light jog and a recurrent sliding of the tendon outside the groove on some motion. Patient was treated with physical therapy and ankle brace for 2 months, however no improvement was observed. Clinical examination revealed boggy swelling and tenderness over the posterolateral aspect of the ankle as shown in Figure 1 and a positive peroneal provocation test. The peroneal tendon was subluxated following active inversion and eversion of ankle. Manipulation of anterior dislocation can also be easily performed both by patient and clinician, as shown in Figure 2. Plain ankle X-ray was unremarkable (Figure 3). Magnetic resonance imaging (MRI) showed a split tear of peroneus brevis tendon at the retromalleolar level.
 |
Figure 1 Clinical photograph of left ankle showing swelling on posterolateral aspect of the ankle. |
 |
Figure 2 Peroneal tendon dislocation visible outside the peroneal groove. The dislocation was manipulated manually by surgeon while patient was under sedation preoperation. |
 |
Figure 3 Ankle X-ray (lateral view). No abnormality found on plain X-ray. |
The second patient, a 31-year-old male, came to the orthopedic clinic with left ankle pain following a twisting injury while playing basketball. He had twisted his ankle several times however this time his ankle was really painful. On physical examination, retromalleolar pain was present in addition to ankle instability. Positive anterior drawer test was noted and talar tilt test showed no end point. MRI result showed peroneal sheath filled with fluid collection in addition to peroneal brevis split tear. Over the lateral ligament complex, the anterior talofibular ligament (ATFL) was redundant and heavily fibrotic. Calcaneofibular ligament (CFL) was fibrotic and redundant as well. Intraarticular pathological findings showed the presence of anterior bony impingement over the distal tibia. We concluded that the source of ankle pain was due to concomitant peroneal tear in lateral ankle instability. We planned to address all symptomatic findings surgically.
The third patient was a 52-year-old male with chronic injury of left ankle. He sustained the trauma through occupational injury more than 10 years ago. He noticed that his tendon often slipped out of the bone however he did not seek treatment. Early this year, he experienced continuous strain and discomfort over peroneal muscle which caused him to seek orthopedic advice. Physical examination revealed dislocated peroneal tendon over the groove without provocation. Tenderness along peroneal muscle belly also noted. MRI showed split tear of peroneal brevis without other significant intra or extra articular injury.
Surgical Technique
An open peroneal tendon retinaculum repair and groove deepening was performed for the first patient. Standard clean and drape was applied with patient under regional anesthesia in supine position and the left leg rotated internally to expose the lateral side of the ankle (Figure 2). A tourniquet was applied around the thigh and was inflated to 300 mmHg for total procedure time of 60 minutes. A longitudinal incision over retromalleolar aspect was made starting from the one third of distal fibula extending to 2 cm distal from the tip of the lateral malleolus. The peroneal tendon sheath was sharply divided to expose the tendon. The superior peroneal retinaculum (SPR) was exposed. Intraoperatively we found an intact peroneal brevis contrary to the MRI findings that showed a split tear peroneal brevis, which is shown in Figure 4. However, intraoperatively we found an accessory peroneal structure in the middle of longus and brevis, often named peroneus quartus. Peroneus quartus is one of the sources of lateral ankle pain. Patients with no history of trauma presenting with chronic ankle pain and findings of peroneus quartus on MRI can undergo peroneal debridement and excision of this accessory peroneus. In this patient, we debrided the edge of peroneal sheath and excised the peroneus quartus. Figure 5 shows the intraoperative exposure of the peroneal tendon. Groove deepening of distal fibula was performed as shown in Figure 6. Peroneal tendon gliding was evaluated, then we proceeded with peroneal sheath repair with two suture anchors (1.8 mm Q-Fix All suture anchor; Smith & Nephew, MA, USA). First anchor was placed 1 cm proximal from tip of lateral malleolus in the center portion of fibula, while second anchor was made 2 cm apart parallel from the first anchor. Sheath was tightened in neutral slightly everted ankle position. Peroneal gliding and ankle range of motion was evaluated. Layered skin closure was performed and wool bandage was applied. Patient was discharged the next day with no weight-bearing protocol for 6 weeks.
 |
Figure 4 Preoperative ankle MRI showed initial diagnosis of peroneal brevis split tear. The yellow circle indicated a split tear of peroneal brevis tendon. |
 |
Figure 5 The peroneal tendon was exposed. |
 |
Figure 6 Anchors were inserted, the newly deepened groove was visible. |
In the second patient, arthroscopic debridement and cheilectomy was performed first to address the intra-articular pathology. Anterior bony impingement was identified and cleared with 4.0 oval burr. Open repair of peroneal was performed through curve incision from retromalleolar level. Peroneal tendons were inspected. We identified a split tear of peroneal brevis. Debridement of frayed tissue and tubularization were performed to repair the peroneal brevis. The tubularization is shown in Figure 7. Gliding of the peroneal tendon was evaluated. Lateral ligament complex repair was performed through standard curvilinear approach. ATFL and CFL were identified. Stump of previous ATFL and CFL were imbricated and repaired with modified Brostrom techniques using 2 suture anchors (1.8 mm Q-Fix All suture anchor; Smith & Nephew, MA, USA).
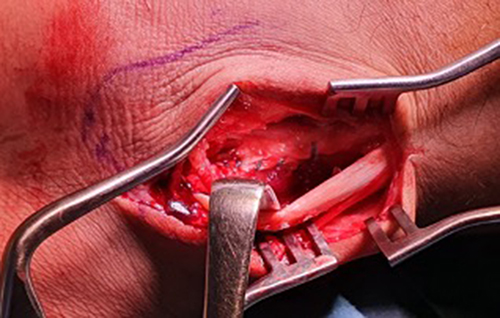 |
Figure 7 Tubularization was performed for peroneal brevis. |
In the third patient, the same retromalleolar incision was made and peroneal tendons were identified. Split tear over peroneal brevis was apparent as shown in Figure 8. Debridement and tubularization were performed and gliding was evaluated. Groove deepening was then performed similar to case number one.
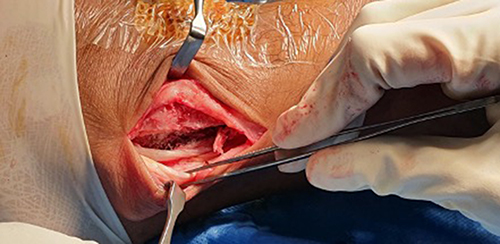 |
Figure 8 Split tear of peroneal brevis tear was identified during surgery, debridement of frayed tissue and tubularization were performed. Note also the groove deepening had been performed. |
The FAAM score was used to evaluate the pre-operative and post-operative physical functioning of the ankle. The post-operative FAAM score was taken 12 weeks following the surgery for the first patient and 24 weeks post-operatively for the second and third patients. The pre-operative score for the first patient was 48 (57%), meanwhile the post-operative score was 82 (98%). In the second patient, the preoperative score was 44 (52%) and the post-operative score was 72 (86%). The third patient got 44 (52%) for the preoperative score and 76 (90%) for the post-operative score. The FAAM scores of all three patients showed that there was an improvement after the surgery.
Following surgery, a posterior splint was applied. All patients were discharged from the hospital after two days. Follow-up in the outpatient clinic was done one week following surgery for wound care and assessment. The ankle was immobilized in a U-slab for 2 weeks after surgery followed by dynamic ankle brace for 4 weeks. Range of motion exercise was started soon after removing brace. After 12 weeks, all patients were able to return to daily activities. Complications following the surgery such as delayed wound healing, wound infection, numbness, and pain were not found in any of the three patients. The instability in all three patients has improved significantly compared to the conditions prior to surgery.
Discussion
The peroneal muscle functions as a dynamic stabilizer of the ankle. A disrupted peroneal function after ankle injury will result in ankle instability, which may lead to persistent pain and swelling. Anatomically, the peroneus longus tendon passes through a fibro-osseous tunnel known as the malleolar-groove posterolaterally to the peroneus brevis tendon, protected by superior peroneal retinaculum (SPR) and inferior peroneal retinaculum (IPR). When there is a sudden ankle inversion, the peroneus muscles are the first muscles to contract as an initial response. Thus, they are vital in controlling the dynamic stability of the lateral ankle. Delayed activation of the peroneal muscles in response to sudden inversion has been a cause of functional instability following lateral ankle sprain.6,8
Peroneal injury often presents with swelling at the posterior side of the fibula or along the lateral wall of the calcaneus, with tenderness along the tendons and also pain with resisted eversion, passive inversion stretch, or resisted plantar flexion. In peroneal tendon tear, acute tears are less common than chronic tears; thus requiring further examinations to diagnose. Brandes Smith classifies peroneal tendon tears according to the anatomical location of the tear. Zone A encapsulates tears which occur under the superior retinaculum, typically as a result of peroneal tendon subluxation or due to the mass effect of a peroneus quartus condition, while zone B is the region of the inferior peroneal retinaculum, where tears may be associated with peroneal tubercle hypertrophy; zone C is the most common site of peroneus longus tendon tear, and is located in the cuboid notch.3 Davda et al1 stated that peroneus brevis tear happens more commonly than peroneus longus tear. It is because peroneal brevis provides more than half of total eversion power. The management of peroneus tendon tear is surgical repair using lateral approach. If the tendon is degenerated severely and tendon repair does not seem feasible, especially when the muscle belly is scarred and heavily fibrotic, tendon transfer using flexor hallucis longus or flexor digitorum longus is preferable.7
Another source of lateral ankle pain is the presence of peroneus quartus. The “overcrowding phenomenon” in retro-malleolar groove can be the source of damage that cause all the pathology event from the peroneus quartus. Associated pathologies are splits or tears in the peroneus brevis and subluxation or dislocation of the peroneal tendon with a thin, lax superior peroneal retinaculum. Usually when it does not cause any symptoms, there is no particular treatment for peroneus quartus. But in symptomatic peroneus quartus, surgical excision is the favorable treatment option.9
Peroneal tendon subluxation occurs when there is a sudden, forceful dorsiflexion of the ankle with hindfoot inversion which causes the contraction of the peroneal tendon and results in SPR disruption. Peroneal dislocation and recurrent subluxation typically manifest as a result of injury to the SPR, the primary ligamentous restraint of the tendons in the distal ankle. When this happens, it will compromise the function of SPR and cause tendon subluxation. Other risk factors include a shallow or convex retromalleolar groove and lateral ankle instability.8 In 1976, Eckert and Davis classified three types of SPR injury after evaluating 73 patients with the injury of SPR. Grade I injury is the most common injury (51% of SPR injuries are classified as grade I injury) and is characterized by an avulsion of the retinaculum from the lateral malleolus. This will result in a subluxation of the tendon into this pouch between the periosteum and fibula. In Grade II injury, there is an avulsion in the fibrocartilaginous ridge and the retinaculum, and the tendon is subluxated into this pouch. In Grade III injury, the least common type, a posterolateral aspect of fibula containing the cartilaginous rim is avulsed and bone flakes permit the tendon to slide beneath the periosteum.7
The treatment for peroneal tendon subluxation can be conservative or surgical. Initial treatment of peroneal tendinosis is nonoperative. Early diagnosis and immediate treatment of peroneal tendon sheath disorders may help prevent progression to more complex injuries, such as tendon rupture. This includes nonsteroidal anti-inflammatory drugs (NSAIDs), rest, ice, compression, elevation, and ankle brace application as a non-invasive option to stabilize the ankle and provide added protection from further injury. When conservative management fails or chronic instability occurs, surgical intervention is preferable. There are some surgical techniques for peroneal tendon subluxation repair, as follows: 1) direct repair of retinaculum; 2) retromalleolar groove deepening; 3) tendon graft reconstruction; 4) bone block procedure; 5) tendon rerouting procedure. Since there is no consensus among foot and ankle surgeons and there is a wide variation of surgical techniques, no randomized study has been performed to determine which surgical technique is superior.4,7 Direct repair of retinaculum is mostly used in an emergency situation. However, this technique is not sufficient to stabilize the subluxated tendon in patients with a convex fibular groove, therefore it will be unable to achieve a complete repair. Direct repair is usually combined with other surgical methods. Peroneal tendon reconstruction aims to repair the peroneal retinaculum by transposition of the ligament soft tissue, such as Achilles tendon, plantar fascia, or calcaneofibular ligament. Bone blocking procedure, first described by Kelly, is a procedure which includes osteotomy of the distal fibula and backward rotation to deepen the fibular notch. Yet, the procedure has some limitations such as complexity, osteotomy complications, internal fixation complications, fracture of the transplanted bone, tendon irritation, non-union, and recurrent subluxation.10,11 Tendon rerouting procedure, or tendon rearrangement is reported to result in pain improvement, functional recovery, and resolution of swelling. Yet it is also found to have a high incidence of sural nerve injury and ankle ankylosis as surgical complications.12 In a study conducted in France by Borgault,13 there were 30 patients with peroneal tendon injury who were treated using various surgical techniques mentioned previously. The study confirmed that the result was satisfactory.
A systematic review study by van Dijk14 reported that rehabilitation is essential following the surgery regardless of the surgical technique. Patients are permitted to partially weight-bear after four weeks. The study also stated that six weeks post-operative, physiotherapy needs to be initiated to restore the range of motion (ROM) and strength. The patient can start with active full ROM exercise: dorsiflexion, plantar flexion, inversion and eversion.
There was no significant difference between three patients who received various surgical techniques and the result was satisfactory. From our study, we can conclude that surgical treatment of peroneal tendon injury following failed conservative treatment is generally successful and has a satisfactory result. However, from another study we found that there was no superiority of one procedure over another in respect to chronicity, severity or satisfaction score.13 The post-operative result showed that overall clinical outcomes were positive in lieu of various surgical interventions for peroneal tendon tears. A weakness of this study is the small number of patients in our case series.
Conclusion
Peroneal tendon injury should always be considered following inversion ankle trauma, especially in case of chronic lateral retromalleolar pain. A variety of peroneal injuries should be considered ranging from split tear to chronic dislocation. Surgeries are often required after failure of conservative treatment that can cause impaired walking, decreased sports performance, or chronic pain and muscle strain, in order to achieve a good result. There is no specific study that has determined the relative effectiveness of one surgical technique over another. In our study, we did the surgical intervention for all of the patients with various surgical techniques and the clinical outcomes of all three patients were satisfactory with no complication found.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Davda K, Malhotra K, O’Donnell P, Singh D, Cullen N. Peroneal tendon disorders. EFORT Open Rev. 2017;2:6. doi:10.1302/2058-5241.2.160047
2. Lugo-Pico JG, Kaiser JT, Sanchez RA, Aiyer AA. Peroneal tendinosis and subluxation. Clin Sports Med. 2020;39(4):845–858. doi:10.1016/j.csm.2020.07.005
3. Bahad SR, Kane JM. Peroneal tendon pathology. Orthop Clin North Am. 2020;51(1):121–130. doi:10.1016/j.ocl.2019.09.001
4. Danna NR, Brodsky JW. diagnosis and operative treatment of peroneal tendon tears. Foot Ankle Orthop. 2020;5(2):247301142091040. doi:10.1177/2473011420910407
5. Mulcahey MK, Bernhardson AS, Murphy CP. The epidemiology of ankle injuries identified at the national football league combine, 2009–2015. Orthop J Sports Med. 2018;6(7):232596711878622. doi:10.1177/2325967118786227
6. van Dijk PAD, Kerkhoffs GMMJ, Chiodo C, DiGiovanni CW. Chronic disorders of the peroneal tendons. J Am Acad Orthop Surg. 2019;27(16):590–598. doi:10.5435/JAAOS-D-18-00623
7. Squires N, Myerson MS, Gamba C. Surgical treatment of peroneal tendon tears. Foot Ankle Clin. 2007;12:4. doi:10.1016/j.fcl.2007.08.002
8. Sharma A, Parekh SG. Pathologies of the peroneals: a review. Foot Ankle Spec. 2021;14(2):170–177. doi:10.1177/1938640020916278
9. Dangintawat P, Apinun J, Huanmanop T, Agthong S, Akkarawanit P, Chentanez V. Unusual accessory peroneal muscles, peroneus quartus, peroneus digiti quinti, and their association with peroneus brevis tendon tear. Asian Biomed. 2019;12:3. doi:10.1515/abm-2019-0011
10. Hu M, Xu X. Treatment of chronic subluxation of the peroneal tendons using a modified posteromedial peroneal tendon groove deepening technique. J Foot Ankle Surg. 2018;57(5):884–889. doi:10.1053/j.jfas.2018.03.009
11. Suh JW, Lee JW, Park JY, Choi WJ, Han SH. Posterior fibular groove deepening procedure with low-profile screw fixation of fibrocartilaginous flap for chronic peroneal tendon dislocation. J Foot Ankle Surg. 2018;57(3):478–483. doi:10.1053/j.jfas.2017.10.033
12. Nishikawa DRC, Duarte FA, Saito GH. Reconstruction of the peroneus brevis tendon tears with semitendinosus tendon autograft. Case Rep Orthop. 2019;2019:1–6. doi:10.1155/2019/5014687
13. Bourgault C, Pougès C, Szymanski C. Clinical results of peroneal tendon repair in a retrospective series of 30 patients. Orthop Traumatol. 2018;104(4). doi:10.1016/j.otsr.2018.01.020
14. van Dijk PAD, Lubberts B, Verheul C, DiGiovanni CW, Kerkhoffs GMMJ. Rehabilitation after surgical treatment of peroneal tendon tears and ruptures. Knee Surg Sports Traumatol Arthrosc. 2016;24(4):1165–1174. doi:10.1007/s00167-015-3944-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.