")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 11
The State of Systematic Therapies in Clinic for Hepatobiliary Cancers
Authors Chen W, Hu Z, Li G, Zhang L , Li T
Received 13 December 2023
Accepted for publication 16 March 2024
Published 27 March 2024 Volume 2024:11 Pages 629—649
DOI https://doi.org/10.2147/JHC.S454666
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Manal Hassan
Weixun Chen,1 Zhengnan Hu,1 Ganxun Li,1 Lei Zhang,1 Tao Li2
1Hepatic Surgery Centre, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, 430030, People’s Republic of China; 2Department of Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, 430022, People’s Republic of China
Correspondence: Tao Li; Lei Zhang, Email [email protected]; [email protected]
Abstract: Hepatobiliary cancer (HBC) includes hepatocellular carcinoma and biliary tract carcinoma (cholangiocarcinoma and gallbladder carcinoma), and its morbidity and mortality are significantly correlated with disease stage. Surgery is the cornerstone of curative therapy for early stage of HBC. However, a large proportion of patients with HBC are diagnosed with advanced stage and can only receive systemic treatment. According to the results of clinical trials, the first-line and second-line treatment programs are constantly updated with the improvement of therapeutic effectiveness. In order to improve the therapeutic effect, reduce the occurrence of drug resistance, and reduce the adverse reactions of patients, the treatment of HBC has gradually developed from single-agent therapy to combination. The traditional therapeutic philosophy proposed that patients with advanced HBC are only amenable to systematic therapies. With some encouraging clinical trial results, the treatment concept has been revolutionized, and patients with advanced HBC who receive novel systemic combination therapies with multi-modality treatment (including surgery, transplant, TACE, HAIC, RT) have significantly improved survival time. This review summarizes the treatment options and the latest clinical advances of HBC in each stage and discusses future direction, in order to inform the development of more effective treatments for HBC.
Keywords: hepatobiliary cancer, systemic treatment, combination therapies
Introduction
Primary hepatobiliary cancer includes hepatocellular carcinoma (HCC) and biliary tract carcinoma (BTC), the latter of which is stratified into cholangiocarcinoma (CCA) (ie, intrahepatic CCA (iCCA), perihilar CCA and distal CCA (eCCA)) and gallbladder carcinoma (GBC). Hepatocellular carcinoma (HCC) is the sixth most commonly diagnosed and the third most lethal malignancy.1 Hepatitis B virus (HBV) infection is the major aetiological factor in HCC worldwide, accounting for ~50% of cases.2 The risk of HCC due to hepatitis C virus (HCV) infection has been significantly reduced as patients have achieved a sustained virological response (SVR) with antiviral drugs. Nevertheless, patients with HCV-induced cirrhosis are considered to be at high risk for HCC even after HCV clearance.3 In addition, chronic alcohol consumption, non-alcoholic steatohepatitis (NASH) and environmental (aflatoxin, aristolochic acid and tobacco) factors have been identified as contributing to cancer development through different specific pathways.4,5 Other less common risk factors for HCC include cirrhosis caused by primary biliary cholangitis (PBC), hemochromatosis, and α1-antitrypsin deficiency. PBC is an autoimmune disease that destroys the small bile ducts in the liver, which can ultimately lead to cirrhosis and indirectly cause liver cancer.6 Hemochromatosis is a genetic disease that leads to an excess of iron in the body. The surplus iron is stored in organs, including the liver, which can cause a series of problems, including hepatitis, cirrhosis, and liver cancer. Alpha-1 antitrypsin deficiency is a genetic disease characterized by a lack of a protein called alpha-1 antitrypsin, which can potentially harm the lungs and liver. Studies have shown that alpha-1 antitrypsin deficiency is associated with cirrhosis and liver cancer. These factors, although less common than viral hepatitis, alcoholic liver disease, or non-alcoholic fatty liver disease (NAFLD), are still noteworthy risk factors for HCC.7 The age-standardized death rate for intrahepatic cholangiocarcinoma (iCCA) increased from 2.15 per 100,000 people in 2009 to 2.95 per 100,000 people in 2018. Similarly, the age-standardized death rate for extrahepatic cholangiocarcinoma (eCCA) increased from 0.28 per 100,000 people in 2009 to 0.39 per 100,000 people in 2018. In contrast, over the course of 10 years, the death rate related to gallbladder cancer decreased from 1.0 per 100,000 people in 2009 to 0.87 per 100,000 people in 2018.8 Potential risk factors for biliary tract tumors include chronic biliary diseases such as primary biliary cholangitis and cholelithiasis; cirrhosis and hepatitis, especially hepatitis B or C; genetic factors like Lynch syndrome and familial adenomatous polyposis may increase the risk of biliary tract tumors in patients; Parasitic infections with Clonorchis sinensis and liver flukes may increase the risk of biliary tract tumors.9–11 In addition, cystic biliary tract diseases are predisposing conditions for bile stasis and stone formation, such as Caroli’s disease, with the incidence of biliary tract cancer (BTC) typically ranging between 7% and 14%.12
After completing disease-related examinations, HCC and BTC patients will formulate treatment plans developed, respectively, according to the Barcelona Clinic Liver Cancer (BCLC) staging system and the 8th edition of the American Joint Committee on Cancer (AJCC) Cancer Staging Manual. Surgical resection is the cornerstone of curative treatment, but it should only be undertaken in the early stages. The conventional treatment philosophy is that for patients with BCLC-B (intermediate stage) HCC, the recommended treatment is typically transarterial chemoembolization (TACE). In addition, in patients presenting with BCLC-C (advanced stage) who are no longer eligible for locoregional or curative therapies, systemic therapies are the only recommended treatment that can provide survival benefits.13 After understanding disease staging (eg, carcinogenic landscape, vascular involvement, distant metastasis), tumor biology, identification of positive predictive biomarkers, molecular mechanisms of resistance to immunotherapy, and liver function grade, novel systemic therapies combined with or without multi-modality treatment are continually being tried, aiming to achieve the best survival prospects. In this review, we summarize the latest advancements in systemic therapies for HBC, outline the clinical findings of systemic therapy combined with other treatments and provide some perspectives for the future.
Therapeutic Landscape for Advanced HCC
The Barcelona Clinic Liver Cancer (BCLC) staging system is used to classify patients with HCC into five stages: 0 (very early), A (early), B (intermediate), C (advanced), and D (end-stage). This staging system provides therapeutic strategies for each stage. Advanced HCC is characterized by the following: The cancer has invaded the blood vessels, has spread to other parts of the body (metastasized), or both. Patients are typically still relatively functional, with an Eastern Cooperative Oncology Group (ECOG) performance status of 1–2.14 From 2007 to 2023, the first-line treatment for advanced HCC evolved from sorafenib, to lenvatinib, and then to the combination of atezolizumab (Tecentriq) and bevacizumab (Avastin).15 Sorafenib was the first drug approved by the FDA for the treatment of advanced HCC in April 2007. It is a type of targeted therapy, known as a multikinase inhibitor, exerting antiproliferative and antiangiogenic effects. The SHARP study, which established selection criteria and stratification factors such as the use of the BCLC staging system, Child-Pugh A grade liver function, and functional status (ECOG 0 or 1), is the benchmark for the clinical trial design of HCC.16 SHARP study constitutes the basis for future Phase III trials of advanced HCC research. In advanced HCC patients, the SHARP trial demonstrated that sorafenib was superior to placebo, representing a breakthrough in the treatment of HCC. In the sorafenib group and the placebo group, the most common drug-related adverse events for all severity levels were diarrhea (39% vs 11%), fatigue (22% vs 16%), hand-foot skin reaction (21% vs 3%), and rash or desquamation (16% vs 11%). From 2007 to 2017, sorafenib was the only standard treatment available for advanced HCC.
Lenvatinib, an oral, multitargeted tyrosine kinase inhibitor that acts by inhibiting tumor angiogenesis and promoting programmed cell death, was approved by the FDA in August 2018 as a first-line treatment for advanced HCC based on the effectiveness demonstrated by a global open label randomized phase III study (REFLECT).17 The REFLECT trial enrolled clinically confirmed unresectable HCC patients. The inclusion criteria were as follows: one or more measurable target lesions according to modified RECIST (mRECIST), BCLC stage B or C, CP-A stage, ECOG-PS score of 0 or 1, and normal liver, kidney, pancreas, bone marrow, and blood function. Exclusion criteria are as follows: patients who have received systemic chemotherapy for advanced/unresectable HCC in the past or have received any anti-cancer or blood-enhancing treatment ≤28 days prior to randomization. Patients with main portal vein invasion, or liver mass ≥50%, or obvious bile duct invasion, were also excluded. The trial showed that the median overall survival (mOS) of the lenvatinib group was 13.6 months (95% CI 12.1–14.9), which was not inferior to that of the sorafenib group at 12.3 months (95% CI 10.4–13.9; hazard ratio 0.92, 95% CI 0.79–1.06), meeting the non-inferiority criteria. However, compared with sorafenib, lenvatinib showed significant improvements in all secondary endpoints (higher objective response rate (ORR) (24.1% vs 9.2%; odds ratio [OR] 3.13; P < 0.001), longer progression-free survival (PFS) (7.4 months vs 3.7 months; hazard ratio [HR] 0.66; P < 0.001) and time to disease progression (TTP) (8.9 months vs 3.7 months; HR .063; P < 0.001)). In addition, the overall tolerability of lenvatinib is manageable with the most common adverse events during treatment being hypertension (42%), diarrhea (39%), decreased appetite (34%), and weight loss (31%). Given the non-inferior efficacy to sorafenib and manageable tolerability profile, lenvatinib, replacing sorafenib, has become a new first-line systemic therapy for advanced HCC patients.
In May 2020, based on the landmark results of the IMbrave150 trial, the combination of atezolizumab and bevacizumab was approved by the US FDA as the standard first-line treatment for advanced HCC. Atezolizumab is an immune checkpoint inhibitor that works by selectively targeting the protein PD-L1 on cancer cells, which blocks its interaction with the receptors PD-1 and B7-1, thereby reversing the inhibition of T cells. Bevacizumab is a monoclonal antibody that targets VEGF, inhibiting angiogenesis and tumor growth. The IMbrave150 study evolved from a Phase 1b study that included 104 patients treated with the combination therapy of atezolizumab plus bevacizumab, which demonstrated an 36% ORR and an expected safety profile.18 The IMbrave 150 trial indicated the supremacy of atezolizumab plus bevacizumab in terms of OS and PFS outcomes than sorafenib, and quality of life measurements favored the combination as well. As far as the toxicity of the combination therapy is concerned, the two groups showed similar rates of all grade 3/4 adverse events. The incidence of grade 3/4 bleeding events was 6.4% with atezolizumab plus bevacizumab vs 5.8% with sorafenib. In addition, 15.2% of patients in the atezolizumab-bevacizumab group experienced grade 3 or 4 hypertension. However, other high-grade toxic effects are rare.15,19
Currently, based on positive Phase III data, three treatment options (regorafenib, cabozantinib, and ramucirumab) and promising Phase Ib/II studies, three additional treatments (nivolumab, pembrolizumab, and nivolumab plus ipilimumab) have been approved by the FDA for the second-line treatment of advanced HCC after progression on sorafenib.20 Regorafenib, an oral multikinase inhibitor that targets VEGFR1–3 and other kinases, was approved for the second-line treatment of patients with advanced HCC who have failed to tolerate or progress after sorafenib treatment. The randomized, double-blind, placebo-controlled phase III clinical trial RESORCE demonstrated significantly better mOS, mPFS and ORR in the regorafenib treatment group than in the placebo group. The most common grade 3–4 events were fatigue (55.3%), hand–foot skin reaction (31.5%), hypertension (15.2%) and diarrhoea (7.8%).21
Cabozantinib, a multi-kinase inhibitor, suppresses tumor growth and metastasis by simultaneously targeting multiple pathways, including VEGFR, MET, and AXL. The CELESTIAL trial demonstrated an improvement in OS (10.2 months versus 8 months in the placebo group; HR 0.76, 95% CI 0.63–0.92; P = 0.0049). PFS was increased with cabozantinib compared with placebo (5.2 months versus 1.9 months; HR 0.44, 95% CI 0.36–0.52; P < 0.001) and ORR was increased from 0.4% in the placebo arm to 3.8% in the cabozantinib arm. The most common adverse reactions in the Cabozantinib group include hand-foot syndrome, hypertension, dry mouth, and fatigue, with hand-foot syndrome being the most common (50% in the Cabozantinib group vs 7% in the placebo group). In the Cabozantinib group, 8% of patients discontinued treatment due to adverse reactions.22
Ramucirumab is currently the only biomarker-guided HCC treatment by targeting the vascular endothelial growth factor receptor-2 (VEGFR-2) in liver cancer cells, inhibiting tumor angiogenesis and growth. The randomized, double-blind, phase III REACH-2 trial, aiming to establish the efficacy of ramucirumab, recruited 542 patients with advanced hepatocellular carcinoma who had previously received sorafenib treatment and had an alpha-fetoprotein concentration of ≥400 ng/mL. The REACH-2 trial demonstrated that the mOS in this subgroup of patients was extended from 7.3 months to 8.5 months, compared to placebo (HR 0.710, 95% CI 0.531–0.949; P = 0.0199). The ramucirumab group had a higher PFS compared with placebo group, while there was no difference in terms of ORR.23 Common grade 3–4 treatment-related adverse events include hypertension, hyponatremia, hepatic and renal function abnormalities, leukopenia, thrombocytopenia, diarrhea, fatigue, and skin reactions. In a meta-analysis of HCC studies including REACH and REACH-2, the ramucirumab group showed improved OS and PFS compared to the placebo group in HCC patients with ascites.24
For patients with HCC who experience disease progression after receiving conventional first-line treatment, especially those with severe liver cirrhosis or cardiovascular diseases and cannot tolerate other TKIs, ICI therapy holds therapeutic potential.5 Surprisingly, in both first-line phase III CheckMate 459 trial (nivolumab vs sorafenib)25 and second-line phase III KEYNOTE-240 trial (pembrolizumab vs placebo),26 monotherapy immune checkpoint inhibitors failed to improve OS despite having a durable response rate of 15% to 20%. The combination therapy of nivolumab (an anti-PD-1 monoclonal antibody) and ipilimumab (an anti-CTLA-4 monoclonal antibody) was the first approved dual immunotherapy regimen for advanced HCC patients after failed first-line treatment. As shown in the CheckMate 040 trial, the combination therapy achieved an ORR of 31%, with a median duration of response of 17 months, and a mOS of 23 months.27 Although the combination therapy of nivolumab plus ipilimumab induced immune-related toxicities requiring systemic corticosteroid administration in 51% of cases, the FDA accelerated the approval of second-line treatment due to the efficacy of the outcomes. Other clinical trials of combination therapy or not for advanced liver cancer without regulatory approval are as follows: ORIENT-32,28 GO30140,18 KEYNOTE-524,29 KEYNOTE-224,30 RESCUE,31 NCT02519348,32 NCT01008358,33 NCT0298992234 (Table 1)
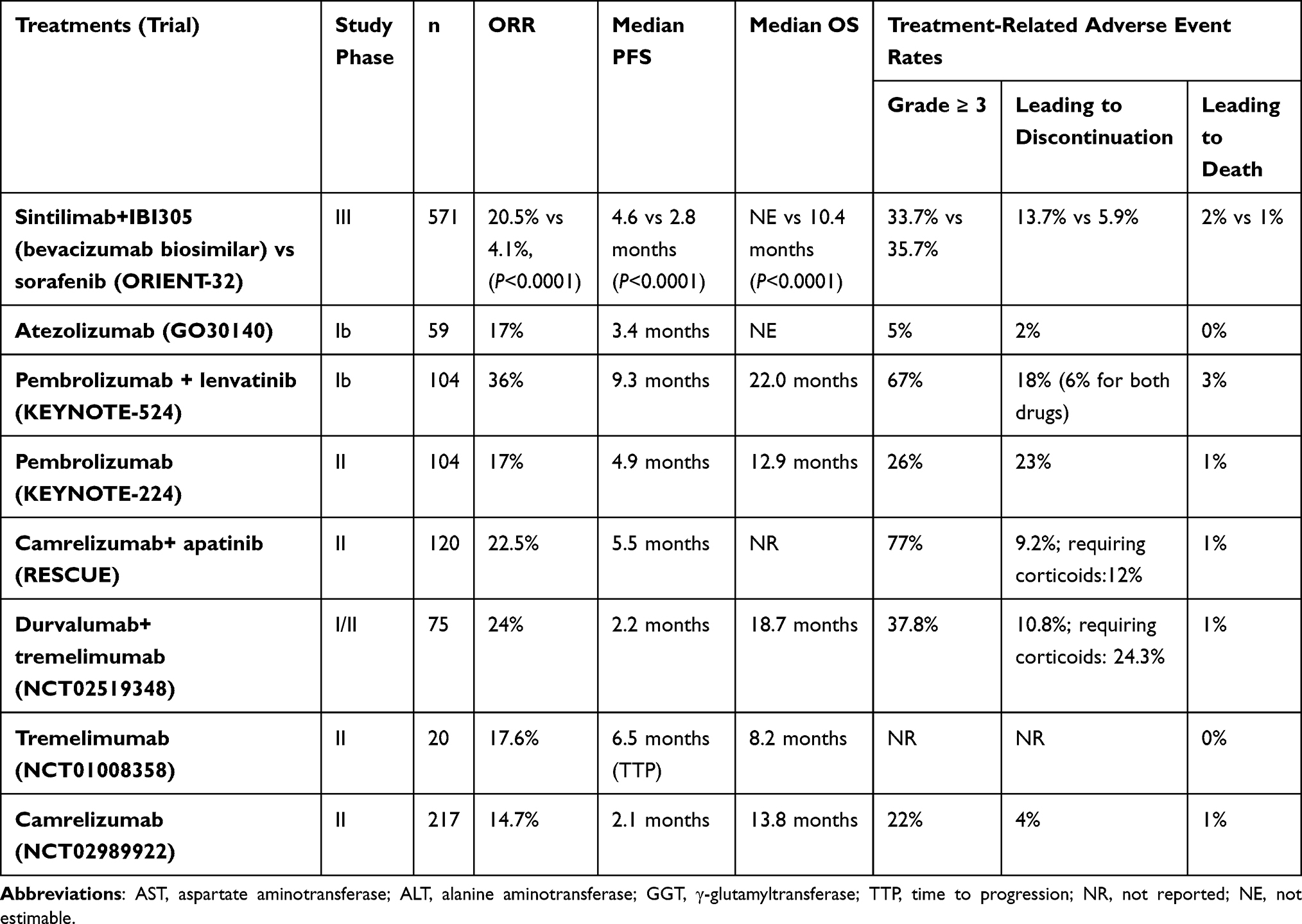 |
Table 1 Clinical Trial Results of Immunotherapies for Advanced-Stage HCC |
Neoadjuvant Treatment for Advanced HCC Patients
Downstaging is defined as reducing the size of a tumor through neoadjuvant therapy to meet the Milan criteria for liver transplantation (a single tumor <5 cm or 2–3 tumors ≤3 cm)35 or the criteria for liver resection. This concept needs to be distinguished from bridging, which refers to the treatment of candidates awaiting liver transplantation or patients who are not eligible for liver resection. To augment the likelihood of successful downstaging, both AASLD and EASL recognize the restriction of initial tumor burden (number and size of lesions) as qualification criteria for downstaging.36,37 Both TACE and TARE have been used in HCC with the aim of downstaging the lesions to improve resectability. In a retrospective study involving over 2,500 patients, effective downstaging of initially beyond Milan criteria HCC patients (n = 465) following locoregional therapy resulted in a mOS of 10 years after liver transplantation.5 A study on downstaging of liver transplant patients beyond the Milan criteria with or without locoregional therapy showed that patients who received locoregional therapy had significantly increased 1-year (95% CI 1.01 to 1.23) and 5-year (95% CI 1.03 to 1.32) survival rates compared to those who did not receive locoregional therapy.38 In a retrospective analysis of 831 patients who underwent TACE treatment, 82 cases were successfully downstaged, and 43 patients underwent surgical resection.39 However, a retrospective, single-center study found that TARE significantly increased the likelihood of successful downstaging compared with conventional TACE (58% and 31%, respectively).40 TARE destroys tumor cells by delivering the radioactive drug directly to the tumor site through the injection of radioactive microspheres (typically erbium-90 or yttrium-90 microspheres) via arterial cannulation of the feeding vessel to the tumor. Neoadjuvant systemic therapy, such as immune checkpoint inhibitors (ICIs), for HCC patients who are on the liver transplant waiting list, is an attractive idea. However, it remains controversial due to the reported risk of rejection and graft loss after transplantation.41 Theoretically, in neoadjuvant therapy, ICIs can utilize the higher levels of tumor antigens present in the primary tumor and promote the expansion of existing tumor-specific T lymphocyte clones in the tumor microenvironment.42 In a phase 1b single-arm study, investigators evaluated the feasibility of cabozantinib and nivolumab as neoadjuvant therapy in patients with hepatocellular carcinoma (HCC), including those who did not meet the traditional resection criteria.43 Among the enrolled 15 patients, 12 (80%) achieved negative surgical margins, with 5 of them (42%) experiencing significant pathological responses. In the neoadjuvant therapy, a shorter duration interval from the initial administration of neoadjuvant immunotherapy to the resection of the primary tumor is necessary to achieve optimal efficacy, while a longer duration interval negates the effectiveness of immunotherapy.44 Neoadjuvant combined (locoregional plus systemic therapy) approaches have been proposed for downstaging treatment in initially unresectable HCC. The results of studies combining TKIs (such as sorafenib or lenvatinib) with locoregional liver-directed therapies (such as TACE, TARE, or radiofrequency ablation) have shown modest outcomes.45–47 However, given the potential synergistic modulation of the tumor immune microenvironment by ICIs and locoregional therapy,48 many research teams have attempted to improve neoadjuvant treatment strategies by combining ICIs with locoregional therapy. There is a record of complete pathological response when using TARE plus nivolumab treatment for initially unresectable HCC lesions.49 Similarly, several case reports have shown that after TACE combined with ICIs treatment, patients exhibited an exceptional response, enabling safe resection of initially unresectable HCC.50,51 The PD-1/PD-L1 immune checkpoint inhibitors can also utilize the changes in the tumor microenvironment induced by RT.52 A pilot study indicated that various combination therapies involving palliative RT, anti-angiogenic TKIs, and PD-1/PD-L1 inhibitors did not demonstrate any unexpected safety signals in the treatment of advanced-stage HCC patients.53 Therefore, neoadjuvant radiotherapy combined with systemic therapy is safe and feasible. A Phase I trial suggests that patients with advanced HCC receiving SBRT plus nivolumab + ipilimumab combination therapy achieved promising outcomes (ORR 57%, median OS 46 months) compared to those receiving nivolumab + ipilimumab monotherapy (Checkmate 040 reported ORR 27–32%).54 Subsequent trials including NCT03482102, a single-arm Phase II trial of durvalumab and tremelimumab with SBRT, and NCT03316872, a single-arm phase II study of pembrolizumab with SBRT will further investigate the potential benefits of SBRT combined with immunotherapy in advanced HCC.
Systemic Therapies for Early and Intermediate-Stage HCC
For patients with very early-stage (BCLC 0) and early-stage (BCLC A) HCC, the current treatment options include surgical resection, radiofrequency ablation (RFA), irreversible electroporation (IRE) and transplantation.4 Surgery is the cornerstone therapy for very early-stage and early-stage HCC. The aim is to achieve negative-margin (R0) resections while preserving the liver to the extent possible, thereby minimizing the risk of postoperative liver failure and death after hepatectomy. The utility of the Child-Pugh score and 15-minute indocyanine green retention rate (ICG R15) to accurately assess liver function before surgery is essential. According to Makuuchi criteria, two-thirds of liver parenchyma can be removed if ICG R15 is less than 10%, and less than one-third could be resected if it is 10%–19%, whereas patients with ICG R15 ≥20% will only tolerate single segmentectomy or less, based on the Child’s A liver function.55 With the advancement of surgical techniques and the innovation of surgical instruments, minimally invasive liver surgery has gradually developed into a safe and effective surgical approach. The advantages of laparoscopic approach include improved visibility due to magnification, reduced fluid requirements, avoidance of long abdominal incisions, fewer surgical manipulations, and decreased respiratory damage. However, complex laparoscopic liver resection requires a longer learning curve than standard resection to be performed proficiently and safely.56,57 A recent meta-analysis, analysing 51 retrospective studies with or without propensity score matching, comparing laparoscopic and open hepatectomy in 6,812 patients with HCC demonstrated a trend towards reduced HCC recurrence rate and improved long-term survival with laparoscopic surgery.58 On a cautionary note, a retrospective registry study involving 1,270 patients found that unplanned conversion from laparoscopic to open hepatectomy for HCC, especially for major hepatectomy, was associated with reduced OS compared to direct open resection.59 The limitations of laparoscopic hepatectomy such as restricted movement of laparoscopic instruments to four degrees of freedom, loss of three-dimensional vision, and magnification of physiological hand tremors caused by elongated instruments pose significant challenges for complex liver resections.60,61 To overcome the limitations of laparoscopic surgery, another minimally invasive hepatectomy, robotic hepatectomy, was developed. The theoretical advantages of robotic technology include improved flexibility, visual, and precision magnification, as well as reduced tremors and fatigue, which may reduce the risk of conversion to open liver resection during complex hepatectomies.62,63 Robotic and laparoscopic hepatectomy have been demonstrated to be safe and effective for patients with BCLC 0-A stage hepatocellular carcinoma (HCC), compared to open hepatectomy. Additionally, these minimally invasive procedures can also lead to a shorter hospital stay. However, there were no significant differences in the 5-year PFS rate and OS rate among the three groups.64 Postoperative recurrence is believed to be due to tumor invasion into the branches of the portal vein, allowing tumor cells to spread and disseminate to other areas of the liver through portal venous flow.65 Given that HCC primarily spreads through the nearest portal vein, the selection of hepatic resection type is of concern. Anatomic hepatectomy (AH) allows for the systematic removal of the portal vein area where the tumor is located, theoretically reducing the risk of tumor recurrence and potentially improving survival rates.66 However, previous studies have yielded conflicting results. Some studies have indicated that AH improves long-term prognosis after surgery compared to non-anatomic hepatectomy (NAH),67–71 while others have not observed any survival benefits.72–75 Surgical margin is an independent risk factor for recurrence after hepatectomy. In view of the above controversy, some scholars believe that AH is unnecessary when a wide (≥ 1cm) tumor-free surgical margin can be obtained.76,77 Interestingly, after evaluating the relationship between AH and marginal status in HBV-associated HCC patients with microvascular invasion, Liu et al indicated that patients in the AH with wide margin (≥1 cm) group had significantly better mOS and disease-free survival compared to the AH with narrow margin (<1cm) group and NAH with wide margin or narrow margin group.69 Therefore, if technically feasible and safe, the combination of AH and wide margin should be considered as a recommended treatment strategy for HCC patients. Surgery as a first-line treatment for early-stage HCC has a 5-year survival rate of about 70%-80%.78 However, the 5-year recurrence rate following surgical resection can be as high as 70%.79 The mOS of ablation is 60 months, with a 5-year recurrence rate including local, distant intrahepatic, and extrahepatic metastases ranging from 50% to 70%.36,37 RFA is another curative treatment option for HCC with a diameter ≤3cm with a relatively good liver functional reserve, according to the guidelines established by the American Association for the Study of the Liver Disease,80 the European Association for the Study of the Liver,81 and Japanese evidence-based guidelines.82,83 When the tumor is located on the surface of the liver, adjacent to other organs that need to be mobilized, or when it cannot be detected by percutaneous ultrasound examination, laparoscopic radiofrequency ablation treatment is recommended.84 The current study showed that laparoscopic radiofrequency ablation resulted in a better long-term outcome in patients with liver damage B or C than endoscopic partial hepatic resection for patients with initial HCC within the Milan criteria (3-year OS: 82% vs 36%, p = 0.003).85 IRE treatment can be considered for patients with liver dysfunction, poor general condition, or tumors in hazardous locations such as biliary structures for thermal ablation therapy because of its less aggressive mechanism of action primarily relying on cell apoptosis rather than necrosis and distortion of connective tissue.86 IRE can provide safe and complete ablation for patients not amenable to thermal ablation therapy. A retrospective clinical study involving 75 cases of HCC with liver cirrhosis demonstrated that after undergoing IRE treatment, the 6-month and 12-month overall local tumor PFS rates were 87% (95% confidence interval [CI]: 77%, 93%) and 70% (95% CI: 56%, 81%), respectively.87
Immune checkpoint inhibitors may be more effective against micro-metastases and residual disease, which is observed in HCC patients with tumor remnants after ablation. In the early stages of HCC, combining systemic treatment with locoregional therapy has the potential to reduce the risk of disease recurrence and prolong survival. In this scenario, however, the STORM Phase 3 trial compared sorafenib with a placebo in 1,114 HCC patients (214 received thermal ablation treatment, 900 received resection treatment), but the data showed no improvement in recurrence-free survival.88 Similarly, other trials have also failed in this setting.89–92 Therefore, systemic treatment after complete ablation has not been recommended to date. Some trials demonstrated that combining other locoregional therapies after ablation has robust superior survival benefits of early-stage HCC patients.93,94 However, these results have not been replicated in phase III studies, and therefore, confirmatory data are needed before these techniques can be adopted in guidelines. The high density of CD3+ and CD8+ T cells in the tumor core and margin, along with the corresponding immune scores (based on the number of CD3+ and CD8+ lymphocytes in the tumor core and margin), is associated with a low recurrence rate after surgical resection of HCC.95 Therefore, there is a reason to integrate immunotherapy into the treatment of early-stage liver cancer in order to increase the chances of cure after HCC surgical treatment. Adoptive cell transfer therapy (ACT) is the most representative cancer immunotherapy method. A phase 3 open-label trial enrolling 230 patients with HCC who underwent surgical resection or ablation showed that the experimental group receiving CIK cell, a mixture of T lymphocytes expanded in vitro with cytokines, had a significantly increased recurrence-free survival compared to the placebo group (44 months vs 30 months HR = 0.63; 95% CI 0.43–0.94; P = 0.010).96 Other clinical trials assessing the suitability of CIK therapy for HCC are summarized in Table 2.97–101 BCLC-B stage patients are defined as intermediate-stage HCC patients. Arterialization is a hallmark of HCC that has been used for the delivery of embolic particles, chemotherapy, and radiation therapy. Two randomized controlled trials (RCTs)102,103 with OS as the primary endpoint and subsequent meta-analysis104 have shown that TACE has demonstrated survival benefits compared to the best supportive care or suboptimal therapies. According to these trial data, guidelines from AASLD, EASL, APASL, and the European Society for Medical Oncology (ESMO) all recommend TACE as the standard treatment for intermediate-stage HCC. In addition, other locoregional therapies for intermediate-stage liver cancer include transarterial embolization, transarterial radioembolization (TARE) and drug-eluting bead transarterial chemoembolization (DEB-TACE). Several phase III trials have indicated that compared to TACE therapy, other locoregional therapies achieve no significant survival benefit105–107 (Table 3). With the emergence of effective systemic therapies, we have witnessed the development of trials combining arterial therapy with systemic treatment or utilizing systemic therapies as a control. The challenges faced in designing such trials are as follows. Firstly, TACE is not a standardized technique, and its indications and outcomes are influenced by various variables, including the type and size of particles, use of iodized oil, chemotherapy, procedure, and degree of selectivity.108 Secondly, there is no consensus on the endpoints yet. Conventional endpoints such as OS, PFS and TTP were used as primary endpoints, but negative outcomes do not adequately define TACE failure. Various new secondary endpoints have been developed, including modifications to PFS, such as time to progression to TACE (including time to progression and death), as well as time to vascular invasion or extrahepatic spread.109 Although there are various methods and endpoints, these trials have not provided convincing evidence of clinical benefit compared to TACE alone45,110–113 (Table 3). Some scholars have proposed specific endpoints, such as time-to-unTACEable progression as evaluation criteria. The criteria are as follows: Patients who cannot undergo further TACE treatment or do not benefit from TACE due to the following reasons: liver tumor progression (increase of more than 25% compared to baseline) according to the “Liver Cancer Efficacy Evaluation Criteria” (RECICL), transient deterioration of liver function to Child-Pugh C grade after TACE, major vessel invasion (MVI), or extrahepatic metastasis.114 A randomized, open-label, multicenter trial named TACTICS found that based on unTACEable progression as co-primary endpoints, the combination therapy of TACE + sorafenib significantly prolonged PFS compared to TACE alone115 (Table 3). This novel TACE-specific endpoint should be examined and validated in future TACE combination trials. Alternative strategies such as TACE combined with immunotherapy are currently under investigation. The prevailing rationale for combining TACE with immunotherapy is strong: locoregional therapy induces immunogenic tumour cell death, resulting in a release of antigens, damage-associated molecular patterns and pro-inflammatory cytokines that facilitate antigen presentation and priming of anti-tumour lymphocytes.116,117 A clinical trial testing the combination of tremelimumab (anti-CTLA4 antibody) with TACE or radiofrequency ablation for HCC showed an ORR of 26.3% and mOS of 19.4 months.118
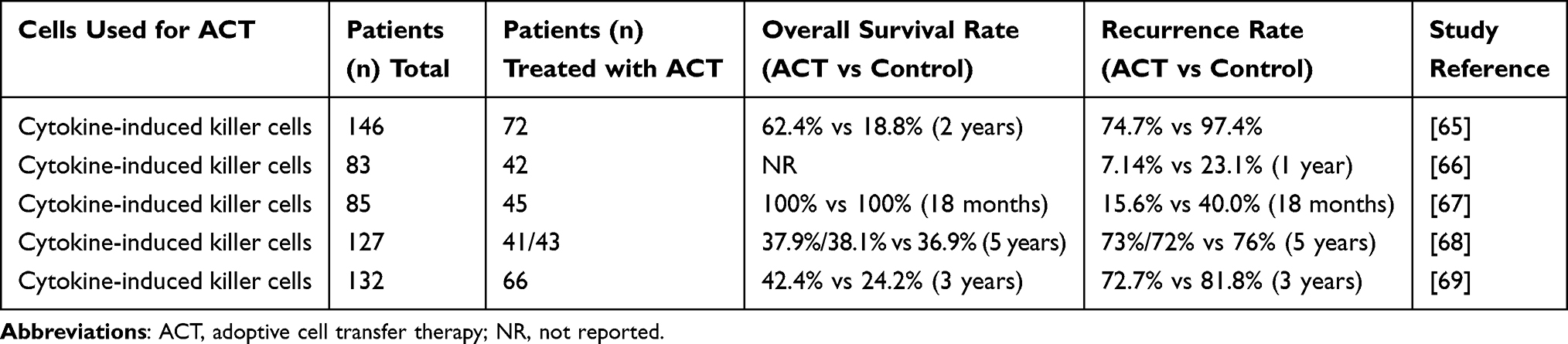 |
Table 2 Summary of Clinical Trials on the Applicability of CIK as HCC Treatment Strategies |
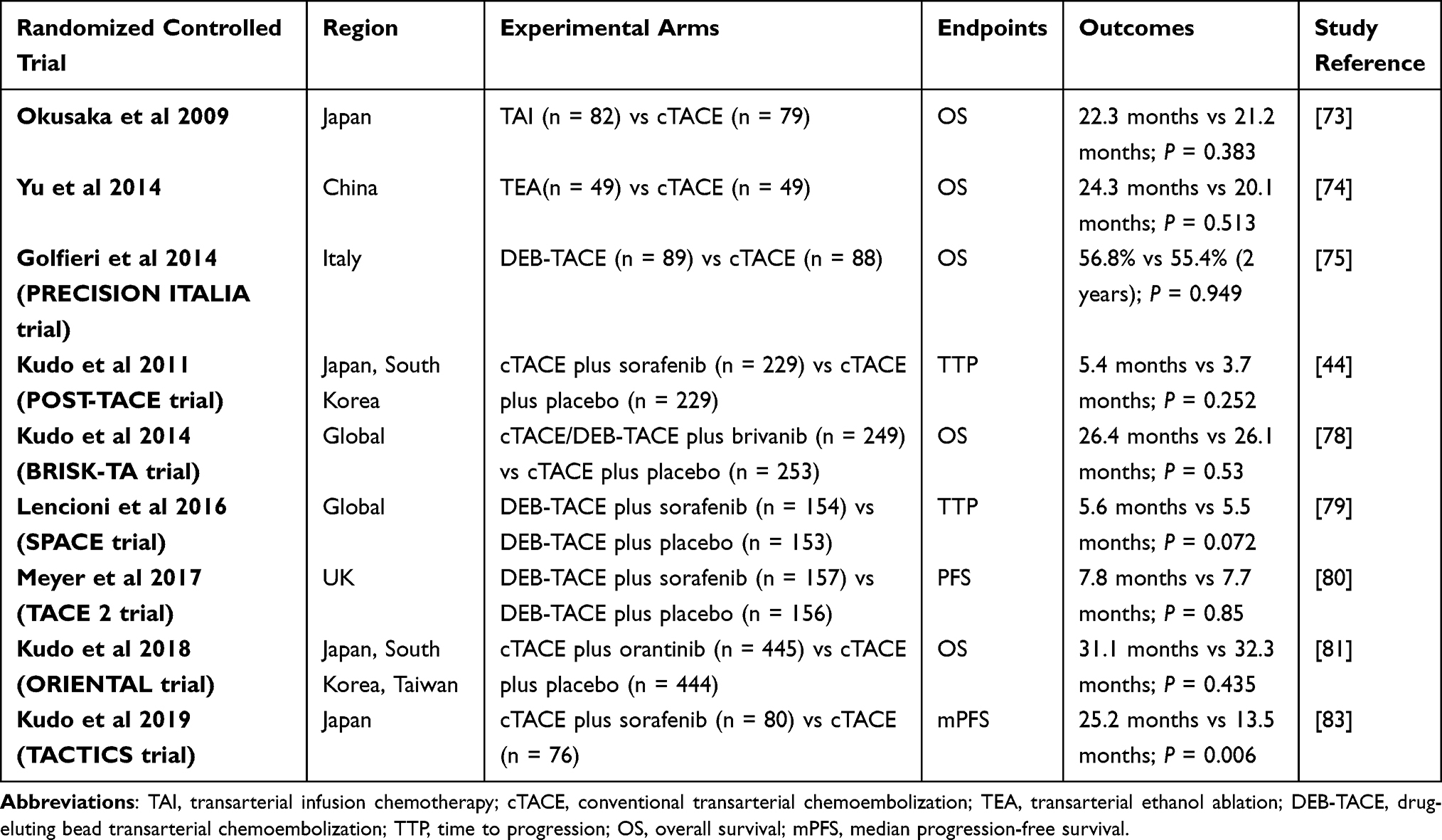 |
Table 3 Outcomes of Randomized Controlled Trial Results for Intra-Arterial Treatment of HCC |
Systemic Treatment Options in Special Populations
Approximately 10%–40% of HCC patients have portal vein tumor thrombosis (PVTT) at the time of diagnosis, leading to the high tumor invasiveness, insufficient hepatic reserve function, and portal hypertension.119,120 PVTT is divided into five grades in the classification system of the Liver Cancer Study Group of Japan121 (Table 4). Based on BCLC staging system, the European36 and American122 as well as the ESMO (European Society for Medical Oncology)123 guidelines for HCC diagnosis and treatment only recommend systemic treatment options such as targeted therapy and even consider PVTT as a contraindication for hepatic resection. However, in recent years, the Asian HCC guidelines have also acknowledged the results from real-world practice, in addition to those from large-scale, multicenter, randomized clinical trials. They also recommend local treatments such as TACE, HAIC, local radiotherapy, and hepatic resection as optional treatment options for patients with PVTT. In 2016, a retrospective study conducted in Japan involving 6474 HCC patients with PVTT revealed that hepatic resection only had advantages in patients with Vp1-3, while there was no significant advantage in patients with Vp4 based on subgroup analysis of PVTT classification.124 A multicenter retrospective study (n = 1580) compared the median survival time of HCC patients with PVTT who underwent hepatic resection, TACE, TACE combined with sorafenib, or radiotherapy.125 Among patients with Vp1-2 PVTT, the hepatic resection group had the best OS. Among patients with Vp3 PVTT, the median survival time was 12.5 months in the hepatic resection group and 10.6 months in the TACE combined with radiotherapy group (p = 0.046). However, among patients with Vp4 PVTT, the median survival time was longer but not statistically significant in the TACE combined with radiotherapy group compared to the hepatic resection group (8.9 months vs 6.0 months, p = 0.401). Until now, there have been no clinical trials or cohort studies investigating the systemic treatment of different types of PVTT. Kaneko et al reported a median survival of only 5.5 months in Vp3/4 PVTT patients treated with sorafenib and lenvatinib.126 Luo et al proposed that linear iodine-125 (125I) seed strand combined with portal vein stent (PVS) implantation plus TACE was a safe and effective palliative treatment option for patients with HCC and Vp4 PVTT.127 Huang et al conducted a real-world study to analyze the use of lenvatinib plus anti-PD-1 antibody as a first-line treatment in HCC patients with major vessel tumor thrombosis (MVTT).128 The tumor response of this combination therapy in MVTT (MVTT ORR: 54.5%) was superior to intrahepatic tumors (32.8%) and lung metastases (37.5%). According to these results, the interventional therapy combined with systemic therapy might be an effective therapy for advanced HCC and PVTT. Zhang et al conducted a single-center retrospective study to evaluate the safety and efficacy of combined interventional therapy (125I seed chain + PVS implantation + TACE) with systemic treatment (lenvatinib + anti-PD-1 antibody) as a first-line treatment for HCC patients with Vp4 PVTT.129 As a result, patients in group A (125I seed chain + PVS implantation + TACE+ lenvatinib + anti-PD-1 antibody) had significantly better intrahepatic tumor control (55.3% vs 17.5%, P < 0.001) and longer OS and PFS than group B (125I seed chain + PVS implantation + TACE+ lenvatinib) (OS, 17.7 ± 1.7 vs 12.0 ± 0.8 months, P = 0.010; PFS, 17.0 ± 4.3 vs 8.0 ± 0.7 months, P < 0.001). In addition, two patients underwent liver transplantation, and one patient underwent surgical resection, suggesting that this combination therapy may provide an opportunity for surgical treatment in patients with unresectable HCC and Vp4 PVTT. In conclusion, the combined treatment approach of interventional therapy and systemic therapy can be considered as a first-line treatment option for patients with unresectable HCC and Vp4 PVTT.
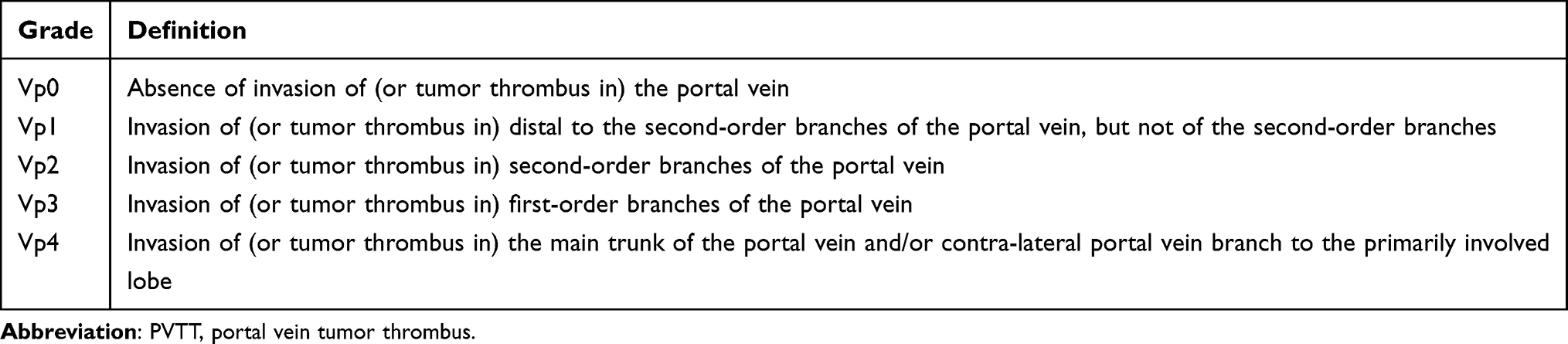 |
Table 4 PVTT Classification System of Japanese Liver Cancer Study Group |
Child Pugh class B(CP B) patients with advanced HCC are a wide heterogenous group with borderline liver function and high risk of post-treatment hepatic deterioration. The treatment decision should weigh the survival benefits provided by existing therapeutic agents against the risk of further liver damage, especially when the balance is already very fragile. Sorafenib is the only multi-kinase inhibitor approved for administration in CP B class patients. Previous studies have indicated that CP B advanced HCC patients may respond to and tolerate sorafenib treatment without extending OS as they often experience disease deterioration of liver, leading to treatment discontinuation and reduced life expectancy.130,131 Lenvatinib, similar to sorafenib, may be effective in treating HCC in CP B patients, but higher rates of discontinuation or withdrawal, treatment-related adverse events, and liver-related deaths, limiting its impact on OS.132,133 Additionally, compared to sorafenib, lenvatinib has no significant OS advantage in patients with decompensated liver cirrhosis (CP B and C).134 The impact of cabozantinib on the survival of advanced HCC patients appears to be significantly dependent on the severity of liver function impairment, with more favorable outcomes observed in patients with lower CP B scores. A recent international real-life study included 60, 22, and 1 cases of CP A, B, and C grade patients, respectively. The results showed that the AE rate was 73% in the CP B group, while it was 43% in the CP A group (P = 0.017). The mOS in the CP B7 group was 7 months, while it was 9.7 months in the CP A group. In comparison, the mOS for CP B8, B9, and C was restricted to 3.4 months.135 In recent years, immune checkpoint inhibitors have completely changed the treatment landscape for HCC. Based on previous research findings, immunotherapy may be a relatively safe option for patients with impaired liver function. In the CheckMate-040 trial, 49 patients with CP B HCC were intravenously administered nivolumab, with a reported ORR of 12% and disease control rate (DCR) of 55%. It is worth mentioning that the safety profile of nivolumab in this population is comparable to that of CP A patients.136 A recent real-world study recruited 431 CP B patients to compare the efficacy and safety of sorafenib and nivolumab. The results showed that the median survival period for the 79 patients who received nivolumab was 5 months, while it was 4 months for the group receiving sorafenib. Among the patients receiving nivolumab, 12% discontinued treatment due to toxicity, while among those receiving sorafenib, 36% (P = 0.001) discontinued treatment due to toxicity.137 A possible reason is that the metabolism of ICIs does not depend on liver function. However, similar to MKIs, the ORR of B CP patients receiving nivolumab treatment was significantly lower than that of CP A patients, and the OS of CP B8 or B9 patients was particularly poor compared to CP B7 patients.138 Atezolizumab-bevacizumab is a first-line treatment with high efficacy in unresectable HCC based on the IMbrave 150 study results. A recent multi-center retrospective study demonstrated that the ORR, and DCR were similar, with no significant differences observed across CP classes.139 However, OS for CP A patients was 16.8 months (95% CI, 14.1–23.9), while for CP B patients, it was 6.7 months (95% CI, 4.3–15.6) (P = 0.0003). This difference is attributed to potential liver damage leading to mortality. Apart from the CP score, the ALBI score is also significantly correlated with OS. Based on this finding, close monitoring should be mandatory, especially when combined with anti-VEGF drugs. The ICIs used in combination with anti-VEGF agents appear to provide a survival benefit, although it may not be as high as that seen in CP A patients, while in carefully selected CP B patients, they still have the potential to extend life expectancy.
Biomarkers Predict the Efficacy of Systemic Therapy
Biomarkers have emerged as powerful tools for diagnosis, prognosis, and predicting treatment response, enabling the maximization of clinical benefits through patient stratification. Currently, systemic therapies typically exhibit high heterogeneity in their efficacy among advanced HCC patients, and therefore, the identification of biomarkers for predicting treatment response and patient selection has become an urgent need. For response to sorafenib, patients with the mutation of the PI3K–AKT–mTOR pathway tended to have a lower ORR and a shorter mOS and PFS.140 In addition, VEGFA amplification and acyl-CoA synthetase long-chain family member 4 (ACSL4) expression in HCC tissue are associated with better responses to subsequent sorafenib treatment.141,142 For lenvatinib, FGF19, ST6GAL1, VEGF, FGF21, and ANG2 may be novel biomarkers that identify lenvatinib-susceptible HCC.143,144 In addition, for second-line therapy, ramucirumab is currently the only alpha-fetoprotein concentration-guided TKIs, as described above. Based on the correlation between clinical samples and potential predictive biomarkers, pre-existing larger infiltration of tumor-infiltrating lymphocytes (TIL) and inflammatory gene signatures of tumor microenvironment (TME) have shown better treatment response to ICI-based therapies. Patients with higher baseline levels of CD8+ TILs show improved prognosis after receiving nivolumab treatment. Additionally, baseline TME inflammatory gene characteristics, including CD8A, CD274, STAT1 and LAG3 genes, are associated with better clinical outcomes in patients treated with nivolumab.145 The GO30140 and IMbrave150 trials conducted comprehensive correlative analyses of tumor samples from 358 patients receiving atezolizumab and bevacizumab, atezolizumab alone, or sorafenib treatment. In GO30140 cohort, better response was associated with higher baseline TIL density and which demonstrated improved survival outcomes in IMbrave150 cohort. In patients treated with the combination of atezolizumab and bevacizumab, pre-existing inflammatory gene signatures were associated with better clinical outcomes. A lower proportion of Treg/Teff gene signature was also linked to improved PFS and OS in patients treated with atezolizumab and bevacizumab together in IMbrave150 cohort. Additionally, patients with mutations in the telomerase reverse transcriptase promoter region in HCC tumors received atezolizumab and bevacizumab had longer PFS and OS compared to those treated with sorafenib alone. Furthermore, low expression levels of AFP and GPC3 in the pre-treatment tumor samples were associated with longer PFS in the atezolizumab and bevacizumab group.146
Combination of Systemic Therapy and Surgery for BTC
Adjuvant Therapy
Biliary tract cancers (BTCs) comprise intrahepatic cholangiocarcinoma (iCCA), extrahepatic cholangiocarcinoma (eCCA) and gallbladder carcinoma (GBC) originating in the epithelium of the biliary tract. Surgical treatment is considered curative for early-stage BTC, but only a small portion of cases (approximately 30%) are feasible.147,148 The feasibility of surgical treatment for iCCA depends on the absence of intrahepatic and distant metastasis, no major vascular invasion, and sufficient future liver remnant (FLR). Margin status and nodal metastasis are associated with survival in patients who undergo resection for iCCA. The median survival is correlated with the width of the surgical margin (≤1mm, 15 months; 2–4mm, 36 months; 5–9mm, 57 months; ≥10mm, 64 months; p < 0.001), and it has been demonstrated that a margin >5mm is an independent predictor of survival (OR, 2.22; 95% CI, 1.59–3.09). However, in patients with lymph node-positive disease, survival after R0 and R1 resection is similar (median, 18 months and 13 months, respectively; p = 0.1).149 Conventional lymph node dissection helps with tumor staging, but its role in improving prognosis is controversial.150 However, multicenter data showed an improved survival with the retrieval of three lymph nodes or higher when compared with patients with one or two nodes removed.151 The AJCC recommends a lymphadenectomy consisting of all fibroadipose and lymphatic tissue within the hepatoduodenal ligament between the hilar plate and the head of the pancreas, inclusive of a minimum of six nodes to ensure accurate staging and prognostication.152 There is currently controversy regarding whether to perform major hepatectomy for type I and type II perihilar cholangiocarcinoma (pCCA). Previous study showed that compared to patients who undergo isolated bile duct resection, adding major hepatectomy does not improve prognosis,153 while other studies have concluded otherwise.154,155 Further prospective studies are needed to evaluate the impact of hepatectomy on type I and type II pCCA. Concomitant caudate resection is often required, especially when studies have demonstrated that caudate lobectomy reduces the possibility of margin-positive and thus decreasing local recurrence.57 Liver transplantation, only approved for certain unresectable pCCA (≤3cm, without lymph node involvement and intrahepatic or extrahepatic metastatic disease) showed better survival rate than resection (3-year: 54% vs 44%; 5-year: 54% vs 29%).156 Distal cholangiocarcinoma (dCCA) may infiltrate the pancreatic head and induce connective tissue hyperplasia. Over the last decade, minimally invasive pancreatoduodenectomy (MIPD), such as laparoscopic pancreatoduodenectomy (LPD) and robotic pancreatoduodenectomy (RPD), has been widely implemented, in a shift away from traditional open pancreatoduodenectomy (OPD). The mOS (30 vs 25 months) and DFS (29 vs 18 months) have no significant difference between MIPD and OPD, as the key to R0 resection was detailed medial perivascular dissection of the superior mesenteric artery (SMA) and perivenous tissue, as well as lymph node dissection.157 The 5-year OS rates for patients who underwent R0 and R1/R2 resections were 60% and 8%, and for lymph node negative and positive patients were 58% and 21%, respectively.158 The criteria for GBC resection include diseases localized to the gallbladder and/or adjacent liver (T1-3), with or without lymph nodes involvement in the hepatoduodenal ligament region (N1-2).159 GBC is often found incidentally after cholecystectomy and should be re-resected if there is no contraindication. The scope of operation includes hepatic segments IVb and V or non-anatomical 2–3 cm wedge and portal lymphadenectomy, while patients at T1a stage are treated with cholecystectomy only.160 With the exception of T1b stage GBC, re-resection significantly improved mOS, with T2 stage from 12.4 to 44.1 months and T3 stage from 9.7 to 23.0 months.161
Adjuvant therapy has been proposed in order to reduce the high incidence of local and distant recurrence in resected BTC patients. The results of three prospective randomized clinical trials (RCTs) investigating the application of experimental adjuvant chemotherapy drugs in resected BTC patients have been published. The BCAT trial in Japan did not achieve its primary endpoint, as there was no significant difference in mOS and RFS between gemcitabine and observation group.162 The PRODIGE-12/ACCORD-18 study in France also failed to demonstrate any benefit of the combination of gemcitabine and oxaliplatin (GEM/OX) as adjuvant therapy compared to observation alone in terms of RFS in patients with CCA and GBC after surgery.163 On the other hand, the BILCAP study164 conducted in the United Kingdom involving patients with CCA and GBC showed clinical benefits of adjuvant capecitabine over observation in terms of mOS (53 months vs 36 months, HR 0.75, 95% CI 0.58–0.97; P = 0.028) in the pre-specified intention-to-treat population (ITT) sensitivity analysis adjusted for prognostic factors such as lymph node status, disease grade, and gender. However, in the ITT analysis, the median RFS with capecitabine (24.4 months, 95% CI 18.6–35.9) was longer compared to the observation group (17.5 months, 95% CI 12.0–23.8) but no difference in the risk of recurrence was demonstrated beyond 24 months. In addition to the differences in BTC subtypes, heterogeneity in risk factors such as lymph node involvement and margin resection among the populations involved in these three adjuvant trials. Furthermore, differences in sample size calculations, statistical power of study design, data maturity, and follow-up time also contribute to the inconsistency in the effectiveness of adjuvant chemotherapy among the three RCT trials.
Neoadjuvant Therapy
Current guidelines recommend surgical resection for TNM 1 and TNM 2, but no recommendations have been given for neoadjuvant therapy except for hCCA that meet the criteria for liver transplantation.165,166 For those with locally advanced disease that is borderline resectable, neoadjuvant therapy provides an opportunity to reduce the tumor size and allow for surgical resection. Similar to HCC, BTC is recommended to assess tumor sensitivity prior to neoadjuvant therapy for optimal therapeutic effect.167 With the development of the Mayo protocol, initial success regarding favorable long-term survival has been achieved in neoadjuvant chemoradiotherapy followed by liver transplant.168,169 Some analyses suggest that patients with locally advanced iCCA who undergo surgery after neoadjuvant chemotherapy have similar short-term and long-term prognosis compared to patients with initially resectable ICC who undergo surgery alone. They may even have a survival advantage compared to patients who receive adjuvant chemotherapy after initial surgery, although no statistical difference is reached.170,171 In addition, analysis specifically focusing on patients with advanced stages (II–III) shows a statistically significant correlation between the utilization of neoadjuvant chemotherapy and improvement in OS.172 Neoadjuvant therapy is not a standard approach in resectable BTCs. Some article showed that 1 cm clear margin is a key factor influencing long-term survival in early-stage BTC. The receipt of either neoadjuvant chemotherapy or adjuvant chemotherapy was not associated with improved OS in resectable BTC and does not support the routine administration of preoperative therapy.173,174 However, a large national database study indicated that neoadjuvant chemotherapy was associated with longer survival in a selected group of patients with BTC compared to those who underwent upfront surgical resection followed by adjuvant chemotherapy.175 There are several theoretical possibilities regarding how neoadjuvant chemotherapy may improve OS compared to adjuvant chemotherapy. One theory is that neoadjuvant chemotherapy provides additional time to identify patients with chemotherapy-resistant micrometastatic disease, who are more likely to progress to overt metastasis regardless of surgical intervention. The observed benefits of neoadjuvant chemotherapy in early-stage cholangiocarcinoma may be due to effective management of micrometastatic disease rather than tumor downstaging. The use of neoadjuvant therapy is based on retrospective studies; therefore, there is no standardized treatment regimen. A total of 133 patients with iCCA received unspecified regimes, Gemcitabine-based regimes in 100 and other regimes including oxaliplatin, cisplatin, irinotecan, tegafur, uracil and Taxotere in 39.170–172,174,176–178 202 patients with hCCA were managed with the Mayo protocol or a similar variant. A total of 179 patients received 5-FU as part of the Mayo protocol. Other patients who did not undergo the Mayo protocol received gemcitabine, 5FU and leucovorin, gemcitabine and cisplatin or tegafur and uracil.179–181 11 dCCA patients underwent neoadjuvant therapy, with 9 received gemcitabine-based regimes, 2 receiving 5-FU-based regimes.173
Immunotherapy in Advanced Biliary Tract Cancers
Based on the results of Advanced Biliary Tract Cancer (ABC-02) Phase 3 and the Japanese BT22 Phase 2 trials, the combination of gemcitabine (Gem) and cisplatin (Cis) is currently the standard first-line treatment for patients with advanced BTC.182,183 Compared with chemotherapy, the effect of immunotherapy is more dependent on the molecular characteristics of BTC. The immune system, regulated by a complex immune checkpoint protein system, has the ability to recognize and destroy abnormal cells. The current ICIs can be broadly divided into three categories: (i) Programmed Cell Death Protein 1 (PD-1) inhibitors such as pembrolizumab and nivolumab; (ii) Programmed Cell Death Ligand 1 (PD-L1) inhibitors such as atezolizumab, avelumab, and durvalumab; (iii) Cytotoxic T-Lymphocyte Antigen 4 (CTLA4) inhibitors such as ipilimumab and tremelimumab. Pembrolizumab is recommended for first-line treatment of patients with mismatch repair deficiency (d-MMR) or high microsatellite instability (MSI-H) and high tumor mutational burden (TMB > 10) in BTC. KEYNOTE-158 Phase 2 clinical trial, as one of the largest published immunotherapy studies, assessed the efficacy of pembrolizumab in patients with MSI-H/dMMR refractory non-colorectal advanced tumors, including BTC. The subgroup analysis of 22 patients with BTC treated with pembrolizumab revealed an ORR of 40.9% (2-CR and 7-PR) with a median PFS of 4.2 months and a mOS of 24.3 months, regardless of PD-L1 positivity.184 Nivolumab has a category 2B recommendation for second-line treatment (according to the National Comprehensive Cancer Network or NCCN guidelines) and is typically offered to patients without targetable mutations and who may be intolerant to chemotherapy.185 The single-group, multi-center nivolumab-related Phase-II study with 46 patients indicated that ORR was 22% (11/46, 0-CR, 10-PR, and 1 unconfirmed PR) with a disease control rate of 59% (27 of 46). In the intent-to-treat population, mPFS was 3.68 months (95% CI, 2.30–5.69 months), and mOS was 14.24 months (95% CI, 5.98 months to not reached). In order to enhance the efficacy of immunotherapy for BTC, different treatment combinations are currently being tested. One approach involves combining immunotherapy with chemotherapy. Early clinical data of nivolumab in combination with the standard-of-care chemotherapy, Gem and Cis as a first-line treatment showed signs of anti-tumor activity with an ORR of 37%, a mPFS of 4.2 months and mOS of 15.4 months.186 In addition, in an open-label, single-arm, phase II trial, patients with unresectable or metastatic BTC also received nivolumab plus GemCis. The ORR was 55.6%, with mPFS and mOS 6.1 and 8.5 months, respectively.187 The recently published phase III study TOPAZ-1 evaluates the addition of durvalumab, a PD-L1 inhibitor, to GemCis providing the encouraging result. The trial involved 685 previously untreated, unresectable recurrent/metastatic BTC patients and achieved the primary endpoint of the expected OS. The estimated OS was 12.8 months in the durvalumab combined with GemCis group, which was superior to the GemCis group (11.5 months; HR: 0.80). Furthermore, an improvement in mPFS was observed with the combination treatment of durvalumab and GemCis (7.2 vs 5.7 months), while the overall toxicity between the treatment groups was similar. The ORR was also favorable in the durvalumab group (26.7% vs 18.7%).188 A randomized, double-blind, placebo-controlled Phase 3 trial, KEYNOTE-966, confirmed the efficacy and safety of pembrolizumab in combination with GemCis therapy. The mOS in the pembrolizumab group was 12.7 months (95% CI 11.5–13.6), while in the placebo group, it was 10.9 months (95% CI 9.9–11.6) (HR 0.83 [95% CI 0.72–0.95]; one-sided P = 0.0034) with similar treatment-related adverse events.189 A single-arm phase II study was conducted, enrolling 50 patients with advanced biliary tract cancer (BTC), to explore the safety and efficacy of the combination of toripalimab, a PD-1 inhibitor, with gemcitabine and S-1 as first-line treatment for advanced BTC. After a median follow-up time of 24.0 months (IQR: 4.3–31.0 months), the mPFS was 7.0 months (95% CI: 5.0–8.9 months); mOS was 15.0 months (95% CI: 11.6–18.4 months). An ORR of 30.6% (95% CI: 17.2%–44.0%) and a DCR of 87.8% (95% CI: 78.2%–97.3%) were achieved.190 The most common grade 3 or worse treatment-related adverse events (TRAEs) were leukopenia (38%) and neutropenia (32%), which have similar incidence rates as observed in previous studies with gemcitabine. Clinically, pembrolizumab in combination with TKI such as lenvatinib resulted in promising antitumor activity in patients with refractory BTC.191 On this basis, a single-arm, open-label, phase II study was conducted to investigate lenvatinib plus PD-1 inhibitors (pembrolizumab, tislelizumab, sintilimab, camrelizumab or toripalimab) as a first-line treatment for initially unresectable BTC. Among 38 enrolled patients, the ORR was 42.1% and the DCR was 76.3% with 8.0 months (95% CI: 4.6–11.4) of mPFS and 17.7 months (95% CI: not estimable) of mOS.192 Atezolizumab is a humanized immunoglobulin G1 (IgG1) monoclonal antibody that can bind to PD-L1 and block its interaction with PD-1 and B7.1 receptor. Preclinical and early clinical data suggest that MEK inhibition (MEKi) can enhance tumor infiltration of T-cells, expression of MHC-I and PD-L1, modulate the tumor microenvironment to enhance host anti-tumor immune response, and augment response to PD-1 blockade.193–196 Based on this theory, the National Cancer Institute (NCI) Experimental Therapeutics Clinical Trials Network (ETCTN) conducted a randomized phase II study in which atezolizumab alone or in combination with cobimetinib (a MEK inhibitor) was investigated. The study included 86 patients with advanced, pre-treated biliary tract cancer (BTC). Although the combination therapy group had a higher PFS (3.65 months vs 1.87 months; P = 0.027), the OS and ORR were similar between the two groups.197 The astonishing therapeutic effect of the combination of atezolizumab and bevacizumab has made it a first-line treatment for advanced HCC. Considering the crucial role of vascular endothelial growth factor (VEGF) in regulating the immune suppressive mechanisms within the tumor microenvironment of BTC, as well as the enhanced effect of cytotoxic chemotherapy on tumor immunity, the combination of atezolizumab and bevacizumab may improve the efficacy of first-line GEMOX chemotherapy in advanced BTC. A multicenter, single-arm, retrospective study of 30 patients with advanced BTC treated with the triple combination of atezolizumab, bevacizumab, and GEMOX revealed an ORR of 76.7% and a DCR of 90.0% with a mPFS of 12 months and the mOS was not reached.198 Only 10.0% of patients experienced grade 3 or higher TRAEs, which is significantly better than the trial (70%) combining camrelizumab and GEMOX in advanced BTC, indicating that the triple therapy may have a safety advantage over other treatment strategies with similar mechanisms of action.199 Additionally, multiple ongoing first-line trials are studying other ICI monotherapy combined with chemotherapy. A novel anti-PD-L1 antibody, envafolimab (KN035), is being investigated in a randomized phase III trial (NCT03478488) that compares gemcitabine/cisplatin with or without envafolimab. Ongoing phase II trials include NCT04172402 (nivolumab plus gemcitabine and S-1), NCT04191343 (toripalimab plus gemcitabine/oxaliplatin), and NCT03796429 (toripalimab plus gemcitabine and S-1).
Conclusions
In recent decades, there have been significant advancements in the systemic treatment of advanced HCC. First-line therapies have been approved, starting from sorafenib to lenvatinib, and subsequently with the combination of atezolizumab and bevacizumab. However, as it has been proven that ICIs as monotherapy (pembrolizumab and nivolumab) cannot improve OS in HCC patients who have failed first-line treatment, the combination immunotherapy regimen of nivolumab and ipilimumab has been approved as a new second-line treatment. Surgery, ablation, or liver transplantation are the preferred treatment options for patients with very early and early-stage HCC. Adjuvant therapy after surgery, such as systemic treatment combined with local therapy, can improve patient survival. Surgery, ablation, or liver transplantation are the preferred treatment options for patients with very early and early-stage HCC. Adjuvant therapy after surgery, such as systemic treatment combined with locoregional therapy, can improve patient survival. TACE is the standard treatment for intermediate-stage HCC. With the emergence of effective systemic treatment methods and the induction of immunogenic tumor cell death through local therapy, which leads to the release of antigens, damage-associated molecular patterns, and pro-inflammatory cytokines, promoting antigen presentation and activation of anti-tumor lymphocytes, trials combining arterial therapy with systemic treatment are continuously being conducted. TACE and TARE are both used for advanced or beyond Milan criteria HCC, with the aim of downstaging the lesions to achieve surgical resection or liver transplantation. The use of novel systemic therapies, such as ICIs, as neoadjuvant treatments for liver transplantation, remains controversial due to reported risks of rejection and graft loss. However, neoadjuvant combination therapies (such as TACE or RT combined with immunotherapy) have been utilized to downstage initially unresectable HCC and have been proven to be safe and effective. The use of novel systemic treatment regimens for specific populations, such as patients with unresectable HCC Vp4 PVTT, can be complex. Research has shown that combination therapies involving TACE with implantation of linear iodine-125 seed chain in the portal vein stent, as well as lenvatinib combined with anti-PD-1 antibodies, can prolong patient survival and even potentially provide an opportunity for surgical treatment. Immunotherapy may be a relatively safe option for patients with Child-Pugh B liver function, as the metabolism of ICIs is not dependent on liver function. However, close monitoring of liver function is still necessary, especially when used in combination with anti-VEGF drugs. To maximize clinical benefits for patients, it is recommended to identify biomarkers before systemic treatment to predict treatment response and guide drug selection. Biliary tract cancers are characterized by clinical and pathological heterogeneity, with poor response to chemotherapy and dismal prognosis. Only the BILCAP study has shown that adjuvant treatment with capecitabine is beneficial for mOS in patients after resection of cholangiocarcinoma and gallbladder cancer compared to the placebo group. Neoadjuvant therapy is not a standard approach in resectable BTCs. Currently, guidelines recommend surgical resection for TNM1 and TNM2 stages. However, apart from perihilar cholangiocarcinoma that meets the criteria for liver transplantation, there are no recommendations for neoadjuvant therapy yet. For those patients with locally advanced tumors that are resectable, neoadjuvant therapy offers the opportunity to shrink the tumor size and allow for surgical removal. Patients who receive neoadjuvant therapy and undergo successful surgery have similar survival outcomes as patients who are initially eligible for surgery. Due to the fact that current research on neoadjuvant therapy is based on retrospective studies, there is no standardized treatment regimen. The combination of gemcitabine and cisplatin is currently the standard first-line treatment for patients with advanced BTC. In order to improve the efficacy of treatment for advanced stage BTC, immune-based combination therapies are being continuously explored. The combination of immunotherapy with first-line GEMOX chemotherapy has achieved remarkable efficacy in the treatment of advanced BTC. The triple therapy of atezolizumab and bevacizumab as first-line treatment for advanced HCC with GEMOX chemotherapy has been shown to have more safety advantages compared with other therapeutic strategies with similar mechanisms of action. Multiple trials involving the efficacy of triple therapy and other ICIs in combination with chemotherapy for advanced BTC are currently ongoing. Although the treatment options available for BTC patients are still limited, the rapid growth of information in this field supports a more optimistic outlook in the near future.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Koulouris A, Tsagkaris C, Spyrou V, Pappa E, Troullinou A, Nikolaou M. Hepatocellular Carcinoma: an Overview of the Changing Landscape of Treatment Options. J Hepatocell Carcinoma. 2021;8:387–401. doi:10.2147/JHC.S300182
2. Akinyemiju T, Abera S, Ahmed M, et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: results From the Global Burden of Disease Study. JAMA Oncol. 2017;3(12):1683–1691. doi:10.1001/jamaoncol.2017.3055
3. Kanwal F, Kramer J, Asch SM, Chayanupatkul M, Cao Y, El-Serag HB. Risk of Hepatocellular Cancer in HCV Patients Treated With Direct-Acting Antiviral Agents. Gastroenterology. 2017;153(4):996–1005.e1001. doi:10.1053/j.gastro.2017.06.012
4. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nature Reviews Disease Primers. 2021;7(1):6. doi:10.1038/s41572-020-00240-3
5. Llovet JM, Castet F, Heikenwalder M, et al. Immunotherapies for hepatocellular carcinoma. Nat Rev Clin Oncol. 2022;19(3):151–172. doi:10.1038/s41571-021-00573-2
6. Eaton JE, Talwalkar JA, Lazaridis KN, Gores GJ, Lindor KD. Pathogenesis of primary sclerosing cholangitis and advances in diagnosis and management. Gastroenterology. 2013;145(3):521–536. doi:10.1053/j.gastro.2013.06.052
7. Dragani TA. Risk of HCC: genetic heterogeneity and complex genetics. J Hepatol. 2010;52(2):252–257. doi:10.1016/j.jhep.2009.11.015
8. Kim D, Konyn P, Cholankeril G, Bonham CA, Ahmed A. Trends in the Mortality of Biliary Tract Cancers Based on Their Anatomical Site in the United States From 2009 to 2018. Am J Gastroenterol. 2021;116(5):1053–1062. doi:10.14309/ajg.0000000000001151
9. Hsing AW, Bai Y, Andreotti G, et al. Family history of gallstones and the risk of biliary tract cancer and gallstones: a population-based study in Shanghai, China. Int j Cancer. 2007;121(4):832–838. doi:10.1002/ijc.22756
10. Tyson GL, El-Serag HB. Risk factors for cholangiocarcinoma. Hepatology. 2011;54(1):173–184. doi:10.1002/hep.24351
11. Chapman MH, Webster GJ, Bannoo S, Johnson GJ, Wittmann J, Pereira SP. Cholangiocarcinoma and dominant strictures in patients with primary sclerosing cholangitis: a 25-year single-centre experience. Eur J Gastroenterol Hepatol. 2012;24(9):1051–1058. doi:10.1097/MEG.0b013e3283554bbf
12. Ulrich F, Pratschke J, Pascher A, et al. Long-term outcome of liver resection and transplantation for Caroli disease and syndrome. Ann Surg. 2008;247(2):357–364. doi:10.1097/SLA.0b013e31815cca88
13. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
14. Bruix J, Chan SL, Galle PR, Rimassa L, Sangro B. Systemic treatment of hepatocellular carcinoma: an EASL position paper. J Hepatol. 2021;75(4):960–974. doi:10.1016/j.jhep.2021.07.004
15. Yang C, Zhang H, Zhang L, et al. Evolving therapeutic landscape of advanced hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2023;20:203–222.
16. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. New Engl J Med. 2008;359(4):378–390. doi:10.1056/NEJMoa0708857
17. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
18. Lee MS, Ryoo BY, Hsu CH, et al. Atezolizumab with or without bevacizumab in unresectable hepatocellular carcinoma (GO30140): an open-label, multicentre, phase 1b study. Lancet Oncol. 2020;21(6):808–820. doi:10.1016/S1470-2045(20)30156-X
19. Rimassa L, Finn RS, Sangro B. Combination immunotherapy for hepatocellular carcinoma. J Hepatol. 2023;79(2):506–515. doi:10.1016/j.jhep.2023.03.003
20. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus Durvalumab in Unresectable Hepatocellular Carcinoma. NEJM Evidence. 2022;1:EVIDoa2100070. doi:10.1056/EVIDoa2100070
21. Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66. doi:10.1016/S0140-6736(16)32453-9
22. Abou-Alfa GK, Meyer T, Cheng AL, et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. New Engl J Med. 2018;379(1):54–63. doi:10.1056/NEJMoa1717002
23. Zhu AX, Kang YK, Yen CJ, et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(2):282–296. doi:10.1016/S1470-2045(18)30937-9
24. Demir T, Lee SS, Kaseb AO. Systemic therapy of liver cancer. Adv Cancer Res. 2021;149:257–294.
25. Yau T, Park JW, Finn RS, et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2022;23(1):77–90. doi:10.1016/S1470-2045(21)00604-5
26. Finn RS, Ryoo BY, Merle P, et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: a Randomized, Double-Blind, Phase III Trial. J Clin Oncol. 2020;38(3):193–202. doi:10.1200/JCO.19.01307
27. Yau T, Kang YK, Kim TY, et al. Efficacy and Safety of Nivolumab Plus Ipilimumab in Patients With Advanced Hepatocellular Carcinoma Previously Treated With Sorafenib: the CheckMate 040 Randomized Clinical Trial. JAMA Oncol. 2020;6(11):e204564. doi:10.1001/jamaoncol.2020.4564
28. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, phase 2-3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
29. Finn RS, Ikeda M, Zhu AX, et al. Phase Ib Study of Lenvatinib Plus Pembrolizumab in Patients With Unresectable Hepatocellular Carcinoma. J Clin Oncol. 2020;38(26):2960–2970. doi:10.1200/JCO.20.00808
30. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
31. Xu J, Shen J, Gu S, et al. Camrelizumab in Combination with Apatinib in Patients with Advanced Hepatocellular Carcinoma (RESCUE): a Nonrandomized, Open-label, Phase II Trial. Clin Cancer Res. 2021;27(4):1003–1011. doi:10.1158/1078-0432.CCR-20-2571
32. Kelley RK, Sangro B, Harris W, et al. Safety, Efficacy, and Pharmacodynamics of Tremelimumab Plus Durvalumab for Patients With Unresectable Hepatocellular Carcinoma: randomized Expansion of a Phase I/II Study. J Clin Oncol. 2021;39(27):2991–3001. doi:10.1200/JCO.20.03555
33. Sangro B, Gomez-Martin C, de la Mata M, et al. A clinical trial of CTLA-4 blockade with tremelimumab in patients with hepatocellular carcinoma and chronic hepatitis C. J Hepatol. 2013;59(1):81–88. doi:10.1016/j.jhep.2013.02.022
34. Qin S, Ren Z, Meng Z, et al. Camrelizumab in patients with previously treated advanced hepatocellular carcinoma: a multicentre, open-label, parallel-group, randomised, phase 2 trial. Lancet Oncol. 2020;21(4):571–580. doi:10.1016/S1470-2045(20)30011-5
35. Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. New Engl J Med. 1996;334(11):693–699. doi:10.1056/NEJM199603143341104
36. O’Donnell JS. EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
37. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
38. Kulik L, Heimbach JK, Zaiem F, et al. Therapies for patients with hepatocellular carcinoma awaiting liver transplantation: a systematic review and meta-analysis. Hepatology. 2018;67(1):381–400. doi:10.1002/hep.29485
39. Zhang Y, Huang G, Wang Y, et al. Is Salvage Liver Resection Necessary for Initially Unresectable Hepatocellular Carcinoma Patients Downstaged by Transarterial Chemoembolization? Ten Years of Experience. oncologist. 2016;21(12):1442–1449. doi:10.1634/theoncologist.2016-0094
40. Lewandowski RJ, Kulik LM, Riaz A, et al. A comparative analysis of transarterial downstaging for hepatocellular carcinoma: chemoembolization versus radioembolization. Am j Transplantation. 2009;9(8):1920–1928. doi:10.1111/j.1600-6143.2009.02695.x
41. Nordness MF, Hamel S, Godfrey CM, et al. Fatal hepatic necrosis after nivolumab as a bridge to liver transplant for HCC: are checkpoint inhibitors safe for the pretransplant patient? Am j Transplantation. 2020;20(3):879–883. doi:10.1111/ajt.15617
42. Topalian SL, Taube JM, Pardoll DM. Neoadjuvant checkpoint blockade for cancer immunotherapy. Science. 2020;368(6489):367. doi:10.1126/science.abb5060
43. Ho WJ, Zhu Q, Durham J, et al. Neoadjuvant Cabozantinib and Nivolumab Converts Locally Advanced HCC into Resectable Disease with Enhanced Antitumor Immunity. Nat Cancer. 2021;2(9):891–903. doi:10.1038/s43018-021-00234-4
44. Liu J, O’Donnell JS, Yan J, et al. Timing of neoadjuvant immunotherapy in relation to surgery is crucial for outcome. Oncoimmunology. 2019;8(5):e1581530. doi:10.1080/2162402X.2019.1581530
45. Meyer T, Fox R, Ma YT, et al. Sorafenib in combination with transarterial chemoembolisation in patients with unresectable hepatocellular carcinoma (TACE 2): a randomised placebo-controlled, double-blind, phase 3 trial. Lancet Gastroenterol Hepatol. 2017;2(8):565–575. doi:10.1016/S2468-1253(17)30156-5
46. Ricke J, Klümpen HJ, Amthauer H, et al. Impact of combined selective internal radiation therapy and sorafenib on survival in advanced hepatocellular carcinoma. J Hepatol. 2019;71(6):1164–1174. doi:10.1016/j.jhep.2019.08.006
47. Kawamura Y, Kobayashi M, Shindoh J, et al. Lenvatinib-Transarterial Chemoembolization Sequential Therapy as an Effective Treatment at Progression during Lenvatinib Therapy for Advanced Hepatocellular Carcinoma. Liver Cancer. 2020;9(6):756–770. doi:10.1159/000510299
48. Tampaki M, Ionas E, Hadziyannis E, Deutsch M, Malagari K, Koskinas J. Association of TIM-3 with BCLC Stage, Serum PD-L1 Detection, and Response to Transarterial Chemoembolization in Patients with Hepatocellular Carcinoma. Cancers. 2020;12(1):212. doi:10.3390/cancers12010212
49. Wehrenberg-Klee E, Goyal L, Dugan M, Zhu AX, Ganguli S. Y-90 Radioembolization Combined with a PD-1 Inhibitor for Advanced Hepatocellular Carcinoma. Cardiovascular Interventional Radiol. 2018;41(11):1799–1802. doi:10.1007/s00270-018-1993-1
50. Chao J, Zhu Q, Chen D, et al. Case Report: transarterial Chemoembolization in Combination With Tislelizumab Downstages Unresectable Hepatocellular Carcinoma Followed by Radical Salvage Resection. Front Oncol. 2021;11:667555. doi:10.3389/fonc.2021.667555
51. Xin H, Zhang C, Ding Z, Zhang M, Ding G, Li N. TACE plus PD-1 inhibitor (Camrelizumab) treatment for bridging to tumor resection in HCC: case reports. Clin Res Hepatol Gastroenterol. 2022;46(1):101777. doi:10.1016/j.clinre.2021.101777
52. Kim HJ, Park S, Kim KJ, Seong J. Clinical significance of soluble programmed cell death ligand-1 (sPD-L1) in hepatocellular carcinoma patients treated with radiotherapy. Radiotherapy Oncol. 2018;129(1):130–135. doi:10.1016/j.radonc.2017.11.027
53. Zhong L, Wu D, Peng W, et al. Safety of PD-1/PD-L1 Inhibitors Combined With Palliative Radiotherapy and Anti-Angiogenic Therapy in Advanced Hepatocellular Carcinoma. Front Oncol. 2021;11:686621. doi:10.3389/fonc.2021.686621
54. Juloori A, Katipally RR, Lemons JM, et al. Phase 1 Randomized Trial of Stereotactic Body Radiation Therapy Followed by Nivolumab plus Ipilimumab or Nivolumab Alone in Advanced/Unresectable Hepatocellular Carcinoma. Int J Radiat Oncol Biol Phys. 2023;115(1):202–213. doi:10.1016/j.ijrobp.2022.09.052
55. Makuuchi M, Kosuge T, Takayama T, et al. Surgery for small liver cancers. Seminars Surgical Oncol. 1993;9(4):298–304. doi:10.1002/ssu.2980090404
56. Abu Hilal M, Aldrighetti L, Dagher I, et al. The Southampton Consensus Guidelines for Laparoscopic Liver Surgery: from Indication to Implementation. Ann Surg. 2018;268(1):11–18. doi:10.1097/SLA.0000000000002524
57. Bhutiani N, Scoggins CR, McMasters KM, et al. The impact of caudate lobe resection on margin status and outcomes in patients with hilar cholangiocarcinoma: a multi-institutional analysis from the US Extrahepatic Biliary Malignancy Consortium. Surgery. 2018;163(4):726–731. doi:10.1016/j.surg.2017.10.028
58. Xiangfei M, Yinzhe X, Yingwei P, Shichun L, Weidong D. Open versus laparoscopic hepatic resection for hepatocellular carcinoma: a systematic review and meta-analysis. Surg Endosc. 2019;33(8):2396–2418. doi:10.1007/s00464-019-06781-3
59. Stiles ZE, Glazer ES, Deneve JL, Shibata D, Behrman SW, Dickson PV. Long-Term Implications of Unplanned Conversion During Laparoscopic Liver Resection for Hepatocellular Carcinoma. Ann Surg Oncol. 2019;26(1):282–289. doi:10.1245/s10434-018-7073-6
60. Ballantyne GH. The pitfalls of laparoscopic surgery: challenges for robotics and telerobotic surgery. Surgical Laparoscopy Endoscopy & Percutaneous Techniques. 2002;12(1):1–5. doi:10.1097/00129689-200202000-00001
61. Berguer R, Rab GT, Abu-Ghaida H, Alarcon A, Chung J. A comparison of surgeons’ posture during laparoscopic and open surgical procedures. Surg Endosc. 1997;11(2):139–142. doi:10.1007/s004649900316
62. Idrees K, Bartlett DL. Robotic liver surgery. Surgical Clin North Am. 2010;90(4):761–774. doi:10.1016/j.suc.2010.04.020
63. Cipriani F, Fiorentini G, Magistri P, et al. Pure laparoscopic versus robotic liver resections: multicentric propensity score-based analysis with stratification according to difficulty scores. J Hepato-Biliary-Pancreatic Sci. 2022;29(10):1108–1123. doi:10.1002/jhbp.1022
64. Zhu P, Liao W, Zhang WG, et al. A Prospective Study Using Propensity Score Matching to Compare Long-term Survival Outcomes After Robotic-assisted, Laparoscopic, or Open Liver Resection for Patients With BCLC Stage 0-A Hepatocellular Carcinoma. Ann Surg. 2023;277(1):e103–e111. doi:10.1097/SLA.0000000000005380
65. Kang KJ, Ahn KS. Anatomical resection of hepatocellular carcinoma: a critical review of the procedure and its benefits on survival. World J Gastroenterol. 2017;23(7):1139–1146. doi:10.3748/wjg.v23.i7.1139
66. Makuuchi M, Hasegawa H, Yamazaki S. Ultrasonically guided subsegmentectomy. Surg Gynecology Obstetrics. 1985;161:346–350.
67. Shindoh J, Hasegawa K, Inoue Y, et al. Risk factors of post-operative recurrence and adequate surgical approach to improve long-term outcomes of hepatocellular carcinoma. j Int Hepato Pancreato Biliary Assoc. 2013;15(1):31–39. doi:10.1111/j.1477-2574.2012.00552.x
68. Shindoh J, Makuuchi M, Matsuyama Y, et al. Complete removal of the tumor-bearing portal territory decreases local tumor recurrence and improves disease-specific survival of patients with hepatocellular carcinoma. J Hepatol. 2016;64(3):594–600. doi:10.1016/j.jhep.2015.10.015
69. Zhang XP, Xu S, Lin ZY, et al. Significance of anatomical resection and resection margin status in patients with HBV-related hepatocellular carcinoma and microvascular invasion: a multicenter propensity score-matched study. Int j Surgery. 2023;109(4):679–688. doi:10.1097/JS9.0000000000000204
70. Jung DH, Hwang S, Lee YJ, et al. Small Hepatocellular Carcinoma With Low Tumor Marker Expression Benefits More From Anatomical Resection Than Tumors With Aggressive Biology. Ann Surg. 2019;269(3):511–519. doi:10.1097/SLA.0000000000002486
71. Eguchi S, Kanematsu T, Arii S, et al. Comparison of the outcomes between an anatomical subsegmentectomy and a non-anatomical minor hepatectomy for single hepatocellular carcinomas based on a Japanese nationwide survey. Surgery. 2008;143(4):469–475. doi:10.1016/j.surg.2007.12.003
72. Hidaka M, Eguchi S, Okuda K, et al. Impact of Anatomical Resection for Hepatocellular Carcinoma With Microportal Invasion (vp1): a Multi-institutional Study by the Kyushu Study Group of Liver Surgery. Ann Surg. 2020;271(2):339–346. doi:10.1097/SLA.0000000000002981
73. Tanaka K, Shimada H, Matsumoto C, et al. Anatomic versus limited nonanatomic resection for solitary hepatocellular carcinoma. Surgery. 2008;143(5):607–615. doi:10.1016/j.surg.2008.01.006
74. Famularo S, Di Sandro S, Giani A. Long-term oncologic results of anatomic vs. parenchyma-sparing resection for hepatocellular carcinoma. A propensity score-matching analysis. Eur j Surgical Oncol. 2018;44(10):1580–1587. doi:10.1016/j.ejso.2018.05.018
75. Li SQ, Huang T, Shen SL, et al. Anatomical versus non-anatomical liver resection for hepatocellular carcinoma exceeding Milan criteria. Br J Surg. 2017;104:118–127. doi:10.1002/bjs.10311
76. Poon RT, Fan ST, Ng IO, Wong J. Significance of resection margin in hepatectomy for hepatocellular carcinoma: a critical reappraisal. Ann Surg. 2000;231:544–551. doi:10.1097/00000658-200004000-00014
77. Zhong FP, Zhang YJ, Liu Y, Zou SB. Prognostic impact of surgical margin in patients with hepatocellular carcinoma: a meta-analysis. Medicine. 2017;96(37):e8043. doi:10.1097/MD.0000000000008043
78. O’Donnell JS. Corrigendum to “EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol. 2019;70(4):817. doi:10.1016/j.jhep.2019.01.020
79. Roayaie S, Obeidat K, Sposito C, et al. Resection of hepatocellular cancer ≤2 cm: results from two Western centers. Hepatology. 2013;57(4):1426–1435. doi:10.1002/hep.25832
80. Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology. 2005;42(5):1208–1236. doi:10.1002/hep.20933
81. Bruix J, Sherman M, Llovet JM, et al. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. J Hepatol. 2001;35(3):421–430. doi:10.1016/S0168-8278(01)00130-1
82. Makuuchi M, Kokudo N, Arii S, et al. Development of evidence-based clinical guidelines for the diagnosis and treatment of hepatocellular carcinoma in Japan. Hepatol Res. 2008;38(1):37–51. doi:10.1111/j.1872-034X.2007.00216.x
83. Imai K, Beppu T, Chikamoto A, et al. Comparison between hepatic resection and radiofrequency ablation as first-line treatment for solitary small-sized hepatocellular carcinoma of 3 cm or less. Hepatol Res. 2013;43(8):853–864. doi:10.1111/hepr.12035
84. Doi K, Beppu T, Ishiko T, et al. Endoscopic radiofrequency ablation in elderly patients with hepatocellular carcinoma. Anticancer Res. 2015;35(5):3033–3040.
85. Tsukamoto M, Imai K, Yamashita YI, et al. Endoscopic hepatic resection and endoscopic radiofrequency ablation as initial treatments for hepatocellular carcinoma within the Milan criteria. Surgery Today. 2020;50(4):402–412. doi:10.1007/s00595-019-01903-9
86. Lee EW, Chen C, Prieto VE, Dry SM, Loh CT, Kee ST. Advanced hepatic ablation technique for creating complete cell death: irreversible electroporation. Radiology. 2010;255:426–433.
87. Sutter O, Calvo J, N’Kontchou G, et al. Safety and Efficacy of Irreversible Electroporation for the Treatment of Hepatocellular Carcinoma Not Amenable to Thermal Ablation Techniques: a Retrospective Single-Center Case Series. Radiology. 2017;284(3):877–886. doi:10.1148/radiol.2017161413
88. Bruix J, Takayama T, Mazzaferro V, et al. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): a phase 3, randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2015;16(13):1344–1354. doi:10.1016/S1470-2045(15)00198-9
89. Llovet JM, Zucman-Rossi J, Pikarsky E, et al. Hepatocellular carcinoma. Nature Reviews Disease Primers. 2016;2:16018. doi:10.1038/nrdp.2016.18
90. Kulik L, El-Serag HB. Epidemiology and Management of Hepatocellular Carcinoma. Gastroenterology. 2019;156(2):477–491.e471. doi:10.1053/j.gastro.2018.08.065
91. Llovet JM, Montal R, Sia D, Finn RS. Molecular therapies and precision medicine for hepatocellular carcinoma. Nat Rev Clin Oncol. 2018;15(10):599–616. doi:10.1038/s41571-018-0073-4
92. Greten TF, Lai CW, Li G, Staveley-O’Carroll KF. Targeted and Immune-Based Therapies for Hepatocellular Carcinoma. Gastroenterology. 2019;156(2):510–524. doi:10.1053/j.gastro.2018.09.051
93. Peng ZW, Zhang YJ, Chen MS, et al. Radiofrequency ablation with or without transcatheter arterial chemoembolization in the treatment of hepatocellular carcinoma: a prospective randomized trial. J Clin Oncol. 2013;31(4):426–432. doi:10.1200/JCO.2012.42.9936
94. Chen K, Chen G, Wang H, et al. Increased survival in hepatocellular carcinoma with iodine-125 implantation plus radiofrequency ablation: a prospective randomized controlled trial. J Hepatol. 2014;61(6):1304–1311. doi:10.1016/j.jhep.2014.07.026
95. Gabrielson A, Wu Y, Wang H, et al. Intratumoral CD3 and CD8 T-cell Densities Associated with Relapse-Free Survival in HCC. Cancer Immunol Res. 2016;4(5):419–430. doi:10.1158/2326-6066.CIR-15-0110
96. Lee JH, Lee JH, Lim YS, et al. Adjuvant immunotherapy with autologous cytokine-induced killer cells for hepatocellular carcinoma. Gastroenterology. 2015;148:1383–1391.e1386. doi:10.1053/j.gastro.2015.02.055
97. Hao MZ, Lin HL, Chen Q, Ye YB, Chen QZ, Chen MS. Efficacy of transcatheter arterial chemoembolization combined with cytokine-induced killer cell therapy on hepatocellular carcinoma: a comparative study. Chinese j Cancer. 2010;29:172–177. doi:10.5732/cjc.009.10410
98. Pan CC, Huang ZL, Li W, et al. Serum alpha-fetoprotein measurement in predicting clinical outcome related to autologous cytokine-induced killer cells in patients with hepatocellular carcinoma undergone minimally invasive therapy. Chinese j Cancer. 2010;29:596–602. doi:10.5732/cjc.009.10580
99. Weng DS, Zhou J, Zhou QM, et al. Minimally invasive treatment combined with cytokine-induced killer cells therapy lower the short-term recurrence rates of hepatocellular carcinomas. J Immunother. 2008;31(1):63–71. doi:10.1097/CJI.0b013e31815a121b
100. Hui D, Qiang L, Jian W, Ti Z, Da-Lu K. A randomized, controlled trial of postoperative adjuvant cytokine-induced killer cells immunotherapy after radical resection of hepatocellular carcinoma. Digestive Liver Dis. 2009;41(1):36–41. doi:10.1016/j.dld.2008.04.007
101. Yu X, Zhao H, Liu L, et al. A randomized phase II study of autologous cytokine-induced killer cells in treatment of hepatocellular carcinoma. J Clin Immunol. 2014;34(2):194–203. doi:10.1007/s10875-013-9976-0
102. Llovet JM, Real MI, Montaña X, et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. 2002;359(9319):1734–1739. doi:10.1016/S0140-6736(02)08649-X
103. Lo CM, Ngan H, Tso WK, et al. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology. 2002;35(5):1164–1171. doi:10.1053/jhep.2002.33156
104. Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology. 2003;37(2):429–442. doi:10.1053/jhep.2003.50047
105. Okusaka T, Kasugai H, Shioyama Y, et al. Transarterial chemotherapy alone versus transarterial chemoembolization for hepatocellular carcinoma: a randomized phase III trial. J Hepatol. 2009;51(6):1030–1036. doi:10.1016/j.jhep.2009.09.004
106. Yu SC, Hui JW, Hui EP, et al. Unresectable hepatocellular carcinoma: randomized controlled trial of transarterial ethanol ablation versus transcatheter arterial chemoembolization. Radiology. 2014;270(2):607–620. doi:10.1148/radiol.13130498
107. Golfieri R, Giampalma E, Renzulli M, et al. Randomised controlled trial of doxorubicin-eluting beads vs conventional chemoembolisation for hepatocellular carcinoma. Br. J. Cancer. 2014;111(2):255–264. doi:10.1038/bjc.2014.199
108. Marelli L, Stigliano R, Triantos C, et al. Transarterial therapy for hepatocellular carcinoma: which technique is more effective? A systematic review of cohort and randomized studies. Cardiovascular Interventional Radiol. 2007;30(1):6–25. doi:10.1007/s00270-006-0062-3
109. Llovet JM, Villanueva A, Marrero JA, et al. Trial Design and Endpoints in Hepatocellular Carcinoma: AASLD Consensus Conference. Hepatology. 2021;73 Suppl 1(S1):158–191. doi:10.1002/hep.31327
110. Kudo M, Imanaka K, Chida N, et al. Phase III study of sorafenib after transarterial chemoembolisation in Japanese and Korean patients with unresectable hepatocellular carcinoma. Eur. J. Cancer. 2011;47(14):2117–2127. doi:10.1016/j.ejca.2011.05.007
111. Kudo M, Han G, Finn RS, et al. Brivanib as adjuvant therapy to transarterial chemoembolization in patients with hepatocellular carcinoma: a randomized phase III trial. Hepatology. 2014;60(5):1697–1707. doi:10.1002/hep.27290
112. Lencioni R, Llovet JM, Han G, et al. Sorafenib or placebo plus TACE with doxorubicin-eluting beads for intermediate stage HCC: the SPACE trial. J Hepatol. 2016;64(5):1090–1098. doi:10.1016/j.jhep.2016.01.012
113. Kudo M, Cheng AL, Park JW, et al. Orantinib versus placebo combined with transcatheter arterial chemoembolisation in patients with unresectable hepatocellular carcinoma (ORIENTAL): a randomised, double-blind, placebo-controlled, multicentre, phase 3 study. Lancet Gastroenterol Hepatol. 2018;3(1):37–46. doi:10.1016/S2468-1253(17)30290-X
114. Kudo M, Kubo S, Takayasu K, et al. Response Evaluation Criteria in Cancer of the Liver (RECICL) proposed by the Liver Cancer Study Group of Japan (2009 Revised Version). Hepatol Res. 2010;40(7):686–692. doi:10.1111/j.1872-034X.2010.00674.x
115. Kudo M, Ueshima K, Ikeda M, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut. 2020;69(8):1492–1501. doi:10.1136/gutjnl-2019-318934
116. Llovet JM, De Baere T, Kulik L. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2021;18(5):293–313. doi:10.1038/s41575-020-00395-0
117. Greten TF, Mauda-Havakuk M, Heinrich B, Korangy F, Wood BJ. Combined locoregional-immunotherapy for liver cancer. J Hepatol. 2019;70(5):999–1007. doi:10.1016/j.jhep.2019.01.027
118. Duffy AG, Ulahannan SV, Makorova-Rusher O, et al. Tremelimumab in combination with ablation in patients with advanced hepatocellular carcinoma. J Hepatol. 2017;66(3):545–551. doi:10.1016/j.jhep.2016.10.029
119. Quirk M, Kim YH, Saab S, Lee EW. Management of hepatocellular carcinoma with portal vein thrombosis. World J Gastroenterol. 2015;21(12):3462–3471. doi:10.3748/wjg.v21.i12.3462
120. Llovet JM, Bustamante J, Castells A. Natural history of untreated nonsurgical hepatocellular carcinoma: rationale for the design and evaluation of therapeutic trials. Hepatology. 1999;29(1):62–67. doi:10.1002/hep.510290145
121. Deng ZJ, Li L, Teng YX, et al. Treatments of Hepatocellular Carcinoma with Portal Vein Tumor Thrombus: current Status and Controversy. J Clin Translational Hepatol. 2022;10(1):147–158. doi:10.14218/JCTH.2021.00179
122. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
123. Vogel A, Cervantes A, Chau I, et al. Correction to: “Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up”. Ann Oncol. 2019;30(5):871–873. doi:10.1093/annonc/mdy510
124. Kokudo T, Hasegawa K, Matsuyama Y, et al. Survival benefit of liver resection for hepatocellular carcinoma associated with portal vein invasion. J Hepatol. 2016;65(5):938–943. doi:10.1016/j.jhep.2016.05.044
125. Wang K, Guo WX, Chen MS, et al. Multimodality Treatment for Hepatocellular Carcinoma With Portal Vein Tumor Thrombus: a Large-Scale, Multicenter, Propensity Mathching Score Analysis. Medicine. 2016;95(11):e3015. doi:10.1097/MD.0000000000003015
126. Kaneko S, Tsuchiya K, Yasui Y, et al. Strategy for advanced hepatocellular carcinoma based on liver function and portal vein tumor thrombosis. Hepatol Res. 2020;50(12):1375–1385. doi:10.1111/hepr.13567
127. Luo JJ, Zhang ZH, Liu QX, Zhang W, Wang JH, Yan ZP. Endovascular brachytherapy combined with stent placement and TACE for treatment of HCC with main portal vein tumor thrombus. Hepatol Internat. 2016;10(1):185–195. doi:10.1007/s12072-015-9663-8
128. Huang C, Zhu XD, Shen YH, et al. Organ specific responses to first-line lenvatinib plus anti-PD-1 antibodies in patients with unresectable hepatocellular carcinoma: a retrospective analysis. Biomarker Res. 2021;9(1):19. doi:10.1186/s40364-021-00274-z
129. Zhang ZH, Hou SN, Yu JZ, et al. Combined iodine-125 seed strand, portal vein stent, transarterial chemoembolization, lenvatinib and anti-PD-1 antibodies therapy for hepatocellular carcinoma and Vp4 portal vein tumor thrombus: a propensity-score analysis. Front Oncol. 2022;12:1086095. doi:10.3389/fonc.2022.1086095
130. Lencioni R, Kudo M, Ye SL, et al. GIDEON (Global Investigation of therapeutic DE cisions in hepatocellular carcinoma and Of its treatment with sorafeNib): second interim analysis. Int J Clin Pract. 2014;68(5):609–617. doi:10.1111/ijcp.12352
131. McNamara MG, Slagter AE, Nuttall C, et al. Sorafenib as first-line therapy in patients with advanced Child-Pugh B hepatocellular carcinoma-a meta-analysis. Eur. J. Cancer. 2018;105:1–9. doi:10.1016/j.ejca.2018.09.031
132. Huynh J, Cho MT, Kim EJ, Ren M, Ramji Z, Vogel A. Lenvatinib in patients with unresectable hepatocellular carcinoma who progressed to Child-Pugh B liver function. Therapeut Adv Med Oncol. 2022;14:17588359221116608. doi:10.1177/17588359221116608
133. Tsuchiya K, Kurosaki M, Sakamoto A, et al. The Real-World Data in Japanese Patients with Unresectable Hepatocellular Carcinoma Treated with Lenvatinib from a Nationwide Multicenter Study. Cancers. 2021;13(11):2608. doi:10.3390/cancers13112608
134. Park MK, Lee YB, Moon H, et al. Effectiveness of Lenvatinib Versus Sorafenib for Unresectable Hepatocellular Carcinoma in Patients with Hepatic Decompensation. Dig Dis Sci. 2022;67(10):4939–4949. doi:10.1007/s10620-021-07365-9
135. Finkelmeier F, Scheiner B, Leyh C, et al. Cabozantinib in Advanced Hepatocellular Carcinoma: efficacy and Safety Data from an International Multicenter Real-Life Cohort. Liver Cancer. 2021;10(4):360–369. doi:10.1159/000515490
136. El-Khoueiry AB, Sangro B, Yau T, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet. 2017;389(10088):2492–2502. doi:10.1016/S0140-6736(17)31046-2
137. Chapin WJ, Hwang WT, Karasic TB, McCarthy AM, Kaplan DE. Comparison of nivolumab and sorafenib for first systemic therapy in patients with hepatocellular carcinoma and Child-Pugh B cirrhosis. Cancer Med. 2023;12(1):189–199. doi:10.1002/cam4.4906
138. Choi WM, Lee D, Shim JH, et al. Effectiveness and Safety of Nivolumab in Child-Pugh B Patients with Hepatocellular Carcinoma: a Real-World Cohort Study. Cancers. 2020;12(7):1968. doi:10.3390/cancers12071968
139. D’Alessio A, Fulgenzi CAM, Nishida N, et al. Preliminary evidence of safety and tolerability of atezolizumab plus bevacizumab in patients with hepatocellular carcinoma and Child-Pugh A and B cirrhosis: a real-world study. Hepatology. 2022;76(4):1000–1012. doi:10.1002/hep.32468
140. Harding JJ, Nandakumar S, Armenia J, et al. Prospective Genotyping of Hepatocellular Carcinoma: clinical Implications of Next-Generation Sequencing for Matching Patients to Targeted and Immune Therapies. Clin Cancer Res. 2019;25(7):2116–2126. doi:10.1158/1078-0432.CCR-18-2293
141. Horwitz E, Stein I, Andreozzi M, et al. Human and Mouse VEGFA -Amplified Hepatocellular Carcinomas Are Highly Sensitive to Sorafenib Treatment. Cancer Discovery. 2014;4(6):730–743. doi:10.1158/2159-8290.CD-13-0782
142. Feng J, Lu PZ, Zhu GZ, et al. ACSL4 is a predictive biomarker of sorafenib sensitivity in hepatocellular carcinoma. Acta Pharmacol. Sin. 2021;42(1):160–170. doi:10.1038/s41401-020-0439-x
143. Myojin Y, Kodama T, Maesaka K, et al. ST6GAL1 Is a Novel Serum Biomarker for Lenvatinib-Susceptible FGF19-Driven Hepatocellular Carcinoma. Clin Cancer Res. 2021;27(4):1150–1161. doi:10.1158/1078-0432.CCR-20-3382
144. Finn RS, Kudo M, Cheng AL, et al. Pharmacodynamic Biomarkers Predictive of Survival Benefit with Lenvatinib in Unresectable Hepatocellular Carcinoma: from the Phase III REFLECT Study. Clin Cancer Res. 2021;27(17):4848–4858. doi:10.1158/1078-0432.CCR-20-4219
145. Sangro B, Melero I, Wadhawan S, et al. Association of inflammatory biomarkers with clinical outcomes in nivolumab-treated patients with advanced hepatocellular carcinoma. J Hepatol. 2020;73(6):1460–1469. doi:10.1016/j.jhep.2020.07.026
146. Zhu AX, Abbas AR, de Galarreta MR, et al. Molecular correlates of clinical response and resistance to atezolizumab in combination with bevacizumab in advanced hepatocellular carcinoma. Nature Med. 2022;28(8):1599–1611. doi:10.1038/s41591-022-01868-2
147. Vogel A, Saborowski A. Current and Future Systemic Therapies in Biliary Tract Cancer. Visceral Medicine. 2021;37(1):32–38. doi:10.1159/000513969
148. Neumann UP, Schmeding M. Role of surgery in cholangiocarcinoma: from resection to transplantation. Best Practice Research Clin Gastroenterol. 2015;29(2):295–308. doi:10.1016/j.bpg.2015.02.007
149. Farges O, Fuks D, Boleslawski E, et al. Influence of surgical margins on outcome in patients with intrahepatic cholangiocarcinoma: a multicenter study by the AFC-IHCC-2009 study group. Ann Surg. 2011;254(5):824–829. doi:10.1097/SLA.0b013e318236c21d
150. Brauer DG, Fields RC, Tan BR, et al. Optimal extent of surgical and pathologic lymph node evaluation for resected intrahepatic cholangiocarcinoma. j Int Hepato Pancreato Biliary Assoc. 2018;20(5):470–476. doi:10.1016/j.hpb.2017.11.010
151. Sahara K, Tsilimigras DI, Merath K, et al. Therapeutic Index Associated with Lymphadenectomy Among Patients with Intrahepatic Cholangiocarcinoma: which Patients Benefit the Most from Nodal Evaluation? Ann Surg Oncol. 2019;26(9):2959–2968. doi:10.1245/s10434-019-07483-9
152. Zhang XF, Xue F, Dong DH, et al. Number and Station of Lymph Node Metastasis After Curative-intent Resection of Intrahepatic Cholangiocarcinoma Impact Prognosis. Ann Surg. 2021;274(6):e1187–e1195. doi:10.1097/SLA.0000000000003788
153. Jang JY, Kim SW, Park DJ, et al. Actual long-term outcome of extrahepatic bile duct cancer after surgical resection. Ann Surg. 2005;241(1):77–84. doi:10.1097/01.sla.0000150166.94732.88
154. Ito F, Agni R, Rettammel RJ, et al. Resection of hilar cholangiocarcinoma: concomitant liver resection decreases hepatic recurrence. Ann Surg. 2008;248(2):273–279. doi:10.1097/SLA.0b013e31817f2bfd
155. Feng JW, Yang XH, Wu BQ, Jiang Y, Qu Z. Progress in diagnosis and surgical treatment of perihilar cholangiocarcinoma. Gastroenterologia y hepatologia. 2019;42(4):271–279. doi:10.1016/j.gastrohep.2018.11.003
156. Sapisochín G, Fernández de Sevilla E, Echeverri J, Charco R. Liver transplantation for cholangiocarcinoma: current status and new insights. World j Hepatol. 2015;7(22):2396–2403. doi:10.4254/wjh.v7.i22.2396
157. Uijterwijk BA, Lemmers DHL, Bolm L, et al. Long-term Outcomes After Laparoscopic, Robotic, and Open Pancreatoduodenectomy for Distal Cholangiocarcinoma: an International Propensity Score-matched Cohort Study. Ann Surg. 2023;278(3):e570–e579. doi:10.1097/SLA.0000000000005743
158. Murakami Y, Uemura K, Hayashidani Y, et al. Prognostic significance of lymph node metastasis and surgical margin status for distal cholangiocarcinoma. J Surgical Oncol. 2007;95(3):207–212. doi:10.1002/jso.20668
159. Roa JC, García P, Kapoor VK, Maithel SK, Javle M, Koshiol J. Gallbladder cancer. Nature Reviews Disease Primers. 2022;8(1):69. doi:10.1038/s41572-022-00398-y
160. Zaidi MY, Maithel SK. Updates on Gallbladder Cancer Management. Curr Oncol Rep. 2018;20(2):21. doi:10.1007/s11912-018-0664-3
161. Lundgren L, Muszynska C, Ros A, et al. Management of incidental gallbladder cancer in a national cohort. Br J Surg. 2019;106(9):1216–1227. doi:10.1002/bjs.11205
162. Ebata T, Hirano S, Konishi M, et al. Randomized clinical trial of adjuvant gemcitabine chemotherapy versus observation in resected bile duct cancer. Br J Surg. 2018;105(3):192–202. doi:10.1002/bjs.10776
163. Edeline J, Benabdelghani M, Bertaut A, et al. Gemcitabine and Oxaliplatin Chemotherapy or Surveillance in Resected Biliary Tract Cancer (PRODIGE 12-ACCORD 18-UNICANCER GI): a Randomized Phase III Study. J Clin Oncol. 2019;37(8):658–667. doi:10.1200/JCO.18.00050
164. Primrose JN, Fox RP, Palmer DH, et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): a randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019;20(5):663–673. doi:10.1016/S1470-2045(18)30915-X
165. Bridgewater J, Galle PR, Khan SA, et al. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J Hepatol. 2014;60:1268–1289. doi:10.1016/j.jhep.2014.01.021
166. Mansour JC, Aloia TA, Crane CH, Heimbach JK, Nagino M, Vauthey JN. Hilar cholangiocarcinoma: expert consensus statement. j Int Hepato Pancreato Biliary Assoc. 2015;17(8):691–699. doi:10.1111/hpb.12450
167. Fulgenzi CAM, D’Alessio A, Airoldi C, et al. Comparative efficacy of novel combination strategies for unresectable hepatocellular carcinoma: a network metanalysis of phase III trials. Eur. J. Cancer. 2022;174:57–67. doi:10.1016/j.ejca.2022.06.058
168. DeVreede I, Steers JL, Burch PA. Prolonged disease-free survival after orthotopic liver transplantation plus adjuvant chemoirradiation for cholangiocarcinoma. Liver Transplantation. 2000;6(3):309–316. doi:10.1053/lv.2000.6143
169. Rosen CB, Heimbach JK, Gores GJ. Surgery for cholangiocarcinoma: the role of liver transplantation. j Int Hepato Pancreato Biliary Assoc. 2008;10(3):186–189. doi:10.1080/13651820801992542
170. Le Roy B, Gelli M, Pittau G, et al. Neoadjuvant chemotherapy for initially unresectable intrahepatic cholangiocarcinoma. Br J Surg. 2018;105(7):839–847. doi:10.1002/bjs.10641
171. Merath K, Chen Q, Bagante F, et al. A Multi-institutional International Analysis of Textbook Outcomes Among Patients Undergoing Curative-Intent Resection of Intrahepatic Cholangiocarcinoma. JAMA Surgery. 2019;154(6):e190571. doi:10.1001/jamasurg.2019.0571
172. Utuama O, Permuth JB, Dagne G, et al. Neoadjuvant Chemotherapy for Intrahepatic Cholangiocarcinoma: a Propensity Score Survival Analysis Supporting Use in Patients with High-Risk Disease. Ann Surg Oncol. 2021;28(4):1939–1949. doi:10.1245/s10434-020-09478-3
173. Cloyd JM, Prakash L, Vauthey JN, et al. The role of preoperative therapy prior to pancreatoduodenectomy for distal cholangiocarcinoma. Am J Surg. 2019;218(1):145–150. doi:10.1016/j.amjsurg.2018.08.024
174. Glazer ES, Liu P, Abdalla EK, Vauthey JN, Curley SA. Neither neoadjuvant nor adjuvant therapy increases survival after biliary tract cancer resection with wide negative margins. J Gastrointestinal Surgery. 2012;16:1666–1671. doi:10.1007/s11605-012-1935-1
175. Yadav S, Xie H, Bin-Riaz I, et al. Neoadjuvant vs. adjuvant chemotherapy for cholangiocarcinoma: a propensity score matched analysis. Eur j Surgical Oncol. 2019;45(8):1432–1438. doi:10.1016/j.ejso.2019.03.023
176. Buettner S, Koerkamp BG, Ejaz A, et al. The effect of preoperative chemotherapy treatment in surgically treated intrahepatic cholangiocarcinoma patients-A multi-institutional analysis. J Surgical Oncol. 2017;115(3):312–318. doi:10.1002/jso.24524
177. Omichi K, Cloyd JM, Yamashita S, et al. Neutrophil-to-lymphocyte ratio predicts prognosis after neoadjuvant chemotherapy and resection of intrahepatic cholangiocarcinoma. Surgery. 2017;162(4):752–765. doi:10.1016/j.surg.2017.05.015
178. Riby D, Mazzotta AD, Bergeat D, et al. Downstaging with Radioembolization or Chemotherapy for Initially Unresectable Intrahepatic Cholangiocarcinoma. Ann Surg Oncol. 2020;27(10):3729–3737. doi:10.1245/s10434-020-08486-7
179. Welling TH, Feng M, Wan S, et al. Neoadjuvant stereotactic body radiation therapy, capecitabine, and liver transplantation for unresectable hilar cholangiocarcinoma. Liver Transplantation. 2014;20(1):81–88. doi:10.1002/lt.23757
180. Jung JH, Lee HJ, Lee HS, et al. Benefit of neoadjuvant concurrent chemoradiotherapy for locally advanced perihilar cholangiocarcinoma. World J Gastroenterol. 2017;23(18):3301–3308. doi:10.3748/wjg.v23.i18.3301
181. Kuriyama N, Usui M, Gyoten K, et al. Neoadjuvant chemotherapy followed by curative-intent surgery for perihilar cholangiocarcinoma based on its anatomical resectability classification and lymph node status. BMC Cancer. 2020;20(1):405. doi:10.1186/s12885-020-06895-1
182. Valle J, Wasan H, Palmer DH, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. New Engl J Med. 2010;362(14):1273–1281. doi:10.1056/NEJMoa0908721
183. Okusaka T, Nakachi K, Fukutomi A, et al. Gemcitabine alone or in combination with cisplatin in patients with biliary tract cancer: a comparative multicentre study in Japan. Br. J. Cancer. 2010;103(4):469–474. doi:10.1038/sj.bjc.6605779
184. Marabelle A, Le DT, Ascierto PA, et al. Efficacy of Pembrolizumab in Patients With Noncolorectal High Microsatellite Instability/Mismatch Repair-Deficient Cancer: results From the Phase II KEYNOTE-158 Study. J Clin Oncol. 2020;38(1):1–10. doi:10.1200/JCO.19.02105
185. Kim RD, Chung V, Alese OB, et al. A Phase 2 Multi-institutional Study of Nivolumab for Patients With Advanced Refractory Biliary Tract Cancer. JAMA Oncol. 2020;6(6):888–894. doi:10.1001/jamaoncol.2020.0930
186. Ueno M, Ikeda M, Morizane C, et al. Nivolumab alone or in combination with cisplatin plus gemcitabine in Japanese patients with unresectable or recurrent biliary tract cancer: a non-randomised, multicentre, open-label, phase 1 study. Lancet Gastroenterol Hepatol. 2019;4(8):611–621. doi:10.1016/S2468-1253(19)30086-X
187. Feng K, Liu Y, Zhao Y, et al. Efficacy and biomarker analysis of nivolumab plus gemcitabine and cisplatin in patients with unresectable or metastatic biliary tract cancers: results from a phase II study. J ImmunoTherapy Cancer. 2020;8(1):e000367. doi:10.1136/jitc-2019-000367
188. Ebia MI, Sankar K, Osipov A, Hendifar AE, Gong J. TOPAZ-1: a new standard of care for advanced biliary tract cancers? Immunotherapy. 2023;15(7):473–476. doi:10.2217/imt-2022-0269
189. Kelley RK, Ueno M, Yoo C, et al. Pembrolizumab in combination with gemcitabine and cisplatin compared with gemcitabine and cisplatin alone for patients with advanced biliary tract cancer (KEYNOTE-966): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2023;401(10391):1853–1865. doi:10.1016/S0140-6736(23)00727-4
190. Li W, Wang Y, Yu Y, et al. Toripalimab in advanced biliary tract cancer. Innovation. 2022;3(4):100255. doi:10.1016/j.xinn.2022.100255
191. Lin J, Yang X, Long J, et al. Pembrolizumab combined with lenvatinib as non-first-line therapy in patients with refractory biliary tract carcinoma. Hepatobiliary Surgery Nutrition. 2020;9(4):414–424. doi:10.21037/hbsn-20-338
192. Zhang Q, Liu X, Wei S, et al. Lenvatinib Plus PD-1 Inhibitors as First-Line Treatment in Patients With Unresectable Biliary Tract Cancer: a Single-Arm, Open-Label, Phase II Study. Front Oncol. 2021;11:751391. doi:10.3389/fonc.2021.751391
193. Dennison L, Mohan AA, Yarchoan M. Tumor and Systemic Immunomodulatory Effects of MEK Inhibition. Curr Oncol Rep. 2021;23(2):23. doi:10.1007/s11912-020-01008-4
194. Ebert PJR, Cheung J, Yang Y, et al. MAP Kinase Inhibition Promotes T Cell and Anti-tumor Activity in Combination with PD-L1 Checkpoint Blockade. Immunity. 2016;44(3):609–621. doi:10.1016/j.immuni.2016.01.024
195. Liu L, Mayes PA, Eastman S, et al. The BRAF and MEK Inhibitors Dabrafenib and Trametinib: effects on Immune Function and in Combination with Immunomodulatory Antibodies Targeting PD-1, PD-L1, and CTLA-4. Clin Cancer Res. 2015;21(7):1639–1651. doi:10.1158/1078-0432.CCR-14-2339
196. Hellmann MD, Kim TW, Lee CB, et al. Phase Ib study of atezolizumab combined with cobimetinib in patients with solid tumors. Ann Oncol. 2019;30(7):1134–1142. doi:10.1093/annonc/mdz113
197. Yarchoan M, Cope L, Ruggieri AN, et al. Multicenter randomized phase II trial of atezolizumab with or without cobimetinib in biliary tract cancers. J Clin Invest. 2021;131(24). doi:10.1172/JCI152670.
198. Wang K, Liu ZH, Yu HM, et al. Efficacy and safety of a triple combination of atezolizumab, bevacizumab plus GEMOX for advanced biliary tract cancer: a multicenter, single-arm, retrospective study. Ther Adv Gastroenterol. 2023;16:17562848231160630. doi:10.1177/17562848231160630
199. Chen X, Wu X, Wu H, et al. Camrelizumab plus gemcitabine and oxaliplatin (GEMOX) in patients with advanced biliary tract cancer: a single-arm, open-label, phase II trial. J ImmunoTherapy Cancer. 2020;8(2):e001240. doi:10.1136/jitc-2020-001240
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.