Back to Journals » Advances in Medical Education and Practice » Volume 17
The Silent “Teacher”: A Conceptual Framework and Teaching Model for Cultivating Medical Humanities in Morphological Experiments
Received 29 December 2025
Accepted for publication 19 March 2026
Published 25 March 2026 Volume 2026:17 592495
DOI https://doi.org/10.2147/AMEP.S592495
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sateesh Arja
Gaoshang Chai, Xiaorun Zhai
Department of Basic Medicine, Wuxi School of Medicine, Jiangnan University, Wuxi, Jiangsu, 214122, People’s Republic of China
Correspondence: Xiaorun Zhai, Department of Basic Medicine, Wuxi School of Medicine, Jiangnan University, Wuxi, Jiangsu, 214122, People’s Republic of China, Email [email protected]
Abstract: Objective: This paper aims to propose a structured pedagogical framework (Ritual–Narrative–Responsibility) for seamlessly integrating medical humanities into morphological experiment teaching, and to elaborate its theoretical foundations, specific implementation pathways, and preliminary evaluation strategies. The morphology laboratory is the initial space where medical students first confront the authenticity of life, serving as a venue for learning cellular structures and histopathology while guiding learners to perceive the profound life connotations behind microscopic specimens. Nevertheless, against the backdrop of increasingly technologized and instrumentalized medical education, morphological experiment curricula are facing a severe crisis: the gradual decline of humanistic spirit. As a conceptual framework and teaching model study, this paper explores the approach of integrating medical humanities education into morphological experiment teaching like salt dissolving in water. Based on a critical analysis of the “alienation” phenomenon in current teaching, it constructs an integrated model with “Ritual–Narrative–Responsibility” as three core pillars: fostering reverence for life through ritualized practices, inspiring empathy via narrative medicine, and forging professional accountability through ethical reflection. This paper expounds the theoretical bases, detailed implementation routes, and evaluation propositions of the three pillars respectively, emphasizing that medical humanities education is not an external appendage to morphological teaching, but an inherent requirement for its return to the essence of “life education”. It intends to guide students to focus on the complete “person” while exploring “diseases”, shape their professional virtues of reverence, empathy, and responsibility, and lay a solid humanistic foundation for cultivating future physicians with both medical expertise and compassionate hearts.
Keywords: morphological experiments, medical humanities, silent teacher, empathy education, medical ethics
Introduction
When technological rationality overshadows humanistic care, an intangible “alienation” occurs quietly in the laboratory. In the morphology laboratory filled with the smell of formalin, a prominent “dehumanization” tendency prevails. We often witness scenes where students discuss trivial daily matters while dissecting selflessly donated cadavers; groups rush to find cancer cells under microscopes, only showing the excitement of solving puzzles without compassion for the deceased; tissue slides carrying years of individual suffering are reduced to mere specimens for identification and grading. This “alienation” does not stem from students’ innate indifference, but exposes a structural defect in the education system: in the pursuit of efficient and objective knowledge transmission, the intrinsic connection between “morphology” and “life”, “disease” and “patient” has been systematically severed. Students are trained as skilled “morphology interpreters” but may lose the core ability of being “emotional resonators”. Long-term exposure to this model may cultivate “technically proficient strangers” who master advanced tools but are isolated by intangible barriers, unable to perceive patients’ sufferings.1
However, crises also contain seeds of hope. The morphology laboratory is an irreplaceable key field for resisting this trend and carrying out medical humanities education.2 It is the origin for medical students to understand life: the first time they step out of textbook images to touch real human structures; the first time they face the “scene” of diseases at the microscopic level.3 In this unique space, the integration of scientific cognition and humanistic perception has the most direct and impactful physical carriers. Every “Silent Teacher” is an eternal symbol of dedication and sacrifice;4 every pathological slide seals a personal illness narrative. Ignoring this dimension, morphology teaching will be reduced to pure technical training, deviating from the people-centered foundation of medicine. Therefore, systematically integrating humanities education into experimental teaching is not a dispensable ornament, but a profound return to the essential core of medical education.5
This conceptual pedagogical framework aims to construct a structured and operable teaching model and explore the theoretical and practical pathways of integrating medical humanities into morphological experiment teaching. This study holds that the effective integration of medical humanities into morphology laboratory teaching must rely on three interdependent core pillars to form a comprehensive educational framework.
Integration Path: Construction of the “Trinity” Model for Medical Humanities Integration
To transcend mere emotional appeals or scattered practices, this paper proposes the “Ritual–Narrative–Responsibility” trinity integrated model. It cultivates reverence for life through ritualized practices, builds an empathy bridge to patients’ worlds via narrative medicine, and forges professional responsibility through ethical reflection. The three pillars correspond to affective cultivation, cognitive comprehension, and volitional tempering respectively, jointly shaping students’ professional virtues.
Pillar 1: Ritual – Cultivating Reverence for Life Through Ritualized Practices
Ritual is not empty formalism.6 Anthropological and sociological studies show that a set of fixed symbolic behavioral procedures has strong emotional cohesion and value orientation, which can instantly change the atmosphere, guide participants into a specific psychological state, effectively arouse noble emotions, strengthen collective memory, and convey core values. In the specific context of medical education, solemn rituals are the most intuitive and profound way to convey core concepts such as “life first” and “gratitude for donation” to future physicians.7
Initiation Ritual: Spiritual Baptism on the First Day
When students enter the morphology laboratory for the first time, a brief and solemn collective ritual is held before distributing equipment and explaining rules: all observe a minute of silence to calm their minds, detach from daily disturbances, and enter a space for thinking about the essence of life. The instructor delivers a carefully prepared speech in a calm, solemn and sincere tone.
Example Instructor Address:
Dear students, we are about to start the exploration of the human body in this special space. Always remember: what lies before us is never inanimate matter or silent objects. Every Silent Teacher was once a vibrant life, with thoughts, emotions and stories just like us. They transcended cultural barriers to make the brave and noble decision of donation, dedicating their bodies as the foundation of our learning. They are the first guides leading us into the palace of medicine. From today on, may every precise dissection and every careful observation be filled with the deepest respect—this is the only legitimate response to this ultimate gift.
All participants bow three times to the Silent Teachers and pioneers who donated their bodies for medical progress.8,9 This ritual aims to lay an ethical foundation for the entire course and internalize “gratitude and respect” as the primary norm of laboratory culture.
Daily Tribute: Integrating Reverence into Every Observation
Before each histological or pathological experiment, a brief guiding session is arranged to pay tribute to the tissue slides to be used.
Example Instructor Address:
Today you will observe the myocardial tissue of a patient who fought against heart failure for a long time. His disease course has deepened our understanding of myocardial remodeling. Please observe with inquiry and compassion, for every fibrosis here records the last efforts of a heart to sustain life.
Normalizing the tribute aims to avoid emotional attenuation caused by “one-time rituals”, continuously remind students of the humanistic origin behind learning materials, and embed reverence into the fabric of learning.
Farewell Ceremony: Completing the Gratitude Loop and Passing the Spiritual Torch
After the completion of systematic anatomy and other courses, a formal and solemn “Farewell Ceremony” is held, including flower offering, recitation of commemorative poems, and sharing of insights and oaths by student representatives. It aims to draw a successful conclusion to the dedication of the Silent Teachers, provide students with a formal channel to express gratitude, serve as a coming-of-age ceremony to confirm their medical identity, and inspire them to repay this gift with benevolent medical skills in the future.10
Pillar 2: Narrative – Inspiring Empathy Through Life Stories
Empathy, the ability to understand others’ subjective worlds and respond emotionally, is the cornerstone of healing relationships and has healing power in itself. Medical practices without empathy, no matter how technically proficient, are still cold, objectified and alienated. Morphology teaching should take the initiative to undertake the responsibility of cultivating this key ability in the early stage, rather than delaying it entirely to clinical training.11,12
Endowing Slides with Life: Constructing Clinical Background Stories
When explaining any pathological slide, efforts are made to provide a fictional but medically reasonable and substantial “clinical background story”.
Example 1 (Liver Cirrhosis Slide): In addition to explaining fibrous septa and regenerative nodules, a narrative is added:
This patient was a 50-year-old engineer under long-term high work pressure. He might have ignored physical warnings due to his perseverance. These extensively hyperplastic fibrous tissues, like cages inside the liver, restrict hepatocyte function. His later years might have been spent suffering from severe ascites, persistent pruritus, and intermittent confusion. His once meticulous mind was trapped by a failing liver.
Example 2 (Atherosclerosis Slide): While analyzing plaques, the narrative continues:
The owner of this plaque might be a retired teacher who loved delicious food. This ‘lipid core’ in her artery is a silent volcano, accumulating over decades. Finally, on an ordinary morning preparing breakfast for her grandchildren, the plaque ruptured, thrombosis formed, and the radiance of life faded away. That unfinished breakfast became an eternal memory for her family.
Such narratives aim to pierce the veil of technology, connect abstract pathological changes with specific personal life experiences, emotions and sufferings, and turn knowledge acquisition into an experience filled with humanistic warmth and memory.13,14
Transformation of Questioning Paradigm: From Cognitive Assessment to Empathy Awakening
Fundamentally transform classroom questioning methods, shifting from pure cognitive identification to reflective inquiries that trigger deep empathy.
Traditional Paradigm: What is this structure? What are the diagnostic criteria?
Empathetic Paradigm: For emphysema slides:
Imagine how laborious every exhalation is for him, like squeezing a lifeless bellows. How did his life change from being agile to being breathless even during simple actions such as dressing and eating?
For invasive breast cancer slides:
For this woman, surgery removes not only the diseased organ, but also her body image, female identity and social confidence. Beyond pursuing cure, how should our medical care comprehensively care for her injured soul and life in the future?15,16
“Life Diary” Reflective Writing: In-Depth Self-Dialogue
For key modules, assign reflective writing tasks such as “life diary” or “situational narrative” to replace part of traditional descriptive reports. Examples: “Write a diary from the perspective of this cirrhosis patient” “Draft a professional and warm informed letter to the patient’s family as the attending physician”.
This embodied learning practice is designed to force students to step out of the role of cold observers, attempt to enter others’ life experiences and inner worlds, and serve as a feasible approach to cultivating deep empathy and humanistic care.17
Pillar 3: Responsibility – Forging Accountability Through Ethical Reflection
The philosophical connotation of responsibility: Medicine is a profession of prudence. The Hippocratic Oath of “first, do no harm” carries heavy inherent ethical responsibility, which is based on extreme rigor, prudence and humility.18 Morphological diagnosis, especially pathological diagnosis, is known as the “gold standard” for disease judgment, with extremely heavy conclusions that directly determine clinical strategies and patients’ life trajectories.19 Therefore, in morphology teaching, the pursuit of precision itself is regarded as the highest form of humanistic care.
Confronting Uncertainty: Ethical Decision-Making in Diagnostic Gray Zones
In teaching design, diagnostic gray zones, atypical cases and easily misdiagnosed slides are deliberately selected as core teaching materials. For instance, students are shown difficult slides requiring differentiation between reactive lymphoid hyperplasia and low-grade malignant lymphoma. After group discussions and debates, real or simulated cases are introduced—such as a young patient misdiagnosed in an outside hospital, suffering tremendous psychological pressure and nearly receiving overtreatment, and finally diagnosed correctly after expert re-examination. This guides discussions around core questions:
When microscopic evidence is ambiguous and clinical pressure demands a clear conclusion, how should a responsible pathologist choose?
Through this process, students are guided to refine several key principles: the courage to acknowledge diagnostic limitations—in scientific practice, being honest about uncertainty is more professionally ethical than forcing wrong conclusions; collaborative accountability—timely initiating in-hospital consultations or seeking external expert opinions, with collective wisdom being the strongest guarantee against individual cognitive bias; rational application of auxiliary examinations—recommending and adopting techniques such as immunohistochemistry and molecular detection to obtain objective evidence; prudent practice—objectively describing morphological findings in pathological reports, clearly listing differential diagnoses, and avoiding deterministic statements that may be misleading.
Deconstructing the “Gold Standard”: Revealing the Sacred Process of Pathological Reporting
This teaching method systematically displays the comprehensive and rigorous multi-step process from specimen reception to final report issuance: source verification—strict dual verification of specimens and application forms to ensure absolute accuracy; standardized processing—strict implementation of procedures and quality control for fixation, tissue processing, embedding, sectioning and staining; initial diagnosis—completion of morphological descriptions by residents or junior physicians; hierarchical review—systematic revision and confirmation by senior pathologists; dual-signature system—all malignant and major diagnoses are co-signed by at least two senior pathologists to achieve collective supervision and shared responsibility; permanent archiving—long-term safe storage of slides, wax blocks and reports for subsequent re-examination and research. Ultimately, through this structured process, the core concept is conveyed to students: every pathological report not only carries a rigorous quality assurance system, but also embodies the accountability of the medical community, reflecting profound respect for patients’ well-being and the ethical weight of diagnostic medicine.
Building a Safety Culture: Wisdom and Courage to Learn from Mistakes
Create a “blame-free” classroom atmosphere to analyze diagnostic errors openly and honestly. Carry out “error analysis workshops”, select classic misdiagnosed cases, guide students to analyze root causes (knowledge gaps, cognitive biases, negligence, communication failures?), and jointly design systematic “safety nets” to prevent recurrence. This model aims to cultivate a scientific view of errors—the real failure is not making mistakes, but failing to learn from them; establish a modern medical quality and safety culture prioritizing “system safety” over “individual error-free”.
Implementation Blueprint and Support System
Detailed Implementation Blueprint
To ensure the model is reproducible, operable and easy to promote in practical teaching, a detailed implementation blueprint with clear operational specifications is formulated, covering core links of the three pillars, implementation details, supporting resources and supporting arrangements. The specific contents are shown in (Table 1), which clarifies the operational standards of each link to avoid randomness in teaching implementation and ensures the stable landing of the humanistic integration teaching model.
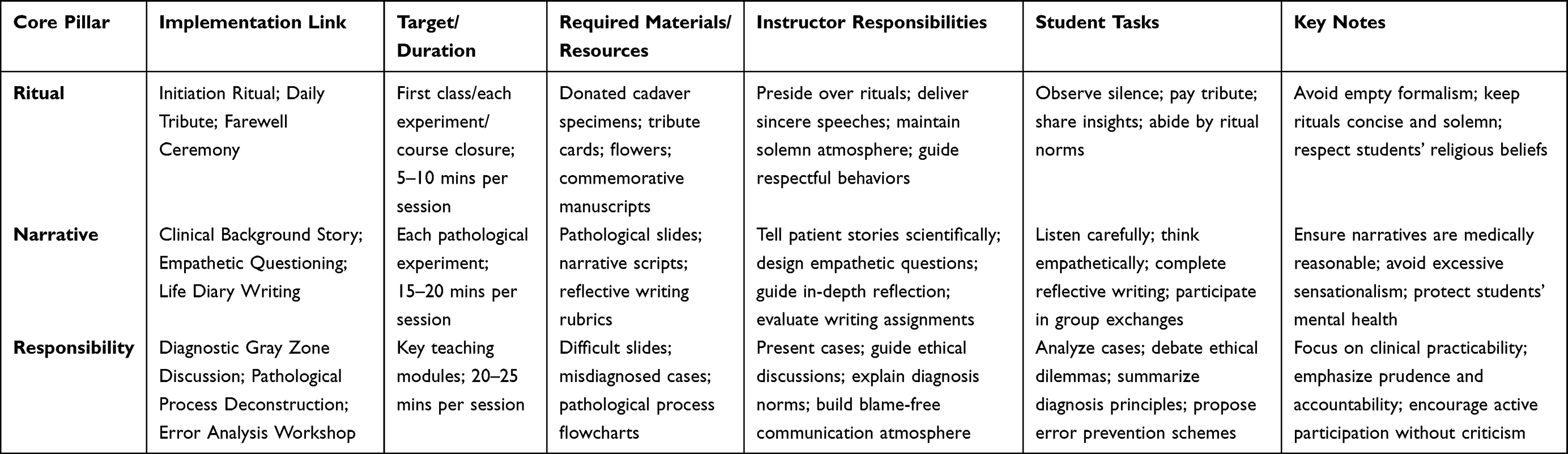 |
Table 1 Implementation Blueprint for the “Ritual-Narrative-Responsibility” Framework |
This implementation blueprint takes into account the actual teaching scenarios of morphology laboratories, balances humanistic education objectives and classroom teaching efficiency, and provides clear operational guidelines for teachers to carry out related teaching activities, which is convenient for flexible adjustment according to class scale, curriculum schedule and student characteristics.
Multidimensional Evaluation Framework
To prevent humanities education from becoming superficial, core humanistic elements are directly embedded into the evaluation system to form a sustainable positive reinforcement cycle.20 A balanced multidimensional evaluation framework combining formative and summative evaluation is proposed (this is a theoretical evaluation design without empirical data support). Formative Evaluation (50% of the total score): Classroom humanistic participation (15%)—assessed based on demeanor in rituals, quality and depth of ethical discussions, and attitude towards caring for specimens and equipment; Reflective writing (20%)—scored according to the sincerity, ideological depth and humanistic insights of assignments such as “life diaries”; Group case analysis reports (15%)—based on the quality of collaborative analysis and rationality of schemes. Summative Evaluation (50% of the total score): A humanities module is set in the final exam, adopting specific question types such as essay questions—“Combined with specific experiences in this course, discuss the profound impact of the “Silent Teacher” on the formation of your professional values” and situational analysis questions presenting clinical pathological ethical dilemmas, requiring students to integrate medical knowledge with humanistic and ethical principles.
Fundamental Transformation of Teacher Roles and Team Building
The deep integration of medical humanities into the curriculum fundamentally depends on teachers. Teachers themselves must be true believers, consistent practitioners and effective communicators of humanistic spirit.21
Firstly, teach by example: instructors’ gentle handling of specimens, compassionate tone when telling patients’ sufferings, and patience in answering students’ questions collectively constitute the most powerful humanities education—actions speak louder than words. Secondly, deliberate capacity building: teachers should actively learn narrative medicine, medical ethics and medical history, deepen their own understanding, and improve their ability to guide students in meaningful dialogues and critical reflections. Finally, build a departmental collaborative culture: regularly hold teaching seminars, share excellent resources and cases of humanities teaching, jointly solve teaching difficulties, and ultimately form a mutual aid community that upholds and advances the humanistic mission of medical education.
Discussion
Conceptual Coherence and Educational Value
The systematic integration of medical humanities into morphological experiment teaching represents a profound paradigm shift, requiring a redefinition of the laboratory: it is not only a space for knowledge transmission but also a field for character forging. Through the synergy of the three pillars of “Ritual–Narrative–Responsibility”, this model strives to imprint a distinct humanistic mark at the starting point of medical students’ professional lives. When future physicians can seamlessly integrate technical precision with artistic empathy, and scientific judgment with ethical prudence, they will bring not only disease cure but also life solace. This is a lofty goal that all medical educators should unremittingly pursue.
Limitations of the Study
As a conceptual framework and teaching model study, this paper has not carried out systematic empirical verification, and has multiple limitations that need to be clarified. Firstly, feasibility constraints: the implementation of ritualized practices, narrative teaching and ethical discussions increases class hours and faculty workload, facing promotion pressure in large-class teaching and tight curriculum schedules. Secondly, cultural variability: differences in regional cultures, institutional traditions and student groups may affect the adaptability of the model, requiring localized adjustment. Thirdly, student resistance risks: some students may hold a utilitarian view of medical learning, showing resistance to humanistic links and reducing the implementation effect. Fourthly, emotional distress risks: cadaver dissection and disease narrative teaching may trigger negative emotions such as anxiety and depression in individual students, requiring supporting psychological counseling mechanisms and voluntary participation options. Fifthly, lack of empirical support: this paper only constructs a theoretical framework and implementation pathways, without collecting empirical data such as student empathy scale scores, professional identity assessments and teaching feedback; claims regarding the model’s effectiveness are theoretical propositions, not empirically validated conclusions, and cannot confirm causal relationships between the model and humanistic literacy improvement.
Future Research Directions
Follow-up research can be carried out in two aspects: if transforming into an empirical study, supplement the model development process based on theoretical grounding and literature synthesis, clarify participant characteristics and institutional contexts, formulate a detailed implementation protocol, adopt a pre-post test mixed-methods evaluation design, select validated scales (such as JSPE) to measure empathy and professional identity, formulate a data analysis plan, and obtain ethical approval.22 If maintaining the conceptual framework positioning, optimize the implementation blueprint, add a logic model (inputs–activities–outputs–outcomes), strengthen the integration of classic medical education theories such as professional identity formation, hidden curriculum and transformative learning, and discuss the contextual transferability of the model.
Conclusion
This paper proposes and constructs a conceptual framework and teaching model for integrating medical humanities into morphological experiment teaching, with “Ritual–Narrative–Responsibility” as the core pillars, focusing on cultivating life reverence, empathy and professional responsibility. This model promotes the transformation of morphological teaching from pure skill training to life-oriented education, guiding students to focus on the complete “person” while exploring pathological morphology. As a theoretically grounded conceptual pedagogical exploration, this model has not been empirically validated, and its actual effectiveness remains to be tested by subsequent teaching practice and empirical research. It provides a referable implementation path for the integration of medical humanities and morphological experiment teaching, and contributes to the return of medical education to its humanistic essence.
Funding
This work was supported by the Special Topic of Laboratory Management of 1. Jiangnan University: Construction of Digital Slice Library Based on Pathological Specimens (JDSYS202223); 2. Jiangnan University Graduate Online Course: Advanced Pathology (YJSZXKC22-029); 3. Jiangnan University Graduate Education and Teaching Reform Research and Practice Project (YJSJGZD24-004); 4. Jiangsu Province Degree and Graduate Education and Teaching Reform Project (JGKT25-C068).
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Smydra R, May M, Taranikanti V, Mi M. Integration of arts and humanities in medical education: a narrative review. J Cancer Educ. 2022;37(5):1267–8. doi:10.1007/s13187-021-02058-3
2. Axelrod C, Brenna CT, Gershon A, Peterkin A, Nyhof-Young J. The companion curriculum: medical students’ perceptions of the integration of humanities within medical education. Can Med Educ J. 2023;14(2):119–124. doi:10.36834/cmej.72907
3. Wong LP, Alias H, Tan SL, Saw A. Conduct of body donation and cadaveric dissection training during the COVID-19 pandemic: challenges, impacts and mitigation. Anat Sci Int. 2023;98(4):558–565. doi:10.1007/s12565-023-00723-9
4. Lai HL, Perng SJ, Huang CY. Nursing students’ perceptions of a silent mentor program in an anatomy course. Anat Sci Educ. 2019;12(6):627–635. doi:10.1002/ase.1863
5. Guo K, Luo T, Zhou LH, et al. Cultivation of humanistic values in medical education through anatomy pedagogy and gratitude ceremony for body donors. BMC Med Educ. 2020;20(1):440. doi:10.1186/s12909-020-02292-1
6. Lee SY, Sasaki S, Kurokawa H, Ohtake F. The school education, ritual customs, and reciprocity associated with self-regulating hand hygiene practices during COVID-19 in Japan. BMC Public Health. 2022;22(1):1663. doi:10.1186/s12889-022-14012-z
7. Evans DJR, Pawlina W. Effects of Covid-19: the need to assess the real value of anatomy education. Anat Sci Educ. 2021;14(2):129–131. doi:10.1002/ase.2061
8. Chin KF, Chin TMK, Lee ZY, Tseng GF. Silent mentor programme increases medical students’ empathy levels. Med Educ. 2023;57(11):1128–1129. doi:10.1111/medu.15219
9. Wong LP, Tan SL, Alias H, Sia TE, Saw A. Longitudinal follow-up of death anxiety and psychophysical-symptom experience of participants in the silent mentor program. Omega. 2023;88(1):157–170. doi:10.1177/00302228211043613
10. Chen L, Liu J, Fu L, Guo C, Chen Y. The impact of gratitude on connection with nature: the mediating role of positive emotions of self-transcendence. Front Psychol. 2022;13:908138. doi:10.3389/fpsyg.2022.908138
11. Barker ME, Crowfoot G, King J. Empathy development and volunteering for undergraduate healthcare students: a scoping review. Nurse Educ Today. 2022;116:105441. doi:10.1016/j.nedt.2022.105441
12. Xue M, Sun H, Xue J, et al. Narrative medicine as a teaching strategy for nursing students to developing professionalism, empathy and humanistic caring ability: a randomized controlled trial. BMC Med Educ. 2023;23(1):38. doi:10.1186/s12909-023-04026-5
13. Scott-Conner CEH, Agarwal D. Applications of narrative medicine to surgical education. Am Surg. 2022;88(12):2851–2856. doi:10.1177/00031348211029851
14. Kitta A, Masel EK. Unveiling narrative medicine in palliative care. Ann Palliat Med. 2024;13(4):751–753. doi:10.21037/apm-24-76
15. Turner R, Vallée-Tourangeau F. Challenges of measuring empathic accuracy: a mentalizing versus experience-sharing paradigm. Br J Soc Psychol. 2023;62(2):972–991. doi:10.1111/bjso.12612
16. Kaldjian LC. Communication about medical errors. Patient Educ Couns. 2021;104(5):989–993. doi:10.1016/j.pec.2020.11.035
17. Doukas DJ, Ozar DT, Darragh M, de Groot JM, Carter BS, Stout N. Virtue and care ethics & humanism in medical education: a scoping review. BMC Med Educ. 2022;22(1):131. doi:10.1186/s12909-021-03051-6
18. Sioutis S, Reppas L, Bekos A, Limneos P, Saranteas T, Mavrogenis AF. The hippocratic oath: analysis and contemporary meaning. Orthopedics. 2021;44(5):264–272. doi:10.3928/01477447-20210819-08
19. Talbert ML, Ashwood ER, Brownlee NA, et al. Resident preparation for practice: a white paper from the College of American Pathologists and Association of Pathology Chairs. Arch Pathol Lab Med. 2009;133(7):1139–1147. doi:10.5858/133.7.1139
20. Isaac M. Role of humanities in modern medical education. Curr Opin Psychiatry. 2023;36(5):347–351. doi:10.1097/YCO.0000000000000884
21. Sweeney CD. DAISY faculty: role modeling compassion for the next generation of nurses. J Nurs Adm. 2019;49(3):113–115. doi:10.1097/NNA.0000000000000721
22. Spatoula V, Panagopoulou E, Montgomery A. Does empathy change during undergraduate medical education? - A meta-analysis. Med Teach. 2019;41(8):895–904. doi:10.1080/0142159X.2019.1584275
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.