")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
The Role of the Multidisciplinary Health Care Team in the Management of Patients with Systemic Sclerosis
Authors Farina N, Benanti G , De Luca G, Palmisano A, Peretto G, Tomassetti S, Giorgione V , Forma O, Esposito A, Danese S, Dagna L , Matucci-Cerinic M, Campochiaro C
Received 11 December 2021
Accepted for publication 11 April 2022
Published 20 April 2022 Volume 2022:15 Pages 815—824
DOI https://doi.org/10.2147/JMDH.S295478
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nicola Farina,1,2,* Giovanni Benanti,1,2,* Giacomo De Luca,1,2 Anna Palmisano,2,3 Giovanni Peretto,4 Sara Tomassetti,5 Veronica Giorgione,6 Ornella Forma,7 Antonio Esposito,2,3 Silvio Danese,2,8 Lorenzo Dagna,1,2 Marco Matucci-Cerinic,1,9 Corrado Campochiaro1,2
1Unit of Immunology, Rheumatology, Allergy and Rare Diseases, IRCCS San Raffaele Hospital, Milan, Italy; 2School of Medicine, Vita-Salute San Raffaele University, Milan, Italy; 3Unit of Clinical and Experimental Radiology, IRCCS San Raffaele Hospital, Milan, Italy; 4Unit of Cardiac Electrophysiology and Arrhythmology, IRCCS San Raffaele Hospital, Milan, Italy; 5Department of Experimental and Clinical Medicine, Careggi University Hospital, Florence, Italy; 6Molecular and Clinical Sciences Research Institute, Fetal Medicine Unit, Department of Obstetrics and Gynaecology, St. George’s University Hospitals NHS Foundation Trust, London, UK; 7Vulnology Nursing Service, IRCCS San Raffaele Scientific Institute, Milan, Italy; 8Unit of Gastroenterology and Endoscopy, IRCCS San Raffaele Hospital, Milan, Italy; 9Department of Experimental and Clinical Medicine, University of Florence and Division of Rheumatology AOUC, Florence, Italy
*These authors contributed equally to this work
Correspondence: Corrado Campochiaro, Unit of Immunology, Rheumatology, Allergy and Rare Diseases, IRCCS San Raffaele Hospital, Via Olgettina 60, Milan, 20132, Italy, Tel +39 0226437060, Fax +39 0226433729, Email [email protected]
Abstract: Systemic sclerosis (SSc) is a rare connective tissue disease characterised by immune dysfunction, vascular damage and fibrosis affecting the skin and multiple internal organs. The clinical spectrum of SSc is wide and its manifestations may lead to severe morbidity and mortality, in addition to a great impact on patients’ quality of life. Due to the multifaceted clinical manifestations of SSc, its management requires a combined expertise of different medical specialists to guarantee an adequate disease control and prevent organ complications. Multi-disciplinary teams (MDT), which are composed by physicians and other specialized health professionals, represent therefore a key element for the comprehensive management of SSc patients. Moreover, MTD can improve communication and patients’ empowerment while the presence of dedicated nurses can help patients to ask questions about their condition. The scope of this narrative review is to analyse the available evidences regarding the role of MDT in the management of SSc patients, and how this holistic approach may improve different disease domains and the overall prognosis. MDT regarding the cardiovascular and lung complication are the more represented in literature, given the great impact in prognosis. Nonetheless, MDT have been shown to be fundamental also in other disease domains as they can intercept early manifestations, thus stratifying patients based on the individual risks in order to personalize patients’ follow-up. MDTs may also minimize the treatment delay, enabling fast-track specialist referral. On the other hand, there are few trials specifically studying MDT in SSc and several authors have highlight the lack of standardization.
Keywords: systemic sclerosis, scleroderma, multidisciplinary team, shared management
Introduction
Systemic sclerosis (SSc) is a rare connective tissue disease characterised by immune dysfunction, vascular damage and fibrosis affecting the skin and multiple internal organs, such as the cardiovascular and respiratory systems.1 The clinical spectrum of SSc is wide and its manifestations may lead to severe morbidity and mortality, in addition to a great impact on patients’ quality of life.2
In the last decades, the therapeutic algorithm of SSc has broadened to encompass a combination of immunomodulatory and vasodilatative drugs along with non-pharmacological measures, with beneficial effects on survival rates and morbidity.3,4
Due to the multifaceted clinical manifestations of SSc, its management requires, in addition to rheumatologic care, the combined expertise of different medical specialists to guarantee an adequate disease control and prevent its complications (Figure 1).3 Multi-disciplinary teams (MDT) are composed of rheumatologists and other specialists and comprise both physicians and other health professionals, such as specialised nurses and physical therapists. MDT’s members can effectively deal with several aspects of the disease that impact on SSc patients’ prognosis and quality of life,5 improving communication and patients’ empowerment.6 Moreover, the presence of dedicated nurses helps patients to feel free to ask questions about their condition.7
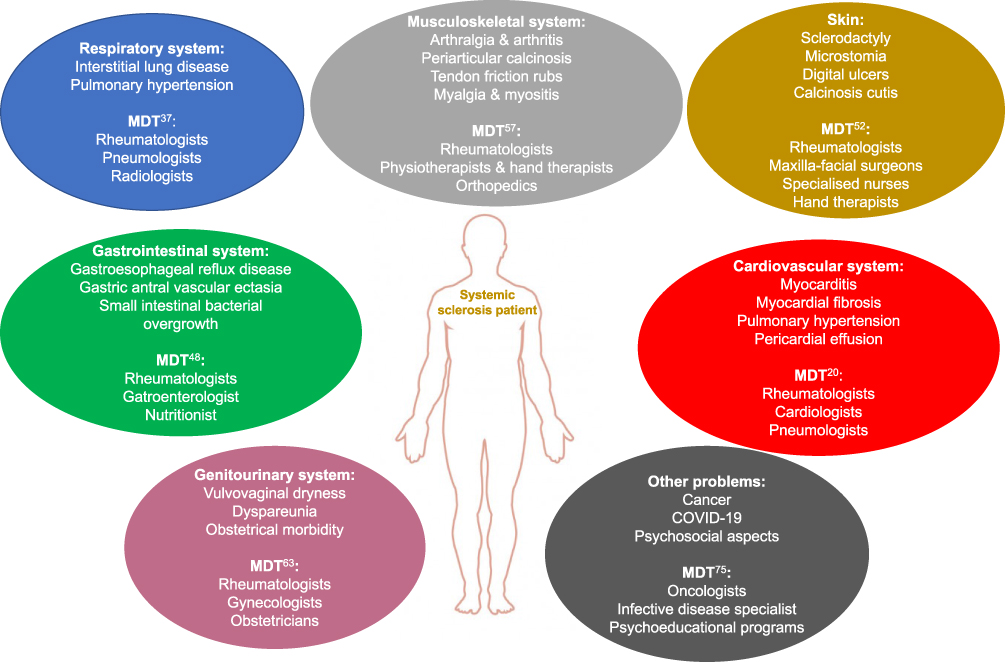 |
Figure 1 Different clinical domains of systemic sclerosis and a suggested multidisciplinary approach. Abbreviation: MDT, multidisciplinary teams. |
The scope of this narrative review is to analyse the available evidence regarding the role of MDT in the management of SSc, and how this holistic approach may improve different disease domains and the overall prognosis.
Cardiovascular System
Cardiovascular involvement is one of the most severe clinical manifestations of SSc, as it may complicate the disease course in both limited and diffuse cutaneous subsets.8 Heart involvement is one of the leading cause of death and a poor prognostic factor in SSc.9 Myocardial involvement is mainly characterized by immune-mediated inflammation, microvascular dysfunction, and progressive evolution toward fibrosis. Myocardial inflammatory-mediated damage10 was reported in up to 12% of SSc patients in cardiac magnetic resonance (CMR) series, but this prevalence is believed to be underestimated11 for limited sensitivity of conventional STIR sequences in the assessment of chronic oedema and a limited number of study adopting new mapping technique able to detect subtle oedema.
In parallel to immune-mediated myocardial inflammation, SSc-related endothelial dysfunction can independently promote collagen deposition through defects in micro-perfusion and thus lead to myocardial fibrosis (found in up to 60% of SSc).10
Myocardial fibrosis is usually asymptomatic, however it may lead to cardiac arrhythmias, which further complicate the disease course in up to 50% of SSc patients.12
Furthermore, in some SSc cases the increase of pulmonary vessels resistance for lung involvement, leads to pulmonary hypertension with increased right ventricular afterload and higher risk of right heart failure.13 Moreover, atherosclerosis contributes to increasing cardiovascular risk.14 Additionally, beside direct myocardial involvement, echocardiography shows subclinical pericardial effusion in up to 43% of SSc patients.15
In SSc, the clinical relevance of cardiologic manifestations requests the presence of a MTD composed of Rheumatologists and Cardiologists to guarantee an appropriate care and follow-up.16 In this scenario, a screening programme, with periodical imaging, clinical and biochemical evaluation, may allow an early detection of heart disease both at baseline and follow-up. In fact, the identification of SSc patients with high risk profile for the development of cardiomyopathy is very important. Male gender, an age at onset greater than 65 years, positive serology (anti-topoisomerase, anti-RNA polymerase anti-Ku, anti-Histone and anti-U3-RNP, anti-heart and anti-intercalated disk), and certain clinical manifestations (diffuse cutaneous and lung involvement, digital ulcers, tendon friction rubs, myositis) should prompt the rheumatologist to periodically screen patients for cardiac involvement.8
Laboratory screening for heart involvement in SSc relies on the measurement of levels of brain natriuretic peptide, troponin, and creatine kinase.17 Likewise, ECG and echocardiography are pivotal for the early identification of cardiac complication of this disease.16 Indeed, both these approaches – while being widely available and inexpensive – are far from being as sensitive and specific as more invasive techniques such as CMR and endomyocardial biopsy.11,17 These diagnostic tools should therefore be performed to confirm heart involvement in SSc patients when screening tests suggest so.18,19
In the 2017 consensus of the UK SSC Study group, Bissell et al16 suggested that blood tests should be performed annually in all SSc patients, while the periodicity should be reduced to six-month in symptomatic and at-risk patients, together with a cardiological evaluation. Additionally, an annual screening for coronary artery disease is recommended for high-risk patients requiring CT coronary angiogram and, if needed, coronarography.
Indeed, some red flags (dyspnoea, orthopnoea, limb oedema) should be carefully assessed in SSc patients as they may indicate the presence of heart failure, and to prevent its evolution patients should be instructed by the MDT to report as soon as possible these signs and symptoms.16
The importance of a dedicated MDT in the management of cardiac manifestations in SSc patients is supported by the experience of Spinella et al.20 They reported that a cardio-rheumatologic MDT led to an easier and faster access to a further cardiologic diagnostic study of SSc patients. In their case, the first cardiologic evaluation was performed within 10 days from the initial request and second- and third-level examinations were guaranteed within 25 days. This multidisciplinary approach may therefore lead to the timely identification and management of cardiologic manifestations of SSc.
Cardiovascular involvement is one of the major causes of death in SSc. A strict collaboration with cardiologists and cardiac-radiologists is of fundamental importance for a prompt diagnosis and for establishing an adequate therapeutic program.
Respiratory System
Lung disease can be detected in over 40% of SSc patients9 and its major clinical manifestations are pulmonary arterial hypertension (PAH) and interstitial lung disease (ILD). Both PAH and ILD are included in the 2013 ACR/EULAR SSc classification criteria.21
Pulmonary hypertension (PH), present in 10% of SSc patients,22 is defined by a mean pulmonary artery pressure equal or higher than 20 mmHg at right heart catheterisation (RCH).13 The most common pathogenic mechanisms that may lead to PH in SSc patients are represented either by pulmonary arterial vasculopathy (PAH) and ILD-related PH. Sometimes multiple mechanisms are overlapping, and a precise phenotype identification is impossible.23 However, PAH is rather frequent in SSc patients, as they represent up to one-third of all PAH patients.24 PAH is defined by a pulmonary artery wedge pressure less than or equal to 15 mmHg and a pulmonary vascular resistance higher than 3 WU without other cause of pre-capillary pulmonary hypertension.23
While PAH may be clinically silent, it can manifest itself with dyspnoea, fatigue, syncope and right ventricular failure. When compared to idiopathic PAH, SSc patients with PAH have a worse prognosis.25 While RHC represents the gold standard for PAH diagnosis, echocardiography is a useful tool if routinely performed because it may lead to an early identification of increased pulmonary arterial pressure and right heart dysfunction, thus prompting RHC evaluation. Additionally, the presence of an isolated reduction in diffusion capacity of carbon monoxide (DLCO) with a reduced ratio of DLCO to alveolar ventilation, is suggestive for PAH. For this reason, pulmonary function tests should be implemented in the evaluation of SSc patients along with echocardiography to screen for PAH.18,26,27 Serum brain natriuretic peptide should also be measured as a rise in its levels also suggests the presence of increased pulmonary arterial pressure.18 Concentrations of troponin and uric acid should be tested as well, since they might be elevated in this clinical scenario.28,29
At autopsy, ILD is present in up to 70% of SSc patients,30 being more frequent in the diffuse cutaneous subset (prevalence 50%) than in the limited one (35%).31 Older age at onset, recent disease onset, ethnicity and positive anti-Scl-70/anti-topoisomerase I antibody are well-known risk factors for ILD development.32
In these cases, lung biopsies show non-specific interstitial pneumonia pattern in the majority of cases, with a minority of usual interstitial pneumonia. Correlation of specific histopathologic subsets with prognosis and treatment response remains unclear. In general, fibrotic SSc-ILDs carries the worst prognosis, whereas cellular and inflammatory features correlate with a better response to immunomodulatory treatment, with the organizing pneumonia pattern showing the best treatment response. Other common histopathologic features include microvascular injuries and abundance of myofibroblasts.33 In SSc, ILD leads to a progressive functionally restrictive pattern (ie reduction of total lung and forced vital capacity), along with a reduction in the diffusion capacity of DLCO that is usually associated with a normal ratio to alveolar ventilation.34 These patients typically present with progressive dyspnoea and non-productive cough, even though, if left untreated, they can progress to respiratory failure and death.35
In the early phase of SSc, ILD diagnosis can be challenging due to the lack of specific symptoms, this is why a recent European consensus agreed on the application of chest high-resolution computed tomography (HRCT) as the gold standard for SSc-ILD diagnosis.36 While pulmonary function tests still represent a useful and non-invasive tool to evaluate patients with SSc both at baseline and during follow-up, they do not identify lung involvement in a significant proportions of cases.37 Hence, HRCT has increasingly become a pivotal part of the screening for ILD even in early and asymptomatic cases of SSc, especially if risk factors are present.37 Nevertheless, in order to reduce radiation exposure and to obtain functional information, other tools including pulmonary function tests, 6 minutes walking test, and patients reported outcomes questionnaires are still recommended in the follow-up of SSc patients.38 Interestingly, the use of HRCT with high increment and reduced number of slices has been proven to accurately identify SSc-ILD while exposing patients to very low doses of radiations when compared to traditional CT studies.39,40 This innovative approach is very sensitive - especially in young SSc patients - and might lead to a wider implementation of radiological ILD screening.
The treatment of this severe manifestation usually requires immunosuppressive therapy so to prevent the progression to pulmonary fibrosis and respiratory failure.34 In fact, the presence of ILD is linked to early mortality in SSc patients, with 35% of deaths in SSc being accountable to ILD, according to EUSTAR database.9
A shared management of SSc patients by rheumatologists, cardiologists, pneumologists and lung radiologists is pivotal to properly diagnose and treat their vascular and interstitial lung involvement.
An early diagnosis of PAH and ILD is essential to improve treatment response and prognosis. As stated above, newly diagnosed SSc patients should undergo pulmonary function tests with DLCO, HRCT and heart echocardiography so to early detect signs of ILD or PAH. Additionally, measurement of brain natriuretic peptide, troponin and uric acid may help in detecting such complications.23 These investigations should be then performed annually to identify the onset of lung vascular or inflammatory involvement later in the history of the disease. Patients should also be educated to alert clinicians if they experience respiratory symptoms like breathlessness, dyspnoea, decreased exercise tolerance, or peripheral oedema. A periodic evaluation by cardiologists and pneumologists with an expertise in the field of SSc is important to grant an appropriate sensibility when visiting such patients to properly detect cardiopulmonary complications. Along with clinical evaluation, instrumental tests such as echocardiography are often operator-dependent techniques and experienced specialists are therefore required to perform them adequately.27, Furthermore, a fast-track for the execution of third-level tests such as right heart catheterisation and endomyocardial biopsy, is possible only in the context of MDTs.
Lung involvement in SSc can manifest as either ILD or PAH. Chest HRCT represents the gold-standard for SSc-ILD diagnosis whereas RCH is the gold-standard for SSc-PAH diagnosis. MDTs composed of rheumatologists, cardiologists, pneumologists and radiologists with expertise in cardiothoracic imaging are pivotal for the management of SSc patients and are a prerequisite in a modern Scleroderma Clinic.
Gastrointestinal System
Gastrointestinal (GI) manifestations represent a frequent and protean involvement of SSc and are frequently present early in the development of the disease. Upper GI tract oesophageal dysmotility, which typically manifests as gastro-oesophageal reflux disease, is by far the most common GI manifestation as it affects more than 90% of SSc patients.41 Its pathogenesis is linked to neurogenic dysfunction that can be related to either tissue fibrosis or autoantibodies against enteric neurons.42 Such GI complication is associated with a higher risk of developing ILD and can additionally lead to complications like oesophagitis, oesophageal stricture, and adenocarcinoma.
Another upper GI complication that is frequently observed in SSc patients is the gastric antral vascular ectasia, which is characterised by dilated capillary alterations that may lead to bleeding and anaemia.42
In SSc, lower GI tract symptoms such as abdominal distension due the small intestinal bacterial overgrowth due to intestinal dysmotility is frequently observed.
Along with direct GI tissue involvement, SSc can also impair oral hygiene and chewing mechanics through microstomia and xerostomia.43
All these manifestations synergically and negatively impact on the quality of life and the nutrition state of SSc patients.44 As a consequence, one-third of SSc patients are at high risk of malnutrition.45
A combined management of SSc patients by rheumatologists and gastroenterologists is essential to improve GI symptoms.46 Such a cooperation can lead to an early performance of endoscopy and manometry test in patients reporting GI symptoms, so to rapidly diagnose GI dysmotility and subsequently start prokinetic therapies. Furthermore, an early detection of GERD and its complications, such as haemorrhage or cancer, can be life-saving.47,48 Additionally, the presence of a dietitian in the dedicated MDT guarantees an adequate monitoring and correction of the nutritional status of patients, which is a relevant prognostic factor and also impact on patients’ quality of life.44 Indeed, in 2017 Doerflers et al showed in a pilot study that medical nutritional therapy, led by expert dietitians, can improve the nutritional status and, subsequently, the quality of life of SSc patients.45 Likewise, the randomised controlled trial led by Schouffoer et al showed that a weekly intervention by both a nutritional expert, a rheumatologist and a physical therapist was associated with an improvement in parameters such as grip strength, six-minutes-walking-test and HAQ score.49
Gastrointestinal involvement is extremely common in SSc patients and can significantly impact on patients’ quality of life. In order to provide effective diagnostic and therapeutic strategies, a close collaboration with dietary professional and gastroenterologists is highly recommended.
Skin
Skin involvement represents the most paradigmatic clinical manifestation of SSc. Microvascular dysfunction, inflammation and impaired collagen deposition initially determine oedema in the extremities, that typically presents with “puffy fingers”. The other well-known early manifestation of SSc is Raynaud’s phenomenon, an abnormal vasoconstriction of digital arteries and cutaneous arterioles. The early SSc inflammatory phase is followed by progressive skin sclerosis, along with the potential development of digital ulcers. Other frequent cutaneous manifestations in SSc patients are telangiectasias, microstomia and subcutaneous calcinosis.
Beside the important aesthetical consequences of skin sclerosis and vasculopathic changes, severe complications may develop. As stated above, microstomia can lead to severe malnutrition, while super-infection of digital ulcers may lead to amputation and gangrene. A referral to a specialized ulcer clinic is therefore mandatory to adequately manage digital ulcers and to educate patients on how they should implement local management to prevent digital ulcer occurrence and recurrence. Additionally, lipo-filling performed by experienced maxillofacial surgeons may contrast the progression of microstomia and restore normal chewing mechanics along with a significant improvement in terms of aesthetics.50
Skin involvement is the hallmark of SSc. SSc patients are frequently plagues by digital ulcers that require a meticulous attention by specialized DU nurses. Microstomia is also a major issue and it can be managed with lipo-filling procedures by maxillofacial surgeons.
Musculoskeletal System
Joint involvement in patients with SSc is frequent and multifaceted.51 While arthralgia is common, overt inflammatory arthritis is less frequent. Even if resorption of the distal phalangeal joints (acro-osteolysis) is a typical finding in SSc, joint erosions are rare in the absence of overlapping rheumatoid arthritis.51 Of note, limitation of joint mobility may also develop as a result of fibrosis around articular structures and may be associated with tendon friction rubs, which represent a negative prognostic factor in patients with SSc (especially for what concerns the development of scleroderma renal crisis).52 Likewise, dystrophic periarticular and intra-articular calcifications greatly impact on quality of life of patients as they may significantly impair range of movement.53
Muscle weakness and myalgia in SSc may result from either inflammation, fibrosis, or both.54 Measurement of creatine-kinase, troponin, aldolase, and lactate dehydrogenase is pivotal in newly diagnosed SSc patients and during follow-up to detect myositis, which should be then confirmed with electromyography and MRI.
A shared approach with rheumatologists, physiotherapists and hand therapists is paramount to improve function of affected joints and muscles. Indeed, pharmacological therapy (ie, anti-malarials and immunosuppressants) may not always lead to function restoration, especially when in the absence of overt inflammation. Targeted exercises are therefore pivotal to improve quality of life of patients.55,56 Furthermore, orthopedic surgeons may intervene in case of extensive periarticular fibrosis and calcifications to improve joint mobility and pain.
Genital System and Pregnancy
The extent of the SSc impact on sexual and reproductive activities of patients is wide. Gynaecologic symptoms, including vulvovaginal dryness and dyspareunia, are common in SSc and can greatly affect patients’ quality of life.57 In addition to the impact on intercourse, urogenital involvement can also lead to genital infections from bacteria or Candida Albicans. From reproductive points of view, conflicting findings in pregnancy rates have been reported among women with SSc. However, when pregnancy starts, SSc bears significant obstetrical consequences, as shown by a recent meta-analysis reporting an increased frequency of miscarriages, fetal growth restriction, preterm deliveries and newborns with low birth weight in SSc patients.58 Moreover, severe skin fibrosis might cause difficulties in delivery. Nonetheless, SSc seems to remain stable throughout pregnancy.
Hence, women affected by SSc need both gynaecological care and a careful pregnancy planning and monitoring. As far as the obstetrical management is regarded, it is advisable to conceive the baby only when disease is in a stable phase, especially in women affected by the diffuse cutaneous form of SSc.59
Of note, EULAR recommendations currently advise to avoid pregnancy in SSc patients with PAH as this complication is associated with a significant pregnancy risk and a maternal mortality up to one third of cases.60 Regardless of the concomitant treatment with teratogenic medications, contraceptives should be prescribed in SSc-PAH patients, if not contraindicated.
Pharmacological therapies must be modified in order to administer only safe drugs during pregnancy, as it is recommended by EULAR guidelines.59 Antimalarials, calcineurin inhibitors and glucocorticoids are safe to use during pregnancy, while methotrexate, mycophenolate mofetil and cyclophosphamide must be withdrawn at least six months before conception as they are teratogenic.59
MDTs of rheumatologist and obstetricians are recommended to best monitor pregnant SSc patients and improve fetal outcome.61 Fetal well-being as well as maternal blood pressure and other signs of cardiopulmonary or renal distress in the mother should be monitored during pregnancy in order to detect disease progression or other obstetrical complications such as pre-eclampsia and fetal growth restriction.
A shared rheumatologist and gynae-obstetrician care is recommended for female SSc patients. Pregnancy planning is of uttermost importance considering the age of onset of SSc.
Systemic Sclerosis and Malignancies
The relationship between SSc and malignant neoplasms is well-known and bi-directional.
Several reports have shown an increased risk of malignancy in patients with SSc.62 The most relevant association appears to be with lung cancer, which represents one-third of the malignancies seen in SSc patients.63 However, the cause of an increased cancer risk in SSc is not clear. It has been hypothesized that sites of disease activity may be prone to malignant transformation. On the other hand, SSc may be itself a manifestation of latent cancer, especially in patients with autoantibodies to RNA polymerase III64,65. It has been shown that tumors harbouring somatic mutations in the POLR3A gene may lead to SSc.66 Additionally, cases of SSc induced by immune-checkpoint inhibitors have been described.67
A shared rheumatological-oncological approach is therefore necessary in neoplastic SSc patients, to guarantee an adequate choice of the immunosuppressive therapeutic regimen68 as well as of chemotherapeutic drugs. Furthermore, a thorough screening for occult neoplasms is essential in patients with risk factors and disease characteristics suggestive for the presence of cancer (eg, anti-RNA polymerase III antibodies). Chest X-ray, abdomen ultrasound, and fecal occult blood test should be performed yearly and, if positive, they should prompt second-level investigations (eg, chest and abdomen CT, gastroscopy and colonoscopy). According to age and sex of patients, cervical smear test, mammography, and measurement of prostate specific antigen should also be annually performed.
SSc can be a paraneoplastic disease especially in those with anti-RNA-polymerase III antibody positivity. A neoplastic screening should therefore be carried out in specific SSc patients and a shared rheumatological-oncological care is advisable for neoplastic SSc patients.
Systemic Sclerosis and Psychosocial Aspects
More than 50% of patients with SSc suffers from depression.69 Likewise, fatigue and sleep disturbances are very common in this scenario and significantly impair quality of life.70,71 Furthermore, skin changes and appearance changes are strongly associated with social anxiety and body images distress, and contribute to mood disorders in SSc patients.72 Hence, SSc significantly impacts on quality of life of patients, and psychological aspects of this disease must be addressed by rheumatologists and healthcare professionals trained in clinical psychology. Indeed, patients with SSc have been shown to benefit from psychoeducational programs.73,74 Furthermore, an approach based on MDT per se is associated with an improvement of quality of life.49
Systemic Sclerosis and COVID-19
Recently, coronavirus Disease 19 (COVID-19) pandemic has been a major challenge to global health, having caused more than 5 millions of deaths to date.75 Moreover, COVID-19 has impacted rheumatological patients in several ways. First of all, a continuous clinical assistance could not be guaranteed in all cases because of the great effort hospitals have spent in admitting and treating the large number of COVID-19 patients and this has been particularly true for SSc patients.76–78 Additionally, the outcome of COVID-19 was reported to be worse in severe SSc patients treated with rituximab.79 On the other hand, SARS-CoV-2 infection has been reported to possibly induce SSc progression even in previously clinically stable patients.19
As a consequence, SSc patients have to be educated to respect all the necessary measures to prevent SARS-CoV-2 infection, with a specific focus on vaccination to reduce any vaccination hesitancy.80 Furthermore, a careful monitoring of SARS-CoV-2-infected SSc patients is mandatory to early identify signs of respiratory failure and possible signs of SSc progression, even in the absence of clinically relevant manifestations of COVID-19.19
Conclusions
Systemic sclerosis is a heterogeneous and complex disease which needs a combined approach by different specialists and professional figures to help the rheumatologists to optimise the management and guarantee the best care of patients. Even though data exists about the significant importance of this shared approach in improving SSc outcomes, more controlled data are required to further understand how MTD can positively impact the management of SSc patients and help to tailor the therapeutic algorithm for each patient.
Author Details
These authors equally contributed as first authors: Nicola Farina and Giovanni Benanti.
Disclosure
Sara Tomassetti reports speaker’s fees from Boehringer Ingelheim and Roche. Silvio Danese reports personal fees from AbbVie, Alimentiv, Allergan, Amgen, AstraZeneca, Athos Therapeutics, Biogen, Boehringer Ingelheim, Celgene, Celltrion, Dr Falk Pharma, Eli Lilly, Enthera, Ferring Pharmaceuticals Inc., Gilead, Hospira, Inotrem, Janssen, Johnson & Johnson, MSD, Mundipharma, Mylan, Pfizer, Roche, Sandoz, Sublimity Therapeutics, Takeda, Tigenix, UCB Inc., and Vifor, outside the submitted work. The authors report no other potential conflicts of interest for this work.
References
1. Denton CP, Khanna D. Systemic sclerosis. Lancet. 2017;390(10103):1685–1699. doi:10.1016/S0140-6736(17)30933-9
2. Pagkopoulou E, Arvanitaki A, Daoussis D, Garyfallos A, Kitas G, Dimitroulas T. Comorbidity burden in systemic sclerosis: beyond disease-specific complications. Rheum Int. 2019;39(9):1507–1517. doi:10.1007/s00296-019-04371-z
3. Kowal-Bielecka O, Fransen J, Avouac J, et al. Update of EULAR recommendations for the treatment of systemic sclerosis. Ann Rheum Dis. 2017;76(8):1327–1339. doi:10.1136/annrheumdis-2016-209909
4. Campochiaro C, Allanore Y. An update on targeted therapies in systemic sclerosis based on a systematic review from the last 3 years. Arthritis Res Ther. 2021;23(1). doi:10.1186/s13075-021-02536-5
5. Vliet Vlieland TPM. Multidisciplinary team care and outcomes in rheumatoid arthritis. Curr Opin Rheumatol. 2004;16(2):153–156. doi:10.1097/00002281-200403000-00015
6. Nakayama A, Tunnicliffe DJ, Thakkar V, et al. Patients’ perspectives and experiences living with systemic sclerosis: a systematic review and thematic synthesis of qualitative studies. J Rheumatol. 2016;43(7):1363–1375. doi:10.3899/jrheum.151309
7. Denton CP, Laird B, Moros L, Luis J, Flores L. Things left unsaid: important topics that are not discussed between patients with systemic sclerosis, their carers and their healthcare professionals-a discourse analysis. Clin Rheum. 2021;40(4):1399–1407. doi:10.1007/s10067-020-05371-2
8. Psarras A, Soulaidopoulos S, Garyfallos A, Kitas G, Dimitroulas T. A critical view on cardiovascular risk in systemic sclerosis. Rheumatol Int. 2017;37(1):85–95. doi:10.1007/s00296-016-3530-3
9. Tyndall AJ, Bannert B, Vonk M, et al. Causes and risk factors for death in systemic sclerosis: a study from the EULAR scleroderma trials and research (EUSTAR) database. Ann Rheum Dis. 2010;69(10):1809–1815. doi:10.1136/ard.2009.114264
10. Desai CS, Lee DC, Shah SJ. Systemic sclerosis and the heart: current diagnosis and management. Curr Opin Rheumatol. 2011;23(6):545. doi:10.1097/BOR.0b013e32834b8975
11. Mavrogeni SI, Schwitter J, Gargani L, et al. Cardiovascular magnetic resonance in systemic sclerosis: “Pearls and pitfalls.”. Semin Arthritis Rheum. 2017;47(1):79–85. doi:10.1016/j.semarthrit.2017.03.020
12. Seferovic PM, Ristic AD. Cardiac arrhythmias and conduction disturbances in autoimmune rheumatic diseases. Rheumatology. 2006;45(suppl_4):iv39–iv42. doi:10.1093/rheumatology/kel315
13. Thenappan T, Ormiston ML, Ryan JJ, Archer SL. State of the art review: pulmonary arterial hypertension: pathogenesis and clinical management. BMJ. 2018;360:j5492.
14. Hettema ME, Bootsma H, Kallenberg CGM. Macrovascular disease and atherosclerosis in SSc. Rheumatology. 2008;47(5):578–583. doi:10.1093/rheumatology/ken078
15. Fernández Morales A, Iniesta N, Fernández-Codina A, et al. Cardiac tamponade and severe pericardial effusion in systemic sclerosis: report of nine patients and review of the literature. Int J Rheum Dis. 2017;20(10):1582–1592. doi:10.1111/1756-185X.12952
16. Bissell LA, Anderson M, Burgess M, et al. Consensus best practice pathway of the UK systemic sclerosis study group: management of cardiac disease in systemic sclerosis. Rheumatology. 2017;56(6):912–921. doi:10.1093/rheumatology/kew488
17. Ross L, Moxey J, Nikpour M. Are troponin and B-type natriuretic peptides useful biomarkers for the diagnosis of systemic sclerosis heart involvement? A systematic literature review. Semin Arthritis Rheum. 2021;51(1):299–309. doi:10.1016/j.semarthrit.2020.10.016
18. Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016;37(1):67–119. doi:10.1093/eurheartj/ehv317
19. Campochiaro C, de Luca G, Farina N, et al. Severe acute respiratory syndrome coronavirus-2-induced flare of systemic sclerosis. Scand J Rheumatol. 2022;51(2):156–158. doi:10.1080/03009742.2021.1932582
20. Spinella A, Coppi F, Mattioli AV, et al. Management of cardiopulmonary disease in patients with systemic sclerosis: cardiorheumatology clinic and patient care standardization proposal. J Cardiovasc Med. 2018;19(9):513–515. doi:10.2459/JCM.0000000000000693
21. van den Hoogen F, Khanna D, Fransen J, et al. 2013 classification criteria for systemic sclerosis: an American college of rheumatology/European league against rheumatism collaborative initiative. Ann Rheum Dis. 2013;72(11):1747–1755. doi:10.1136/annrheumdis-2013-204424
22. Young A, Moles VM, Jaafar S, et al. Performance of the DETECT algorithm for pulmonary hypertension screening in a systemic sclerosis cohort. Arthritis Rheuma. 2021;73(9):1731–1737. doi:10.1002/art.41732
23. Launay D, Sobanski V, Hachulla E, Humbert M. Pulmonary hypertension in systemic sclerosis: different phenotypes. Eur Respir Rev. 2017;26(145):145. doi:10.1183/16000617.0056-2017
24. Mcgoon MD, Benza RL, Escribano-Subias P, et al. Pulmonary arterial hypertension epidemiology and registries. J Am Coll Cardiol. 2013;62(25):D51–D59. doi:10.1016/j.jacc.2013.10.023
25. Hoffmann-Vold AM, Allanore Y, Alves M, et al. Progressive interstitial lung disease in patients with systemic sclerosis-associated interstitial lung disease in the EUSTAR database. Ann Rheum Dis. 2021;80(2):219–227. doi:10.1136/annrheumdis-2020-217455
26. Sobanski V, Launay D, Hachulla E, Humbert M. Current approaches to the treatment of systemic-sclerosis-associated pulmonary arterial hypertension (SSc-PAH). Curr Rheumatol Rep. 2016;18(2):1–14. doi:10.1007/s11926-015-0560-x
27. Gargani L, Voilliot D, D’Alto M, et al. Pulmonary circulation on the crossroads between the left and right heart in systemic sclerosis: a clinical challenge for cardiologists and rheumatologists. Heart Fail Clin. 2018;14(3):271–281. doi:10.1016/j.hfc.2018.02.004
28. Xu SL, Yang J, Zhang CF, et al. Serum cardiac troponin elevation predicts mortality in patients with pulmonary hypertension: a meta-analysis of eight cohort studies. Clin Respir J. 2019;13(2):82–91. doi:10.1111/crj.12991
29. Savale L, Akagi S, Tu L, et al. Serum and pulmonary uric acid in pulmonary arterial hypertension. Eur Respir J. 2021;58(2):2000332. doi:10.1183/13993003.00332-2020
30. Mathai SC, Danoff SK. Management of interstitial lung disease associated with connective tissue disease. BMJ. 2016;352. doi:10.1136/bmj.h6819
31. George PM, Wells AU. Disease staging and sub setting of interstitial lung disease associated with systemic sclerosis: impact on therapy. Expert Rev Clin Immunol. 2018;14(2):127–135. doi:10.1080/1744666X.2018.1427064
32. Wells AU, Margaritopoulos GA, Antoniou KM, Denton C. Interstitial lung disease in systemic sclerosis. Semin Respir Crit Care Med. 2014;35(2):213–221. doi:10.1055/s-0034-1371541
33. Silver RM, Wells AU. Histopathology and bronchoalveolar lavage. Rheumatology. 2008;47(Suppl 5):v62. doi:10.1093/rheumatology/ken272
34. Roofeh D, Jaafar S, Vummidi D, Khanna D. Management of systemic sclerosis-associated interstitial lung disease. Curr Opin Rheumatol. 2019;31(3):241. doi:10.1097/BOR.0000000000000592
35. Cottin V, Brown KK. Interstitial lung disease associated with systemic sclerosis (SSc-ILD). Respir Res. 2019;20(1). doi:10.1186/s12931-019-0980-7
36. Hoffmann-Vold AM, Maher TM, Philpot EE, et al. The identification and management of interstitial lung disease in systemic sclerosis: evidence-based European consensus statements. Lancet Rheum. 2020;2(2):e71–e83. doi:10.1016/S2665-9913(19)30144-4
37. Suliman YA, Dobrota R, Huscher D, et al. Brief report: pulmonary function tests: high rate of false-negative results in the early detection and screening of scleroderma-related interstitial lung disease. Arthritis Rheuma. 2015;67(12):3256–3261. doi:10.1002/art.39405
38. Hoffmann-Vold AM, Allanore Y, Bendstrup E, et al. The need for a holistic approach for SSc-ILD - achievements and ambiguity in a devastating disease. Respir Res. 2020;21(1). doi:10.1186/s12931-020-01459-0
39. Frauenfelder T, Winklehner A, Nguyen TDL, et al. Screening for interstitial lung disease in systemic sclerosis: performance of high-resolution CT with limited number of slices: a prospective study. Ann Rheum Dis. 2014;73(12):2069–2073. doi:10.1136/annrheumdis-2014-205637
40. Winklehner A, Berger N, Maurer B, Distler O, Alkadhi H, Frauenfelder T. Screening for interstitial lung disease in systemic sclerosis: the diagnostic accuracy of HRCT image series with high increment and reduced number of slices. Ann Rheum Dis. 2012;71(4):549–552. doi:10.1136/annrheumdis-2011-200564
41. Schmeiser T, Saar P, Jin D, et al. Profile of gastrointestinal involvement in patients with systemic sclerosis. Rheumatol Int. 2012;32(8):2471–2478. doi:10.1007/s00296-011-1988-6
42. Sallam H, McNearney TA, Chen JDZ. Systematic review: pathophysiology and management of gastrointestinal dysmotility in systemic sclerosis (scleroderma). Aliment Pharmacol Ther. 2006;23(6):691–712. doi:10.1111/j.1365-2036.2006.02804.x
43. Alantar A, Cabane J, Hachulla E, et al. Recommendations for the care of oral involvement in patients with systemic sclerosis. Arthritis Care Res. 2011;63(8):1126–1133. doi:10.1002/acr.20480
44. Harrison E, Herrick AL, Mclaughlin JT, Lal S. Review malnutrition in systemic sclerosis. Rheumatology. 2012;51(10):1747–1756. doi:10.1093/rheumatology/kes160
45. Doerfler B, Allen TS, Southwood C, Brenner D, Hirano I, Sheean P. Medical nutrition therapy for patients with advanced systemic sclerosis (MNT PASS): a pilot intervention study. J Parenter Enter Nutr. 2017;41(4):678–684. doi:10.1177/0148607115597883
46. Sakkas LI, Simopoulou T, Daoussis D, Liossis SN, Potamianos S. Intestinal involvement in systemic sclerosis: a clinical review. Dig Dis Sci. 2018;63(4):834–844. doi:10.1007/s10620-018-4977-8
47. Patti MG, Vela MF, Odell DD, Richter JE, Fisichella PM, Vaezi MF. The intersection of GERD, aspiration, and lung transplantation. J Laparoendosc Adv Surg Tech. 2016;26(7):501–505. doi:10.1089/lap.2016.0170
48. Host LV, Campochiaro C, Afonso A, Nihtyanova SI, Denton CP, Ong VH. High proton pump inhibitor exposure increases risk of calcinosis in systemic sclerosis. Rheumatology. 2021;60(2):849–854. doi:10.1093/rheumatology/keaa332
49. Schouffoer AA, Ninaber MK, Beaart-van De Voorde LJJ, et al. Randomized comparison of a multidisciplinary team care program with usual care in patients with systemic sclerosis. Arthritis Care Res. 2011;63(6):909–917. doi:10.1002/acr.20448
50. Virzì F, Bianca P, Giammona A, et al. Combined platelet-rich plasma and lipofilling treatment provides great improvement in facial skin-induced lesion regeneration for scleroderma patients. Stem Cell Res Ther. 2017;8(1). doi:10.1186/s13287-017-0690-3
51. Sandler RD, Matucci-Cerinic M, Hughes M. Musculoskeletal hand involvement in systemic sclerosis. Semin Arthritis Rheum. 2020;50(2):329–334. doi:10.1016/j.semarthrit.2019.11.003
52. Doré A, Lucas M, Ivanco D, Medsger TA, Domsic RT. Significance of palpable tendon friction rubs in early diffuse cutaneous systemic sclerosis. Arthritis Care Res. 2013;65(8):1385–1389. doi:10.1002/acr.21964
53. Devogelaer JP, Huaux JP, Maldague B, Malghem J, Noël H, de Deuxchaisnes CN. Intra-articular calcification in progressive systemic sclerosis. Clin Rheumatol. 1986;5(2):262–267. doi:10.1007/BF02032367
54. Ranque B, Authier FJ, Le-guern V, et al. A descriptive and prognostic study of systemic sclerosis-associated myopathies. Ann Rheum Dis. 2009;68(9):1474–1477. doi:10.1136/ard.2008.095919
55. Varjú C, Pethö E, Kutas R, Czirják L. The effect of physical exercise following acute disease exacerbation in patients with dermato/polymyositis. Clin Rehabil. 2003;17(1):83–87. doi:10.1191/0269215503cr572oa
56. Paik JJ, Wigley FM, Shah AA, et al. Association of fibrosing myopathy in systemic sclerosis and higher mortality. Arthritis Care Res. 2017;69(11):1764–1770. doi:10.1002/acr.23291
57. Impens AJ, Rothman J, Schiopu E, et al. Sexual activity and functioning in female scleroderma patients. Clin Exp Rheumatol. 2009;27(3 Suppl):54.
58. Munira S, Christopher-Stine L. Pregnancy in myositis and scleroderma. Best Pract Res Clin Obstet Gynaecol. 2019;64:59–67.
59. Skorpen CG, Hoeltzenbein M, Tincani A, et al. The EULAR points to consider for use of antirheumatic drugs before pregnancy, and during pregnancy and lactation. Ann Rheum Dis. 2016;75(5):795–810. doi:10.1136/annrheumdis-2015-208840
60. Clark KEN, Etomi O, Ong VH. Systemic sclerosis in pregnancy. Obstetric Med. 2020;13(3):105–111. doi:10.1177/1753495X19878042
61. Miniati I, Guiducci S, Mecacci F, Mello G, Matucci-Cerinic M. Pregnancy in systemic sclerosis. Rheumatology. 2008;47(Suppl 3):iii16–iii18. doi:10.1093/rheumatology/ken174
62. Bonifazi M, Tramacere I, Pomponio G, et al. Systemic sclerosis (scleroderma) and cancer risk: systematic review and meta-analysis of observational studies. Rheumatology. 2013;52(1):143–154. doi:10.1093/rheumatology/kes303
63. Bielefeld P, Meyer P, Caillot D, et al. [Systemic scleroderma and cancers: 21 cases and review of the literature]. La Revue de Med Interne. 1996;17(10):810–813. French. doi:10.1016/0248-8663(96)82683-X
64. Shah AA, Rosen A, Hummers L, Wigley F, Casciola-Rosen L. Close temporal relationship between onset of cancer and scleroderma in patients with RNA polymerase I/III antibodies. Arthritis Rheum. 2010;62(9):2787–2795. doi:10.1002/art.27549
65. Lazzaroni MG, Campochiaro C, Bertoldo E, et al. Association of anti-RNA polymerase III antibody with silicone breast implants rupture in a multicentre series of Italian patients with systemic sclerosis. Clin Exp Rheumatol. 2021;39(4):25–28. doi:10.55563/clinexprheumatol/mg0paj
66. Joseph CG, Darrah E, Shah AA, et al. Association of the autoimmune disease scleroderma with an immunologic response to cancer. Science. 2014;343(6167):152–157. doi:10.1126/science.1246886
67. Terrier B, Humbert S, Preta LH, et al. Risk of scleroderma according to the type of immune checkpoint inhibitors. Autoimmun Rev. 2020;19(8):102596. doi:10.1016/j.autrev.2020.102596
68. Cavalli G, Farina N, Campochiaro C, et al. Repurposing of biologic and targeted synthetic anti-rheumatic drugs in COVID-19 and hyper-inflammation: a comprehensive review of available and emerging evidence at the peak of the pandemic. Front Pharmacol. 2020;11. doi:10.3389/fphar.2020.598308
69. Thombs BD, Taillefer SS, Hudson M, Baron M. Depression in patients with systemic sclerosis: a systematic review of the evidence. Arthritis Rheum. 2007;57(6):1089–1097. doi:10.1002/art.22910
70. Frech T, Hays RD, Maranian P, Clements PJ, Furst DE, Khanna D. Prevalence and correlates of sleep disturbance in systemic sclerosis–results from the UCLA scleroderma quality of life study. Rheumatology. 2011;50(7):1280–1287. doi:10.1093/rheumatology/ker020
71. Bassel M, Hudson M, Taillefer SS, Schieir O, Baron M, Thombs BD. Frequency and impact of symptoms experienced by patients with systemic sclerosis: results from a Canadian National Survey. Rheumatology. 2011;50(4):762–767. doi:10.1093/rheumatology/keq310
72. Malcarne VL, Fox RS, Mills SD, Gholizadeh S. Psychosocial aspects of systemic sclerosis. Curr Opin Rheumatol. 2013;25(6):707–713. doi:10.1097/01.bor.0000434666.47397.c2
73. Mozzetta A, Antinone V, Alfani S, et al. Mental health in patients with systemic sclerosis: a controlled investigation. J Eur Acad Dermatol Venereol. 2008;22(3):336–340. doi:10.1111/j.1468-3083.2007.02426.x
74. Kwakkenbos L, Bluyssen SJM, Vonk MC, et al. Addressing patient health care demands in systemic sclerosis: pre-post assessment of a psycho-educational group programme. Clin Exp Rheumatol. 2011;29(2 Suppl):65.
75. Farina N, Ramirez GA, de Lorenzo R, et al. COVID-19: pharmacology and kinetics of viral clearance. Pharmacol Res. 2020;161:105114.
76. Denton CP, Campochiaro C, Bruni C, Distler O, Iagnocco A, Matucci Cerinic M. COVID-19 and systemic sclerosis: rising to the challenge of a pandemic. J Scleroderma Relat Disord. 2021;6(1):58–65. doi:10.1177/2397198320963393
77. Ferri C, Giuggioli D, Raimondo V, et al. Covid-19 and rheumatic autoimmune systemic diseases: role of pre-existing lung involvement and ongoing treatments. Curr Pharm Des. 2021;27(41):4245–4252. doi:10.2174/1381612827666210903103935
78. Orlandi M, Landini N, Sambataro G, et al. The role of chest ct in deciphering interstitial lung involvement: systemic sclerosis versus covid-19. Rheumatology. 2021. doi:10.1093/rheumatology/keab801
79. Avouac J, Airó P, Carlier N, Matucci-Cerinic M, Allanore Y. Severe COVID-19-associated pneumonia in 3 patients with systemic sclerosis treated with rituximab. Ann Rheum Dis. 2020;80(3):e37.
80. Campochiaro C, Trignani G, Tomelleri A, Cascinu S, Dagna L. Potential acceptance of COVID-19 vaccine in rheumatological patients: a monocentric comparative survey. Ann Rheum Dis. 2021;80(6):816–817. doi:10.1136/annrheumdis-2020-219811
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.