")
Back to Journals » Psychology Research and Behavior Management » Volume 16
The Role of Maternal Personality Organization and of the p Factor in Predicting Parental Distress, the Quality of Parental Care, and Offspring’s Dysregulation Symptoms
Authors Cimino S, Tambelli R, Cerniglia L
Received 27 June 2023
Accepted for publication 5 August 2023
Published 25 September 2023 Volume 2023:16 Pages 3963—3971
DOI https://doi.org/10.2147/PRBM.S423698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Silvia Cimino,1 Renata Tambelli,1 Luca Cerniglia2
1Sapienza. University of Rome. Department of Dynamic, Clinical and Health, Rome, Italy; 2International Telematic university Uninettuno, Faculty of Psychology, Rome, Italy
Correspondence: Luca Cerniglia, International Telematic university Uninettuno, Faculty of Psychology, Corso Vittorio Emanuele II. 39, Rome, 00186, Italy, Tel +39066920761, Email [email protected]
Background: It has been posited that parental distress, the quality of maternal care and offspring’s dysregulation can be predicted by maternal maladaptive characteristics. However, only a few studies have considered mothers’ personality organizations and features of the p factor in mothers as possible predictors of symptoms in their children.
Methods: In a sample of N=524 subjects, this study evaluated the effect of mothers’ personality organization and of the p factor on parental distress, parental care and offspring’s dysregulation symptoms. Mothers filled out the IPO, the ASR, and the PSI-SF; children’s teachers filled out the TRF; children were administered the PBI.
Results: We found that different mother groups (neurotic, borderline, psychotic organization) have distinct impact on parental distress, quality of care, and children’s dysregulation, mediated by the p factor.
Conclusion: This study can contribute to the understanding of the key factors underpinning mothers and children’s psychopathology.
Keywords: personality organization, p factor, parental distress, maternal care, dysregulation
Introduction
Caspi et al posited the presence of a General Psychopathological Factor (p factor) that represents a general vulnerability to psychopathology.1 The implications of the p factor are far-reaching. If all psychopathology is underpinned by a single factor, then this carries significant consequences for our understanding of the nature of mental disorders. It also has implications for treatment, as interventions that target the p factor may be more effective at reducing psychopathology than those that focus on specific disorders. Moreover, it has implications for the mechanisms of transmission of psychopathological risk from parents to their offspring (due to possible shared genetic vulnerability and to children’s exposure to maladaptive environment). In sum, this factor consists of an element of liability to psychopathology, which can be dimensionally different (less or more severe), and that can negatively affect offspring’s emotional/behavioral functioning. Scientific literature has debated about how to measure the p factor as a continuous variable, proposing different solutions.2 One way of measuring it on a continuum from lesser to greater severity has been recently suggested by Cervin et al.3 These authors posited to use the sum of all subscales of Achenbach’s tools joint in one general factor of vulnerability and distress for psychopathology.
Kernberg’s theory of personality organization suggests a correlation between the p factor model and a continuum of personality pathology severity. This continuum encompasses three primary dimensions: Identity, Defense mechanisms, and Reality-testing, which progress from the neurotic level to the borderline level and ultimately to the psychotic level. Considering Caspi’s and Kernberg’s theorizations together, it is possible to suggest that the conventional approach to parent-to-child transmission of psychopathological risk should be evaluated with a focus on personality organization considering a general psychopathological factor, rather than putting emphasis on specific parental psychiatric diagnosis as a risk factor for negative outcomes in offspring.4–6
Some studies have concentrated on the consequences of maternal neurotic, borderline and psychotic personality organization on offspring emotional/behavioral functioning7,8 and it has been posited that children of parents with neurotic personality organization are unlikely to provide psychologically stable home environments and may show anxiety and depression, with higher than normal frequency of separation anxiety, overdependence, and inhibited affectivity.9,10 Parents characterized by borderline personality organization may struggle with constructing and maintaining intense and prolonged bonds with others. So, children can be exposed to frequent changes of mood and behavior experiencing minimal sense of safety and predictability of the world.11 They may also feel the need to fill their parents’ chronic feelings of emptiness and loneliness, developing role-reversing behaviors and psychopathological symptoms such as separation anxiety. Due to the unpredictable environment, children of these mothers may adopt a constant state of hypervigilance and become easily overwhelmed by emotions, which they are unable to self-regulate.12 Parents who have psychotic personality organization tend to be emotionally detached from or too involved with their children. This can lead offspring to be unable to modulate their own and interpersonal emotional distance, with severe negative consequences on their social adaptability. These parents may be abusive and fail to give needed psychological care to their children. This may cause feelings of loneliness and/or anger in offspring.13 Similar to the p factor, literature has proposed several ways of measuring personality organization.14 Cerniglia et al15 suggested using the Inventory of Personality Organization (IPO), which reduces the time and effort needed for the assessment of personality organization through a structured clinical interview, while retaining reliability and sensitivity.
The Present Study
In sum, at least three main dimensions seem to be crucial in this theoretical-clinical framework: parental distress, the quality of maternal care as perceived by the child and offspring’s regulation vs dysregulation processes. It could be hypothesized that these features might be associated with specific personality organizations and specific features of the p factor in mothers, eventually leading to behavioral/emotional maladaptive outcomes both in the parents and in their offspring. In particular, it could be interesting to evaluate this hypothesis in a sample of mothers with children aged around eight years. Indeed, the developmental stage around the age of 8 has been shown to be a crucial period that significantly influences the future psychological well-being of children. This importance can be attributed to the enhanced ability for emotion regulation and the development of improved social skills during this phase, which contribute to determining positive or negative outcomes.15 This study aimed at evaluating the effect of Neurotic, Borderline, and Psychotic organization (considered categorically), and the mediating role of the p factor (measured on a continuum using Achenbach’s model16) in predicting lower/higher parental distress, poor/good quality of parental bond as perceived by the child and offspring’s less or more severe dysregulation symptoms.
Materials and Methods
Participants and Procedure
In Central Italy, N = 524 mothers with their school-age children were recruited over the course of one year via mental health clinics through a consecutive sampling. A team of professional psychologists met mothers and children at their home and youths’ teachers at school and explained the study’s goals and methodology; they also described how the surveys would be used and obtained written informed consent from each adult participant (registering their own consent and the consent given as parents or guardians for the child). This study has been authorized by the Ethical Committee of Sapienza University before its start (n. 23/2020), in accordance with the Declaration of Helsinki. Mothers were asked to fill out the Inventory of Personality Organization (IPO16) to self-report their personality organization and the Adult Self-Report (ASR16), children filled out the Parental Bonding Inventory (PBI17), and teachers were administered with the Teachers Report-Form (TRF16) to report about children’s emotional/behavioral characteristics and psychopathological symptoms. These measures were chosen due to their wide use in research in the field and due to their robust validation. Based on mothers’ reports, three groups have been composed: a) mothers with neurotic personality organization (Group = Neu; N=195 subjects); b) mothers with borderline personality organization (Group = Bord; N=173 subjects); and c) mothers with psychotic personality organization (Group = Psych; N=156 subjects). Missing data (~3%) were revised using multiple imputation in SPSS software (version 25). We decided to recruit only mothers who have been just admitted at the outpatient’s mental health center and had not started pharmacological or psychological/psychiatric treatment, to avoid the bias of the effect of intervention. Mothers’ mean age was 34.42 years (SD = 3.12) and children’s mean age was 8.31 years (SD = 1.46). The large majority of the mothers (89%) had an average socioeconomic status (SES; 25,000–30,000 euros per year). Seventy-nine percent of mothers belonged to intact families; 89% of mothers worked; 91% of children attended primary school. All of the mothers selected for the current study were the children’s biological mothers, and all subjects were Caucasian. The three groups did not significantly differ for the above characteristics (p > 0.05).
Measures
Personality Organization
The Inventory of Personality Organization (IPO14) is a tool used to assess personality organization, consisting of 57 items rated on a Likert scale ranging from 1 to 5. The original version of this instrument comprises three scales: Identity diffusion, Primitive defenses, and Reality-testing. To calculate the score for each dimension, the mean score of the items within that particular dimension is determined (Cronbach's alpha = 0.84).
P Factor
Fried, Ashley, Greene, and Eaton18 proposed a dimensional measurement of the p factor by utilizing the combined raw scores of Internalizing, Externalizing, and Thought Problems from the Adult Self-Report (ASR16). We used this method to categorize mothers in this study. The ASR is a self-report questionnaire designed to assess the psychological functioning of adults aged 18–59. It consists of 126 items that are rated on a 3-point Likert scale, ranging from 0 (indicating “not true”) to 2 (indicating “very true”). The ASR yields scores for eight syndrome scales (anxious/depressed, withdrawn, somatic complaints, thought problems, attention problems, aggressive behavior, rule-breaking behavior, and intrusive behavior; example items are as follows: ‘I feel lonely’; ‘I feel tired without a reason’; ‘I repeat certain acts over and over’; I get in many fights; etc.) and six DSM-oriented scales (depressive problems, anxiety problems, somatic problems, avoidant personality problems, attention-deficit/hyperactivity problems, and antisocial personality problems). Additionally, a total score is available in this assessment, representing the sum of the syndromic scale scores, with a Cronbach’s alpha reliability coefficient of 0.81.
Parental Distress
The Parenting Stress Index-Short Form (PSI-SF)19 is a self-report questionnaire consisting of 36 items that assess parental stress. The scores on this scale were totaled to calculate the overall scores, with higher scores indicating higher levels of parenting stress. Example items are as follows: “I sometimes worry whether I am doing enough for my children”; “The major source of stress in my life is my child”; “I feel overwhelmed by the responsibility of being a parent” etc. In this study, the internal consistency of the scale was good, with a Cronbach’s alpha reliability coefficient of 0.85.
Quality of Maternal Care
The quality of maternal care experienced by children was measured using the Italian version of the Parental Bonding Inventory (PBI17,20). The PBI includes two subscales: one assessing maternal warmth/care and the other assessing maternal overprotection. For the purposes of this study, the total score (obtained by summing the scores of the two dimensions after reversing the overprotection items) was used, as suggested by Kelly and Dupasquier.21 Example items are as follows: “Did not help me as much as I needed”; “Tried to control everything I did”; “Let me decide things for myself”, etc.
Participants rated the extent to which each statement reflected their own experiences on a four-point scale. The PBI has demonstrated good reliability, validity, long-term stability, satisfactory construct and convergent validity, and independence from mood effects.22 The Cronbach’s alpha reliability coefficient for this scale was 0.81.
Children’s Dysregulation
Children’s dysregulation was evaluated using the Teachers Report-Form (TRF16), which assesses emotional-behavioral functioning in children aged 6–18 years. Teachers rated 99 problem items based on the child’s behavior over the previous six months, using a three-point scale (0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true). The items could be grouped into six DSM-5-oriented scales and eight empirically based syndrome scales. The TRF DP scores were obtained by summing the items from the syndrome scales Anxious/Depressed, Attention Problems, and Aggressive Behavior.23 Example items are as follows: “Feels too guilty; Daydreams or gets lost in Thoughts; Physically attacks people”, etc. The Cronbach’s alpha reliability coefficient for this scale was 0.89.
Plan of Analyses
The data were analyzed using IBM SPSS Statistics (Version 25) and LISREL 8.80.24 Descriptive statistics, frequencies, mean scores, and percentages were used for qualitative analyses to determine the reliability of the measures. Quantitative analysis involved conducting multivariate analyses of variance (ANOVAs) on the p factor total score, the child’s DP scores, parental distress, and quality of caring as perceived by the child. The variable “group” served as the between-subjects factor (Neu vs Bord vs Psych). Pearson’s correlation coefficient was applied to examine associations between personality organization, p factor scores, parental distress, the quality of maternal care, and child’s dysregulation. Structural equation modeling (SEM) was employed to test the causal assumptions about the structural relationships among the measures. Cronbach’s alpha coefficient was used during preliminary analysis to assess the reliability of the instruments, with a coefficient value of 0.819.
Results
Vulnerability to Psychopathology in Mothers
Multivariate ANOVAs were conducted to evaluate differences between groups identified based on personality organization of the mothers. Table 1 shows the average scores, SDs for the p factor. The analyses showed that mothers belonging to the Neu group presented lower scores (less maladaptive) than mothers in the Bord group (p < 0.001; eta square = 0.58) and Psych group (p < 0.001; eta square = 0.59) on p factor; mothers in the Bord group showed lower scores than Psych group (p < 0.001; eta square = 0.64).
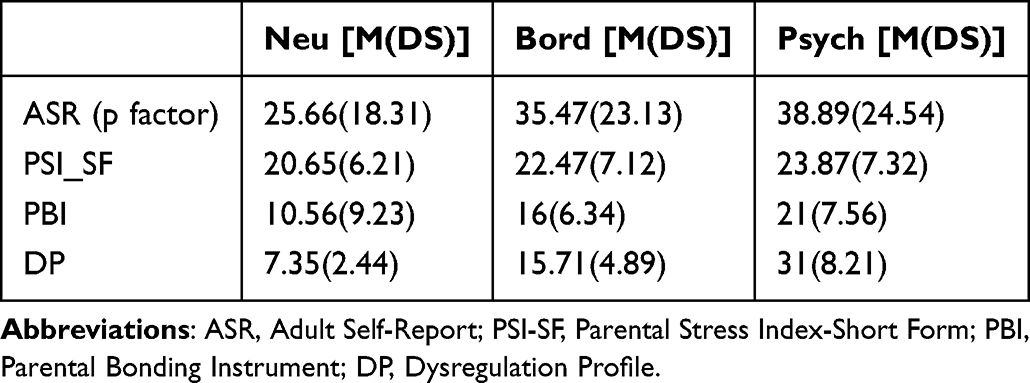 |
Table 1 Means and Standard Deviations of Variables Scores |
Parental Distress
Multivariate ANOVAs were conducted to evaluate differences between groups identified based on personality organization of the mothers. Table 1 shows the average scores, SDs for parental distress. The analyses showed that mothers belonging to the Neu group presented lower scores (less maladaptive) than mothers in the Bord group (p < 0.001; eta square = 0.62) and Psych group (p < 0.001; eta square = 0.66) on p factor; mothers in the Bord group showed lower scores than Psych group (p < 0.001; eta square = 0.58).
Quality of Maternal Care Perceived by Children
Multivariate ANOVAs were conducted to evaluate differences between groups identified based on personality organization of the mothers. Table 1 shows the average scores, SDs for the quality of maternal care as perceived by the children. The analyses showed that children with mothers belonging to the Neu group presented less maladaptive scores than mothers in the Bord group (p < 0.001; eta square = 0.69) and Psych group (p < 0.001; eta square = 0.71) on p factor; children in the Bord group showed less maladaptive scores than Psych group (p < 0.001; eta square = 0.62).
Children’s Dysregulation
Multivariate ANOVAs were conducted to evaluate differences between groups identified based on personality organization of the mothers. Table 1 shows the average scores, SDs for the quality of maternal care as perceived by the children. The analyses showed that children with mothers belonging to the Neu group presented lower scores than children in the Bord group (p < 0.001; eta square = 0.59) and Psych group (p < 0.001; eta square = 0.51) on p factor; children with mothers in the Bord group showed lower scores than Psych group (p < 0.001; eta square = 0.52).
Correlations Between Variables and Main Effect of Personality Organization and Mediated Effect of p Factor Scores
All outcome variables demonstrated significant correlations, as expected per previous literature, which had suggested bidirectional links between these constructs (p < 0.01, two-tailed). To investigate the main effect of maternal personality organization (Neurotic, Borderline, and Psychotic) and the mediated effect of p factor scores on outcome variables (Maternal Distress, Perceived Quality of Care, and Dysregulation), a path analysis model was constructed using LISREL 8.80.24 This software allows for simultaneous testing of complex sets of relationships. The model results included path coefficients, which indicate the parameter estimates of the relative effect one variable has on another. Standardized regression weights (β) indicate the strength of the linear relationship and imply an unmediated connection between changes in the variables.
To assess the overall fit of the data to the model, several measures were employed. The chi-square value, goodness-of-fit indices, and squared multiple correlations were examined. The chi-square assessment determines whether the hypothesized model adequately fits the data. Goodness-of-fit indices range from 0 to 1, with values closer to 1 indicating a better fit. Squared multiple correlations indicate the amount of variability accounted for by the specific equation.
The model demonstrated acceptable results,25 with a non-statistically significant chi-square value or a chi-square-to-degrees-of-freedom ratio (χ2/df) below 3, indicating an excellent fit.26 In terms of goodness-of-fit indices, the non-normed fit index (NNFI) and the comparative fit index (CFI) yielded high values of 0.98 and 0.97, respectively, indicating a strong fit between the model and the actual data. The root mean square error of approximation (RMSEA) also provided satisfactory results, with a value of 0.076. According to Chen, Curran, Bollen, Kirby, and Paxton,27 a value between 0.05 and 0.08 is considered adequate. With respect to maternal personality organization, Psych showed unmediated and significant effect: maternal distress, β = 0.47, p < 0.05, quality of maternal care, β = 0.68, p < 0.05. Bord showed main effect on offspring’s dysregulation symptoms, β = 0.59, p < 0.05. Neu showed significant main effect only on maternal distress β = 0.61, p < 0.05. Psych influenced the quality of perceived maternal care and children dysregulation through the mediating effect of the p factor score, p < 0.05. Bord influenced the quality of bonding, β = 0.54, p < 0.05, through the mediating effect of p factor, p < 0.05. Figure 1 shows the model (only significant effects are shown).
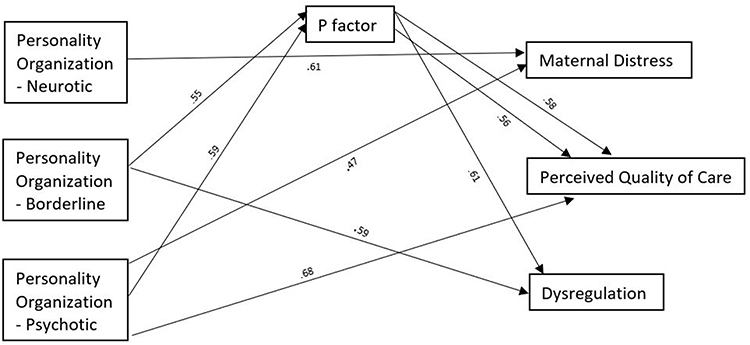 |
Figure 1 Path model significant parameter estimates for the effects of personality organization and p factor scores on outcome scores. |
Discussion
This study considered the theories of Caspi et al about the existence of a General Psychopathological Factor (p factor),1 and Kernberg’s principles about the tripartite nature of the personality organization.28 Rooting on these theoretical premises, this research aimed at evaluating the effect of Neurotic, Borderline, and Psychotic organization and the mediating role of the p factor in predicting lower/higher maternal distress, poor/good quality of parental care as perceived by the child and offspring’s less or more severe dysregulation symptoms.
First, descriptive analyses have been performed to evaluate possible differences on a series of variables (p factor scores, parental distress, quality of care, dysregulation) between groups identified based on personality organization of the mothers. Our results showed that a spectrum of maladaptive characteristics seems to exist in association with the different personality organizations, ranging from the least to the most problematic. Neurotic mothers, in fact, presented less maladaptive scores in all the above variables when compared with mothers with borderline or psychotic organization and Bord group showed less severe scores than Psych group. Previous literature has shown that individuals with neurotic personality organization are generally less vulnerable to psychopathology29 than individuals with borderline or psychotic organization. In fact, although neurotic mothers are posited to be irritable and quarrelsome, emotionally cold and authoritarian, and sometimes even rejecting, when compared with subjects with borderline or psychotic organization neurotic individuals, they usually show higher self-awareness, self-control, and a high degree of emotional regulation.30,31 They are also usually able to identify distorted cognitions and fix them through emotional regulation before they develop into full-blown anxious/depressive thoughts. This capacity seems to be supported at a neurobiological level by a high level of activation in the ventral anterior cingulate cortex, which is involved in detecting errors, discrepancies, anomalies and predicting emotional and motivational states.32 Moreover, neurotic individuals generally display lower levels of amygdala activation, which is involved in emotional response to stressing experiences and mediate the tendency to react with anger, negative emotions, and aggression.33,34 It could be for this reason that neurotic mothers in our sample showed less parental distress than mothers with borderline and psychotic organization. Moreover, from a clinical point of view, mothers with a neurotic organization are capable of using mature defense strategies, can rely on a robust reality-testing and identity, which allow them to effectively respond to distressing situations, and to have a balanced and generally unbiased representation of their children requests (that they do not feel as inadequate and overwhelming).
Their offspring, on their part, showed less dysregulation symptoms compared to offspring of mothers with borderline and psychotic organization. We may speculate, however, that the reduced dysregulation problems could be due to a tendency of youth children of neurotic mothers to over-controlling emotions.35
The path analysis model showed that belonging to the group of mothers with psychotic personality organization had a direct, positive and significant effect on maternal distress and quality of maternal care, in the sense that these mothers experienced higher parental distress and their children perceived a poorer quality of caregiving, compared with mothers and youths of other groups. As for the mediated effects, the psychotic organization influenced the quality of perceived maternal care and children’s dysregulation through the mediating effect of the p factor score. We can speculate that as these mothers frequently tend to suppress feelings of hate and hostility in their children, youths can react with aggressive, oppositional behavior or with severe withdrawal.36 Mothers with psychotic organization are easily and rapidly stressed and tend to react with violence, often directed at their children. These mothers may exhibit paranoid and depressive symptoms and are likely to put their children in very controlling situations that emphasize sameness and repetitive rituals. As a result, offspring may show rebellion against their parents, with oppositional behaviors.37 Moreover, having a mother with psychotic organization may induce chaotic, ambivalent communication, severe impairments in the ability of parenting, parenting stress, disorganized attachment, and disrupted parenting. Their parenting capacities are also hindered by the difficulty in comprehending infants’ cues and react appropriately.38
Belonging to the group with mothers with borderline personality organization had a direct, positive and significant effect on offspring’s dysregulation symptoms, so that children of these mothers showed higher dysregulation problems. The borderline organization was also associated with poorer quality of caring through the mediating effect of p factor. It is possible to hypothesize that mothers who are characterized by borderline personality organization may find it difficult to integrate their own selves with those of their children; they could tend to seeing their children as extensions of themselves and, as a result, these parents often act in ways that are contradictory, manipulative, and unstable, and their children often lack an appropriate model for managing their own inner experience, and so may show psychopathological symptoms.39 Moreover, these mothers tend to have children at an earlier age. Due to the distress of parenting at early age, these mothers often neglect their children.40 Thus, the neglected children often feel anxious and lonely, and lack a parent figure to depend on for soothing when stressed, finding it difficult to regulate their emotions, particularly those concerning anger and fear. Some research has shown that parents with borderline personality organization (BPO) may threaten to abandon their children.9 Regardless from the fact that they act this threaten, their children may develop a sense of helplessness adopting a submissive attitude towards the parent as a response in order to avoid abandonment. In a vicious circle, however, as they adopt this passive behavior they behave in ways that prompt caretakers to feel angry or frustrated, which increases the likelihood of rejection from the mothers.
Finally, belonging to the group with mothers with neurotic personality organization had a direct, positive and significant effect only on maternal distress, ie mothers in this group reported higher scores at the PSI-SF. Mothers with neurotic personality organization are suggested to be prone to psychological distress. As parenting is generally a source of distress, parents-children dyads can experience frequent conflicts, also because these parents have been shown to be more irritable and quarrelsome than non-neurotic parents. Moreover, in line with the Developmental Psychopathology theoretical and clinical framework (that posits a transgenerational transmission of vulnerability to psychological problems), they could have sensitive children who internalize their parents’ anxiety, tendency to overcontrol and tension. They can also be emotionally cold and authoritarian, rejecting, or indifferent toward their children, making them feel insecure, unloved and inadequate. Offspring can therefore generalize this attitude to all individuals interacting with them, developing paranoid beliefs that others are against them. On the other hand, parents with neurotic personality organization can also be over-indulgent with their children and fail to pose limits. In this case, their children could show emotion dysregulation in the area of aggressiveness, hostility and rule-breaking and may show temper tantrums and stubbornness; they may also be very demanding and attention seeking.
This study has limitations. First, it did not consider fathers in the assessment of the general functioning of the family, whereas several authors have demonstrated that fathers have an influence (protective or of adjunct risk) both on maternal and children’s psychopathological problems.33,41 Second, this is a cross-sectional study; although predictive effects have been hypothesized, no causal conclusion can be drawn from our results. Third, the sample was very homogeneous for potentially important variables such as level of schooling, household income, and geographical origin, limiting the generalizability of our results. Finally, this study did not consider other possible theoretical and empirical models to explain links between variables, such as the Baumrind’s Y-model and Maccoby and Martin’s two-dimensional theoretical model that proposed four parenting styles based on warmth and strictness dimensions: authoritative, authoritarian, indulgent, and neglectful.42–52,53
Conclusions
In conclusion, this study explored how different personality organizations in mothers impact maternal distress, quality of parental care, and offspring’s dysregulation symptoms. Neurotic mothers showed better emotional regulation and had children with fewer dysregulation problems, while mothers with borderline or psychotic organization experienced higher distress and provided less stable caregiving, resulting in more severe dysregulation symptoms in their children.
Future studies should consider the influence of fathers in family dynamics and their role in maternal and child psychopathological risks, also utilizing longitudinal research designs can help establish causal relationships between variables. By addressing these areas in future research, a deeper understanding of the complexities of parent–child interactions could be gained, to enhance support for families facing psychopathological challenges.
Data Sharing Statement
Data are available at reasonable request to the authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising and critically reviewing the article; gave final approval of the version published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Caspi A, Moffitt TE. When do individual differences matter? A paradoxical theory of personality coherence. Psychol Inq. 1993;4(4):247–271. doi:10.1207/s15327965pli0404_1
2. Allegrini AG, Cheesman R, Rimfeld K, et al. The p factor: genetic analyses support a general dimension of psychopathology in childhood and adolescence. J Child Psychol Psychiatry. 2020;61(1):30–39. doi:10.1111/jcpp.13113
3. Cervin M, Norris LA, Ginsburg G, et al. The p factor consistently predicts long-term psychiatric and functional outcomes in anxiety-disordered youth. J Am Acad Child Adolesc Psychiatry. 2021;60(7):902–912.e5. doi:10.1016/j.jaac.2020.08.440
4. Ammaniti M, Lucarelli L, Cimino S, D’olimpio F. Intergenerational transmission: early feeding disorders and maternal psychopathology. Devenir. 2004;16(3):173–198. doi:10.3917/dev.043.0173
5. Rutter M. Developmental psychopathology: a paradigm shift or just a relabeling? Dev Psychopathol. 2013;25(4 Pt 2):1201–1213. doi:10.1017/S0954579413000564
6. Maremmani AGI, Cerniglia L, Cimino S, Bacciardi S, Rovai, L, Pellucchini, A, Spera, V, Perugi, G, Maremmani, I. Further evidence of a specific psychopathology of addiction. Differentiation from other psychiatric psychopathological dimensions (such as obesity). IJERPH. 2017;14(8). doi:
7. Carlson EA, Egeland B, Sroufe LA. A prospective investigation of the development of borderline personality symptoms. Dev Psychopathol. 2009;21(4):1311–1334. doi:10.1017/S0954579409990174
8. Stepp SD, Whalen DJ, Pilkonis PA, Hipwell AE, Levine MD. Children of mothers with borderline personality disorder: identifying parenting behaviors as potential targets for intervention. Personal Disord. 2012;3(1):76–91. doi:10.1037/a0023081
9. Caligor E, Clarkin JF, Sowislo JF. Levels of Personality Organization. Personality Disorders; 2021.
10. Ensink K, Borelli JL, Normandin L, Target M, Fonagy P. Childhood sexual abuse and attachment insecurity: associations with child psychological difficulties. Am J Orthopsychiatry. 2020;90(1):115. doi:10.1037/ort0000407
11. Petfield L, Startup H, Droscher H, Cartwright-Hatton S. Parenting in mothers with borderline personality disorder and impact on child outcomes. Evid Based Ment Health. 2015;18(3):67–75. doi:10.1136/eb-2015-102163
12. Hobson RP, Patrick M, Crandell L, García-Pérez R, Lee A. Personal relatedness and attachment in infants of mothers with borderline personality disorder. Dev Psychopathol. 2005;17(2):329–347. doi:10.1017/s0954579405050169
13. Campbell LE, Hanlon M-C, Galletly CA, et al. Severity of illness and adaptive functioning predict quality of care of children among parents with psychosis: a confirmatory factor analysis. Aust N Z J Psychiatry. 2018;52(5):435–445. doi:10.1177/0004867417731526
14. Lenzenweger MF, Clarkin JF, Kernberg OF, Foelsch PA. The Inventory of Personality Organization: psychometric properties, factorial composition, and criterion relations with affect, aggressive dyscontrol, psychosis proneness, and self-domains in a nonclinical sample. Psychol Assess. 2001;13(4):577–591. doi:10.1037/1040-3590.13.4.577
15. Cimino S, Cerniglia L, Porreca A, Ballarotto G, Marzilli E, Simonelli A. Impact of parental binge eating: exploring children’s emotioanl/behavioral problems and the quality of parental feeding interactions. Inf Ment Health. 2018;39(5):552–568. doi:
16. Achenbach TM, Rescorla LA. Manual for the ASEBA school-age forms & profiles: an integrated system of multi-informant assessment. Res Cent Children Youth Families. 2001;2001:1617.
17. Scinto A, Marinangeli MG, Kalyvoka A, Daneluzzo E, Rossi A. The use of the Italian version of the Parental Bonding Instrument (PBI) in a clinical sample and in a student group: an exploratory and confirmatory factor analysis study. Epidemiol Psichiatr Soc. 1999;8(4):276–283. doi:10.1017/S1121189X00008198
18. Fried EI, Greene AL, Eaton NR. The p factor is the sum of its parts, for now. World Psychiatry. 2021;20(1):69–70. doi:10.1002/wps.20814
19. Abidin RR. Parenting Stress Index: Manual, Administration Booklet. ERIC; 1983.
20. Rossi A, Daneluzzo E, Arduini L, Di Domenico M, Pollice R, Petruzzi C. A factor analysis of signs and symptoms of the manic episode with bech–rafaelsen mania and melancholia scales. J Affect Disord. 2001;64(2–3):267–270. doi:10.1016/S0165-0327(00)00228-7
21. Kelly AC, Dupasquier J. Social safeness mediates the relationship between recalled parental warmth and the capacity for self-compassion and receiving compassion. Pers Individ Dif. 2016;89:157–161. doi:10.1016/j.paid.2015.10.017
22. Parker G, Tupling H, Brown LB. A parental bonding instrument. Br J Clin Psychol. 1979;52(1):1–10. doi:10.1111/j.2044-8341.1979.tb02487.x
23. Basten MM, Althoff RR, Tiemeier H, Jaddoe VW, Hofman A, Hudziak JJ. The dysregulation profile in young children: empirically defined classes in the generation R study. J Am Acad Child Adolesc Psychiatry. 2013;52(8):841–850. doi:10.1016/j.jaac.2013.05.007
24. Jöreskog KG, Sörbom D, Wallentin FY. Latent variable scores and observational residuals. Retr June. 2006;7:2009.
25. Schermelleh-Engel K, Moosbrugger H, Müller H. Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. Methods Psychol Res Online. 2003;8:23–74.
26. Browne MW, Cudeck R. Alternative ways of assessing model fit. Sociol Methods Res. 1992;21(2):230–258. doi:10.1177/0049124192021002005
27. Chen F, Curran PJ, Bollen KA, Kirby J, Paxton P. An empirical evaluation of the use of fixed cutoff points in RMSEA test statistic in structural equation models. Sociol Methods Res. 2008;36(4):462–494. doi:10.1177/0049124108314720
28. Clarkin JF, Levy KN, Lenzenweger MF, Kernberg OF. The personality disorders institute/borderline personality disorder research foundation randomized control trial for borderline personality disorder: rationale, methods, and patient characteristics. J Pers Disord. 2004;18(1):52–72. doi:10.1521/pedi.18.1.52.32769
29. Fischer-Kern M, Buchheim A, Hörz S, et al. “The relationship between personality organization, reflective functioning, and psychiatric classification in borderline personality disorder”: correction to Fischer-Kern et al (2010). Psychoanal Psychol. 2011;28(1):74. doi:10.1037/a0022611
30. Baumeister RF, Boden JM. Aggression and the self: high self-esteem, low self-control, and ego threat. In: Human Aggression. Academic Press; 1998:111–137.
31. Lai C, Altavilla D, Mazza M, et al. Neural correlate of internet use in patients undergoing psychological treatment for internet addiction. J Ment Health. 2017;26(3):276–282. doi:10.1080/09638237.2017.1294745
32. Bush G, Luu P, Posner MI. Cognitive and emotional influences in anterior cingulate cortex. Trends Cogn Sci. 2000;4(6):215–222. doi:10.1016/s1364-6613(00)01483-2
33. Tafa’ M, Cerniglia L, Cimino S, Ballarotto G, Marzilli E, Tambelli, R. Predictive values of early parental loss and psychopathological risk for physical problems in early adolescents. Front Psychol. 2018;9():.
34. Stansbury K, Gunnar MR. Adrenocortical activity and emotion regulation. Monogr Soc Res Child Dev. 1994;59(2–3):108–134. doi:10.1111/j.1540-5834.1994.tb01280.x
35. Pollock KM, Feinstein RE. Employing psychodynamic process-oriented group psychotherapy with personality disorders. Personal Disord. 2021;3:363.
36. Zhang X, Gatzke-Kopp LM, Fosco GM, Bierman KL. Parental support of self-regulation among children at risk for externalizing symptoms: developmental trajectories of physiological regulation and behavioral adjustment. Dev Psychol. 2020;56(3):528–540. doi:10.1037/dev0000794
37. Fooladvand M, Nadi MA, Abedi A, Sajjadian I. Parenting styles for children with oppositional defiant disorder: scope review. J Educ Health Promot. 2021;10. doi:10.4103/jehp.jehp_566_19
38. Rabha A, Padhy SK, Grover S. Parenting skills of patients with chronic schizophrenia. Indian J Psychiatry. 2021;63(1):58–65. doi:10.4103/psychiatry.IndianJPsychiatry_107_20
39. Öztürk E. Dysfunctional generations versus natural and guiding parenting style: intergenerational transmission of trauma and intergenerational transfer of psychopathology as dissociogenic agents. Med Sci. 2022;11(2):886–904. doi:10.5455/medscience.2022.04.090
40. King LS, Humphreys KL, Gotlib IH. The neglect-enrichment continuum: characterizing variation in early caregiving environments. Devell Rev. 2019;51:109–122. doi:10.1016/j.dr.2019.01.001
41. Mahedy L, Harold GT, Maughan B, Gardner F, Araya R, Jones RB. Resilience in high-risk adolescents of mothers with recurrent depressive disorder: the contribution of fathers. J Adolesc. 2018;65(1):207–218. doi:10.1016/j.adolescence.2018.03.016
42. Alcaide M, Garcia OF, Queiroz P, Garcia F. Adjustment and maladjustment to later life: evidence about early experiences in the family. Front Psychol. 2023. doi:10.3389/fpsyg.2023.1059458
43. Baumrind D. Authoritarian vs authoritative parental control. Adolescence. 1968;3:255–272.
44. Baumrind D. Effective parenting during the early adolescent transition. In: Cowan PA, Herington EM, editors. Advances in Family Research Series. Family Transitions. Lawrence Erlbaum Associates, Inc; 1991:111–163.
45. Chao RK. Extending research on the consequences of parenting style for Chinese Americans and European Americans. Child Dev. 2001;72:1832–1843. doi:10.1111/1467-8624.00381
46. Climent-Galarza S, Alcaide M, Garcia OF, Chen F, Garcia F. Parental socialization, delinquency during adolescence and adjustment in adolescents and adult children. Behav Sci (Basel). 2022;12(11). doi:10.3390/bs12110448
47. Darling N, Steinberg L. Parenting style as context: an integrative model. Psychol Bull. 1993;113(3):487–496. doi:10.1037/0033-2909.113.3.487
48. Deater-Deckard K, Dodge KA, Bates JE, Pettit GS. Physical discipline among African American and European American mothers: links to children’s externalizing behaviors. Dev Psychol. 1996;32(6):1065–1072. doi:10.1037/0012-1649.32.6.1065
49. Dwairy M, Achoui M. Introduction to three cross-regional research studies on parenting styles, individuation, and mental health in Arab societies. J Cross Cult Psychol. 2006;37(3):221–229. doi:10.1177/0022022106286921
50. Fuentes MC, Garcia OF, Alcaide M, Garcia-Ros R, Garcia F. Analyzing when parental warmth but without parental strictness leads to more adolescent empathy and self-concept: evidence from Spanish homes. Front Psychol. 2022;13. doi:10.3389/fpsyg.2022.1060821
51. Garcia F, Gracia E. The indulgent parenting style and developmental outcomes in South European and Latin American countries. In: Selin H, editor. Parenting Across Cultures. Springer; 2014:419–433. doi:10.1007/978-94-007-7503-9_31
52. Garcia F, Gracia E. Is always authoritative the optimum parenting style? Evidence from Spanish families. Adolescence. 2009;44(173):101–131.
53. Marzilli E, Cerniglia L, Tambelli R, et al. The covid-19 pandemic and its impact on families’ mental health: the role played by parenting stress, parents’ past trauma, and resilience. IJERPH. 2021;18(21):11450.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.