")
Back to Journals » International Journal of General Medicine » Volume 14
The Role of Environmental PM2.5 in Admission Acute Heart Failure in ST-Elevation Myocardial Infarction patients - An Observational Retrospective Study
Authors Sinkovic A , Markota A, Krasevec M , Suran D , Marinsek M
Received 23 September 2021
Accepted for publication 29 October 2021
Published 18 November 2021 Volume 2021:14 Pages 8473—8479
DOI https://doi.org/10.2147/IJGM.S340301
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Andreja Sinkovic,1 Andrej Markota,1 Manja Krasevec,2 David Suran,3 Martin Marinsek1
1Department of Medical Intensive Care, University Clinical Centre Maribor, Maribor, Slovenia; 2Medical Faculty of University Maribor, Maribor, Slovenia; 3Department of Cardiology, University Clinical Centre Maribor, Maribor, Slovenia
Correspondence: Andreja Sinkovic
Department of Medical Intensive Care, University Clinical Centre Maribor, Ljubljanska 5, Maribor, 2000, Slovenia
Tel +38641337822
Email [email protected]
Background: Air pollution with increased concentrations of fine (< 2.5 μm) particulate matter (PM2.5) increases the risk of cardiovascular morbidity and mortality. Even short-term increase of PM2.5 may help trigger ST-elevation myocardial infarction (STEMI) and heart failure (HF) in susceptible individuals, even in areas with good air quality.
Purpose: To evaluate the role of PM2.5 levels ≥ 20 μg/m3 in admission acute HF in STEMI patients.
Materials and Methods: In 290 STEMI patients with the leading reperfusion strategy primary percutaneous coronary intervention (PPCI), we retrospectively studied independent predictors of admission acute HF and included admission demographic and clinical data as well as ambient PM2.5 levels ≥ 20 μg/m3. We defined admission acute HF in STEMI patients as classes II–IV by Killip Kimball classification.
Results: Acute admission HF was observed in 34.5% of STEMI patients. PPCI was performed in 87.1% of acute admission HF patients and in 94.7% non-HF patients (p= 0.037). Significant independent predictors of acute admission HF were prior diabetes (OR 2.440, 95% CI 1.100 to 5.400, p=0.028), admission LBBB (OR 10.190, 95% CI 1.160 to 89.360, p=0.036), prior resuscitation (OR 2.530, 95% CI 1.010 to 6.340, p=0.048), admission troponin I≥ 5μg/l (OR 3.390, 95% CI 1.740 to 6.620, p< 0.001), admission eGFR levels (0.61, 95% CI 0.52 to 0.72, p < 0.001), and levels of PM2.5 ≥ 20 μg/m3 (OR 2.140, 95% CI 1.005 to 4.560, p=0.049) one day before admission.
Conclusion: Temporary short-term increase in PM2.5 levels (≥ 20 μg/m3) one day prior to admission in an area with mainly good air quality was among significant independent predictors of acute admission HF in STEMI patients.
Keywords: admission acute heart failure, ST-elevation myocardial infarction, air pollution, PM2.5
Introduction
Acute heart failure (HF) at presentation is an important determinant of morbidity and mortality in ST-elevation myocardial infarction (STEMI) patients in spite of early reperfusion therapy by primary percutaneous coronary intervention (PCI), combined with evidence-based pharmacological treatment.1,2 STEMI patients with acute admission HF receive less evidence-based therapies and/or interventions compared to patients without admission HF.3,4
Acute admission HF in STEMI patients is a complex event, precipitated by myocardial ischemia and modified by primary PCI, time delay to primary PCI, pre-existing cardiac disease, and environmental factors such as air pollution.2,5 Increased exposure to air pollution is associated with increased cardiovascular morbidity and mortality, in particular in areas with extremely high concentrations of air pollutants.6 However, even in areas with relatively good air quality, temporary traffic-related increased concentrations of fine (<2.5 μm) particulate matter (PM2.5) within prior hours were strongly associated with ischemic stroke, increased risk of myocardial infarction, and increased risk of hospitalization or death due to HF.7–10
In addition to ozone, carbon monoxide, lead, nitrogen dioxide, volatile organic compounds and sulphur dioxide, PM2.5 plays an important role in the deleterious effect of air pollution upon human health. Long-term air pollution from PM2.5 alone is responsible for increased risk of premature death from stroke by 19% and from coronary heart disease by 13% even in exposures below the current European air quality limit values, ie, less than 10μg/m3 for mean annual levels and less than 25μg/m3 for 24-hour mean annual levels.11
There is also evidence that short-term exposure – hours or days – to elevated 24-hour mean daily levels of PM2.5 >25 μg/m3 may help trigger acute coronary syndromes, in particular STEMI and HF exacerbation in susceptible individuals.12
However, the results on short-term effects of air pollution on a range of cardiovascular events from the MINAP database found no clear evidence for pollution effects on STEMIs and stroke, but for pulmonary embolism.13 The strongest associations with air pollution were observed with non-MI outcomes.13
Our aim was to evaluate predictive role of PM2.5, measured on admission and one day prior to hospital admission for acute HF in STEMI patients at presentation.
Materials and Methods
Patients
We retrospectively included 290 STEMI patients (100 women and 190 men), hospitalized at the University clinical Centre in 2018 from the Maribor (Slovenia) area. From the institutional medical information system we retrospectively registered their clinical, demographic, and mortality data.
Methods
Institutional Medical Ethics Committee (University clinical centre Maribor – Medical Ethics Committee (KME)) approved the retrospective observational study (approval UKC-MB-KME-62/19). The requirement of informed consent of included patients was waived due to the retrospective nature of the study. The study was in accordance with the 1964 Declaration of Helsinki and its subsequent amendments. Personal data of the patients were protected by the Law on Personal Data Protection.
The care of STEMI patients started with emergency medical services after the diagnosis was established according to well-known criteria.14 According to current guidelines, at first medical contact, early treatment consisted of dual antiplatelet therapy (acetylsalicylic acid (ASA) and clopidogrel or ticagrelor or prasugrel), heparin IV up to 5000 I.E, oxygen in hypoxemia (target SatO2 95%), morphine iv. in case of chest pain, and sublingual nitroglycerine. In case of pulmonary edema, emergency IV. diuretic and in cardiogenic shock, noradrenalin IV infusion was started. In case of cardiac arrest, patients were resuscitated, intubated, and mechanically ventilated.14
After arrival to the Catheterization Laboratory, invasive cardiologist performed primary PCI as soon as possible. After primary PCI, STEMI patients were admitted to the medical ICU or coronary unit (CU) and were monitored for at least 24 hours (continuous ECG monitoring, pulse oximetry, hourly non-invasive or continuous invasive blood pressure measurements), or longer, if necessary. Standard laboratory tests were performed on admission and later on daily basis during in-hospital stay. Standard ECG was recorded each day.14
STEMI patients with admission acute HF were treated in hospital with oxygen to correct hypoxemia, either by face mask, or by the nasal cannula in case of mild hypoxemia or by non-invasive positive pressure ventilation in respiratory distress with respiratory rate >25 breaths/min. In severe hypoxemia (PaO2 <8.0 kPa) with hypercapnia (PaCO2 >6.65 kPa) and acidosis (pH <7.35), not responding to non-invasive ventilation, patients were intubated and mechanically ventilated. Concomitantly, blood pressure was measured. Fluids and/or noradrenalin and/or inotropes were administered IV in case of hypotension, and diuretic in pulmonary edema.14,15 Patients were monitored for fluid responsiveness by 2-D echocardiographic measurement of left ventricular contractility and respiratory changes in the diameter of the inferior vena cava.14
After primary PCI, the patients received IV infusions of crystalloids (50–100 mL/h) to prevent contrast-induced renal injury, according to fluid responsiveness.14
During ICU/CU stay, STEMI patients received all recommended pharmacological therapies, consisting of statins, dual antiplatelet therapy (ASA and clopidogrel or prasugrel or ticagrelor) in maintenance dose to prevent in-stent thrombosis, as well as beta receptor blockers, and angiotensin-converting enzyme inhibitors, if necessary.14
We performed echocardiography after primary PCI within hours of admission, before discharge, and in case of complications. We also performed other diagnostic procedures if necessary (chest radiograph, ECG, laboratory tests), in case of complications.14 We confirmed the diagnosis of STEMI by the rise and fall of Troponin I levels in addition to ECG changes.14
Registered demographic and clinical data on admission included age, gender and comorbidities (arterial hypertension, diabetes, prior myocardial infarction, left bundle branch block (LBBB)), prior resuscitation, time interval to primary PCI, increased admission Troponin I levels, serum creatinine, eGFR-EPI levels and admission acute HF. Admission HF was classified by the Killip-Kimball classification as classes II–IV and included pulmonary congestion, pulmonary edema, cardiogenic shock or any hypotension or low cardiac output state, if vasopressors were needed.14,16 Admission serum creatinine was measured by enzymatic method. The formula for eGFR used the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. Levels of eGFR-EPI < 90 mL/min/1.73 m2 were classified as chronic kidney dysfunction.17
We retrospectively registered 24-hour mean daily levels of PM2.5 on the admission day and one day prior to admission for every single STEMI patient in the area of their residence. Mean daily PM2.5 levels were measured and registered on a daily basis by the Chemical analytic laboratory of Environmental agency of Republic Slovenia (ARSO), establishing a system of quality in line with the ISO 9001:2008 and ISO/SIST/IEC 17025 international standards for accredited Calibration Laboratory and the Chemical Analysis Laboratory. The data were freely available.18
We also retrospectively registered the use of primary PCI, TIMI III flow after primary PCI, peak troponin I ≥ 50ug/L, EF measurements by echocardiography after primary PCI after admission, and in-hospital mortality.
We compared the admission data between STEMI patients with and without admission acute HF and evaluated significant independent predictors of acute admission HF in STEMI patients. In addition, we evaluated the importance of admission HF for the use of primary PCI and hospital mortality.
Statistical Analysis
Statistical analyses were performed using the SPPS Statistical package, version 19 (IBM Corp., Armonk, N.Y., USA) for Windows. We presented the data as means ± standard deviation or percentages. We used the two-sided Student’s t-test to test the differences between the groups for means ± standard deviation and Fisher’s exact test for percentages. A p value <0.05 was considered statistically significant. We used the model of bivariate logistic regression to assess independent predictors of admission heart failure (Killip classes II–IV) by entering statistically significant parameters from the descriptive statistics to the model of logistic regression.
Results
Admission characteristics of included STEMI patients, and comparison between the STEMI patients with and without acute admission HF are presented in Table 1.
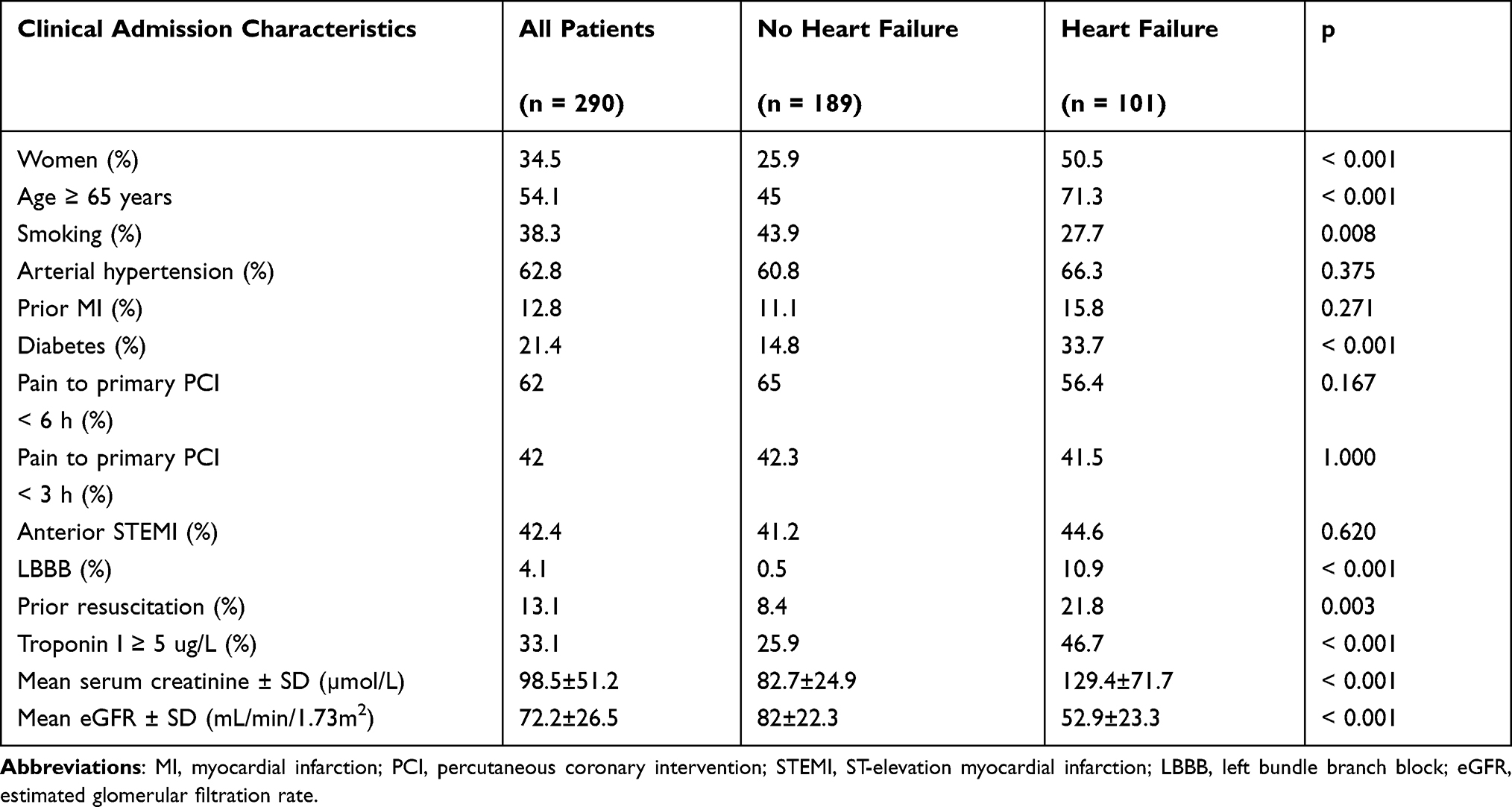 |
Table 1 Baseline Characteristics of STEMI Patients and Comparison Between STEMI Patients without and with Acute Admission Heart Failure |
Among 290 STEMI patients we observed acute admission HF in 34.5% of cases. STEMI patients with acute admission HF in comparison to STEMI patients without HF were significantly more likely women, aged over 65 years, with diabetes, LBBB, resuscitated before admission and with increased admission troponin I ≥ 5 ug/L, eGFR, but there were nonsignificant differences in arterial hypertension, prior myocardial infarction, time to primary PCI, anterior STEMI.
PM2.5 levels on admission and one day before admission are presented in Table 2. Only PM2.5 levels ≥ 20 ug/m3 one day before admission were associated with admission acute HF in our STEMI patients.
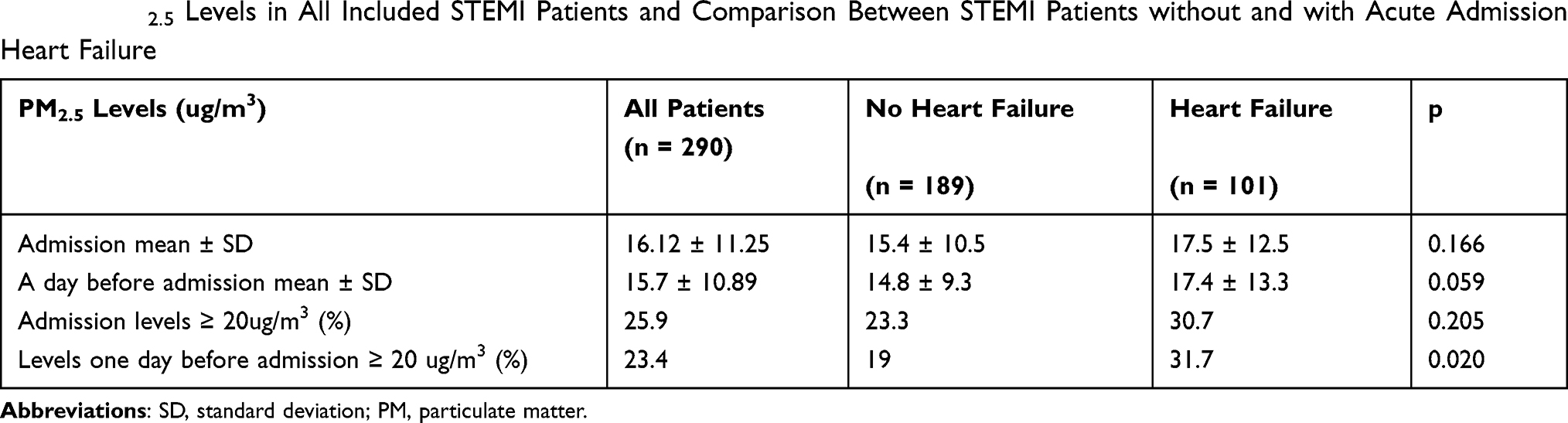 |
Table 2 PM2.5 Levels in All Included STEMI Patients and Comparison Between STEMI Patients without and with Acute Admission Heart Failure |
Significant parameters of the descriptive statistics on admission (gender, age over 65 years, prior diabetes, smoking, LBBB, prior resuscitation, increased admission troponin I levels, PM2.5 levels ≥ 20ug/m3 one day before admission, admission eGFR) were entered in the model of logistic regression. Independent predictors of admission heart failure are presented in Table 3. Admission eGFR, diabetes, LBBB, prior resuscitation, admission Troponin I≥5µg/L and PM2.5 levels ≥ 20ug/m3 one day before admission were among significant independent predictors of admission acute HF in STEMI patients.
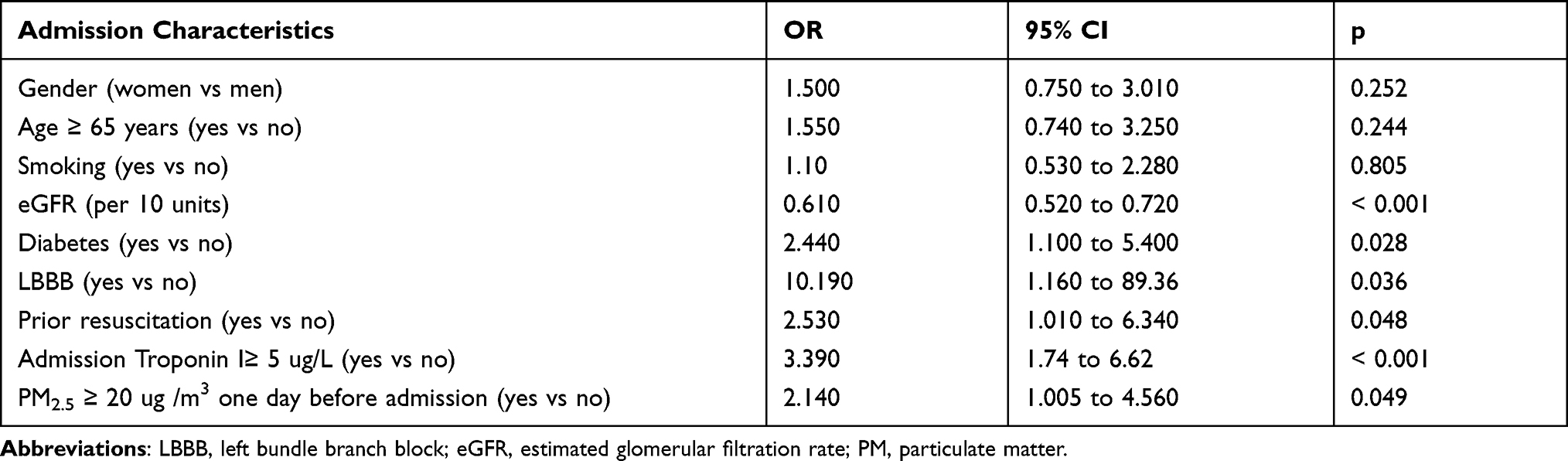 |
Table 3 Independent Predictors of Admission Acute Admission Heart Failure in STEMI Patients |
The use of primary PCI, TIMI III flow after primary PCI, increased peak hospital Troponin I levels, mean EF levels and EF levels < 50%, IABP and hospital mortality in all included STEMI patients and comparison between STEMI patients without and with acute admission HF are presented in Table 4.
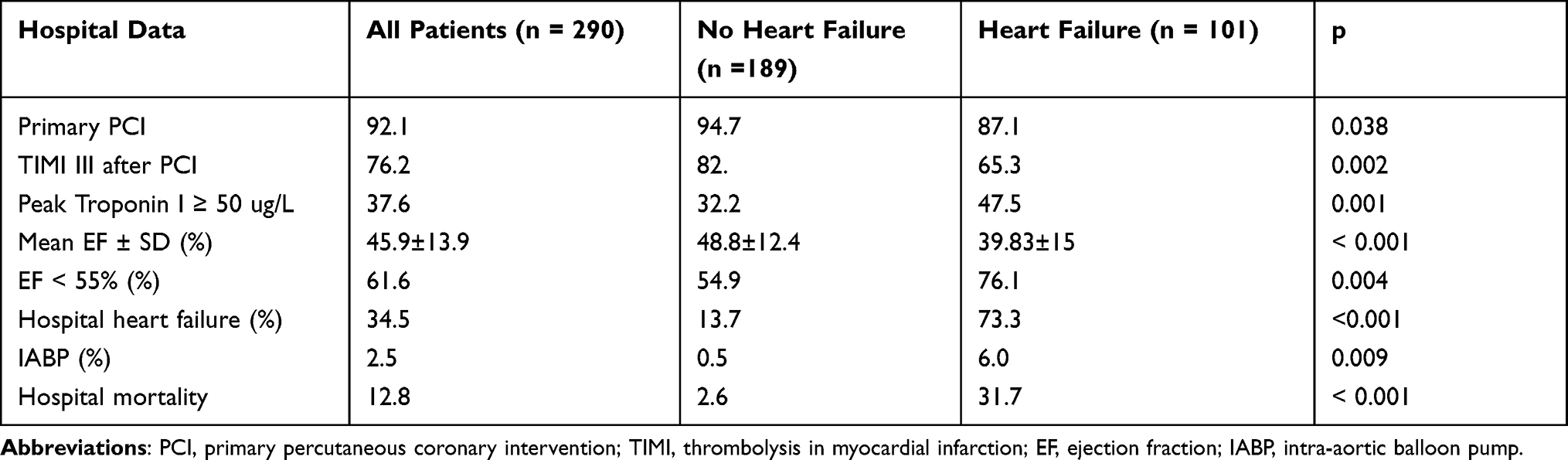 |
Table 4 Hospital Treatment and Mortality in All Included STEMI Patients and Comparison Between STEMI Patients without and with Acute Admission Heart Failure |
We observed that admission HF was associated with significantly less likely performed primary PCI, less likely achieved TIMI III flow after primary PCI, with significantly increased peak troponin I levels over 50 ug/L, significantly decreased mean EF levels, significantly more likely EF < 55% and significantly increased hospital mortality (Table 4).
Discussion
Acute admission HF in STEMI patients is multifactorial and above all the consequence of prolonged ischemia due to coronary artery occlusion. Admission HF included mild to moderate pulmonary congestion (Killip class II), pulmonary edema (Killip class III) and cardiogenic shock (Killip IV) with typical signs and symptoms or any hypotension and/or low output state of different causes (valvular dysfunction, hypovolemia, arrhythmias, right or left ventricular dysfunction); requiring iv. vasopressors to maintain normotension are included as well.14
In our STEMI patients, significant independent predictors of acute admission HF were, increased admission troponin levels, suggesting prolonged ischemia, admission LBBB and prior resuscitation, in particular in the out-of-hospital settings, and eGFR.
In STEMI patients, chronic kidney dysfunction is associated with increased risk of hospital complications such as bleeding, HF, and hospital mortality. Primary PCI in STEMI patients is usually performed before any assessment of renal function is available. Therefore, patients with chronic kidney dysfunction receive frequently increased dosing of antithrombotics and contrast agents. To prevent further acute decline in renal function, eGRF should be assessed as soon as possible, the dose of antithrombotics reduced properly, proper hydration started at least after primary PCI, and preferably low-osmolality contrast agents used in every STEMI patient.14 Acute and chronic renal dysfunction are particularly important independent determinants of hospital mortality in STEMI patients, complicated by cardiogenic shock and prolonged hypotension in spite of primary PCI, as demonstrated in several studies.14,19–21
According to studies, it mostly takes several hours – at least six, but mostly 24 hours – until shock develops with typical symptoms and signs.14 On admission, cases of hypotension or low output state with the need of iv. vasopressor and/or inotropes are frequently observed, that is often reversed after primary PCI.14 The same happened with our patients. Therefore, there was a different distribution of hospital HF in our STEMI patients – more than 13% of hospital HF did not experience HF on admission and only 2/3 of admission HF patients experienced hospital HF.
In addition, seasonal temporary short-term increase in PM2.5 over 20 ug/m3 one day prior to hospital admission was among significant independent predictors of admission acute HF in STEMI patients. In addition, acute admission HF was associated with less likely performed and less successful primary PCI, increased hospital troponin I, and increased hospital mortality.
In our patients, seasonal increase in 24-hour mean PM2.5 levels was observed mostly from January to April and from October to December 2018. Average annual exposure to PM2.5 in our area was 18 µg/m3 in the year 2018, not exceeding current 24-hour annual regulatory limits for PM2.5 of less than 25μg/m3. However, mean annual level of PM2.5 of 10 µg/m3, recommended by WHO, was exceeded in our area in 2018, even in 70 days.22
PM2.5, originating predominantly from the combustion of fossil fuels such as emissions from industrial plants or vehicles, is harmful to the cardiovascular system via several mechanisms such as autonomic imbalance with vasoconstriction and heightened arrhythmia potential, inflammation and endothelial dysfunction, prothrombotic and procoagulant changes.23,24 Underlying susceptibilities and comorbidities may determine the predominant pathways in an individual.25
The Global Burden of Disease 2010 analysis reported comparative burden of disease risk assessments from 67 risk factors. These assessments estimate that both ambient and household air pollution are among the top 10 contributors to global burden of disease, in large part because of the estimated effect of PM2.5 on ischemic heart disease.26
Elevated ambient concentration of PM2.5 may help trigger acute coronary events, including myocardial infarction and unstable angina events, mainly in persons with pre-existing coronary artery disease but not in those with nondiseased coronary arteries.12 Therefore, the population most susceptible to cardiovascular injury by PM2.5 is the elderly with pre-existing coronary atherosclerosis.27 Due to the adverse effect of air pollutants in ambient air, the European Union has developed an extensive body of legislation, establishing health based standards and objectives for a number of pollutants present in the air. Ambient Air Quality Directive of EU in 2008 guidelines for PM2.5 are mean annual levels less than 10μg/m3 and 24-hour mean level less than 25μg/m3, respectively.23,28
Additionally, we observed that STEMI patients with acute admission HF were significantly undertreated with reperfusion therapy with primary PCI and that, if performed, reperfusion therapy was even less likely successful regarding TIMI III flow after primary PCI. The consequence was significantly increased peak troponin I levels, suggesting large STEMI with increased risk for hospital mortality. This finding confirms the results of clinical studies, demonstrating that admission HF – in particular pulmonary edema or cardiogenic shock in the elderly – is an important determinant of increased mortality in STEMI population.4 GRACE registry in 2004 already demonstrated that acute HF patients were undertreated with primary PCI.4 In spite of advances within the last decade in pharmacological and interventional therapies and decreased hospital mortality of STEMI patients in general, Jeger et al in 2017 reported highest mortality and the lowest treatment rates in acute coronary syndromes (ACS) with acute HF.3 Mortality of ACS patients with acute HF remained unchanged over the last decade and was an independent predictor of in-hospital outcome in ACS patients.3 In spite of early reperfusion therapy there is still a need for additional strategies to improve the outcomes in these patients.3
According to the statement from the Acute Heart Failure Committee of the Heart Failure Association of the European Society of Cardiology from 2020, patients with confirmed ACS and acute HF are always considered a high-risk group.5 Immediate invasive strategy for STEMI is recommended. Reperfusion therapy with primary PCI should be prioritized and acute HF therapies administered in parallel to stabilize the patients.5
Conclusion
Our conclusions are that improvement in air quality represents an additional strategy to decrease the incidence of ACS in the long term and short term to decrease the incidence of acute HF in this subset of patients. Promotion of clean air should be included in preventive strategies and control of chronic diseases in every country. Compliance with legislation, better control of ambient air concentrations could protect health, cut healthcare costs, and save lives not only in countries with poor air quality but also in countries with relatively good quality air.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Puymirat E, Simon T, Steg PG, et al.; USIK USIC2000 Investigators, FAST MI Investigators. Association of changes in clinical characteristics and management with improvement in survival among patients with ST-elevation myocardial infarction. JAMA. 2012;308(10):998–1006. doi:10.1001/2012.jama.11348.
2. Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J. 2016;37(42):3232–3245. doi:10.1093/eurheartj/ehw334
3. Jeger RV, Pfister O, Radovanovic D, et al. for the AMIS-Plus Investigators. Hea rt failure in patients admitted for acute coronary syndromes: a report from a large national registry. Clin Cardiol. 2017;40:907–913. doi:10.1002/clc.22745
4. Steg PG, Dabbous OH, Feldman LJ, et al.; for the Global Registry of Acute Coronary Events (GRACE) Investigators. Determinants and prognostic impact of heart failure complicating acute coronary syndromes. Observations from the Global Registry of Acute Coronary Events (GRACE). Circulation. 2004;109(4):494–499. doi:10.1161/01.CIR.0000109691.16944.DA.
5. Harjola V-P, Parissis J, Bauersachs J, et al. Acute coronary syndromes and acute heart failure: a diagnostic dilemma and high-risk combination. A statement from the Acute Heart Failure Committee of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2020;22(8):1298–1314. doi:10.1002/ejhf.1831
6. Chen R, Kan H, Chen B, et al.; on Behalf of the CAPES Collaborative Group. Association of particulate air pollution with daily mortality: the China air pollution and health effects study. Am J Epidemiol. 2012;175(11):1173–1181. doi:10.1093/aje/kwr425.
7. Wellenius GA, Burger MR, Coull BA, et al. Ambient air pollution and the risk of acute ischemic stroke. Arch Intern Med. 2012;172(3):229–234. doi:10.1001/archinternmed.2011.732
8. Mustafic H, Jabre P, Caussin C, et al. Main air pollutants and myocardial infarction. A systematic review and meta-analysis. JAMA. 2012;307(7):713–721. doi:10.1001/jama.2012.126
9. Franklin BA, Brook R, Pope C. Air pollution and cardiovascular disease. Curr Probl Cardiol. 2015;40(5):207–238. doi:10.1016/j.cpcardiol.2015.01.003
10. Shah ASV, Langrish JP, Nair H, et al. Global association of air pollution and heart failure: a systematic review and meta-analysis. Lancet. 2013;382(9897):1039–1048. doi:10.1016/S0140-6736(13)60898-3
11. Cesaroni G, Forastiere F, Stafoggia M, et al. Long term exposure to ambient air pollution and incidence of acute coronary events: prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ. 2014;348:f7412. doi:10.1136/bmj.f7412
12. Pope CA, Muhlestein JB, Anderson JL, et al. Short-term exposure to fine particulate matter air pollution is preferentially associated with the risk of ST-segment elevation acute coronary events. J Am Heart Assoc. 2015;4(12):e002506. doi:10.1161/JAHA.115.002506
13. Milojevic A, Wilkinson P, Armstrong B, Bhaskaran K, Smeeth L, Hajat S. Short-term effects of air pollution on a range of cardiovascular events in England and Wales: case-crossover analysis of the MINAP database, hospital admissions and mortality. Heart. 2014;100(14):1093–1098. doi:10.1136/heartjnl-2013-304963
14. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177.
15. Ponikowsli P, Voors AA, Anker SD, et al.; ESC Scientific Document Group. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200.
16. Killip T, Kimball JT. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am J Cardiol. 1967;20(4):457–464. doi:10.1016/0002-9149(67)90023-9
17. Levey AS, Stevens LA, Schmid CH, et al.; for the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI). A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006.
18. Chemical analytic laboratory of environmental agency of Republic Slovenia (ARSO). Avalable from: https://www.arso.gov.si/en/about%20the%20agency/laboratories/.
19. Hayıroğlu Mİ, Keskin M, Uzun AO, et al. Predictors of in-hospital mortality in patients with ST-segment elevation myocardial infarction complicated with cardiogenic shock. Heart Lung Circ. 2019;28(2):237–244. doi:10.1016/j.hlc.2017.10.023
20. Çinar T, Hayiroğlu Mİ, Şeker M, et al. The predictive value of age, creatinine, ejection fraction score for in-hospital mortality in patients with cardiogenic shock. Coron Artery Dis. 2019;30(8):569–574. doi:10.1097/MCA.0000000000000776
21. Hayıroğlu Mİ, Çanga Y, Yıldırımtürk Ö, et al. Clinical characteristics and outcomes of acute coronary syndrome patients with intra-aortic balloon pump inserted in intensive cardiac care unit of a tertiary clinic. Turk Kardiyol Dern Ars. 2018;46(1):10–17. doi:10.5543/tkda.2017.11126
22. ARSO Okolje. Kakovost zraka v Sloveniji v 2018. Available from: https://www.arso.gov.si/zrak/kakovost%20zraka/poro%C4%8Dila%20in%20publikacije/kakovost_letna.html.
23. Peters A, Fröhlich M, Döring A, et al. Particulate air pollution is associated with an acute phase response in men; results from the MONICA-Augsburg Study. Eur Heart J. 2001;22(14):1198–1204. doi:10.1053/euhj.2000.2483
24. Brook R, Rajagopalan S, Pope A, et al. Particulate matter air pollution and cardiovascular disease an update to the scientific statement from the American Heart Association. Circulation. 2010;121(21):2331–2378. doi:10.1161/CIR.0b013e3181dbece1
25. Bai L, Shin S, Burnett RT, et al. Exposure to ambient air pollution and the incidence of congestive heart failure and acute myocardial infarction: a population-based study of 5.1 million Canadian adults living in Ontario. Environ Int. 2019;132:105004. doi:10.1016/j.envint.2019.105004
26. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–2260.
27. Wang C, Tu Y, Yu Z, Lu R. PM2.5 and cardiovascular diseases in the elderly: an overview. Int J Environ Res Public Health. 2015;12(7):8187–8197. doi:10.3390/ijerph120708187
28. European Environment Agency 2018. Air quality in Europe — 2018 report. Available from: https://www.eea.europa.eu/publications/air-quality-in-europe-2018.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.