")
Back to Journals » International Journal of General Medicine » Volume 16
The Role of CT Scan in Pediatric Airway Foreign Bodies
Authors Wang ML, Png LH , Ma J, Lin K, Sun MH, Chen YJ, Tang XC, Bi XY, Gao YQ, Zhang TS
Received 16 December 2022
Accepted for publication 9 February 2023
Published 15 February 2023 Volume 2023:16 Pages 547—555
DOI https://doi.org/10.2147/IJGM.S398727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Woon-Man Kung
Mei-Lan Wang,1,* Lu Hui Png,2,* Jing Ma,1 Ken Lin,1 Mei-hua Sun,1 Yi-Jun Chen,3 Xian-Chao Tang,4 Xian-Yun Bi,1 Ying-Qin Gao,1 Tie-Song Zhang1
1Department of Otolaryngology, Head and Neck Surgery, Kunming Children’s Hospital, Kunming, People’s Republic of China; 2Department of Otorhinolaryngology – Head and Neck Surgery, Singapore General Hospital, Singapore, Singapore; 3Department of Otolaryngology, Head and Neck Surgery, Kunming Children’s Hospital, Kunming Medical University, Kunming, People’s Republic of China; 4Department of Radiology, Kunming Children’s Hospital, Kunming, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lu Hui Png; Tie-Song Zhang, Email [email protected]; [email protected]
Objective: We aim to determine the utility of CT scan as a method to accurately confirm pediatric airway foreign bodies (AFBs), the current gold standard of which is chest X-ray as the primary imaging modality in the investigation screening of AFBs with progression to microlaryngobronchoscopy.
Methods: A retrospective cohort study of children diagnosed with suspected AFBs between July 2019 and June 2020 was conducted. The primary outcome of missed AFBs from radiologic investigations was recorded.
Results: A total of 226 children with an average age of 1.94 years were included in this study. One hundred and two children were eventually admitted to the hospital for microlaryngobronchoscopy. A total of 89 cases were initially examined by chest X-ray with the diagnosis confirmed in 26 cases. The initial examination was chest CT scan in 105 cases, of which the diagnosis was confirmed in 46 cases. The initial examination was chest CT scan with airway reconstruction in 32 cases, and the diagnosis was confirmed in 17 cases. Patients with negative chest CT scan with airway reconstruction were observed to have resolution of symptoms with no further need for bronchoscopy.
Conclusion: Chest CT scan with airway reconstruction had the highest rate of confirmed diagnosis of pediatric AFBs on initial scanning, followed by chest CT scan, and finally chest X-ray with fluoroscopy; there was no missed diagnosis in chest CT scan with airway reconstruction. Chest CT scan with airway reconstruction can accurately and quickly detect AFBs and reduce unnecessary bronchoscopy.
Keywords: airway foreign body, chest X-ray, chest CT scan, airway reconstruction, microlaryngobronchoscopy
Introduction
Seven percent of sudden deaths in children under 4 years of age are due to airway foreign bodies (AFBs), with tracheal foreign bodies being one of the most common emergencies in clinical departments such as otolaryngology, pediatrics, respiratory medicine and emergency medicine.1–3 Foreign bodies can lodge in various locations such as the throat, trachea or bronchi causing symptoms such as cough, shortness of breath or hoarseness, and can be associated with severe respiratory distress. 94.8% of tracheal foreign bodies occur in children between the ages of 4 months and 3 years old, with younger children being more likely to inhale a foreign body and delayed diagnosis of tracheal foreign bodies leading to serious acute and chronic complications.4 Early diagnosis is effective in reducing complications and decreasing mortality.5
What is Already Known on the Subject?
Current clinical guidelines recommend chest X-ray as the primary imaging modality in the screening of AFBs with progression to microlaryngobronchoscopy in the event of a negative scan with ongoing suspicion for aspiration.6 However, bronchoscopy presents with many risks including that of general anesthesia and inherent procedural risks such as bleeding and airway injury.
What This Study Adds?
In this study, we seek to investigate the utility of CT scanning as an alternative to microlaryngobronchoscopy in confirming the presence of pediatric AFBs.
Materials and Methods
Clinical Information
The clinical records of 226 children seen in our outpatient clinic in Kunming Children’s Hospital, the largest tertiary pediatric hospital in Yunnan Province, with the diagnoses of suspected AFBs between July 2019 and June 2020 were retrospectively reviewed. Records were reviewed in particular looking at the primary outcome of missed AFBs during radiologic investigations. Other clinical information examined included demographics, duration of symptoms prior to presentation, and lung auscultation characteristics.
No statistical evaluation was performed because of the small number of patients in different diagnostic groups. Therefore, the relationship between discrete variables was investigated using absolute numbers only.
This study complies with the Declaration of Helsinki and was approved by the Kunming Children’s Hospital Institutional Review Board (approval number 2022-03-395-K01).
Radiological Investigations and Post-Processing Techniques
Chest X-Ray
Chest X-ray with fluoroscopy was performed using GMM T30CS digital gastrointestinal X-ray machine. Children under 3 years old had chest X-ray performed in supine position with the long axis of the body parallel to the long axis of the examination bed, and the image was acquired by capturing images during the inspiratory phase. Children over 3 years old had chest X-ray performed in standing, anterior-posterior position with the back close to the detector. Chest fluoroscopy was performed in supine position with inspiratory and expiratory phases examined by observing chest rise and fall.
Plain Chest CT Scan
Plain chest CT scan was performed using GE Optima 660 64-row spiral CT scanner with tube voltage 100/120kv, fixed tube current adjusted according to the age of the child (<1 year old: 120mA; 1–5 years old 130mA; 5–10 years old: 140mA; >10 years old 150mA), pitch 0.984:1, image layer thickness 5mm. Sedation was given for patients uncooperative with CT scanning.
Chest CT Scan with Airway Reconstruction
Chest CT scan with airway reconstruction was performed using GE Optima 660 64-row spiral CT scanner with tube voltage 100/120kv, fixed tube current adjusted according to the age of the child (<1 year old: 120mA; 1–5 years old: 130mA; 5–10 years old: 150mA; >10 years old 160mA), pitch 0.984:1, image layer thickness 3.75 mm, reconstruction thin layer thickness 0.625mm. 3D reconstruction was performed by transferring thin layer data to the post-processing workstation and applying CT post-processing.
Imaging Algorithm
Different imaging modalities were selected in the outpatient clinic for initial imaging after consultation. Chest x-ray with fluoroscopy, plain chest CT scan and chest CT scan with airway reconstruction were chosen as options for initial imaging depending on physician preference, with a more detailed scan being performed in succession if suspicion for AFBs was still present despite negative previous scans. Hierarchy for successive scanning from less detailed to more detailed was as such: chest x-ray with fluoroscopy then chest CT scan then chest CT scan with airway reconstruction (Figure 1). Children with negative chest X-ray with fluoroscopy but still suspected of AFBs underwent plain chest CT scan for further evaluation while children with negative plain chest CT scan but still suspected of AFBs underwent chest CT scan with airway reconstruction. Patients with negative scans and low suspicion of AFBs had close follow-up for 12 months to ensure no complications from undiagnosed foreign bodies occurred. These follow-ups include monthly patient reviews, focusing on detailed history taking and clinical examination.
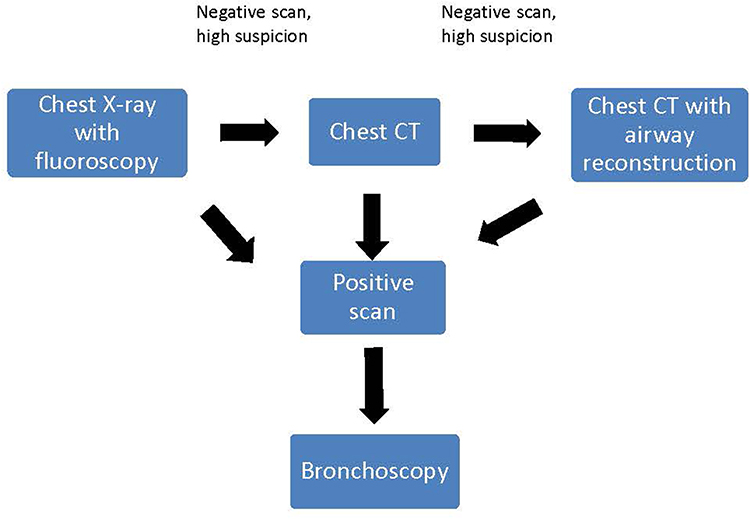 |
Figure 1 Algorithm for initial imaging. |
Bronchoscopy and Foreign Body Removal
After radiologic confirmation of AFBs, children were examined via microlaryngobronchoscopy (Storz, Germany) under general anesthesia with detected AFBs removed in the same setting. Patients were given general anesthesia with propofol, vecuronium, fentanyl, penehyclidine hydrochloride and inhaled sevoflurane. Once a foreign body was found, it was removed with various grasping forceps depending on the type and size of the foreign body with the tracheobronchial tree re-examined by another senior physician to ensure that no AFBs remained.
Results
There were 147 (65%) males and 79 (35%) females with ages ranging between 1 month and 13 years old and a mean age of 1.94 years. Duration of symptoms prior to presentation ranged from 0.5 hours to 1 year and 8 months with a mean duration of symptoms prior to presentation of 16.31 days. Lung auscultation characteristics were analyzed with 195 (86.3%) cases of abnormal breath sounds noted on auscultation. There were 60 (26.5%) cases of decreased breath sounds unilaterally and 19 (8.4%) cases of decreased breath sounds bilaterally. One hundred and fifty-one (66.8%) cases had dry rales or wheezing sounds noted on auscultation. Symptomatically, 173 (76.5%) patients had cough and wheezing, 14 (6.2%) patients had dyspnea, 31 (13.7%) patients had fever, and 4 (1.8%) patients had hoarseness at the time of consultation.
Initial imaging included chest X-ray with fluoroscopy in 89 (39.4%) cases, with the diagnosis confirmed in 26 (11.5%) cases on initial scan, 10 (4.4%) cases on subsequent scanning with chest CT scan, and 1 (0.4%) case after final scanning using chest CT scan with airway reconstruction. The initial examination was chest CT scan in 105 (46.5%) cases, with the diagnosis confirmed in 46 (20.4%) cases on initial scan and 2 (0.9%) cases on chest CT scan with airway reconstruction. The initial examination was chest CT scan with airway reconstruction in 32 (14.2%) cases, with the diagnosis was confirmed in 17 (7.5%) cases on initial scan (Table 1).
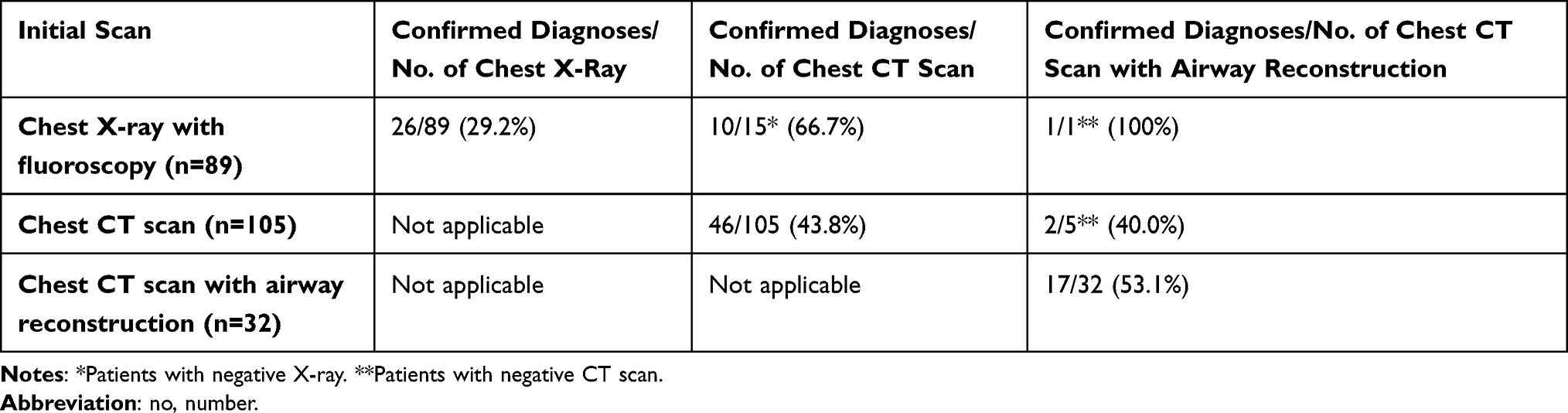 |
Table 1 Progression of Scans and Rates of Confirmed Diagnoses |
One hundred and two (45.1%) cases were highly suspicious for AFBs on radiological investigation and underwent microlaryngobronchoscopy with 101 (44.7%) cases confirming foreign bodies and 1 (0.4%) case showing tracheal collapse. Of the removed foreign bodies, there were 89 cases of plant-based foreign bodies (88.0%); 2 cases of animal-based foreign bodies (2.0%); 4 cases of metal-based foreign bodies (4.0%); 4 cases of synthetic foreign bodies (4.0%), and 2 cases of endogenous foreign bodies (2.0%) (Table 2). One child presented with severe respiratory distress on initial presentation and had foreign body removal performed emergently under sedation in the emergency department. Unique cases are highlighted in Figures 2–7.
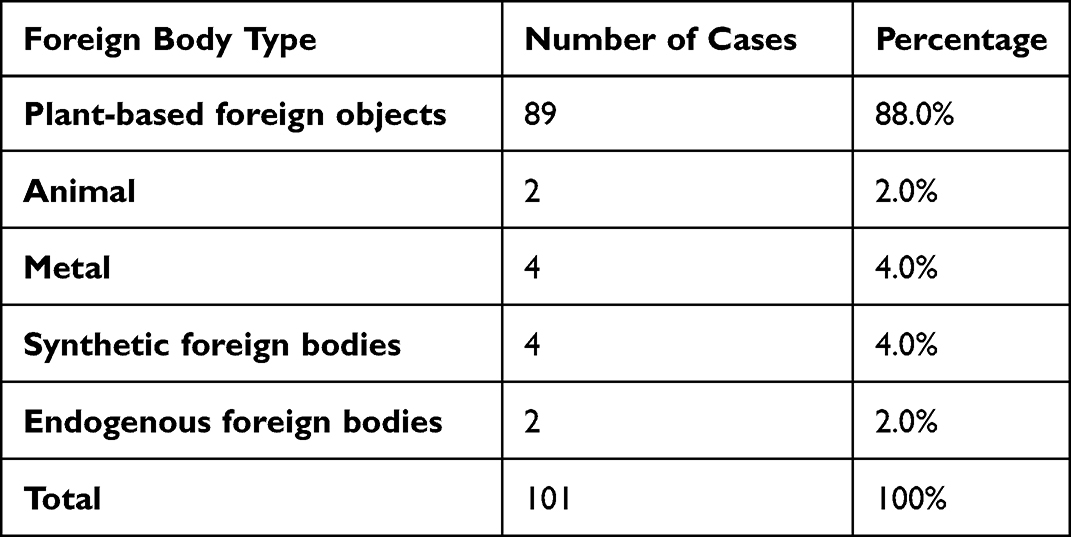 |
Table 2 Distribution of Foreign Body Types |
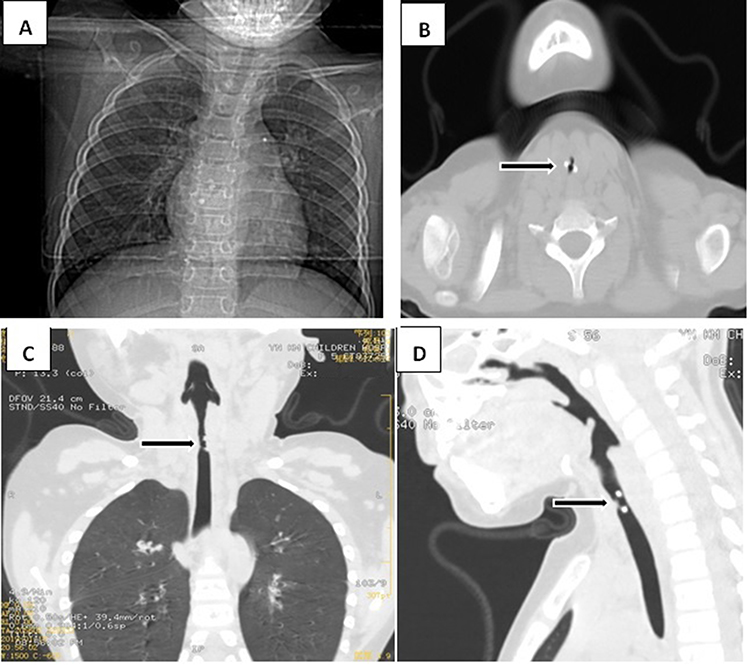 |
Figure 2 5-year-old girl presented to the clinic with recurrent cough for 5 days. A chest X-ray performed did not show any signs of a foreign body. Further chest CT scan with airway reconstruction revealed a high-density ring-like foreign body within the trachea. |
 |
Figure 3 2-year-old boy presented with history of recurrent cough. The chest X-ray and chest fluoroscopy done showed no abnormality. After 26 days of symptomatic treatment, the recurrent cough did not improve and a chest CT scan with airway reconstruction was performed, suggesting a foreign body in the left main bronchus. One piece of crushed pea was removed from the left bronchus intra-operatively. |
 |
Figure 4 4-year-old boy presented with a recurrent cough for 2 weeks. Chest X-ray showed slightly increased translucency in the right lung, with no other abnormality seen. Further chest CT scan with airway reconstruction was performed, showing narrowing of the bronchial opening in the lower lobe of the left lung which was also seen to be filled with a high-density focus. Bronchoscopy was performed with purulent secretions seen and removed from the lower lobe of the left lung, resolving the cough. |
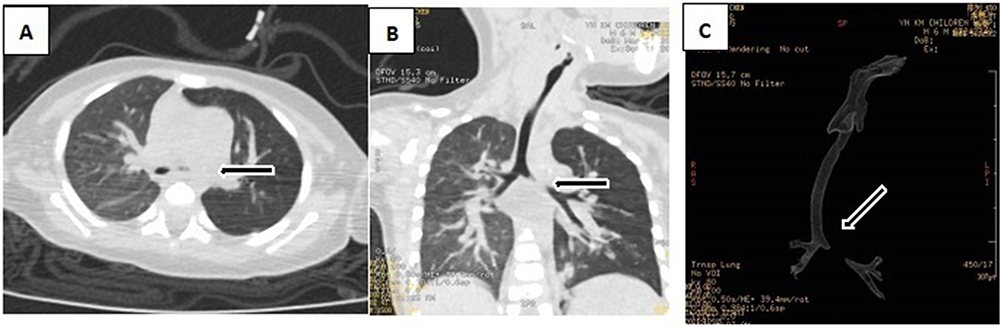 |
Figure 5 6-month-old child presented with cough and wheezing for 7 days. On auscultation, the breath sounds in the left lung were significantly reduced. Chest CT scan with airway reconstruction showed increased translucency of the left lung, with multiple patchy high-density shadows bilaterally. On bronchoscopy, a small amount of sputum was seen in the left main bronchus with the left main bronchus softened and collapsed causing obstruction. |
 |
Figure 6 1-year 6 month-old boy presented to the hospital with coughing and wheezing for 1 month after choking on a meal. At the time of presentation, the breath sounds of the left lung were reduced on auscultation with chest X-ray and chest fluoroscopy showing increased translucency of the left lung. Bronchoscopy was performed with several pieces of crushed peanuts noted and removed from the left main bronchus. |
 |
Figure 7 1-year 3 month-old girl was seen for 8 days for coughing and wheezing after choking on peanuts with no obvious abnormality seen on chest X-ray and chest fluoroscopy. Chest CT scan with airway reconstruction performed showed irregular, dotted soft tissue density foci in the proximal segment of the right main bronchus. Bronchoscopy was performed with several pieces of crushed peanuts noted and removed from the right main bronchus. |
Discussion
The majority of children with tracheal and bronchial foreign bodies are not expediently diagnosed until 24 hours after aspiration as AFBs are easily missed and misdiagnosed.7 Shorter durations of foreign body retention usually result in only superficial bronchial injury, but after 5 days of retention, serious injury to the lung parenchyma can occur with extent of injury directly correlating to duration of foreign body retention.8 Therefore, early diagnosis and removal of these foreign bodies is important to avoid severe respiratory complications.
However, the diagnosis of AFBs remains a challenge for physicians and delayed diagnosis tends to be a recalcitrant problem with 17–69% of patients being diagnosed more than 7 days after foreign body aspiration.9 Currently, the gold standard for diagnosis of pediatric AFBs is bronchoscopy.10 Prompt diagnosis depends heavily on the first physician seen and clinical history is the most important factor in the early diagnosis of a foreign body in the airway. The history of a choking episode can usually be obtained from the parent or caregiver, and it has been reported that 72% of children with AFBs have a history of choking.11 It is important to note that the absence of a choking event does not exclude a foreign body and may be a risk factor for delayed diagnosis.11,12 Therefore, precise adjunctive examination modalities such as radiological investigations can be critical to clinch the diagnosis.
In general, chest CT scan demonstrates a high sensitivity (94.0%). Compared with other techniques such as chest X-ray, plain chest CT scan has a potentially shorter examination time and finer image detail to clearly detect the location, size and shape of AFBs. Therefore, chest CT scans have excellent potential utility in investigating suspected AFBs, avoiding unnecessary bronchoscopy and associated morbidities.13 However, it is important to note that a chest CT scan also has certain disadvantages. First, it cannot be used as a therapeutic tool to remove foreign bodies as compared to microlaryngobronchoscopy which has both diagnostic and therapeutic capabilities. Secondly, various pathologies such as mucus plugging, airway infection, airway tumors, tracheobronchial malacia and tracheobronchial stenosis may all still lead to false positives. In our series, there were two cases in which an external foreign body was suspected on chest CT scan with airway reconstruction, of which both were confirmed to be endogenous sputum plugs on subsequent bronchoscopy. Another case of a false-positive examination was that of a 6-month-old child whose chest CT scan with airway reconstruction suggested a foreign body initially. Intra-operative examination revealed tracheomalacia resulting in a collapsed tracheal segment which masqueraded as the foreign body on airway reconstruction, illustrating our previous point. Radiological investigations are not a replacement for good clinical judgment, and it is important to remember the potential risks of radiation in children and apply these scans judiciously. Low-dose CT scans have more recently been proposed for the diagnosis of AFBs. These CT scans are useful for the diagnosis of inhaled AFBs in children because of the lower absorption of radiation as well as lower image noise compared to adults when the same scan parameters are used.14 The use of multi-detector CT scanners with a low-dose protocol reduces exposure to ionizing radiation to 1–3 mSv.15 We are cognizant of the risks of radiation in children, and hence the low-dose protocol would potentially be preferred to mitigate the aforementioned risk.16
Current clinical guidelines recommend chest X-ray as the primary investigation modality in AFBs, with bronchoscopy indicated in patients with a negative scan but still having a high index of suspicion for a foreign body.6,17 In an effort to reduce the incidence of delayed diagnosis and complications associated with these AFBs, bronchoscopy tends to be overused in some healthcare facilities. This may result in waste of medical resources as well as procedural related complications such as bronchospasm, hypoxemia, bronchial laceration, laryngeal edema, pneumothorax, cardiac arrest and other anesthesia-related risks.13 It has been reported in the literature that the reconstructed 3D images of multi-detector chest CT scanners can improve the sensitivity (100%) and specificity (81–100%) of diagnosis,18 a finding which is consistent with our results. Having a chest CT scan with airway reconstruction performed can instill a higher degree of confidence in the attending clinician in the instance of a negative scan, avoiding an unnecessary procedure. In our series, patients who had negative airway reconstruction and were still a suspect case were continually observed and all had subsequently resolved symptoms, avoiding bronchoscopy. In the event of a patient having persistent symptoms, plans for follow-up bronchoscopy were made.
It is interesting to note that in our series, the mean duration of symptoms prior to presentation was 16.31 days, with one child even presenting after 1 year and 8 months of symptoms before a diagnosis of a foreign body was made. These are much longer periods compared to modern Western standards, and we attribute this to the fact that our catchment area of patients is that of a rural district with families generally having lower socioeconomic statuses. Due to poorer education in the area, many children and parents are unaware of the symptoms and risks of AFBs and continue with their daily activities despite a history of foreign body aspiration. An unclear medical history is one of the main reasons for delayed diagnosis and treatment.19 Failure of the guardian to provide an accurate history of foreign body inhalation makes diagnosis more difficult, prolongs the length of visit and increases the incidence of surgical complications.20 Other factors include community physicians tending to lack the necessary experience in the diagnosis and management of AFBs, easily misdiagnosing them as lung infections or asthma. Early, accurate diagnosis by the community physician can lead to prompt referral to the tertiary hospital, reducing length of stay. Therefore, education on AFBs for both the public and community physician is critical in the management of this condition.4,21 If guardians have the relevant knowledge and take effective first aid measures before the consultation, patients can gain valuable time for medical resuscitation, reducing the incidence of mortality caused by AFBs. On stabilization, the child should present to the hospital as early as possible and a history of foreign body aspiration should be promptly provided to the attending physician to allow for early intervention.22
Conclusion
In this article, we explore the accuracy of various radiological investigations used to diagnose AFBs in infants and children. Although chest radiographs are usually considered the first-line radiological investigation, the presence of a foreign body cannot be ruled out when the chest radiograph does not show any abnormality. Chest CT scans with airway reconstruction are highly sensitive in detecting AFBs as well as associated airway and parenchymal complications, avoiding unnecessary bronchoscopy. This presents as an alternative, solitary investigation for patients who would have otherwise needed both a screening chest radiograph and diagnostic bronchoscopy, reducing unnecessary complications, diagnostic delay and cost.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declare that they have no conflicts of interest.
References
1. Metrangelo S, Monetti C, Meneghini L, et al. Eight years’ experience with foreign-body aspiration in children: what is really important for a timely diagnosis? J Pediatr Surg. 1999;34(8):1229–1231. doi:10.1016/S0022-3468(99)90157-4
2. Black RE, Johnson DG, Matlak ME. Bronchoscopic removal of aspirated foreign bodies in children. J Pediatr Surg. 1994;29:682–4.3. doi:10.1016/0022-3468(94)90740-4
3. Mantor PC, Tuggle DW, Tunell WP. An appropriate negative bronchoscopy rate in suspected foreign body aspiration. Am J Surg. 1989;158(6):622–624. doi:10.1016/0002-9610(89)90208-0
4. Gao YQ, Tan JL, Wang ML, et al. How can we do better? Learning from 617 pediatric patients with airway foreign bodies over a 2-year period in an asian population. Front Pediatr. 2020;8:578. doi:10.3389/fped.2020.00578
5. Alhamad M, Alnahwi T, Alshayeb H, et al. Medical emergencies encountered in dental clinics: a study from the Eastern Province of Saudi Arabia. J Family Community Med. 2015;22(3):175–179. doi:10.4103/2230-8229.163038
6. The Royal Children’s Hospital Melbourne (RCH). Clinical Practice Guidelines: Foreign Bodies Inhaled [Internet]. Melbourne: The Royal Children’s Hospital Melbourne (RCH); 2021. Available from: https://www.rch.org.au/clinicalguide/guideline_index/Foreign_bodies_inhaled/.
7. Chai J, Wu XY, Han N, et al. A retrospective study of anesthesia during rigid bronchoscopy for airway foreign body removal in children: propofol and sevoflurane with spontaneous ventilation. Paediatr Anaesth. 2015;24(10):1031–1036. doi:10.1111/pan.12509
8. Hughes CK, Christensen CL, Maturo SC, et al. Organic vs inorganic tracheobronchial airway foreign body aspiration: does type/duration matter? Laryngoscope. 2020;131(3):490–495. doi:10.1002/lary.29006
9. Lima JAB, Fischer GB. Foreign body aspiration in children. Paediatr Respir Rev. 2002;3(4):303–307. doi:10.1016/S1526-0542(02)00265-8
10. Yadav SP, Singh J, Aggarwal N, et al. Airway foreign bodies in children: experience of 132 cases. Singapore Med J. 2007;48(9):850–853.
11. Tomaske M, Gerber AC, Stocker S, et al. Tracheobronchial foreign body aspiration in children - diagnostic value of symptoms and signs. Swiss Med Wkly. 2006;136(33–34):533–538. doi:10.4414/smw.2006.11459
12. Pinto A, Scaglione M, Pinto F, et al. Tracheobronchial aspiration of foreign bodies: current indications for emergency plain chest radiography. Radiol Med. 2006;111(4):497–506. doi:10.1007/s11547-006-0045-0
13. Shen J, Huang L, Hao C. Value of MSCT for diagnosis of tracheobronchial foreign body aspiration in children: 5-year retrospective study. Pediatr Int. 2020;62(10):1184–1188. doi:10.1111/ped.14269
14. Sun HF, Zhang HY, Ding CM. CT imaging findings of primary tracheal tumors and its diagnostic value. Chin J CT MRI. 2016;14(2):35–38.
15. Brisse HJ, Aubert B. CT exposure from pediatric MDCT: results from the 2007–2008 SFIPP/ISRN survey. J Radiol. 2009;90(2):207–215. doi:10.1016/S0221-0363(09)72471-0
16. Hintenlang KM, Williams JL, Hintenlang DE. A survey of radiation dose associated with pediatric plain-film chest x-ray examinations. Pediatr Radiol. 2002;32(11):771–777. doi:10.1007/s00247-002-0734-3
17. Mallick MS. Tracheobronchial foreign body aspiration in children: a continuing diagnostic challenge. Afr J Paediatr Surg. 2014;11(3):225–228. doi:10.4103/0189-6725.137330
18. Bhat KV, Hegde JS, Nagalotimath US, Patil GC. Evaluation of computed tomography virtual bronchoscopy in paediatric tracheobronchial foreign body aspiration. J Laryngol Otol. 2010;124(8):875–879. doi:10.1017/S0022215110000769
19. Reilly J, Thompson J, MacArthur C, et al. Pediatric aerodigestive foreign body injuries are complications related to timeliness of diagnosis. Laryngoscope. 1997;107(1):17–20. doi:10.1097/00005537-199701000-00006
20. Shlizerman L, Mazzawi S, Rakover Y, et al. Foreign body aspiration in children: the effects of delayed diagnosis. Am J Otolaryngol. 2010;31(5):320–324. doi:10.1016/j.amjoto.2009.03.007
21. Celik N, Arikan D. The effect of the training given to the child development students about foreign body aspiration upon their knowledge levels. Int J Pediatr Otorhinolaryngol. 2013;77(11):1811–1817. doi:10.1016/j.ijporl.2013.08.010
22. Skoulakis CE, Doxas PG, Papadakis CE, et al. Bronchoscopy for foreign body removal in children. A review and analysis of 210 cases. Int J Pediatr Otorhinolaryngol. 2000;53(2):143–148. doi:10.1016/S0165-5876(00)00324-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.