Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
The Role of Computed Tomography and Artificial Intelligence in Evaluating the Comorbidities of Chronic Obstructive Pulmonary Disease: A One-Stop CT Scanning for Lung Cancer Screening
Authors Lin X, Zhang Z ![]() , Zhou T, Li J, Jin Q, Li Y, Guan Y
, Zhou T, Li J, Jin Q, Li Y, Guan Y ![]() , Xia Y, Zhou X, Fan L
, Xia Y, Zhou X, Fan L ![]()
Received 26 November 2024
Accepted for publication 25 April 2025
Published 6 May 2025 Volume 2025:20 Pages 1395—1406
DOI https://doi.org/10.2147/COPD.S508775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Xiaoqing Lin,1,2,* Ziwei Zhang,1,* Taohu Zhou,1 Jie Li,1,2 Qianxi Jin,1 Yueze Li,1 Yu Guan,1 Yi Xia,1 Xiuxiu Zhou,1 Li Fan1
1Department of Radiology, Second Affiliated Hospital of Naval Medical University, Shanghai, People’s Republic of China; 2College of Health Sciences and Engineering, University of Shanghai for Science and Technology, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Fan, Email [email protected]
Abstract: Chronic obstructive pulmonary disease (COPD) is a major cause of morbidity and mortality worldwide. Comorbidities in patients with COPD significantly increase morbidity, mortality, and healthcare costs, posing a significant burden on the management of COPD. Given the complex clinical manifestations and varying severity of COPD comorbidities, accurate diagnosis and evaluation are particularly important in selecting appropriate treatment options. With the development of medical imaging technology, AI-based chest CT, as a noninvasive imaging modality, provides a detailed assessment of COPD comorbidities. Recent studies have shown that certain radiographic features on chest CT can be used as alternative markers of comorbidities in COPD patients. CT-based radiomics features provided incremental predictive value than clinical risk factors only, predicting an AUC of 0.73 for COPD combined with CVD. However, AI has inherent limitations such as lack of interpretability, and further research is needed to improve them. This review evaluates the progress of AI technology combined with chest CT imaging in COPD comorbidities, including lung cancer, cardiovascular disease, osteoporosis, sarcopenia, excess adipose depots, and pulmonary hypertension, with the aim of improving the understanding of imaging and the management of COPD comorbidities for the purpose of improving disease screening, efficacy assessment, and prognostic evaluation.
Keywords: chronic obstructive pulmonary disease, COPD, cardiovascular disease, CVD, lung cancer, osteoporosis, computed tomography, CT
Introduction
Chronic obstructive pulmonary disease (COPD) ranks as the third most common cause of death globally, distinguished by its progressive and irreversible airflow restriction.1 Economically, the disease imposes a heavy burden on health care, with billions of dollars in direct medical costs and productivity losses annually.2 Although COPD mainly affects the lungs, it is a complex multicomponent disease characterized by chronic systemic inflammation, which often coexists with other diseases, called comorbidities, mainly including lung cancer, cardiovascular disease (CVD), osteoporosis, and so on. The underlying mechanisms of COPD and its comorbidities remain incompletely understood.3 Notably, the risk of hospitalization and mortality in patients with COPD is closely related to its comorbidities, and the risk of some comorbidities increases with the frequency of acute exacerbations of COPD.4,5 There is some positive feedback between the two. In China, the prevalence of COPD in adults over 40 years of age is 13.7%, but the disease awareness rate is less than 1%, and there is a large blind spot in the publicity and management of COPD comorbidities.6,7
Due to the high prevalence and negative impact of comorbidities in the COPD population, effective screening and management can improve outcomes and quality of life in the disease population. COPD disease management strategies fail to provide clear recommendations on how to assess and manage comorbidities.3 The current gold standard for diagnosing and evaluating COPD is the pulmonary function test (PFT).8 Yet, PFT can only reflect the global lung function changes in COPD patients, not the focal changes and comorbidities. In recent years, advanced imaging techniques—including cardiac MRI and Single Photon Emission Computed Tomography (SPECT)—have been widely adopted for assessing COPD-related complications such as cardiovascular disease (CVD) and lung cancer. However, their clinical utility is constrained by significant limitations, notably prolonged scan durations and high costs.9,10 In the era of large-scale lung cancer screening (LCS), chest CT, which can locate and characterize the pathological abnormalities of chest diseases, has a high prevalence rate in major diseases.11 As a non-invasive tool, CT is of great clinical value in the early diagnosis, monitoring, and follow-up of diseases in primary medical units. It can be used for long-term disease management of COPD comorbidities and maximize cost-effectiveness with promising one-stop scanning.
Artificial Intelligence (AI) is the technology that displays human intelligence through computer programs, capable of using algorithms to analyze a large amount of reliable data, automatically learning the hidden information in the data, and making predictions about unknown events in the real world.12 The application of AI-based systems has been reported to excel in early screening, staged diagnosis, and prognosis of many chest diseases while reducing the workload of radiologists and maintaining diagnostic accuracy.13–17 As AI technology leveraging CT imaging progresses rapidly, CT has emerged as a highly potent and widely utilized diagnostic tool, offering immense promise in identifying and managing COPD comorbidities. Especially in the absence of standardized screening guidelines, the integration of AI-based tools would be helpful. However, data bias and model generalizability make AI challenging that need to be validated by in-depth research.18 In this paper, we have conducted a comprehensive review of the research progress on various comorbidities of COPD, including lung cancer, CVD, osteoporosis, sarcopenia, excess adipose depots, and pulmonary hypertension, from the perspectives of CT and AI. Research on the application of CT in COPD comorbidities is shown in Table 1.
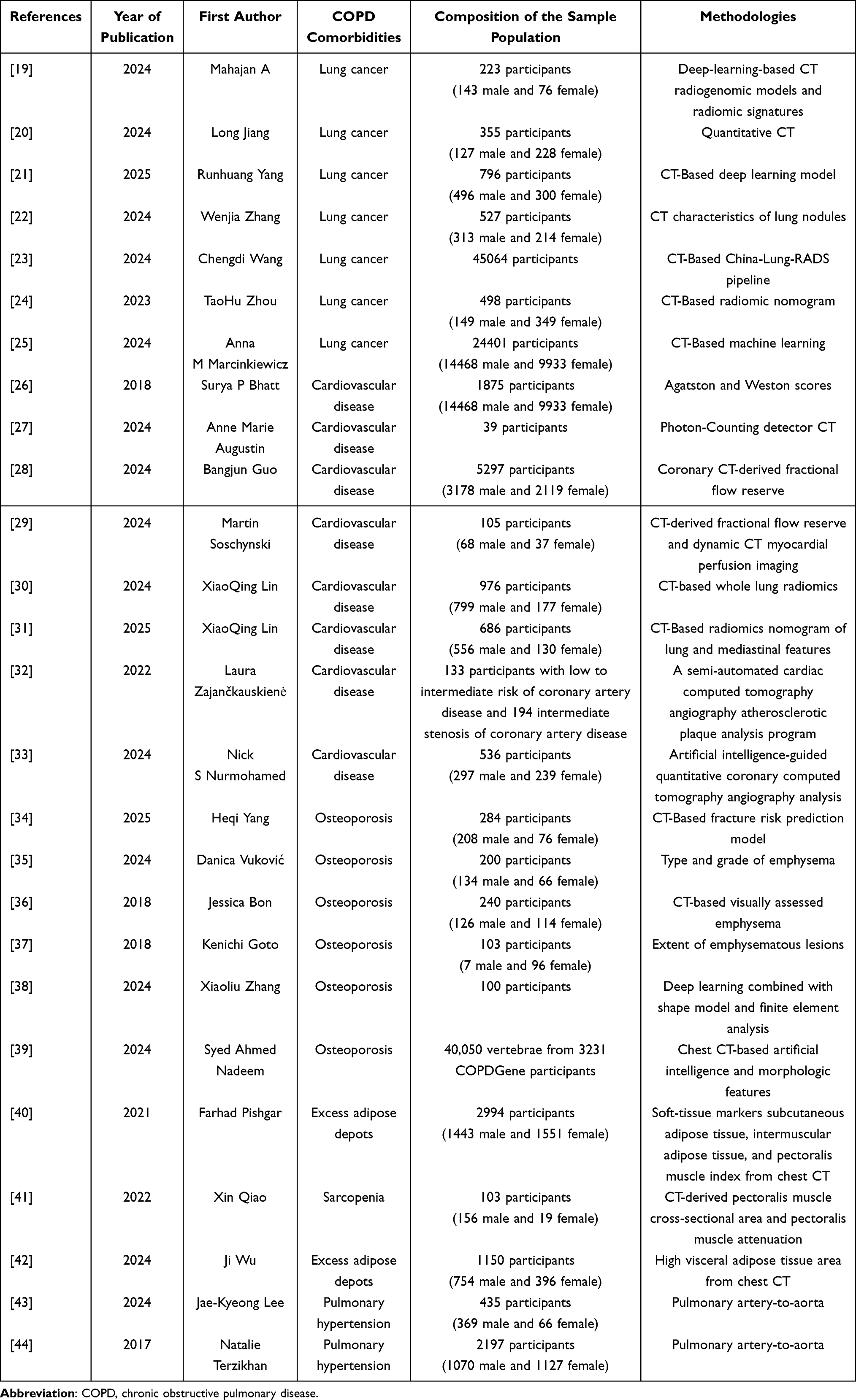 |
Table 1 Research on the Application of CT in COPD Comorbidities |
COPD and Lung Cancer
Many patients with lung cancer have a history of COPD.45 Lung cancer is a common complication of COPD, while COPD is considered an important risk factor for lung cancer.46,47 COPD and lung cancer share common risk factors such as tobacco intake, DNA damage pathways, immune microenvironments, inflammation, and imbalanced proteases/antiproteases.48–50 Smokers who have COPD are at a three to six times higher risk of developing lung cancer compared to non-smokers with COPD, with a lung cancer incidence of 0.8 to 1.7%/year.51 The occurrence of acute exacerbations in COPD patients increased the risk of lung cancer development by 2.77 times.52 The majority of the patients affected with lung cancer are common diagnosed at an advanced stage and Lung cancer appears frequently in patients with COPD.53–55 Since patients with COPD undergo regular checkups in the hospital, it is reasonable to assume that lung cancer patients with COPD can hopefully be detected earlier in the clinical practice compared to patients without COPD. However, the overlapping symptoms of lung cancer and COPD may also lead to a delay in the diagnosis of lung cancer when patients with known COPD experience worsening symptoms of lung disease.8,47,56 Lung cancer diagnosis and staging using an electronic nose (e-nose) based on machine learning is an emerging field in medical electronics with a diagnostic accuracy of 91.67%.57,58 However, when applying the algorithm to other disease cohorts in a blinded fashion, the specificity of e-nose for LC diagnosis is low and its clinical applicability needs to be further validated.59 Therefore, we need more accurate screening modalities to manage COPD combined with lung cancer and improve prognosis.
Chest CT scan can provide important information about pulmonary nodules, emphysema, and other fine structures, which is of great significance in the assessment of lung cancer risk in patients with COPD.60 Patients with COPD are at a higher risk of developing lung cancer, especially in centrilobular emphysema,61,62 and emphysema is also a risk factor for poor prognosis in lung cancer patients.62–64 Quantitative CT (QCT) can analyze lung density, pulmonary vessel, and airway, and clearly shows the distribution of lung disease features such as emphysema, as shown in Figure 1. Mahajan et al19 constructed a machine learning model based on the emphysema index, which has been shown to detect circulating tumor DNA mutations in COPD patients with lung cancer. AI is anticipated to utilize chest CT scans to categorize the risk level of isolated solid pulmonary nodules, facilitating early detection of lung cancer, as well as determine the pathological grade of the cancer, enabling a comprehensive and streamlined approach to managing lung cancer cases.20–22 Recently, based on a large cohort study of 60,000 patients, C-Lung-RADS was proposed for Chinese patients, which assesses lung nodules in phases and multimodality, and provides doctors with a more professional and suitable solution for accurate diagnosis and assessment of lung nodules in the Chinese population.23 In the future, it is expected that personalized CT evaluation systems for lung nodules will be developed for different populations in conjunction with the Lung-RADS.65 Of interest, low-dose computed tomography (LDCT), which reduces radiation dose and increases cost-effectiveness, has also been shown to be more effective in LCS.66–68 At the same time, radiomics nomogram have been shown to predict COPD in lung cancer patients, enabling a one-stop shop for CT scans to check for both diseases in the broader context of LCS.24,69,70 CT screening will go a long way toward reducing the risk of both lung cancer and COPD.
 |
Figure 1 Quantitative CT analysis of lung density (a), airway (b) and vessel (c); (d and e): A 66-year-old male patient diagnosed with centrilobular emphysema. |
In addition, the treatment and prognosis for patients with lung cancer is also one of the hotspots of current research. CT radiomics model is able to assess lung cancer metastasis,71 and the CT-based ensemble AI model can predict 10-year mortality and assess individualized structure risk scores.25 Deep learning models are able to automatically draw approximate disease profiles for patients with primary lung lesions and/or hilar/mediastinal nodal disease.72,73 Quantitative CT can assess immunotherapy response.74 Relying on AI-assisted diagnosis technology, the personalized diagnosis and treatment system of lung cancer for different ethnic groups is expected to be popularized globally in the future, which will promote the early screening and early diagnosis of COPD patients with lung cancer, reduce the delay in the diagnosis of lung cancer that may be caused by the overlap of the symptoms of the two diseases, improve the early diagnosis rate and five-year survival rate of those who have a combination of lung cancer.
COPD and CVD
Compared to the general populace, individuals suffering from COPD are at an elevated risk of developing CVD, and associated with increased mortality.75 Furthermore, acute exacerbations of COPD also increase the risk of CVD.76,77 Existing guidelines underscore that individuals already predisposed to ischemic heart disease face an escalated threat of atherosclerotic cardiovascular disease complications subsequent to exacerbations of COPD.8 However, there are no accepted guidelines for screening for comorbid CVD to mitigate this risk, which may lead to under-treatment of patients with comorbid CVD. Early recognition and management of comorbid CVD are of paramount importance. Early detection of CVD can be done by minimal checkup (eg, medical history, physical examination, blood tests, cardiovascular risk scoring) and, if further studies are needed, by imaging procedures such as chest CT.78,79
Multiple chest CT methods are associated with the incidence of CVD in COPD patients. Coronary calcification on chest CT imaging can predict coronary events occurring in the general population. The Agatston score is an imaging scoring method commonly used to assess the degree of coronary artery calcification, which is calculated based on multiplying the area of each calcified lesion by a weighting factor corresponding to the CT value of that calcified lesion.80 The Weston score, a visual score that scores calcification in each major coronary vessel, correlates well with the quantitative Agatston score and can predict incident coronary artery disease (CAD) in patients with COPD.26 This suggests that a routine chest CT can be used to assess CVD risk. Recent studies have found that coronary artery calcification (CAC) is a common additional finding on low-dose computed tomography for LCS. Calcification scoring on LDCT screening allows for simultaneous assessment of lung cancer and CVD risk. In the current era of LCS, this certainly provides research support for one-stop screening for both diseases.81,82 Dual-energy CT (DECT) is capable of diagnosing coronary artery disease, whereas photon-counting CT (PCCT), which has fewer artifacts and higher signal-to-noise ratio, provides a 55% improvement in diagnostic confidence for coronary artery disease compared with DECT, and it shows that the diagnostic confidence for peripheral arterial disease may surpass that of DSA.27,83 Coronary CT angiography (CCTA) plus fractional flow reserve (CT-FFR) is a method capable of mimicking coronary physiology to calculate the hemodynamic differences in the coronary microcirculation at maximal congestion. Study has shown that CT-FFR reduces the incidence of 90-day invasive coronary angiography, and has similar diagnostic accuracy to CCTA plus CT perfusion in detecting hemodynamically relevant CAD.28,29 In our previous study, lung or mediastinal radiomics features based on CT can provide incremental predictive value over and above clinical risk factors in predicting CVD (AUC: 0.79, 95% CI [0.72, 0.86] for lung; 0.86, 95% CI [0.81, 0.92]) for mediastinum),30,31 and two examples of applying dynamic nomogram are shown in Figure 2. AI in combination with CT undoubtedly provides significant assistance in screening for CVD.
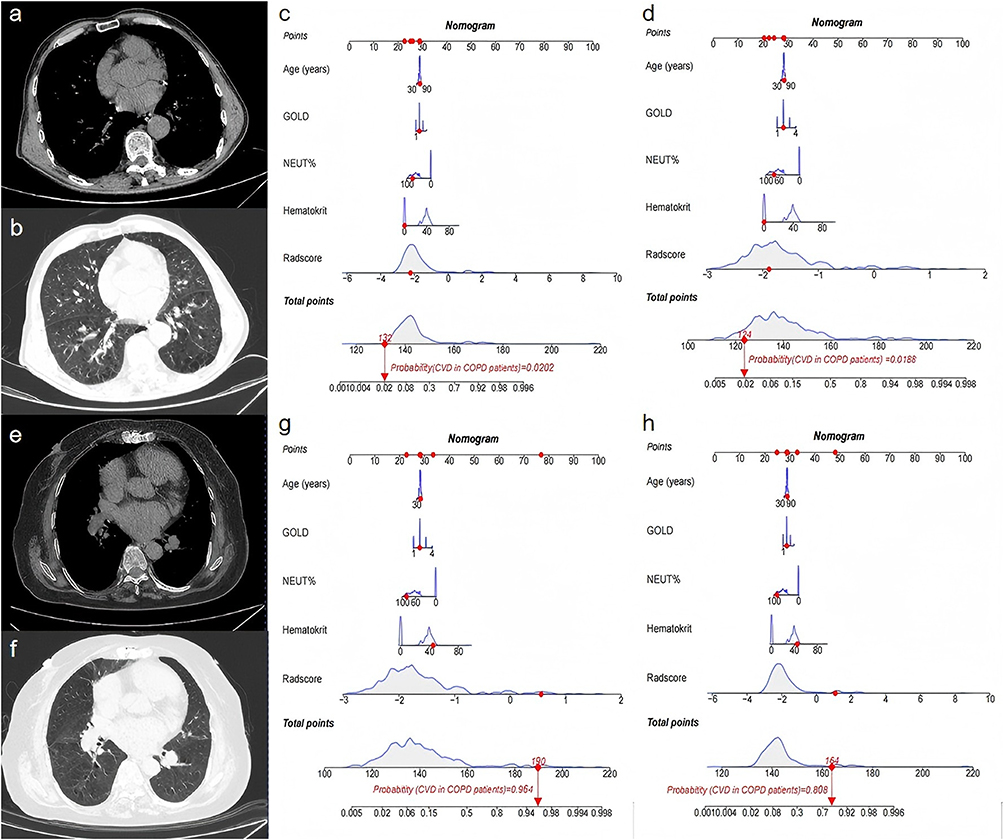 |
Figure 2 (a–d) A 73-year-old male patient diagnosed with COPD. The lung dynamic nomogram shows the total points were 132, and the corresponding prediction probability of CVD was 0.020; the mediastinum dynamic nomogram shows the total points were 124, and the corresponding prediction probability of CVD was 0.019. (d–h) A 73-year-old female patient diagnosed with COPD and coronary atherosclerotic heart disease. The dynamic nomogram shows the total points were 164, and the corresponding prediction probability of CVD was 0.808; the mediastinum dynamic nomogram shows the total points were 190, and the corresponding prediction probability of CVD was 0.964. Abbreviations: COPD, chronic obstructive pulmonary disease; CVD, Cardiovascular disease. |
For the management of CVD, the risk prediction of major adverse cardiovascular events (MACE) is undoubtedly crucial. There is an association between some imaging markers and MACE. In the clinical setting, the Agatston score is widely considered as the gold standard for calcification scores in cardiac CT scans and is significantly associated with MACE.32 Physicians can stratify the risk of CVD based on the above imaging markers and further evaluate individuals at high risk. Guidelines for the primary prevention of atherosclerotic cardiovascular disease (ASCVD) recommend a risk calculator (ASCVD risk score), with risk factors encompassing age, gender, smoking status, systolic blood pressure, hypertension treatment, total cholesterol level, high-density lipoprotein cholesterol level, and prevalent diabetes mellitus.84 However, AI-guided quantitative coronary computed tomography angiography analysis has also been shown to have predictive value, with an AUC for 10-year MACE of 0.78.33 With the help of AI, we can dig deeper into the information of imaging images, which is helpful to identify high-risk COPD patients for early cardiovascular risk adjustment.
COPD and Osteoporosis
Osteoporosis is an asymptomatic COPD comorbidity that is closely associated with COPD and often goes unrecognized clinically.85 Osteoporosis is characterized by loss of bone mass and deterioration of the microstructure of bone tissue, leading to bone fragility and fractures.86 A meta-analysis of 58 studies reported that the global prevalence of comorbid osteoporosis COPD was 38% and that COPD increased the likelihood of osteoporosis [odds ratio (OR) = 2.83].87 Both acute exacerbation of COPD and recent fracture events are independent risk factors for progression in COPD patients with combined osteoporosis.88,89 Fractures associated with COPD can further impair lung function and hinder daily activities, creating a harmful cycle that puts a serious strain on these individuals; it contributes to poor health status and mortality.85 Chronic inflammation of the airways and lungs in patients with COPD can stimulate bone resorption and impair bone formation, reduced physical activity due to dyspnea can lead to lower bone mass density (BMD), long-term use of corticosteroids in COPD patients can promote bone loss and increase the risk of osteoporosis, and there is also a common risk factor for both diseases, smoking.90–92 However, the underlying mechanisms and physiological changes responsible for COPD-associated osteoporosis remain poorly understood and necessitate additional research.91,93
Dual-energy X-ray absorptiometry (DXA) is the gold standard for determining BMD.94 However, DXA possesses inherent limitations, such as its planar technique, limited predictive sensitivity for fractures, and inadequate utilization in population-wide screening.34,95 These deficiencies have restricted its universal adoption and impeded its practical implementation in clinical settings. The fracture risk assessment tool (FRAX) is a multivariate screening algorithm widely used in clinical practice to assess an individual’s risk of fracture in osteoporotic patients over the next 10 years.96 A CT-based fracture risk prediction model in the recent studies, capable of quantitatively separating and analyzing cortical and cancellous bone, provided a highly accurate and personalized prediction of fracture risk in COPD patients with a C-index of 0.797, and a prediction accuracy superior to that of the FRAX.34,97 In contrast to the underutilization of DXA, CT scans are universally available for patients with COPD. Although CT scans are not commonly used to diagnose osteoporosis, they can improve overall screening for osteoporosis, and in combination with AI techniques have the potential to reduce the incidence of future fractures, especially in situations where DXA screening is often lacking. Studies have shown that the degree of emphysema on CT is a significant predictor of osteoporosis in patients with COPD, even after adjustment for competing risk factors (including age, sex, airflow obstruction, and corticosteroid use).35–37 In QCT analyses, emphysema and vascular quantitative parameters were significantly associated with reduced BMD rather than airway parameters,98 but it should be noted that the best predictors of osteoporosis risk events in patients with COPD still need to be further researched and validated as QCT parameters continue to be refined and deepened. However, the higher price and radiation dose of CT compared to DXA also poses a challenge to generalize its use in osteoporosis. At present, ultra-low dose hip CT-based automated method have been shown to be able to assess the bulk BMD of the proximal femoral subregion in COPD patients.38 The automated method of fracture assessment based on LDCT is also highly accurate, further expanding the scope of LDCT.39 Noticeably, LDCT, which reduces cumulative radiation exposure, will certainly be one of the most important research directions in the future.
COPD and Other Systemic Diseases
Sarcopenia, a progressive and generalized skeletal muscle disorder involving the accelerated loss of muscle mass and function, is a common comorbidity in patients with COPD, and its progression is linked to the severity of COPD; the prevalence of sarcopenia is relatively low in patients with stable COPD.99–101 The estimated prevalence of sarcopenia among patients with COPD is 22%.102 Significant transcriptional alterations were present in COPD patients with abnormal muscle fiber ratios.99 Sarcopenia was associated with a higher risk of COPD mortality and impaired functional status.40 CT is the preferred method for assessing muscle mass.40 Dual-energy X-ray absorptiometry (DEXA) can be employed in research environments to quantify lean mass, bone mass, and fat mass; however, it is not routinely utilized for the assessment of muscle mass in clinical practice.103,104 CT-derived cross-sectional area of the pectoralis major muscle (PMA) and attenuation of the pectoralis major muscle (PMT) are independent predictors of COPD severity.41
In addition to the quantification of muscle mass, excess adipose depots, ie, body mass index≥25, are associated with poor prognosis and outcome in COPD.105,106 However, obesity is associated with lower mortality in patients with COPD, known as the obesity paradox.107 Quantitative analysis of chest CT showed that a higher intermuscular adipose tissue index was linked to an elevated risk of mortality compared to a higher subcutaneous adipose tissue index among individuals with COPD.40 High visceral adipose tissue area is also an independent risk factor for COPD exacerbation, and is associated with comorbidities (CVD) or risk factors (hypertension, hyperlipidemia, and diabetes) for COPD.42,108 Previous study has shown that a deep learning model based on adipose tissue measured by quantitative CT can accurately predict COPD exacerbations.42 Nevertheless, the existence of the obesity paradox suggests that “normal” versus “abnormal” adipose tissue and its distribution need to be studied in greater depth, and a more comprehensive understanding of how these metrics can be used to risk-stratify patients with COPD is needed in order to improve the long-term prognosis of COPD patients more effectively.
Pulmonary hypertension (PH) is a complication of COPD, which plays an important role in its progression to cardiopulmonary disease.109 The progression of PH is linked to clinical decline, deterioration in gas exchange, and heightened mortality rates among individuals with COPD.110 Patients suffering from both COPD and PH (COPD-PH) exhibit greater functional impairment and a poorer prognosis compared to those with idiopathic pulmonary arterial hypertension (PAH).109 Although right heart catheterization is the gold standard for the diagnosis of pulmonary hypertension, its invasive nature limits its use as a screening tool in many populations, particularly in those without clinically significant symptoms.105 Before considering referral for invasive right heart catheterization, it is beneficial to use noninvasive methods to identify individuals at risk for PH for initial screening. On chest CT images, the diameters of the pulmonary artery and the ascending aorta (PA/A) ratio of 1 or greater are both reliable indicators of pulmonary hypertension and associated with an increased risk of acute exacerbations and long-term mortality in patients with COPD.43,44,111 AI cardiac CT segmentation is an efficient and accurate method, and these segmenting are in good agreement with the radiologist’s segmentation, thereby providing clinically valuable indicators in a shorter time. Moreover, AI-based lung parenchyma assessment can accurately identify and quantify lung disease patterns by integrating multiple radiomics techniques, such as texture analysis and classification, providing important indicators for the diagnosis, phenotype, and prognosis of patients with PH.112 These studies suggest that noninvasive markers on chest CT scans may increase the frequency of PH detection in a susceptible COPD population.
The Challenge of AI Adoption
The performance of AI is highly dependent on the quality, diversity and representativeness of the training data. If the data is biased, the model may output biased results and risk misdiagnosis. And when there is insufficient data, the model is prone to overfitting or underfitting.113 Deep learning models are often regarded as “black box” and lack of interpretability, which also limits the debugging and optimization efficiency of the models. In the actual implementation process, AI may face data silos, format inconsistency and other issues, and need to invest in high-cost cleaning and labeling data. There are also high requirements for computing power. Further, regular training for physicians is needed to better apply and debug AI models.113,114 Further, AI models require certain development and maintenance costs, and AI systems need to continuously update data and algorithms. However, in terms of long-term benefits, AI models are expected to reduce labor costs and increase diagnostic accuracy.18,113 In future research, small-scale pilot applications of AI models in clinical practice are also needed to assess the predictive performance and clinical utility of the models. The performance of the model should also be monitored in real time during the application process to ensure that its performance on new data is consistent with the training data, and then the model can be optimized.
Conclusions
In response to the current absence of standardized guidelines for managing COPD comorbidities, this review innovatively synthesizes cutting-edge studies on AI combined with CT. This is expected to lead to one-stop screening of COPD comorbidities using CT scans in the future. AI tools have are capable of recognizing high-risk features in all structures visible on the CT scan, and have led to research advances in the assessment, diagnosis, prognosis, and prediction of the disease. The development of chest CT technology requires parallel development of AI techniques to maximize the use of more detailed pathophysiological data. Integration of these tools into clinical practice could provide real-time support to improve diagnostic accuracy and facilitate early detection of COPD comorbidities unrelated to the primary indication for scanning, followed by early intervention and risk adjustment, perhaps yielding meaningful improvements in prognosis and quality of life for COPD patients. However, due to the inherent limitations of AI models, there is still a long way to go for future clinical applications. Collaborative and focused research endeavors in this field will ultimately lead to deeper comprehension and more effective management of COPD worldwide.
Abbreviations
AI, Artificial Intelligence; ASCVD, atherosclerotic cardiovascular disease; BMD, bone mass density; CAC, coronary artery calcification; CAD, coronary artery disease; CCTA, Coronary CT angiography; COPD, Chronic obstructive pulmonary disease; CT-FFR, fractional flow reserve; CVD, cardiovascular disease; DECT, Dual-energy CT; DXA, Dual-energy X-ray absorptiometry; DEXA, Dual-energy X-ray absorptiometry; FRAX, fracture risk assessment tool; LCS, lung cancer screening; LDCT, low-dose computed tomography; MACE, major adverse cardiovascular events; PA/A, the diameters of the pulmonary artery and the ascending aorta; PAH, pulmonary arterial hypertension; PCCT, photon-counting CT; PFT, pulmonary function test; PH, Pulmonary hypertension; PMA, pectoralis major muscle; PMT, pectoralis major muscle; QCT, quantitative CT; SPECT, Single-Photon Emission Computed Tomography.
Disclosure
The author(s) report no conflicts of interest in this work. This work was supported by the National Natural Science Foundation of China (82430065 and 82171926), the National Key Research and Development Program of China (2022YFC2010002, 2022YFC2010000, 2022YFC2010005 and 2022YFC2010006), and Excellent Health Sector Program of Shanghai Municipal Health Commission (20254Z0003).
References
1. Labaki WW, Rosenberg SR. Chronic obstructive pulmonary disease. Ann Intern Med. 2020;173(3):ITC17–ITC32. doi:10.7326/AITC202008040
2. Collaborators GCRD. Global burden of chronic respiratory diseases and risk factors, 1990-2019: an update from the global burden of disease study 2019. EClinicalMedicine. 2023;59:101936.
3. Negewo NA, Gibson PG, Mcdonald VM. COPD and its comorbidities: impact, measurement and mechanisms. Respirology. 2015;20(8):1160–1171. doi:10.1111/resp.12642
4. Rabe KF, Hurst JR, Suissa S. Cardiovascular disease and COPD: dangerous liaisons? Eur Respir Rev. 2018;27(149):180057. doi:10.1183/16000617.0057-2018
5. Wallström O, Stridsman C, Lindberg A, et al. Exacerbation history and risk of myocardial infarction and pulmonary embolism in chronic obstructive pulmonary disease. Chest. 2024;166(6):1347–1359. doi:10.1016/j.chest.2024.07.150
6. Xu J, Ji Z, Zhang P, Chen T, Xie Y, Li J. Disease burden of COPD in the Chinese population: a systematic review. Therap Adv Resp Dis. 2023;2023:17.
7. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China pulmonary health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
8. Global strategy for prevention, diagnosis and management of COPD: 2024 Report. 2024. Available from: https://goldcopdorg/2024-gold-report/.
9. Lee DA-O, Oh JA-O, Kim JA-O, et al. Imaging bone turnover assessment through volumetric density-adjusted standardized uptake value using quantitative bone SPECT/CT in osteoporosis. EJNMMI Res. 2024;14(1):75. doi:10.1186/s13550-024-01137-y
10. Sadeghpour A, Jiang Z, Hummel YM, et al. An automated machine learning-based quantitative multiparametric approach for mitral regurgitation severity grading. JACC Cardiovasc Imaging. 2024;18:S1936–878X(24)00247–X. doi:10.1016/j.jcmg.2024.06.011
11. Baeza S, Gill D, Sanchez C, et al. Radiomics and clinical data for the diagnosis of incidental pulmonary nodules and lung cancer screening: radiolung integrative predictive model. Arch Bronconeumol. 2024;S0300-2896(24):00192–3.
12. Exarchos KA-O, Kostikas KA-O. Artificial intelligence in COPD: possible applications and future prospects. Respirology. 2021;26(7):641–642. doi:10.1111/resp.14061
13. Kong SA-O, Cho WA-OX, Park SA-O, et al. A computed tomography-based fracture prediction model with images of vertebral bones and muscles by employing deep learning: development and validation study. J Med Internet Res. 2024;12(26):e48535. doi:10.2196/48535
14. Xu KA-OX, Khan MS, Li TA-O, et al. AI body composition in lung cancer screening: added value beyond lung cancer detection. Radiology. 2023;308(1):e222937. doi:10.1148/radiol.222937
15. Alshmrani GM, Ni Q, Jiang R, Pervaiz H, Elshennawy NM. A deep learning architecture for multi-class lung diseases classification using chest X-ray (CXR) images. Alex Eng J.
16. Ibrahim MD, Elshennawy NM, Sarhan AM. Deep-chest: multi-classification deep learning model for diagnosing COVID-19, pneumonia, and lung cancer chest diseases. Comput Biol Med. 2021;132:104348. doi:10.1016/j.compbiomed.2021.104348
17. Mathew VABMSYSL. Prediction of pulmonary diseases with electronic nose using SVM and XGBoost. IEEE Sens J. 2021; 21(18):20886–95.
18. Hamet P, Tremblay J. Artificial intelligence in medicine. Metabolism. 2019;69S:S36–S40.
19. Mahajan AA-O, Kania V, Agarwal U, et al. Deep-learning-based predictive imaging biomarker model for EGFR mutation status in non-small cell lung cancer from CT imaging. Cancers. 2024;16(6):1130. doi:10.3390/cancers16061130
20. Jiang LA-OX, Zhou Y, Miao W, et al. Artificial intelligence-assisted quantitative CT parameters in predicting the degree of risk of solitary pulmonary nodules. Ann Med. 2024;56(1). doi:10.1080/07853890.2024.2405075.
21. Yang R, Li W, Yu S, et al. Deep learning model for pathological grading and prognostic assessment of lung cancer using CT imaging: a study on NLST and external validation cohorts. Acad Radiol. 2024;17:S1076–6332.
22. Zhang W, Cui X, Wang J, et al. The study of plain CT combined with contrast-enhanced CT-based models in predicting malignancy of solitary solid pulmonary nodules. Sci Rep. 2024;14(1):21871.
23. Wang CA-O, Shao J, He Y, et al. Data-driven risk stratification and precision management of pulmonary nodules detected on chest computed tomography. Nat Med. 2024;30:3184–3195. doi:10.1038/s41591-024-03211-3
24. Taohuzhou M, Wenting TU, MS Pengdong, Duan Shaofeng. CT-based radiomic nomogram for the prediction of chronic obstructive pulmonary disease in patients with lung cancer. Acad Radiol. 2023;30(12):2894–2903. doi:10.1016/j.acra.2023.03.021
25. Marcinkiewicz AA-O, Buchwald MA-O, Shanbhag AA-O, et al. AI for multistructure incidental findings and mortality prediction at chest CT in lung cancer screening. Radiology. 2024;312(3):e240541. doi:10.1148/radiol.240541
26. Bhatt SP, Kazerooni EA, Newell JD, et al. Visual estimate of coronary artery calcium predicts cardiovascular disease in COPD. Chest. 2018;154(3):579–587. doi:10.1016/j.chest.2018.05.037
27. Augustin AM, Hartung V, Grunz JP, et al. Photon-counting detector CT angiography versus digital subtraction angiography in patients with peripheral arterial disease. Acad Radiol. 2023;31(7):2973–2986. doi:10.1016/j.acra.2024.02.008
28. Guo BA-O, Xing WA-O, Hu CA-O, et al. Clinical effectiveness of automated coronary CT-derived fractional flow reserve: a Chinese randomized controlled trial. Radiology. 2024;313(1):e233354. doi:10.1148/radiol.233354
29. Soschynski MA-O, Storelli RA-O, Birkemeyer C, et al. CT myocardial perfusion and CT-FFR versus invasive FFR for hemodynamic relevance of coronary artery disease. Radiology. 2024;312(2):e233234. doi:10.1148/radiol.233234
30. Lin X, Zhou T, Ni J, et al. CT-based whole lung radiomics nomogram: a tool for identifying the risk of cardiovascular disease in patients with chronic obstructive pulmonary disease. Eur Radiol. 2024;34(8):4852–4863. doi:10.1007/s00330-023-10502-9
31. Lin X, Zhou T, Ni J, et al. CT-Based radiomics nomogram of lung and mediastinal features to identify cardiovascular disease in chronic obstructive pulmonary disease: a multicenter study. BMC Pulm Med. 2025;25(1):121.
32. Zajančkauskienė L, Radionovaitė L, Jankauskas A, et al. Coronary CT value in quantitative assessment of intermediate stenosis. Medicina. 2022;58(7):964.
33. Nurmohamed NS, Bom MJ, Jukema RA, et al. AI-guided quantitative plaque staging predicts long-term cardiovascular outcomes in patients at risk for atherosclerotic CVD. JACC Cardiovasc Imaging. 2024;17(3):269–280. doi:10.1016/j.jcmg.2023.05.020
34. Yang H, Li Y, Yang H, et al. A novel CT-based fracture risk prediction model for COPD patients. Acad Radiol. 2024;10:1043–53.
35. Vuković DA-O, Budimir Mršić DA-O, Ordulj IA-O, et al. Is type and grade of emphysema important for bone mineral density and aortic calcifications? J Clin Med. 2024;13(13):3947. doi:10.3390/jcm13133947
36. Bon J, Zhang Y, Leader JK, et al. Radiographic emphysema, circulating bone biomarkers, and progressive bone mineral density loss in smokers. Ann Am Thorac Soc. 2018;15(5):615–621. doi:10.1513/AnnalsATS.201709-743OC
37. Goto K, Ogawa E, Shimizu K, et al. Relationship of annual change in bone mineral density with extent of emphysematous lesions and pulmonary function in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2018;20(13):639–644. doi:10.2147/COPD.S153750
38. Zhang X, Nadeem SA, Dicamillo PA, et al. Ultra-low dose Hip CT-based automated measurement of volumetric bone mineral density at proximal femoral subregions. Med Phys. 2023;51(11):8213–31. doi:10.1002/mp.17319
39. Nadeem SA, Comellas AP, Regan EA, et al. Chest CT-based automated vertebral fracture assessment using artificial intelligence and morphologic features. Med Phys. 2024;51(6):4201–4218. doi:10.1002/mp.17072
40. Pishgar FA-O, Shabani MA-OX, Quinaglia ACSTA-O, et al. Quantitative analysis of adipose depots by using chest CT and associations with all-cause mortality in chronic obstructive pulmonary disease: longitudinal analysis from mesarthritis ancillary study. Radiology. 2021;299(3):703–711. doi:10.1148/radiol.2021203959
41. Qiao X, Hou G, Kang J, et al. CT attenuation and cross-sectional area of the pectoralis are associated with clinical characteristics in chronic obstructive pulmonary disease patients. Front Physiol. 2022;3(13):833796. doi:10.3389/fphys.2022.833796
42. Wu J, Lu Y, Dong S, et al. Predicting COPD exacerbations based on quantitative CT analysis: an external validation study. Front Med Lausanne. 2024;12(11):1370917. doi:10.3389/fmed.2024.1370917
43. Lee JK, Kho BG, Yoon JY, et al. The clinical characteristics associated with the ratio between the main pulmonary artery and ascending aorta diameter in patients with acute exacerbation of chronic obstructive pulmonary disease. J Thorac Dis. 2024;16(8):4924–4934. doi:10.21037/jtd-24-62
44. Terzikhan N, Bos D, Lahousse L, et al. Pulmonary artery to aorta ratio and risk of all-cause mortality in the general population: the Rotterdam Study. Eur Respir J. 2017;49(6):1602168. doi:10.1183/13993003.02168-2016
45. Hou W, Hu S, Li C, et al. Cigarette smoke induced lung barrier dysfunction, EMT, and tissue remodeling: a possible link between COPD and lung cancer. Biomed Res Int. 2019;2019. doi:10.1155/2019/2025636
46. Xu J, Shang Y, Cai F, et al. Correlation between lung cancer and the HHIP polymorphisms of chronic obstructive pulmonary disease (COPD) in the Chinese Han population. Genes Immun. 2019: 20(4):273–80.
47. Cunningham Y, Wyke S, Blythk G, et al. Lung cancer symptom appraisal among people with chronic obstructive pulmonary disease: a qualitative interview study. Psychooncology. 2019; 28(4):718–25.
48. Sweef OA-OX, Mahfouz RA-O, Taşcıoğlu TA-O, et al. Decoding LncRNA in COPD: unveiling prognostic and diagnostic power and their driving role in lung cancer progression. J Int J Mol Sci. 2024;25:9001. doi:10.3390/ijms25169001
49. Lunardi FA-O, Nardo G, Lazzarini EA-OX, et al. Is there a link between chronic obstructive pulmonary disease and lung adenocarcinoma? A clinico-pathological and molecular study. J Pers Med. 2024;14(8):839. doi:10.3390/jpm14080839
50. Xu Y, Li M, Bai L. Pulmonary epithelium cell fate determination: COPD, lung cancer, or both. Am J Respir Cell Mol Biol. 2024;2024:1.
51. Machida H, Inoue S, Shibatay A-O, et al. The incidence and risk analysis of lung cancer development in patients with chronic obstructive pulmonary disease: possible effectiveness of annual CT-screening. Int J Chron Obstruct Pulmon Dis. 2021;2021:1178–2005.
52. Satici C, Beke O. The role of electronic nose analysis of exhaled air in detection of lung cancer among patients with COPD. Chest. 2024;165:1931–3543.
53. Binson VA-O, Subramoniam M, Mathew L. Discrimination of COPD and lung cancer from controls through breath analysis using a self-developed e-nose. J Breath Res. 2021;15(4):046003. doi:10.1088/1752-7163/ac1326
54. Xu K, Zhang C, Du T, et al. Progress of exosomes in the diagnosis and treatment of lung cancer. Biomed Pharmacother. 2021;134:111111. doi:10.1016/j.biopha.2020.111111
55. Park HY, Kang D, Shin SH, et al. Pulmonary tuberculosis and the incidence of lung cancer among patients with chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2022;19(4):640–648. doi:10.1513/AnnalsATS.202010-1240OC
56. Banghenriksen M, Hansen TF, Jensen LH, et al. Lung cancer among outpatients with COPD: a 7-year cohort study. ERJ Open Res. 2024;10(4). doi:10.1183/23120541.00064-2024.
57. Va B, Mathew P, Thomas S, et al. Detection of lung cancer and stages via breath analysis using a self-made electronic nose device. Expert Rev Mol Diagn. 2024;24(4):341–353. doi:10.1080/14737159.2024.2316755
58. Binson VA, Subramoniam M, Mathew L. Prediction of lung cancer with a sensor array based e-nose system using machine learning methods. Microsyst Technol. 2024; 30(11):1421–34.
59. Krauss E, Haberer JFAU, Barreto G, et al. Recognition of breathprints of lung cancer and chronic obstructive pulmonary disease using the Aeonose ® electronic nose. J Breath Res. 2020;14(4):046004. doi:10.1088/1752-7163/ab8c50
60. Mazzone PJ, Lam L. Evaluating the patient with a pulmonary nodule: a review. JAMA. 2024;327(3):264–273.(1538–3598. doi:10.1001/jama.2021.24287
61. Durawa AA-O, Dziadziuszko KA-O, Jelitto MA-O, et al. Emphysema and lung cancer risk. Transl Lung Cancer Res. 2024;13(8):1918–1928. doi:10.21037/tlcr-24-197
62. Steiger D, Siddiqi MF, R Yip, et al. The importance of low-dose CT screening to identify emphysema in asymptomatic participants with and without a prior diagnosis of COPD. Clin Imaging. 2021;78:136–141. doi:10.1016/j.clinimag.2021.03.012
63. Ishida M, Mimae T, Okada M. ASO author reflections: how does emphysema contribute to poor prognosis after lung cancer surgery? Ann Surg Oncol. 2024;31(7):4323–4324. doi:10.1245/s10434-024-15171-6
64. Ishida M, Mimae T, Kamigaichi A, et al. The role of emphysema on postoperative prognosis in early-stage nonsmall cell lung cancer. Ann Surg Oncol. 2024;31(8):5055–5063. doi:10.1245/s10434-024-15126-x
65. IASLC’s Annual Report 2023. 2024. Available from: https://wwwiaslcorg/.
66. Rajabi T, Szilberhorn L, Győrbíró D, Tatár M, Vokó Z, Nagy B. Cost-effectiveness of lung cancer screening with low-dose computed tomography: comparing Hungarian screening protocols with the US NLST. Cancers. 2024;16(17):2933.
67. Yao Y, Su X, Deng L, et al. Effects of tube voltage, radiation dose and adaptive statistical iterative reconstruction strength level on the detection and characterization of pulmonary nodules in ultra-low-dose chest CT. Cancer Imaging. 2024;24(1):123. doi:10.1186/s40644-024-00770-z
68. Cai JA-O, Vonder M, Du YA-O, et al. Who is at risk of lung nodules on low-dose CT in a Western country? A population-based approach. Eur Respir J. 2024;63(6):2301736. doi:10.1183/13993003.01736-2023
69. Binson VA, Thomas S, Philip PC, Thomas A, Pillai P. Detection of early lung cancer cases in patients with COPD using eNose technology: a promising non-invasive approach. IEEE RASSE. 2023;2023:1.
70. Wang X, Ren H, Ren J, et al. Machine learning-enabled risk prediction of chronic obstructive pulmonary disease with unbalanced data. Comput Methods Programs Biomed. 2023;230:107340. doi:10.1016/j.cmpb.2023.107340
71. Li Y, Deng J, Ma X, et al. Diagnostic accuracy of CT and PET/CT radiomics in predicting lymph node metastasis in non-small cell lung cancer. Eur Radiol. 2024. doi:10.1007/s00330-024-11036-4
72. Bi S, Yuan Q, Dai Z, et al. Advances in CT-based lung function imaging for thoracic radiotherapy. Front Oncol. 2024;2(14):1414337.
73. Skett S, Patel T, Duprez D, et al. Autocontouring of primary lung lesions and nodal disease for radiotherapy based only on computed tomography images. Phys Imaging Radiat Oncol. 2024;31:100637. doi:10.1016/j.phro.2024.100637
74. Noda Y, Shiroyama T, Masuhiro K, et al. Quantitative evaluation of emphysema for predicting immunotherapy response in patients with advanced non-small-cell lung cancer. Sci Rep. 2022;12(1):8881. doi:10.1038/s41598-022-13131-2
75. Sá-sousa AA-O, Rodrigues CA-O, Jácome CA-O, et al. Cardiovascular risk in patients with chronic obstructive pulmonary disease: a systematic review. J Clin Med. 2024;13(17):5173. doi:10.3390/jcm13175173
76. Yang HA-O, Ryu MA-O, Carey VA-O, et al. Chronic obstructive pulmonary disease exacerbations increase the risk of subsequent cardiovascular events: a longitudinal analysis of the COPDgene study. J Am Heart Assoc. 2024;13(11):e033882. doi:10.1161/JAHA.123.033882
77. Mosher CA-O, Osazuwa-Peters OL, Nanna MG, et al. Risk of atherosclerotic cardiovascular disease hospitalizations after COPD hospitalization among older adults. Ann Am Thorac Soc. 2024;21:1516–1523. doi:10.1513/AnnalsATS.202401-017OC
78. Morgan AD, Zakeri R, Quint JK. Defining the relationship between COPD and CVD: what are the implications for clinical practice? Ther Adv Respir Dis. 2018;12:1753465817750524. doi:10.1177/1753465817750524
79. Perone FA-O, Bernardi MA-O, Redheuil A, et al. Role of cardiovascular imaging in risk assessment: recent advances, gaps in evidence, and future directions. J Clin Med. 2023;12(17):5563. doi:10.3390/jcm12175563
80. Wang W, Yang L, Wang S, et al. An automated quantification method for the Agatston coronary artery calcium score on coronary computed tomography angiography. Quant Imaging Med Surg. 2022;12(3):1787–1799. doi:10.21037/qims-21-775
81. Bonney AA-O, Chua M, Mccusker MW, et al. Coronary artery calcification detected on low-dose computed tomography in high-risk participants of an Australian lung cancer screening program: a prospective observational study. Respirology. 2024. doi:10.1111/resp.14832
82. Berzingi S, Piechowski K, Hendricks E, et al. Integrating cardiovascular risk assessment into mobile low-dose CT lung screenings in rural Appalachia: a comprehensive analysis of the relationship between lung cancer risk, coronary artery calcium burden, and cardiovascular risk reduction strategies. Am J Prev Cardiol. 2024;11(19):100719.
83. Douek A-O, Boccalini S, Oei EA-O, et al. Clinical applications of photon-counting ct: a review of pioneer studies and a glimpse into the future. Radiology. 2023;309(1):e222432. doi:10.1148/radiol.222432
84. Arnett DKBR, Albert MA, Albert MA, et al. ACC/AHA guideline on the primary prevention of cardiovascular disease: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;74:1376–1414. doi:10.1016/j.jacc.2019.03.009
85. Kaenmuang P, Keeratichananont W, Geaters L, et al. Prevalence, predictors, dynamic bone change, and treatment efficacy of osteoporosis among chronic obstructive pulmonary disease patients: a prospective cohort study. Front Med Lausanne. 2023;8(10):1214277.
86. Compston JE, Mcclung MR, Leslie WD. Osteoporosis. Lancet. 2019;393(10169):364–376. doi:10.1016/S0140-6736(18)32112-3
87. Chen YW, Ramsook AH, Coxson HO, et al. Prevalence and risk factors for osteoporosis in individuals with COPD: a systematic review and meta-analysis. Chest. 2019;156(6):1092–1110. doi:10.1016/j.chest.2019.06.036
88. Van Dort MJ, Geusens P, Driessen JH, et al. High imminent vertebral fracture risk in subjects with COPD with a prevalent or incident vertebral fracture. J Bone Miner Res. 2018;33(7):1233–1241. doi:10.1002/jbmr.3429
89. Kiyokawa H, Muro S, Oguma T, et al. Impact of COPD exacerbations on osteoporosis assessed by chest CT scan. COPD. 2012;9(3):235–42. doi:10.3109/15412555.2011.650243
90. Penedones A, Mendes D, Alves C, et al. Relationship between chronic obstructive pulmonary disease and osteoporosis: a scoping review. COPD. 2024;21(1):2356510. doi:10.1080/15412555.2024.2356510
91. Li Y, Gao H, Zhao L, et al. Osteoporosis in COPD patients: risk factors and pulmonary rehabilitation. Clin Respir J. 2022;16(7):487–496. doi:10.1111/crj.13514
92. Zhong H, Ni X, Chen R, et al. Smoking contribution to the global burden of metabolic disorder: a cluster analysis. Med Clin. 2024;163(1):14–20. doi:10.1016/j.medcli.2024.02.001
93. Tsukamoto MA-O, Nabeshima T, Wang KY, et al. The impact of chronic obstructive pulmonary disease on bone strength. J Bone Miner Metab. 2024;42(4):421–427. doi:10.1007/s00774-024-01496-5
94. Anam AK, Insogna K. Update on osteoporosis screening and management. Med Clin North Am. 2021;105(6):1117–1134. doi:10.1016/j.mcna.2021.05.016
95. Messina C, Fusco S, Gazzotti S, et al. DXA beyond bone mineral density and the REMS technique: new insights for current radiologists practice. Radiol Med. 2024;129(8):1224–1240. doi:10.1007/s11547-024-01843-6
96. Chen YW, Ramsook AH, Coxson HO, et al. Prevalence and risk factors for osteoporosis in individuals with COPD: a systematic review and meta-analysis. JAMA Oncol. 2024;3:e244318.
97. Li Y, Yao Q, Yu H, et al. Automated segmentation of vertebral cortex with 3D U-net-based deep convolutional neural network. Front Bioeng Biotechnol. 2022;10:996723.
98. Sakurai-Iesato Y, Kawata N, Tada Y, et al. The relationship of bone mineral density in men with chronic obstructive pulmonary disease classified according to the global initiative for chronic obstructive lung disease (GOLD) combined chronic obstructive pulmonary disease (COPD) assessment system. Intern Med. 2017;56(14):1781–1790. doi:10.2169/internalmedicine.56.6910
99. Chiles JWRA-O, Wilson AC, Tindal R, et al. Differentially co-expressed myofibre transcripts associated with abnormal myofibre proportion in chronic obstructive pulmonary disease. J Cachexia Sarcopenia Muscle. 2024;15(3):1016–1029. doi:10.1002/jcsm.13473
100. Ma J, Yao J, Zhang L, et al. Causal association between sarcopenia and chronic obstructive pulmonary disease: a two-sample Mendelian randomization. Asian J Surg. 2024;27:S1015–9584(24)01793–7. doi:10.1016/j.asjsur.2024.08.066
101. Kim SH, Hong CH, Shin MJ, et al. Prevalence and clinical characteristics of Sarcopenia in older adult patients with stable chronic obstructive pulmonary disease: a cross-sectional and follow-up study. BMC Pulm Med. 2024;24(1):219. doi:10.1186/s12890-024-03034-5
102. Benz E, Trajanoska K, Lahoussel A-O, et al. Sarcopenia in COPD: a systematic review and meta-analysis. Eur Respir Rev. 2019;28(154):190049. doi:10.1183/16000617.0049-2019
103. Mcdonald MA-O, Diaz AA, Rutten E, et al. Chest computed tomography-derived low fat-free mass index and mortality in COPD. Eur Respir J. 2017;50(6):1701134. doi:10.1183/13993003.01134-2017
104. Wilson AC, Bon JM, Mason S, et al. Increased chest CT derived bone and muscle measures capture markers of improved morbidity and mortality in COPD. Respir Res. 2022;23(1):311. doi:10.1186/s12931-022-02237-w
105. Singhvi D, Bon J. CT imaging and comorbidities in COPD: beyond lung cancer screening. Chest. 2021;159(1):147–153. doi:10.1016/j.chest.2020.08.2053
106. World Health Organization. 2025. Available from: https://www.who.int/health-topics/obesity/#tab=tab_10.
107. Wu TD, Ejike CO, Wise RA, McCormack MC, Brigham EP. Investigation of the obesity paradox in chronic obstructive pulmonary disease, according to smoking status, in the United States. Am J Epidemiol. 2019;188(11):1977–1983. doi:10.1093/aje/kwz185
108. Nicholson JM, Orsso CE, Nourouzpour S, et al. Computed tomography-based body composition measures in COPD and their association with clinical outcomes: a systematic review. Chron Respir Dis. 2022;19:14799731221133387. doi:10.1177/14799731221133387
109. Vizza CD, Hoeperm M, Huscher D, et al. Pulmonary hypertension in patients with COPD: results from the comparative, prospective registry of newly initiated therapies for pulmonary hypertension (COMPERA. Chest. 2021;160(2):678–689. doi:10.1016/j.chest.2021.02.012
110. Liang RA-O, Liu D, Li H, et al. The efficacy and safety of herbal formulas for adults with pulmonary hypertension combined with chronic obstructive pulmonary disease: a systematic review and meta-analysis involving 1865 participants. J Thorac Dis. 2024;16(9):5923–5935. doi:10.21037/jtd-24-471
111. Wu XG, Shi YJ, Wang XH, et al. Diagnostic value of computed tomography-based pulmonary artery to aorta ratio measurement in chronic obstructive pulmonary disease with pulmonary hypertension: a systematic review and meta-analysis. Clin Respir J. 2022;16(4):276–283. doi:10.1111/crj.13485
112. Sharkey MJ, Checkley EW, Swift AJ. Applications of artificial intelligence in computed tomography imaging for phenotyping pulmonary hypertension. Curr Opin Pulm Med. 2024;30(5):464–472. doi:10.1097/MCP.0000000000001103
113. Yu KA-O, Healey E, Leong TY, et al. Medical artificial intelligence and human values. N Engl J Med. 2024;390(20):1895–1904. doi:10.1056/NEJMra2214183
114. Wang HA-OX, Fu T, Du Y, et al. Scientific discovery in the age of artificial intelligence. Nature. 2023; 620(7972):47–60.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Chronic Obstructive Pulmonary Disease and Survival in Patients with Lung Cancer: A Nationwide Cohort Study
Chan KH, Liu WC, Chang YC, Konara Mudiyanselage SP, Chuang TJ, Tsai YT
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:617198
Published Date: 23 June 2026