Back to Journals » OncoTargets and Therapy » Volume 19
The Robotic Interval Surgery, A Game-Changer in Optimal Debulking for Ovarian Cancer: A Systematic Review and Meta-Analysis
Authors Maharani AJ, Salsabila PL, Radina NI, Suhamdy F ![]() , Nugra EA, Nugrahani AD
, Nugra EA, Nugrahani AD ![]() , Hidayat YM
, Hidayat YM ![]()
Received 30 August 2025
Accepted for publication 7 January 2026
Published 21 January 2026 Volume 2026:19 559860
DOI https://doi.org/10.2147/OTT.S559860
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Gaetano Romano
Amanda Jessie Maharani,1 Pricillia Laurenza Salsabila,1 Najla Istyari Radina,1 Frederick Suhamdy,1 Eurico Al Nugra,1 Annisa Dewi Nugrahani,2,3 Yudi Mulyana Hidayat3
1Undergraduate Medical Education Program, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Doctoral Program, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 3Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran/Dr. Hasan Sadikin General Hospital, Bandung, West Java, Indonesia
Correspondence: Amanda Jessie Maharani, Undergraduate Medical Education Program, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia, Email [email protected]
Purpose: This study evaluates the role of robotic-interval debulking surgery (robotic IDS) compared to traditional laparotomy as the game-changer in surgical outcome and complications for ovarian cancer patients.
Patients and Methods: Following PRISMA guidelines, relevant literature published between 2014 and 2024 was retrieved from PubMed, Scopus, Google Scholar, EBSCOHost, and SAGE Journals. Out of 816 studies, four were included, assessed for bias using ROBINS-I and analyzed with random-effects meta-analysis with RevMan 5.4.
Results: A total of four studies involving 166 patients were analyzed. The findings indicate that robotic IDS has a significant result on achieving complete cytoreduction (OR of 6.67 [p = 0.0003]), reducing estimated blood loss (SMD of − 0.71 [p = 0.02]), and shorter hospital stay (SMD of − 1.58 [p< 0.00001]). The result also shows promising effects on intraoperative complications with an OR of 0.82 [p=0.86] and postoperative complications with an OR of 0.40 [p=0.11]. Conversely, there is a longer operative time in robotic IDS compared to laparotomy with a SMD of 0.40 [p = 0.26].
Conclusion: Robotic IDS advances surgical management of advanced-stage (stage III–IV) and recurrent ovarian cancer, offering improved cytoreduction rates, reduced blood loss, and shorter hospital stays. A promising effect was also observed on intraoperative and postoperative complications, although operative time was longer. Further research is needed to demonstrate clearer clinical advantages.
Keywords: laparotomy, ovarian cancer, robotic interval debulking surgery, surgical outcomes
Introduction
Ovarian cancer remains one of the most lethal gynecologic malignancies, with an estimated 19,680 new cases and 12,740 deaths by 2024, varying across countries.1,2 Primary surgery followed by adjuvant chemotherapy is the standard approach. However, achieving optimal cytoreduction (residual tumor < 1–2 cm) can be challenging in advanced-stage or poor medical conditions, prompting alternative strategies such as neoadjuvant chemotherapy (NAC) and interval debulking surgery (IDS).3 In conditions where primary debulking surgery is not possible (or not being attempted at all) and only a biopsy is performed for diagnostic purposes, neoadjuvant chemotherapy (NAC) will be administered, and after 2–4 cycles and responses, secondary surgery or the so-called interval debulking surgery (IDS) between chemotherapy cycles may be possible.4 Despite advances in treatment and surgical techniques, optimal cytoreduction remains a significant barrier to improved survival in ovarian cancer patients. Traditional laparotomy IDS after NAC has demonstrated advantages, including enhanced perioperative parameters and follow-up results. However, achieving a shorter recovery and complete cytoreduction remains a challenge due to tumor burden, surgical complexity, and variability in surgical expertise.5 The emergence of robotic-assisted surgery offers the potential to enhance precision, reduce intraoperative and perioperative complications, and improve optimal debulking rates in interval surgery. Still, its comparative effectiveness against conventional approaches remains unclear.6 While previous meta-analyses have explored the benefits of robotic surgery compared to NAC in ovarian cancer, this study focuses specifically on comparing robotic interval debulking surgery and laparotomy. Therefore, this systematic review and meta-analysis aim to evaluate the role of robotic-assisted surgery in interval debulking and assess its impact on surgical outcomes, including complete cytoreduction, operative time, estimated blood loss, hospital stay, intraoperative complications, and postoperative complications.
Materials and Methods
This systematic review was conducted in accordance with the guidelines recommended by the Cochrane Group and carried out following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 statement.7 A detailed protocol has been previously registered in PROSPERO (CRD42025631453).
Search Strategy
Two independent investigators performed thorough literature searches, with discrepancies resolved by a third investigator in a blinded. We initially searched PubMed, Scopus, EBSCOhost, and SAGE for studies published up to 20 December 2024. Additionally, an extensive search of gray literature was performed using Google Scholar. The search strategy incorporated keywords combined with boolean operators and Medical Subject Heading (MeSH) related to “ovarian cancer”, “robotic interval debulking surgery”, “surgical outcomes” including “complete cytoreduction”, “length of hospital stay”, “estimated blood loss”, “operative time”, “complication” and their synonym listed on Supplementary Table S1 Subsequently, the retrieved results were deduplicated and screened against the pre-specified eligibility criteria.
Study Eligibility Criteria
Inclusion criteria were set to filter observational studies investigating the outcome of robotic interval debulking surgery on ovarian cancer patients (FIGO stage I–IV) compared to laparotomy, with only studies published in the last ten years (2014–2024) included. Outcomes of interest are the surgical outcomes, including complete cytoreduction, length of hospital stay, estimated blood loss, operative time, and complications. Conversely, studies were excluded if any of the following criteria were met: (1) irretrievable full-text articles and (2) non-English articles.
Data Extraction and Risk of Bias Assessment
Data extraction and risk of bias assessment were conducted by three independent reviewers (AJM, PLS, and ADN) using a pre-specified form, and discrepancies between authors were resolved by the fourth author (YMH). The extracted data included (1) first author and publication year, (2) study design, (3) country, (4) sample size, (5) stage of cancer, and (6) chemotherapy treatment. Any discrepancies were resolved through consensus with an independent third investigator. The primary outcomes in this study are surgical outcomes among ovarian cancer patients with both treatments. Surgical outcomes refer to clinical measures resulting from surgical procedures, including both short- and long-term effects, such as complete cytoreduction, length of hospital stay, estimated blood loss, operative time, and complications. When available, data on progression-free survival (PFS) and overall survival (OS) were collected to define the prospective oncologic outcomes of robotic interval debulking surgery (IDS). Included studies underwent methodological quality assessment using the Risk of Bias in Non-randomised Studies-of Interventions (ROBINS-I). However, quality assessment was not used as an exclusion criterion for the included studies.
Statistical Analysis
Dichotomous data, such as overall survival, were analyzed by pooling odds ratios (ORs) using the Mantel–Haenszel method. For continuous data, such as operative time, mean differences (MD) were pooled using inverse variance weighting. Continuous data are presented as means with standard deviations (SD). When the mean or SD was unavailable, the corresponding authors were contacted to request the missing information. A minimum of 3 authors were contacted to confirm the study scenario and obtain the necessary data. If there was no response or the data were not provided, the missing means and SD were estimated using a method based on the median, interquartile range (IQR), range, and sample size, as detailed in the formula by Wan et al.8
A meta-analysis was conducted using Review Manager v5.4 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen). A random-effects model was applied due to anticipated clinical heterogeneity. Heterogeneity among studies was evaluated using the chi-square test, the Cochran Q test, and the I2 statistic. The I2 values were categorized as follows: negligible (0–25%), low (25–50%), moderate (50–75%), and substantial (>75%) heterogeneity. Additionally, when the number of studies was sufficient (n ≥ 10), potential publication bias was assessed visually by inspecting funnel plots and quantitatively using Egger’s test. A p-value of <0,05 was considered statistically significant.
Results
Study Selection and Characteristics
We retrieved 816 relevant articles from the included databases and removed 101 duplicates. The remaining articles were screened by title and abstract, resulting in 10 records that were fully assessed for eligibility. Only four studies were considered suitable and were analyzed in this review (Figure 1).
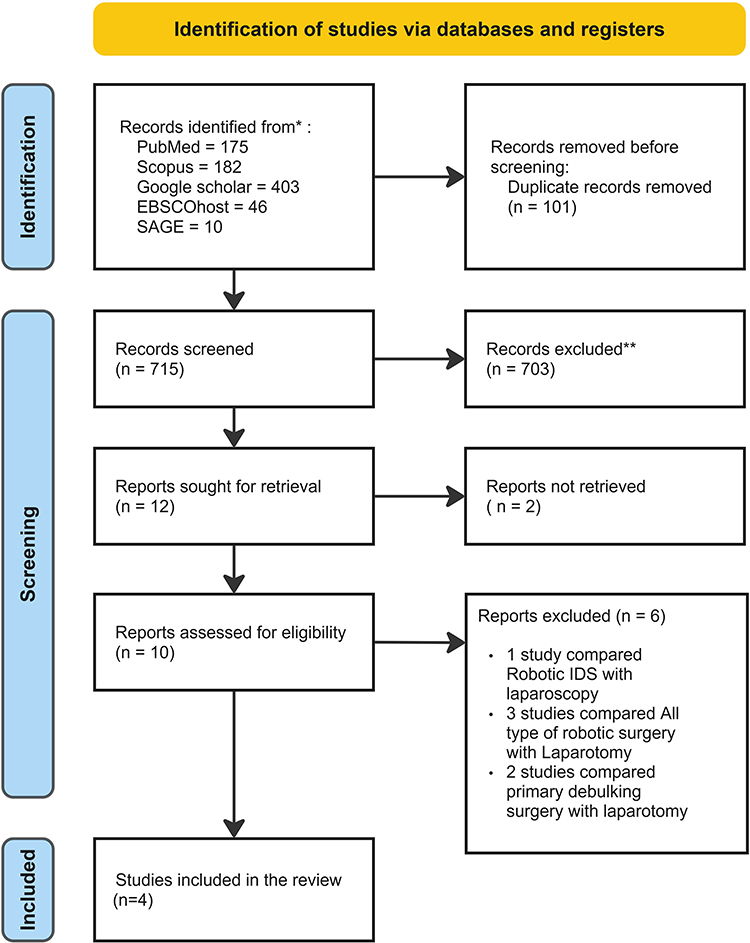 |
Figure 1 PRISMA flow chart. *In this flowchart, records are tracked only through databases (no registers). **Based on the study’s exclusion criteria, articles that contained only a review or an abstract of grey literature were not included. |
The origin of our analyzed studies varies with each study conducted in Western and East Asia regions, including Canada, the United Kingdom, Belgium, and Taiwan. Bias assessment revealed a low risk of bias for every domain assessed (Figures 2 and 3), with detailed characteristics summarized in Table 1. Studies involved a total of 221 participants, ranging from 50 to 71 years old, with advanced or recurrent ovarian cancer who had already received a cycle of neoadjuvant chemotherapy. The control group received traditional or laparotomy interval debulking surgery, while the intervention group received robotic interval debulking surgery.
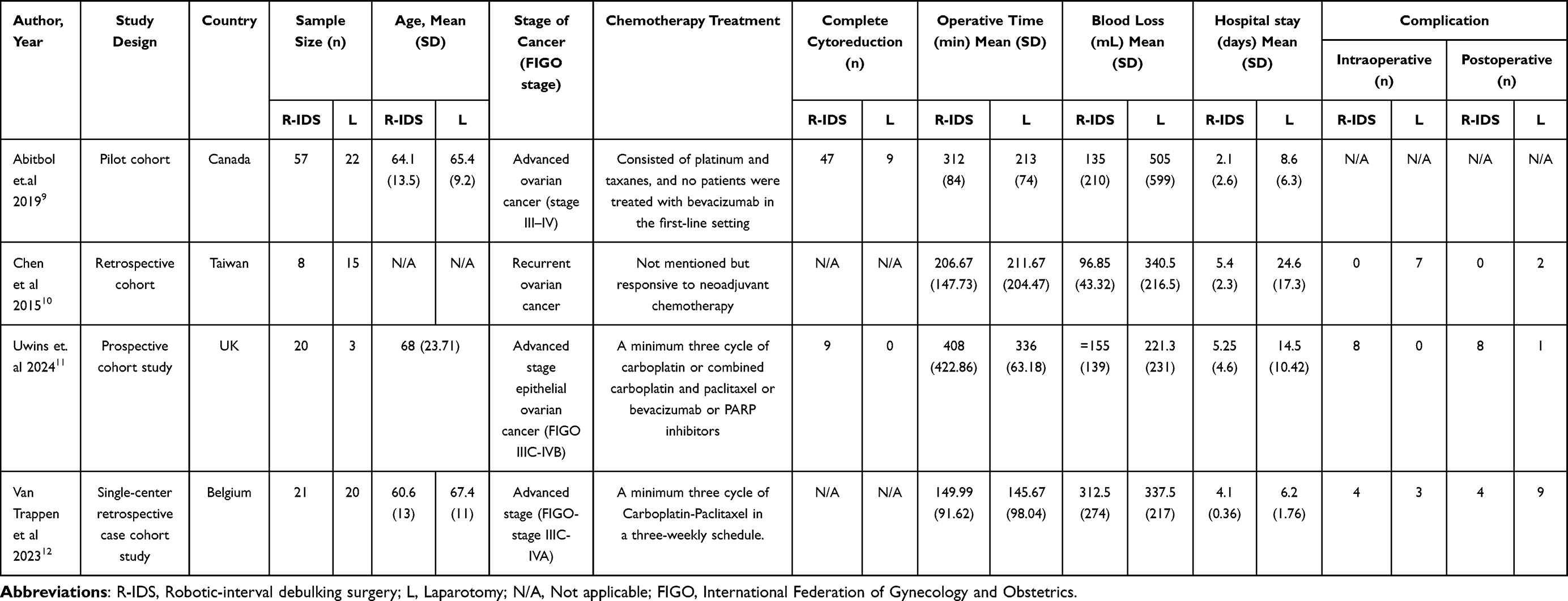 |
Table 1 Characteristic Table of the Included Study |
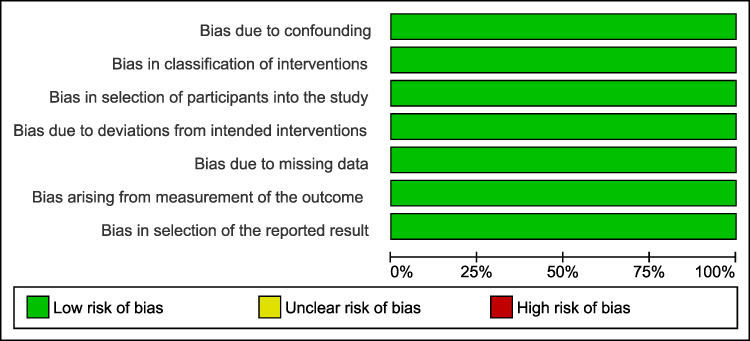 |
Figure 2 Risk of Bias Graph using ROBINS-I. |
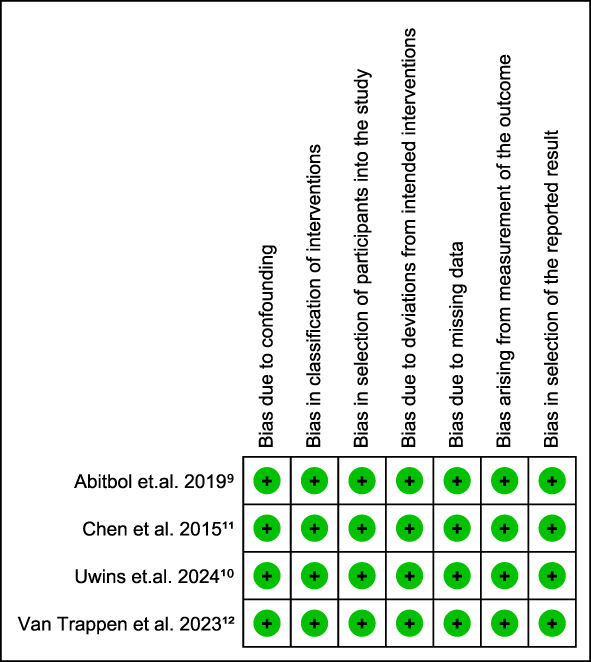 |
Figure 3 Risk of Bias Summary using ROBINS-I. |
Outcomes
Complete Cytoreduction
The only studies that included the analysis of complete cytoreduction were the ones by Abitbol et al 20199 and Uwins et al 2024.11 According to Figure 4, with an OR=6.67 [95% CI: 2.39–18.64, p=0.0003] the Robotic IDS shows a higher likelihood of having complete cytoreduction. This finding may significantly improve the course of the disease. Also, there was no evidence of significant heterogeneity (I2=0%, pheterogeneity =0.92)
 |
Figure 4 The Impact of Interval Debulking Surgery on Complete Cytoreduction in Ovarian Cancer Patients. |
Operative Time
All four studies were included.9–12 It was not statistically significant, and Figure 5 showed that laparotomy had a slightly faster time than the robotic IDS (SMD = 0.40 [95% CI: −0.30–1.11, p = 0.26]). This refers to the time needed from skin incision to skin closure, and the longer time needed is due to the complexity and precision required. As an addition, this study discovered a high level of heterogeneity (I2=72%, pheterogeneity =0.01)
 |
Figure 5 The Impact of Interval Debulking Surgery on Operative Time in Ovarian Cancer Patients. |
Estimated Blood Loss
The effect of the intervention on estimated blood loss is shown in Figure 6. A meta-analysis revealed that, in comparison to laparotomy, those who used robotic IDS experienced less estimated blood loss (SMD = −0.71; 95% CI = −1.29 – −0.13, p= 0.02). Furthermore, it demonstrates statistical significance with moderate heterogeneity (I2=57%, pheterogeneity =0.07). This suggests a moderate level of consistency in the findings across different studies, reinforcing the reliability of the observed effect.
 |
Figure 6 The Impact of Interval Debulking Surgery on Estimated Blood Loss in Ovarian Cancer Patients. |
Hospital Stay
Figure 7 depicts a meta-analysis of hospital stay durations for robotic IDS and laparotomy. The pooled standardized mean difference (SMD) of −1.58 (95% CI: −1.96 to −1.20) suggests that robotic IDS use results in a significantly shorter hospital stay. Overall, the effect is very substantial (Z=8.10, p<0.00001) with no evidence of significant heterogeneity (I2=0%, pheterogeneity< 0.94). These results demonstrate that, compared with laparotomy, robotic IDS is more effective at minimizing hospital stays.
 |
Figure 7 The Impact of Interval Debulking Surgery on Hospital Stay in Ovarian Cancer Patients. |
Intraoperative Complications
Figure 8 presents a meta-analysis comparing intraoperative complication rates between robotic interval debulking surgery (IDS) and laparotomy. The odds ratio of 0.82 (95% CI: 0.10–6.99) indicates a trend toward fewer intraoperative complications with robotic IDS. However, this difference is not statistically significant (Z = 0.18, p = 0.86), and heterogeneity is moderate (I2 = 54%, pheterogeneity = 0.11). These findings suggest that while robotic IDS may be associated with a lower likelihood of intraoperative complications compared to laparotomy, the evidence remains inconclusive, necessitating further investigation to establish definitive clinical benefits.
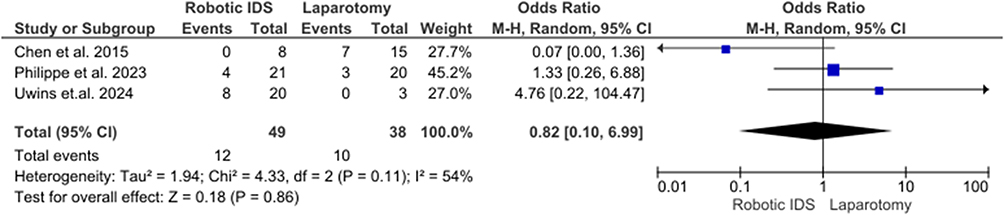 |
Figure 8 The Impact of Interval Debulking Surgery on Intraoperative Complication Rate in Ovarian Cancer Patients. |
Postoperative Complications
Figure 9 showcases a meta-analysis comparing postoperative complication rates between robotic and laparotomic interval debulking surgery (IDS). With an odds ratio of 0.40 (95% CI: 0.13–1.24), the results indicate a possible reduction in postoperative complications associated with robotic IDS. Although statistical significance is not achieved (Z = 1.59, p = 0.11), the low heterogeneity (I2 = 0%, pheterogeneity= 0.58) suggests consistency across studies.
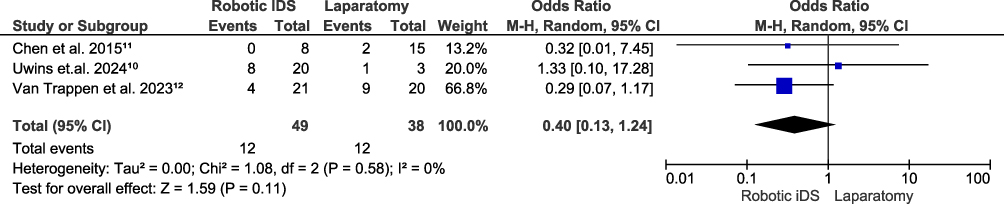 |
Figure 9 The Impact of Interval Debulking Surgery on Postoperative Complication Rate in Ovarian Cancer Patients. |
Discussion
Principal Findings
Robotic interval debulking surgery (R-IDS) represents a significant advancement in the surgical management of advanced-stage ovarian cancer (Stage III–IV) and recurrent ovarian cancer, including improved complete cytoreduction rates, reduced blood loss, and shorter hospital stay. These benefits are supported by enhanced surgical precision through 3D visualization and superior instrument control. Recent advances in minimally invasive technology further strengthen this approach. Earlier single-port systems, such as the da Vinci Single-Site platform, offered cosmetic advantages but were limited by reduced dexterity and a non-articulating instrument. The newer da Vinci SP system addresses these limitations by delivering an articulating camera and three flexible EndoWrist SP instruments to improve triangulation and access in narrow pelvic spaces.13 Despite these advantages, many patients remain unaware of the potential benefits of robotic-assisted surgery. Prior studies indicate that 75% of patients are eligible for robotic IDS, highlighting its feasibility as an alternative to conventional laparotomy in selected cases.4
The challenge lies in achieving optimal debulking in recurrent and advanced-stage ovarian cancer (Stage III to IV), particularly in cases with extensive disease involvement. Such procedures are often complex, potentially requiring extensive bowel resection, significant blood loss, and an increased risk of morbidity. In situations where primary debulking surgery is challenging, induction neoadjuvant chemotherapy may help reduce tumor size. If the tumor responds well after a few cycles, robotic IDS may become an accessible option.
Align with that, our meta-analysis’s findings which were also supported by Psomiadou et al,14 reveals robotic IDS is associated with a significantly reduced estimated blood loss (SMD = −0.71; [95% CI = −1.29–-0.13], p = 0.02) and hospital stay (SMD = −1.58; [95% CI = −1.96–-1.20, p < 0.00001). In addition, the majority of debulking surgeries achieved 80% complete cytoreduction, with a higher proportion in patients undergoing robotic IDS than in those receiving laparotomy (74.5% vs 53.1%), respectively.14 Our results also align with those studies, with a significant result for robotic IDS (OR=6.67 [95% CI: 2.39–18.64, p=0.0003]). Moreover, studies have revealed a lower prevalence of complications in the robotic IDS group.15 Our findings show that the robotic IDS could reduce intraoperative (Z = 0.18, p = 0.86) and postoperative (Z = 1.59, p = 0.11) complications, but these differences were not statistically significant. Lastly, robotic IDS has a longer operative time than laparotomy in all studies and in our results, due to the complexity and precision required (SMD = 0.40 [95% CI: −0.30–1.11, p = 0.26]).
Furthermore, we were unable to provide prognostic factors, such as progression-free and overall survival, due to limited data. One included study reported that the overall survival was 42.8 months in the robotic IDS group, compared to 37.9 months in the laparotomy group.9 However, these findings should be interpreted cautiously in the context of microscopic residual disease (MRD), which may persist even when no macroscopic disease is visible, particularly in the pelvis and mid-abdomen.16 MRD in three or more anatomical areas has been shown to increase relapse risk significantly.16 This consideration is highly relevant because, although robotic IDS is designed to enhance precision in cytoreduction, microscopic foci of disease may still escape detection intraoperatively. Integrating MRD data into the interpretation of survival outcome provides essential context, suggesting that even in cases of apparent optimal cytoreduction, the burden and distribution of MRD may influence long-term prognosis regardless of surgical approach.
Implications in Clinical Practice
Robot-assisted interval surgery has significant clinical implications. By enhancing surgical precision, visualization, and patient recovery, this approach has the potential to improve the completeness of cytoreduction, a critical determinant of survival outcomes in advanced and recurrent ovarian cancer. Additionally, reduced surgical trauma may translate to reduced estimated blood loss and shorter hospital stays. If validated in clinical trials, robot-assisted interval debulking surgery could be adopted as a new standard of care, bridging the gap between maximal cytoreduction and minimally invasive robotic approaches, and ultimately improving both short- and long-term outcomes for women with ovarian cancer.
Strength and Limitations
The main advantage of this study is that, to the best of our knowledge, it is the first meta-analysis that compares robotic interval debulking surgery and laparotomy in ovarian cancer. The bias risk associated with each included study was carefully assessed and found to be low, indicating the quality of the studies. Furthermore, this offers a more helpful perspective while making clinical decisions. There are a few restrictions that must be considered, though. First, some of the studies had quite diverse sample sizes. Second, the study was restricted to America, Europe, and Asia, suggesting that, at present, this kind of research is still uncommon, especially in middle- and lower-income countries, yet it offers a robust innovation. Third, the number of included studies in this analysis was limited because not all studies reported comparisons of interval debulking surgery with laparotomy in ovarian cancer populations, along with their surgical outcomes and follow-up profiles. However, follow-up profiles, including overall and progression-free survival, were reported in only one study. As a result, only a small number of variables could be analyzed using meta-analysis.
Conclusion
This study revealed that robotic-assisted interval debulking surgery shows promising surgical outcomes in women with recurrent and advanced stages of ovarian cancer. The small number of included studies and the moderate risk of bias in the adequacy of follow-up cohort parameters should be considered when interpreting the findings. Additional research is required to validate these results.
Acknowledgments
The authors express their gratitude to Mas Rizky A.A. Syamsunarno for his guidance and support, particularly in facilitating our coordination with the relevant stakeholders. Additionally, acknowledge the assistance of Fayyaza Faiz Adams in the ideation and screening process.
Funding
Internal Research Grant from Universitas Padjadjaran.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hendrick RE, Monticciolo DL. Surveillance, epidemiology, and end results data show increasing rates of distant-stage breast cancer at presentation in U.S. women. Radiology. 2024;313(3):e241397. doi:10.1148/RADIOL.241397
2. Ovarian cancer statistics | world cancer research fund. Available from: https://www.wcrf.org/preventing-cancer/cancer-statistics/ovarian-cancer-statistics/.
3. Davidson BA, Broadwater G, Crim A, et al. Surgical complexity score and role of laparoscopy in women with advanced ovarian cancer treated with neoadjuvant chemotherapy. Gynecol Oncol. 2019;152(3):554–10. doi:10.1016/J.YGYNO.2018.12.011
4. Carbajal-Mamani SL, Schweer D, Markham MJ, et al. Robotic-assisted interval cytoreductive surgery in ovarian cancer: a feasibility study. Obstet Gynecol Sci. 2020;63(2):150–157. doi:10.5468/OGS.2020.63.2.150
5. Martinez A, Ngo C, Leblanc E, et al. Surgical complexity impact on survival after complete cytoreductive surgery for advanced ovarian cancer. Ann Surg Oncol. 2016;23(8):2515–2521. doi:10.1245/s10434-015-5069-z
6. Menderes G, Black JD, Azodi M. The role of minimally invasive interval debulking surgery in advanced epithelial ovarian cancer. Expert Rev Anticancer Ther. 2016;16(9):899–901. doi:10.1080/14737140.2016.1219658
7. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:372. doi:10.1136/BMJ.N71
8. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14(1). doi:10.1186/1471-2288-14-135
9. Abitbol J, Gotlieb W, Zeng Z, et al. Incorporating robotic surgery into the management of ovarian cancer after neoadjuvant chemotherapy. Int J Gynecological Cancer. 2019;29(9):1341–1350. doi:10.1136/IJGC-2019-000413
10. Chen HH, Chen CH, Liu WM. Comparison of robotics, laparoscopy and laparotomy in the management of recurrent ovarian cancer. J Minim Invasive Gynecol. 2015;22(6):S239. doi:10.1016/j.jmig.2015.08.839
11. Uwins C, Assalaarachchi H, Bennett K, et al. MIRRORS: a prospective cohort study assessing the feasibility of robotic interval debulking surgery for advanced-stage ovarian cancer. Int J Gynecological Cancer. 2024;34(6):886–897. doi:10.1136/IJGC-2024-005265
12. Van Trappen P, De Cuypere E, Claes N. Robotic surgery in early and advanced ovarian cancer: case selection for surgical staging and interval debulking surgery. Eur J Obstetrics Gynecol Reprod Biol. 2023;280:7–11. doi:10.1016/j.ejogrb.2022.11.005
13. Chiofalo B, Bruno V, Mancini E, et al. Feasibility and safety of robotic single-port surgical staging in epithelial ovarian cancer using the da Vinci SP platform: a preliminary experience. Int J Gynecological Cancer. 2025;35(8):101977. doi:10.1016/j.ijgc.2025.101977
14. Psomiadou V, Prodromidou A, Fotiou A, Lekka S, Iavazzo C. Robotic interval debulking surgery for advanced epithelial ovarian cancer: current challenge or future direction? A systematic review. J Robot Surg. 2021;15(2):155–163. doi:10.1007/s11701-020-01155-7
15. Cardenas-Goicoechea J, Wang Y, McGorray S, et al. Minimally invasive interval cytoreductive surgery in ovarian cancer: systematic review and meta-analysis. J Robot Surg. 2019;13(1):23–33. doi:10.1007/S11701-018-0838-X
16. Di Donato V, Caruso G, Golia D’Augè T, et al. Prognostic impact of microscopic residual disease after neoadjuvant chemotherapy in patients undergoing interval debulking surgery for advanced ovarian cancer. Arch Gynecol Obstet. 2025;311(2):429–436. doi:10.1007/s00404-024-07775-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.