Back to Journals » OncoTargets and Therapy » Volume 11
The return of gemtuzumab ozogamicin: a humanized anti-CD33 monoclonal antibody–drug conjugate for the treatment of newly diagnosed acute myeloid leukemia
Received 9 August 2018
Accepted for publication 16 October 2018
Published 22 November 2018 Volume 2018:11 Pages 8265—8272
DOI https://doi.org/10.2147/OTT.S150807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Takuya Aoki
Pamela C Egan, John L Reagan
Division of Hematology and Oncology, Rhode Island Hospital, The Alpert Medical School of Brown University, Providence, RI, USA
Abstract: Through the years gemtuzumab ozogamicin (GO) has moved from a panacea in the treatment of acute myeloid leukemia (AML) to a pariah and back again. Early promise of targeted therapy with accelerated approval in the United States in 2000 gave way to fear over increased toxicity in the absence of efficacy, which subsequently resulted in the drug manufacturer voluntarily withdrawing GO from the market in 2010. We outline the history of GO in terms of initial drug development and early clinical trials that ultimately led the way to GO frontline use in AML based on a series of Phase III studies. Among these studies, we discuss the similarities and differences in terms of dosing, frequency, response rates, and toxicities that ultimately led to the re-approval of GO in 2017 based on efficacy, particularly in patients with core-binding factor (CBF) leukemia. Herein, we also review the clinical efficacy of GO in the frontline treatment of acute promyelocytic leukemia, which is based on either initial patient high-risk disease or potential co-morbidities that preclude the use of arsenic trioxide (ATO). Finally, we assess the current evidence for biomarkers aside from initial cytogenetics that may predict a favorable response to GO.
Keywords: leukemia, AML, treatment, core binding factor
Introduction
From the 1970s to 2000, the treatment of acute myeloid leukemia (AML) remained essentially stagnant.1 Most patients with a good performance status received a combination of an anthracycline and cytarabine. Meanwhile, patients with a poor performance status received best supportive care and, predictably, outcomes remained dismal.1,2 While the treatment of patients not eligible for intensive therapy changed significantly with the advent of hypomethylating agents, progress in the treatment of patients suitable for intensive therapy was limited to the refinement of dosing and schedules.2 The efforts to elucidate different subtypes of AML based on molecular and cytogenetic changes raised great hopes of improvements in therapies with targeted agents, and in the last 2 years those improvements have begun to take shape.3,4 Played out in parallel to this overarching story of promise, disappointment, and newfound promise is the saga of gemtuzumab ozogamicin (GO), the first antibody–drug conjugate to be approved for cancer treatment.5,6
With its approval in 2000 for the single-agent treatment of relapsed/refractory AML, GO was among the first wave of the new age of cancer drugs that seemed poised to change the course of cancer treatment with the promise of precision treatment based on direct chemotherapeutic targeting of cluster of differentiation 33 (CD33). When an interim analysis showed no benefit and increased induction fatalities, GO was removed from the market in 2010.7 The results of a subsequent trial, ALFA-0701, and an individual patient level data meta-analysis of GO used in the frontline setting showing a survival benefit led to its re-approval in 2017.7
In light of this approval, for both newly diagnosed adults with CD33-positive AML and patients 2 years of age and older with relapsed/refractory CD33-positive AML, we endeavor to review the drug’s history from pre-clinical promise and initial early data supporting it’s conditional approval to the events that led to its removal from the market and the subsequent clinical data that allowed re-approval.
Pre-clinical data
CD33, or myeloid differentiation antigen, is expressed only on hematopoietic cells committed to the myeloid lineage and is expressed on the surface of the majority of AML blasts.8 Development of GO grew out of the thought that specifically targeting the CD33 antigen would spare the presumably normal precursors and allow for restoration of normal hematopoiesis.5,8,9 This idea was supported in work by Bernstein et al that demonstrated that CD33-CD34+ cells from patients with CD33+ AMLs in vitro grew normal colony-forming cells.10
It was first demonstrated that an anti-CD33 radio-immunoconjugate was efficiently internalized by CD33-positive cells, first in a xenograft murine model and then in humans.11,12 Collaborators in academia then worked with industry to develop a humanized anti-CD33 antibody conjugated with a derivative of calicheamicin, a chemotherapeutic agent that causes tumor cell death through DNA binding and resultant double strand cuts.5,9,13 The bond between antibody and drug is stable in circulation and then dissolves, once intracellular, to allow the calicheamicin to bind with the DNA.6 This drug antibody conjugate, CMA-676, became known as GO.
Early trials and initial approval
The first trial to use GO was a Phase I dose escalation study in 40 adult patients (age 16–70) with relapsed or refractory AML, more than 50% of whom had poor risk disease.14 Three patients had a complete remission (CR) and five had a CR with incomplete platelet recovery (CRp); the idea of CRp as a response to be included in overall response (OR) was a designation novel to this trial.6,14 Infusion reactions, prolonged myelosuppression, and reversible hepatotoxicity were the most frequent adverse effects.14 This trial defined a dose of 9 mg/m2 as the target dose for subsequent trials.6
Three Phase II trials were conducted in 142 adults with de novo AML in the first relapse at a dose of 9 mg/m2 every 2 week for two doses. The side effect profile was consistent with that identified in the Phase I trial while the OR rate was 30% (16% CR, and 13% CRp); it was noted that hepatotoxicity was increased in patients with post allogeneic stem cell transplant (allo-SCT) and three patients who went for transplant after GO died of sinusoidal obstruction syndrome (SOS).14 Based on these studies, the drug was granted accelerated approval with the rationale that patients over 60 with relapsed AML would benefit. However, the approval was contingent on the design and success of prospective randomized trials for which the S0106 trial was specifically designed.6
GO incorporation into induction
The use of GO as induction therapy has been extensively evaluated in five large randomized controlled studies (Tables 1 and 2) from which patient level data were incorporated into one meta-analysis (Figure 1). The UK MRC AML15 Phase III randomized controlled trial (RCT) examined the use of GO in induction and consolidation in 1,113 younger (predominantly less than 60 years old) patients with non-acute promyelocytic leukemia (APL) AML across all risk groups15 (Table 1). Patients were randomized to GO 3 mg/m2 for one dose on D1 of induction and consolidation chemotherapy. Within this study, the chemotherapy backbone was also randomized (Table 2). Transplant was allowed in first CR for non-favorable risk patients and for intermediate risk patients if a matched sibling donor was available. There was no difference in OR, early mortality, 5-year overall survival (OS), 5-year relapse-free survival (RFS), or treatment-related mortality (TRM). However, in pre-planned analysis there was a significant survival benefit by the addition of GO to induction in patients with favorable risk disease and a trend toward a survival benefit for patients with intermediate risk disease. There was no benefit of GO use in consolidation.
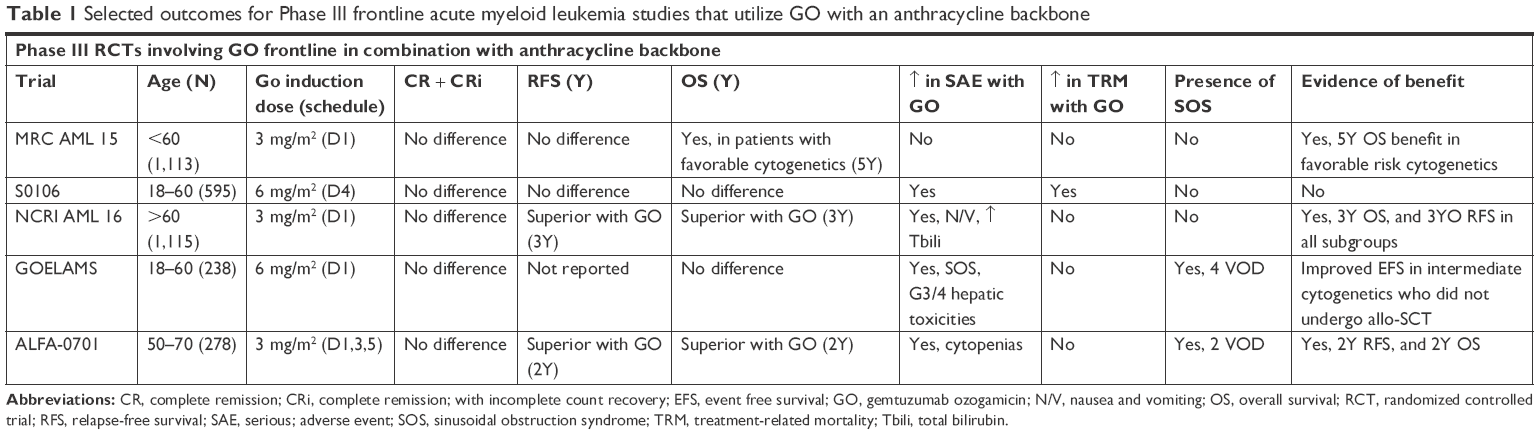 | Table 1 Selected outcomes for Phase III frontline acute myeloid leukemia studies that utilize GO with an anthracycline backbone |
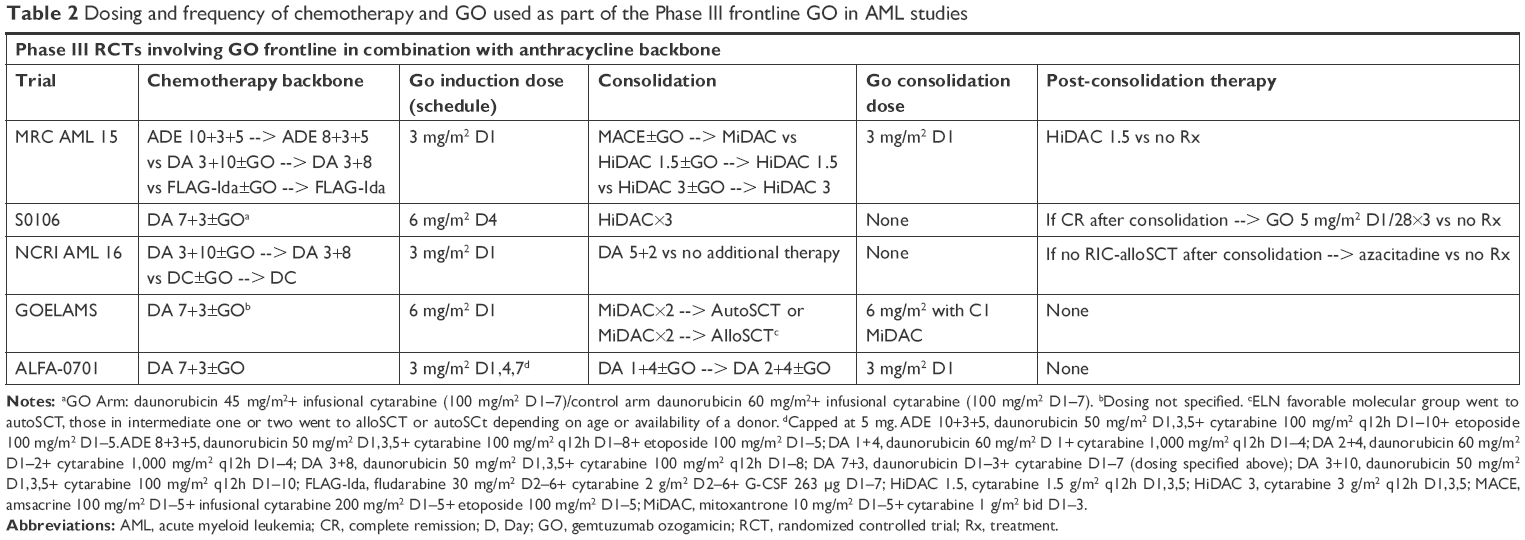 | Table 2 Dosing and frequency of chemotherapy and GO used as part of the Phase III frontline GO in AML studies |
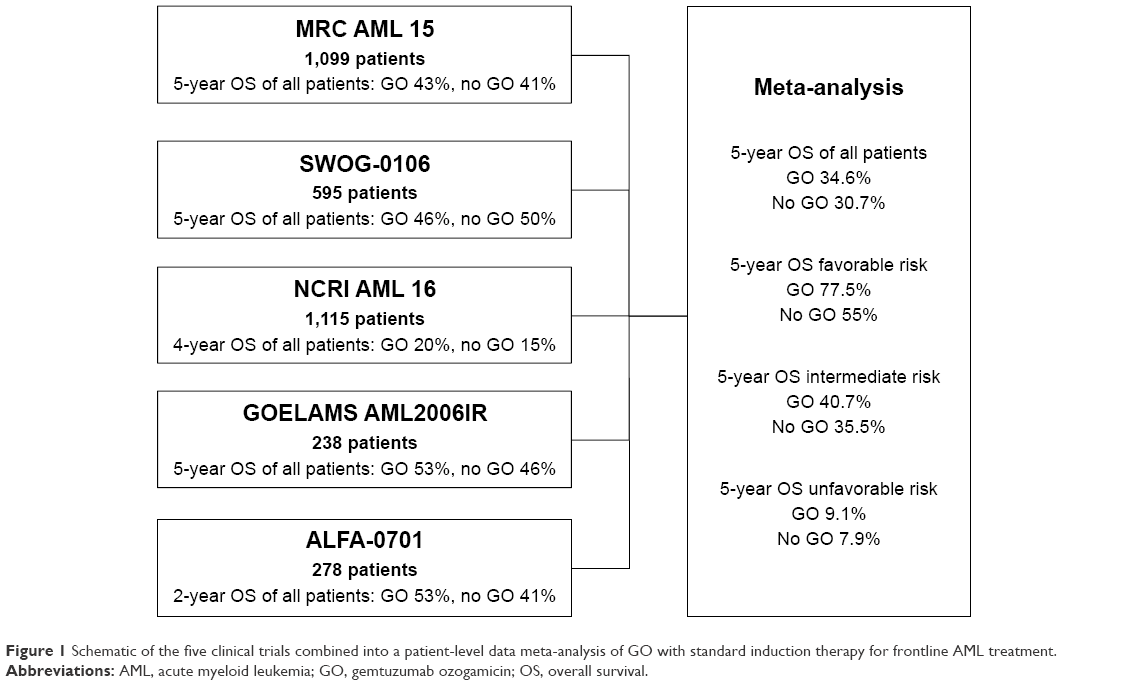 | Figure 1 Schematic of the five clinical trials combined into a patient-level data meta-analysis of GO with standard induction therapy for frontline AML treatment. |
The SWOG S0106 Phase III RCT examined the use of GO in induction and post-consolidation for younger patients (18–60) with non-APL AML across all risk groups16 (Table 1). Patients were randomized to receive GO 6 mg/m2 on day 3 (D3) with daunorubicin 45 mg/m2 D1–3 and cytarabine 100 mg/m2 D1–7 or the same dose of daunorubicin and cytarabine without GO. After consolidation with three courses of high-dose cytarabine, patients remaining in CR were again randomized to GO 5 mg/m2 every 28 days ×3 doses. There was an increase in fatal toxicities during induction in the + GO group and no benefit in CR or disease-free survival (DFS), which subsequently led to accrual closure in 2009 and raised concerns over the continued use of GO.
The first Phase-III RCT to use GO in the frontline induction regimens for older AML and high-risk myelodysplastic syndrome patients was the subsequent UK NCRI AML16 trial17 (Table 1). Patients included were across all risk groups although, notably not surprisingly, in a study of older AML patients, favorable risk patients were underrepresented in comparison to other trials. Patients received GO 3 mg/m2 on D1 induction with a randomized chemotherapy backbone followed by randomly assigned consolidation (without GO) vs no consolidation (Table 2). Patients who did not subsequently go to transplant, which was a vast majority of included patients, were randomized to azacitidine maintenance vs no maintenance. Notably, in the GO cohort there was a 3-year cumulative incidence of relapse (68% vs 76%) and OS (25% vs 20%) benefit in all risk groups and no increased toxicities.
In the French GOELAMS AML 2006IR study, 238 patients between 18 and 60 years of age who had been randomized to a standard 7+3 induction with or without GO 6 mg/m2 were analyzed18 (Table 1). GO was also incorporated into a first mitoxantrone and intermediate dose cytarabine consolidation course. CR rates were high with 92% of the GO group attaining CR and 86.5% of the standard care group. Toxicities were more prevalent in the GO cohort as four patients developed SOS and more Grades 3 and 4 hepatic toxicities were seen (23% vs 13%, P=0.031). There was no difference in 3-year (event free survival (EFS) (51% vs 33%) or OS (53% vs 46%) in the GO compared to the standard arm. Interestingly though, they did find significantly improved 3-year EFS (54% vs 27%) for the GO arm in the subset of patients who could not go on to consolidative allo-SCT although this improvement did not carry over to OS and was seen primarily in patients with intermediate risk molecular classification.
The ALFA-0701 trial was a Phase-III RCT designed to evaluate the effect of adding GO to a backbone of 7+3 (DNR 60 mg/m2) in patients aged 50–70 with newly diagnosed non-APL AML19 (Table 1). Patients received 3 g/m2 GO on D1, 4, and 7. Patients in CR or CRp were then given consolidation with or without GO based on initial randomization. There was a significant improvement in OS, 2-year EFS, and 2-year RFS in the GO group. In a subgroup analysis, cytogenetics and genotype were the only important prognostic factors aside from treatment group. When adjusted for these factors, the GO group showed improved EFS and RFS but not OS. There was no increased risk of fatal toxicities in the GO group, but there were two cases of fatal SOS, with one occurring during induction while the other occurred during consolidation.
Based on the results of these five trials, an individual patient-level data meta-analysis was undertaken (Figure 1). The Hills et al meta-analysis found that with the addition of GO although CR was not improved, the risk of relapse (RR) was reduced (OR 0.81, 95% CI 0.73–0.9, P=0.0001), and 5-year OS increased (OR 0.9, 95% CI 0.82–0.98, P=0.01).20 Results were unchanged when transplant patients were censored in sensitivity analysis. Patients with favorable risk cytogenetics had the largest benefit, intermediate risk cytogenetics had a smaller benefit, and adverse cytogenetics did not benefit. Transplanted patients given the 3 mg dose did not have increased 100-day mortality but 6 mg dose patients did show an increase. There was no evidence of any benefit linked to a particular chemotherapy backbone. Likewise, no benefit of GO administration was associated with NPM1 or FLT3 mutations, age, or gender. Importantly, this meta-analysis led to the reassessment of GO use and review of its licensing status.
Further trials that examined the use of GO in induction with intensive chemotherapy include the NCRI AML17 RCT, which compared the use of D1 3 mg vs 6 mg doses of GO in combination with anthracycline-based chemotherapy and found no difference in outcomes between doses, and did find increased toxicities, including increased early mortality, with the 6 mg dose.21 A trial to examine the fractionated dosing used in the ALFA-0701 trial and a one-time 3 mg flat dose on D1 is currently underway.21
In addition to concurrent use, GO has also been used sequentially with anthracycline-based chemotherapy. In the EORTC-GIMEMA AML-17 RCT, patients aged 61–75 years were randomized to either GO at a dose of 6 mg/m2 on D1 and D15 followed by induction with mitoxantrone, etoposide, and cytarabine.22 Patients who achieved remission were then randomized to receive consolidation with or without idarubicin, cytarabine, and etoposide. Out of 472 total patients, 223 (47%) attained CR and CRp. There was no benefit of the addition of GO regarding OS and early mortality/toxicities were greater, leading the authors to conclude that there is no role for GO-sequenced therapy as frontline treatment for AML patients over 60.
In the frontline monotherapy realm, the EORTC-GIMEMA AML-19 RCT studied the use of GO as monotherapy in 237 patients aged 61 or older, who were unfit for intensive therapy and were randomized to GO vs best supportive care. The GO dose was 6 mg/m2 on D1 and 3 mg/m2 on D8. Those who had no progression of disease23 after the first cycle could receive monthly doses of 2 mg/m2 monthly for up to eight cycles. CR + complete remission with incomplete count recovery (CRi) were 27% in the GO group. There was a modest but statistically significant median OS benefit in the GO group and the 1-year OS in the GO group was 24% vs 10% in the BSC group. There was no significant difference in toxicities. The survival benefit was, again most pronounced in favorable cytogenetic risk groups, in women, and in patients with more than 20% CD33 expression, which was a finding unique to this trial.
GO in APL
In APL, CD33 was initially selected as a target based on its persistence in patients with minimal residual disease (MRD). The subsequent recognition that therapeutic targeting of this antigen could convert MRD-positive to MRD-negative status with resultant prolonged periods of remission led to its further development.24
The first report of GO for the treatment of APL was a patient who attained a prolonged remission after being given two doses of GO in the third relapse.25 This was followed up by an initial trial of GO in combination with all-trans retinoic acid (ATRA) for the frontline treatment of APL. GO was given as 9 mg/m2 on either D1 or 5 during induction with an additional eight doses of GO 9 mg/m2 administered every 4–5 weeks for those patients in CR. Sixteen of 19 (84%) patients attained CR.26 A later study from the same center incorporated GO with ATRA and arsenic trioxide (ATO) on D1 for high-risk patients, who were defined as patients with a WBC count on presentation of ≥10×109/L. The CR and CRi rate was 92% with an estimated 3-year OS of 85%.27
The utility of GO for high-risk patients was later confirmed in the UK MRC AML 17 multi-center trial, albeit with a reduced dose of GO at 6 mg/m2 on D1 for those patients randomized to ATRA and ATO. Out of 30 high-risk patients who were treated with ATRA and ATO, 28 received GO. Although the 4-year OS of the group was 89%, the authors were unable to conclude what effect GO had on OS due to lack of randomization.28
Recently, the long-term outcome of gemtuzumab was reported when combined with ATRA and ATO for high-risk patients and low-risk patients who developed leukocytosis during induction. In this analysis of three prospective studies on 187 patients, the overall CR rate was 96%. Of the 133 low risk patients, 45% required either GO or idarubicin for leukocytosis. The 5-year event free and OS rates were 85% and 88%, respectively.29 Although not randomized, these results suggest a clear role for frontline GO in high-risk disease, and for low-risk disease when leukocytosis occurs. Moreover, the addition of GO to frontline treatment of APL should be considered in APL patients with cardiac issues that preclude the use of ATO.30
Biomarkers for GO response
Given the heterogeneity seen in the above responses to GO, the next logical step was to determine if there were leukemia-specific genetic and protein expression factors that could predict response aside from conventional karyotype. In a prospective review of GO, containing regimens as part of the Children’s Oncology Group, Pollard et al studied the association of CD33 expression in response and found that high CD33 expressers were associated with poor-risk disease features like FLT-3/internal tandem duplication mutations and served as independent predictors of worse outcomes.31 In a follow-up study, they then examined the effects of GO based on CD33 expression and determined that, in pediatric AML, GO lacks efficacy in patients with low CD33 expression but decreased risk of relapse (32% vs 49%, P<0.001) and improved EFS (53% vs 41%, P=0.005) in the GO cohort.32 Improved outcomes with GO for patients with high expression of CD33 was later confirmed in adults as well.33 Interestingly, in adults, low CD33 expression is associated with adverse cytogenetics and core-binding factor (CBF) leukemia. Therefore, the authors concluded that the patients least likely to benefit from GO at the lower, now standard dose, are non-CBF leukemia patients with low CD33 expression.
Based on the favorable association of CD33 expression with clinical response, researchers next examined whether single nucleotide polymorphisms (SNPs) in CD33 were also predictive of response. The coding SNPs rs35112940 and rs12459419 were among those SNPs initially found to be associated with clinical outcomes in patients aged 0–29.34 More recently, the CC genotype for rs12459419 was shown to predict response to GO among patients in the same age group by virtue of decreased relapse rate (26% vs 49%; P<0.001) and improved DFS (65% vs 46%, respectively; P=0.004) in the GO vs no GO arm.35 The same group developed an “SNP score” to identify patients who would benefit clinically from the addition of GO in their treatment.36 However, Gale et al subsequently reported that, in an analysis of patients enrolled in the UKMRC AML 15 and NCRI AML 17 trials, they were unable to demonstrate a similar predictive effect of the CC genotype despite a similar distribution of genotype frequencies and CD33 expression.37 As it stands, there is currently no clear role for using knowledge of SNP genotypes to guide clinical practice in adults, but we eagerly anticipate further developments in this area.
Discussion
GO was removed from the market for two issues, lack of demonstrated efficacy and evidence of increased toxicity. However, this removal appears to have been premature, as high-quality data reported subsequently supported both the safety and efficacy of GO in induction. This highlights the potential pitfalls when basing conditional approval of new drugs on a single trial. Indeed, there were thoughtful and well-substantiated pleas in literature, well before the re-approval of the drug, to consider the data available outside of the S0106 trial.38
The S0106 was ended early due to an increase in induction deaths. However, there were three major issues with this trial. The first is, as the authors of the study note, the death rate in induction in the control group was remarkably low at 1.4%.39 This is well below the expected rate of approximately 5% based on the outcomes of previous trials, Furthermore, the induction fatality rate in the GO group was actually comparable to what would be expected with standard anthracycline based induction.39 Second, GO was administered on D4 in this trial, but in all other trials was given on D1. Notably, in the MRC AML 16 trial, GO was given on D1 unless WBC count was high and then it was given on D4. In the patients who received it on D4, the benefit appeared to be less.17 Furthermore, the daunorubicin dose in the GO group was 45 mg/m2 in induction, which has been demonstrated to be less effective,40–42 while the safety of full-dose anthracycline and GO has been established.
In terms of safety, the four subsequently reported GO frontline RCTs have not borne out the previous safety concerns, although the heterogeneity of the trial designs can make this a daunting task. First, in none of the subsequent trials was there an increase in TRM when GO was added to induction therapy. There was, however, some increase in serious incidences. What is notable, however, is that these appear to be dose dependent and at the approved fractionated dosing schedule, they do not appear to outweigh the potential benefit of the drug. Indeed, the one trial after the S0106 that used a 6 mg/m2 dose had a significant increase in Grades 3 and 4 hepatic toxicities and had four cases of SOS. With the use of a one-time 3 mg/m2 dose that was used in both the UK MRC AML15 and NCRI AML16, there were only increased nausea and vomiting along with mild total bilirubin elevations in the NCRI16 trial, which notably was composed of older leukemics. The intermediate, fractionated dosing used in ALFA-0701 had significantly increased cytopenias but did not result in increased fatalities. There were two cases of fatal SOS in the ALFA-0701 trial, and none in the two trials that used a D1 3 mg/m2 dose. This may lead some to exercise caution in using GO in the fractionated dosing scheduled in patients who will go on to transplant. It may be that the ideal dosing schedule is as yet, not defined. A one-time D1 3 mg/m2 dose as used in the MRC15 trial appears to be the safest, and has a survival benefit in patients with favorable cytogenetics.
So, if GO is deemed safe then the second question becomes whether or not it is effective. In a disease with such poor outcomes and slow therapeutic progress, the benefits associated with GO in the trials subsequent to S0106 are not to be ignored. Three of the four trials after S0106 demonstrated a small but significant OS benefit. In the MRC AML 15 trial, this was reserved for those with favorable cytogenetics (in a pre-planned subgroup analysis) but in MRC16 and ALFA-0701, this was seen among all patients. In the ALFA-0701, the effect was most pronounced in favorable or intermediate cytogenetics, but this was not a pre-planned subgroup analysis. In the meta-analysis of AML 15 and AML 16, the benefit is marked in those with favorable cytogenetics. In the Hills et al meta-analysis, however, there appears to be a marked benefit in patients with favorable cytogenetics. Indeed, the NCCN has incorporated the use of gemtuzumab into induction but specifies only in CBF AML.30 The lack of improved CR with GO in the presence of a survival benefit suggests that, perhaps, it improves survival by eradicating MRD, an area of active research in AML, and a possible future endpoint for GO use.
Our current institutional practice is to confirm CBF leukemia via fluorescence in situ hydribization prior to starting induction, provided the patient is stable enough to wait the 48–72 hours for this result. We then add GO to anthracycline-based induction in CBF leukemias only. It appears from the data that it is critical that GO is given on D1 of treatment; therefore, we prefer to have that data back before treatment initiation.
In a time of great excitement for the treatment of AML, when many new drugs have been approved in the last 2 years and even more new approvals are on the horizon, questions will continue to arise about which therapy is most suitable for certain patient populations. As seen in the case of GO, it will be important to fully evaluate not only the use of the drug but also how it is dosed, at what time it is given during treatment, at what frequency, and with what other combinations in order to ensure the maximum patient benefit to improve AML cure rates. As such, future Phase III RCTs will be necessary to separate toxicity and benefit across this heterogeneous AML landscape.
Disclosure
The authors report no conflicts of interest in this work.
References
Döhner H, Weisdorf DJ, Bloomfield CD. Acute Myeloid Leukemia. N Engl J Med. 2015;373(12):1136–1152. | ||
Alibhai SM, Leach M, Minden MD, Brandwein J. Outcomes and quality of care in acute myeloid leukemia over 40 years. Cancer. 2009;115(13):2903–2911. | ||
Stone RM, Mandrekar SJ, Sanford BL, et al. Midostaurin plus chemotherapy for acute myeloid leukemia with a FLT3 mutation. N Engl J Med. 2017;377(5):454–464. | ||
Dinardo CD, Stein EM, de Botton S, et al. Durable remissions with ivosidenib in IDH1-mutated relapsed or refractory AML. N Engl J Med. 2018;378(25):2386–2398. | ||
Appelbaum FR, Bernstein ID. Gemtuzumab ozogamicin for acute myeloid leukemia. Blood. 2017;130(22):2373–2376. | ||
Bross PF, Beitz J, Chen G, et al. Approval summary: gemtuzumab ozogamicin in relapsed acute myeloid leukemia. Clin Cancer Res. 2001;7(6):1490–1496. | ||
Norsworthy KJ, Ko CW, Lee JE, et al. FDA Approval summary: mylotarg for treatment of patients with relapsed or refractory CD33-positive acute myeloid leukemia. Oncologist. 2018;23(9):1103–1108. | ||
Walter RB, Appelbaum FR, Estey EH, Bernstein ID. Acute myeloid leukemia stem cells and CD33-targeted immunotherapy. Blood. 2012;119(26):6198–6208. | ||
Bernstein ID. Monoclonal antibodies to the myeloid stem cells: therapeutic implications of CMA-676, a humanized anti-CD33 antibody calicheamicin conjugate. Leukemia. 2000;14(3):474–475. | ||
Bernstein ID, Singer JW, Smith FO, et al. Differences in the frequency of normal and clonal precursors of colony-forming cells in chronic myelogenous leukemia and acute myelogenous leukemia. Blood. 1992;79(7):1811–1816. | ||
van der Jagt RH, Badger CC, Appelbaum FR, et al. Localization of radiolabeled antimyeloid antibodies in a human acute leukemia xenograft tumor model. Cancer Res. 1992;52(1):89–94. | ||
Scheinberg DA, Lovett D, Divgi CR, et al. A phase I trial of monoclonal antibody M195 in acute myelogenous leukemia: specific bone marrow targeting and internalization of radionuclide. J Clin Oncol. 1991;9(3):478–490. | ||
Zein N, Sinha AM, McGahren WJ, Ellestad GA. Calicheamicin gamma 1I: an antitumor antibiotic that cleaves double-stranded DNA site specifically. Science. 1988;240(4856):1198–1201. | ||
Sievers EL, Larson RA, Stadtmauer EA, et al; Mylotarg Study Group. Efficacy and safety of gemtuzumab ozogamicin in patients with CD33-positive acute myeloid leukemia in first relapse. J Clin Oncol. 2001;19(13):3244–3254. | ||
Burnett AK, Hills RK, Milligan D, et al. Identification of patients with acute myeloblastic leukemia who benefit from the addition of gemtuzumab ozogamicin: results of the MRC AML15 trial. J Clin Oncol. 2011;29(4):369–377. | ||
Petersdorf SH, Kopecky KJ, Slovak M, et al. A phase 3 study of gemtuzumab ozogamicin during induction and postconsolidation therapy in younger patients with acute myeloid leukemia. Blood. 2013;121(24):4854–4860. | ||
Burnett AK, Russell NH, Hills RK, et al. Addition of gemtuzumab ozogamicin to induction chemotherapy improves survival in older patients with acute myeloid leukemia. J Clin Oncol. 2012;30(32):3924–3931. | ||
Delaunay J, Recher C, Pigneux A, et al. Addition of Gemtuzumab Ozogamycin to Chemotherapy Improves Event-Free Survival but Not Overall Survival of AML Patients with Intermediate Cytogenetics Not Eligible for Allogeneic Transplantation. Results of the GOELAMS AML 2006 IR Study. Blood. 2011;118(21):79. | ||
Castaigne S, Pautas C, Terré C, et al; Acute Leukemia French Association. Effect of gemtuzumab ozogamicin on survival of adult patients with de-novo acute myeloid leukaemia (ALFA-0701): a randomised, open-label, phase 3 study. Lancet. 2012;379(9825):1508–1516. | ||
Hills RK, Castaigne S, Appelbaum FR, et al. Addition of gemtuzumab ozogamicin to induction chemotherapy in adult patients with acute myeloid leukaemia: a meta-analysis of individual patient data from randomised controlled trials. Lancet Oncol. 2014;15(9):986–996. | ||
Burnett A, Cavenagh J, Russell N, et al; UK NCRI AML Study Group. Defining the dose of gemtuzumab ozogamicin in combination with induction chemotherapy in acute myeloid leukemia: a comparison of 3 mg/m2 with 6 mg/m2 in the NCRI AML17 Trial. Haematologica. 2016;101(6):724–731. | ||
Amadori S, Suciu S, Stasi R, et al. Sequential combination of gemtuzumab ozogamicin and standard chemotherapy in older patients with newly diagnosed acute myeloid leukemia: results of a randomized phase III trial by the EORTC and GIMEMA consortium (AML-17). J Clin Oncol. 2013;31(35):4424–4430. | ||
Palareti G, Cosmi B, Legnani C, et al; PROLONG Investigators. D-dimer testing to determine the duration of anticoagulation therapy. N Engl J Med. 2006;355(17):1780–1789. | ||
Jurcic JG, DeBlasio T, Dumont L, Yao TJ, Scheinberg DA. Molecular remission induction with retinoic acid and anti-CD33 monoclonal antibody HuM195 in acute promyelocytic leukemia. Clin Cancer Res. 2000;6(2):372–380. | ||
Petti MC, Pinazzi MB, Diverio D, et al. Prolonged molecular remission in advanced acute promyelocytic leukaemia after treatment with gemtuzumab ozogamicin (Mylotarg CMA-676). Br J Haematol. 2001;115(1):63–65. | ||
Estey EH, Giles FJ, Beran M, et al. Experience with gemtuzumab ozogamycin (“mylotarg”) and all-trans retinoic acid in untreated acute promyelocytic leukemia. Blood. 2002;99(11):4222–4224. | ||
Ravandi F, Estey E, Jones D, et al. Effective treatment of acute promyelocytic leukemia with all-trans-retinoic acid, arsenic trioxide, and gemtuzumab ozogamicin. J Clin Oncol. 2009;27(4):504–510. | ||
Burnett AK, Russell NH, Hills RK, et al; UK National Cancer Research Institute Acute Myeloid Leukaemia Working Group. Arsenic trioxide and all-trans retinoic acid treatment for acute promyelocytic leukaemia in all risk groups (AML17): results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2015;16(13):1295–1305. | ||
Abaza Y, Kantarjian H, Garcia-Manero G, et al. Long-term outcome of acute promyelocytic leukemia treated with all-trans-retinoic acid, arsenic trioxide, and gemtuzumab. Blood. 2017;129(10):1275–1283. | ||
O’Donnell MR, Tallman MS, Abboud CN, et al. Acute Myeloid Leukemia, Version 3.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2017;15(7):926–957. | ||
Pollard JA, Alonzo TA, Loken M, et al. Correlation of CD33 expression level with disease characteristics and response to gemtuzumab ozogamicin containing chemotherapy in childhood AML. Blood. 2012;119(16):3705–3711. | ||
Pollard JA, Loken M, Gerbing RB, et al. CD33 Expression and Its Association With Gemtuzumab Ozogamicin Response: Results From the Randomized Phase III Children’s Oncology Group Trial AAML0531. J Clin Oncol. 2016;34(7):747–755. | ||
Khan N, Hills RK, Virgo P, et al. Expression of CD33 is a predictive factor for effect of gemtuzumab ozogamicin at different doses in adult acute myeloid leukaemia. Leukemia. 2017;31(5):1059–1068. | ||
Mortland L, Alonzo TA, Walter RB, et al. Clinical significance of CD33 nonsynonymous single-nucleotide polymorphisms in pediatric patients with acute myeloid leukemia treated with gemtuzumab-ozogamicin-containing chemotherapy. Clin Cancer Res. 2013;19(6):1620–1627. | ||
Lamba JK, Chauhan L, Shin M, et al. CD33 splicing polymorphism determines gemtuzumab ozogamicin response in de novo acute myeloid leukemia: report from randomized Phase III children’s oncology group trial AAML0531. J Clin Oncol. 2017;35(23):2674–2682. | ||
Lamba J, Chauhan L, Shin M. CD33-Single Nucleotide Polymorphism (CD33-SNP) Score Predicts Gemtuzumab Ozogamicin Response in Childhood Acute Myeloid Leukemia: Report from Children’s Oncology Group AAML0531 Trial. Blood. 2017;130(Suppl 1):3826. | ||
Gale RE, Popa T, Wright M, et al. No evidence that CD33 splicing SNP impacts the response to GO in younger adults with AML treated on UK MRC/NCRI trials. Blood. 2018;131(4):468–471. | ||
Rowe JM, Löwenberg B. Gemtuzumab ozogamicin in acute myeloid leukemia: a remarkable saga about an active drug. Blood. 2013;121(24):4838–4841. | ||
Petersdorf SH, Kopecky KJ, Slovak M, et al. A Phase 3 study of gemtuzumab ozogamicin during induction and postconsolidation therapy in younger patients with acute myeloid leukemia. Blood. 2013;121(24):4854–4860. | ||
Fernandez HF, Sun Z, Yao X, et al. Anthracycline dose intensification in acute myeloid leukemia. N Engl J Med. 2009;361(13):1249–1259. | ||
Löwenberg B, Ossenkoppele GJ, van Putten W, et al; Dutch-Belgian Cooperative Trial Group for Hemato-Oncology (HOVON); German AML Study Group (AMLSG); Swiss Group for Clinical Cancer Research (SAKK) Collaborative Group. High-dose daunorubicin in older patients with acute myeloid leukemia. N Engl J Med. 2009;361(13):1235–1248. | ||
Lee JH, Joo YD, Kim H, et al; Cooperative Study Group A for Hematology. A randomized trial comparing standard versus high-dose daunorubicin induction in patients with acute myeloid leukemia. Blood. 2011;118(14):3832–3841. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.