Back to Journals » Advances in Medical Education and Practice » Volume 17
The Resident Experience of Feedback in Clinical Training: Emotional, Cognitive, and Behavioural Responses: A Qualitative Study
Authors Alabdulghafour A, AlKhadragy R, Scanlan GM
Received 22 December 2025
Accepted for publication 22 May 2026
Published 19 June 2026 Volume 2026:17 586107
DOI https://doi.org/10.2147/AMEP.S586107
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Abrar Alabdulghafour,1 Rania AlKhadragy,2 Gillian Marion Scanlan2
1Pediatrics Department, Amiri Hospital, Kuwait City, Kuwait; 2Centre for Medical Education, Faculty of Health, Ninewells Hospital, Dundee, Scotland, UK
Correspondence: Abrar Alabdulghafour, Pediatrics Department, Amiri Hospital, Kuwait City, Kuwait, Tel +965-99782265, Email [email protected]
Background: Feedback is a key component of medical education and professional development, yet there is limited understanding of residents’ emotional, cognitive, and behavioral responses to feedback in clinical training settings. Previous studies, primarily using quantitative questionnaire-based approaches, have explored feedback experiences in medical education; however, limited research has examined these experiences in postgraduate pediatric training in Kuwait, particularly the cultural, interpersonal, and contextual factors that influence feedback. This study explored the experiences of pediatricians who completed residency training between 2015 and 2020.
Methods: This qualitative study used semi-structured, open-ended interviews. Eleven pediatric residents and three supervisors participated. Interviews were conducted face-to-face or online, recorded, manually transcribed, and analyzed using inductive thematic analysis. Data collection continued until sufficient information power was achieved.
Results: Five themes were generated through the researchers’ interpretive engagement with the data: factors influencing feedback experiences, consequences of feedback, learning how to provide feedback, characteristics of feedback received, and challenges in the feedback process. Participants described both supportive feedback that enhanced confidence and learning, and negative experiences that caused demotivation and uncertainty. Cultural hierarchy, institutional practices, and workload pressures strongly influenced these experiences.
Conclusion: This study provides new qualitative and contextual insights into feedback practices in postgraduate pediatric training in Kuwait.
Keywords: feedback, medical education, pediatrics, residency training, Kuwait
Introduction
Feedback provides learners with information about the quality of their academic or clinical performance.1 It is recognized as a central element in both teaching and learning, especially within medical education. However, the effect of feedback is not always the same. Depending on how it is delivered, it can have either a positive or a negative impact on the learner.2 For instance, feedback that is vague or overly judgmental may reduce motivation, affect emotions, and even damage relationships between supervisors and learners.3 In contrast, effective feedback supports learners in evaluating their own performance, developing self-monitoring skills,4 gaining self-awareness, identifying strengths and weaknesses, and staying motivated in their training.5 Despite this importance, learners’ perspectives of feedback have often been underestimated, with research focusing more on the teacher’s role in the process than on the learner’s experience.6 This highlights the need to explore how learners themselves experience feedback in medical training.
This study specifically explores the feedback reception experiences of paediatricians who completed their postgraduate training in Kuwait between 2015 and 2020. The research questions include: What were the experiences of receiving feedback among these residents? What were the key features of the feedback they received? How did these experiences influence their training and professional development? By answering these questions, the study provides insight into the current state of feedback practices in Kuwait and identifies areas for improvement.
My personal experience as a graduate of the Kuwait Institute for Medical Specialization (KIMS) pediatric postgraduate program in 2012 shaped my interest in this research. During my residency, feedback was often limited, poorly structured, or focused only on negatives. Verbal feedback was rare, and in many cases, supervisors simply filled out evaluation forms without discussing the results. When feedback was provided, it was often untimely, judgmental, and without an action plan.7 These shortcomings may have been due to underdeveloped faculty training in feedback skills at the time.8 The lack of effective feedback affected my learning, as mistakes were left uncorrected and strong performance was not reinforced, leaving competence to develop largely through trial and error.9 Reflecting on this experience raised important questions: Has feedback practice changed in recent years? Have new workshops and “train the trainer” programs improved feedback delivery? Are current residents still experiencing the same challenges?
KIMS is the national body responsible for postgraduate residency training, operating independently from the hospital where clinical work takes place. The KIMS pediatric residency program is the only postgraduate pediatric training pathway in Kuwait. It spans five years and includes rotations across all major government hospitals and subspecialties.10 Feedback is expected from tutors, site coordinators, and program directors, both verbally and in writing. However, the quality and consistency of this feedback remain unclear, underscoring the importance of residents’ perspectives in evaluating current practices.
My position within this study required ongoing reflexivity. Although I did not hold a formal administrative or evaluative role within KIMS, I worked closely with residents in my capacity as a pediatric consultant within the same clinical environment. This proximity provided familiarity with the training context while maintaining some separation from institutional assessment structures, reflecting elements of both insider and outsider positioning described in qualitative research methodology.11 Throughout the study, I remained attentive to the potential influence of my professional role on data collection and interpretation and took deliberate steps to maintain reflexivity, ethical integrity, and appropriate professional boundaries.
In summary, feedback is a powerful but complex part of medical education. Its effectiveness depends not only on how it is delivered but also on how learners experience it. This study seeks to explore pediatric residents’ experiences receiving feedback in Kuwait, using their perspectives to better understand the strengths and challenges of current practices. The findings may inform improvements in feedback delivery and enhance medical education in Kuwait.
Literature Review
The overarching research question of this study is: What are the feedback reception experiences among paediatricians who completed their postgraduate training in Kuwait between 2015 and 2020? To address this question and identify the knowledge gap, a literature review was conducted focusing on the definition and importance of feedback, feedback models, principles of effective feedback, challenges, the role of psychological safety, and the influence of role models.
Search Strategy
The review followed the approach described by Grant and Booth.12 Searches were conducted in PubMed using the keywords medical education and feedback, initially yielding over 16,000 articles. Narrowing the search with the terms postgraduate and Kuwait reduced the results to only two relevant studies, neither of which directly addressed feedback reception. Additional searches using “medical education,” “feedback,” and “Kuwait” produced ten articles, none directly exploring feedback experiences (both qualitative and quantitative). This confirms a lack of published work on the perspectives of Kuwaiti postgraduate residents. Articles in English, published within the last five years (with exceptions for seminal works), were screened and appraised using the CASP checklists to ensure quality.13
Definitions and Importance of Feedback
Definitions of feedback vary across the literature. Ramaprasad described it as information that identifies a gap between actual and desired performance,14 while Ende defined it as information on students’ performance intended to guide improvement.9 More recent perspectives place emphasis on learners, framing feedback as a process through which learners interpret information and use it to enhance performance.15 In medical education, feedback is especially important for skill development, reflection, and professional growth.1,5 Its role is evident in competency-based education, where feedback is central to learner progress.16
Models of Feedback
Several models have been proposed to guide effective feedback. Classical approaches include the “sandwich” method,17 SET-GO,18 Pendleton’s rules,19 and ALOBA.20 While widely used, these models are often criticized for being unidirectional or overly prescriptive. More recent frameworks, such as SPIKES21 and R2C2,22 emphasize learner engagement, dialogue, and coaching. These approaches better align with modern educational principles but require more time and training to implement effectively.
Principles, Challenges, and Psychological Safety
Effective feedback should be specific, timely, based on direct observation, and focused on behaviours rather than personal traits.9,23 It should also be dialogic, enabling learners to self-assess and co-create action plans.24 Despite this, challenges remain. Feedback is often hindered by time pressures, hierarchical structures, lack of privacy, and insufficient faculty training.8,25 Learners may also perceive feedback negatively if delivered harshly, reducing motivation and engagement.23 Psychological safety is essential, as learners must feel secure to admit gaps, ask questions, and respond openly to feedback.26,27
Role Models and Feedback Culture
Feedback is most effective in a positive learning environment where supervisors act as professional role models. Tutors who demonstrate desirable clinical and interpersonal behaviors influence not only learners’ skills but also their attitudes toward receiving and giving feedback.28,29 Establishing a feedback culture with a growth mindset encourages learners to actively seek feedback and use it for professional development.30
In summary, the literature highlights the central role of feedback in postgraduate medical education, its evolving definitions, and the variety of models and principles designed to improve practice. However, significant challenges persist, particularly in contexts where hierarchy and workload pressures limit the effectiveness of feedback. Importantly, there is a clear gap in research on experiences of receiving feedback in Kuwait. This study addresses this gap by exploring the perspectives of pediatricians who trained in Kuwait, aiming to generate insights that can inform improvements in feedback practices within the region.
This study aimed to explore experiences with feedback among pediatricians who completed or were still enrolled in postgraduate training in Kuwait between 2015 and 2020. A qualitative research design was chosen, as it is best suited to exploring personal experiences in depth and allows participants to describe their perspectives in their own words.31
Research Paradigm
The study was conducted within a constructivist paradigm, which assumes that reality is subjective and shaped by individual experiences.32 This paradigm was considered appropriate because experiences of feedback are socially and individually interpreted rather than objectively experienced in a uniform way. Constructivism also recognizes the existence of multiple perspectives and the co-construction of meaning between researcher and participants.33
Methodological Orientation
Within this constructivist framework, an interpretive (hermeneutic) phenomenological orientation was adopted to explore and interpret participants’ lived experiences of feedback during postgraduate training.34,35 This approach supported in-depth exploration of how participants understood, interpreted, and attached meaning to their feedback experiences within their clinical and educational contexts.
Study Design and Participants
Qualitative research was selected because it focuses on language, meaning, and context rather than numerical data.36 Semi-structured interviews allowed participants to reflect on their experiences and provided opportunities for clarification and elaboration. The study population included residents who completed or were still studying in the pediatric postgraduate program between 2015 and 2020. Inclusion criteria covered male and female residents in years three to five of their residency training. Exclusion criteria included pediatricians trained outside Kuwait, those who had completed training before 2015, junior residents (years one and two), and residents during 2021–2022, when the COVID-19 pandemic disrupted training.
A total of eleven pediatric residents (nine female, two male) were interviewed, along with three supervisors (a program director, a site coordinator, and a tutor). Participants were recruited based on availability and willingness to participate. Although random stratified sampling was initially planned, practical constraints, such as the small population size, necessitated a more pragmatic approach.
Data Collection
Interviews were conducted face-to-face where possible, with three held online due to hospital locations. One small group interview was conducted with three participants. Semi-structured, open-ended questions explored perceptions of effective feedback, frequency of feedback, and the individuals usually responsible for delivering it (Table 1). All interviews were conducted by the main researcher. Data collection was conducted between July 2022 and September 2022. Most interviews were conducted face-to-face, while three interviews were conducted online because participants were working in different hospitals and remote locations. With consent, interviews were audio-recorded, manually transcribed, and anonymized (Appendix A). One participant declined to be recorded and was excluded. Transcripts were validated through member checking, giving participants an opportunity to review their responses.37
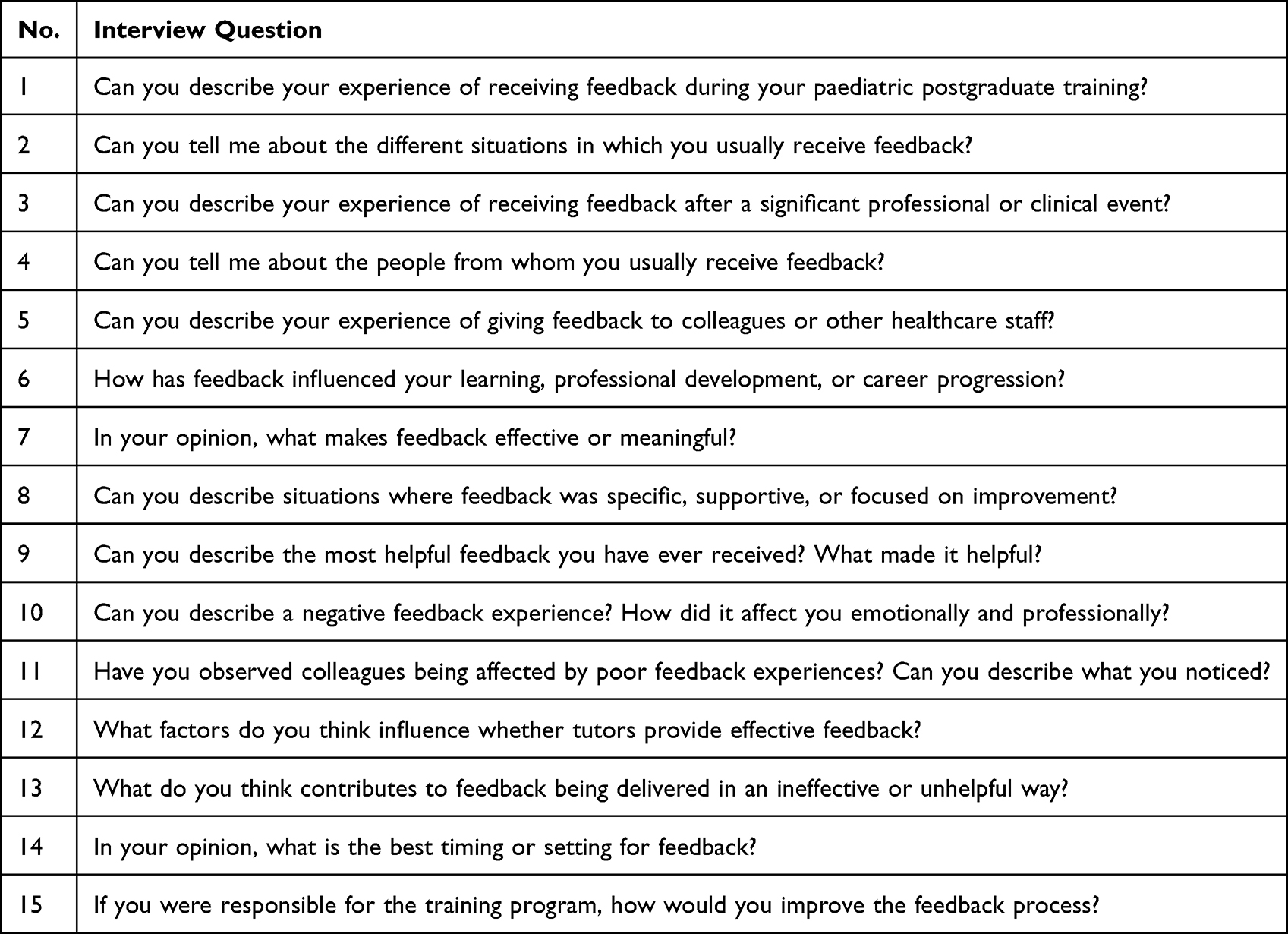 |
Table 1 Semi-Structured Interview Guide |
Data Analysis
An inductive thematic analysis approach was used.38 This involved familiarizing oneself with the transcripts, generating initial codes, grouping codes into themes, reviewing and refining these themes, and producing the final report. No predetermined coding framework was applied; several themes were identified and developed during the analytic process.
Ethics
This study was conducted in accordance with the principles of the World Medical Association Declaration of Helsinki. Ethical approval was obtained from the University of Dundee (SMED REC Number 22/23) and the Kuwait Ministry of Health (Research number 1390/2020). The study formed part of a master’s degree at the University of Dundee, under the supervision of two academic supervisors who provided methodological and academic oversight throughout the research process. The principal investigator was based in Kuwait and conducted the study within the clinical training environment in which the participants were undertaking residency training. Written informed consent was obtained from all participants, who were informed of their right to withdraw at any time. To ensure confidentiality, data were stored in password-protected files and identifying information was removed.
Rigour
Trustworthiness was ensured by applying the four criteria of Lincoln and Guba.39 Credibility was supported through member checking and peer review of transcripts. Data triangulation was achieved by including perspectives from both pediatric residents and clinical supervisors, allowing comparison of experiences and perceptions across different roles within the postgraduate training program. Dependability was enhanced by keeping detailed records of the data collection process. Confirmability was addressed by presenting participants’ quotes to ensure findings reflected their views rather than the researcher’s. Transferability was supported by providing contextual detail to allow readers to assess applicability to other settings.
Overall, this qualitative study, grounded in constructivist principles, used semi-structured interviews and thematic analysis to explore paediatric residents’ experiences of feedback in Kuwait. Ethical safeguards and strategies for rigour strengthened the study, ensuring credible and meaningful insights into the feedback process.
Results/Findings
This study explored the experiences of receiving feedback among paediatricians who completed their postgraduate training in Kuwait between 2015 and 2020. Eleven residents (nine female, two male) and three supervisors (a programme director, a site coordinator, and a tutor) were interviewed. Thematic analysis produced five major themes: factors influencing feedback experiences, consequences of receiving feedback, learning to give feedback, features of feedback, and challenges in the feedback process (Table 2).
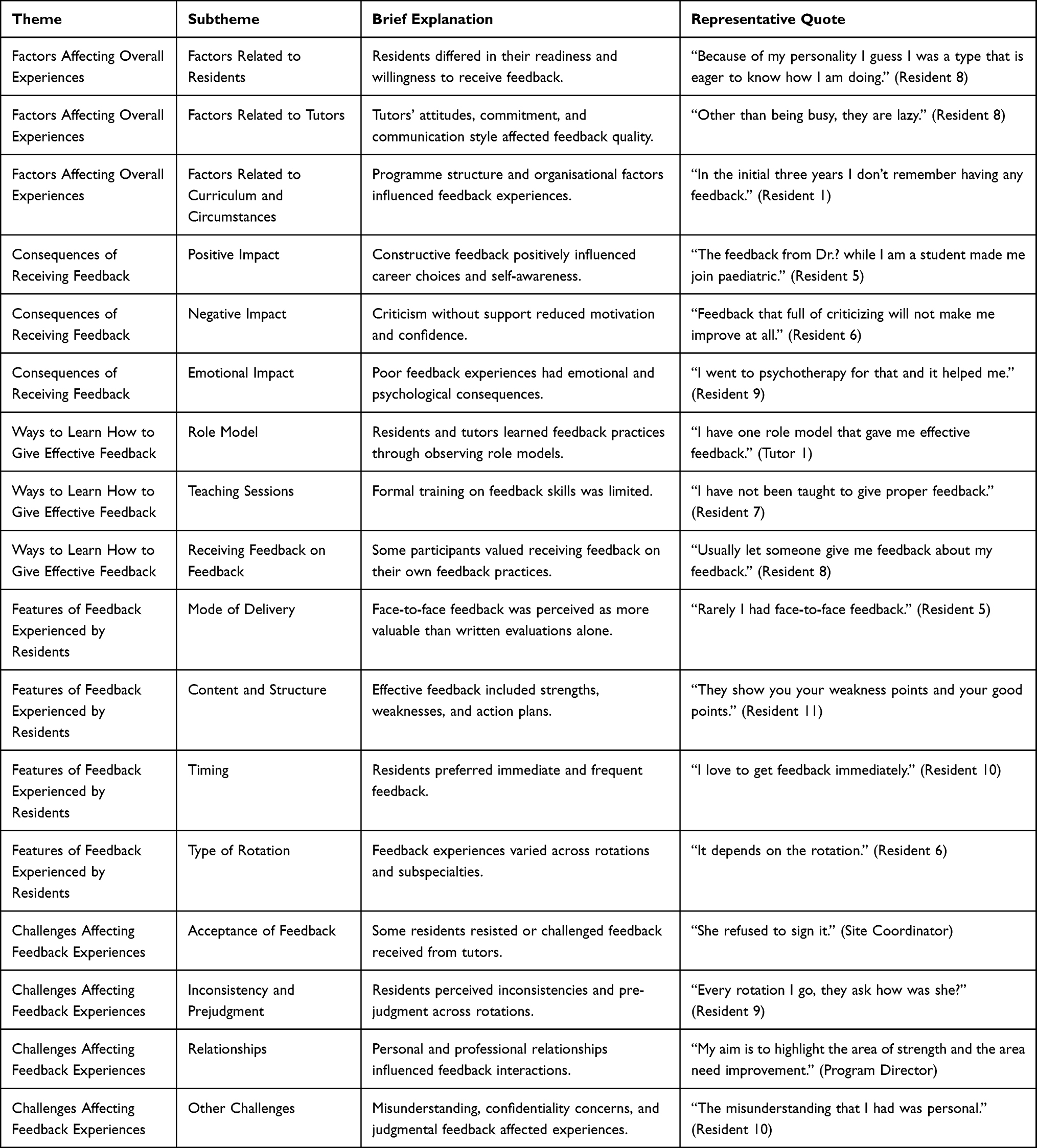 |
Table 2 Summary of Themes, Subthemes, and Representative Quotes |
Factors Affecting Feedback Experiences
Feedback experiences were shaped by resident, tutor, and curriculum-related factors. Some residents described actively seeking feedback to understand their strengths and weaknesses, while others avoided it, feeling overconfident or defensive. Tutors’ approaches also varied; some were described as careful and punctual, while others were perceived as too busy in providing feedback. Curriculum structure, scheduling, and changes in programme leadership also influenced opportunities for feedback, with residents reporting inconsistent experiences across rotations.
Consequences of Receiving Feedback
Feedback had both positive and negative impacts. Positive feedback built confidence, guided career decisions, and served as a “mirror” for self-reflection. Negative or overly critical feedback was described as demotivating and, in some cases, emotionally damaging. One resident reported seeking psychotherapy after repeated judgmental comments, while others described anger, frustration, or avoidance of supervisors.
Learning to Give Feedback
Residents’ experiences influenced how they planned to provide feedback in future. Many highlighted the importance of role models, though most struggled to recall supervisors who consistently gave effective feedback. Both residents and tutors acknowledged a lack of formal training in feedback skills. Some described the value of receiving feedback on how they themselves gave feedback, emphasizing the need for reciprocal and reflective practice.
Features of Feedback
Residents described variation in the mode, timing, and content of feedback. Written evaluations were often viewed as unhelpful compared to face-to-face discussions. Feedback that included both strengths and weaknesses, supported by clear action plans, was valued most. Timely, on-the-spot feedback was preferred, but many residents reported infrequent or delayed sessions, sometimes limited to end-of-rotation reports. The quality of feedback also varied between rotations, with some subspecialty supervisors providing structured, individualized feedback, while others gave little or none.
Challenges in Feedback
Residents and tutors described multiple barriers to effective feedback. Some residents resisted negative evaluations, while others felt unable to challenge unfair comments. Inconsistency between supervisors’ evaluations created confusion, and pre-judgment based on reputation sometimes followed residents between rotations. Relationships also influenced experiences, with personal connections both helping and hindering the process. Concerns were raised about confidentiality, with some residents reporting that mistakes were shared widely without their knowledge. Others highlighted problems with vague, judgmental feedback not based on observed performance.
In summary, the findings demonstrate that paediatric residents in Kuwait experienced feedback as highly variable. While constructive feedback supported growth and motivation, negative or inconsistent feedback caused frustration, emotional distress, and distrust. Residents valued feedback that was timely, specific, and balanced, but they also highlighted structural and cultural barriers that limited its effectiveness. These findings suggest the need for faculty development, structured feedback practices, and systems that ensure fairness and confidentiality in postgraduate medical education.
Discussion
This qualitative study explored how pediatric residents in Kuwait experienced and responded to feedback during postgraduate clinical training. Through inductive thematic analysis, five interconnected themes were constructed: limited face-to-face feedback, variable quality of feedback, challenges related to psychological safety and feedback acceptance, limited tutor preparation, and inconsistency in feedback practices. Together, these themes illustrate that feedback was often experienced not as an ongoing educational dialogue but as an inconsistent and emotionally charged process shaped by institutional culture, interpersonal relationships, and structural constraints.
One of the most significant findings was the perceived avoidance of direct verbal feedback. Many residents described feedback encounters as dominated by written evaluations completed primarily for administrative purposes rather than for meaningful learning. Although written assessments are necessary within competency-based training systems, participants perceived them as insufficient because they lacked dialogue, clarification, and opportunities for reflection. This finding aligns with previous literature showing that written feedback alone is often less educationally effective than interactive verbal exchanges.6 Residents described how time pressures, limited observation opportunities, and tutors’ discomfort with feedback conversations contributed to the reduction of meaningful verbal engagement.25,40,41 The findings, therefore, suggest that feedback within this setting may function more as an institutional requirement than as a formative learning process. This distinction is important because the absence of meaningful feedback may negatively affect not only professional development but also clinical performance and patient care.21,42
The findings also demonstrated that the quality of feedback strongly influenced how residents interpreted and emotionally responded to feedback encounters. Residents frequently described receiving vague comments such as “good job” or “needs improvement” without specific explanation or actionable guidance. Such comments were perceived as having limited educational value because they failed to identify learning gaps or provide direction for improvement. Previous studies have shown that effective feedback should be specific, actionable, timely, and linked to observable performance.43,44 In contrast, some residents in this study recalled feedback experiences that felt judgmental, overly personal, or humiliating. These encounters often resulted in reduced confidence, emotional distress, and disengagement from future feedback interactions. Importantly, participants noted that unconstructive feedback practices were not limited to tutors trained locally, suggesting that feedback quality may be shaped less by geographic training background and more by workplace culture and educational norms. This highlights the importance of examining how institutional environments influence feedback behaviors and expectations.
Psychological safety emerged as a central issue influencing residents’ willingness to engage with feedback. Many participants described feedback interactions as emotionally unsafe, particularly when feedback was delivered publicly, focused exclusively on weaknesses, or communicated in a punitive tone. Within psychologically unsafe environments, residents reported becoming defensive, anxious, or reluctant to seek clarification. Current medical education literature emphasizes that effective feedback depends on supportive learner-centred environments characterized by trust, respect, and dialogue.8,27,30 The present findings suggest that when these conditions are absent, feedback may lose its developmental value and instead become associated with fear and avoidance. This finding may also be understood through Maslow’s framework, which suggests that individuals who feel psychologically threatened may struggle to engage fully in learning and self-improvement processes.45 Thus, emotional safety appears to be not simply a desirable characteristic of feedback, but a necessary condition for meaningful educational engagement.
Another important finding was the complexity of feedback acceptance. The study demonstrated that resistance to feedback was not solely a learner-related issue but reflected a relational and cultural process involving both residents and tutors. Some residents acknowledged reacting defensively to criticism, particularly when feedback was delivered harshly or perceived as unfair. At the same time, some tutors reportedly avoided giving honest feedback because they feared conflict, damaging relationships, or causing emotional discomfort.23,46 This mutual discomfort appeared to contribute to superficial or diluted feedback exchanges. Structured feedback approaches such as Pendleton’s rules and the ALOBA model have been proposed to reduce defensiveness and promote collaborative dialogue.20,41,47 However, few participants described experiencing feedback delivered through structured educational frameworks. This may indicate limited faculty preparation in educational communication skills and feedback methodologies.
The study further highlighted the limited pedagogical preparation of clinical tutors. While participants generally respected tutors’ clinical expertise, many believed that tutors lacked formal training in educational methods, feedback delivery, and learner support. Previous literature similarly notes that clinicians are often expected to teach without receiving structured preparation for educational roles.42 Residents in this study valued tutors who delivered feedback respectfully, observed performance directly, and engaged in constructive dialogue. This finding reinforces the need for faculty development initiatives focused not only on feedback techniques but also on communication, emotional intelligence, and learner-centered educational practices. Structured faculty development programs using models such as SPIKES, R2C2, and coaching-based feedback approaches may help strengthen feedback quality and consistency.6,21,48,49 Importantly, participants also highlighted that tutors themselves rarely received feedback regarding their teaching performance, suggesting a broader institutional gap in educational quality improvement.
Collectively, the findings reveal a mismatch between the intended goals of competency-based medical education and residents’ lived experiences of feedback within clinical training environments. Although competency-based systems emphasize continuous formative feedback and learner development, participants frequently described feedback as inconsistent, emotionally difficult, and heavily dependent on individual tutor practices. Consistent with previous studies, negative feedback experiences were often remembered more vividly than positive ones.6 Nevertheless, residents clearly valued feedback that was respectful, balanced, specific, and delivered within supportive relationships, reflecting principles widely recognized in contemporary medical education literature.50
This study has several limitations. Data collection occurred during the COVID-19 pandemic, which limited opportunities for in-person interactions and restricted the use of focus groups. The study was also limited to paediatric training experiences within Kuwait, which may affect transferability to other specialties or healthcare contexts. In addition, as one of the first qualitative studies exploring residents’ feedback experiences in this setting, the research process required ongoing development of expertise in qualitative interviewing and reflexive thematic analysis. However, reflexive engagement, continuous supervision, and iterative analysis were used to strengthen methodological rigor throughout the study.
Despite these limitations, the study contributes important insights into the emotional, cognitive, and behavioural dimensions of feedback experiences within postgraduate medical training. The findings suggest that improving feedback practices requires more than introducing assessment tools or formal requirements. Attention must also be directed toward institutional culture, faculty development, psychological safety, and the relational aspects of educational interactions.
Conclusion
This study explored the feedback reception experiences of paediatricians in Kuwait who completed their postgraduate residency training at the Kuwait Institute of Medical Specialization (KIMS). Using qualitative semi-structured interviews, five major themes were identified: factors influencing feedback experiences, consequences of feedback, feedback features, challenges affecting feedback, and effective approaches to giving feedback. Overall, the findings suggest that feedback practices within paediatric residency training remain insufficiently developed. Residents frequently described feedback as inconsistent, overly focused on weaknesses, lacking actionable guidance, and at times judgmental or personal, with negative effects on confidence and professional development. In contrast, constructive and balanced feedback was perceived as highly valuable and influential in shaping clinical growth and career development.
This study contributes important learner-perspective evidence to the limited literature on feedback culture in postgraduate medical education in Kuwait. The findings highlight the need for structured faculty development, improved tutor training, and psychologically safe environments for feedback that promote respectful dialogue and learner-centered supervision. Incorporating structured feedback approaches, such as the R2C2 model, and expanding professional development opportunities for supervisors may help strengthen feedback quality and educational effectiveness within residency training. The dissemination of these findings through KIMS “training the trainers” workshops further supports their practical relevance and potential contribution to educational reform. Future research should explore feedback experiences across different specialties, institutions, and educational systems, while also examining faculty perspectives and the organizational barriers that influence effective feedback practices.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request, subject to ethical and confidentiality considerations.
Ethical Approval
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Centre for Medical Education, University of Dundee (SMED REC Number 22/23) and from the Kuwait Ministry of Health Research Committee (Research Number 1390/2020). Written informed consent was obtained from all participants.
Acknowledgments
This study was conducted as part of the requirements for a Master’s degree at the University of Dundee, United Kingdom.
Author Contributions
Abrar Alabdulghafour contributed to the study conception, data collection, data analysis, and manuscript drafting. Rania AlKhadragy contributed to supervision, draft feedback, and critical revision of the manuscript. Gillian Marion Scanlan contributed to supervision and methodological guidance. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts interest in relation to this work.
References
1. Hounsell D. Essay-writing and the quality of feedback. In: Student Learning: Research in Education and Cognitive Psychology. The Society for Research into Higher Education & Open University Press; 1987:109–11.
2. Hattie J, Timperley H. The power of feedback. Rev Educ Res. 2007;77(1):81–112. doi:10.3102/003465430298487
3. Henderson M, Ajjawi R, Boud D, Molloy E. Identifying feedback that has impact. In: The Impact of Feedback in Higher Education. Springer International Publishing; 2019:15–34.
4. McKimm J. Giving effective feedback. Br J Hosp Med. 2009;70(3):158–161. doi:10.12968/hmed.2009.70.3.40570
5. Lloyd M, Watmough S, O’Brien S, Furlong N, Hardy K. How to give and receive constructive feedback. Pharm J. 2016;296(7887):296.
6. Urquhart LM, Rees CE, Ker JS. Making sense of feedback experiences: a multi-school study of medical students’ narratives. Med Educ. 2014;48(2):189–203. doi:10.1111/medu.12304
7. Weallans J, Roberts C, Hamilton S, Parker S. Guidance for providing effective feedback in clinical supervision in postgraduate medical education: a systematic review. Postgrad Med J. 2022;98(1156):138–149. doi:10.1136/postgradmedj-2020-139566
8. Bing-You RG, Trowbridge RL. Why medical educators may be failing at feedback. JAMA. 2009;302(12):1330–1331. doi:10.1001/jama.2009.1393
9. Ende J. Feedback in clinical medical education. JAMA. 1983;250(6):777–781. doi:10.1001/jama.1983.03340060055026
10. Kuwait Institution for Medical Specialization. Pediatric residency training program. Manual. 2018.
11. Unluer S. Being an insider researcher while conducting case study research. Qual Rep. 2012;17(29):1–14.
12. Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Info Libr J. 2009;26(2):91–108. doi:10.1111/j.1471-1842.2009.00848.x
13. Singh J. Critical appraisal skills programme. J Pharmacol Pharmacother. 2013;4(1):76. doi:10.4103/0976-500X.107697
14. Ramaprasad A. On the definition of feedback. Behav Sci. 1983;28(1):4–13. doi:10.1002/bs.3830280103
15. Carless D, Boud D. The development of student feedback literacy: enabling uptake of feedback. Assess Eval High Educ. 2018;43(8):1315–1325. doi:10.1080/02602938.2018.1463354
16. Kelly E, Richards JB. Medical education: giving feedback to doctors in training. BMJ. 2019;366:l4840.
17. Dohrenwend A. Serving up the feedback sandwich. Fam Pract Manag. 2002;9(10):43.
18. Silverman J. The Calgary-Cambridge approach to communication skills teaching II: the SET-GO method of descriptive feedback. Educ Gen Pract. 1997;8(1):16–23.
19. Pendleton D, Schofield T, Tate P, Havelock P. The Consultation: An Approach to Learning and Teaching. Oxford University Press; 1984.
20. Chowdhury RR, Kalu G. Learning to give feedback in medical education. Obstet Gynaecol. 2004;6(4):243–247. doi:10.1576/toag.6.4.243.27023
21. Kistler EA, Chiappa V, Chang Y, Baggett M. Evaluating the SPIKES model for improving peer-to-peer feedback among internal medicine residents: a randomized controlled trial. J Gen Intern Med. 2021;36(11):3410–3416. doi:10.1007/s11606-020-06459-w
22. Sargeant J, Mann K, Manos S, et al. R2C2 in action: testing an evidence-based model to facilitate feedback and coaching in residency. J Grad Med Educ. 2017;9(2):165–170. doi:10.4300/JGME-D-16-00398.1
23. Hernandez MR, Wang JT. Feedback in medical education is a journey; pack more than a sandwich. Med Educ. 2021.
24. Shrivastava SR, Shrivastava PS. Strengthening the delivery of feedback in medical institutions by establishing feedback culture. Med J Babylon. 2022;19(2):304. doi:10.4103/MJBL.MJBL_25_22
25. Spencer J. Learning and teaching in the clinical environment. BMJ. 2003;326(7389):591–594. doi:10.1136/bmj.326.7389.591
26. Tsuei SH, Lee D, Ho C, Regehr G, Nimmon L. Exploring the construct of psychological safety in medical education. Acad Med. 2019;94(11 suppl):S28–S35. doi:10.1097/ACM.0000000000002897
27. Johnson CE, Keating JL, Molloy EK. Psychological safety in feedback: what does it look like and how can educators work with learners to foster it? Med Educ. 2020;54(6):559–570. doi:10.1111/medu.14154
28. Sternszus R, Macdonald ME, Steinert Y. Resident role modeling: “it just happens. Acad Med. 2016;91(3):427–432. doi:10.1097/ACM.0000000000000996
29. Khan AH, Yasmeen R, Awan WS, Niazi SNK, Malik U. Role modeling in medical education and its influences on professional behaviours. Ann King Edward Med Univ. 2020;26(1):83–87.
30. Ramani S, Könings KD, Ginsburg S, van der Vleuten CP. Twelve tips to promote a feedback culture with a growth mind-set: swinging the feedback pendulum from recipes to relationships. Med Teach. 2019;41(6):625–631. doi:10.1080/0142159X.2018.1432850
31. Cleland JA. Exploring versus measuring: considering the fundamental differences between qualitative and quantitative research. In: Cleland JA, Durning SJ editors. Researching Medical Education. John Wiley & Sons; 2015:1–14. doi:10.1002/9781118838983.ch1
32. Bunniss S, Kelly DR. Research paradigms in medical education research. Med Educ. 2010;44(4):358–366. doi:10.1111/j.1365-2923.2009.03611.x
33. Creswell JW, Poth CN. Qualitative Inquiry and Research Design: Choosing Among Five Approaches. Sage Publications; 2016.
34. Starks H, Brown Trinidad S. Choose your method: a comparison of phenomenology, discourse analysis, and grounded theory. Qual Health Res. 2007;17(10):1372–1380. doi:10.1177/1049732307307031
35. Morse JM. Determining sample size. Qual Health Res. 2000;10(1):3–5. doi:10.1177/104973200129118183
36. Schutt RK. Investigating the Social World: The Process and Practice of Research. Sage Publications; 2018.
37. Burnard P, Gill P, Stewart K, Treasure E, Chadwick B. Analysing and presenting qualitative data. Br Dent J. 2008;204(8):429–432. doi:10.1038/sj.bdj.2008.292
38. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
39. Lincoln YS, Guba EG. Naturalistic Inquiry. Sage Publications; 1985.
40. Burgess A, Mellis C. Feedback and assessment for clinical placements: achieving the right balance. Adv Med Educ Pract. 2015;6:373–381. doi:10.2147/AMEP.S77890
41. Tuma F, Nassar AK. Feedback in medical education. In: StatPearls. StatPearls Publishing; 2023.
42. Ramani S, Leinster S. AMEE Guide No. 34: teaching in the clinical environment. Med Teach. 2008;30(4):347–364. doi:10.1080/01421590802061613
43. Archer JC. State of the science in health professional education: effective feedback. Med Educ. 2010;44(1):101–108. doi:10.1111/j.1365-2923.2009.03546.x
44. de Ridder JM V, McGaghie WC, Stokking KM, ten Cate OT. Variables that affect the process and outcome of feedback, relevant for medical training: a meta-review. Med Educ. 2015;49(7):658–673. doi:10.1111/medu.12744
45. Milheim KL. Towards a better experience: examining student needs in the online classroom through Maslow’s hierarchy of needs model. J Online Learn Teach. 2012;8(2):159.
46. Brown N, Cooke L. Giving effective feedback to psychiatric trainees. Adv Psychiatr Treat. 2009;15(2):123–128. doi:10.1192/apt.bp.106.003293
47. Silverman JD, Kurtz SM, Draper J. The Calgary-Cambridge approach to communication skills teaching I: agenda-led, outcome-based analysis of the consultation. Educ Gen Pract. 1996;4:288–299.
48. Lockyer J, Armson H, Könings KD, et al. In-the-moment feedback and coaching: improving R2C2 for a new context. J Grad Med Educ. 2020;12(1):27–35. doi:10.4300/JGME-D-19-00508.1
49. Atkinson A, Watling CJ, Brand PL. Feedback and coaching. Eur J Pediatr. 2021;180:1–6. doi:10.1007/s00431-020-03737-x
50. Wilbur K, BenSmail N, Ahkter S. Student feedback experiences in a cross-border medical education curriculum. Int J Med Educ. 2019;10:98–105. doi:10.5116/ijme.5ce1.149f
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.