")
Back to Journals » Journal of Pain Research » Volume 16
The Relationship of Postoperative Pain and Opioid Consumption to Postoperative Delirium After Spine Surgery
Authors Sica R , Wilson JM, Kim EJ, Culley DJ, Meints SM, Schreiber KL
Received 2 July 2022
Accepted for publication 22 January 2023
Published 28 January 2023 Volume 2023:16 Pages 287—294
DOI https://doi.org/10.2147/JPR.S380616
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Erica Wegrzyn
Ryan Sica,1 Jenna M Wilson,1 Erin J Kim,1 Deborah J Culley,1,2 Samantha M Meints,1 Kristin L Schreiber1
1Department of Anesthesiology, Perioperative, and Pain Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA; 2Department of Anesthesiology and Critical Care, University of Pennsylvania, Philadelphia, PA, USA
Correspondence: Ryan Sica, Brigham and Women’s Hospital, 75 Francis Street, Boston, MA, 02115, USA, Tel +1 617 732-8210, Email [email protected]
Purpose: To examine the relationship between postoperative pain and opioid use and the development of postoperative delirium (POD), with attention to the preoperative opioid use status of patients.
Methods: This was a secondary analysis of data from a prospective observational study of patients (N = 219; ≥ 70 years old) scheduled to undergo elective spine surgery. Maximal daily pain scores (0– 10) and postoperative morphine milligram equivalents per hour (MME/hr) were determined for postoperative days 1– 3 (D1-3). POD was assessed by daily in-person interviews using the Confusion Assessment Method and chart review.
Results: Patients who reported regular preoperative opioid use (n = 58, 27%) reported significantly greater maximal daily pain scores, despite also requiring greater daily opioids (MME/hr) in the first 3 days after surgery. These patients were also more likely to develop POD. Interestingly, while postoperative pain scores were significantly higher in patients who developed POD, postoperative opioid consumption was not significantly higher in this group.
Conclusion: POD was associated with greater postoperative pain, but not with postoperative opioid consumption. While postoperative opioid consumption is often blamed for delirium, these findings suggest that uncontrolled pain may actually be a more important factor, particularly among patients who are opioid tolerant. These findings underscore the importance of employing multimodal perioperative analgesic management, especially among older patients who have a predilection to developing POD and baseline tolerance to opioids.
Keywords: postoperative delirium, pain, opioids, spine surgery, postoperative pain
Introduction
Postoperative delirium (POD) is linked with cognitive and noncognitive morbidity and mortality, with reported incidence ranging from 5% to 52% depending on the definition and sample studied.1 In the acute setting, POD increases total hospital length of stay3 and is associated with more persistent complications including postoperative neurocognitive decline, loss of independence, and increased mortality.4–9 The most notable patient-related risk factor for POD is increasing age,1 with POD occurring most commonly in patients over 65, a group which undergoes more than 33% of all surgical procedures.2 Therefore, it is particularly important to study older adult patients to inform efforts to prevent the development of POD among this at-risk group.
Given the importance of POD, previous work has investigated risk factors, including older age, higher BMI, preexisting co-morbidities or dementia, impaired preoperative cognitive status, depression, and higher American Society of Anesthesiologists physical status classification.4,10–12 Additionally, some studies have shown an association between postoperative pain and the development of POD, even among patients classified as low risk for the development of delirium based on their preoperative characteristics.13–15 This association may be of importance, as postoperative pain is potentially modifiable, in contrast to other risk factors, such as age.4,16–18 Acute postoperative pain is also accompanied by negative patient-related consequences, including lower quality of life, impaired functional status, increased recovery time, and higher healthcare costs,19–21 making better postoperative pain control an important goal.
Spine surgery is associated with significant postoperative pain.22,23 In addition, even before surgery, many patients suffer from back pain and management of this pain with opioids remains a relatively common practice. While some studies have shown a significant association between opioid use and delirium postoperatively,24 multiple other studies have not observed this association.13,25,26 Importantly, patients taking opioids preoperatively typically receive higher opioid doses in the postoperative period, but despite this, still experience severe postoperative pain. The reasons for this may be multifaceted and can include opioid tolerance or potentially opioid-induced hyperalgesia, which is defined as a paradoxical nociceptive response to certain stimuli from opioid analgesics resulting in ineffective pain control.27,28 Thus, an important question that arises is whether it is the uncontrolled postoperative pain or the increased postoperative opioid use that contributes more importantly to POD, especially in patient who are taking opioids preoperatively.
An association between preoperative opioid use and POD had previously been observed in this cohort,11 but at that time no information about postoperative pain and postoperative opioid consumption in these individuals had been collected. For the current study, we therefore extracted data regarding postoperative pain scores and opioid utilization in these patients. Using these data, we investigated the associations between preoperative opioid use with postoperative pain and postoperative opioid consumption, as well as the associations of POD with postoperative pain and postoperative opioid consumption. We hypothesized that patients using preoperative opioids would experience greater postoperative pain and require higher doses of postoperative opioids. Furthermore, we hypothesized that patients who developed POD would also experience greater postoperative pain and report higher doses of postoperative opioids.
Materials and Methods
This is a secondary analysis of data from a prospective observational study approved by the Partners Human Research Committee/Institutional Review Board. The investigation of the relationship between preoperative frailty and postoperative delirium in this cohort has been previously reported by Susano et al.11 Additional data separate from that report was subsequently collected, including postoperative pain scores and postoperative opioid consumption for each patient, and the analysis of these data in this cohort form the substance of the current report.
Participants and Procedure
Patients scheduled to undergo elective spine surgery between April 17, 2017 and October 9, 2018 at Brigham and Women’s Hospital (Boston, Massachusetts) were recruited. Inclusion criteria included ≥70 years old and expected admission postoperatively. Exclusion criteria included prior history of stroke or brain tumor, scheduled outpatient surgery, vision or hearing impairment resulting in inability to see or hear instructions, inability to draw and/or inability to speak, read, or understand English. All participants provided informed consent prior to participating.
Measures
Pain
Postoperative pain scores were recorded in the electronic medical record by the primary nursing staff. During each nursing assessment throughout the day, nursing staff asked each patient to rate their current pain score, using a numerical rating scale 0–10, typically before and after the administration of pain medication, but also during times of sleeping in which case a pain score of 0 was recorded. These pain scores were extracted for each 24-hour epoch according to calendar day (midnight-midnight), and recorded for that postoperative day (D1, D2, D3). A maximum pain score for each day was determined to assess the peak degree of uncontrolled pain for that time period, which was used for the primary analysis.
Opioid Consumption
Preoperative opioid use was assessed at the preoperative evaluation visit. All opioid analgesics administered intraoperatively and postoperatively via intravenous or oral routes (hydromorphone, hydrocodone, oxycodone, morphine, fentanyl, and tramadol) were extracted from the medication administration report in the electronic medical record for postoperative days 1–3. All postoperative opioid consumption was then converted to morphine milligram equivalents (MME) to allow for comparison. This was then normalized as MME per hour (MME/hr) to account for differing day lengths for the day of patient discharge.
Development of Delirium
Postoperative delirium (POD) was assessed as previously reported by Susano et al,11 including both in-person assessment and chart review. For the in-person assessment, a blinded investigator administered the Confusion Assessment Method to each patient on postoperative days 1–3, or until the patient was discharged if before day 3.29–31 Notably, POD is characterized by fluctuating or waxing and waning of consciousness or cognition, and thus, it can be missed if the assessment is administered during a waning period. Chart review assessment of physician and nursing notes was used in a complementary fashion because it captures all events during a day, although it may miss hypoactive POD. By utilizing both forms of assessment, a patient was considered to be delirious if they were positive for at least 1 postoperative day by either assessment.
Analytic Approach
We used Chi-Square, independent samples t-test, or Mann–Whitney U-test as appropriate to investigate differences in postoperative pain and opioid consumption between patient groups (patients with and without preoperative opioid use, patients who did and did not develop POD).
Results
Sample Characteristics
Patients ≥70 years scheduled for elective spine surgery were initially screened for eligibility at the preoperative evaluation clinic, with 229 enrolled, and 219 ultimately included in the study and analysis (Figure 1). Overall sample mean age was 76, with 57% males (n = 124) and 43% females (n = 95). Approximately 27% of patients reported taking opioids preoperatively (n = 58). One quarter (25%) of patients developed delirium during the first 3 postoperative days (n = 55). Full demographic and baseline characteristics are reported previously in Susano et al.11
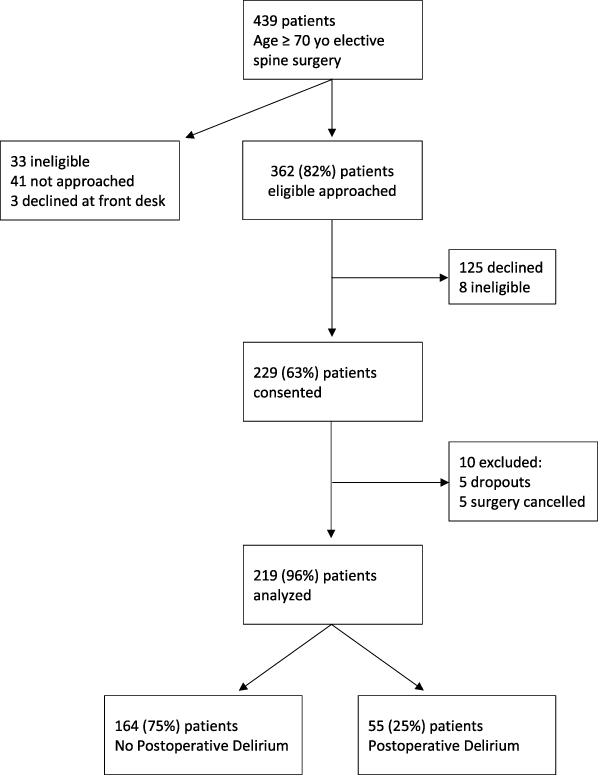 |
Figure 1 Study flow diagram. |
Associations of Preoperative Opioid Use with Postoperative Pain and Opioid Consumption
Given that preoperative opioid use is often associated with difficulty in managing postoperative pain, we examined differences in postoperative pain and postoperative opioid consumption between patients taking opioids preoperatively vs opioid naïve patients. Postoperative pain scores (range: 0–10) and opioid consumption (range: 0–15.5 MME/hr) varied widely among study participants (Figure 2). Patients taking opioids preoperatively had significantly higher daily maximum pain scores postoperatively across D1-3 (D1: 7.2 vs 6.1, p < 0.01; D2: 7.2 vs 5.8, p < 0.01; D3: 6.8 vs 5.6, p < 0.01; Figure 2A), despite the fact that these patients received about twice as much postoperative opioid analgesic (MME/hr on D1: 3.0 vs 1.5, p < 0.001; D2: 2.5 vs 1.3, p < 0.001; D3: 2.6 vs 1.3, p < 0.001; Figure 2B).
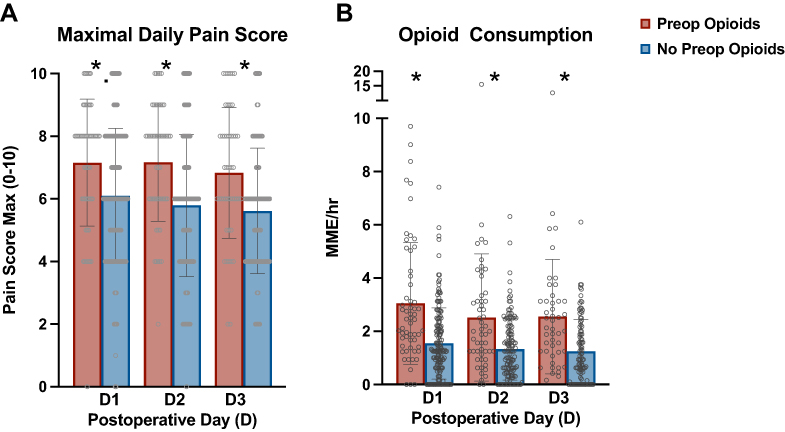 |
Figure 2 Differences in Postoperative Pain and Opioid Consumption based on Preoperative Opioid Use. Postoperative pain (A) and opioid consumption (B) in patients taking opioids preoperatively (red) versus those that were not (blue). Patients taking preoperative opioids reported significantly higher daily pain scores (A) (D1: 7.2 vs 6.1, p<0.01; D2: 7.2 vs 5.8, p<0.01; D3: 6.8 vs 5.6, p<0.01) and received significantly more postoperative opioids (B) (MME/hr on D1: 3.0 vs 1.5, p<0.001; D2: 2.5 vs 1.3, p<0.001; D3: 2.6 vs 1.3, p<0.001). Statistical analysis included independent samples t-test for (A) and Mann–Whitney U for (B). *A significant difference between those taking preoperative opioids versus those not taking preoperative opioids. |
Associations of Postoperative Delirium with Postoperative Pain and Opioid Consumption
Maximal postoperative pain scores and postoperative opioid consumption were compared between those who developed POD and those who did not develop POD. Significantly higher maximum postoperative pain scores across D1-3 were observed in patients who developed POD compared to those who did not develop POD (D1: 7.1 vs 6.1, p < 0.01; D2: 6.8 vs 5.9, p = 0.02; D3: 6.6 vs 5.7, p = 0.01; Figure 3A). However, there was not a clinically significant difference in postoperative opioid consumption on any of the three days between patients who developed POD and those that did not develop POD (MME/hr on D1: 2.1 vs 2.2, p > 0.05; D2: 1.7 vs 1.7, p > 0.05; D3: 1.4 vs 1.8, p > 0.05; Figure 3B).
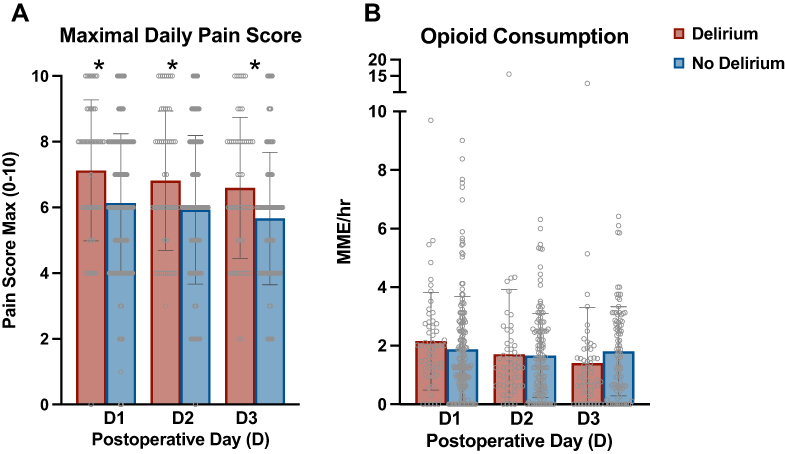 |
Figure 3 Differences in Postoperative Pain and Opioid Consumption among patients who did and did not develop Postoperative Delirium (POD). Postoperative pain (A) and postoperative opioid consumption (B) in patients that developed postoperative delirium (red) versus patients that did not (blue). Patients who developed POD had significantly higher daily pain scores compared with those who did not develop POD (A) (D1: 7.1 vs 6.1, p<0.01; D2: 6.8 vs 5.9, p=0.02; D3: 6.6 vs 5.7, p=0.01). However, there was not a significant difference in postoperative opioid consumption between the two groups (B) (MME/hr on D1: 2.1 vs 2.2, p>0.05; D2: 1.7 vs 1.7, p>0.05; D3: 1.4 vs 1.8, p>0.05). Statistical analysis included independent samples t-test for (A) and Mann–Whitney U for (B). *A significant difference between those who developed postoperative delirium versus those who did not. |
Discussion
Understanding the relationships between preoperative opioid use, postoperative pain and opioid consumption, and the development of postoperative delirium is a crucial insight that may inform efforts to prevent the development of POD. As previously reported in Susano et al,11 preoperative opioid use was associated with a greater likelihood of developing POD. We expanded upon these findings by showing that, interestingly, the development of POD was not associated with greater postoperative opioid consumption during the first 3 postoperative days. However, POD was consistently associated with higher daily maximal pain scores, suggesting that a lack of adequate pain control, rather than a superfluous of opioids, was more prominently related to POD in these patients.
Preoperative Opioid Use and Tolerance
Prior research has shown that patients chronically taking opioids have postoperative pain that is more difficult to manage, typically requiring higher opioid doses post-surgically.27 Our findings are in concurrence with this, in that we observed higher postoperative opioid consumption among patients who were taking opioids preoperatively. Other previous research suggests that patients who consume opioids preoperatively are at an increased risk to have uncontrolled postoperative pain,27 which is also in agreement with our findings that showed significantly higher postoperative pain scores among patients taking opioids preoperatively, despite these patients receiving greater opioids postoperatively. Taking opioids on a consistent basis may lead to opioid tolerance, or even have an element of opioid-induced hyperalgesia.28 In addition, being prescribed opioids to manage pain implies a greater level of pain sensitivity.
Opioid Use, Pain and Delirium
It seems plausible that greater opioid consumption would increase the risk of POD because of the sedative impact of opioids in the central nervous system, potentially inhibiting cognition and increasing disorientation. The association between opioid consumption and POD is variable among studies, however.12–15 As reported previously within this cohort, taking opioids preoperatively was itself associated with a significantly increased incidence of POD.11 Interestingly, however, postoperative opioid consumption was not in fact higher among those that developed POD. Alternatively, some previous studies have noted that postoperative pain itself may increase risk of POD,13–15 which is consistent with our findings. Patients who developed POD in the present study reported significantly higher maximal daily pain scores. Taken together, the association of pain with POD, and the lack of association of postoperative opioid consumption with POD, suggests that it is the uncontrolled postoperative pain itself, rather than the amount of opioids consumed, which might be an important factor in the development of POD. Uncontrolled pain is an extremely salient stimulus which takes valuable attention, potentially causing a patient to be less aware of other external cues and surroundings, thus losing this set of orienting cues which can be helpful to patients in the disrupted postoperative environment.
Prevention of Postoperative Delirium
POD is linked with both cognitive and noncognitive morbidity and mortality.4–9 Although several risk factors for POD have been identified, many of these preoperative risk factors such as age, cognitive status, and frailty11 are not necessarily modifiable. Pain management, on the other hand, is potentially something that anesthesiologists and acute pain physicians may optimize through thoughtfully selected multimodal analgesic strategies. The relationship between sleep, pain and delirium is complex, but it is clear that the diagnosis and adequate treatment of pain remains a key component of a preventive strategy to reduce postoperative delirium, as it also supports sleep.32 Although multimodal analgesic strategies, including scheduled nonopioid analgesics and regional analgesia, have demonstrated success in reducing pain, their association with reduced POD is often attributed to opioid reduction. Our findings suggest that reduction of pain itself may be more closely related to decreased delirium risk, and that use of all available analgesic strategies may be particularly important when considering the perioperative analgesic management of patients who may have baseline tolerance to opioids, as their pain is typically difficult to control in the postoperative period.
Limitations
The current study needs to be interpreted in light of several limitations. First, the amount of opioids preoperatively was not quantified, nor was the duration of preoperative opioid therapy, making it difficult to verify the presence or to assess the degree of opioid tolerance. Future studies should carefully quantify daily preoperative opioid consumption in order to define what degree of preoperative opioid use may be explicitly associated with higher risk of POD. Second, pain scores were gathered from the electronic medical record. While pain was frequently and regularly recorded with and between vital sign assessments, there was likely both subjectivity and variability in the reported scores, a limitation inherent to collection of assessments by different hands-on providers over the course of an inpatient stay, making this a potential source of error. Third, this study was performed at a single academic medical center and may not generalize to other clinical settings and samples. Fourth, the observational nature of this study precludes any speculation about whether uncontrolled pain (or opioid use) are important causative influences for POD. Fifth, this study only included older patients (≥70 years) having spinal surgery, and thus, findings may not generalize to a younger sample. In future studies, including a larger and more age-diverse patient population, as well as randomization of patients to an intervention, are needed to confirm whether optimizing postoperative pain control through intensive multimodal analgesia in opioid-tolerant patients may decrease the risk of POD.
Conclusion
This study showed that POD was not significantly associated with postoperative opioid consumption, but instead was associated with greater postoperative pain, especially in patients who were taking opioids preoperatively. This identifies an important, potentially modifiable risk factor in this older patient population, and should be an important consideration when determining the perioperative analgesic management of patients who may have baseline tolerance to opioids, as their pain is typically difficult to control in the postoperative period.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Partners Human Research Committee (PHRC)/Institutional Review Board (IRB).
Consent to Participate
All participants provided informed consent before participating in the study.
Funding
The conduct of this study was supported by a grant from the NIH/NIGMS: R35 GM128691 (K.L.S).
Disclosure
There were no relevant conflicts of interest for any of the authors.
References
1. Dasgupta M, Dumbrell AC. Preoperative risk assessment for delirium after noncardiac surgery: a systematic review. J Am Geriatr Soc. 2006;54:1578–1589. doi:10.1111/j.1532-5415.2006.00893.x
2. Hall MJ, DeFrances CJ, Williams SN, Golosinskiy A, Schwartzman A. National Hospital Discharge Survey: 2007 summary. Natl Health Stat Report. 2010;1–20:24.
3. Radtke FM, Franck M, MacGuill M, et al. Duration of fluid fasting and choice of analgesic are modifiable factors for early postoperative delirium. Eur J Anaesthesiol. 2010;27(5):411. doi:10.1097/EJA.0b013e3283335cee
4. Robinson TN, Raeburn CD, Tran ZV, Angles EM, Brenner LA, Moss M. Postoperative delirium in the elderly: risk factors and outcomes. Ann Surg. 2009;249(1):173–178. doi:10.1097/SLA.0b013e31818e4776
5. Saczynski JS, Marcantonio ER, Quach L, et al. Cognitive trajectories after postoperative delirium. N Engl J Med. 2012;367(1):30–39. doi:10.1056/NEJMoa1112923
6. Edelstein DM, Aharonoff GB, Karp A, Capla EL, Zuckerman JD, Koval KJ. Effect of postoperative delirium on outcome after Hip fracture. Clin Orthop Relat Res. 2004;422:195–200. doi:10.1097/01.blo.0000128649.59959.0c
7. Lundström M, Edlund A, Bucht G, Karlsson S, Gustafson Y. Dementia after delirium in patients with femoral neck fractures. J Am Geriatr Soc. 2003;51:1002–1006. doi:10.1046/j.1365-2389.2003.51315.x
8. Pompei P, Foreman M, Rudberg MA, Inouye SK, Braund V, Cassel CK. Delirium in hospitalized older persons: outcomes and predictors. J Am Geriatr Soc. 1994;42(8):809–815. doi:10.1111/j.1532-5415.1994.tb06551.x
9. Koster S, Hensens AG, Schuurmans MJ, van der Palen J. Consequences of delirium after cardiac operations. Ann Thorac Surg. 2012;93:705–711. doi:10.1016/j.athoracsur.2011.07.006
10. Susano MJ, Scheetz SD, Grasfield RH, et al. Retrospective analysis of perioperative variables associated with postoperative delirium and other adverse outcomes in older patients after spine surgery. J Neurosurg Anesthesiol. 2019;31:385–391. doi:10.1097/ANA.0000000000000566
11. Susano MJ, Grasfield RH, Friese M, et al. Brief preoperative screening for frailty and cognitive impairment predicts delirium after spine surgery. Anesthesiology. 2020;133:1184–1191. doi:10.1097/ALN.0000000000003523
12. Dyer CB. Postoperative delirium: a review of 80 primary data-collection studies. Arch Intern Med. 1995;155:461. doi:10.1001/archinte.1995.00430050035004
13. Lynch EP, Lazor MA, Gellis JE, Orav J, Goldman L, Marcantonio ER. The impact of postoperative pain on the development of postoperative delirium. Anesth Analg. 1998;86:781. doi:10.1213/00000539-199804000-00019
14. Vaurio LE, Sands LP, Wang Y, Mullen EA, Leung JM. Postoperative delirium: the importance of pain and pain management. Anesth Analg. 2006;102:1267–1273. doi:10.1213/01.ane.0000199156.59226.af
15. Leung JM, Sands LP, Lim E, Tsai TL, Kinjo S. Does preoperative risk for delirium moderate the effects of postoperative pain and opiate use on postoperative delirium? Am J Geriatr Psychiatry. 2013;21:946–956. doi:10.1016/j.jagp.2013.01.069
16. Fineberg SJ, Nandyala SV, Marquez-Lara A, Oglesby M, Patel AA, Singh K. Incidence and risk factors for postoperative delirium after lumbar spine surgery. Spine. 2013;38:1790–1796. doi:10.1097/BRS.0b013e3182a0d507
17. Smulter N, Lingehall HC, Gustafson Y, Olofsson B, Engström KG. Delirium after cardiac surgery: incidence and risk factors. Interact Cardiovasc Thorac Surg. 2013;17:790–796. doi:10.1093/icvts/ivt323
18. Norkiene I, Ringaitiene D, Misiuriene I, et al. Incidence and precipitating factors of delirium after coronary artery bypass grafting. Scand Cardiovasc J. 2007;41:180–185. doi:10.1080/14017430701302490
19. Joshi GP, Ogunnaike BO. Consequences of inadequate postoperative pain relief and chronic persistent postoperative pain. Anesthesiol Clin North Am. 2005;23:21–36. doi:10.1016/j.atc.2004.11.013
20. Wu CL, Naqibuddin M, Rowlingson AJ, Lietman SA, Jermyn RM, Fleisher LA. The effect of pain on health-related quality of life in the immediate postoperative period. Anesth Analg. 2003;97:1078–1085. doi:10.1213/01.ane.0000081722.09164.d5
21. Peters ML, Sommer M, de Rijke JM, et al. Somatic and psychologic predictors of long-term unfavorable outcome after surgical intervention. Ann Surg. 2007;245:487–494. doi:10.1097/01.sla.0000245495.79781.65
22. Kim H-J, Park J-H, Kim J-W, et al. Prediction of postoperative pain intensity after lumbar spinal surgery using pain sensitivity and preoperative back pain severity. Pain Med. 2014;15:2037–2045. doi:10.1111/pme.12578
23. Gerbershagen HJ, Aduckathil S, van Wijck AJM, Peelen LM, Kalkman CJ, Meissner W. Pain intensity on the first day after surgery. Anesthesiology. 2013;118:934–944. doi:10.1097/ALN.0b013e31828866b3
24. Leung JM, Sands LP, Rico M, et al. Pilot clinical trial of gabapentin to decrease postoperative delirium in older patients. Neurology. 2006;67:1251–1253. doi:10.1212/01.wnl.0000233831.87781.a9
25. Burkhart CS, Dell-Kuster S, Gamberini M, et al. Modifiable and nonmodifiable risk factors for postoperative delirium after cardiac surgery with cardiopulmonary bypass. J Cardiothorac Vasc Anesth. 2010;24:555–559. doi:10.1053/j.jvca.2010.01.003
26. Marcantonio ER. The relationship of postoperative delirium with psychoactive medications. JAMA. 1994;272:1518. doi:10.1001/jama.1994.03520190064036
27. Armaghani SJ, Lee DS, Bible JE, et al. Preoperative opioid use and its association with perioperative opioid demand and postoperative opioid independence in patients undergoing spine surgery. Spine. 2014;39:E1524–E1530. doi:10.1097/BRS.0000000000000622
28. Chu LF, Clark DJ, Angst MS. Opioid tolerance and hyperalgesia in chronic pain patients after one month of oral morphine therapy: a preliminary prospective study. J Pain. 2006;7:43–48. doi:10.1016/j.jpain.2005.08.001
29. Culley DJ, Flaherty D, Fahey MC, et al. Poor performance on a preoperative cognitive screening test predicts postoperative complications in older orthopedic surgical patients. Anesthesiology. 2017;127:765–774. doi:10.1097/ALN.0000000000001859
30. Inouye SK. Clarifying confusion: the confusion assessment method: a new method for detection of delirium. Ann Intern Med. 1990;113:941. doi:10.7326/0003-4819-113-12-941
31. Kuhn E, Du X, McGrath K, et al. Validation of a consensus method for identifying delirium from hospital records. PLoS One. 2014;9:e111823. doi:10.1371/journal.pone.0111823
32. O’Gara BP, Gao L, Marcantonio ER, Subramaniam B. Sleep, pain, and cognition: modifiable targets for optimal perioperative brain health. Anesthesiology. 2021;135:1132–1152. doi:10.1097/ALN.0000000000004046
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.