")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
The Relationship of Hyperferritinemia to Metabolism and Chronic Complications in Type 2 Diabetes
Authors Shang X, Zhang R, Wang X, Yao J, Zhao X, Li H
Received 7 November 2021
Accepted for publication 20 December 2021
Published 15 January 2022 Volume 2022:15 Pages 175—182
DOI https://doi.org/10.2147/DMSO.S348232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Xiaojing Shang,1 Rui Zhang,2 Xiaolai Wang,1 Junxin Yao,1 Xiaoying Zhao,1 Huanming Li3
1Department of Endocrinology, Tianjin Fourth Central Hospital, Tianjin, People’s Republic of China; 2Division of Health Management, Tianjin Fourth Central Hospital, Tianjin, People’s Republic of China; 3Department of Cardiology, Tianjin Fourth Central Hospital, Tianjin, People’s Republic of China
Correspondence: Huanming Li Email [email protected]
Aim: Elevated serum ferritin has been found to be closely related to type 2 diabetes mellitus. This study aimed to explore the relationship of high serum ferritin to metabolism and chronic complications in type 2 diabetes.
Methods: This was a cross-sectional study. A total of 330 type 2 diabetes patients who visited an endocrine clinic were included for the analysis. Serum ferritin and metabolic parameters were recorded. The prevalence of chronic diabetic complications was evaluated. Based on serum ferritin, participants were divided into hyperferritinemia and normal-ferritin groups. Metabolic parameters and prevalence of chronic diabetic complications were compared. The relationship between hyperferritinemia and chronic diabetic complications was explored with multivariate logistic regression models. Data were statistically analyzed by sex.
Results: Compared with the normal-ferritin group, the hyperferritinemia group showed higher levels of the serum inflammatory marker CRP and higher prevalence of diabetic retinopathy (DR) and coronary heart disease (CHD), regardless of sex (p< 0.05). Moreover, male patients with hyperferritinemia had increased serum triglyceride, alanine transferase, γ-glutamyltranspeptidase, urea nitrogen, creatinine, and uric acid and higher prevalence of microalbuminuria (p< 0.01). After controlling for demographics and metabolic profiles, hyperferritinemia remained an independent risk factor of DR (male OR 3.957, 95% CI 1.559– 10.041, p=0.004; female OR 2.474, 95% CI 1.127– 5.430, p=0.024) and CHD (male OR 2.607, 95% CI 1.087– 6.257, p=0.032; female OR 2.293, 95% CI 1.031– 5.096, p=0.042).
Conclusion: This study found that hyperferritinemia was associated with increased CRP and higher prevalence of DR and CHD in type 2 diabetes. In men, high serum ferritin was also associated with dyslipidemia, hepatic dysfunction, and microalbuminuria.
Keywords: diabetes mellitus, type 2, ferritin, metabolism, chronic complication
Introduction
Serum ferritin is widely recognized as an index of total iron stores. High serum ferritin indicates an overload of iron in the body.1 This overload is associated with the production of reactive oxygen species.2 Iron-induced oxidative stress is involved in various pathological conditions, such as type 2 diabetes mellitus (T2DM),3,4 cancers,5 and cardiovascular conditions.6,7 Serum ferritin is also considered a marker of systemic inflammation.8 Hyperferritinemia is linked to proinflammatory and immunosuppressive effects.9 Studies have shown that increased oxidative stress and inflammation are important mechanisms involved in the pathogenesis of T2DM and its complications. As such, the relationship of hyperferritinemia to T2DM and its complications is worthy of study. To our knowledge, little research has focused on the impact of hyperferritinemia on metabolic parameters in T2DM patients. Furthermore, the relationship between serum ferritin and diabetic complications is under debate. Suárez et al10 reported that high ferritin was associated with decreased cardiovascular disease risk in T2DM. Hermans et al11 reported that T2DM patients with high serum ferritin had lower prevalence of coronary artery disease, cerebrovascular disease, and peripheral artery disease. However, Mokhtari et al12 reported that serum ferritin had a significantly positive correlation with the likelihood and severity of coronary artery disease. Smotra et al13 reported a significant association between increased serum ferritin and nephropathy, retinopathy, and neuropathy. The purpose of this study was to describe and evaluate the relationship of hyperferritinemia to metabolism and chronic complications in T2DM.
Methods
Participants
This cross-sectional observational study included 330 T2DM patients with a DM course >5 years who attended Tianjin Fourth Central Hospital. Patients attending the endocrine clinic for improving glycemic control or screening complications were included. Exclusion criteria were malignant disease, acute inflammatory disease, primary liver or kidney disease, anemia (Hb <12 g%), hereditary hemochromatosis, a history of abundant alcohol intake (women >40 g/day, men >60 g/day), overt thyroid dysfunction, and taking such drugs as iron supplements, steroids, and antirheumatic drugs. The study has been conducted according to the principles expressed in the Declaration of Helsinki and was approved by the institutional review board of Tianjin Fourth Central Hospital (2017-SZXL017). All participants provided informed written consent.
Serum-Ferritin Measurement
Serum ferritin was measured using chemiluminescence (Cobas E411 Roche Diagnostics). Coefficient variations for intra- and interassays were <2% and <6.6% respectively. The reference interval was 30–400 μg/L in male, and 15–150 μg/L in female.14 Hyperferritinemia was defined as serum ferritin >400 μg/L in men or >150 μg/L in women. Patients with normal ferritin comprised the control group.
Determination of Metabolic Indices
Serum triglycerides (TGs), total cholesterol (TC), low–density lipoprotein cholesterol (LDL-C), blood urea nitrogen (BUN), creatinine (Cr), uric acid (UA), alanine transferase (ALT), γ-glutamyltranspeptidase (GGT), and fasting plasma glucose (FPG) were measured by enzymatic procedures using an autoanalyzer (Hitachi 7600-020). CRP was measured by immunoturbidimetry (Beckman Coulter). Glycated hemoglobin A1c (HbA1c) was measured by high-pressure liquid chromatography (Bio-Rad). Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration’s equation.15
Chronic Diabetes Complications
Diabetic retinopathy (DR) was defined as per the criteria of the Early Treatment for Diabetic Retinopathy Study based on nonmydriatic fundus photography. We used the ratio of urinary albumin to creatinine to define microalbuminuria (MAU). MAU was defined as an albumin:creatinine ratio ≥30 mg/g on two consecutive urine tests. Urine samples were excluded if microscopic urinalysis showed erythrocytes >5/high-power field, white blood cells >5/high-power field, epithelial cells >5/high-power field or apparent casts or bacteria. Coronary heart disease (CHD) was determined according to patient history, coronary arteriography, coronary computed tomography angiography, or echocardiography. Cerebrovascular disease was judged according to patient history or cranial computed tomography. Hypertension was determined according to patient history and blood pressure.
Statistical Analysis
Statistical analysis was performed using SPSS 11.0. Continuous variables are expressed as means ± SD or medians (IQR). Categorical variables are expressed as counts and percentages. Significance of differences was assessed by independent t-tests for normally distributed variables or Mann–Whitney U tests for variables with skewed distribution. For comparison of qualitative data, χ2 tests were used. Strength of association between two variables was assessed with Spearman correlation analyses. Logistic regression was used to identify the relationship between chronic DM complications and hyperferritinemia. Covariates controlled in multivariate logistic models were DM duration, age, smoking status, body-mass index (BMI), TC, TGs, LDL-C, BUN, Cr, FPG, HbA1c, and CRP. Results were expressed as odds ratios (OR) and 95% confidence intervals (CIs). Two-sided p<0.05 was considered statistically significant.
Results
Comparison of Clinical Characteristics and Metabolic Parameters Between Hyperferritinemia and Normal-Ferritin Groups
Of the 330 patients, 179 were men and 151 women. In men, median serum ferritin in the hyperferritinemia and normal-ferritin groups was 562.1 (254.5) μg/L and 211.5 (122.6) μg/L, respectively (p<0.01). There were no significant differences for DM duration, age, smoking rate, BMI, TC, LDL-C, eGFR, FPG, or HbA1c between the hyperferritinemia and normal-ferritin groups (p>0.05). However, serum TGs, ALT, GGT, BUN, UA, Cr, and CRP in the hyperferritinemia group were significantly higher than in the normal-ferritin group (p<0.01, Table 1). In women, median serum ferritin in the hyperferritinemia and normal-ferritin groups was 223.1 (109.6) μg/L and 108.1 (54.6) μg/L, respectively (p<0.01). Only serum CRP in the hyperferritinemia group was significantly higher (p<0.01, Table 1).
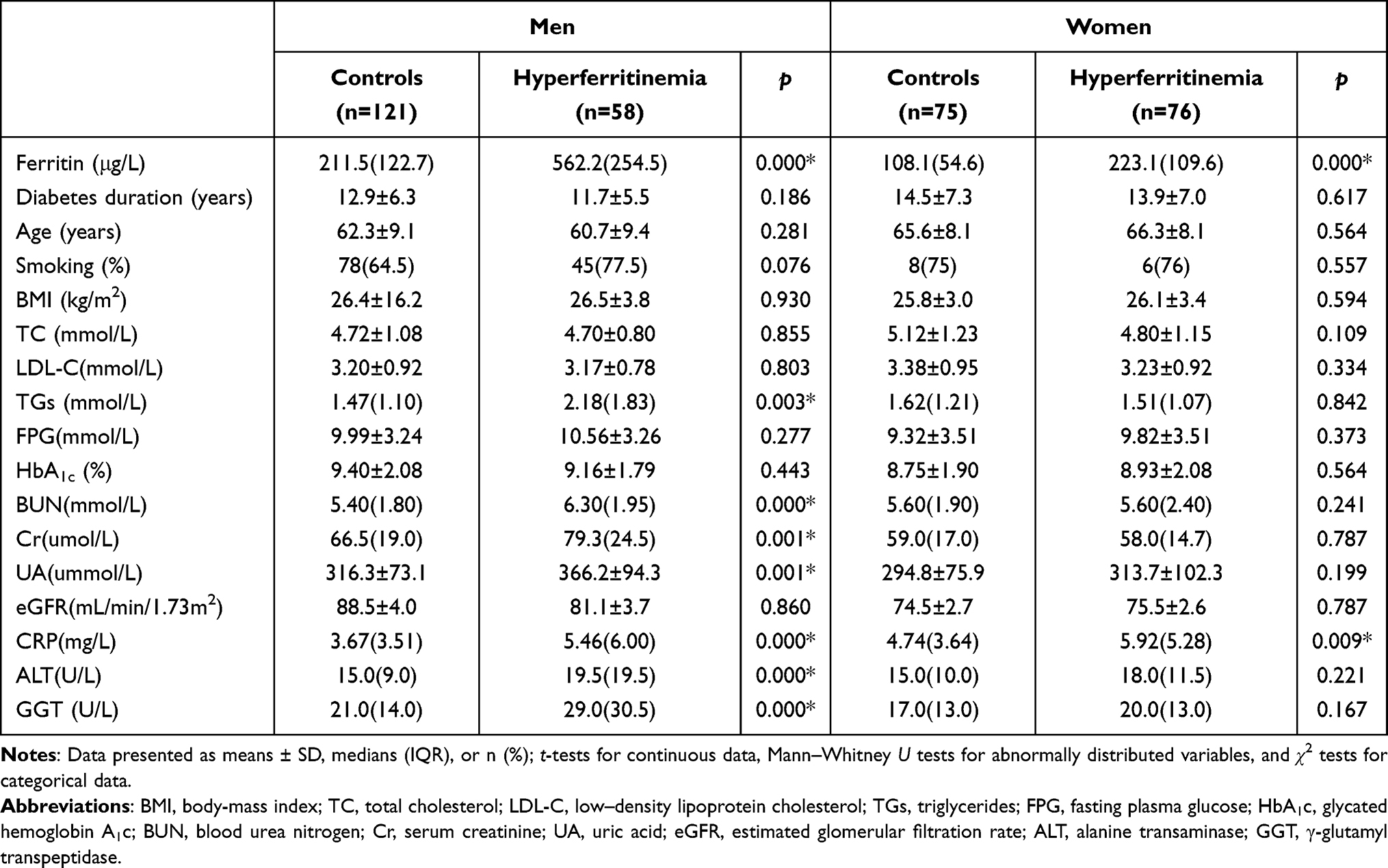 |
Table 1 Clinical characteristics and metabolic parameters in hyperferritinemia and normal-ferritin groups |
Comparison of Prevalence of Chronic Diabetes Complications Between Hyperferritinemia and Normal-Ferritin Groups
As shown in Table 2, the prevalence of DR and CHD for both men and women was significantly higher in the hyperferritinemia group (p<0.05), while cerebrovascular disease showed no difference (p>0.05).The prevalence of MAU and hypertension in the hyperferritinemia group was also significantly higher than the normal-ferritin group in men (p<0.05).
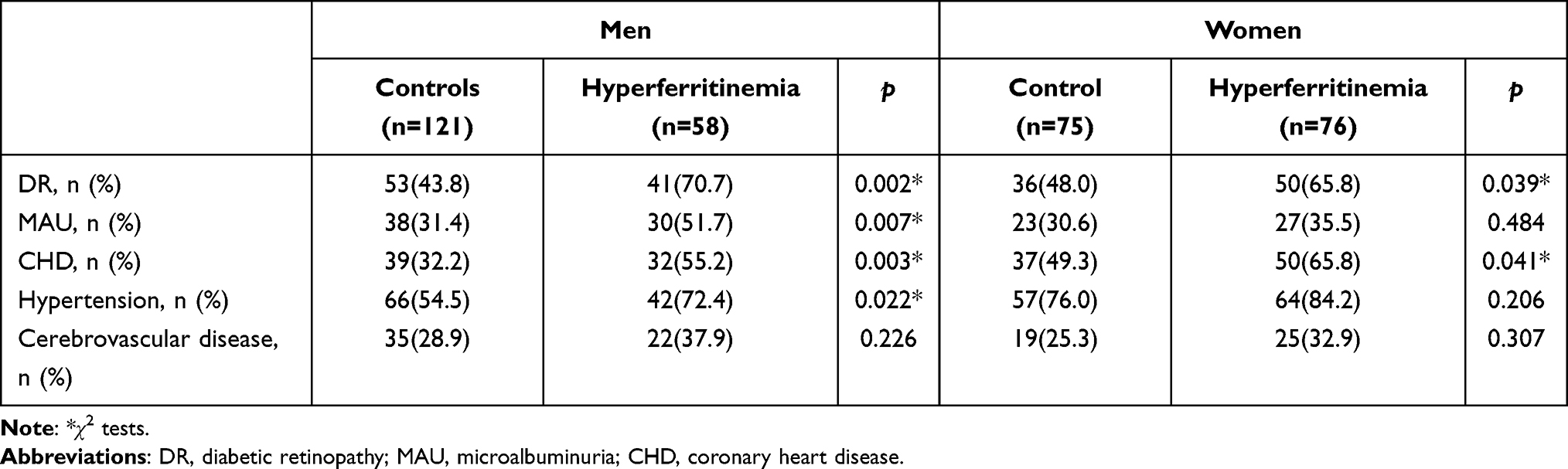 |
Table 2 Chronic diabetic complications in hyperferritinemia and normal-ferritin groups |
Correlation of Hyperferritinemia with Metabolic Parameters and Chronic Diabetes Complications
In men, hyperferritinemia was positively correlated with ALT (r=0.315, p=0.000), GGT (r=0.274, p=0.000), CRP (r=0.299, p=0.000), BUN (r=0.279, p=0.000), Cr (r=0.244, p=0.001), UA (r=0.231, p=0.002), TGs (r=0.227 p=0.002), DR (r=0.243, p=0.002), CHD (r=0.219, p=0.003), MAU (r=0.204, p=0.007), hypertension (r=0.171, p=0.022), and BMI (r=0.196, p=0.009). In women, hyperferritinemia was positively correlated with CRP (r=0.216, p=0.008), DR (r=0.175, p=0.040), and CHD (r=0.167, p=0.041).
Logistic Regression Analysis of Associations Between Chronic Diabetes Complications and Hyperferritinemia
In multivariate logistic models, after controlling for demographic and metabolic variables, DR was identified as the dependent variable. Hyperferritinemia remained independently associated with DR (male OR 3.957, 95% CI 1.559–10.041, p=0.004; female OR 2.474, 95% CI 1.127–5.430, p=0.024) (Table 3). Similarly, when CHD was identified as the dependent variable, hyperferritinemia remained an independent risk factor of CHD (male OR 2.607, 95% CI 1.087–6.257, p=0.032; female OR 2.293, 95% CI 1.031–5.096, p=0.042; Table 4). The association between hyperferritinemia and MAU remained significant in men (OR 2.162, 95% CI 1.096–5.055; p=0.045; Table 5).
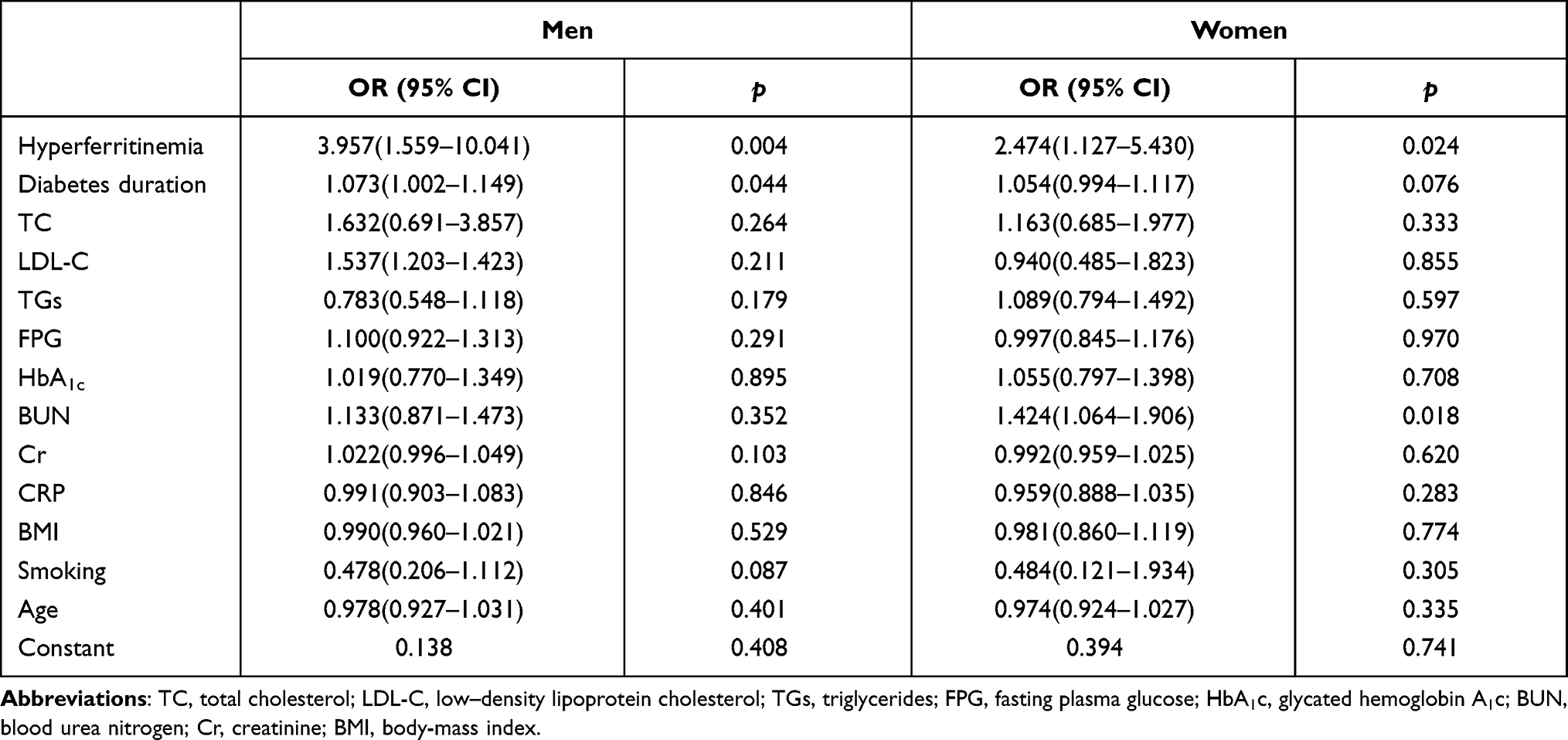 |
Table 3 Logistic regression analysis of associations between DR and hyperferritinemia |
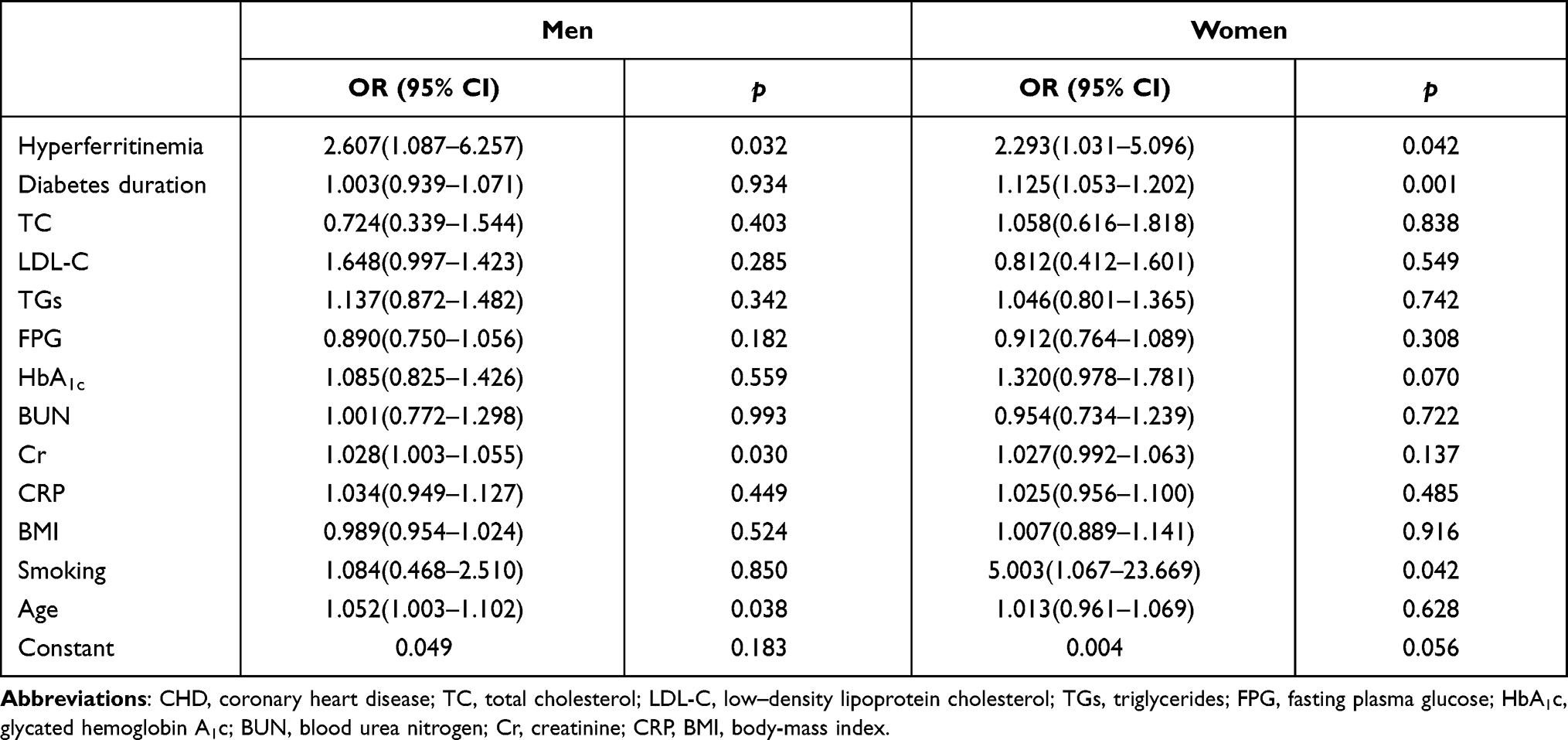 |
Table 4 Logistic regression analysis of associations between CHD and hyperferritinemia |
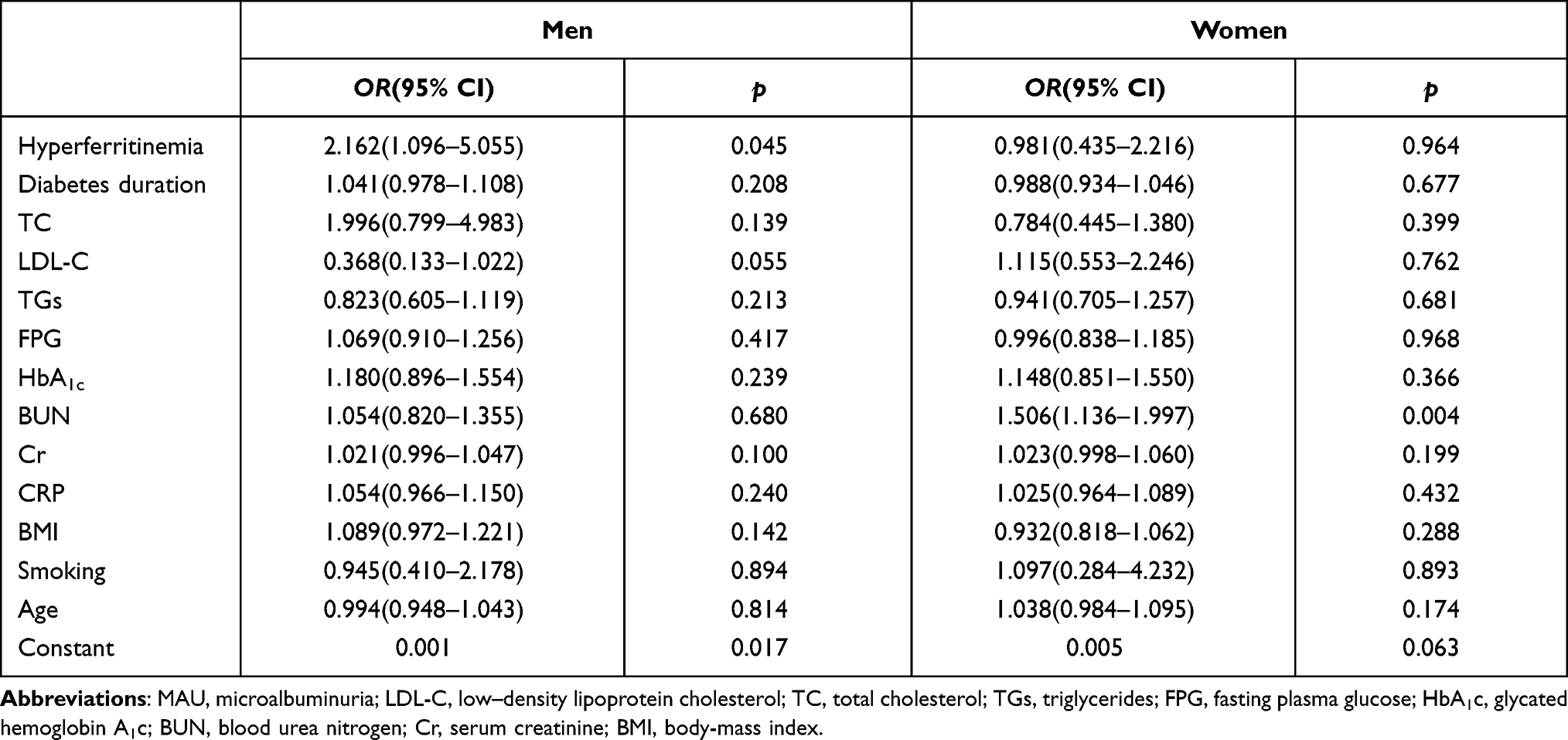 |
Table 5 Logistic regression analysis of associations between MAU and hyperferritinemia |
Discussion
The relationship between hyperferritinemia and metabolism and chronic complication in T2DM is controversial. The present study demonstrates that hyperferritinemia has a relationship with metabolism and chronic complications in T2DM. We have shown here that hyperferritinemia is associated with increased CRP levels and prevalence of DR and CHD. Another important outcome of the present study was that hyperferritinemia was associated with increased serum TGs, ALT, GGT, BUN, UA, and Cr and higher prevalence of MAU in men.
Associations Between Hyperferritinemia and Metabolic Characteristics in Type 2 Diabetes Patients
There was no significant difference in BMI or glycemic control index (FPG, HbA1c) values between the hyperferritinemia and normal-ferritin groups, ie, high serum ferritin was not associated with BMI or poor glycemic control in longer-course DM patients. Patients with hyperferritinemia had higher CRPs level regardless of sex, with a significantly positive correlation between hyperferritinemia and CRPs. Our results are in agreement with Khan et al,16 who reported a strong positive correlation between ferritin and CRP (r=0.87, p<0.001). Accumulated evidence supports serum ferritin being considered a marker of systemic inflammation and a key mediator of immunodysregulation.9
Notably, levels of TGs, ALT, GGT, BUN, Cr, and UA in the hyperferritinemia group were higher than the normal-ferritin group in men. A significant positive correlation was found between hyperferritinemia and metabolic index values. Musina et al17 reported ferritin concentration was positively correlated with TG levels (r=0.244, p<0.05). Smotra et al13 found that serum ferritin had a significantly positive correlation with TGs, but not with LDL-C. In addition, Chen et al18 found that serum ferritin was independently associated with metabolic syndrome and insulin resistance. It has been inferred that hyperferritinemia may be an additional cause of insulin resistance in T2DM and metabolic syndrome.19,20
With regard to the relationship between hyperferritinemia and ALT/GGT, as early as the 1990s, dysmetabolic iron-overload syndrome was described as “liver-iron overload” for the first time.21 A number of studies22,23 had shown that iron overload was significantly associated with the severity of nonalcoholic fatty-liver disease (NAFLD) and that serum ferritin was an independent risk factor of NAFLD progression to nonalcoholic steatohepatitis. Studies by Ruddell et al24 in rat hepatic stellate cells showed that ferritin, as a proinflammatory mediator acting through the nuclear factor-kappa B-signaling pathway, played a potential role in inflammatory processes associated with hepatic fibrogenesis. Yang et al25 reported that subjects with higher dietary iron intake were subject to a higher prevalence of NAFLD in a dose–response manner. Interestingly, their study also found that the association probably only exists in men. Therefore, it can be taken that serum ferritin plays a very important role in the occurrence of chronic liver injury and even cirrhosis in men.
In our study, statistically significant correlations were found between hyperferritinemia and BUN, Cr, and UA levels in men. This finding was similar to Smotra et al,13 who found that serum ferritin was positively correlated with the level of serum UA (p<0.05). The underlying mechanism to explain this relationship remains unknown. Nutrition research has shown that red meat is the main source of heme iron, which is the major factor affecting iron load in the body,26,27 so it may be that the association between red-meat intake and serum ferritin is one of the reasons. The sex-based difference observed in the present study might be explained by the different serum-ferritin levels between men and women. The reasons for this difference in serum ferritin may be28 menstruation and dietary factors.29 However, further mechanisms still need to be revealed.
Association Between Hyperferritinemia and Chronic Complications in Type 2 Diabetes Patients
Our results showed that 70.7% of men and 65.8% of women who had T2DM >5 years with hyperferritinemia had DR, 55.2% of men and 65.8% of women had CHD, both significantly higher than the control population with normal serum ferritin. Interestingly, a relationship between hyperferritinemia and cerebrovascular disease was not found. DR and nephropathy are the most common microvascular complications in T2DM patients. These two complications are characterized by inflammation, microvascular alteration, and neurodegeneration. An overload of iron can cause cell damage through mechanisms involved in increased oxidative stress, activation of inflammatory cytokines, and macrophage infiltration. As such, high ferritin itself may also be responsible for the incidence and development of DR and nephropathy. Studies have explored this relationship. Hsu et al30 showed that hyperferritinemia may be an independent risk factor of nephropathy in patients with T2DM. Wu et al31 reported that serum ferritin independently predicts the incidence of chronic kidney disease in patients with T2DM. Our study showed that there was a positive correlation between hyperferritinemia and DR, regardless of sex.
After adjustment for confounding factors, hyperferritinemia remained an independent risk factor of DR. A positive correlation between hyperferritinemia and MAU was found in male subjects (r=0.204, p=0.007). A similar relationship between increased serum ferritin and DR and nephropathy was evident in Smotra et al,13 in which persistent hyperglycemia appeared to be the primary factor to explain the association. However, in our study, levels of FPG and HbA1c in the hyperferritinemia and normal-ferritin group was approximate and the association between hyperferritinemia and DR and MAU independent of glycemic control. Therefore, it can be inferred that increased serum ferritin may be another risk factor of DR or microalbuminuria in patients with T2DM, especially in men.
Possible mechanisms to explain the association have been studied in experimental animalresearch. Chaudhary et al32 found that retinal iron-overload affected integrity of the blood–retina barrier and accelerated retinal cells loss by enhancing oxidative stress and inflammatory signals. Iron overload also induced retinal renin expression. Through these mechanisms, iron overload aggravated the progression of DR in mice. Chaudhary et al33 reported that renal iron accelerated the progression of diabetic nephropathy in association with renal–renin–angiotensin system activation. These results remain to be confirmed in future clinical research.
Iron may possibly be another additional risk factor involved in cardiovascular disease. However, the evidence for this is still controversial. You et al34 found high levels of L-ferritin in coronary arteries in patients with CHD, indicating that iron had accumulated in atherosclerotic plaques. However, Gill et al35 reported that there was a negative association between high iron status and CHD risk. More evidence is needed for the relationship between iron and CHD. We compared the prevalence of CHD between a hyperferritinemia group and a normal-ferritin group. The association between hyperferritinemia and CHD was also analyzed. The results showed that CHD prevalence in the hyperferritinemia group was significantly higher than the normal-ferritin group. Hyperferritinemia remained an independent risk factor of CHD on logistic regression analysis, consistent with Salonen et al,36 who reported a positive correlation between serum ferritin and acute myocardial infarction in men, and Mokhtari et al,12 who reported that serum ferritin had significant efficiency to predict CHD (AUC=0.61, p=0.02). Although the exact mechanism of iron-induced atherosclerosis is uncertain, it is likely to be mediated by catalysis of the formation of reactive oxygen species, oxidation of lipoproteins, and vascular dysfunction.37
Nevertheless, when interpreting the findings of the current work, some limitations should be considered. Firstly, this study was cross-sectional study, which allows no conclusions on cause and effect. Secondly, because the sample was relatively small, we could not present data as quartiles/quintiles of ferritin, and this may have limited possible associations. Thirdly, the determination of CHD in subjects in this study was based on typical symptoms, with a lack of objective methods by means of instruments and equipments. Therefore, there may be some deviations between the statistical results and the real values.
Conclusion
The current study showed that hyperferritinemia was related to increased CRP levels and higher prevalence of DR and CHD in T2DM patients. In men, high serum ferritin was also associated with dyslipidemia, hepatic dysfunction, and microalbuminuria. Ferritin may be used as an important biomarker to assess metabolic disorders and the risk of chronic complications in patients with T2DM.
Funding
This work was supported by Tianjin Major Science and Technology Projects (17ZXMFSY00200) and Tianjin Science and Technology Development Strategy Research Projects (18ZLZXZF00740).
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
References
1. Recalcati S, Gammella E, Buratti P, et al. Molecular regulation of cellular iron balance. IUBMB Life. 2017;69(6):389–398. doi:10.1002/iub.1628
2. Brissot P, Ropert M, Le Lan C, et al. Non-transferrin bound iron: a key role in iron overload and iron toxicity. Biochim Biophys Act. 2012;1820(3):403–410. doi:10.1016/j.bbagen.2011.07.014
3. Podmore C, Meidtner K, Schulze MB, et al. Association of multiple biomarkers of iron metabolism and type 2 diabetes: the EPIC-interact study. Diabetes Care. 2016;39(4):572–581. doi:10.2337/dc15-0257
4. Altamura S, Kopf S, Schmidt J, et al. Uncoupled iron homeostasis in type 2 diabetes mellitus. J Mol Med. 2017;95(12):1387–1398. doi:10.1007/s00109-017-1596-3
5. Zhang C, Zhang F. Iron homeostasis and tumorigenesis: molecular mechanisms and therapeutic opportunities. Protein Cell. 2015;6(2):88–100. doi:10.1007/s13238-014-0119-z
6. Kell DB. Iron behaving badly: inappropriate iron chelation as a major contributor to the aetiology of vascular and other progressive inflammatory and degenerative diseases. BMC Med Genomics. 2009;8(2). doi:10.1186/1755-8794-2-2
7. Kobayashi M, Suhara T, Baba Y, et al. Pathological roles of iron in cardiovascular disease. Curr Drug Targets. 2018;19(9):1068–1076. doi:10.2174/1389450119666180605112235
8. Recalcati S, Invernizzi P, Arosio P, et al. New functions for an iron storage protein: the role of ferritin in immunity and autoimmunity. J Autoimmun. 2008;30(1–2):84–89. doi:10.1016/j.jaut.2007.11.003
9. Kernan KF, Carcillo JA. Hyperferritinemia and inflammation. Int Immunol. 2017;29(9):401–409. doi:10.1093/intimm/dxx031
10. Suárez-Ortegón MF, McLachlan S, Price AH, et al. Decreased iron stores are associated with cardiovascular disease in patients with type 2 diabetes both cross-sectionally and longitudinally. Atherosclerosis. 2018;272:193–199. doi:10.1016/j.atherosclerosis.2018.03.028
11. Hermans MP, Ahn SA, Amoussou-Guenou KD, et al. Do high ferritin levels confer lower cardiovascular risk in men with Type 2 diabetes? Diabet Med. 2010;27:417–422. doi:10.1111/j.1464-5491.2010.02979.x
12. Mokhtari H, Bagherib B, Rasoulia M. Iron hypothesis and coronary artery disease in geriatric patients. Arch Physiol Biochem. 2020;126(1):1,17–22. doi:10.1080/13813455.2018.1486429
13. Smotra S, Kudyar RP. Relationship between serum ferritin and type-2 diabetes mellitus. JK Sci. 2008;10(4):170–174.
14. Hong S, San WY, Yu SZ. National Clinical Laboratory Operating Procedures. Beijing, China: People’s Health Publishing House; 2015:121.
15. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
16. Khan A, Khan WM, Ayub M, et al. Ferritin is a marker of inflammation rather than iron deficiency in overweight and obese People. J Obes. 2016;2016:1937320. doi:10.1155/2016/1937320
17. Musina N, Saprina VT, Prokhorenko ST, et al. Correlations between iron metabolism parameters, inflammatory markers and lipid profile indicators in patients with type 1 and type 2 diabetes mellitus. J Pers Med. 2020;10(3):70. doi:10.3390/jpm10030070
18. Chen L, Li Y, Zhang F, et al. Association of serum ferritin levels with metabolic syndrome and insulin resistance in a Chinese population. J Diabetes Complications. 2017;31(2):364–368. doi:10.1016/j.jdiacomp.2016.06.018
19. Tang Q, Liu Z, Tang Y, et al. High serum ferritin level is an independent risk factor for metabolic syndrome in a Chinese male cohort population. Diabetol Metab Syndr. 2015;7(1):11. doi:10.1186/s13098-015-0004-9
20. Tofano RJ, Pescinni-Salzedas LM, Chagas EFB, et al. Association of metabolic syndrome and hyperferritinemia in patients at cardiovascular risk. Diabetes Metab Syndr Obes. 2020;13:3239–3248. doi:10.2147/DMSO.S271050
21. Rametta R, Fracanzani AL, Fargion S, et al. Dysmetabolic hyperferritinemia and dysmetabolic iron overload syndrome (DIOS): two related conditions or different entities? Curr Pharm Des. 2020;26(10):1025–1035. doi:10.2174/1381612826666200131103018
22. Datz C, Müller E, Aigner E. Iron overload and non-alcoholic fatty liver disease. Minerva Endocrinol. 2017;42(2):173–183. doi:10.23736/S0391-1977.16.02565-7
23. Buzzetti E, Petta S, Manuguerra R, et al. Evaluating the association of serum ferritin and hepatic iron with disease severity in non-alcoholic fatty liver disease. Liver Int. 2019;39(7):1325–1334. doi:10.1111/liv.14096
24. Ruddell RG, Hoang-le D, Barwood JM, et al. Ferritin functions as a proinflammatory cytokine via iron-independent protein kinase C zeta/ nuclear factor kappa B-regulated signaling in rat hepatic stellate cells. Hepatology. 2009;49(3):887. doi:10.1002/hep.22716
25. Yang Z, Wu J, Li X, et al. Association between dietary iron intake and the prevalence of nonalcoholic fatty liver disease: a cross-sectional study. Medicine. 2019;98(43):e17613. doi:10.1097/MD.0000000000017613
26. Qi L, van Dam RM, Rexrode K, et al. Heme iron from diet as a risk factor for coronary heart disease in women with type 2 diabetes. Diabetes Care. 2007;30(1):101–106. doi:10.2337/dc06-1686
27. Misra R, Balagopal P, Raj S, et al. Red meat consumption (Heme Iron Intake) and risk for diabetes and comorbidities? Curr Diab Rep. 2018;18(11):100. doi:10.1007/s11892-018-1071-8
28. Hou Y, Zhang S, Wang L, et al. Estrogen regulates iron homeostasis through governing hepatic hepcidin expression via an estrogen response element. Gene. 2012;511(2):398–403. doi:10.1016/j.gene.2012.09.060
29. Huang LN, Wang HJ, Wang ZH, et al. Association of red meat usual intake with serum ferritin and the risk of metabolic syndrome in Chinese adults: a longitudinal study from the China Health and Nutrition Survey. Biomed Environ Sci. 2020;33(1):19–29. doi:10.3967/bes2020.003
30. Hsu YH, Huang MC, Chang HY, et al. Association between serum ferritin and microalbuminuria in Type 2 diabetes in Taiwan. Diabet Med. 2013;30(11):1367–1373. doi:10.1111/dme.12257
31. Wu YH, Wang SY, Li MX, et al. Serum ferritin independently predicts the incidence of chronic kidney disease in patients with type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2020;13:99–105. doi:10.2147/DMSO.S228335
32. Chaudhary K, Promsote W, Ananth S, et al. Iron overload accelerates the progression of diabetic retinopathy in association with increased retinal renin expression. Sci Rep. 2018;8(1):1–12. doi:10.1038/s41598-018-21276-2
33. Chaudhary K, Chilakala A, Ananth S, et al. Renal iron accelerates the progression of diabetic nephropathy in the HFE gene knockout mouse model of iron overload. Am J Physiol Renal Physiol. 2019;317(2):512–517. doi:10.1152/ajprenal.00184.2019
34. You SA, Archacki SR, Angheloiu G, et al. Proteomic approach to coronary atherosclerosis shows ferritin light chain as a significant marker: evidence consistent with iron hypothesis in atherosclerosis. Physiol Genomics. 2003;13(1):25–30. doi:10.1152/physiolgenomics.00124.2002
35. Gill D, Del Greco MF, Walker AP, et al. The effect of iron status on risk of coronary artery disease: a Mendelian randomization study-brief report. Arterioscler Thromb Vasc Biol. 2017;37(9):1788–1792. doi:10.1161/ATVBAHA.117.309757
36. Salonen JT, Nyyssonen K, Korpela H, et al. High stored iron levels are associated with excess risk of myocardial infarction in eastern Finnish men. Circulation. 1992;86(3):803–811. doi:10.1161/01.cir.86.3.803
37. Xu S. Iron and atherosclerosis: the link revisited. Trends Mol Med. 2019;25(8):659–661. doi:10.1016/j.molmed.2019.05.012
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.