Back to Journals » Psychology Research and Behavior Management » Volume 16
The Relationship Between Risk Perception, Physical Activity, and Adolescent Mental Health: A Cross-Lagged Analysis
Received 14 June 2023
Accepted for publication 12 August 2023
Published 24 August 2023 Volume 2023:16 Pages 3347—3357
DOI https://doi.org/10.2147/PRBM.S422982
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mei-Chun Cheung
Siyuan Li, Ying Wang
College of Education, Adamson University, Manila, Philippines
Correspondence: Siyuan Li, Email [email protected]
Background: During the novel coronavirus pandemic, the prevalence of anxiety and depressive symptoms among adolescents rose dramatically to 31% and 34%, respectively. This study aims to elucidate the relationship between perceived disease risk, physical activity, and adolescent mental health, questioning whether physical activity maintains its protective role amidst heightened disease risk.
Methods: In a longitudinal study design, questionnaires were administered twice, in December 2022 and January 2023, to a cohort of students across five high schools. These questionnaires measured adolescents’ perception of disease risk, their physical activity levels, and their mental health status during the pandemic. A total of 344 students participated in this study.
Results: The data revealed significant gender differences in risk perception, with gender difference effects of 0.255 (d=0.416) and 0.195 (d=0.402) across both indicators, and in mental health, with gender difference effects of 0.159 (d=0.262) and 0.179 (d=0.278). Risk perception at Time 1 was found to be a significant predictor of both physical activity and mental health (β values of 0.28 and 0.19, P < 0.01, respectively). Physical activity at Time 1 was also a significant predictor of mental health at Time 2 (β = 0.33, P < 0.01). Moreover, physical activity mediated the relationship between risk perception and mental health, as suggested by a significant indirect effect (mediator effect of 0.012, Z value of 0.112, and a Bootstrap 95% CI excluding 0).
Conclusion: This study underscores a longitudinal relationship between adolescents’ perception of disease risk, physical activity, and mental health. It highlights the potential benefits of promoting physical activity awareness among adolescents as a strategy to improve mental health outcomes during pandemics.
Keywords: teenagers, risk perception, mental health, physical activity, cross-lagging analysis
Introduction
The impact of the global new coronavirus pandemic (COVID-19) has been imprinted on everyone’s mind. This sudden threat of disease, combined with social, economic, and psychological stress, has had a significant impact on the mental health of the adolescent population. A complex and subtle relationship between adolescents’ perception of disease risk and their psychological health has also arisen.
To clarify the relationship between adolescent risk perception and mental health, it is proposed, based on social risk theory, that specific risk factors, such as epidemics, may pose a threat to society or individuals under specific social circumstances and conditions. People’s perception of this threat may further affect their mental health. That is, it is shown that when the risk of epidemics is evident, adolescents’ perception of risk may increase, which in turn may trigger their negative emotions such as anxiety and depression.1 On the other hand, combing through the available relevant studies revealed that physical activity is an effective strategy to relieve adolescents’ psychological stress;2 however, in the context of an epidemic, adolescents may reduce their participation in outdoor physical activities due to fear of disease infection, which may further negatively affect their psychological health. This context therefore emphasizes the need for a deeper understanding and study of the relationship between adolescents’ disease risk perceptions and mental health so that we can develop more effective strategies to help them cope with the various challenges posed by the epidemic.
In summary, this study developed a theoretical framework to explore the interaction between adolescents’ perceptions of disease risk, physical activity, and mental health. In the theoretical framework, “disease risk perception” is interpreted as adolescents’ personal understanding and evaluation of the risk of disease transmission and infection; “physical activity” covers the time and frequency of outdoor activities that adolescents devote to each week; and “mental health status” is assessed and quantified by using a standardized mental health assessment tool. In other words, we explore the interrelationships between adolescents’ personal perceptions of disease risk, their level of physical activity participation, and their mental health status as derived from professional tools.
To explore in depth the dynamic relationship between these three factors, a cross-lagged analysis will be used. This is a statistical method that has been used to study the causal relationship between two or more time series variables. This method reveals how a change in one variable affects a change in another variable after a time delay.3 This method has been widely used in various fields such as economics, psychology, and biostatistics. Specifically, we will collect data through a longitudinal design in which data on adolescents’ disease risk perceptions, physical activity, and mental health will be collected at multiple time points during the epidemic. Cross-lagged analyses will then be used to examine the dynamic relationships between these variables, such as how disease risk perceptions affect physical activity and how physical activity affects mental health, or whether there is a time delay in these relationships. It is hoped that this study will provide public health policymakers with more targeted strategies to maintain the mental health of adolescents and help them navigate safely and healthily through the global pandemic epidemic.
Study Design
Implementation Procedures
Mental health problems among high school-aged adolescents are becoming increasingly prominent in the current social environment. In order to better understand and prevent these problems, this study will explore the effects of risk perception and physical activity on adolescent mental health. Therefore, we hypothesise that there is an interaction between risk perception and physical activity that has a more significant effect on adolescent mental health. Specifically, we hypothesised that physical activity would have a more positive impact on mental health for those adolescents with lower risk perception, whereas the impact of physical activity on mental health would be less significant for those adolescents with higher risk perception. We wished to test this hypothesis through cross-lagged analyses. A random sampling method was used to select five high school schools in three regions of China to conduct two questionnaire surveys. Survey T1 was conducted in December 2022, 200 questionnaires were distributed in high schools, 32 invalid questionnaires were excluded, and 168 valid questionnaires were obtained; survey T2 was a re-survey of the first respondents in January 2023, and cross-lagged analyses were used to assess the effects of risk perception (T1) and physical activity (T1) on psychological well-being (T2 and T2), as well as the risk perception and physical activity interaction effects. This study may contribute to a better understanding and prevention of mental health problems among adolescents in high school and provide more targeted strategies for mental health interventions.
Ethical Procedures
All participants (including their parents or guardians, if the subject is under 18 years of age) must sign the informed consent form only after clearly understanding the purpose of the study, the methods, the possible risks and benefits, and their rights. If subjects choose to withdraw, the investigator should respect their decision. And do everything in their power to protect the privacy of participants. Participants’ personal information should be desensitised as far as possible and results should be reported anonymously to protect participants’ identity.
Subjects of the Survey
Adolescents are the transitional period when children change their adult roles, and also refers to the human life group during the transition from children to adults. Generally speaking, adolescents are divided into two stages: 14–17 years old and 18–25 years old, and this study focuses on adolescents aged 14–17 years old.
Sample Size, Sample Selection and Form of Participation
Two questionnaire surveys were conducted in five high schools in three regions of China through random sampling. Survey T1 was conducted in December 2022, 200 questionnaires were distributed in the high schools, 32 invalid questionnaires were excluded, and 168 valid questionnaires were obtained; Survey T2 was conducted in January 2023, the respondents of Survey T1 were re-surveyed, 200 questionnaires were distributed, 24 invalid questionnaires were excluded, and 176 valid questionnaires were obtained. As a final valid sample size, 344 data were used.178 (51.75%) male and 166 (48.25%) female students gave informed consent to participate in this study.
Collection Tools
Based on the questionnaire on physical exercise prepared by the Institute of Sports Science of the State General Administration of Sport and the National Physical Fitness Monitoring Centre,4 as well as the measurement indexes of exercise behaviour proposed by Qiu Fen et al. On this basis, a questionnaire on physical exercise for adolescent students was compiled, with 12 questions, including 3 dimensions of exercise attitude, exercise time and exercise frequency.
The Generalised Anxiety Disorder 7 (GAD-7) is a self-assessment scale for screening anxiety symptoms based on the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) and Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-V) diagnostic criteria published by the American Psychiatric Association.5 It is a valid tool for identifying the likelihood or tendency of Generalised Anxiety Disorder, and has been shown to have good reliability and validity in previous studies.
The Perceived Social Risk Scale (PSRS) is a measurement tool developed by Cui Xiaoqian and other scholars, with a total of 9 questions, divided into 3 dimensions: severity, susceptibility, and controllability.6 The severity dimension aims to assess the individual’s perception of the importance and severity of the consequences of a particular social risk; the susceptibility dimension focuses on the individual’s perception of his or her own or the community’s vulnerability or susceptibility to a particular social risk; and the controllability dimension evaluates the individual’s perception of the controllability and manageability of a social risk. The scale can be widely used in research in the social sciences, psychology, and social work to help understand how people perceive and assess potential risks in the social environment, as well as their knowledge of and confidence in preventive measures. Previous studies have also shown that the scale has good reliability and validity and can effectively measure different aspects of social risk perception.
Data Collection and Transformation
Data Collection
In the study “Cross-lagged Analysis of the Relationship between Risk Perception, Physical Activity, and Mental Health of Adolescents in High School”, we first collected data through a questionnaire. Perceived risk was assessed through a series of questions or statements that participants rated on a scale that could involve perceptions of uncertainty, fear of negative outcomes, etc. The scale consisted of seven items, each symptom of which was rated by the participant. The scale consists of 7 entries, with each symptom entry rated on a 4-point scale from 0 to 3, for a total score of 21. According to the scale, the GAD-7 score was divided into 4 groups: 0 to 4 as no obvious anxiety symptoms, 5 to 9 as mild anxiety, 10 to 14 as moderate anxiety, and 15 to 21 as severe anxiety due. The total scale Cronbach’s alpha was 0.914 (T1) and 0.925 (T2). The split-half reliabilities were 0.922 (T1) and 0.941 (T2). The stability coefficient was 0.871 (p<0.01).
Physical activity, on the other hand, was recorded through a questionnaire that recorded the participants’ attitudes towards the physical activities they performed, the duration of each activity, and the frequency of the activities. Adolescent mental health was assessed using standardised mental health scales such as the Adolescent Self-Reported Mental Health Scale. A 5-point Likert scale was used. The total scale Cronbach’s α was 0.926 (T1) and 0.930 (T2). The split-half reliabilities were 0.902 (T1) and 0.911 (T2), and the stability coefficient was 0.835 (P<0.01).
The Perceived Social Risk Scale had a total of 9 questions, containing 3 dimensions of severity, susceptibility, and controllability, using a 5-point Likert scale, with the perceived severity, susceptibility, and controllability of risk increasing in order from “low (1)” to “high (5)”. Cronbach’s alpha for the total scale was 0.901 (T1) and 0.913 (T2). Split-half reliabilities were 0.874 (T1) and 0.908 (T2), with a stability coefficient of 0.866 (p<0.01).
After collecting the data, we performed a series of variable transformations. Risk perception was assessed by summing or averaging scores across all items and possibly factor analyses to derive more specific dimensions of risk perception. Mental health scores, on the other hand, were derived by summing or averaging the scores of all items on the scale, and possibly factor analyses to derive more specific dimensions of mental health. These methods of transformation may be adapted according to the actual research question, type of data, and analytical needs.
Data Conversion
Statistical software was used to test the normal distribution of the recovered data, numerical values were used for descriptive and statistical purposes, and gender was chosen as the moderator variable. In multi-cluster analysis, various parameters need to be restricted to find out the most suitable model, through the comparison of the suitability of six models, namely, the preset model, the path coefficient equality model, the covariance equality model, the model invariance, and the variance equality model, and finally the measurement error model model was selected as the analytical model. Exploratory factor analysis KM0 values of 0.82 (T1) and 0.88 (T2), Bartlett’s test of sphericity, approximate X2=409.878, df=5, P<0.01 (T1) and approximate X2=413.617, df=5, P<0.01 (T2) were used to analyse the data using AMOS 21.0 with SPSS.
Literature Review and Hypothesis
Risk perception and physical activity are two topics that have received a lot of attention in the field of adolescent mental health. Many studies have shown that risk perception plays an important role in adolescent mental health. Risk perception theory emphasises that an individual’s perception of risk can significantly influence their behavioural choices and coping strategies.7 In the context of adolescents, a high perception of risk may lead to excessive anxiety and stress, which in turn affects their mental health status.8
On the other hand, the Health Belief Model asserts that people’s health behaviours (including mental health behaviours) are influenced by their perceptions of the threat of illness (both perceptions of the likelihood of illness and perceptions of the severity of illness).9 In the context of adolescents, this may manifest itself in perceptions of risky behaviours (eg, substance abuse, unprotected sex, etc.), which may influence their mental health. Thus, both theories provide a theoretical basis for understanding the role of risk perception in adolescent mental health. High risk perception may lead to excessive anxiety and stress, which may negatively affect mental health. At the same time, low risk perception may cause adolescents to be too bold and engage in behaviours that may harm their mental and physical health. Therefore, we propose the following hypotheses
H1: There is a negative correlation between risk perception and mental health, ie, the higher the risk perception, the worse the mental health.
Meanwhile, physical activity has been shown to have a positive impact on improving mental health. The theoretical basis for the positive effects of physical activity on mental health is mainly derived from the Biopsychosocial Model and Self-Determination Theory. The Biopsychosocial Model emphasises the influence of physiological, psychological and social factors on an individual’s health.10 Within the perspective of this model, physical activity is viewed as a powerful physiological factor that can lead to increased mental health by improving physical health.11 Physical activity can help reduce stress levels, increase self-efficacy, and improve mood states, all of which contribute to improved mental health. Whereas in self-determination theory asserts that an individual’s behavioural choices are influenced by both intrinsic and extrinsic motivation.12 In the context of physical activity, an individual’s intrinsic motivations, such as having fun and improving skills, can drive their continued participation in exercise, a self-driven activity process that is inherently conducive to improved mental health.13 Regular physical activity reduces stress levels, increases self-confidence, improves mood, and increases self-efficacy, all of which are positive mental health indicators for adolescents.
Therefore, we propose the following hypothesis
H2: There is a positive correlation between physical activity and mental health, ie the more frequent the physical activity, the better the mental health.
The relationship between risk perception and physical activity has been explored in several studies. In particular, high perceptions of risk may influence adolescents’ willingness and behaviour to engage in physical activity. This is because risk perception may play a key role in the decision to participate in physical activity. For example, if adolescents are hypersensitive to the risk of sports injuries, they may become alienated from physical activity.14 In addition, a high level of risk perception may lead them to choose safer, less risky activities.15 Therefore, understanding adolescents’ risk perception is essential for predicting and explaining their physical activity behaviour. It is also possible that for adolescents with higher perceived risk, physical activity may have a greater positive impact on their mental health.
H3: There is a negative correlation between risk perception and physical activity, ie, the higher the risk perception, the lower the likelihood that adolescents will be physically active. H4: Risk perception and physical activity may have an interaction effect on mental health.
In summary, both risk perception and physical activity have important effects on adolescents’ mental health. Research can explore how to balance the relationship between risk perception and physical activity to achieve better mental health outcomes.
Results
Common Method Bias Test
In order to avoid the bias of the two surveys to the unity dimension, the strength of the procedure and Harman one-way test were used to measure the questionnaire form through the questionnaire star for the network distribution and bolding in the stem and title. T1 and T2 extracted seven characteristic root factors greater than 1, and the eigenvalues of the primary factors were counted as T1=19.323% and T2=21.542%. According to the principle of the common method bias test, the primary characteristic explanation rate is less than 40%, which means that the common method bias of the survey test can be accepted.
Results of Direct Relationships
Independent samples t-tests were used to examine gender differences in the variables (Table 1), which showed that there were stable gender differences in mental health (p<0.001), risk perception (p<0.001), and physical activity (p<0.001) over time spans for both T1 and T2, and combined with a comparison of the means in Table 2, it was found that males reported higher scores in mental health than females, while females had higher levels of mental health than females in the two repetitions of the test risk perception levels were higher for women than for men. The measured gender-specific effect sizes were 0.159 (d=0.262) and 0.179 (d=0.278) for the two administrations of the mental health level, and 0.255 (d=0.416) and 0.195 (d=0.402) for the two administrations of the risk perception level, respectively.
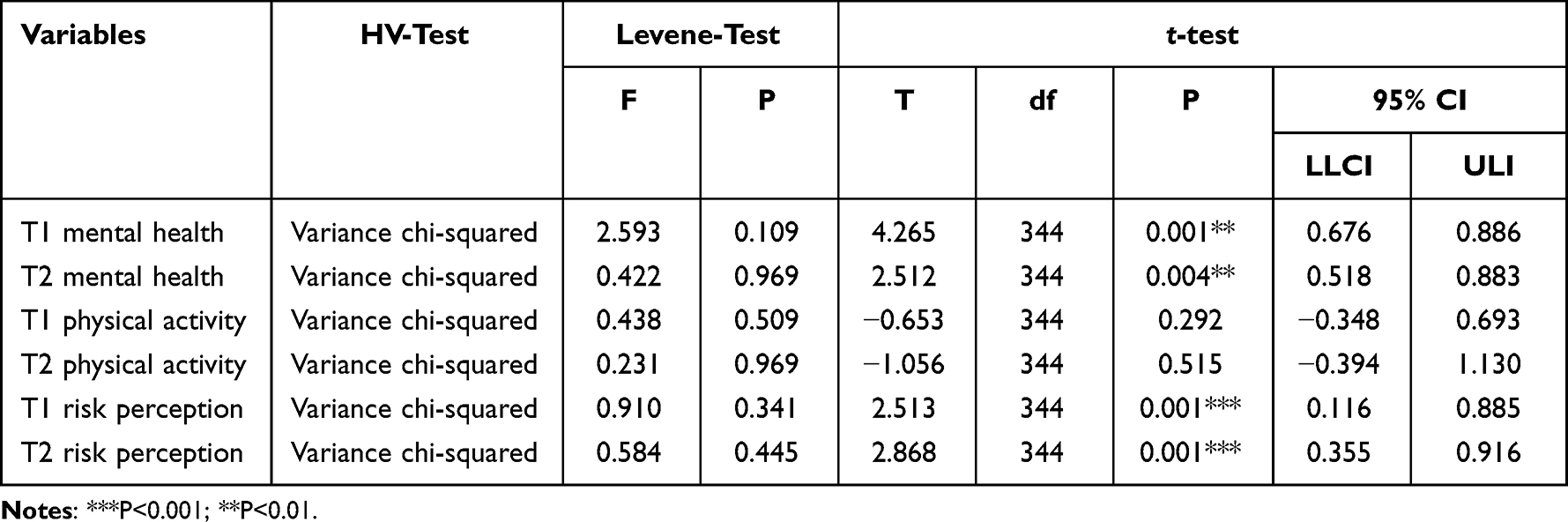 |
Table 1 Gender-Independent Sample t-test |
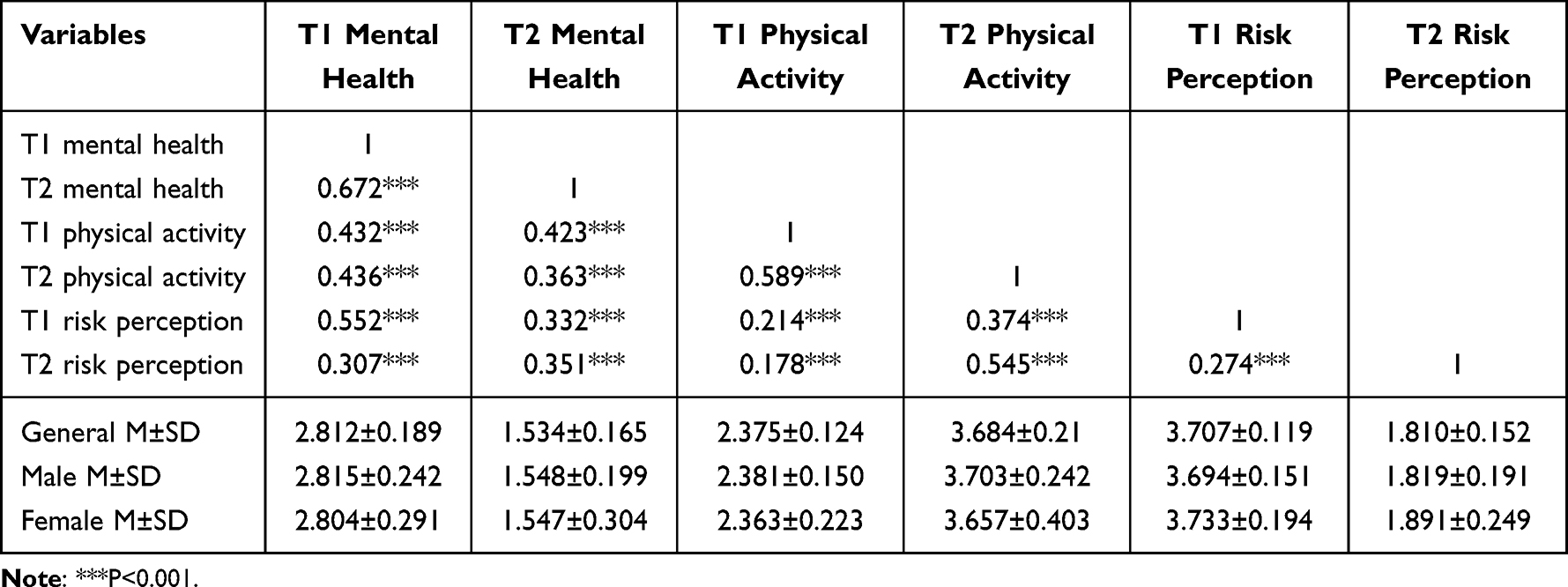 |
Table 2 Results of Descriptive Statistics and Partial Correlation Analysis for Each Variable |
In order to eliminate the interference of factors in demographic variables, partial correlation analyses were conducted on the three elements of mental health, physical activity, and risk perception, and gender was added for comparison, in an effort to achieve more precise findings (Table 2). The results showed that T1 mental health and T2 mental health (r=0.672), T1 physical activity and T2 physical activity (r=0.589), and T1 risk perception and T2 risk perception (r=0.274) were all significantly and positively correlated (P<0.001). In the first survey, T1 mental health, T1 physical activity and T1 risk perception were positively correlated (P<0.001), and in the second survey, T2 mental health, T2 physical activity and T2 risk perception were also positively correlated (P<0.001), which indicated that the recovered data were stable and synchronised over the time span.
Results of Mediation and Indirect Relationships
Cross-lagged analysis of risk perception, physical activity and mental health of adolescents, through the pre-correlation analysis and bias scores in accordance with the packaged dimensionality reduction technique, the use of AMOS25.0 statistical software to build data models (Figure 1), in the cluster analysis, it is necessary to limit the various parameters to find out the most suitable model, through the pre-determined model, path coefficient equality model, covariance equality model, model invariance, and variance-equivalent model six models of fitness comparison, and finally choose the measurement error model model as the analysis model. The data fit well to the model, X²/df = 1.713 (P < 0.01); absolute fit index RMSEA = 0.082; relative fit index CFI = 0.911, GFI = 0.931, NF1 = 0.935, IF1 = 0.959, and TLI = 0.956, and the three variables of risk perception T1, physical activity T2, and mental health T2,3 were constructed into separate mediation effect models. Variables to construct a separate mediation effect model, using Bootstrap method to test the mediation effect of physical activity T2 between risk perception T1 and mental health T2, the root of Bootstrap method is to analyse the correlation of a*b. On the one hand, the Sobel test is adopted, in the Sobel test the data requirements are high, the sample size needs to be large and conform to normal distribution, so the efficiency of this method of testing is low. On the other hand, the original sample sampling test test method. Bootstrap sampling method is the more mainstream test method due to its high efficiency, and sampling method has no restriction on the mediating effect sampling distribution law. Bootstrap sampling method is based on repeated sampling of the original sample, and the significance of the coefficients of the mediating effect through the 95% confidence intervals (CI) to test. Hayes (2009) suggested that in Bootstrap mediated effects test, the original sample is repeatedly sampled up to 1000 times. If the results of Bootstrap mediated effects test indicated that Bootstrap test CI does not contain a value of 0, the indirect effect starts to operate (Chen et al, 2013). In this study, the mediation effect test was conducted based on 1000 times of sampling of the sample to calculate the mediation effect Bootstrap 95% CI. The point estimate of the direct effect of risk perception T1 → physical activity T2 → mental health T2 is 1.010, the mediator effect is 0.012, the Z-value is 0.112, and the indirect effect Bootstrap 95% CI generated by this path is not 0 value, which indicates that the mediating effect of physical activity is significant between risk perception and mental health.
 |
Figure 1 Model of cross-lagged effects of risk perception physical activity and mental health in adolescents. |
The results showed that mental health T1 had a statistically significant effect on physical exercise physical exercise T2 (β=0.08), physical exercise T1 had a statistically significant effect on mental health health T2 (β=0.33), and risk perception T1 had a statistically significant effect on mental health T2 (β=0.28) and physical exercise T2 (β=0.19). The effects of mental health T1 (β=−0.01) and physical activity T1 (β=−0.27) on risk perception T2 (p>0.05) were not statistically significant.
According to the results of the data study, there are gender differences in risk perception and mental health among adolescents. This may indicate a relationship between risk perception and mental health. Especially in the context of social diseases, adolescents’ fear of outdoor physical activity may trigger mental health problems. In addition, a positive correlation was found between physical activity and mental health, ie, physical activity T1 predicted mental health T2 (β = 0.33, p < 0.01), supporting the H2 hypothesis that the more frequent the physical activity, the better the mental health. However, the higher the adolescents’ risk perception, the lower the likelihood of physical activity, ie, risk perception T1 was able to predict physical activity (β = 0.28, P < 0.01), which supported hypothesis H3, ie, the higher the risk perception, the lower the likelihood of adolescents’ physical activity. Finally, it was found that risk perception and physical activity may have an interaction effect on mental health, ie, the path of risk perception T1→physical activity T2→mental health T2 produced a significant indirect effect, indicating that the mediating effect of physical activity between risk perception and mental health was significant, which supported hypothesis H4. Meanwhile, the higher the risk perception, the worse the mental health, which supports the H1 hypothesis.
Discussion
This study explored the relationship between risk perception, physical activity, and mental health among adolescents in high school. The results of the study indicated that there was a weak positive correlation between the three. Specifically, risk perception T1 predicts physical activity T2 and mental health T2, while physical activity T1 predicts mental health T2. This is consistent with the findings of the existing literature that there is a positive correlation between adolescents’ levels of risk perception and physical activity and mental health16 At the same time, the results of the analyses indicate that female adolescents are higher than male adolescents in risk perception scores, which is also in line with other scholars’ research. It has been suggested that this may be due to the fact that males are more likely to engage in physical activity, which in turn promotes physical health and mental health.17 There are several potential reasons why female adolescents may have stronger risk perceptions than males. One possible explanation is that females tend to have more developed empathy, which may lead them to be more aware of potential dangers and risks in their environment. In addition, social and cultural factors may play a role, as females are often socialised to be more cautious and aware of potential dangers. Research also suggests that girls tend to be exposed to more risk information and receive more safety-related messages compared to boys. Males are less worried about viral infections compared to females, females perceive a shorter period of time for the disease to end than males, and female adolescents have high risk perceptions of viral susceptibility partly because they are dissatisfied with the government’s release of information in real time, the speed of emergency preparedness, and the implementation of integrated prevention and control. Therefore, future research could explore ways to promote female participation in physical activity to improve their physical and mental health. In addition, this study found gender differences in risk perception among adolescents. Specifically, females had higher levels of risk perception than males. This is different from the findings of previous studies, and it has been suggested that this may be due to the fact that females are more concerned about their safety and risks.18 Psychological problems resulting from risk perception in adolescents are closely related to gender as well as the social messages they are exposed to.
Regression analyses showed that adolescent risk perception has an impact on mental health, a result that goes in line with previous results. The study suggests that those with higher risk perceptions tend to experience more anxiety,19 depression and stress. Adolescents may be particularly vulnerable to the impact of social illness risk on their mental health due to disruptions to their daily lives and social networks, as well as the uncertainty and fear caused by illness. Increased risk perception among adolescents can lead to increased anxiety, worry, and fear, which can negatively impact their mental health. In addition, adolescents with high risk perceptions may be more likely to adopt maladaptive coping strategies, the Mental health exists in the form of a person’s cognitive reappraisal, emotional regulation, and volitional shaping processes.20 The analysis of cognitive reappraisal through distraction theory found that attention is the pointing and focusing of mental activity on a certain object, which has the characteristics of both pointing and focusing, and when an individual points and focuses his or her consciousness on a certain activity, his or her awareness of everything around him or her decreases accordingly.21 According to the distraction theory, exercise can divert and disperse an individual’s attention from unfavourable stimuli, ignore negative stimuli and focus on positive stimuli, thus achieving the effect of mood improvement. From this perspective, the individual’s attentional cognitive resources are limited, and when cognitive resources are completely occupied, new stimuli will not be processed.22 When individuals allocate cognitive resources to important activities, such as immersing themselves in exercise, negative emotions are excluded from attention, and individuals will only experience the positive feelings brought about by exercise. A reappraisal of novel cognitions will then occur, thus shifting the focus of attention on the negative event, which is effective in improving anxiety and depression in students. Secondly the social interaction theory for emotion regulation found that the inherent social relationships prevalent in physical activity,23 as well as the mutual support between individuals involved in exercise, play an important role in the effects of exercise on mental health. There is a positive effect of social support on mental health.
Using a longitudinal design scheme and a typical quasi-experimental study-cross-lagged analysis, the present study explored the intrinsic relationship between adolescent risk perception, physical activity, and psychological well-being at the high school level,24 and the conclusions obtained are of some relevance in shedding light on the influence of social factors on the shaping of adolescents’ psychological well-being. Admittedly, this study only covered adolescents at the high school level and did not include adolescents at the elementary and middle school levels as a study group. In the future, the scope of the study should be expanded to examine the individual differences of adolescents in different stages of schooling, in order to grasp the characteristics of adolescents’ mental activities in a comprehensive manner.
Conclusion
The results of this study suggest that there is a longitudinal causal relationship between disease risk perception, physical activity and mental health among adolescents. In particular, female adolescents had higher risk perception scores than male adolescents, which may be due to the fact that females tend to have more developed empathy, making them more aware of potential dangers and risks in their environment. Social and cultural factors may also play a role, as females are often socialised to be more cautious and aware of potential dangers. In addition, girls tend to be exposed to more risk information and receive more safety-related messages than boys.
However, male adolescents have better physical activity behaviours than females, possibly because physical activity helps them cope better with stress and anxiety. Adolescent risk perception has implications for mental health, with those with higher risk perception tending to experience more anxiety, depression and stress. Adolescents may be particularly vulnerable to the impact of social illness risk on their mental health due to disruptions to their daily lives and social networks, as well as the uncertainty and fear caused by illness.
We therefore need to pay more attention to the mental health of adolescents, especially when at risk of illness. We need to provide more information and support to help them understand and cope with risk, as well as encourage them to engage in physical activity to improve their mental health. These findings are of great value to our understanding of adolescent mental health and risk perception, and provide us with possible ways to improve adolescent mental health.
Data Sharing Statement
Data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Statement
I, as the principal investigator of this study, hereby solemnly declare that my study “Cross-lagged analysis of the relationship between risk perception, physical activity, and adolescent mental health” of study design, implementation, and evaluation have strictly followed the requirements and guidelines of the Declaration of Helsinki.
My research plan has been appropriately reviewed and approved by the ethics review board of my academic institution. All subjects have voluntarily chosen to participate in the study after being informed about the content, intent, possible risks and benefits of the study. We assured all participants that they had the right to withdraw at any time during the study and would not face any negative consequences.
In our research, the rights and well-being of young students are paramount. We respect their privacy and are committed to keeping their personal information confidential under all circumstances. We will use our best efforts to prevent data breaches and ensure data security.
All research activities are designed to gain scientific knowledge about the relationship between adolescent risk perception, physical activity and mental health in order to advance the understanding of adolescent health development and improve appropriate health strategies and interventions, without compromising any of the adolescent’s rights.
The results of this study will be reported in a scientific, fair and truthful manner without any falsification or misrepresentation of data.
I hereby promise that all research activities will be based on respect for human dignity and rights, and respect for scientific truth and impartiality. I will make every effort to follow the highest ethical and professional standards to ensure that I have conducted and reported my research in full compliance with the spirit and requirements of the Declaration of Helsinki.
Acknowledgments
Many thanks to the second author, Ying Wang, for providing the data collection and the support from various high school units.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Fischhoff B. Risk perception and communication unplugged: twenty years of process 1. Risk Analysis. 1995;15(2):137–145. doi:10.1111/j.1539-6924.1995.tb00308.x
2. Biangyuan L. A review of domestic trauma theory research in the past five years. J Guangdong Instit Petrochem Technol. 2017;27(2):30–32.
3. LaCaille LJ, Hooker SA, Marshall E, LaCaille RA, Owens R. Change in perceived stress and health behaviors of emerging adults amid the COVID-19 pandemic. Ann Behav Med. 2021;55(11):1080–1088.
4. Gao Y, Fu N, Mao Y, Shi L. Recreational screen time and anxiety among college athletes: findings from Shanghai. Int J Environ Res Public Health. 2021;18(14):7470. doi:10.3390/ijerph18147470
5. Doree RE. The relationship between cell phone use and motivation to exercise in college students. The University of North Dakota; 2019.
6. Yufu D. A study on the relationship between physical activity status and psychological health of college students. China Health Educ. 2005;21(6):468–470.
7. Fang C, Huang B. A new species of the genus Pseudococcus (Hymenoptera, Braconidae) from China: Can physical activity promote adolescents' cognitive development? --An empirical study based on data from the China Education Tracking Survey. Journal of East China Normal University (Education Science Edition. 2011;39(3):84.
8. Qiu F, Cui DG, Yang J. Examination and revision of the Exercise Commitment Scale (ECS) in the context of physical activity among Chinese university students. J Wuhan Institute Phys Educ. 2013;46(12):51–58.
9. Xiaoqian C, Yanhua H, Siyu T, et al. 2011 A new species of the genus Cicilia (Hymenoptera, Ichneumonidae) from China. Reliability testing and application of the new coronary pneumonia risk perception scale - an empirical study based on a large data sample. Chine Public Health. 2021;37(7):1086–1089.
10. Zhou H, Long LR. A statistical test and control method for common method bias. Adv Psychol Sci. 2004;12(6):942–950.
11. Zewei M, Quan P. The mediating role of depression in the relationship between core self-evaluation and suicidal ideation in adolescents: an empirical study based on the Bootstrap and MCMC methods. Psychol Sci. 2015;38(2):379–382.
12. Liu B, Liu H, Han B, et al. Trends and factors associated with risk perception, anxiety, and behavior from the early outbreak period to the controlled period of the COVID-19 epidemic: four cross-sectional online surveys in China in 2020. Front Public Health. 2022;9:2028. doi:10.3389/fpubh.2021.768867
13. Hagan JE Jr, Quansah F, Frimpong JB, Ankomah F, Srem-Sai M, Schack T. Gender risk perception and coping mechanisms among Ghanaian university students during the COVID-19 pandemic. MDPI. 2022;10(4):687.
14. Brown GD, Largey A, McMullan C. The impact of gender on risk perception: implications for EU member states’ national risk assessment processes. Int J Dis Risk Reduction. 2021;63:102452. doi:10.1016/j.ijdrr.2021.102452
15. Cuesta A, Alvear D, Carnevale A, Amon F. Gender and public perception of disasters: a multiple hazards exploratory study of EU citizens. Safety. 2022;8(3):59. doi:10.3390/safety8030059
16. Xia X, Liu S. An empirical study on physical activity behavior of postgraduate students in colleges and universities. J East China Normal Univ. 2018;36(5):114–128.
17. Wang CS, Yan JH. The relationship between perceived risk of new coronary pneumonia epidemic and physical activity and mental health among college students. School Health China. 2022;43(11):1664–1667.
18. Liu Z, Li M, Ren C, Zhu G, Zhao X. Relationship Between Physical Activity, Parental Psychological Control, Basic Psychological Needs, Anxiety, and Mental Health in Chinese Engineering College Students During the COVID-19 Pandemic. Front Psychol. 2022;13:802477.
19. Coulter KS. Intimidation and distraction in an exercise context. Int J Sport Exercise Psychol. 2021;19(4):668–686. doi:10.1080/1612197X.2020.1739108
20. Falsafi N. A randomized controlled trial of mindfulness versus yoga: effects on depression and/or anxiety in college students. J Am Psychiatr Nurses Assoc. 2016;22(6):483–497. doi:10.1177/1078390316663307
21. Dour HJ, Wiley JF, Roy‐Byrne P, et al. Perceived social support mediates anxiety and depressive symptom changes following primary care intervention. Depress Anxiety. 2014;31(5):436–442. doi:10.1002/da.22216
22. Rueger SY, Malecki CK, Pyun Y, Aycock C, Coyle S. A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychol Bull. 2016;142(10):1017. doi:10.1037/bul0000058
23. Xu T, Shao M, Liu R, Wu X, Zheng K. Risk Perception, Perceived Government Coping Validity, and Individual Response in the Early Stage of the COVID-19 Pandemic in China. Int J Environ Res Public Health. 2023;20(3):1982.
24. Skaalvik C. School principal self-efficacy for instructional leadership: relations with engagement, emotional exhaustion and motivation to quit. Soc Psychol Educ. 2020;23(2):479–498. doi:10.1007/s11218-020-09544-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.